Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Predictors of Passive and Active Suicidal Ideation and Suicide Attempt Among Older People: A Study in Tertiary Care Settings in Thailand
Authors Booniam S, Wongpakaran T ![]() , Lerttrakarnnon P
, Lerttrakarnnon P ![]() , Jiraniramai S, Kuntawong P, Wongpakaran N
, Jiraniramai S, Kuntawong P, Wongpakaran N ![]()
Received 20 September 2020
Accepted for publication 8 December 2020
Published 17 December 2020 Volume 2020:16 Pages 3135—3144
DOI https://doi.org/10.2147/NDT.S283022
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Taro Kishi
Somboon Booniam,1 Tinakon Wongpakaran,1 Peerasak Lerttrakarnnon,2 Surin Jiraniramai,2 Pimolpun Kuntawong,1 Nahathai Wongpakaran1
1Department of Psychiatry, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 2Department of Family Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Correspondence: Nahathai Wongpakaran
Geriatric Psychiatry Unit, Department of Psychiatry, Faculty of Medicine, Chiang Mai University, 110 Intawaroros Road, T. Sriphum, A. Muang, Chiang Mai 50200, Thailand
Tel +66 53 93 5422 ext 320
Fax +66 53 93 5426
Email [email protected]
Purpose: This study compared predictors of passive suicidal ideation (SI), active SI, and suicide attempt (SA) among elderly Thai patients in tertiary care settings.
Patients and Methods: Psychiatric diagnoses and suicidality of 803 older people were assessed using the Mini-International Neuropsychiatric Interview and the Structured Clinical Interview for DSM-IV-TR. All participants completed the Montreal Cognitive Assessment, multidimensional scale of perceived social support (MSPSS), 15-item Thai geriatric depression scale (TGDS-15), 10-item perceived social scale and the Core Symptoms Index. The chi-square test, t-test and ANOVA were used for bivariate analysis of predictors of specific suicidality types. Multiple logistic regression was used to determine the predictors for each type of suicidality.
Results: The patients’ mean age was 69.24 ± 6.90 years, and the majority were female (69.74%). Passive SI, active SI and SA were found among 20.42%, 3.74% and 2.37%, respectively, of the patients. Major depressive disorder (MDD) was a predictor of both passive and active SI (OR = 2.06 and 3.74, respectively). Other predictors of passive SI included hypomania (OR = 8.27) and positive score on the TGDS-15 (OR = 1.29). Predictors of active SI included agoraphobia (OR = 6.84) and hypomania (OR = 7.10). Predictors of SA included a family history of alcohol dependence (OR = 14.16), a history of depression (OR = 4.78) and agoraphobia (OR = 19.89). Surprisingly, hypertension and self-reported anxiety symptoms were protective factors for passive SI (OR = 0.51 and 0.85, respectively). Likewise, MSPSS was a protective factor for SA (OR = 0.90).
Conclusion: Predictors of each type of suicidality differed. MDD was the main predictor for SI; however, agoraphobia and poor perceived social support were more pronounced among individuals with SA. Further investigation, especially in longitudinal fashion, should be warranted.
Keywords: suicide, elderly, risk, predictor
Introduction
Suicide is a major mental health problem and more prevalent among older people1 with the highest rate among those aged 70 years or older.2 Different forms of suicidal behavior include suicidal ideation (passive or active), suicide planning, attempting suicide and committing suicide.3 SI is thinking about killing oneself, while a SA is the behavior in which one attempts to kill or cause injury to oneself. Suicide results in death from self-killing behavior.4 Passive SI is a wish to die, denoting the earliest stage of suicidality. Active SI is defined as thoughts that involve an existing wish to die accompanied by a plan to carry out the death. A European study found that cultural acceptance of suicide, religiosity and intergenerational cohabitation were predictors of passive SI among older adults.5 Growing evidence shows that individuals who have passive SI in later life may not have clinical depression.6
The rate of suicide among older adults ranges from 8.32 (in Thailand) to 140 (in China) per 100,000 populations.7,8 The prevalence of SI in European countries ranges between 6.9% (in Italy and the Netherlands) and 21.1% (in France).5 A global study found that the rates of SI and SA over 12 months were 2% and 0.5%, respectively.9 Prevalence was as high as 1.81% for SI and 0.41% for SA during the economic crisis (from 2011 to 2012) in Spain.10 In Asian populations, the lifetime prevalence of any SI among older people residing in Sri Lanka was 13.0% (11.7% to 14.3%) for men and 21.8% (20.3% to 23.2%) for women, with no significant difference between twins and nontwins.11
Related research found that males had a higher risk of SA than females.7,12 However, one study reported no difference existed between males and females.7,12 Factors associated with SA included separation from a spouse, education ≥6 years, residential areas (urban) and physical diseases such as cancer, neurologic disorder, pain, liver disease, genital disorders or rheumatoid disorders.13
Regarding suicidal thoughts, females were prone to higher risk of SI than males.9,13 Variables associated with SI included area of residence, separation/divorce, higher education, losing a parent while young, low standard of living and stressful life events in the preceding 12 months, perceived poor health, poorer cognitive functioning and consuming alcohol (but only among males).11,13,14 Other studies have found that a low level of education, being widowed, living alone, being in a nursing home, having financial problems and disability were related to SI among older adults.9,10
Having psychiatric disorders, especially anxiety disorder, increases the risk of SA.15,16 Depressive disorders and depressive symptoms were the most influential predictors of SI.10,11,17–19 Disorders such as alcohol use disorder, panic symptoms, early-onset fearful panic attacks, intense anxiety, sleep disturbances, a past history of suicide, a history of physical illness, chronic diseases and disabilities were also associated with SI.9,20–22
Among older people, psychosocial variables have been found to be related to suicidality, including personality traits, feelings of isolation, hopelessness, desperation, negative affect and perceived stress and lack of support. Older people who have attempted suicide have scored higher on the neuroticism scale than nonsuicidal older people who have attempted suicide.22–25 Similar results have been found for SI, with older people who have suicidal thoughts showing high neuroticism and low extraversion.26 All Diagnostic and Statistical Manual (DSM)-personality disorders are related to SI, except for histrionic personality.27 However, correlations between personality disorders and SA remain undemonstrated.
Few studies have compared predictors between passive SI, active SI and SA, especially among older people, so understanding predictors is important to plan interventions. Therefore, this study aimed to examine variables that predict each type of suicidality among older people receiving services at psychiatric clinics in tertiary care hospitals. Based on related research, the variables evaluated in this study included sociodemographic variables, clinical variables such as psychiatric disorders rated by clinicians, and variables in self-reporting questionnaires including personality traits, perceived stress, perceived social support, anxiety and depression.
Patients and Methods
This constituted a secondary analysis of the Depression, Anxiety, and Suicidality (DAS) database.28 The research was approved by the Thailand Central Research Ethics Committee and the Institutional Review Board of each hospital. Informed consent was obtained from all participants. The DAS was conducted in accordance with the Declaration of Helsinki.
DAS was a multi-center study conducted between January 2012 and April 2013 at four tertiary care hospitals in Thailand, ie, two university hospitals, one psychiatric hospital and one neurologic hospital with geriatric psychiatry services. The participants comprised 803 elderly Thai residents, who were new patients presenting symptoms such as anxious mood, loss of interest, sleep problems, eating problems, fatigue, memory problems or inability to explain physical symptoms. The criterion for inclusion was age 60 years or older. Patients with severe physical illness, ie, dyspnea, disorientation, severe substance addiction, inability to complete the questionnaires, schizophrenia, severe manic episode affecting the completion of questionnaires or communication with researchers, or schizoaffective disorders were excluded. All participants were assessed according to DSM-IV-TR using Mini-International Neuropsychiatric Interview (MINI) and SCID-I (dysthymia). Patients were divided into three groups as passive SI, active SI and SA.
Information on sex, years of education, marital status, monthly income, psychiatric illness, family history of psychiatric disorder and history of substance use was collected. All participants were assessed using the MINI for psychiatric diagnoses. SCID–I was used for diagnosing dysthymia due to the low kappa value for dysthymic disorder in the Thai MINI. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), and neuroticism personality trait was also assessed. Self-rating of perceived social support and perceived stress was evaluated. Self-reporting symptoms included depression and anxiety assessed using the Thai Geriatric Depression Scale-15 (TGDS-15) and the Core Symptom Index.
Instruments
Mini-International Neuropsychiatric Interview
The MINI is a semi-structured interview used to diagnose DSM-IV psychiatric disorders and suicidality. The level of risk was assessed for suicide using the MINI. Suicide was assessed using Module C of the MINI to determine suicide risk categorized from low to high. The risk was assessed during the past months. Passive SI was reflected by the item, “think that you would be better off dead or wish you were dead”. Active SI was reflected by items, “want to harm, hurt or injure yourself”, “think about suicide” and “have a suicide plan”. The Thai version of the MINI has been validated and is used widely. The inter-rater reliability of each psychiatric diagnosis was acceptable, except for dysthymic disorder.4
Structured Clinical Interview for DSM or SCID-I (P)
The SCID-I/P was used to evaluate dysthymia. The reliability of SCID-I was 0.35 to 0.81.29 In this study, the interrater reliability of the SCID-I (dysthymia) ranged from 0.95 to 1.0.
Multidimensional Scale of Perceived Social Support (MSPSS)
MSPSS is a tool to measure social support perceived by an individual from significant others, friends and family members. It consists of 12 questions,30 and the answers are rated using a 7-point scale, with 1 = very strongly disagree to 7 = very strongly agree. The total score ranges between 12 and 84 points. The higher the score, the greater would be the social support. The Thai version has an excellent Cronbach’s alpha coefficient for the total scale and for each subdomain.31 Its structure has been studied in an elderly population with depression,32 and the Cronbach’s alpha coefficient was 0.89 in this study.
Neuroticism Inventory (NI)
NI is a self-rating inventory to detect the neuroticism personality trait using the five-factor model.28 This rating scale has 15 items, with responses ranging from 1 (the most unlike the respondent) to 4 (the most like the respondent). The reliability was good for older people,28,33 and Cronbach’s alpha coefficient was 0.80 in this study.
MoCA
MoCA evaluates 11 domains of cognitive function, is used to measure mild cognitive impairment (MCI) and gives a total score of 30. The Thai version uses a cut-off score of 25. The Cronbach’s alpha coefficient was 0.74 in this study, with a sensitivity of 0.70 and specificity of 0.95 for MCI.34
Fifteen-Item TGDS-15
TGDS is a widely used, self-reporting assessment of depressive symptoms within the past week among older people. The cut-off score of the Thai version is similar to that of the original version with a sensitivity of 0.92 and specificity of 0.87. Major depression was evaluated in a geriatric outpatient clinic. Cronbach’s alpha coefficient was 0.81 for this study.35
Core Symptom Index (CSI)
CSI assesses anxiety and depression. It demonstrates excellent reliability among older people, either cognitively intact or cognitively impaired, with a Cronbach’s alpha of 0.91.36,37 CSI provides a high level of sensitivity and specificity (100% and 90.32%, respectively) for SI as measured by MINI. It consists of 15 questions with a 5-point rating scale ranging from 0 (never) to 4 (almost always). The higher the score, the higher would be the level of severity.35 In this study, the Cronbach’s alpha was 0.84.
Ten-Item Thai Perceived Stress Scale (T-PSS-10)
PSS is a self-reporting tool evaluating a person’s perceived stress. Ten questions cover perception in the past month. It uses a 5-point Likert scale, with 0 = never to 4 = very often. The total scores of the stress perception questionnaire range from 10 to 40 points. The higher the score, the higher would be the perceived stress level.38 In this study, the Cronbach’s alpha was 0.85.
Data Analysis
Descriptive statistics, eg, mean, percentage and standard deviation, were used to analyze demographic information such as sex, age, education level, etc. and scores of psychosocial variables, eg, MSPSS, T-PSS-10, etc. To examine normality of the variables, skewness and kurtosis were calculated. All variables showed skew and kurtosis values ranged from −0.704 to 1.603, indicating acceptable normality. t-test and ANOVA were used to compare each continuous variable, such as MPSS and MoCA scores, in each type of suicidality, ie, passive SI, active SI and SA, while the chi-square test was used to compare each categorical variable for each type of suicidality. Homogeneity of variance, an assumption of the t-test, was investigated.
Multiple logistic regression was used to find the predictors of each type of suicidality. Only variables that were significant in bivariate analyses were included in the logistic regression models. The enter method of logistic regression was adopted. Multicollinearity related to the high correlation of independent variables was not observed. The Hosmer‐Lemeshow test was used to determine the goodness‐of‐fit for the logistic regression model, and all showed the p-value >0.05, indicating all the models were correctly specified. Results are expressed as odds ratios (ORs) with 95% confidence intervals (95% CIs). The percentage of variance explained by each model was calculated using pseudo R2 indicated by McFadden. The Firth's procedure was applied for logistic regression for rare events. Missing data in MINI Module C were excluded from the analysis. The statistical significance level was set at p< 0.05. All analyses were performed using IBM SPSS Version 22, and Stata, Version 15.
Results
The mean age of the 803 participants was 69.24 years (SD = 6.90). The majority were young to old (60 to 74 years old) and female (69.74%). The prevalence of passive SI, active SI, and SA was 20.42%, 3.74% and 2.37%, respectively.
Sociodemographic Predictors
The three groups differed significantly in age, with those with passive SI being older than the others. The average age of the SA group was less than that of the SI group. A significant difference was found in the number of years of education between passive SI and active SI while SA revealed no difference. Significant differences in income and marital status were found only in passive SI (Table 1).
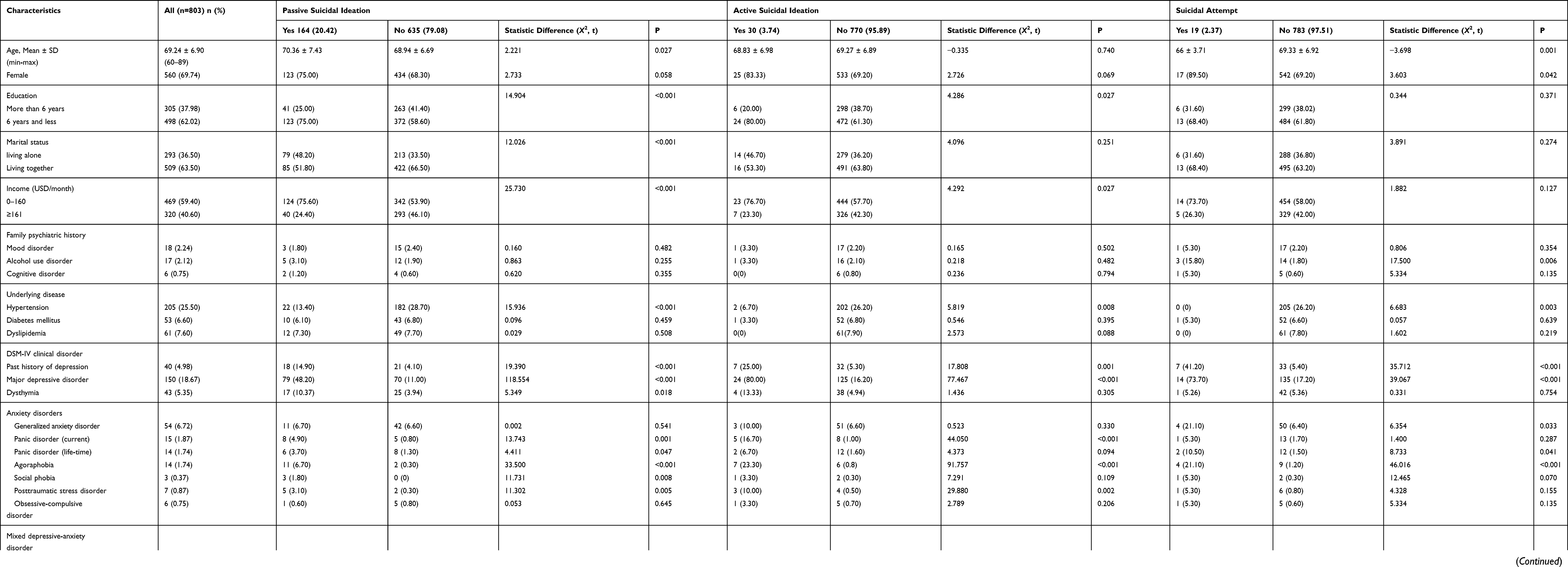 |
Table 1 Demographic Data of Respondent Patients |
Medical and Clinical Psychiatric Disorders
The number of participants who had hypertension was significantly less in the control group than in the suicidality group. The prevalence of major depressive disorder, as well as of a past history of depressive disorder, was high in all suicidality groups while anxiety disorders were more common in the passive SI group than in the other groups. Anxiety disorders found to be predictors included panic disorder, agoraphobia, social phobia and posttraumatic stress disorder. Current mania and current hypomania were found in both passive SI and active SI groups; the same was obtained using MoCA (Table 1).
Psychosocial Predictors
In the psychosocial variable group, all variables significantly differed between suicidality and nonsuicidality groups. As expected, the suicidality group perceived a low level of social support and high level of stress, showed a high level of neuroticism and self-reported a high level of depression and anxiety.
Predictors of Passive SI, Active SI and SA
Multiple logistic regression showed that passive SI was found to have more predictors than the other groups. Interestingly, hypertension was a protective factor for passive SI (OR = 0.51, 0.28 to 0.93) as well as anxiety symptoms reported by the patients (OR = 0.85, 0.77 to 0.93). Major depressive disorder was a predictor of SI, but not of SA. A family history of alcohol consumption and agoraphobia were significant predictors of SA. Notably, perceived social support was a significant protective variable for SA (OR = 0.92, 0.86 to 0.97; Table 2). All model Χ2 was significant (p < 0.05). In terms of the percentage of variance explained by each model, for PSI, McFadden was 0.330. For ASI, McFadden was 0.553. For SA, McFadden was 0.298.
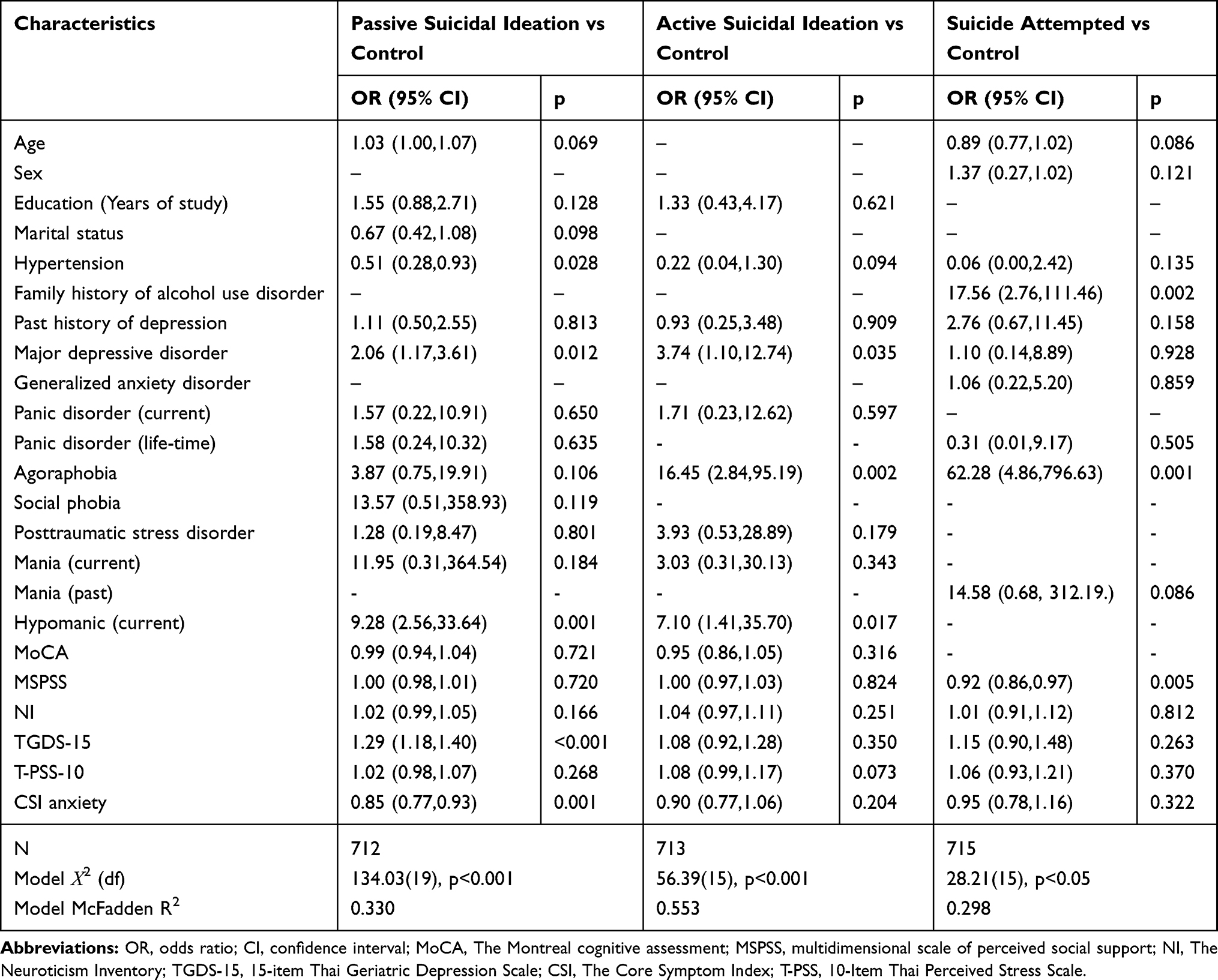 |
Table 2 Logistic Regression Model Predicting Suicidality |
Discussion
To the best of our knowledge, this study was one of the few to explore the predictive factors of suicidal behaviors among elderly patients attending psychiatric services for the first time in tertiary care settings. Unexpectedly, passive SI was the most common, followed by active SI and SA. Our findings were consistent with a related study in a Spanish community that found a prevalence of 1.81% for SI and 0.41% for SA.10 However, the fact that the present study found a higher rate of suicidality may have been due to being conducted in a tertiary care setting where older people came for psychiatric services because they experienced mental health problems.
The demographic factors significantly differed among the three groups as compared to those without these conditions. Zygo et al found that parents’ alcohol consumption was an important factor influencing suicidal behavior in youth.39 Researchers believe that multiple genetically related intermediate phenotypes may influence the relationship between alcohol consumption and suicide.40 Regarding parental alcohol use disorder, adverse childhood events may have long-lasting effects, ie, the negative effects of growing up with a parent with alcohol use disorder may have persisted resulting in an association with SA. What pathway exhibits likely increased risk of SA of individuals having a genetic predisposition to alcohol consumption, especially as they grow old, remains unclear. Therefore, further study is needed.
Interestingly, major depressive disorder and hypomanic disorder are related to SI but not to SA. In the case of hypomanic disorder, some factors such as hopelessness may be involved and give rise to suicidal behavior.41 Moreover, agoraphobic disorder may increase the risk of SI.42,43 We agree with Norton et al44 and Sareen et al45 that SI may be attributable to the distress and anxiety that comorbid patients experience as well as the desire to escape from this distress. Notably, agoraphobia may play a vital role in active SI and SA, and seems to have a stronger effect than depressive disorder on SA. This observation may provide an important clue for clinicians to be aware of SA among older adults, which may differ from that in younger age groups.
In addition to depressive and phobic disorders, self-reported depressive and anxiety symptoms also play a role in passive SI as shown by other studies.46 In contrast to depressive symptoms, anxiety symptoms reported by the patient become a protective factor. In other words, the greater the anxiety individuals express, the less SI they experience. We assume that the anxiety symptoms in this case may be viewed as coping mechanisms in dealing with distress.47 However, in the more severe form of SI and attempts; their effects are diluted to nonsignificant. Remarkably however, perceived social support was a significant protective factor for SA. Although many studies have shown that SI is related to poor social support,5,43,48–51 this study, perceived social support came into play in SA but not in SI. This study emphasizes the importance of social support in reducing the likelihood of individuals with SI attempting suicide.
Finally, physical illness had no association with any type of suicidality, except for hypertension. Studies concerning the association between hypertension and SI are however limited. In contrast to the present findings, hypertension was found to be associated with SI and SA.52,53 Bolton et al demonstrated that patients with newly diagnosed hypertension had an increased risk of suicide within the first three months, but a lower risk of suicide after three months and beyond the first year.53 Another study conducted among patients with hypertension revealed that psychological distress rather than other factors was significantly associated with SI.54 Based on the aforementioned studies, hypertension could be either increased or decreased risk of suicide. What contributed to such results is not fully understood. We assume that early experience of hypertension may be related to stress and depression, leading to suicidality, while subsequent experience of hypertension might be related to the opportunity to see a doctor regularly, which would provide an opportunity to express their anxiety/worries and receive support, which may result in fewer suicidal thoughts. Unlike the present study, the aforementioned studies were conducted in both adult and elderly populations. The effect of perceived social support, eg, from the healthcare team, is pronounced among older adult.
These findings add more clinical implication regarding the predictors for each type of suicidality. Particularly, the early identification of those who experience depressive and anxiety symptom is important to capture and further probe on SI. Even though the design was cross-sectional and the causal relationship between SI and SA could not be established, early intervention of enhancing social support is empirically a remedial strategy for older adults with SI especially those with depressive disorder. Adding screening tools to assess anxiety, depressive symptoms and perceived social support in a routine evaluation would be useful and a practical method in clinical settings.32,55
Strengths and Limitations
To the best of our knowledge, this study is the first in Thailand to examine a variety of predictors of suicidality among older adults. Compared with sociodemographic variables that cannot be modified, recognizing some psychosocial variables could provide clinical benefit as clinicians would be able to apply appropriate measures to reduce incidence. For example, clinicians can help patients to express their anxiety and ensure that they have greater social support. One limitation of this study was its cross-sectional design; hence, a precise causal relationship between the predictors and suicidality could not be established. A long-term design may help further clarify these relationships. Another limitation was that the number of subjects, especially in the SA group, was small, which may have led to error in the results of data analysis. The study recruited participants from a tertiary care hospital, which would not represent elderly patients with suicidality being treated elsewhere or in the general population. Lastly, greater physical health burden that would be associated with suicidality was excluded from the study due to ethics concerns. Therefore, the association between physical illness and suicidality was not that strong except for hypertension.
Conclusion
Suicidality was found in one fourth of older people who came for psychiatric services in tertiary care settings, with SI being more common than SA; passive SI was found in the majority of cases of SI. Different predictors were associated with different types of suicidality. For passive SI, predictors included having hypertension, depressive disorders, current hypomanic disorder and self-reporting a high level of depression. For active SI, predictors included agoraphobia, depressive disorders and current hypomanic disorder. For SA, predictors included a family history of alcohol dependence, agoraphobia and perceived lack of social support. Hypertension, expression of anxiety symptoms and perceived social support were protective factors for suicidality. A longitudinal study should be further conducted to investigate more robust relationship. More attention should be paid for comorbidity, especially agoraphobia. Poor social support should be carefully identified and remedied by appropriate intervention among older adults with SI.
Acknowledgments
The authors thank the DAS Research Group for their effort in developing the study and collecting data. The authors thank the National Research Council of Thailand for funding DAS research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Organization WH. Distribution of suicides rates (per 100000) by gender and age. Available from: https://www.who.int/mental_health/prevention/suicide/suicide_rates_chart/en/.
2. Organization WH. Preventing suicide: a global imperative. Available from: https://www.who.int/mental_health/suicide-prevention/world_report_2014/en/.
3. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):
4. Kittirattanapaiboon P, Khamwongpin M. The validity of the mini international neuropsychiatric interview (MINI)-Thai version. J Mental Health Thailand. 2005;13(3):125–135.
5. Stolz E, Fux B, Mayerl H, É R, Freidl W. Passive suicide ideation among older adults in Europe: a multilevel regression analysis of individual and societal determinants in 12 countries (SHARE). J Gerontol B Psychol Sci Soc Sci. 2016;71(5):947–958. doi:10.1093/geronb/gbw041
6. Dong L, Kalesnikava VA, Gonzalez R, Mezuk B. Beyond depression: estimating 12-months prevalence of passive suicidal ideation in mid- and late-life in the health and retirement study. Am J Geriatr Psychiatry. 2019;27(12):1399–1410. doi:10.1016/j.jagp.2019.06.015
7. Koo YW, Kolves K, De Leo D. Suicide in older adults: a comparison with middle-aged adults using the Queensland Suicide Register. Int Psychogeriatr. 2017;29(3):419–430. doi:10.1017/s1041610216001848
8. Conejero I, Olié E, Courtet P, Calati R. Suicide in older adults: current perspectives. Clin Interv Aging. 2018;13:691–699. doi:10.2147/cia.s130670
9. Cabello M, Miret M, Ayuso-Mateos JL, et al. Cross-national prevalence and factors associated with suicide ideation and attempts in older and young-and-middle age people. Aging Ment Health. 2019:1–10. doi:10.1080/13607863.2019.1603284
10. Miret M, Caballero FF, Huerta-Ramirez R, et al. Factors associated with suicidal ideation and attempts in Spain for different age groups. Prevalence before and after the onset of the economic crisis. J Affect Disord. 2014;163:1–9. doi:10.1016/j.jad.2014.03.045
11. Dutta R, Ball HA, Siribaddana SH, et al. Genetic and other risk factors for suicidal ideation and the relationship with depression. Psychol Med. 2017;47(14):2438–2449. doi:10.1017/s0033291717000940
12. Fung YL, Chan ZC. A systematic review of suicidal behaviour in old age: a gender perspective. J Clin Nurs. 2011;20(15–16):2109–2124. doi:10.1111/j.1365-2702.2010.03649.x
13. Lee H, Seol KH, Kim JW. Age and sex-related differences in risk factors for elderly suicide: differentiating between suicide ideation and attempts. Int J Geriatr Psychiatry. 2018;33(2):e300–e306. doi:10.1002/gps.4794
14. Ayalon L, Mackin S, Arean PA, Chen H, McDonel Herr EC. The role of cognitive functioning and distress in suicidal ideation in older adults. J Am Geriatr Soc. 2007;55(7):1090–1094. doi:10.1111/j.1532-5415.2007.01237.x
15. Pascal de Raykeer R, Hoertel N, Blanco C, et al. Effects of psychiatric disorders on suicide attempt: similarities and differences between older and younger adults in a national cohort study. J Clin Psychiatry. 2018;79(6). doi:10.4088/JCP.17m11911
16. Park S, Lee Y, Youn T, et al. Association between level of suicide risk, characteristics of suicide attempts, and mental disorders among suicide attempters. BMC Public Health. 2018;18(1):477. doi:10.1186/s12889-018-5387-8
17. Ge D, Sun L, Zhou C, Qian Y, Zhang L, Medina A. Exploring the risk factors of suicidal ideation among the seniors in Shandong, China: a path analysis. J Affect Disord. 2017;207:393–397. doi:10.1016/j.jad.2016.09.031
18. Kim S, Ha JH, Yu J, Park DH, Ryu SH. Path analysis of suicide ideation in older people. Int Psychogeriatr. 2014;26(3):509–515. doi:10.1017/S1041610213002366
19. O’Rourke N, Heisel MJ, Canham SL, Sixsmith A, Team BS. Predictors of suicide ideation among older adults with bipolar disorder. PLoS One. 2017;12(11):e0187632. doi:10.1371/journal.pone.0187632
20. Huang MF, Yen CF, Lung FW. Moderators and mediators among panic, agoraphobia symptoms, and suicidal ideation in patients with panic disorder. Compr Psychiatry. 2010;51(3):243–249. doi:10.1016/j.comppsych.2009.07.005
21. Goodwin RD, Hamilton SP. The early-onset fearful panic attack as a predictor of severe psychopathology. Psychiatry Res. 2002;109(1):71–79. doi:10.1016/s0165-1781(01)00357-2
22. McClure JR, Criqui MH, Macera CA, Ji M, Nievergelt CM, Zisook S. Prevalence of suicidal ideation and other suicide warning signs in veterans attending an urgent care psychiatric clinic. Compr Psychiatry. 2015;60:149–155. doi:10.1016/j.comppsych.2014.09.010
23. Wiktorsson S, Runeson B, Skoog I, Ostling S, Waern M. Attempted suicide in the elderly: characteristics of suicide attempters 70 years and older and a general population comparison group. Am J Geriatr Psychiatry. 2010;18(1):57–67. doi:10.1097/JGP.0b013e3181bd1c13
24. Almeida OP, Draper B, Snowdon J, et al. Factors associated with suicidal thoughts in a large community study of older adults. Br J Psychiatry. 2012;201(6):466–472. doi:10.1192/bjp.bp.112.110130
25. Zhuori N, Cai Y, Yan Y, Cui Y, Zhao M. Does social support affect the health of the elderly in rural China? A meta-analysis approach. Int J Environ Res Public Health. 2019;16(18):18. doi:10.3390/ijerph16183471
26. Szücs A, Szanto K, Wright AGC, Dombrovski AY. Personality of late- and early-onset elderly suicide attempters. Int J Geriatr Psychiatry. 2020;35(4):384–395. doi:10.1002/gps.5254
27. Szücs A, Szanto K, Aubry JM, Dombrovski AY. Personality and suicidal behavior in old age: a systematic literature review. Front Psychiatry. 2018;9:128. doi:10.3389/fpsyt.2018.00128
28. Wongpakaran N, Wongpakaran T, Lerttrakarnnon P, et al. Prevalence, clinical and psychosocial variables of depression, anxiety and suicidality in geriatric tertiary care settings. Asian J Psychiatr. 2019;41:38–44. doi:10.1016/j.ajp.2018.10.007
29. First MB, Spitzer RL, Gibbon M, Williams JB. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition. 2002.
30. Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990;55(3–4):610–617. doi:10.1080/00223891.1990.9674095
31. Wongpakaran N, Wongpakaran T. A revised Thai multi-dimensional scale of perceived social support. Span J Psychol. 2012;15(3):1503–1509. doi:10.5209/rev_SJOP.2012.v15.n3.39434
32. Wongpakaran T, Wongpakaran N, Sirirak T, Arunpongpaisal S, Zimet G. Confirmatory factor analysis of the revised version of the Thai multidimensional scale of perceived social support among the elderly with depression. Aging Ment Health. 2018;22(9):1143–1148. doi:10.1080/13607863.2017.1339778
33. Banjongrewadee M, Wongpakaran N, Wongpakaran T, Pipanmekaporn T, Punjasawadwong Y, Mueankwan S. The role of perceived stress and cognitive function on the relationship between neuroticism and depression among the elderly: a structural equation model approach. BMC Psychiatry. 2020;20(1):25. doi:10.1186/s12888-020-2440-9
34. Tangwongchai S, Phanasathit M, Charernboon T, et al. The validity of Thai version of the Montreal cognitive assessment (MoCA-T). Dement Neuropsychol. 2009;3(2):172.
35. Wongpakaran N, Wongpakaran T, Lertkachatarn S, Sirirak T, Kuntawong P. Core Symptom Index (CSI): testing for bifactor model and differential item functioning. Int Psychogeriatr. 2019;1–11.
36. Wongpakaran N, Wongpakaran T. Prevalence of major depressive disorders and suicide in long-term care facilities: a report from northern Thailand. Psychogeriatrics. 2012;12(1):11–17. doi:10.1111/j.1479-8301.2011.00383.x
37. Wongpakaran T, Wongpakaran N. Detection of suicide among the elderly in a long term care facility. Clin Interv Aging. 2013;8:1553–1559. doi:10.2147/CIA.S53355
38. Wongpakaran N, Wongpakaran T. The Thai version of the PSS-10: an Investigation of its psychometric properties. Biopsychosoc Med. 2010;4:6. doi:10.1186/1751-0759-4-6
39. Zygo M, Pawłowska B, Potembska E, Dreher P, Kapka-Skrzypczak L. Prevalence and selected risk factors of suicidal ideation, suicidal tendencies and suicide attempts in young people aged 13–19 years. Ann Agric Environ Med. 2019;26(2):329–336. doi:10.26444/aaem/93817
40. Pompili M, Serafini G, Innamorati M, et al. Suicidal behavior and alcohol abuse. Int J Environ Res Public Health. 2010;7(4):1392–1431. doi:10.3390/ijerph7041392
41. Valtonen HM, Suominen K, Haukka J, et al. Hopelessness across phases of bipolar I or II disorder: a prospective study. J Affect Disord. 2009;115(1–2):11–17. doi:10.1016/j.jad.2008.06.013
42. Brown LA, Gaudiano BA, Miller IW. The impact of panic-agoraphobic comorbidity on suicidality in hospitalized patients with major depression. Depress Anxiety. 2010;27(3):310–315. doi:10.1002/da.20609
43. Corna LM, Cairney J, Streiner DL. Suicide ideation in older adults: relationship to mental health problems and service use. Gerontologist. 2010;50(6):785–797. doi:10.1093/geront/gnq048
44. Norton PJ, Temple SR, Pettit JW. Suicidal ideation and anxiety disorders: elevated risk or artifact of comorbid depression? J Behav Ther Exp Psychiatry. 2008;39(4):515–525. doi:10.1016/j.jbtep.2007.10.010
45. Sareen J, Cox BJ, Afifi TO, et al. Anxiety disorders and risk for suicidal ideation and suicide attempts: a population-based longitudinal study of adults. Arch Gen Psychiatry. 2005;62(11):1249–1257. doi:10.1001/archpsyc.62.11.1249
46. Heisel MJ, Duberstein PR, Lyness JM, Feldman MD. Screening for suicide ideation among older primary care patients. J Am Board Fam Med. 2010;23(2):260–269. doi:10.3122/jabfm.2010.02.080163
47. Iavarone A, Ziello AR, Pastore F, Fasanaro AM, Poderico C. Caregiver burden and coping strategies in caregivers of patients with Alzheimer’s disease. Neuropsychiatr Dis Treat. 2014;10:1407–1413. doi:10.2147/ndt.s58063
48. O’Riley AA, Van Orden KA, He H, Richardson TM, Podgorski C, Conwell Y. Suicide and death ideation in older adults obtaining aging services. Am J Geriatr Psychiatry. 2014;22(6):614–622. doi:10.1016/j.jagp.2012.12.004
49. Van Orden KA, Wiktorsson S, Duberstein P, Berg AI, Fässberg MM, Waern M. Reasons for attempted suicide in later life. Am J Geriatr Psychiatry. 2015;23(5):536–544. doi:10.1016/j.jagp.2014.07.003
50. Heisel MJ, Neufeld E, Flett GL. Reasons for living, meaning in life, and suicide ideation: investigating the roles of key positive psychological factors in reducing suicide risk in community-residing older adults. Aging Ment Health. 2016;20(2):195–207. doi:10.1080/13607863.2015.1078279
51. Nam EJ, Lee JE. Mediating effects of social support on depression and suicidal ideation in older Korean adults with hypertension who live alone. J Nurs Res. 2019;27(3):e20. doi:10.1097/jnr.0000000000000292
52. Xu H, Qin L, Wang J, et al. A cross-sectional study on risk factors and their interactions with suicidal ideation among the elderly in rural communities of Hunan, China. BMJ Open. 2016;6(4):e010914. doi:10.1136/bmjopen-2015-010914
53. Bolton JM, Walld R, Chateau D, Finlayson G, Sareen J. Risk of suicide and suicide attempts associated with physical disorders: a population-based, balancing score-matched analysis. Psychol Med. 2015;45(3):495–504. doi:10.1017/s0033291714001639
54. Ge D, Zhang X, Guo X, Chu J, Sun L, Zhou C. Suicidal ideation among the hypertensive individuals in Shandong, China: a path analysis. BMC Psychiatry. 2019;19(1):266. doi:10.1186/s12888-019-2256-7
55. Wongpakaran T, Wongpakaran N, Pinyopornpanish M, et al. Baseline characteristics of depressive disorders in Thai outpatients: findings from the Thai study of affective disorders. Neuropsychiatr Dis Treat. 2014;10:217–223. doi:10.2147/NDT.S56680
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.