Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Predictors and Factors Associated with Counseling Seeking Behavior Against Intimate Partner Violence Among HIV-Positive Women in Southwestern Uganda
Authors Arishaba A, Kiduuma W, Night G, Arinaitwe I, Niyonzima V ![]() , Mubangizi V
, Mubangizi V ![]()
Received 15 February 2022
Accepted for publication 1 June 2022
Published 10 June 2022 Volume 2022:14 Pages 275—283
DOI https://doi.org/10.2147/HIV.S362398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Adella Arishaba,1 Wilson Kiduuma,1 Grace Night,2 Innocent Arinaitwe,3 Vallence Niyonzima,1 Vincent Mubangizi1
1Department of Nursing, Faculty of Medicine Mbarara University of Science and Technology, Mbarara City, Uganda; 2Department of Physiotherapy, Faculty of Medicine Mbarara University of Science and Technology, Mbarara City, Uganda; 3Department of Internal Medicine, Faculty of Medicine Mbarara University of Science and Technology, Mbarara City, Uganda
Correspondence: Vallence Niyonzima, Department of Nursing, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara city, Uganda, Tel +256777842830, Email [email protected]
Purpose: The study intended to establish the proportion of HIV-positive women experiencing IPV and the predictors of counseling-seeking behavior among women living with HIV in Isingiro district.
Methods: The study was a cross-sectional quantitative study. We conducted the study in April 2021 among 296 HIV-positive women receiving ART services at Rwekubo and Nyamuyanja Health Centre fours. Data were collected using a researcher-administered questionnaire. Consecutively participants were recruited from the ART clinic. SPSS Version 23.0 was used to analyze data. We computed the prevalence of intimate partner violence among the study participants. Logistic regression was performed to identify the associated factors and predictors of counseling-seeking behavior.
Results: Of the 296 participants interviewed, 66.2% of the HIV-positive women had experienced IPV. Only 40.2% of those who had experienced IPV had received counseling, 35.5% of the participants sought help for IPV from family and friends and 27% sought help from other service providers including the police. A majority (67.2%) of the participants had a primary level of education and over a third (45.9%) of the participants were from monogamous families. The factors associated with seeking care for IPV were education level (p = 0.002), type of family (p = 0.04), physical abuse within one last year (p < 0.001), emotional abuse (p < 0.001), awareness about IPV services (p < 0.001) and availability of counselors (p < 0.001). The predictors of care-seeking for IPV included awareness about IPV services (aOR: 295.6, 95% CI: 54.3– 1608.9) and availability of counselors (aOR: 5.3, 95% CI: 1.5– 19.2).
Conclusion: The prevalence of IPV is 66.2%, and proportion of HIV-positive women who seek IPV counseling services is low. The predictors of counseling-seeking behavior were awareness about IPV services and availability of counselors. There is a need to improve awareness about IPV services and provide more counselors to offer help to the IPV victims.
Keywords: intimate partner violence, HIV-positive women, counseling, Uganda, cross-sectional study
Introduction
Intimate partner violence (IPV) is a public health concern. The World Health Organization defines IPV as “a range of any behavior that causes physical, sexual, or emotional harm to those in an intimate relationship by the current or former partner”.1 Furthermore, World Health Organization describes IPV as any physical violence which includes hitting, slapping, kicking or beating; sexual violence involving sexual coercion and forced sexual intercourse; psychological/ emotional abuse including belittling, insults, intimidation, humiliation and threats of harm while controlling behavior entails isolating a person from family and friends and restricting access to financial resources.2 Although IPV affects both genders, women are the most affected. The prevalence of cumulative lifetime IPV varies globally and has been reported to be 10–71% among married women.3,4 High prevalence rates of IPV from 20% to 71% have been reported across sub-Saharan African.3,5 According to the 2016 Uganda Demographic and Health Survey, four out of every ten ever-married women experienced some form of IPV during the prior year.6 Recent several studies have documented the existence of various forms of IPV in Uganda including physical, sexual and emotional violence.7–11
IPV and HIV pandemics were shown to be closely related in a systemic review.12 HIV-positive status increases the risk of women being violated by their intimate partners.12–16 Low-and middle-income countries (LMICs) have both the highest IPV and HIV prevalence rates ranging from 40% to 84%,17,18 and women are more affected compared with their males.19 According to Uganda Population-Based HIV Impact Assessment,20 Southwestern Uganda had the highest HIV prevalence of 7.9%. Also, the Ankole region which includes; Isingiro, Kiruhura, Mbarara, Mitooma among others had the highest prevalence of intimate partner violence of 48.6% among ever-married women.21
Correlates of IPV in the general population in Uganda include gender norm perceptions about violence, sociodemographic characteristics, substance abuse (especially alcohol), marital dissatisfaction, and presence of sexual problems.9,11,16,22 Whereas a study conducted in Uganda by Kairania et al23 showed that HIV-positive disclosure was associated with among women living with HIV, another study showed that disclosure was protective against IPV.11 Other factors such as testing for HIV, HIV positive result disclosure, antiretroviral therapy use, requesting for a protective sexual encounter, low education level, and being married may lead to IPV.11,16,23
IPV has adverse consequences on the life of the survivor ranging from physical, psychological, socio-emotional, sexual, and reproductive health problems.18,24 Specifically for HIV, these effects include engaging in risky behaviors,25 incident HIV,12,15 poor acceptance of services to prevent human immunodeficiency virus (HIV) vertical transmission reduced antiretroviral therapy adherence and a lower likelihood of viral load suppression.10,26–28
To address the negative effects of IPV and improve the livelihoods of survivors, policies and laws have been put in place by the government of Uganda.24,29 Counseling of the IPV survivors is one of the services given in Uganda which is following World Health Organization guidelines.18,24,30 The challenge is that few survivors of IPV access or complete the necessary treatment regimen.8,31,32 Factors associated with help-seeking include: whether the victims think they will get help and what they perceive to be barriers to access that help; the presence of social support; perceived benefits of services to be received; and victims being conscious about their health.8,33 Also, both victim and community’s attitudes toward IPV, IPV as well as HIV stigmatization, empowerment indicators, autonomy in decision making, literacy, economic empowerment, the severity and type of abuse determine whether one will seek help or not.34–37
The predictors of counseling seeking behavior in IPV mitigation have not been well documented in developing countries like Uganda.38 We, therefore, conducted this study to establish the predictors and factors associated with counseling-seeking behavior against IPV among HIV-positive women in southwestern Uganda. The findings of this study will provide information about the extent of counseling services provided as well as inform the integration of strategies to prevent and mitigate intimate partner violence into HIV care for women living with HIV in Uganda.
Materials and Methods
Study Design and Setting
This study employed a quantitative cross-sectional design of inquiry and data was collected in April 2021. The study was carried out in Isingiro district which is bordered by Kiruhura district within the north, Rakai district to the East, Ntungamo district to the West, Mbarara district to the North West, and Tanzania to the South. However, according to National Population and Housing Census 2014ʹs Area Specific Profiles published in April 2017, Isingiro has a total population of 492,116 people, 48.3% (237/549) males and 51.7% (254/567) females with an estimated 3.7% (5/450) living with HIV/AIDS and already on care. Comprehensive HIV/AIDS care services in Isingiro are offered exclusively by Public Health facilities that are accredited by ministry of health, Uganda (MoH). Access to these health facilities is not universal as 31.1% of the Households in the district are located 5 km or more from the nearest public health facility. The terrain of the area is mountainous which makes access to services more difficult. Both Rwekubo and Nyamuyanja Health center IVs are public owned facilities accredited to offer HIV-related services for free to the public. These services include HIV testing, counseling, providing antiretroviral therapy, and management of complications of HIV-related infections.
Study Population and Sample Size
The study was carried out among the HIV-positive women receiving HIV care services from Rwekubo HC IV and Nyamuyanja HC IV in Isingiro district, Southwestern Uganda. The sample size of the participants was calculated using Cochran’s formula where Z = 1.96 at 95% confidence interval, p = the proportion of the HIV positive women with IPV which was 26.39, 11, q = 1-p and e= margin of error (5%). n= ((1.96)2X0.2639X0.7361)/(0.05)2 = 298 HIV positive women. By adding 10% to cater for non-response, the minimum sample size was 328 HIV positive women.
Data Collection Procedure
We collected data using a researcher-administered questionnaire to determine the proportions of HIV-positive women experiencing IPV and receiving counseling for IPV prevention and the factors associated with counseling-seeking behavior among HIV-positive women experiencing IPV. The tool was developed from existing literature mainly informed by revised conflicts tactic scale.39 Revised conflict Tactic scale has been previously used in Uganda.9 The tool was pretested among ten HIV-positive women at Mbarara Regional Referral Hospital. The questionnaire focused on the following variables: Number of women counseled for IPV prevention, socio-demographic characteristics, forms of IPV experienced and frequency of occurrence, number of children, type of relationship, HIV status of the husband, knowledge about IPV, and availability of counselors.
HIV-positive women coming for routine HIV care services at the two health centers were consecutively enrolled into the study. The purpose of the study was then explained and we obtained written informed consent from the study participants before participating in the study. We assigned a code to each of the questionnaires and interviewed them separately from others in a private room. The researcher then asked the participant close-ended questions from the researcher administered questionnaire for about 25 minutes and we interviewed 296 participants out of 328.
Data Management and Analysis
The questionnaires were checked for completeness by the investigator. Double data entry using Microsoft excel was done to ensure the accuracy of data. Data were scanned and checked for out-of-range and missing values before data analysis and analyzed using SPSS version 23.0. Continuous variables were analyzed using means and standard deviations and frequencies and percentages for categorical variables. We computed the proportion of participants who had received IPV counseling services and compared participants’ characteristics with their IPV counseling-seeking behavior by using chi-square and Fisher’s exact test for categorical variables. Associations were quantified by using simple and multivariable logistic regression analysis reporting odds ratios and their corresponding 95% confidence intervals. All variables with a p-value less than 0.05 at the bivariate logistic regression level were integrated into the multivariate logistic model. The model fitness was checked using the Hosmer-Lemeshow test at p>0.05 to determine the predictors of counseling-seeking behavior among the HIV-positive at the two selected health facilities.
Ethical Considerations
Approval to conduct the study was obtained from Mbarara University of Science and Technology Research Ethics Committee (MUST-REC) (Ref 04/12-20). Administrative clearance was sought from the district health officer (DHO) Isingiro district before data collection. A voluntary, written informed consent was obtained from study participants at enrollment. The study complied with the declaration of Helsinki.
Results
Socio-Demographic Characteristics of Study Participants
The summary of study participants’ socio-demographic characteristics and prevalence of IPV are indicated in Table 1. A total of 296 participants were included in the study. The mean age was 37.4 ±11.4 years. The majority, 67.2% (199/296) of the participants had attended a primary level of education. Most of the respondents were peasants, 64.5% (191/296). Over a third, 45.9% (136/296) of the participants were from monogamous families.
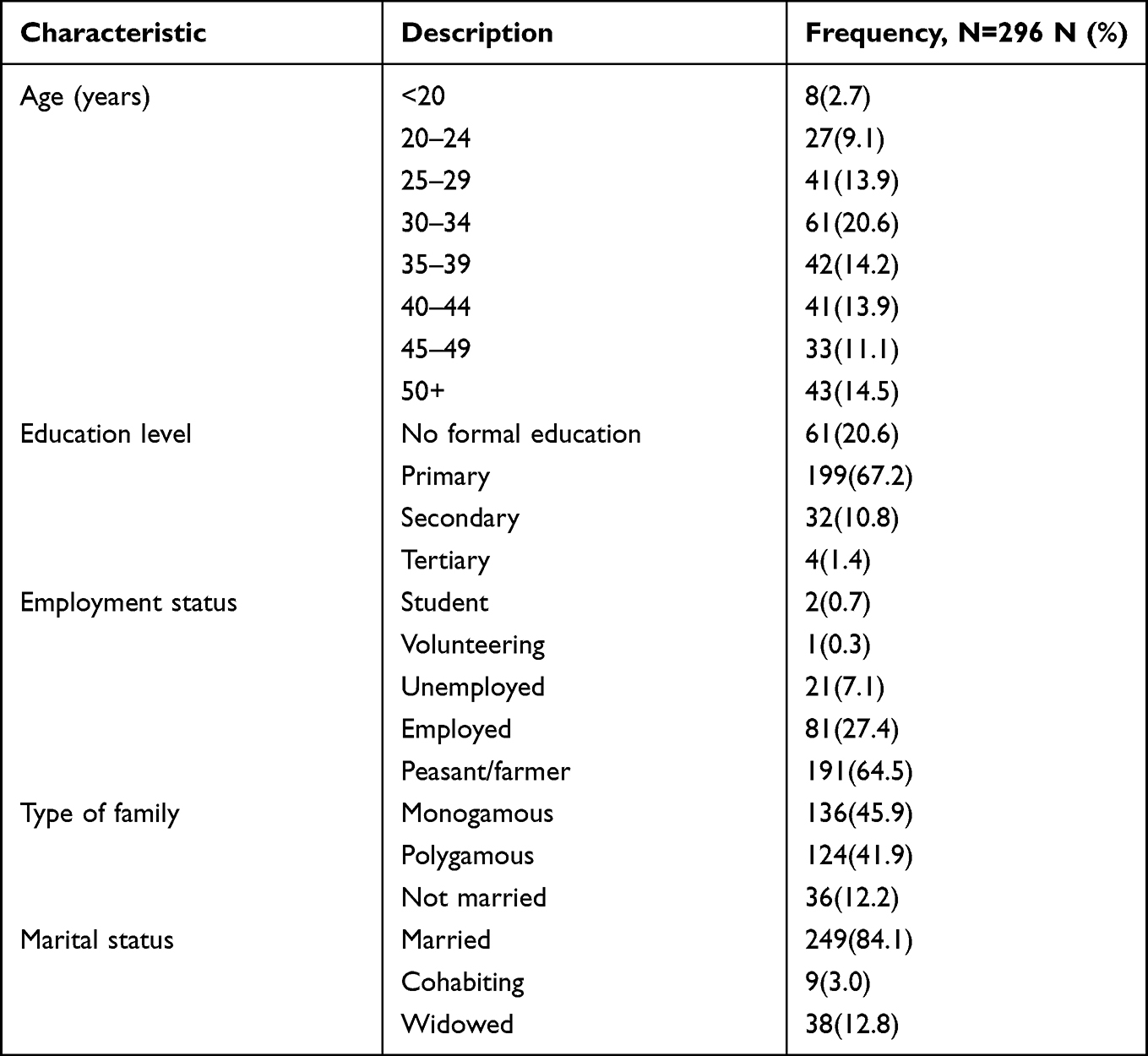 |
Table 1 Socio-Demographic Characteristics of HIV-Positive Women Receiving HIV Care Services at Two Selected Health Facilities in Isingiro District, Southwestern Uganda |
Prevalence of Intimate Partner Violence (IPV) Among the HIV-Positive Women
The prevalence of IPV among HIV-positive women receiving HIV care services at the two selected health facilities was 66.2% (196/295). The different forms of IPV experienced by the study participants included; physical violence, 61.1% (181/296), sexual violence, 36.1% (107/296), and emotional violence, 78% (231/296).
IPV was high among respondents in the following age categories: 30–34 (15.9%, 47/295), 35–39 (10.5%, 31/295), 25–29 (10.2%, 30/295) and 40–44 (9.2%, 27/295). Most, 47.5% (140/295) of the respondents who had attended primary experienced IPV. HIV-positive women in polygamous relationships experienced IPV the most, 33.9% (100/295) compared to those in monogamous relationships. The majority, 62.0% (183/295) of the participants who were married experienced IPV.
Factors Associated with IPV and Predictors of Care Seeking Behavior Among HIV-Positive Women
The proportion of HIV-positive women who received counseling after experiencing IPV was 60.7% (119/196). About half of the participants, 53.5% (105/196) sought help for IPV from family and friends. Also, 40.82% (80/196) of the participants sought help from multiple sources including the police, Local Council 1, and Compassion International.
The factors that were significantly associated with care-seeking for IPV among HIV positive women on bivariate analysis were education level (p=0.002), type of family (p=0.04), physical abuse within one last year (p<0.001), sexual abuse within one last year (p<0.001), emotional abuse within one last year (p<0.001), awareness about IPV services (p<0.001) and availability of counselors (p<0.001). When multivariable logistic regression was done on these variables, only awareness about IPV services and availability of counselors remained statistically significantly associated with care-seeking behavior as shown in Table 2. The care-seeking behavior for IPV among HIV positive women was correlated positively with awareness about IPV services (adjusted odds ratio [aOR]= 5.292, 95% CI (1.462–19.156), p=0.011) and availability of counselors (aOR=5.3, 95% CI (1.5–19.2) p=0.000).
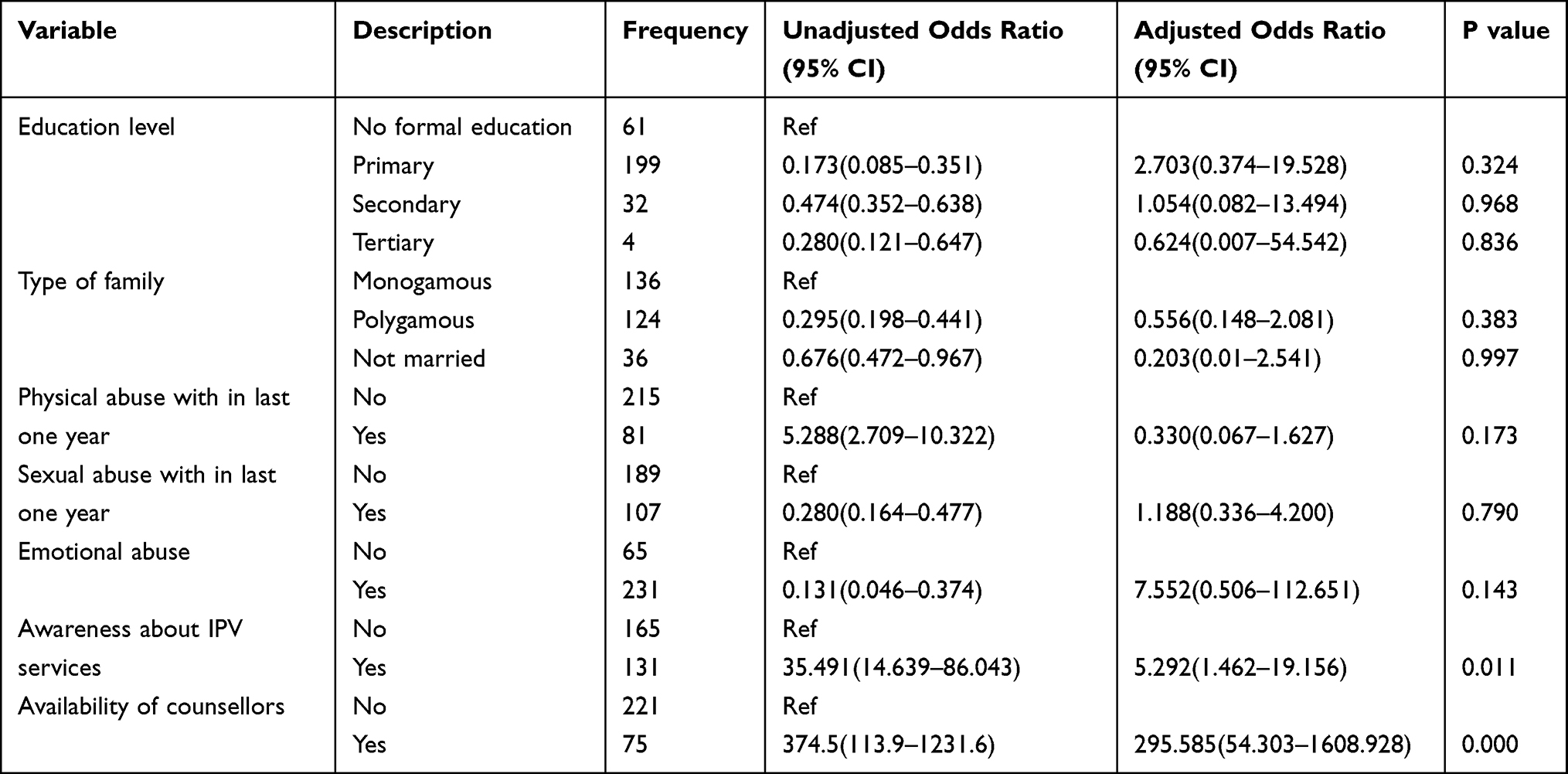 |
Table 2 Factors Associated and Predictors of Care-Seeking for IPV Among HIV-Positive Women Based on Bivariate Analysis and Multivariable Logistic Regression |
Discussion
Our study investigated the predictors and factors associated with counseling-seeking behavior of HIV positive women after experiencing IPV attending Rwekubo and Nyamuyanja HC IVs in Isingiro district, Southwestern Uganda. Consistent with the findings of the UDHS 2016 report, the main source of income in Southwestern Uganda was farming.21
The overall prevalence of IPV among HIV-positive women receiving HIV care services at the two selected health facilities was high at 66.2%. This figure is close to that reported in Togo and South Africa respectively.13,40 This figure is above the rates previously reported in Uganda.10,16 The difference could be attributed to the factor that these two studies only included physical and sexual violence forms of IPV. Also, data of these two studies were corrected between 2014 and 2016.10,16 Our study was done during SARS-CoV 2 virus (COVID 19) pandemic in the situation of stay at home policies, which has been documented to increase IPV.41–47 Emotional violence was the most reported form of IPV at 78% in our study. For unknown reasons, this form of IPV is not included in most studies.10,13,16 Perhaps, some authors do not take the emotional/psychological form of intimate partner violence to be as significant as physical and sexual forms.48,49
This study found that only 40.2% of the women who were violated sought counseling from a formal system. This finding is consistent with the study done among women in the general population in Tanzania, a neighboring country.50 This finding supports earlier studies that showed that survivors of IPV did not seek help from formal support or even disclose their experiences.8,13,31,51–53 If they did seek help, they tended to use informal systems such as friends and family members.8,52,54,55
Awareness about IPV services was significantly associated with counseling-seeking behavior in our study. This was in agreement with other studies.53 Literature shows that women who are aware that IPV is not acceptable in the community were more likely to seek help.53,55 There is a hypothesis that posits that a person’s help-seeking behavior is determined by the attitudes toward seeking help.56 This attitude could be negatively shaped by unpleasant previous experiences.33 Also, an individual’s awareness of the benefits of seeking help may create the agency to seek help.57 Thus, improving community awareness about the available IPV services in health facilities is important in improving the utilization of these services by victims of IPV.
Availability of a counselor was a significant predictor of care-seeking behavior among HIV-positive women. This was consistent with other studies that showed that the availability of counselors to assist survivors of IPV was associated with seeking help from formal system.58 The presence of a trusted counselor would lead to help-seeking behavior. As expected when survivors of IPV are not aware of the presence of counseling services to mitigate the IPV effect, few will utilize such services. Existing literature shows that when the IPV survivor has trust in the institution (of help offering), she is likely to seek that help.53,59,60 On the other hand, previous bad encounters with the system would deter future use. Most institutions in sub-Saharan Africa may not keep information provided by a survivor of IPV confidential, are corrupt and inept.61 This may hinder the victim of IPV from using such a system.
This study found no significant relationship between the socio-demographic characteristics such as age, marital status, level of education of HIV-positive women victims of IPV, and help-seeking. Previous studies have shown mixed results on whether or not socio-demographic characteristics are related to seeking help. This study finding mirrors studies done in Nigeria and Tanzania.37,50 In contrast, other studies show that socio-economic characteristics of women survivors of IPV have a statistically significant relationship with help-seeking.55,62,63 Perhaps, the lack of association in the present study could be due to the effects of a small sample size used.
The study has the strength in that it determines predictors and factors associated with counseling-seeking behavior against IPV among HV-positive women. The study findings should be interpreted bearing in mind the study limitations. There was a possibility of recall bias since participants were asked about past IPV experiences. We minimized this by using a short-time framework of 12 months preceding the data collection. Secondly being a cross-sectional study, we cannot infer a causal relationship. We cannot conclude whether IPV was occurring because of HIV-related experiences (HIV testing, HIV positive status disclosure, care initiation, and/or antiretroviral drug therapy). Thirdly, we did not document how the partners came to know the HIV status of their spouses, yet this could have a bearing on the risk of IPV. Lastly, self-reported data used in this study is prone to social desirability given the socio-cultural views attached to IPV. We minimized this by using interviewers who were previously not known to participants. We also encouraged the participants to be sincere with us and reassured them that the information provided would be kept confidential. Despite these limitations, this study provides useful results that can be used with adaption in similar settings to improve the lives of survivors of sexual violence.
Conclusions and Recommendations
Implementation and perceptions about the IPV intervention services have not well been understood especially in low and middle-income countries, and this has caused IPV victims to seek help from informal sources other than health professionals. Also, studies have recommended the integration of screening for IPV by health-care providers as an integral part of the routine HIV care services as this will ease the identification of victims of IPV and enable them to be helped immediately. This would further assist in referrals and linkages to support groups and other services. We recommend a longitudinal study to establish whether the risk of IPV increases following HIV-positive status disclosure. Also, qualitative research is recommended to explore the barriers to help-seeking in Uganda.
Abbreviations
aOR, Adjusted Odds ratio; CI, Confidence Interval; HIV, Human immune deficiency virus; IPV, Intimate partner violence.
Data Sharing Statement
The datasets generated and analyzed during the study are available from the corresponding author on request.
Acknowledgments
Research reported in this publication was supported by the Fogarty International Center (US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy (S/GAC) and the President’s Emergency Plan for AIDS Relief (PEPFAR)) of the National Institutes of Health under Award Number R25TW011210. We thank the participants who participated in this study, the DHO Isingiro District, and the administration of Rwekubo and Nyamuyanja health centers who contributed towards the success of this study. We also acknowledge the contribution of Frankline Ainomugisha, Milliam Kolukiko, and Gabriel Nuwagaba, our research assistants, who helped to collect the data.
Funding
Research reported in this publication was supported by the Fogarty International Center (US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy [S/GAC] and the President’s Emergency Plan for AIDS Relief [PEPFAR]) of the National Institutes of Health under Award Number R25TW011210. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The content is solely the responsibility of the authors and does not necessarily represent the official views of the study funder, the National Institutes of Health. The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Hoffman JS. World Report on Violence and Health. In: Krug EG, Dahlberg LL, Mercy JA, Zwi A, Lozano R, editors. (Pp 340; $ US 27; Swiss francs 30, developing countries Swiss francs 15). Geneva: World Health Organization; 2002. ISBN 92-4-154561-5.
2. World Health Organization. Planning, Implementing and Monitoring Home-Based HIV Testing and Counselling: A Practical Handbook for Sub-Saharan Africa. World Health Organization; 2012.
3. Devries KM, Mak JY, Garcia-Moreno C, et al. The global prevalence of intimate partner violence against women. Science. 2013;340(6140):1527–1528. doi:10.1126/science.1240937
4. García-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts C. WHO Multi-Country Study on Women’s Health and Domestic Violence Against Women. World Health Organization; 2005.
5. Greene MC, Kane J, Tol WA. Alcohol use and intimate partner violence among women and their partners in sub-Saharan Africa. Global Ment Health. 2017;4. doi:10.1017/gmh.2017.9
6. UBOS. ICF: Uganda Demographic and Health Survey 2016. Kampala, Uganda, and Rockville, Maryland, USA: UBOS and ICF; 2018.
7. Amegbor PM, Pascoe L. Variations in emotional, sexual, and physical intimate partner violence among women in Uganda: a multilevel analysis. J Interpers Violence. 2021;36(15–16):NP7868–NP7898. doi:10.1177/0886260519839429
8. Amwiine E, Ainembabazi B, Obwona I, et al. Perceptions of females about trauma-informed services for survivors of sexual violence in southwestern Uganda-a qualitative study. BMC Public Health. 2021;21(1):1–10. doi:10.1186/s12889-021-12227-0
9. Auma AG, Ayebare E, Olwit C, Ndeezi G, Nankabirwa V, Tumwine JK. Intimate partner violence among pregnant teenagers in Lira district, northern Uganda: a cross-sectional study. Afr J Midwifery Women’s Health. 2020;14(4):1–11. doi:10.12968/ajmw.2020.0011
10. Kabwama SN, Bukenya J, Matovu JK, et al. Intimate partner violence among HIV positive women in care-results from a national survey, Uganda 2016. BMC Women’s Health. 2019;19(1):1–10. doi:10.1186/s12905-019-0831-1
11. Ogbonnaya IN, Wanyenze RK, Reed E, Silverman JG, Kiene SM. Prevalence of and risk factors for intimate partner violence in the first 6 months following HIV diagnosis among a population-based sample in rural Uganda. AIDS Behav. 2020;24(4):1252–1265. doi:10.1007/s10461-019-02673-8
12. Kouyoumdjian FG, Calzavara LM, Bondy SJ, et al. Intimate partner violence is associated with incident HIV infection in women in Uganda. Aids. 2013;27(8):1331–1338. doi:10.1097/QAD.0b013e32835fd851
13. Burgos-Soto J, Orne-Gliemann J, Encrenaz G, et al. Intimate partner sexual and physical violence among women in Togo, West Africa: prevalence, associated factors, and the specific role of HIV infection. Glob Health Action. 2014;7(1):23456. doi:10.3402/gha.v7.23456
14. Shamu S, Zarowsky C, Shefer T, Temmerman M, Abrahams N. Intimate partner violence after disclosure of HIV test results among pregnant women in Harare, Zimbabwe. PLoS One. 2014;9(10):e109447. doi:10.1371/journal.pone.0109447
15. Sileo KM, Kintu M, Kiene SM. The intersection of intimate partner violence and HIV risk among women engaging in transactional sex in Ugandan fishing villages. AIDS Care. 2018;30(4):444–452. doi:10.1080/09540121.2017.1391985
16. Young CR, Kaida A, Kabakyenga J, et al. Prevalence and correlates of physical and sexual intimate partner violence among women living with HIV in Uganda. PLoS One. 2018;13(8):e0202992. doi:10.1371/journal.pone.0202992
17. HIV/AIDS JUNPo. UNAIDS Data 2018. Geneva: UNAIDS; 2018.
18. World Health Organisation. Responding to Intimate Partner Violence and Sexual Violence Against Women: WHO Clinical and Policy Guidelines. World Health Organization; 2013.
19. Hegdahl HK, Fylkesnes KM, Sandøy IF. Sex differences in HIV prevalence persist over time: evidence from 18 countries in sub-Saharan Africa. PLoS One. 2016;11(2):e0148502. doi:10.1371/journal.pone.0148502
20. MoH. Uganda Population-Based HIV Impact Assessment (UPHIA) 2016–2017. Uganda Kampala: Ministry of Health; 2017.
21. UDHS. Uganda Demographic and Health Survey 1016. The DHS Program; 2016. Available from: dhsprogram.com.
22. Amegbor PM, Pascoe L. Variations in emotional, sexual, and physical intimate partner violence among women in Uganda: a multilevel analysis. J Interpers Violence. 2019;36:0886260519839429.
23. Kairania R, Gray RH, Wawer MJ, et al. Intimate partner violence and communication of HIV diagnosis in Rakai, Uganda. Soc Work Public Health. 2015;30(3):272–281. doi:10.1080/19371918.2014.994726
24. World Health Organisation. Strengthening the Health System Response to Violence Against Women in Uganda: Lessons Learned from Adapting and Implementing WHO Guidelines and Tools. World Health Organisation; 2020.
25. Kiene SM, Lule H, Sileo KM, Silmi KP, Wanyenze RK. Depression, alcohol use, and intimate partner violence among outpatients in rural Uganda: vulnerabilities for HIV, STIs, and high-risk sexual behavior. BMC Infect Dis. 2017;17(1):1–13. doi:10.1186/s12879-016-2162-2
26. Biomndo BC, Bergmann A, Lahmann N, Atwoli L. Intimate partner violence is a barrier to antiretroviral therapy adherence among HIV-positive women: evidence from government facilities in Kenya. PLoS One. 2021;16(4):e0249813. doi:10.1371/journal.pone.0249813
27. Hampanda KM. Intimate partner violence and HIV-positive women’s non-adherence to antiretroviral medication for the purpose of prevention of mother-to-child transmission in Lusaka, Zambia. Soc Sci Med. 2016;153:123–130. doi:10.1016/j.socscimed.2016.02.011
28. Hatcher AM, Smout EM, Turan JM, Christofides N, Stöckl H. Intimate partner violence and engagement in HIV care and treatment among women: a systematic review and meta-analysis. Aids. 2015;29(16):2183–2194. doi:10.1097/QAD.0000000000000842
29. Fay KE, Beyeza-Kashesya J, Gossett DR. Ugandan health care professionals’ response to sexual violence survivors: exploring local strategy and international guidelines. J Interpers Violence. 2018;36:6466–6486.
30. MoH. Uganda clinical guidelines, Kampala 2016. 2016.
31. Gatuguta A, Katusiime B, Seeley J, Colombini M, Mwanzo I, Devries K. Should community health workers offer support healthcare services to survivors of sexual violence? A systematic review. BMC Int Health Hum Rights. 2017;17(1):1–15. doi:10.1186/s12914-017-0137-z
32. Uganda Bureau of Statistics. Uganda Demographic and Health Survey. Kampala Uganda: Uganda Bureau of Statistics; 2011.
33. O’connor PJ, Martin B, Weeks CS, Ong L. Factors that influence young people’s mental health help‐seeking behaviour: a study based on the Health Belief Model. J Adv Nurs. 2014;70(11):2577–2587. doi:10.1111/jan.12423
34. Domenech Del Rio I, Sirvent Garcia Del Valle E. Influence of intimate partner violence severity on the help-seeking strategies of female victims and the influence of social reactions to violence disclosure on the process of leaving a violent relationship. J Interpers Violence. 2019;34(21–22):4550–4571. doi:10.1177/0886260516676473
35. Hayes BE, Franklin CA. Community effects on women’s help-seeking behaviour for intimate partner violence in India: gender disparity, feminist theory, and empowerment. Int J Comp Appl Crim Justice. 2017;41(1–2):79–94. doi:10.1080/01924036.2016.1233443
36. Overstreet NM, Quinn DM. The intimate partner violence stigmatization model and barriers to help-seeking. Basic Appl Soc Psych. 2013;35(1):109–122. doi:10.1080/01973533.2012.746599
37. Sedziafa AP, Tenkorang EY, Owusu AY. he always slaps me on my ears”: the health consequences of intimate partner violence among a group of patrilineal women in Ghana. Cult Health Sex. 2016;18(12):1379–1392. doi:10.1080/13691058.2016.1187291
38. Barnham L, Barnes GC, Sherman LW. Targeting escalation of intimate partner violence: evidence from 52,000 offenders. Cambridge J Evidence-Based Policing. 2017;1(2):116–142. doi:10.1007/s41887-017-0008-9
39. Straus MA, Douglas EM. A short form of the revised conflict tactics scales, and typologies for severity and mutuality. Violence Vict. 2004;19(5):507–520. doi:10.1891/vivi.19.5.507.63686
40. Malan M, Spedding MF, Sorsdahl K. The prevalence and predictors of intimate partner violence among pregnant women attending a midwife and obstetrics unit in the Western Cape. Global Ment Health. 2018;5. doi:10.1017/gmh.2018.9
41. Agüero JM. COVID-19 and the rise of intimate partner violence. World Dev. 2021;137:105217. doi:10.1016/j.worlddev.2020.105217
42. Gosangi B, Park H, Thomas R, et al. Exacerbation of physical intimate partner violence during COVID-19 pandemic. Radiology. 2021;298(1):E38–E45. doi:10.1148/radiol.2020202866
43. Katana E, Amodan BO, Bulage L, et al. Violence and discrimination among Ugandan residents during the COVID-19 lockdown. BMC Public Health. 2021;21(1):1–13. doi:10.1186/s12889-021-10532-2
44. Nduna M, Tshona SO. Domesticated poly-violence against women during the 2020 Covid-19 lockdown in South Africa. Psychol Stud. 2021;66(3):347–353. doi:10.1007/s12646-021-00616-9
45. Odeku KO. The surge in intimate partner violence Amid COVID-19 pandemic in South Africa. Gend Behav. 2021;19(2):17945–17949.
46. Rockowitz S, Stevens LM, Rockey JC, et al. Patterns of sexual violence against adults and children during the COVID-19 pandemic in Kenya: a prospective cross-sectional study. BMJ Open. 2021;11(9):e048636. doi:10.1136/bmjopen-2021-048636
47. Uzobo E, Ayinmoro AD. Trapped between two pandemics: domestic violence cases under CoViD-19 pandemic lockdown: a scoping review. Int Q Community Health Educ. 2021;0272684X211022121. Doi:10.1177/0272684X211022121
48. Parvin K, Sultana N, Naved RT. Disclosure and help-seeking behavior of women exposed to physical spousal violence in Dhaka slums. BMC Public Health. 2016;16(1):1–8.
49. Spencer RA, Shahrouri M, Halasa L, Khalaf I, Clark CJ. Women’s help-seeking for intimate partner violence in Jordan. Health Care Women Int. 2014;35(4):380–399. doi:10.1080/07399332.2013.815755
50. Vyas S, Mbwambo J. Physical partner violence, women’s economic status and help-seeking behaviour in Dar es Salaam and Mbeya, Tanzania. Glob Health Action. 2017;10(1):1290426. doi:10.1080/16549716.2017.1290426
51. Deuba K, Mainali A, Alvesson HM, Karki DK. Experience of intimate partner violence among young pregnant women in urban slums of Kathmandu Valley, Nepal: a qualitative study. BMC Women’s Health. 2016;16(1):1–10. doi:10.1186/s12905-016-0293-7
52. Hu R, Xue J, Lin K, Sun IY, Wu Y, The Patterns WX. Influencing factors of help-seeking decisions among women survivors of intimate partner violence in China. J Fam Violence. 2020;36(6):669–681. doi:10.1007/s10896-020-00145-5
53. Tenkorang EY, Owusu AY, Help-Seeking KG. Behavior of female victims of intimate partner violence in Ghana: the role of trust and perceived risk of injury. J Fam Violence. 2018;33(5):341–353. doi:10.1007/s10896-018-9959-2
54. TePoel MR, Saftlas AF, Wallis AB, Harland K, Peek-Asa C. Help-seeking behaviors of abused women in an abortion clinic population. J Interpers Violence. 2018;33(10):1604–1628. doi:10.1177/0886260515619168
55. Parvin K, Sultana N, Naved RT. Disclosure and help-seeking behavior of women exposed to physical spousal violence in Dhaka slums. BMC Public Health. 2016;16(1):383.
56. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
57. Odwe G, Undie CC, Obare F. Attitudes towards help-seeking for sexual and gender-based violence in humanitarian settings: the case of Rwamwanja refugee settlement scheme in Uganda. BMC Int Health Hum Rights. 2018;18(1):15. doi:10.1186/s12914-018-0154-6
58. Malpass A, Sales K, Johnson M, Howell A, Agnew-Davies R, Feder G. Women’s experiences of referral to a domestic violence advocate in UK primary care settings: a service-user collaborative study. Br J Gen Pract. 2014;64(620):e151–e158. doi:10.3399/bjgp14X677527
59. Evans MA, Feder GS. Help‐seeking amongst women survivors of domestic violence: a qualitative study of pathways towards formal and informal support. Health Expectations. 2016;19(1):62–73. doi:10.1111/hex.12330
60. Djikanovic B, Wong SL, Jansen HA, et al. Help-seeking behaviour of Serbian women who experienced intimate partner violence. Fam Pract. 2012;29(2):189–195. doi:10.1093/fampra/cmr061
61. Steinbrenner SY, Shawler C, Ferreira S, Draucker C. The lived experience of help-seeking by South African women after sexual assault. Health Care Women Int. 2017;38(5):425–438. PMID: 28409709. doi:10.1080/07399332.2017.1290097
62. Linos N, Slopen N, Berkman L, Subramanian S, Kawachi I. Predictors of help-seeking behaviour among women exposed to violence in Nigeria: a multilevel analysis to evaluate the impact of contextual and individual factors. J Epidemiol Community Health. 2014;68(3):211–217. doi:10.1136/jech-2012-202187
63. Cho H, Shamrova D, Han J-B LP, Levchenko P. Patterns of intimate partner violence victimization and survivors’ help-seeking. J Interpers Violence. 2017;35(21–22):4558–4582. doi:10.1177/0886260517715027
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.