Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Predictive Value of GAD Antibody for Diabetes in Normal Chinese Adults: A Retrospective Cohort Study in China
Authors Li J ![]() , Lin S, Deng C, Xu T
, Lin S, Deng C, Xu T ![]()
Received 20 December 2020
Accepted for publication 11 February 2021
Published 1 March 2021 Volume 2021:14 Pages 885—893
DOI https://doi.org/10.2147/DMSO.S298068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Jing Li,1 Songbai Lin,1 Chuiwen Deng,2 Tengda Xu1
1Department of Health Management, Peking Union Medical College Hospital, Beijing, People’s Republic of China; 2Rheumatology and Immunology Department, Peking Union Medical College Hospital, Beijing, People’s Republic of China
Correspondence: Tengda Xu
Department of Health Management, Peking Union Medical College Hospital, 1# Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China
Tel/Fax +86 10 6915 9866
Email [email protected]
Purpose: To investigate the prevalence of GAD antibody (GADA) in the general adult population and to evaluate its predictive value for diabetes in China.
Patients and Methods: We searched the PUMCH-HM database and identified 36,731 adult subjects with GADA test results from 2012 to 2015. We then established a retrospective cohort of 4835 nondiabetic subjects at baseline with complete annual health evaluation records through 2019. The median follow-up time was 4.8 (3.0– 7.3) years.
Results: The overall prevalence of GADA was 0.53% and was higher in diabetic subjects (1.25%) than in nondiabetic subjects (0.47%). We found a decrease in baseline body mass index (BMI) from the GADA- to GADAhigh subgroups among baseline diabetic and prediabetic patients and also those who developed diabetes later in the cohort study. A total of 136 subjects (2.8%) developed diabetes after a median follow-up of 3.5 years. For GADA+ participants, BMI was not associated with the risk for diabetes. In the Cox regression model, the GADAlow and GADAhigh exhibited 2.63-fold and 4.16-fold increased risk for diabetes, respectively. This increased risk for diabetes by GADA-positivity is only found in male adults (HR 4.55, 95% CI 2.25– 9.23).
Conclusion: GADA has a low prevalence in China but is associated with a 2.63– 4.16-fold increased risk for diabetes.
Keywords: autoimmune diabetes, glutamic acid decarboxylase antibody, latent autoimmune diabetes in adults, obesity, prevention
Introduction
The prevalence of diabetes in China has increased dramatically in the last three decades from 1% in 1980 to 12.8% in 2017.1,2 China had the largest number of adults with diabetes in 2019 and is estimated to keep as rank 1 in 2030.3 A better understanding of the factors contributing to the diabetes epidemic is crucial for prevention and intervention strategies. The etiology, epidemiology and prevention of type 2 diabetes have drawn enormous attention from Chinese clinicians, while little effort has been made regarding autoimmune diabetes in the adult Chinese population. A few studies have indicated that autoimmune diabetes in adults is much more common than originally thought in China. Most cases of new onset type 1 diabetes in China occurred among adults,4 and 5.9% of newly diagnosed type 2 diabetes patients were actually latent autoimmune diabetes in adults (LADA) according to the LADA China Study.5 Considering the large population, there are likely a large number of autoimmune diabetes patients among Chinese adults.
It has been found that an increasing number of new autoimmune diabetes cases occur during adulthood.6 With the destruction of pancreatic islet beta cells, autoimmune diabetes in adults follows a different clinical course and may quickly progress to insulin-dependent diabetes. Autoantibodies against beta cells include glutamic acid decarboxylase antibody (GADA), insulin autoantibody (IAA), insulinoma-associated antigen-2 autoantibody (IA-2A) and zinc transporter-8 autoantibody (ZnT8A). Among these antibodies, GADA is the most common marker in both adult-onset type 1 diabetes and LADA patients.7,8
It has been reported that autoimmune antibodies may be present years before disease onset,9,10 indicating that there is a prediabetic period in which the disease could be identified before clinical onset through antibody screening in a healthy population. However, there are only a few studies regarding the prevalence of autoantibodies in the general adult population,11,12 and the previous results of the predictive value of GADA in adults are not consistent.13,14 In China, no data on the predictive role of GADA for diabetes are available because no cross-sectional or longitudinal study has been performed in nondiabetic people. Considering the previously reported ethnic differences in autoimmune diabetes prevalence,4,5,15 such studies in China are necessary.
In this study, we investigated the prevalence of GADA in normal Chinese adults and established a 7-year retrospective cohort of baseline nondiabetic adults. We aimed to assess the necessity of screening GADA in normal adults and the impact of autoantibodies in the general population in China.
Patients and Methods
Data Source
The data were collected from the Peking Union Medical College Hospital-Health Management (PUMCH-HM) database. This database was established in 2008 mainly to keep records of annual health evaluations of urban residents in Beijing. By 31-12-2019, the database had collected 844,158 annual health evaluation records of 462,375 participants. These annual health evaluations were paid for by the participants themselves or by their employers since they were not covered by medical insurance in China. All clinical data were collected during a half-day clinic visit. Participants had their medical history reviewed by an internal physician, and previous diagnoses and medicines used were recorded. Blood samples were drawn after the patient had been fasting for at least 8 hours. All the participants were invited to undergo their regular annual health evaluation at PUMCH every year. Clinical data were collected at each visit.
Study Population
We searched the database from 2012 to 2015 and identified 36,731 adult subjects (≥18 years old) with GADA test results and complete clinical records. For the 34,108 nondiabetic subjects, we further searched the database for their records from 2012 to 2019 and identified those who continued their sequential annual health evaluation in PUMCH and had complete medical records through 2019. Through this process, we assembled a retrospective cohort of 4835 nondiabetic participants at baseline. The date of incident diabetes development was defined as the date of their clinic visit at which they first met the definition of diabetes. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Peking Union Medical College Hospital Ethics Committee (No. S-K1368). Informed consent was obtained from all patients for being included in the study.
Definition of Diabetes and Prediabetes
We used the 2020 American Diabetes Association (ADA) definition for diabetes and prediabetes.16 The diabetes diagnostic criteria were defined as meeting any one or a combination of the following: fasting plasma glucose (FPG)≥7.0 mmol/L, HbA1c≥6.5%, or a self-reported previous diagnosis by health care professionals. The prediabetes diagnostic criteria were defined as FPG 5.6 mmol/L to 6.9 mmol/L, or HbA1C 5.7–6.4%, and no previous diagnosis of diabetes. Oral glucose tolerance test (OGTT) data were not available since it is not practical to conduct during a half-day clinic visit for normal participants.
Test of GADA
GADA was analyzed in the PUMCH laboratory by Enzyme-Linked Immunosorbent Assay, ELISA (EUROIMMUN AG, Germany). The assay has a cut‐off of 10 IU/mL according to the manufacturer’s instructions (sensitivity of 92%, specificity of 98% for 150 Diabetes Autoantibody Standardization Program [DASP, 2003] serums from USA) and has a maximum value of 2000 IU/mL. Positive samples were reassessed to confirm their positivity.
Anthropometric and Metabolic Measurements
The subjects’ weight and height were measured by a body composition analyzer. BMI was calculated as weight (kg) divided by squared height (m2). Overweight and obesity were defined as BMI ≥24 kg/m2 and BMI ≥28 kg/m2 according to the 2016 Chinese consensus.17 Central obesity (CO) was defined as waist circumference ≥90 cm for men and ≥80cm for women. Blood pressure was measured twice by experienced nurses, and the mean value was recorded. Blood samples were drawn after the patient had been fasting for at least 8 hours for the measurement of FPG, serum total cholesterol, HDL cholesterol, LDL cholesterol, triglycerides and uric acid. Whole blood was collected for HbA1c measurement. All samples with abnormal results were measured in duplicate.
Statistical Analysis
All statistical analyses were performed using IBM SPSS statistics software version 26 (IBM, Armonk, NY, USA). Data are given as numbers and percentages for categorical data and as the mean (standard deviation (SD)) for continuous data. Triglyceride was log10-transformed to account for the skewed distribution. The chi-square test (Pearson) was used to compare differences in categorical data. t-test and single-factor analysis of variance (ANOVA) was used to test the differences in continuous data between two groups or among more than two groups. Cox’s proportional hazard regression was used to assess the cumulative risk for incident diabetes after proportional hazard assumption tested. Sex, age, BMI (as normal, overweight and obesity), prediabetes and GADA status were included in the multivariate model. A two-tailed P value of 0.05 was considered to be significant.
Results
GADA Prevalence at Baseline
The mean age of the 36,731 adult subjects identified was 44 (18–94) years, and 19,542 (53.2%) participants were male. A total of 2623 (7.1%) participants were diabetic at the baseline, 9886 (26.9%) participants met the criteria of prediabetes. GADA was positive in 195 (0.53%) participants, 94 male and 101 female, P=0.161. The frequency of GADA was significantly elevated in diabetic participants than in nondiabetic ones (n=33, 1.25% vs n=162, 0.47% respectively, P<0.001).
For the GADA+ subjects, the median GADA titer was 51 IU/mL (lower quarter 21 IU/mL, higher quarter 199 IU/mL). We defined GADAhigh as the highest quartile (≥199 IU/mL) and GADAlow as the lower three quartiles (<199IU/mL).
Clinical Parameter Differences According to GADA Status
Table 1 presents demographic and clinical characteristics of participants at baseline according to their GADA status in participants with normal glucose, prediabetes and diabetes. For the 2623 subjects with baseline diabetes, BMI, triglycerides and uric acid declined from the GADA− to GADAlow to GADAhigh subgroups (BMI 26.83 kg/m2, 25.24 kg/m2, 24.11 kg/m2 respectively, P=0.008; triglycerides 1.86 mmol/L, 1.35 mmol/L, 1.10 mmol/L, respectively, P=0.009; uric acid 337 μmol/L, 281 μmol/L, 241 μmol/L, respectively, P<0.001). The trend of BMI decline was also found in prediabetic participants (25.82 kg/m2, 25.13 kg/m2, 23.74 kg/m2 respectively, P=0.024), but not in participants with normal glucose. For GADA+ subjects, no difference of BMI was found between diabetic and nondiabetic groups (24.13 [3.62] kg/m2 vs 25.03 [2.75] kg/m2, P=0.180)
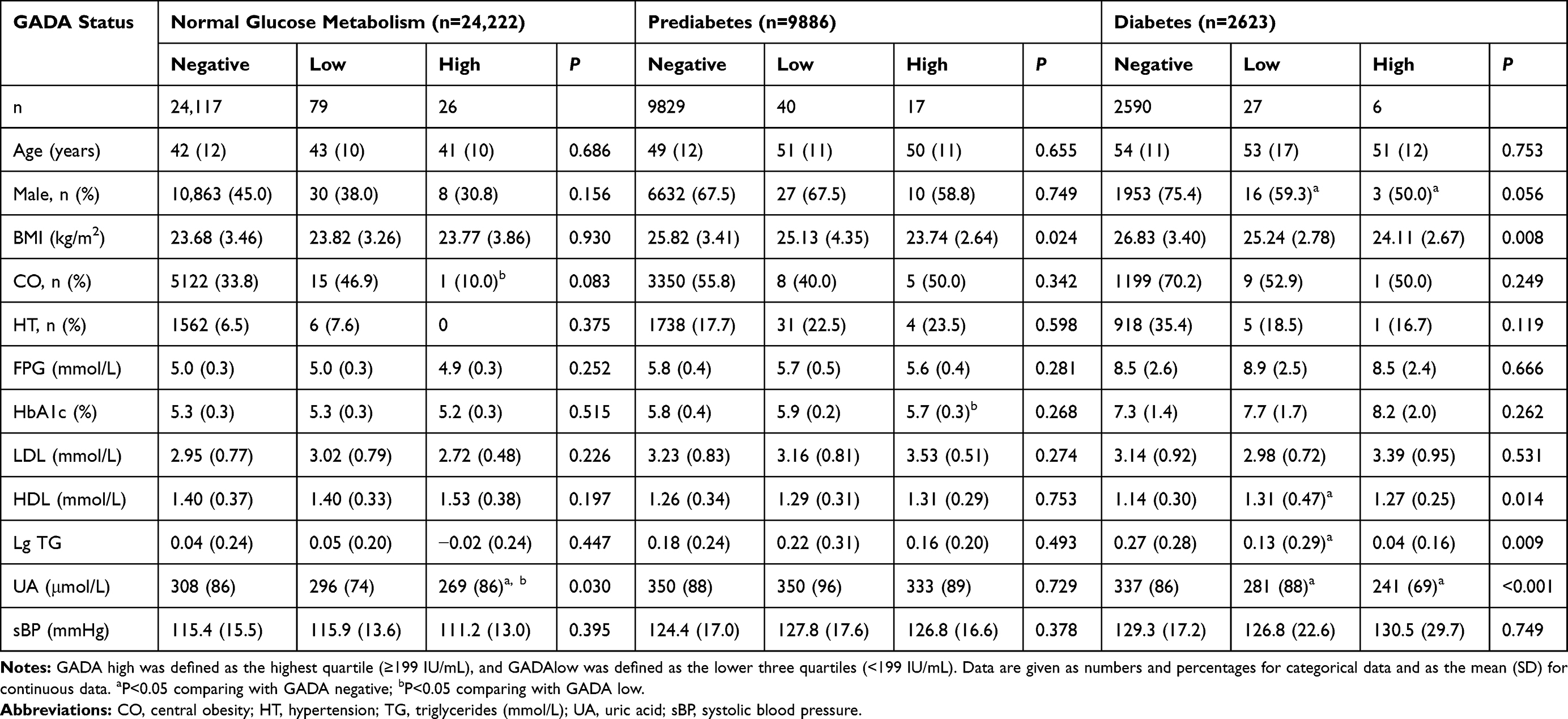 |
Table 1 Demographic and Clinical Characteristics of 36,731 Participants at Baseline According to Their GADA Status |
Incident Diabetes at Follow-Up
Of the 34,108 nondiabetic subjects, 4835 (94 GADA+) continued their sequential annual health evaluation in PUMCH and had full medical records through 2019. The median follow-up time was 4.8 (3.0–7.3) years. A total of 136 subjects (92 male, 44 female) developed diabetes during a median follow-up of 3.5 (0.1–7.0) years after the baseline examination. Table 2 presents demographic and clinical characteristics at baseline of all the 4835 participants and of the 136 ones with incident diabetes according to their GADA status. For the 136 subjects who developed diabetes, baseline BMI decreased significantly from GADA − to GADAlow to GADAhigh (26.57 kg/m2, 26.36 kg/m2, 22.11 kg/m2, respectively, P=0.016). The median age of diabetes diagnosis was reduced from GADA− to GADAlow to GADAhigh but not significantly (55 years old, 53 years old, and 45 years old, respectively, P=0.174).
 |
Table 2 Demographic and Clinical Characteristics of All the 4835 Participants in the Retrospective Cohort and 136 Ones with Incident Diabetes According to Their GADA Status |
The incidence of diabetes development in the different GADA subgroups was 123 (2.6%) among GADA- patients, 8 (12.1%) among GADAlow patients and 5 (17.9%) among GADAhigh patients, P<0.001. More than one-third of the participants (5 of 14) with GADA≥669 IU/mL developed diabetes. We contacted the 13 (9 male, 4 female) participants with incident diabetes in GADA+ group by phone calls to confirm their classification of diabetes and insulin uses. Three subjects with GADAhigh (GADA titer 669 IU/mL, 2000 IU/mL, 1224 IU/mL, respectively) were classified as having type 1 diabetes and started insulin therapy within six months. Only one subject was classified as LADA by his clinical physician and started insulin therapy one year after diagnosis.
Of the 1402 participants with prediabetes at baseline, 124 developed diabetes: 112 (8.2%) in GADA−, 8 (34.8%) in GADAlow and 4 (36.4%) in GADAhigh, P<0.001. Of the 3433 participants with normal glucose metabolism, 655 developed prediabetes (638 [18.9%] in GADA−, 12 [27.9%] in GADAlow, 5 [29.4%] in GADAhigh, P=0.157), 12 developed diabetes (11 [0.3%] in GADA−, 1 [5.9%] in GADAhigh who diagnosed as type 1 diabetes).
Clinical Parameter Differences According to Incident Diabetes
The comparison of clinical characteristics between participants with and without incident diabetes was presented in Table 3. For GADA− participants, those who developed diabetes had significantly different clinical features in age, sex, BMI and all the metabolic parameters (P≤0.001). For GADA+ participants, we only found baseline prediabetes, male sex, and higher uric acid associated with incident diabetes.
 |
Table 3 Comparation of Demographic and Clinical Characteristics of Participants in the Retrospective Cohort According to with/without Incident Diabetes |
Cox Regression of Incident Diabetes
In the Cox’s proportional hazard regression model, increased risk of incident diabetes was associated with GADA positivity (HR: GADAlow 2.63 [95% CI 1.26–5.51], GADAhigh 4.16 [95% CI 1.69–10.25], P=0.004), higher baseline BMI (HR: overweight 1.77 [95% CI 1.17–2.70], obesity 2.42 [95% CI 1.50–3.90], P=0.001), prediabetes (HR: 18.35 [95% CI 9.99–33.70], P<0.001) and older age (HR: 1.02 [95% CI 1.00–1.03], P=0.037). We also found an interaction between GADA positivity and male sex (P<0.001) in the regression. So we further performed Cox’s regression in male and female subgroups and found that GADA positivity increased the risk for incident diabetes only in male (HR: 4.55 [95% CI 2.25–9.23], P<0.001) but not in female (P=0.368), as presented in Figure 1.
 |
Figure 1 Cumulative (Cum) incidence of diabetes among all the subjects and male/female subgroups. Notes: (A and B) Cumulative incidence of diabetes among all the subjects; (C) Cumulative incidence of diabetes among male subjects; (D) Cumulative incidence of diabetes among female subjects. |
Discussion
Our study is by far the largest GADA study in the general adult population worldwide and the first one conducted in China. We observed a low prevalence of GADA in Chinese adults (0.53%) compared with the findings of other reports from Norway,18 Italy,19 the Netherlands,20 Finland,13,21 the United States,11,12 and Japan,22 in which the frequencies range from 1% to 5.9% in the general adult population. The low prevalence in China is consistent with the fact that the incidence of type 1 diabetes in Chinese children was among the lowest; the incidence is 0.1/100,000/year in China compared to 40.9/100,000/year in Finland,4,15 and the frequencies of autoantibodies in type 2 diabetes patients are generally lower in Asians than in Caucasians.23 The reasons for this ethnic difference may be related to the distinct genetic background of Chinese individuals and differences in environmental factors. GADA was more frequently found in diabetic subjects than in nondiabetic ones, which was also reported in previous studies.11,19–21
Autoantibodies might be present 10–20 years before autoimmune diabetes diagnosis.9,10 There is no doubt that autoantibodies predict the incidence of type 1 diabetes in children.24 However, inconsistent results have been found regarding the predictive ability of GADA for diabetes in adults, so its predictive value in the normal adult population is controversial. Previous studies in the general population were limited, and some of the studies had very small samples. In the American Diabetes Prevention Program, GADA was found to not be a predictive factor in 3050 individuals after 3.2 years of follow-up.12 However, the participants in that study were actually at high risk for diabetes and were not normal adults. The other three studies with negative predictive results in northern Italy,19 the USA25 and Sweden26 are limited by their small GADA+ samples. The present study showed that GADAhigh was associated with a 4.16-fold increased risk, and GADAlow was associated with a 2.63-fold increased risk of diabetes among Chinese adults. One-third of the subjects with GADA≥669 IU/mL developed diabetes. Similar results were found in two previous longitudinal studies conducted in Finland and Sweden, in which GADA positivity conferred a 4.9- to 6-fold increased risk of diabetes.13,14 Nevertheless, considering the low prevalence of GADA reported in this study, the economic benefit of screening may not be significant in China.
81% of the epidemiology investigations about type 1 diabetes reported that the incidence in male adults was larger than that in female adults (male-to-female ratio 1.47), even in low–incidence countries such as China.27,28 However the frequency of GADA did not vary between genders, either in our study or previous studies.5,18 We found that the increased risk of diabetes by GADA-positivity is only limited in male adults. This result implicated that there might be a different mechanism of GADA promoting diabetes in male adults but possible explanation of this difference needs further researches.
Reports have indicated that individuals with high levels of autoantibodies have more type 1 diabetes-like phenotypes and that individuals with low levels of autoantibody positivity have more type 2 diabetes-like phenotypes.8 In our study, the three subjects who developed type 1 diabetes were all in the GADAhigh subgroup. All the other 10 GADA+ patients with incident diabetes met the diagnostic criteria of LADA (>30 years old, autoimmune antibody positive, not requiring insulin treatment in 6 months), while only one of them was recognized by his clinical physician. In China, even in a city such as Beijing, which has well-developed medical resources, the knowledge of LADA is still limited, and autoantibody screening has not become a standard process in the diagnosis of diabetes. More attention is needed for autoimmune diabetes in adults in clinical practice in China.
Excessive weight is associated with insulin resistance and is a risk factor for type 2 diabetes. The role of excess weight in the progression of autoimmune diabetes is not clear. In our study, we found that GADA status did not stratify subjects with normal glucose by BMI, as shown in the HUNT study.18 However, for patients with diabetes or prediabetes, GADA+ patients were thinner. This finding is consistent with previous reports from the United States and China that showed that among diabetic participants, being GADA positive was associated with a lower BMI.5,11 We also found that in the subjects who develop diabetes later, GADA+ subjects had reduced baseline BMI, as reported before.13 These findings indicate that although GADA status did not stratify the general population with normal glucose, in those who will develop diabetes later, insulin resistance played a less important role in GADA+ individuals, especially in those with high GADA titers.
The first genome-wide association study (GWAS) of LADA in 2018 showed that both the genetic variants predisposing individuals to type 1 diabetes and the polygenic predisposition to type 2 diabetes contribute to the genetic background of LADA.29 Previous reviews concluded that obesity was associated with an increased risk of LADA, especially in patients with low GADA titers, from the results of HUNT and ESTRID cross-sectional studies.30,31 However, in this study, BMI is not associated with the risk of diabetes for GADA+ participants either in the baseline investigation or in the retrospective cohort study. The small number of incident diabetes in GADA+ participants and limited follow-up time may affect the result. Further prospective investigations exploring the role of obesity in the progression of autoimmune diabetes are needed in the future.
Our study is limited by its retrospective design. The GADA test was not repeated during follow-up, and we know that GADA-positive status may be transient and that the fluctuation of GADA levels is associated with disease progression.9 For the 13 patients with incident diabetes in GADA+ group, we were not able to recall them back to the hospital for further classification of diabetes diagnosis due to the COVID-19. Our study is also limited in the context of extrapolation to the general Chinese population since it is a one-center study, and the participants were mostly citizens with high socioeconomic status from North China.
Conclusion
GADA has a low prevalence in China but is associated with a 2.63–4.16-fold increased risk for diabetes. This increased risk for diabetes is only found in male adults but not in females. Among the participants with diabetes or prediabetes, GADA+ ones were thinner than GADA− ones. BMI was not associated with the risk of diabetes in GADA+ participants either in the baseline cross-sectional investigation or in the cohort study. Further prospective investigations exploring the role of gender and obesity in the progression of autoimmune diabetes are needed.
Acknowledgments
We acknowledge all the health-care workers involved in the establishment of PUMCH-HM database in Peking Union Medical College Hospital.
Funding
This study was supported by the CAMS Innovation Fund for Medical Sciences (CIFMS-2018-I2M-AI-005).
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Diabetes Co-operative Study Group (1981). A mass survey of diabetes mellitus in a population of 300,000 in 24 provinces and municipalities in China. Zhonghua Nei Ke Za Zhi. 1981;20(20):678–683.
2. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: National cross sectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
3. International Diabetes Federation. IDF diabetes atlas [Internet]. 9th ed.; 2019. Available from: http://www.diabetesatlas.org.
4. Weng J, Zhou Z, Guo L, et al. Incidence of type 1 diabetes in China, 2010–13: population based study. BMJ. 2018;360:j5295. doi:10.1136/bmj.j5295
5. Zhou Z, Xiang Y, Ji L, et al. Frequency, immunogenetics, and clinical characteristics of latent autoimmune diabetes in China (LADA China study): a nationwide, multicenter, clinic-based cross-sectional study. Diabetes. 2013;62(2):543–550. doi:10.2337/db12-0207
6. Maddaloni E, Moretti C, Mignogna C, et al. Adult-onset autoimmune diabetes in 2020: an update. Maturitas. 2020;137(March):37–44. doi:10.1016/j.maturitas.2020.04.014
7. Hawa MI, Kolb H, Schloot N, et al. Adult-onset autoimmune diabetes in Europe is prevalent with a broad clinical phenotype: action LADA 7. Diabetes Care. 2013;36(4):908–913. doi:10.2337/dc12-0931
8. Sørgjerd EP. Type 1 diabetes-related autoantibodies in different forms of diabetes. Curr Diabetes Rev. 2019;15(3):199–204. doi:10.2174/1573399814666180730105351
9. Sørgjerd EP, Skorpen F, Kvaløy K, et al. Time dynamics of autoantibodies are coupled to phenotypes and add to the heterogeneity of autoimmune diabetes in adults: the HUNT study, Norway. Diabetologia. 2012;55(5):1310–1318. doi:10.1007/s00125-012-2463-y
10. Tuomilehto J, Zimmet P, Mackay IR, et al. Antibodies to glutamic acid decarboxylase as predictors of insulin-dependent diabetes mellitus before clinical onset of disease. Lancet. 1994;343(8910):1383–1385. doi:10.1016/S0140-6736(94)92521-6
11. Barinas-Mitchell E, Pietropaolo S, Zhang YJ, et al. Islet cell autoimmunity in a triethnic adult population of the third national health and nutrition examination survey. Diabetes. 2004;53(5):1293–1302. doi:10.2337/diabetes.53.5.1293
12. Dabelea D, Ma Y, Knowler WC, et al. Diabetes autoantibodies do not predict progression to diabetes in adults: the diabetes prevention program. Diabet Med. 2014;31(9):1064–1068. doi:10.1111/dme.12437
13. Lundgren VM, Isomaa B, Lyssenko V, et al. GAD antibody positivity predicts type 2 diabetes in an adult population. Diabetes. 2010;59(2):416–422. doi:10.2337/db09-0747
14. Hampe CS, Hall TR, Ågren Å, et al. Longitudinal changes in epitope recognition of autoantibodies against glutamate decarboxylase 65 (GAD65Ab) in prediabetic adults developing diabetes. Clin Exp Immunol. 2007;148(1):72–78. doi:10.1111/j.1365-2249.2007.03334.x
15. Karvonen M. Incidence and trends of childhood Type 1 diabetes worldwide 1990–1999. Diabet Med. 2006;23(8):857–866.
16. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2020. Diabetes Care. 2020;43(January):S14–S31. doi:10.2337/dc20-S002
17. Chinese Expert Consensus Committee for Medical Nutrition Treatment of Overweight and Obesity. Consensus among experts in medical nutrition treatment of overweight/obesity in China (2016 edition). Chin J Diabetes Mellit. 2016;8(9):525–536.
18. Sørgjerd EP, Thorsby PM, Torjesen PA, et al. Presence of anti-GAD in a non-diabetic population of adults; time dynamics and clinical influence: results from the HUNT study. BMJ Open Diabetes Res Care. 2015;3(1):e000076. doi:10.1136/bmjdrc-2014-000076
19. Bosi E, Garancini MP, Poggiali F, et al. Low prevalence of islet autoimmunity in adult diabetes and low predictive value of islet autoantibodies in the general adult population of northern Italy. Diabetologia. 1999;42(7):840–844. doi:10.1007/s001250051235
20. Ruige JB, Batstra MR, Aanstoot HJ, et al. Low prevalence of antibodies to GAD65 in a 50- to 74-year-old general Dutch population: the Hoorn study. Diabetes Care. 1997;20(7):1108–1110. doi:10.2337/diacare.20.7.1108
21. Tuomi T, Carlsson ÅL, Li H, et al. Clinical and genetic characteristics of type 2 diabetes with and without GAD antibodies. Diabetes. 1999;48(1):150–157. doi:10.2337/diabetes.48.1.150
22. Tsuruoka A, Matsuba I, Toyota T, et al. Antibodies to GAD in Japanese diabetic patients: a multicenter study. Diabetes Res Clin Pract. 1995;28(3):191–199. doi:10.1016/0168-8227(95)01101-I
23. Xiang Y, Zhou Z, Deng C, et al. Latent autoimmune diabetes in adults in Asians: similarities and differences between East and West. J Diabetes. 2013;5(2):118–126.
24. Knip M, Korhonen S, Kulmala P, et al. Prediction of type 1 diabetes in the general population. Diabetes Care. 2010;33(6):1206–1212. doi:10.2337/dc09-1040
25. Vigo A, Duncan BB, Schmidt MI, et al. Glutamic acid decarboxylase antibodies are indicators of the course, but not of the onset, of diabetes in middle-aged adults: the atherosclerosis risk in communities study. Brazilian J Med Biol Res. 2007;40(7):933–941. doi:10.1590/S0100-879X2006005000121
26. Rolandsson O, Hägg E, Nilsson M, et al. Prediction of diabetes with body mass index, oral glucose tolerance test and islet cell autoantibodies in a regional population. J Intern Med. 2001;249(4):279–288. doi:10.1046/j.1365-2796.2001.00813.x
27. Diaz-Valencia PA, Bougnères P, Valleron AJ. Global epidemiology of type 1 diabetes in young adults and adults: a systematic review. BMC Public Health. 2015;15:255. doi:10.1186/s12889-015-1591-y
28. Norris JM, Johnson RK, Stene LC. Type 1 diabetes—early life origins and changing epidemiology. Lancet Diabetes Endocrinol. 2020;8(3):226–238. doi:10.1016/S2213-8587(19)30412-7
29. Cousminer DL, Ahlqvist E, Mishra R, et al. First genome-wide association study of latent autoimmune diabetes in adults reveals novel insights linking immune and metabolic diabetes. Diabetes Care. 2018;41(11):2396–2403. doi:10.2337/dc18-1032
30. Carlsson S. Environmental (Lifestyle) risk factors for LADA. Curr Diabetes Rev. 2019;15(3):178–187. doi:10.2174/1573399814666180716150253
31. Hjort R, Ahlqvist E, Carlsson PO, et al. Overweight, obesity and the risk of LADA: results from a Swedish case–control study and the Norwegian HUNT Study. Diabetologia. 2018;61(6):1333–1343. doi:10.1007/s00125-018-4596-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.