Back to Journals » Journal of Asthma and Allergy » Volume 18
Predictive Value of Computed Tomographic Ethmoid-to-Maxillary Ratio in Patients with Chronic Rhinosinusitis and Nasal Polyp
Authors Wu PW ![]() , Wei ZH
, Wei ZH ![]() , Huang CC
, Huang CC ![]() , Chang PH
, Chang PH ![]() , Lee TJ
, Lee TJ ![]() , Huang CC
, Huang CC ![]()
Received 6 June 2025
Accepted for publication 30 July 2025
Published 12 August 2025 Volume 2025:18 Pages 1167—1177
DOI https://doi.org/10.2147/JAA.S536368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Pei-Wen Wu,1,2 Zih-Hao Wei,2 Chi-Che Huang,1,2 Po-Hung Chang,1 Ta-Jen Lee,1– 3 Chien-Chia Huang1,2
1Division of Rhinology, Department of Otolaryngology, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan; 2School of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Department of Otolaryngology, Xiamen Chang Gung Hospital, Xiamen, People’s Republic of China
Correspondence: Chien-Chia Huang, Division of Rhinology, Department of Otolaryngology, Chang Gung Memorial Hospital and Chang Gung University, No. 5, Fu-Shin Street, Kweishan, Taoyuan, 333, Taiwan, Tel +886-3-3281200 ext. 8466, Fax +886-3-3979361, Email [email protected]
Objective: Different types of inflammation in the sinuses require different treatments. Ethmoid dominance was proposed as an indicator on computed tomography (CT) images for type 2 chronic rhinosinusitis with nasal polyp (CRSwNP). This study evaluated the predictive value of the ethmoid-to-maxillary (E/M) ratio based on different CT scoring systems in type 2 CRSwNP.
Methods: Adult patients with bilateral CRSwNP planning to undergo sinus surgery were prospectively recruited. CT images were evaluated using the Lund-Mackay (L-M) and Zinreich scoring systems which involved a more meticulous quantification of opacification on CT images. Tissue eosinophil count (TEC) was determined by histopathological analysis. The expression levels of type 2 cytokines in nasal polyps, including IL-5, IL-13, and eosinophil cationic protein (ECP), were measured using real-time PCR.
Results: A total of 174 participants were enrolled. Eighty of these participants exhibited an E/M ratio > 1, 49 presented with E/M ratio=1, and 45 showed an E/M ratio < 1 based on L-M CT scores. Twenty of the 49 (40.8%) patients with E/M ratio=1 on L-M score turned to E/M ratio > 1 after re-evaluation by Zinreich scoring system. The E/M ratio based on the L-M and Zinreich scoring systems both exhibited correlation with the tissue markers of type 2 inflammation, including TEC, interleukin (IL)-5, IL-13, and ECP expression levels, although the Zinreich E/M ratio showed a higher correlation coefficient.
Conclusion: The E/M ratio based on the L-M and Zinreich scoring systems correlated with tissue markers of type 2 inflammation. A scale with an E/M ratio of 1 in the L-M system should be further investigated using a more detailed scoring system to determine the presence of an ethmoid-dominant shadow. This could help clinicians better evaluate CT images to determine the severity of type 2 inflammation in patients with CRSwNP and provide optimal therapeutic strategies.
Plain Language Summary: Different types of inflammation in the sinuses require different treatments. Ethmoid dominance was proposed as an indicator on computed tomography (CT) images for type 2 chronic rhinosinusitis with nasal polyp (CRSwNP). This study prospectively enrolled 174 adult patients with bilateral CRSwNP. The ethmoid-to-Maxillary (E/M) ratio based on the L-M (Lund-Mackay) score and a more detailed evaluation with Zinreich scoring systems both exhibited correlation with the tissue markers of type 2 inflammation. A scale with an E/M ratio of 1 in the L-M system should be further investigated using a more detailed scoring system to determine the presence of an ethmoid-dominant shadow. This could help clinicians better evaluate CT images to determine the severity of type 2 inflammation in patients with CRSwNP and provide optimal therapeutic strategies.
Keywords: chronic rhinosinusitis with nasal polyp, ethmoid-to-maxillary ratio, Lund-Mackay scoring system, type 2 inflammation, zinreich scoring system
Graphical Abstract:

Introduction
Chronic rhinosinusitis with nasal polyp (CRSwNP) is a persistent inflammation of the sinonasal mucosa with formation of nasal polyp lasting for over 12 weeks.1 The inflammatory pattern for CRSwNP varies across different regions.2,3 Type 2 inflammation involves the activation of type 2 T-helper cells and innate lymphoid cells, along with elevated levels of type 2 cytokines, including IL-4, IL-5, and IL-13. The infiltration of eosinophil predominant inflammatory cells could be observed in more than 80% of CRSwNP cases in Western countries.4,5 However, only 40–60% of Asian patients with CRSwNP exhibit a type 2 inflammation, and many present with a mixed-type inflammation that includes non-type 2 inflammation and neutrophil infiltration in the sinonasal mucosa.6–9 Patients with different inflammatory patterns of CRSwNP may require different management strategies for optimal treatment outcomes, especially given the increasing use of type 2 biologics in treating CRSwNP.10,11 Therefore, distinguishing between type 2 and non-type 2 inflammation is crucial.
Clinical features of type 2 inflammation in patients with CRSwNP include bilateral nasal polyps, comorbid asthma, smell impairment, predominance of disease in ethmoid sinus, elevated blood eosinophil count (BEC), serum total immunoglobulin E (IgE), and serum eosinophil cationic protein (ECP).1,12,13 Among these features, an ethmoid-dominant shadow on computed tomography (CT) images was first proposed as a clinical diagnostic criterion for eosinophilic chronic rhinosinusitis (CRS) in the Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) study.14 Ethmoid dominance could be assessed as the ethmoid-to-Maxillary (E/M) ratio > 1 on CT images using the Lund-Mackay (L-M) scoring system.8,15 Although the L-M scoring system is the most widely used evaluation method in clinical practice, its scoring scale has limitations. The score of 1 covers a broad range between no opacification (score 0) and total opacification (score 2).16 As a result, both slight and near-total opacification receive the same score, potentially leading to inaccuracies in assessing ethmoid sinus dominance when the E/M ratio exceeds 1. Thus, a more detailed evaluation such as Zinreich scoring systems might be required.17 The present study investigated the accuracy of evaluating ethmoid dominance using the L-M scoring system and the predictive value of the E/M ratio on CT images of type 2 eosinophilic CRSwNP. By comparing the associations between different CT scoring systems and the expression of tissue markers of type 2 inflammation. This could help clinicians better evaluate CT images to determine the severity of type 2 inflammation in patients with CRSwNP and provide optimal therapeutic strategies.
Materials and Methods
Patients
After obtaining approval from the Institutional Review Board of Chang Gung Medical Foundation (IRB numbers: 202002219A3, 202102257A3, and 202202075A3), adult patients (≥18 years) with bilateral CRSwNP scheduled to undergo endoscopic sinus surgery were prospectively recruited between July 2020 and May 2024, after providing signed informed consent. All study procedures were performed in accordance with the relevant guidelines and regulations, and the Declaration of Helsinki. The diagnosis of CRSwNP was based on the EPOS2020 definition.1 Participants had failed in previous conservative medical therapies including intranasal corticosteroids (discontinued 1 month before surgery) and nasal douches. Exclusion criteria included patients with (1) sinonasal neoplasms; (2) concomitant diagnosis of immunologic complications or mucociliary disorder; or (3) history of receiving oral corticosteroids, monoclonal antibodies, or immunosuppressive treatment in the month before enrolment.
Demographic data and clinical characteristics of the participants, including medical history, relevant clinical symptoms, laboratory findings, and imaging results, were obtained and reviewed. Nasal symptoms and quality of life were evaluated using the sinonasal outcome test-22 (SNOT-22).18 Laboratory examinations, including peripheral blood inflammatory cell counts, total serum IgE, immunoCAP, and serum ECP levels, were performed and analyzed. Nasal polyps were graded based on the findings of nasal endoscopy using the nasal polyp scoring system as previously described.19
Our previous study in this research project characterized the clinical features of comorbid asthma and its impact on quality of life in patients with chronic rhinosinusitis with nasal polyps.20 In the current study, we evaluated the association of tissue markers of type 2 inflammation and the E/M ratio based on different CT scoring systems including L-M score and the Zinreich scoring systems.
Sinonasal CT Evaluations
Preoperative CT images were obtained for all participants. The severity of CRS was quantified using the L-M score and the Zinreich scoring systems.16,17 Two rhinologists (C.-C.H. and P.-W.W). independently reviewed the CT images based on consensus. The frontal sinus, anterior ethmoidal cells, posterior ethmoidal cells, maxillary sinus, and sphenoid sinus were scored as 0 (no opacification), 1 (partial opacification), and 2 (total opacification) in the L-M scoring system. In contrast, the Zinreich scoring system grades opacification between 0 and 5 based on the percentage of sinus involvement: (0 = 0%, 1 = 1–25%, 2 = 26–50%, 3 = 51–75%, 4 = 76–99%, and 5 = 100% opacification of sinus). The ostiomeatal complex was assigned a score of either 0 (not obstructed) or 2 (obstructed).
The E/M ratio was obtained by dividing the average CT scores of the anterior and posterior ethmoid sinuses by those of the maxillary sinuses.8,9,15 A higher E/M ratio indicated a greater proportion of disease proportion in the ethmoid sinus area, as well as in the central compartment (Figure 1).
 |
Figure 1 Axial (a) coronal (b) and sagittal (c) sections of CT images were evaluated with different score systems (d). Abbreviations: AE, anterior ethmoid sinus; PE, posterior ethmoid sinus; E/M ratio, ethmoid-to-maxillary ratio; L-M, Lund and Mackay scoring system. |
Tissue Eosinophil Count Quantification
The polyp specimens obtained during surgery were fixed in formalin and embedded in paraffin. Haematoxylin and eosin staining was performed on standard 5-µm sections. The tissue eosinophil count (TEC) was evaluated in three microscopic fields at ×400 magnification (high-power field, HPF), focusing on the areas with the most severe inflammatory cell infiltration (Figure 2).
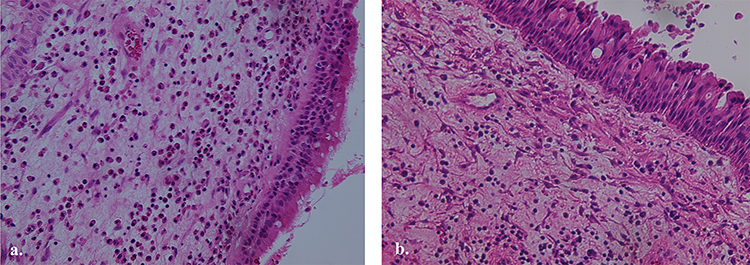 |
Figure 2 Haematoxylin and eosin staining was performed on standard 5-µm sections of nasal polyp specimen. The tissue eosinophil count (TEC) was evaluated in three microscopic fields at ×400 magnification ((a) high-power field, HPF). Type 2 eosinophilic CRSwNP was determined as TEC ≥10/HPF (b) according to the EPOS2020 criteria. |
Tissue Type 2 Marker Expression
Nasal polyp tissues with adequate specimen quantity were processed for real-time polymerase chain reaction (PCR). After homogenization (Retsch, Haan, Germany), total RNA was extracted using an RNeasy Mini Kit (Qiagen GmbH, Strasse, Germany). Random hexamer primers and the High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems, Foster City, CA, USA) were used for reverse transcription. Real-time PCR was performed using primers for IL-5, IL-13, ECP, and glyceraldehyde-3-phosphate dehydrogenase (GAPDH) (Table 1) using the TaqMan assay on an Applied Biosystems 7500 Fast Real-Time PCR System (Applied Biosystems). The conditions for amplification included an initial incubation at 95°C (10 min); followed by 45 cycles of 95°C (10 s), 60°C (20 s), and 72°C (10 s); and then a final cooling to 40°C. Measurements were performed in triplicate for each sample. The relative mRNA levels of the target genes were calculated by the ΔΔCt method, after normalization of the mean threshold cycle (Ct) values to those of GAPDH.
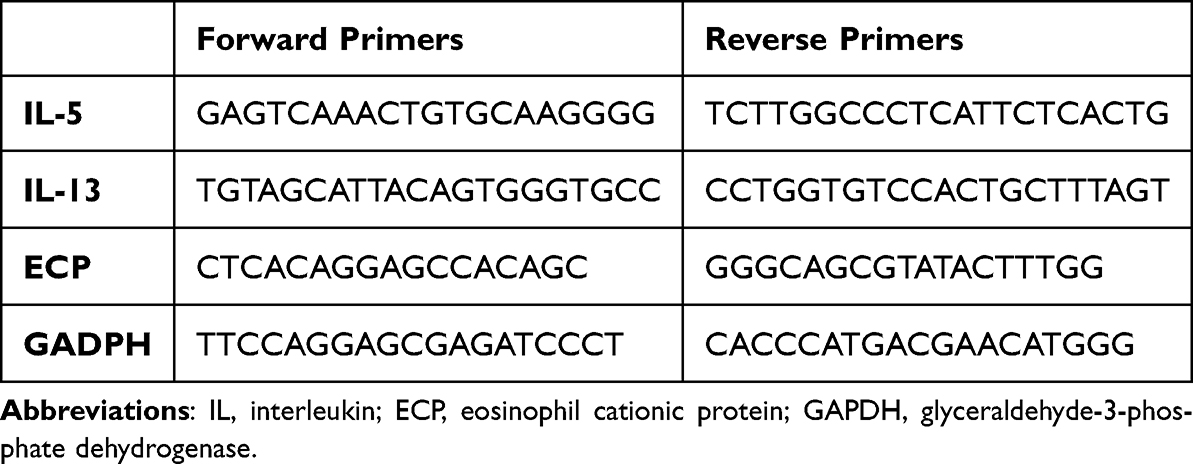 |
Table 1 Primer Sequences Specific to Target Genes |
Statistical Analyses
Statistical analyses were performed using GraphPad Prism 5 (GraphPad Software, San Diego, CA, USA) and SPSS Statistics v27.0. (IBM Corp, Armonk, NY, USA). Correlation analysis between tissue markers of type 2 inflammation and E/M ratio on CT images was performed using Spearman correlation coefficients (rs). Regression analyses were performed to assess the association between the E/M ratio and clinical variables. Receiver operating characteristic (ROC) curves were generated and the area under the ROC curve (AUC) was calculated to identify the cutoff values in predicting patient with eosinophilic CRSwNP (TEC ≥10/HPF according to the EPOS2020 criteria).1 Statistical significance was set at P < 0.05. The power was calculated as 82.7% of the difference between the primary outcomes in the study groups.
Results
Clinical Characteristics of Participants
A total of 174 adult patients with bilateral CRSwNP (124 males and 50 females) were included in this study. The demographic data of the participants are shown in Table 2. Comorbid asthma was present in 32 (18.5%) patients, while 56 (32.4%) had a history of previous sinus surgery. The average SNOT-22 score, L-M score, and nasal polyp score were 48.3 ±19.7, 17.0 ± 3.8, and 5.4 ± 1.6, respectively. The averaged E/M ratios were 1.2 ± 0.4 and 1.3 ± 0.7 as determined by L-M and Zinreich scoring systems respectively. The average BEC and TEC were 302.2 ± 280.9 /μL and 43.3 ± 56.1 /HPF, respectively. A total of 112 (64.0%) patients with TEC ≥ 10/HPF was categorized as type 2 eosinophilic CRSwNP.
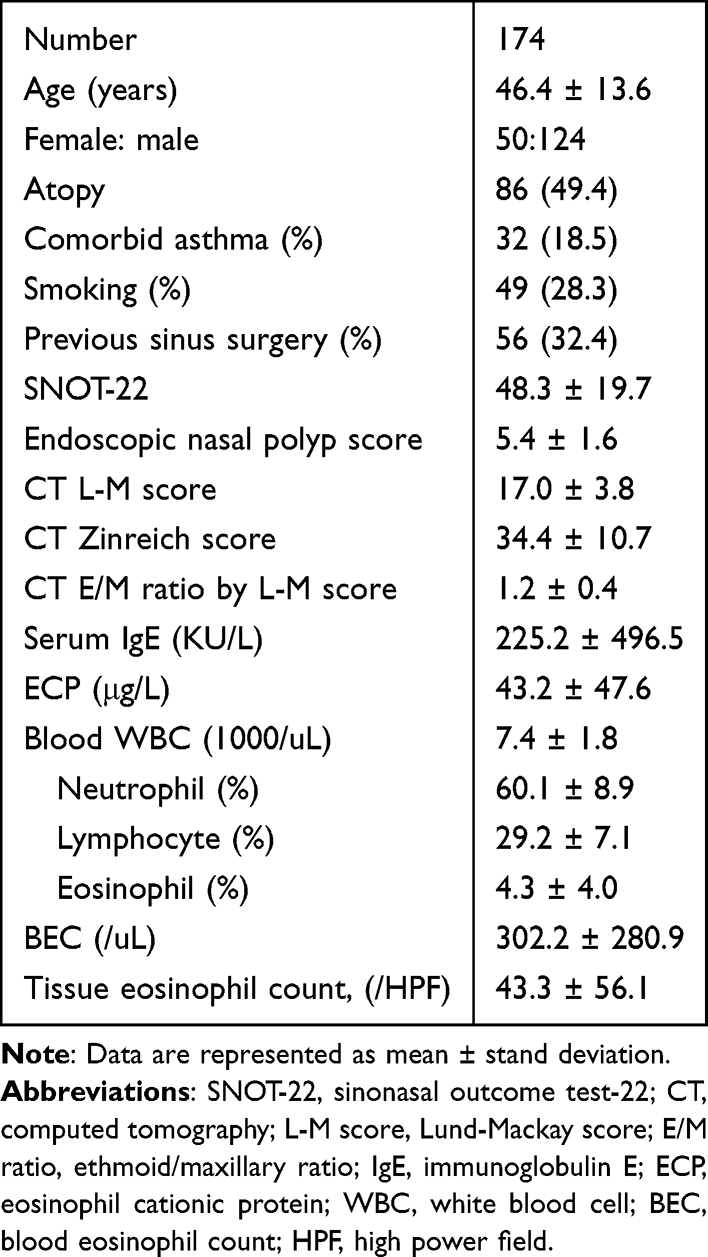 |
Table 2 Clinical Characteristics of Participants |
Ethmoid-Dominant Opacification on CT Images
Among the 174 patients with bilateral CRSwNP, 80 exhibited an E/M ratio > 1, 49 presented an E/M ratio = 1, and 45 showed an EM ratio < 1 based on L-M CT scores. Further evaluation using the Zinreich scoring system in 49 patients presenting with E/M=1 on the L-M score revealed that 20 patients exhibited E/M>1, 7 presented with E/M=1, and 22 showed E/M<1 (Figure 3).
 |
Figure 3 Categorization of ethmoid sinus dominance. Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyp; E/M ratio, ethmoid-to-maxillary ratio. |
Correlation Analysis of E/M Ratio and Markers of Type 2 Inflammation
Linear regression analysis was performed to determine the association between clinical markers of type 2 inflammation and the E/M ratio. The results revealed that comorbid asthma, L-M score, and BEC were significant factors associated with E/M ratio (adjusted β = 0.209, 0.247, and 0.273, all P < 0.05). L-M score and BEC remained statically significant in multiple variable analysis (adjusted β = 0.238 and 0.245, all P < 0.05) (Table 3).
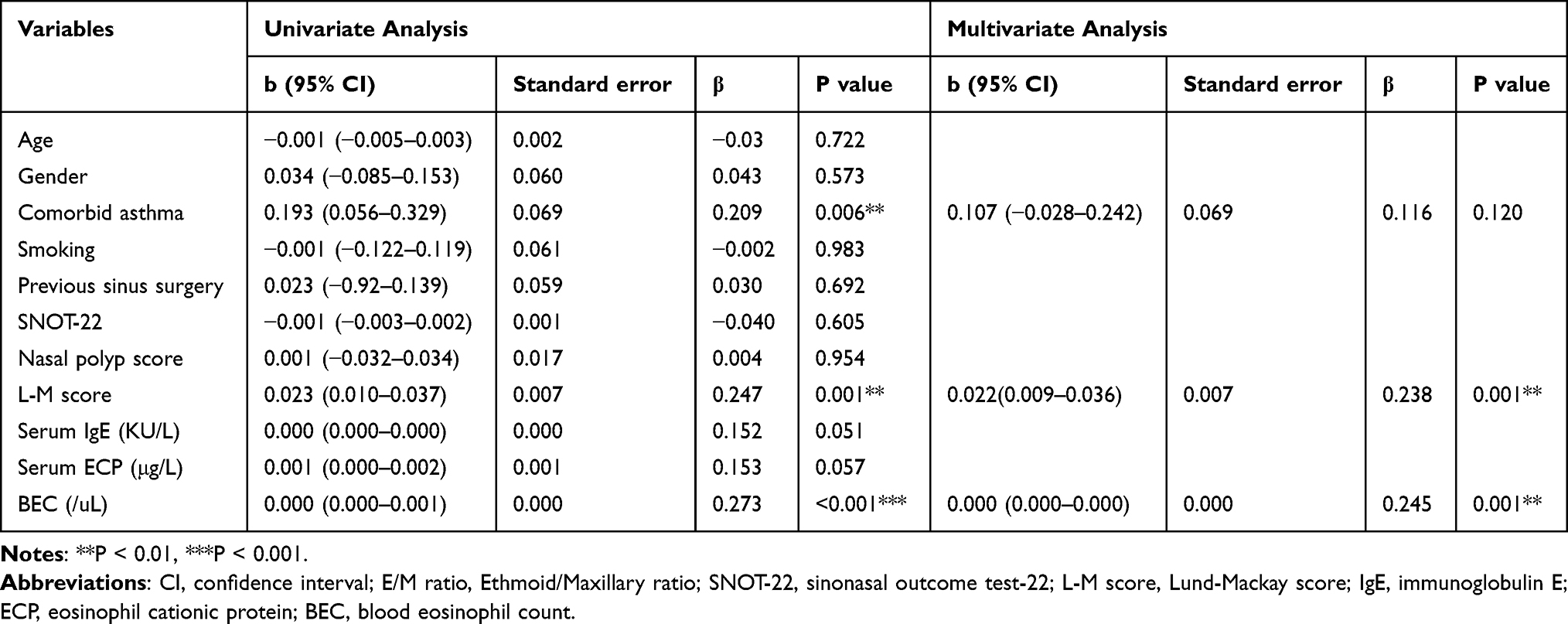 |
Table 3 Linear Regression Analyses of Clinical Variables for E/M Ratio in Participants |
Weak correlations were observed between the L-M E/M ratio and tissue markers of type 2 inflammation, including TEC (Figure 4a), tissue IL-5 (Figure 4b), IL-13 (Figure 4c), and ECP (Figure 4d) expression (rs = 0.279, 0.224, 0.186, and 0.188, respectively; all P < 0.05). Increased correlations were observed between the Zinreich E/M ratio and tissue markers of type 2 inflammation, including TEC (Figure 5a), tissue IL-5 (Figure 5b), IL-13 (Figure 5c), and ECP (Figure 5d) expression (rs = 0.285, 0.282, 0.331, and 0.229, respectively; all P < 0.05).
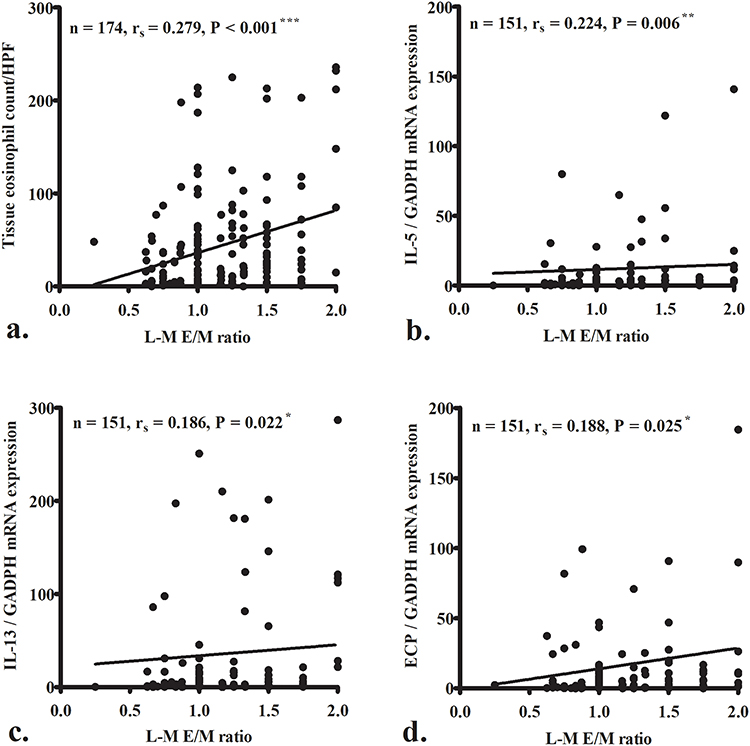 |
Figure 4 Weak correlations were observed between Lund Mackay (L-M) ethmoid-to-maxillary (E/M) ratio and tissue markers of type 2 inflammation, including tissue eosinophil count (TEC) (a), tissue interleukin (IL)-5 (b), IL-13 (c) and eosinophil cationic protein (ECP) (d) expression levels. *P < 0.05; **P < 0.01, ***P < 0.001. GAPDH, glyceraldehyde-3-phosphate dehydrogenase. |
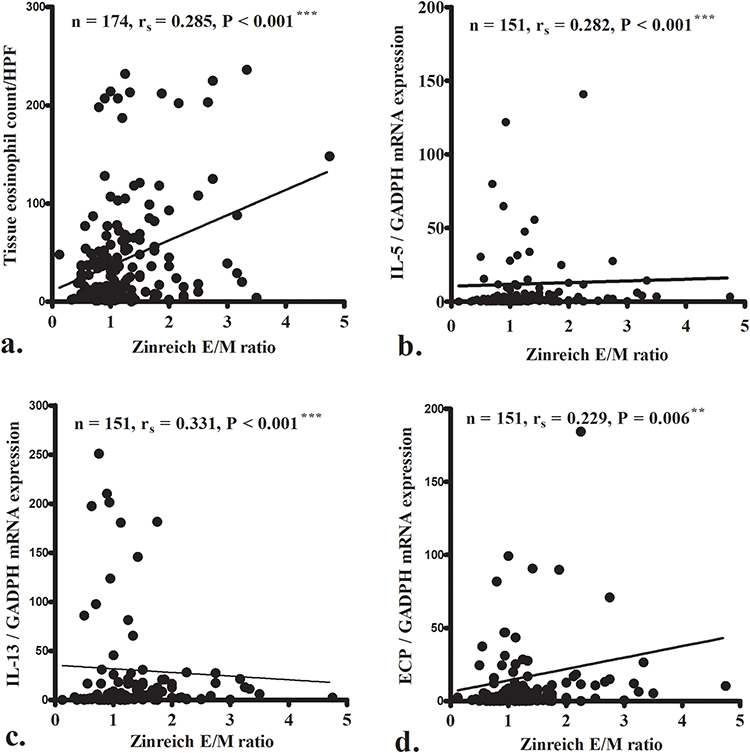 |
Figure 5 Correlations were observed between Zinreich Ethmoid-to-Maxillary (E/M) ratio and tissue markers of type 2 inflammation, including tissue eosinophil count (TEC) (a) tissue interleukin (IL)-5 (b) IL-13 (c) and eosinophil cationic protein (ECP) (d) expression levels. **P < 0.01, ***P < 0.001. GAPDH: glyceraldehyde-3-phosphate dehydrogenase. |
Furthermore, ROC curves were generated, and AUC values were calculated to evaluate the sensitivity and specificity of the L-M and Zinreich E/M ratios for predicting eosinophilic CRSwNP in our cohort. The ROC curves for both L-M (Figure 6a) and the Zinreich (Figure 6b) E/M ratios had AUCs significantly greater than 0.5 (AUC=0.659 and 0.636, respectively; all P < 0.05). The optimal cutoff values for L-M and Zinreich E/M ratios (maximizing the sum of sensitivity and specificity) were L-M E/M ratio > 1.08 (sensitivity, 55.4%; specificity, 71.0%) and Zinreich E/M ratio > 1.07 (sensitivity, 60.7%; specificity, 66.1%).
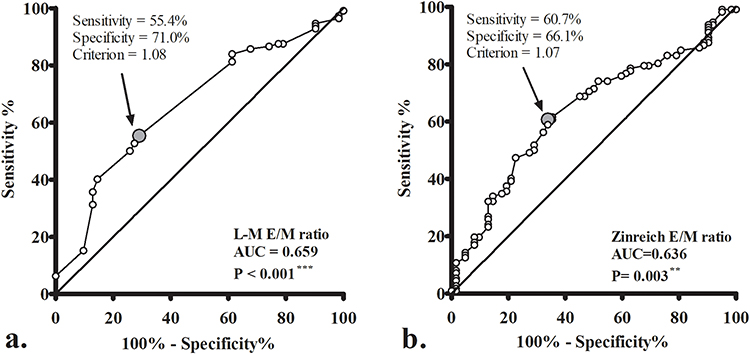 |
Figure 6 Receiver operating characteristic curves of Lund Mackay (L-M) (a) and Zinreich (b) ethmoid-to-maxillary (E/M) ratio were used to predict eosinophilic CRSwNP in our cohort. AUC: area under curve. The optimal cutoff values for L-M and Zinreich E/M ratio (maximizing the sum of sensitivity and specificity) were L-M E/M ratio >1.08 and Zinreich E/M ratio >1.07. **P < 0.01; ***P < 0.001. |
Discussion
Endotype-driven care strategies are crucial in the current treatment of CRSwNP, as severe type 2 eosinophilic CRSwNP is highly susceptible to recurrence after surgery and requires more intensive postoperative care and follow-up.18,21,22 Patients with different inflammatory patterns of CRSwNP may require different management strategies for optimal treatment outcomes. Thus, identifying type 2 eosinophilic CRSwNP is important, especially in an era of biologics being incorporated into the care pathway of CRSwNP.23 According to previous reports, the prevalence of type 2 eosinophilic CRS is approximately 40–60% in various Asian regions, which is relatively lower than that in the Western countries.3 Asian patients with CRSwNP may also exhibit inflammatory pattern with elevated levels of mixed type inflammatory markers.6 These findings also emphasize the importance of differentiating between type 2 and non-type 2 CRSwNP in Asian patients to enhance clinical diagnosis, treatment determination, and outcome prediction.
Among the clinical markers of type 2 CRSwNP, ethmoid-dominant opacification is an indicator of type 2 inflammation on CT imaging and was initially proposed in Japanese study.24 Similar studies were subsequently reported and suggested that the postoperative course was more likely to be poor in patients with high E/M ratio.15,25,26 In the JESREC study, an ethmoid-dominant shadow (ethmoid > maxillary sinus) was suggested as one of the main diagnostic criteria for eosinophilic CRSwNP and an independent predictor of postoperative refractoriness.14
However, ethmoid-dominant shadowing can be difficult to determine objectively. Thus, Meng et al’s study reported that the E/M ratio based on L-M score on CT imaging had the highest predictive value for CRSwNP recurrence in the Chinese population.15 Wu et al’s study revealed that L-M E/M ratio was also a significant clinical predictor for identifying patients with eosinophilic CRSwNP.9 In the current study, regression analysis revealed that comorbid asthma, L-M score, and BEC were significantly associated with E/M ratio. Further multivariable analysis confirmed that L-M score and BEC remained statistically significant predictors. These findings reinforce the E/M ratio as a meaningful indicator of type 2 inflammation on CT imaging.
However, 20 of the 49 participants (40.8%) with E/M ratio=1 based on L-M score, could be further categorized into E/M ratio > 1 after re-evaluation with Zinreich scoring system due to the different scale ranges of the two scoring systems. The L-M scoring system is common and easy to use, but the range of 1 point is wide, as slight or near-total opacification would be scored as the same point. This study further evaluated the correlation between tissue type 2 markers and the E/M ratio based on the L-M and Zinreich score systems. The results showed that both scoring systems exhibited a weak correlation with tissue markers of type 2 inflammation, including TEC, IL-5, IL-13, and ECP expression levels, although the Zinreich E/M ratio showed a slightly higher correlation coefficient. Therefore, a scale with an E/M ratio of 1 and L-M score should be further investigated using a more detailed scoring system, such as the Zinreich scoring system, to determine the presence of an ethmoid-dominant shadow.
Type 2 eosinophilic inflammation in CRS often involves the central sinonasal area, including the nasal septum, olfactory cleft, middle turbinates, and ethmoid cells.12,15 However, the mechanism underlying the predominance of central inflammation in type 2 CRS remains unclear. One proposed hypothesis is that the central sinonasal area is more exposed to inhaled airflow, leading to localized differences in molecular expression patterns.27,28 In our study, the results showed that the E/M ratio with a cutoff values of >1.08 (L-M score) and 1.07 (Zinreich score) can predict eosinophilic CRSwNP, further supporting the clinical utility of these imaging-based parameters in CRSwNP management.
Although the measurement of tissue eosinophil infiltration provides a direct and accurate assessment of type 2 eosinophilic CRSwNP, it requires an invasive procedure to obtain nasal tissue and time-consuming histopathological analysis. Nevertheless, CT imaging is the most widely used diagnostic and evaluative tool for CRS in clinical practice.1 From this standpoint, the E/M ratio appears to be a valuable indicator of type 2 eosinophilic CRSwNP. However, its primary limitation is its reduced diagnostic utility in patients with a pan-sinusitis pattern on CT, where L-M score = 24 and E/M ratio = 1.16,20 Therefore, a scale with an E/M ratio of 1 in the L-M score should be further investigated with a more detailed scoring system to determine the presence of an ethmoid-dominant shadow.
This study has several limitations that warrant consideration. First, this study recruited patients who underwent sinus surgery at a tertiary referral medical center, introducing a potential selection bias. Patients with milder disease or those unwilling to undergo surgery were not included, potentially leading to a higher severity of CRSwNP in the study cohort compared to the general population. Nevertheless, these patients warrant comprehensive evaluation, as they often require multiple treatment modalities, such as surgery and biologics, owing to their high risk of being refractory to treatment or the recurrence of nasal polyps. Second, the cutoff value of expression levels of other type 2 cytokines, such as tissue IL-5, IL-13, and ECP, in determining type 2 eosinophilic CRSwNP were not investigated Additionally, there is no established consensus in the literature regarding these markers.23,29 Instead, we categorized patients with type 2 eosinophilic CRSwNP based on TEC ≥ 10/HPF in histopathological analysis which was suggested by several previous studies.1,8,9 Third, this study did not evaluate treatment response, highlighting the need for future research to determine the predictive value of the E/M ratio in short- and long-term postoperative outcomes. However, our findings suggest that the E/M ratio serves as a useful clinical marker of type 2 inflammation, aiding clinicians in the evaluation and management of CRSwNP to achieve optimal therapeutic outcomes.
Conclusion
The E/M ratio, based on both the L-M and Zinreich scoring systems, correlated with tissue markers of type 2 inflammation, including TEC, IL-5, IL-13, and ECP expression levels. The Zinreich E/M ratio showed a slightly higher correlation coefficient, suggesting it may provide a more refined assessment. Therefore, a scale with an E/M ratio of 1 in the L-M score should be further investigated with a more detailed scoring system to determine the presence of an ethmoid-dominant shadow. This could help clinicians to better evaluate patients with CRSwNP, provide appropriate treatment modalities, and achieve optimal therapeutic outcomes.
Abbreviations
CT, computed tomography; CRSwNP, chronic rhinosinusitis with nasal polyps; E/M ratio, ethmoid-to-maxillary ratio; L-M score, Lund-Mackay score; TEC, Tissue eosinophil count; ECP, eosinophil cationic protein; IL, interleukin; BEC, blood eosinophil count; IgE, immunoglobulin E; CRS, chronic rhinosinusitis; JESREC, Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis; SNOT-22, sinonasal outcome test-22; HPF, high-power field; PCR, polymerase chain reaction; GAPDH, glyceraldehyde-3-phosphate dehydrogenase; ROC, Receiver operating characteristic; AUC, area under the curve.
Funding
The authors received research grants from the Chang Gung Memorial Hospital (CMRPG3P0351 and CMRPG3P0571). The funder played no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(1):1–464. doi:10.4193/Rhin20.401
2. Nakayama T, Lee IT, Le W, et al. Inflammatory molecular endotypes of nasal polyps derived from white and Japanese populations. J Allergy Clin Immunol. 2022;149(4):1296–1308.e6. doi:10.1016/j.jaci.2021.11.017
3. Yao Y, Zeng M, Liu Z. Revisiting Asian chronic rhinosinusitis in the era of type 2 biologics. Clin Exp Allergy. 2022;52(2):231–243. doi:10.1111/cea.14065
4. Kato A, Peters AT, Stevens WW, Schleimer RP, Tan BK, Kern RC. Endotypes of chronic rhinosinusitis: relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy. 2022;77(3):812–826. doi:10.1111/all.15074
5. Cho SH, Hamilos DL, Han DH, Laidlaw TM. Phenotypes of chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2020;8(5):1505–1511. doi:10.1016/j.jaip.2019.12.021
6. Min JY, Kim JY, Sung CM, et al. Inflammatory endotypes of chronic rhinosinusitis in the Korean population: distinct expression of type 3 inflammation. Allergy Asthma Immunol Res. 2023;15(4):437–450. doi:10.4168/aair.2023.15.4.437
7. Yao Y, Zhu HY, Zeng M, Liu Z. Immunological mechanisms and treatable traits of chronic rhinosinusitis in Asia: a narrative review. Clin Otolaryngol. 2023;48(2):363–370. doi:10.1111/coa.14001
8. Lin YT, Lin CF, Liao CK, Yeh TH. Comprehensive evaluation of type 2 endotype and clinical features in patients with chronic rhinosinusitis with nasal polyps in Taiwan: a cross-sectional study. Eur Arch Otorhinolaryngol. 2023;280(12):5379–5389. doi:10.1007/s00405-023-08118-2
9. Wu PW, Huang CC, Chang PH, Lee TJ, Fan YH, Huang CC. Blood eosinophil count is the dominant clinical marker for type 2 inflammatory severity in CRSwNP. Laryngoscope. 2024.
10. Bachert C, Zhang N, Hellings PW, Bousquet J. Endotype-driven care pathways in patients with chronic rhinosinusitis. J Allergy Clin Immunol. 2018;141(5):1543–1551. doi:10.1016/j.jaci.2018.03.004
11. Sima Y, Zhao Y, Wang X, Zhang L. Precision medicine in chronic rhinosinusitis - using endotype and endotype-driven therapeutic options. Expert Rev Clin Immunol. 2023;19(8):949–958. doi:10.1080/1744666X.2023.2232115
12. Stevens WW, Peters AT, Tan BK, et al. Associations between inflammatory endotypes and clinical presentations in chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2019;7(8):2812–2820. doi:10.1016/j.jaip.2019.05.009
13. Fokkens WJ, Viskens AS, Backer V, et al. EPOS/EUFOREA update on indication and evaluation of biologics in chronic rhinosinusitis with nasal polyps 2023. Rhinology. 2023;61(3):194–202.
14. Tokunaga T, Sakashita M, Haruna T, et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: the JESREC study. Allergy. 2015;70(8):995–1003. doi:10.1111/all.12644
15. Meng Y, Lou H, Wang C, Zhang L. Predictive significance of computed tomography in eosinophilic chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2016;6(8):812–819. doi:10.1002/alr.21749
16. Lund VJ, Kennedy DW. Staging for rhinosinusitis. Otolaryngol Head Neck Surg. 1997;117(3):S35–S40. doi:10.1016/S0194-5998(97)70005-6
17. Akiyama K, Samukawa Y, Hoshikawa H. Is the measurement of ethmoid sinus dominance in eosinophilic chronic rhinosinusitis accurate? Braz J Otorhinolaryngol. 2024;90(5):101463. doi:10.1016/j.bjorl.2024.101463
18. Lee SM, Yoo SH, Mo JH. Comparison of long-term postoperative outcomes of the subtypes of chronic rhinosinusitis with nasal polyps. J Clin Med. 2024;13(6):1699. doi:10.3390/jcm13061699
19. Gevaert P, De Craemer J, Bachert C, et al. European academy of allergy and clinical immunology position paper on endoscopic scoring of nasal polyposis. Allergy. 2023;78(4):912–922. doi:10.1111/all.15650
20. Wu PW, Chang PH, Huang CC, Lee TJ, Fan YH, Huang CC. Impact of comorbid asthma on life quality of patients with chronic rhinosinusitis and nasal polyps. J Asthma Allergy. 2025;18:567–578. doi:10.2147/JAA.S517258
21. Wu PW, Chiu CH, Huang YL, et al. Tissue eosinophilia and computed tomography features in paediatric chronic rhinosinusitis with nasal polyps requiring revision surgery. Rhinology. 2023;61(3):348–357. doi:10.4193/Rhin22.435
22. Wu PW, Huang CC, Chang PH, Lee TJ, Huang CC. The benefit of dupilumab as a postoperative short-term adjuvant therapy for chronic rhinosinusitis with nasal polyps: a preliminary study. Laryngoscope Investig Otolaryngol. 2024;9(4):e1296. doi:10.1002/lio2.1296
23. Wang M, Li Y, Li J, et al. New insights into the endotypes of chronic rhinosinusitis in the biologic era. J Allergy Clin Immunol. 2025;S0091-6749(25):00211.
24. Haruna S, Otori N, Moriyama H, Nakanishi M. Olfactory dysfunction in sinusitis with infiltration of numerous activated eosinophils. Auris Nasus Larynx. 2006;33(1):23–30. doi:10.1016/j.anl.2005.09.005
25. Kim JW, Huh G, Rhee CS, et al. Unsupervised cluster analysis of chronic rhinosinusitis with nasal polyp using routinely available clinical markers and its implication in treatment outcomes. Int Forum Allergy Rhinol. 2019;9(1):79–86. doi:10.1002/alr.22221
26. Tao X, Chen F, Sun Y, et al. Prediction models for postoperative uncontrolled chronic rhinosinusitis in daily practice. Laryngoscope. 2018;128(12):2673–2680. doi:10.1002/lary.27267
27. Szucs E, Ravandi S, Goossens A, Beel M, Clement PA. Eosinophilia in the ethmoid mucosa and its relationship to the severity of inflammation in chronic rhinosinusitis. Am J Rhinol. 2002;16(3):131–134. doi:10.1177/194589240201600301
28. Kubota K, Takeno S, Taruya T, Sasaki A, Ishino T, Hirakawa K. IL-5 and IL-6 are increased in the frontal recess of eosinophilic chronic rhinosinusitis patients. J Otolaryngol Head Neck Surg. 2017;46(1):36. doi:10.1186/s40463-017-0214-2
29. Toppila-Salmi S, Reitsma S, Hox V, et al. Endotyping in chronic rhinosinusitis-an EAACI task force report. Allergy. 2025;80(1):132–147. doi:10.1111/all.16418
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.