Back to Journals » Clinical Ophthalmology » Volume 20
Predictive Factors for Macular Sensitivity and Fixation Stability After Pars Plana Vitrectomy for Rhegmatogenous Retinal Detachment Repair with Primary Pars Plana Vitrectomy: A Microperimetry Study
Authors Al-Mulla AH, Al-Souih AI, Gikandi PW, Al-Kharashi AS, Abu El-Asrar AM
Received 10 November 2025
Accepted for publication 4 February 2026
Published 14 February 2026 Volume 2026:20 580261
DOI https://doi.org/10.2147/OPTH.S580261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Abdullah H Al-Mulla,1 Abdulrahman I Al-Souih,1 Priscilla W Gikandi,1 Abdullah S Al-Kharashi,1 Ahmed M Abu El-Asrar1,2
1Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Arab National Bank Research Chair in Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Ahmed M Abu El-Asrar, Department of Ophthalmology, College of Medicine, King Abdulaziz University Hospital, King Saud University, King Abdulaziz Road, PO Box 245, Riyadh, 11411, Saudi Arabia, Tel +0096611-4786100ext.3370, Email [email protected]
Purpose: To identify predictive factors for macular sensitivity and fixation stability following rhegmatogenous retinal detachment (RRD) repair using MP-1 microperimeter.
Methods: Retrospective study of 66 eyes from 66 patients who underwent successful primary pars plana vitrectomy and had postoperative microperimetry assessment.
Results: Median postoperative macular sensitivity was 12.9 decibels and median fixation stability was 81.5%. Median time between RRD repair and microperimetry testing was 10.0 months. Initial visual acuity ≥ 20/200 was associated with higher postoperative macular sensitivity (p=0.021) and fixation stability (p=0.004). Attached macula at presentation was associated with better macular sensitivity (p=0.041) and fixation stability (p=0.034). Gas tamponade resulted in superior outcomes compared to silicone oil for both macular sensitivity (p=0.004) and fixation stability (p< 0.001). Multivariate regression analysis identified gas tamponade as the most significant predictor for better macular sensitivity (odds ratio = 5.53; 95% confidence interval [2.11– 8.94]; p = 0.002). Significant negative correlations were observed between preoperative logarithm of the minimum angle of resolution (LogMAR) visual acuity and postoperative macular sensitivity (r=− 0.253; p=0.043) and fixation stability (r=− 0.408; p=0.001). Final LogMAR visual acuity was negatively correlated with macular sensitivity (r=− 0.581; p< 0.001) and fixation stability (r=− 0.421; p< 0.001).
Conclusion: Better initial visual acuity, attached macula at presentation, and gas tamponade are significant predictors for better postoperative macular function after RRD repair.
Keywords: rhegmatogenous retinal detachment, outcome, macular sensitivity, fixation stability
Introduction
Rhegmatogenous retinal detachment (RRD) occurs when liquefied vitreous passes through a retinal tear, separating the neurosensory retina from the retinal pigment epithelium (RPE). This condition is an ocular emergency that demands urgent surgical intervention to prevent permanent vision loss.1
Pars plana vitrectomy (PPV) followed by the use of either gas or silicone oil as an internal tamponade has become an increasingly favored technique for managing RRD. It allows for the complete removal of the vitreous gel, relief of vitreoretinal traction, and sealing of retinal breaks—essential steps to achieve successful reattachment, with anatomical success rates exceeding 90%.2–4 However, achieving anatomical success does not always translate into functional success, which remains difficult to predict. While visual acuity is typically the primary postoperative measure to assess visual outcomes, it does not fully capture the extent of functional recovery. Patients may continue to experience visual disturbances such as paracentral scotomas, reduced contrast sensitivity, altered color vision, metamorphopsia, and aniseikonia despite good visual acuity. These persistent functional deficits are thought to arise from underlying retinal microstructural and cellular alterations, including photoreceptor damage, synaptic reorganization, and glial cell remodeling, which may not fully recover despite successful anatomical reattachment.5–7
Microperimetry, also known as fundus-controlled perimetry, is a tool used to assess retinal sensitivity and fixation stability across the macula and has emerged as a valuable method for evaluating functional recovery. By mapping macular sensitivity at various loci and analyzing fixation stability with automated eye tracking, it provides a more detailed assessment of visual function.8 Several studies have utilized microperimetry to assess macular function following RRD repair.5,9–16 Nevertheless, the factors that specifically influence macular sensitivity and fixation stability after RRD repair remain underexplored. The aim of this study was to determine the pre-, intra-, and post-operative factors that predict macular sensitivity and fixation stability after successful RRD repair, using microperimetry as the primary assessment tool.
Patients and Methods
We retrospectively reviewed the medical records of patients who underwent successful RRD repair at King Abdulaziz University Hospital, Riyadh, Saudi Arabia, from November 2008 to December 2023, and had postoperative microperimetry testing. All patients underwent primary PPV, followed by the use of either gas or silicone oil as internal tamponade. For all patients, microperimetry was performed after silicone oil removal or when gas resorption exceeded 60%. Also, postoperative microperimetry assessment was performed only for phakic patients without visually significant cataract, for pseudophakic patients, or for aphakic patients after secondary intraocular lens (IOL) insertion. Patients with postoperative media opacity, preoperative proliferative vitreoretinopathy (PVR) grade B or worse, optic nerve pathology, retinochoroidal pathology involving the macula, prior vitreoretinal surgery, or insufficient follow-up were excluded.
Data collection included patient demographics (age, gender, eye laterality, history of trauma, and presence of amblyopia), preoperative clinical characteristics (duration of symptoms, preoperative Snellen visual acuity, preoperative lens status, extent of detachment, macular status, type of detachment, and characteristics of retinal breaks), surgical details (techniques used, any intraoperative complications, and the type of tamponade agent applied), and postoperative outcomes. Postoperative outcomes included best-corrected Snellen visual acuity (BCVA), intraocular pressure (IOP), slit-lamp examination findings, dilated fundus examination results, optical coherence tomography (OCT) findings, microperimetry results, and the time interval between RRD repair and microperimetry testing.
The study adhered to the ethical principles outlined in the Declaration of Helsinki and was reviewed and approved by the Institutional Review Board of King Saud University (Decision No. 24/1290/IRB). All study subjects provided a written informed consent for the surgical procedure. Permission was also obtained to use the collected data for research. Given the retrospective design of the study and the use of de-identified patient data, the Institutional Review Board waived the requirement for patient consent to review medical records. All patient data were handled confidentially and anonymized prior to analysis.
Operation Details
All surgeries were performed under general anesthesia by a single surgeon (A.M.A). In every case, a 2.5 mm-wide solid silicone encircling band was circumferentially placed pre-equatorially to support the posterior margin of the vitreous base. Pars plana lensectomy was performed in eyes with dense cataracts, while posterior capsulectomies were made using a vitreous cutter in pseudophakic eyes to enhance visualization. All eyes underwent 3-port, 20-gauge pars plana vitrectomy (PPV) to remove the vitreous gel and posterior hyaloid. Perfluorocarbon liquid (PFCL) was injected over the posterior pole to drain subretinal fluid through retinal breaks, ensuring that the PFCL bubble remained posterior to the breaks. The encircling band was adjusted as necessary to achieve adequate buckle height, facilitating thorough vitreous base shaving. Meticulous vitreous removal was performed near the retinal breaks, and horseshoe break flaps were excised to relieve traction. In cases where complete drainage through a posterior break was not feasible, an anterior retinotomy near the ora serrata was performed. Chorioretinal adhesion was induced using indirect ophthalmoscope laser photocoagulation around all retinal breaks and extended 360 degrees in the peripheral retina along the vitreous base. After confirming the absence of iatrogenic breaks, a complete fluid-air exchange was performed. Internal tamponade was achieved by injecting either 25% sulfur hexafluoride (SF6), 14% perfluoropropane (C3F8) gas–air mixtures, or silicone oil into the vitreous cavity.
Microperimetry Technique
Microperimetry assessments were conducted using the MP-1 microperimetry system (Nidek Technologies, Padova, Italy) with version 1.4.2 software. The system provided a 45-degree non-mydriatic fundus image and automatically compensated for eye movements. Patients underwent dark adaptation for five minutes before testing and received a brief orientation at the beginning of each follow-up test. For this study, specific testing criteria were applied: stimuli were arranged in a radial grid pattern across the central 12 degrees, focusing on the fovea. The stimuli, similar in size to Goldmann III, were projected for 200 milliseconds on a white background set to 4 apostilbs. A bright red cross (2–3 degrees in size) served as the fixation target, adjusted to the patient’s BCVA. A 4–2 double staircase strategy was employed, along with automatic eye tracking to account for eye movements. Stimulus intensity ranged from 0 to 20 decibels (dB), and fixation stability was determined by the percentage of fixation points within a 2-degree diameter circle. Figure 1 provides examples of MP-1 microperimetry results, showing numerical and color-coded data from two patients with varying levels of macular sensitivity.
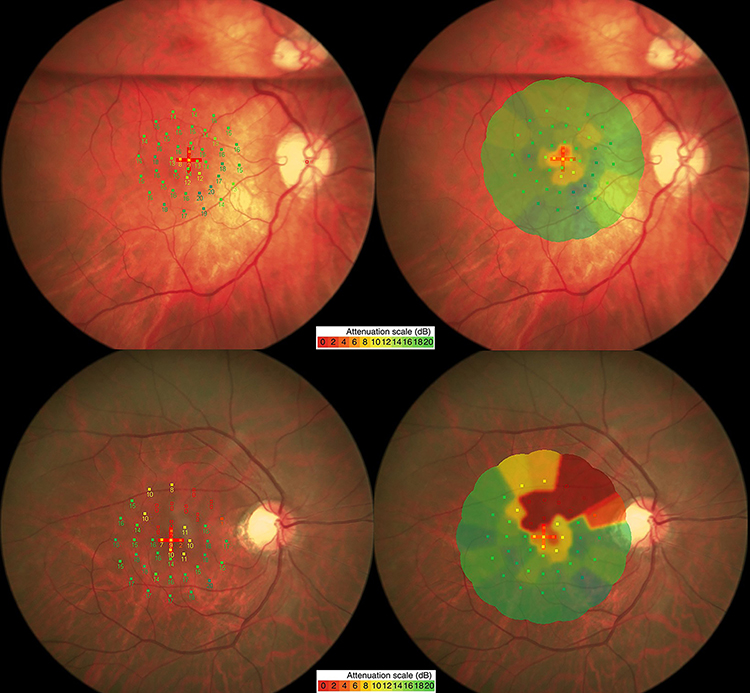 |
Figure 1 MP-1 microperimetry results from two patients included in this study with different levels of macular sensitivity, both with macula-off retinal detachment. The color-coded numeric scale represents retinal sensitivity thresholds in 2 dB steps, ranging from 0 to 20 dB, with green indicating normal sensitivity and red denoting areas of decreased sensitivity. The first patient, shown in the top row, had a preoperative visual acuity (VA) of 20/100 and a final VA of 20/30, with relatively good sensitivity. Numerical microperimetry readings (top left) show a mean retinal sensitivity of 14.7 decibels, with a superior gas bubble visible but not covering the studied area. The color-coded map (top right) shows mostly green to yellow areas, indicating good overall retinal sensitivity. The second patient, shown in the bottom row, had a preoperative VA of counting fingers (CF) and a final VA of 20/60, with lower sensitivity and more significant defects. Numerical microperimetry readings (bottom left) show a mean retinal sensitivity of 11 decibels, with eight retinal loci in the superior macular area having a sensitivity of 0 decibels. The corresponding color-coded map (bottom right) displays red defects in the superior macular area, aligning with the areas of 0 decibels in the numerical data. |
Statistical Methods
Data were collected, stored, and managed in a spreadsheet using Microsoft Excel 2010® software. Data were analyzed and figures were prepared using SPSS® version 21.0 (IBM Inc., Chicago, Illinois, USA). Descriptive statistics were used to summarize the demographic and clinical characteristics of the study population. Categorical variables (eg, gender, macular status, and tamponade type) were presented as frequencies and percentages, while continuous variables (eg, age, visual acuity in logarithm of the minimum angle of resolution [LogMAR], and macular sensitivity) were summarized as medians and interquartile ranges (IQR) due to their non-normal distribution. Mann–Whitney U-tests were performed to explore associations between predictive factors and postoperative macular sensitivity and fixation stability. Multivariate regression analysis was performed to identify independent predictors of macular sensitivity recovery, adjusting for covariates with p value less than 0.2 from the univariate analysis and these were: age, gender, initial visual acuity, macular involvement, and tamponade type. Spearman correlation coefficient was used to evaluate the relationships between preoperative visual acuity, final BCVA, mean macular sensitivity, and fixation stability. A p value of less than 0.05 was considered statistically significant for all analyses.
Results
A total of 66 eyes from 66 patients were included in the study. The median age of the cohort was 51.0 years (IQR 32.3–57.0), with 47 (71.2%) being male. The right eye (OD) was involved in 38 (57.6%) cases, and the left eye (OS) in 28 (42.4%) cases. Six (9.1%) patients had a history of trauma, and one (1.5%) patient had a history of amblyopia. The median duration of symptoms prior to surgical intervention was 7 days (IQR 4.0–30.0).
Regarding preoperative lens status, 42 (63.6%) patients were phakic, 19 (28.8%) were pseudophakic, and 5 (7.8%) were aphakic. Retinal detachments involved two quadrants in 40 (60.6%) patients, three quadrants in 10 (15.2%) patients, and all four quadrants in 9 (13.6%) patients. Macular involvement was observed in 49 (74.2%) patients. Posterior vitreous detachment (PVD)-related retinal breaks were present in 51 (77.3%) patients, while 15 (22.7%) patients had chronic RRD caused by atrophic holes with attached posterior hyaloid. The retinal breaks were smaller than one clock hour in 54 (81.8%) eyes. The number of retinal breaks per patient was observed as follows: 34 (51.5%) patients had 1 break, 13 (19.7%) patients had 2 breaks, 7 (10.6%) patients had 3 breaks, and 12 (18.2%) patients had more than 3 breaks.
For internal tamponade, 42 (63.6%) patients received C3F8 gas, 13 (19.7%) received SF6 gas, and 11 (16.7%) received silicone oil. The indications for using silicone oil in these 11 cases were as follows: giant retinal tear (GRT) (n=3), multiple retinal breaks in different quadrants (n=4), hypotony with coexisting choroidal detachment (n=1), chronic detachment with subluxated IOL (n=1), Marfan’s syndrome with dislocated crystalline lens (n=1), and a pregnant patient with difficult positioning (n=1). Among these patients, the timing of silicone oil removal varied, with a median duration of 6 months (IQR 4.0–10.0).
At the final follow-up, the median mean macular sensitivity was 12.9 dB (IQR 8.1–16.1), and the median fixation stability was 81.5% (IQR 59.0–90.3). The median time between RRD repair and microperimetry testing was 10.0 months (IQR 2.0–25.5).
Factors Predicting Macular Sensitivity and Fixation Stability
Several factors were evaluated for their potential influence on postoperative macular sensitivity and fixation stability (Table 1). Initial visual acuity showed a significant relationship with both outcomes. Patients with better initial visual acuity (≥20/200) had significantly higher median macular sensitivity (13.3 dB, IQR 10.1–15.4) compared to those with worse visual acuity (<20/200), whose median sensitivity was 10.8 dB (IQR 2.8–13.6, p=0.021). Similarly, fixation stability was better in patients with higher initial visual acuity (median 88%, IQR 73–93) compared to those with worse visual acuity (median 69%, IQR 46–84, p=0.004).
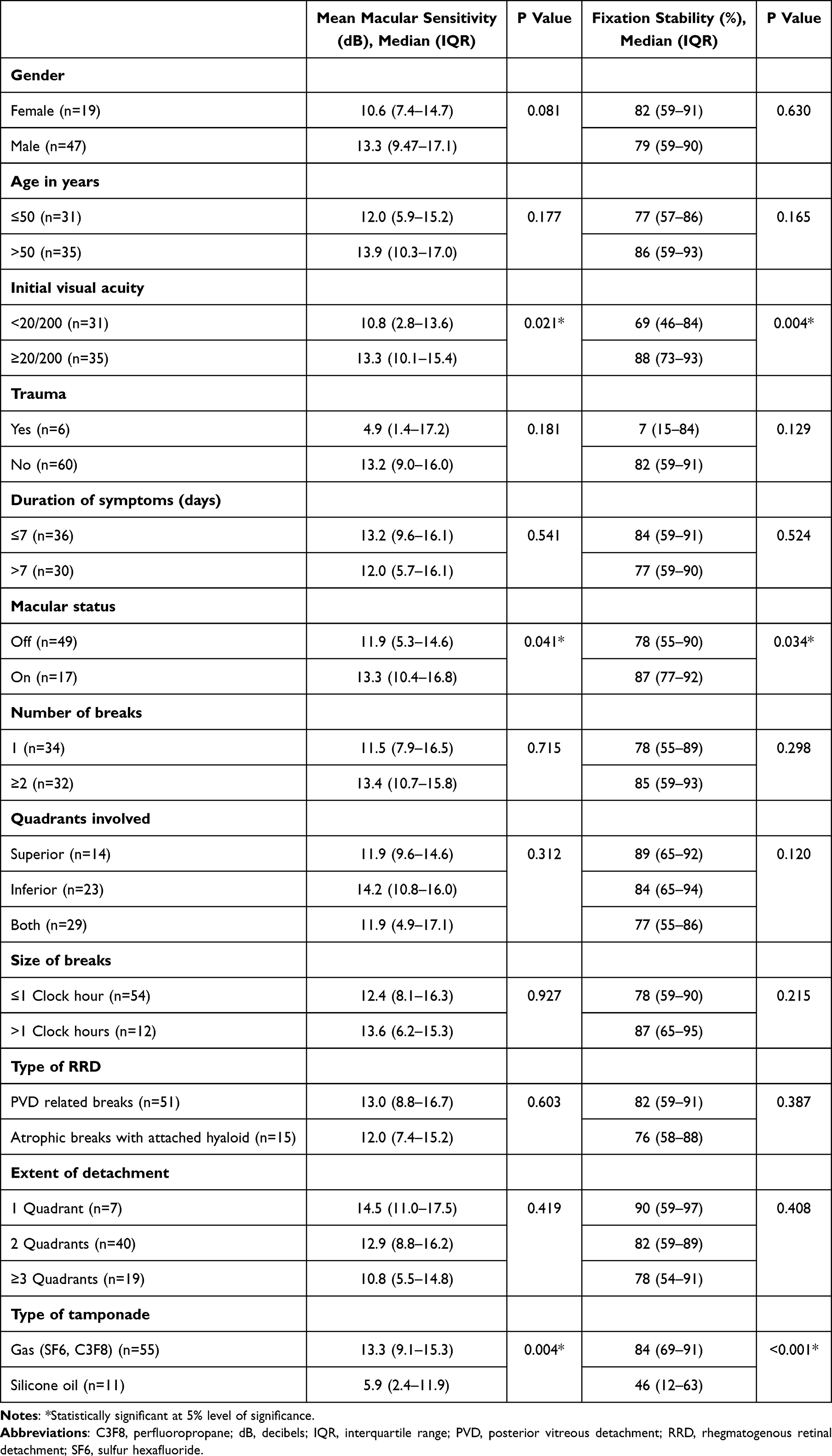 |
Table 1 Factors Influencing Mean Macular Sensitivity and Fixation Stability |
Macular status also had a statistically significant impact on postoperative outcomes. Patients with macula-on RRD had significantly higher macular sensitivity (median 13.3 dB, IQR 10.4–16.8) compared to those with macula-off (median 11.9 dB, IQR 5.3–14.6, p=0.041). Fixation stability followed a similar trend, with patients with macula-on showing better stability (median 87%, IQR 77–92) compared to those with macula-off (median 78%, IQR 55–90, p=0.034).
The type of tamponade used during surgery was another significant factor. Patients who received gas tamponade (SF6 or C3F8) had significantly higher macular sensitivity (median 13.3 dB, IQR 9.1–15.3) compared to those who received silicone oil (median 5.9 dB, IQR 2.4–11.9, p=0.004). Fixation stability was also significantly better in the gas group (median 84%, IQR 69–91) compared to the silicone oil group (median 46%, IQR 12–63, p<0.001).
Multivariate logistic regression analysis was performed to identify the independent predictors of postoperative macular sensitivity (Table 2). The type of tamponade was found to be the only independent predictor for postoperative macular sensitivity. Gas tamponade was associated with a higher likelihood of better macular sensitivity compared to silicone oil (odds ratio [OR] = 5.53, 95% confidence interval [CI] [2.11–8.94], p = 0.002). Initial visual acuity of ≥ 20/200 showed a trend toward better outcomes (OR = 2.35; 95% CI [−0.48–5.18]; p = 0.102), though it did not reach statistical significance (Table 2).
 |
Table 2 Multivariate Analysis to Identify Predictors for Macular Sensitivity |
Correlations Between Preoperative Visual Acuity, Final Visual Acuity, and Microperimetry Findings
There were significant negative correlations between preoperative visual acuity (logMAR) and mean macular sensitivity (r=−0.253, p=0.043) as well as fixation stability (r=−0.408, p=0.001) (Figure 2). Similarly, significant negative correlations were observed between final BCVA (logMAR) and both mean macular sensitivity (r=−0.581, p<0.001) and fixation stability (r=−0.421, p<0.001) (Figure 3).
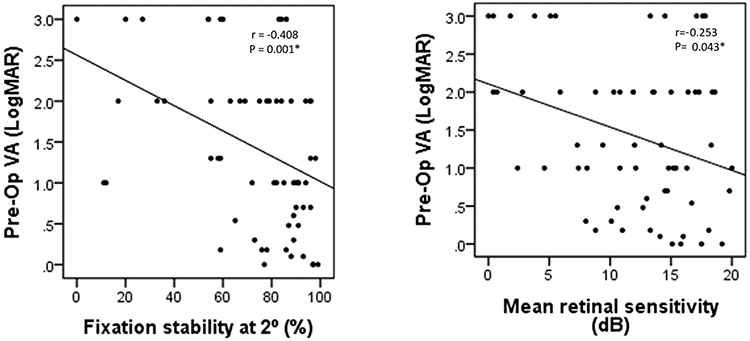 |
Figure 2 Scatterplots showing the relationships between preoperative visual acuity (Pre-op VA), measured on the logarithm of the minimum angle of resolution (LogMAR) scale, and two postoperative functional outcomes. The left plot illustrates the association with mean macular sensitivity (measured in decibels), while the right plot highlights the association with fixation stability (measured as the percentage of fixation points within a 2-degree diameter circle). Both scatterplots reveal that better preoperative visual acuity corresponds to higher macular sensitivity and improved fixation stability. *Statistically significant at 5% level of significance. |
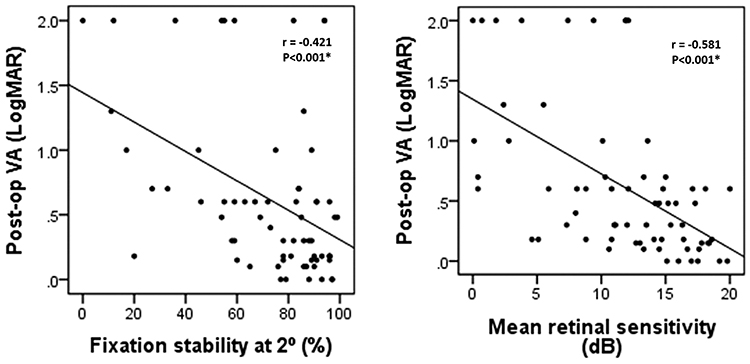 |
Figure 3 Scatterplots illustrating the relationships between postoperative visual acuity (Post-op VA), measured on the logarithm of the minimum angle of resolution (LogMAR) scale, and two postoperative functional outcomes. The left plot represents the association with mean macular sensitivity (in decibels), while the right plot illustrates the association with fixation stability (measured as the percentage of fixation points within a 2-degree diameter circle). Both scatterplots demonstrate that better postoperative visual acuity is associated with higher macular sensitivity and improved fixation stability. *Statistically significant at 5% level of significance. |
Visual Acuity Improvement
A total of 43 (65.2%) eyes experienced an improvement in visual acuity following RRD repair. Visual acuity remained the same in 16 (24.2%) eyes, while it deteriorated in 7 (10.6%) eyes. There was a statistically significant improvement in visual acuity from baseline to the final follow-up, with a median reduction in logMAR BCVA from 1.3 (IQR 0.6–2.3) (Snellen equivalent, 20/400) preoperatively to 0.48 (IQR 0.17–0.70) (Snellen equivalent, 20/60) postoperatively (p<0.001).
Discussion
This study aimed to identify factors predicting macular function following successful RRD repair with primary pars plana vitrectomy, using fundus microperimetry as the primary assessment tool. Our analysis identified three significant predictors for improved postoperative macular function, including initial visual acuity of ≥ 20/200, attached macula at presentation, and the use of gas as a tamponade rather than silicone oil.
The univariate analysis showed that better initial visual acuity is a significant predictor of better postoperative macular function, including macular sensitivity and fixation stability. This finding aligns with previous studies, which have identified initial visual acuity as a main predictive factor of visual outcomes following RRD repair.17–20 This correlation may be attributed to the fact that better initial visual acuity is often observed in cases of RRD with a lesser extent of detachment or with macular sparing. Moreover, this is supported by our analysis, as cases with macula-on RRD were significantly associated with better postoperative macular function.
Regarding type of internal tamponade, univariate analysis revealed that gas tamponade was found to be a significant predictor for better postoperative macular sensitivity and fixation stability compared to silicone oil. On multivariate logistic regression analysis, gas tamponade was identified to be an independent predictor for better outcomes. Scheerlinck et al16 reported similar findings in their study of 40 eyes divided into gas and silicone oil groups for macula-on and macula-off cases. Using microperimetry, they showed superior foveal sensitivity in eyes treated with gas tamponade, regardless of macular status. However, their tamponade selection was not randomized, and silicone oil was more frequently used in complex detachments, including cases with advanced PVR (grade C). This may explain the poorer functional outcomes in their silicone oil group. In our study, eyes with PVR grade B or worse were excluded; however, selection bias may still exist since silicone oil was used in more complex cases. In our view, randomizing tamponade selection is challenging and often impractical, as the decision is largely based on the surgeon’s intraoperative judgment, assessing the estimated risk of redetachment, future PVR formation, or the need for longer tamponade. This variability may introduce some bias toward a worse outcome observed in the silicone oil group. Nevertheless, our findings of lower macular sensitivity in the silicone oil group are supported by other studies. Dou et al14 found improvements in retinal sensitivity and fixation stability after silicone oil removal in eyes with macula-off RRD. Their findings suggested that the duration of silicone oil tamponade and the interval between retinal detachment and surgery were important predictors. They found that prolonged tamponade is associated with impairment of macular function. Additionally, other studies demonstrated silicone oil-related visual loss. It was proposed that visual loss related to silicone oil might result from multiple factors, such as mechanical effects on the retina, subclinical retinal toxicity, and phototoxicity during oil removal.21–24 Collectively, these findings suggest that silicone oil tamponade is associated with a worse macular function.
A key strength of this study is the use of microperimetry as an assessment tool, offering a detailed analysis of macular function. Additionally, to the best of our knowledge, this is the first study to focus on multiple predictive factors for two key macular functions following RRD repair—macular sensitivity and fixation stability—providing a comprehensive approach to understanding the factors influencing postoperative macular recovery. However, the study has several limitations. Its retrospective nature limits control over potential confounding factors, and the small sample size may reduce the statistical power to detect significant associations and might affect the multivariate regression results. Additionally, microperimetry assessments were not conducted at fixed intervals postoperatively due to the retrospective nature of the study, which may introduce variability in the timing of functional outcomes. Also, as previously mentioned, there may be selection bias between the use of gas and silicone oil tamponades, with silicone oil more frequently used in complex detachments, which may have influenced the outcomes.
Conclusion
In conclusion, initial visual acuity, macular status, and tamponade type are significant predictors for postoperative macular function following RRD repair using primary PPV. Gas tamponade appears to offer advantages over silicone oil in enhancing functional recovery. However, selection bias may exist as silicone oil was used in more complex cases. Future prospective studies with larger cohorts and standardized assessment protocols are needed to validate these findings and further explore the role of microperimetry in long-term functional assessment after RRD repair.
Data Sharing Statement
De-identified data are available from the corresponding author (Ahmed M Abu El-Asrar) upon reasonable request.
Ethics Statement
The study adhered to the ethical principles outlined in the Declaration of Helsinki and was reviewed and approved by the Institutional Review Board of King Saud University (Decision No. 24/1290/IRB). All study subjects provided a written informed consent for the surgical procedure. Permission was also obtained to use the collected data for research. Given the retrospective design of the study and the use of de-identified patient data, the Institutional Review Board waived the requirement for patient consent to review medical records. All patient data were handled confidentially and anonymized prior to analysis.
Acknowledgments
The authors thank Ms. Crisalis Longanilla-Bautista for secretarial assistance.
Funding
This work was supported by King Saud University through the Vice Deanship of Research Chair, National Arab Bank Research Chair in Ophthalmology (Abu El-Asrar AM).
Disclosure
Abdullah H Al-Mulla is currently affiliated with Department of Ophthalmology, Ministry of Health, Al-Ahsa, Saudi Arabia. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Ghazi NG, Green WR. Pathology and pathogenesis of retinal detachment. Eye. 2002;16(4):411–10. doi:10.1038/sj.eye.6700197
2. Schwartz SG. Pars plana vitrectomy for primary rhegmatogenous retinal detachment. Clin Ophthalmol. 2008;2(1):57–63. doi:10.2147/OPTH.S1511
3. Hillier RJ, Felfeli T, Berger AR, et al. The pneumatic retinopexy versus vitrectomy for the management of primary rhegmatogenous retinal detachment outcomes randomized trial (PIVOT). Ophthalmology. 2019;126(4):531–539. doi:10.1016/j.ophtha.2018.11.014
4. Abu El-Asrar AM, Al-Kwikbi HF, Kangave D. Prognostic factors after primary vitrectomy and perfluorocarbon liquids for bullous rhegmatogenous retinal detachment. Eur J Ophthalmol. 2009;19(1):107–117. doi:10.1177/112067210901900116
5. Huvard MJ, Patnaik JL, Kleinman DM, et al. An evaluation of the repeatability of visual function following surgical repair of macula-off rhegmatogenous retinal detachment. Transl Vis Sci Technol. 2023;12(11):35. doi:10.1167/tvst.12.11.35
6. Van de Put MA, Croonen D, Nolte IM, et al. Postoperative recovery of visual function after macula-off rhegmatogenous retinal detachment. PLoS One. 2014;9(6).
7. Lina G, Xuemin Q, Qinmei W, Lijun S. Vision-related quality of life, metamorphopsia, and stereopsis after successful surgery for rhegmatogenous retinal detachment. Eye. 2016;30(1):40–45. doi:10.1038/eye.2015.171
8. Pfau M, Jolly JK, Wu Z, et al. Fundus-controlled perimetry (microperimetry): application as outcome measure in clinical trials. Prog Retin Eye Res. 2021;82:100907. doi:10.1016/j.preteyeres.2020.100907
9. Reumueller A, Wassermann L, Salas M, et al. Morphologic and functional assessment of photoreceptors after macula-off retinal detachment with adaptive-optics OCT and microperimetry. Am J Ophthalmol. 2020;214:72–85. doi:10.1016/j.ajo.2019.12.015
10. Díaz-Barreda MD, Bartolomé-Sesé I, Boned-Murillo A, et al. Microperimetry-assessed functional alterations and OCT-changes in patients after retinal detachment surgery using pars plana vitrectomy and SF6 tamponade. Diagnostics. 2021;11(7):1157. doi:10.3390/diagnostics11071157
11. Ng HJ, Vermeer KA, La Heij EC, et al. Retinal damage extends beyond the border of the detached retina in fovea-on retinal detachment. Acta Ophthalmol. 2024;102(3):285–295. doi:10.1111/aos.15713
12. Noda H, Kimura S, Hosokawa MM, et al. Effect of rhegmatogenous retinal detachment on preoperative and postoperative retinal sensitivities. Sci Rep. 2020;10(1):21497. doi:10.1038/s41598-020-78693-5
13. Baba T, Mizuno S, Tatsumi T, et al. Outer retinal thickness and retinal sensitivity in macula-off rhegmatogenous retinal detachment after successful reattachment. Eur J Ophthalmol. 2012;22(6):1032–1038. doi:10.5301/ejo.5000148
14. Dou R, Li R, Li R-C, et al. Evaluation of retinal structural and functional changes after silicone oil removal in patients with rhegmatogenous retinal detachment: a retrospective study. Int J Retina Vitreous. 2024;10(1):1. doi:10.1186/s40942-023-00519-z
15. Delolme MP, Dugas B, Nicot F, et al. Anatomical and functional macular changes after rhegmatogenous retinal detachment with macula off. Am J Ophthalmol. 2012;153(1):128–136. doi:10.1016/j.ajo.2011.06.010
16. Scheerlinck LM, Schellekens PA, Liem AT, et al. Retinal sensitivity following intraocular silicone oil and gas tamponade for rhegmatogenous retinal detachment. Acta Ophthalmol. 2018;96(6):641–647. doi:10.1111/aos.13685
17. Zaletel Benda P, Vratanar B, Petrovski G, et al. Prognostic factor analysis of visual outcome after vitrectomy for rhegmatogenous retinal detachment. J Clin Med. 2020;9(10):3251. doi:10.3390/jcm9103251
18. Suzuki N, Kunikata H, Aizawa N, et al. Predicting visual outcomes for macula-off rhegmatogenous retinal detachment with optical coherence tomography. J Ophthalmol. 2014;2014:269837. doi:10.1155/2014/269837
19. Yazici B, Gelişken O, Avci R, et al. Prediction of visual outcome after retinal detachment surgery using the Lotmar visometer. Br J Ophthalmol. 2002;86(3):278–281. doi:10.1136/bjo.86.3.278
20. Cai LZ, Lin J, Starr MR, et al. PRO score: predictive scoring system for visual outcomes after rhegmatogenous retinal detachment repair. Br J Ophthalmol. 2023;107(4):555–559. doi:10.1136/bjophthalmol-2021-320440
21. Scheerlinck LM, Schellekens PA, Liem AT, et al. Incidence, risk factors and clinical characteristics of unexplained visual loss after intraocular silicone oil for macula-on retinal detachment. Retina. 2016;36(2):342–350. doi:10.1097/IAE.0000000000000711
22. Christensen UC, la Cour M. Visual loss after use of intraocular silicone oil associated with thinning of inner retinal layers. Acta Ophthalmol. 2012;90(8):733–737. doi:10.1111/j.1755-3768.2011.02248.x
23. Lee J, Cho H, Kang M, et al. Retinal changes before and after silicone oil removal in eyes with rhegmatogenous retinal detachment using swept-source optical coherence tomography. J Clin Med. 2021;10(22):5436. doi:10.3390/jcm10225436
24. Dogramaci M, Williams K, Lee E, et al. Foveal light exposure is increased at the time of removal of silicone oil with the potential for phototoxicity. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):35–39. doi:10.1007/s00417-012-2033-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.