Back to Journals » Open Access Emergency Medicine » Volume 14
Predicting Suitable Percutaneous Endovascular Arterial Embolization for Traumatic Abdominopelvic Injuries: A Retrospective Cohort Study
Authors Al-Sharydah AM ![]()
Received 16 June 2022
Accepted for publication 31 August 2022
Published 1 October 2022 Volume 2022:14 Pages 545—556
DOI https://doi.org/10.2147/OAEM.S376819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Abdulaziz Mohammad Al-Sharydah
Diagnostic and Interventional Radiology Department, Imam Abdulrahman Bin Faisal University, College of Medicine, King Fahd Hospital of the University, Al-Khobar City, Eastern Province, Saudi Arabia
Correspondence: Abdulaziz Mohammad Al-Sharydah, Diagnostic and Interventional Radiology Department, Imam Abdulrahman Bin Faisal University, College of Medicine, King Fahd Hospital of the University, PO Box: 31952, Al-Khobar City, Eastern Province, 4398, Saudi Arabia, Fax +966 013 8676697, Email [email protected]
Purpose: This study evaluated the pre-procedural attributes of trauma patients to determine their suitability to undergo Percutaneous Endovascular Arterial Embolization (PEAE), and the current state of endovascular repair as an option for trauma-related injuries in traumatic abdominopelvic arterial injuries was explored.
Patients and Methods: We retrospectively evaluated the charts of 638 adults with traumatic abdominopelvic injuries treated from March 2011 to February 2021, extensively reviewing their pre-operative indices, pre-operative optimization requirements, and multi-modality imaging records.
Results: In total, 235 patients (30.63%) were “hemodynamically unstable” on admission, mainly due to hypotension (n=437 [68.5%]). Additionally, laboratory-defined acquired coagulopathies and inherited bleeding disorders were found in 268 patients (42.01%). The computerized tomography bleeding protocol was performed on 408 (63.94%) patients. Percutaneous endovascular therapy by arterial embolization was performed on 146 patients. The mean number of requested pre-intervention blood units for trauma patients significantly exceeded the number of units transfused post-intervention (P< 0.0005). Apart from hemodynamics (ie heart rate, mean blood pressure); hemoglobin, and lactic acid levels were independently associated indices of PEAE outcomes (p < 0.01).
Conclusion: Despite the recommendations from the Society of Interventional Radiology on endovascular intervention for trauma and bleeding risk, 36.84% of study patients had hemodynamic instability and other unfeasible parameters that would limit the option of minimally invasive procedures. Early recognition and consideration of suitable treatment options is essential for optimizing patient outcomes. It is imperative that standardized algorithms and management protocols based on available resources be developed.
Keywords: interventional radiology, injury, embolization, surgery, emergency medicine
Plain Language Summary
Diagnostic and interventional radiology play a major role in the diagnoses and management of patients who have sustained abdominopelvic trauma. Motor vehicle collisions are a significant cause of morbidity and mortality worldwide. This study assessed the pre-operative characteristics of patients associated with suitability for percutaneous endovascular embolization as an option to manage bleeding. Also, this study identified the underlying barriers to using this minimally invasive option in emergency trauma victims. These findings will aid physicians dealing with trauma patients in their triage planning and strategic implementation of best processes at point-of-care.
Introduction
Trauma is a leading cause of mortality and morbidity worldwide.1 In 2004, deaths from motor vehicle collisions (MVCs) were ranked second globally after deaths from ischemic heart diseases.1,2 According to the World Health Organization, in 2018, there were 28.8 fatalities from MVCs per 100,000 population in Saudi Arabia, which exceeded the fatality rates in the United States of America, United Kingdom, and Australia.3 Continuous assessment and triaging of injuries according to the severity of the damage and the extent of vital organ involvement enables proper medical care.4 Furthermore, a multidisciplinary trauma team can efficiently manage trauma patients by implementing a standardized workflow algorithm.5
Diagnostic and interventional radiology (IR) play a major role in the diagnosis, management, and follow-up of patients injured in MVCs.6 Since their revolutionary introduction in the 1970s, percutaneous endovascular techniques have contributed to important developments in medical equipment, damage-control strategies, and procedures,7 and IR has become an integral part of the medical care provided by the trauma team.8 The Society of Interventional Radiology (SIR) recommends that Percutaneous Endovascular Arterial Embolization (PEAE) in trauma patients requires the availability of an IR-ready team in the hospital within 60 minutes of the decision to proceed with angiography or transfer of the patient to another center where timely PEAE can be performed.9,10 Nonetheless, performing PEAE in the traumatized unstable patients is more challenging than comparable elective situations with stable patients.9
This study was conducted with a primary aim of bridging the gap in the literature with regard to determining the predictors of effective PEAE as a minimally invasive management option for arterial repair in patients who have sustained traumatic abdominopelvic injuries, based on their pre-intervention characteristics. Second, it aimed to formulate a graphical pre-operative algorithm based on pre-operative indices from our academic unicentral data, to improve patient selection at point of care when PEAE is clinically indicated. Also, it reflects the implementation of recommended evidence from SIR Consensus Guidelines for the periprocedural management of thrombotic and bleeding risk in patients undergoing image-guided procedures,11 to minimize risk and maximize benefit.
Materials and Methods
Setting
The study was conducted at King Fahd Hospital of the University (KFHU), a tertiary-care, 650-bed, university teaching hospital located in the Eastern Province of Saudi Arabia. This academic hospital is accredited by the Joint Commission International and The Saudi Central Board for Accreditation of Healthcare Institutions. According to its 2018 annual report, the hospital received approximately 270,000 annual outpatient (21,767 outpatients department and 247,331 emergency room [ER]) visits. The radiology department has been operational since 1981, and the IR division, comprising four modern angiography suites operated by seven trained interventional radiologists, was established in 2010. In 2017, approximately 800 patients benefited from the IR unit, compared to 700 patients in 2016.
Study Design and Study Population
This STROBE-compliant retrospective chart review study included trauma patients treated between March 2011 and February 2021, identified from the Electronic Medical Record System, and confirmed based on a review of pre-operative indices, pre-operative optimization requirements, and multi-modality imaging records. The sample size was determined (1 – β= 0.80) using G*Power version 3.1.9.7. software (RRID:SCR_013726, available at: http://www.gpower.hhu.de/) to ensure sufficient statistical power.
Data Collection and Inclusion and Exclusion Criteria
“Trauma victims” were defined as adult patients (> 14-years-old) with traumatic abdominopelvic injuries quantified using the Injury Severity Score (ISS).12
Data were retrospectively obtained through multistage collection using the keyword “trauma” in the International Classification of Diseases 10th Edition (ICD-10) coding system, as well as the codes S30–S39, for injuries to the abdomen and pelvis, to identify relevant patient charts from the electronic medical record archival system at KFHU. We excluded pediatric patients <14 years old (94 patients) and patients with missing demographics, laboratory results, or multi-modality imaging data (58 patients).
The hospital radiology department database was then reviewed using the picture archiving and communication system to screen the data collected from March 2011 to February 2021, including pertinent radiography, sonography, digital subtracted angiography, and computerized tomography (CT) imaging studies. The absence of missing data or duplication was audited and confirmed. The list obtained was used to identify cases that met the inclusion criteria of this study (Figure 1).
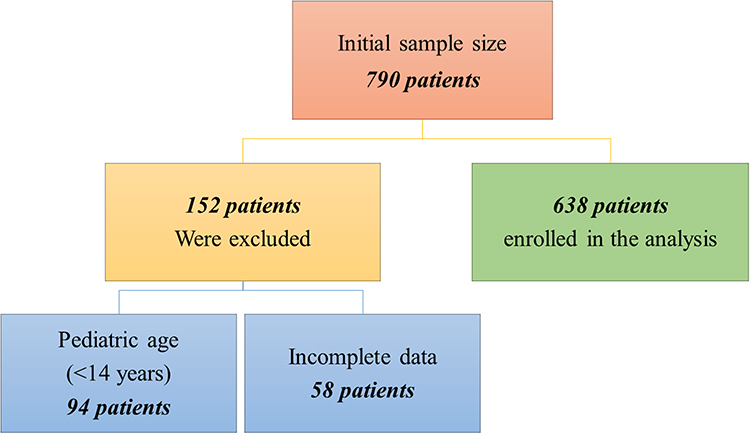 |
Figure 1 Flowchart of patient selection showing inclusion and exclusion criteria and final sample size. |
An extensive chart review of each case was performed using both digital and paper-based data to collect the study-related variables over an 8-month period. Patients were divided into three groups according to management options: those treated non-operatively (ie conservative management); those treated in angio suites (ie PEAE); and those treated with open laparotomy (ie in the surgical theater).
Hemodynamic “(in) stability” was defined based on available objective criteria (blood pressure, cardiac output, rate of vasopressor, or inotrope).13 Trauma-Induced Coagulopathy (TIC) is a known reason for coagulation derangement defined as imbalance between clotting, fibrinolysis, and anti-coagulation.14
Statistical Analysis
Statistical analyses were conducted using R v 3.6.3 Counts (R Core Team, Vienna, Austria) and Minitab version 17.0 (Minitab, LLC, 2021. Minitab, available at: https://www.minitab.com). Categorical and continuous variables are expressed as percentages and mean ± standard deviation (SD), respectively. Unpaired t-test and an independent analysis of variance (ANOVA) tests were used to compare continuous and categorial variables, respectively. Hypothesis were investigated at a significance level of 5%. Non-parametric data were analyzed using the Kruskal–Wallis test. Univariate logistic regression analysis was used to independently examine multiple variables checked by interventionalists pre-operatively. Non-significant predictive variables of poor outcome were excluded from the multivariate analysis. Significant variables were entered into multivariate binary forward stepwise logistic regression models to identify the most parsimonious model of independent preoperative predictors of poor outcomes. The final model was the basis for the suggested algorithm.
Ethical Approval
This study was performed in accordance with the Helsinki Declaration of 1975 (revised in 1983). The Imam Abdulrahman Bin Faisal University Institutional Review Board considered the descriptive and retrospective nature of this study and granted approval for the study to be conducted at KFHU (IRB-2022-01-183). Anonymized data were collected, analyzed, and reported only in aggregate form, and no identifiable participant information was revealed in the study.
Results
Demographics
After applying the inclusion (n=790) and exclusion (n=152) criteria, the charts of 638 patients were selected for review and analysis (Figure 1). Among these 638 participants (age, mean ± SD [range] = 28 ± 10 [14–57] years), 504 (78.9%) were Saudis, 302 (59.92%) were men, and 202 (40.08%) were women.
Injury Type
Participants were categorized as MVC victims (n=505, [79.74%]) or non-MVC victims (n=133, [20.26%]). Iatrogenic injuries (91/133 [68,42%]) represented the majority of non-MVC patients, followed by stab wounds (61/133, [45,86%]). Liver injuries were the most frequent acute solid-organ injury (n=139 [21.78%]), and hemoperitoneum (n=244 [38.25%]) was the most commonly associated finding (Figure 2).
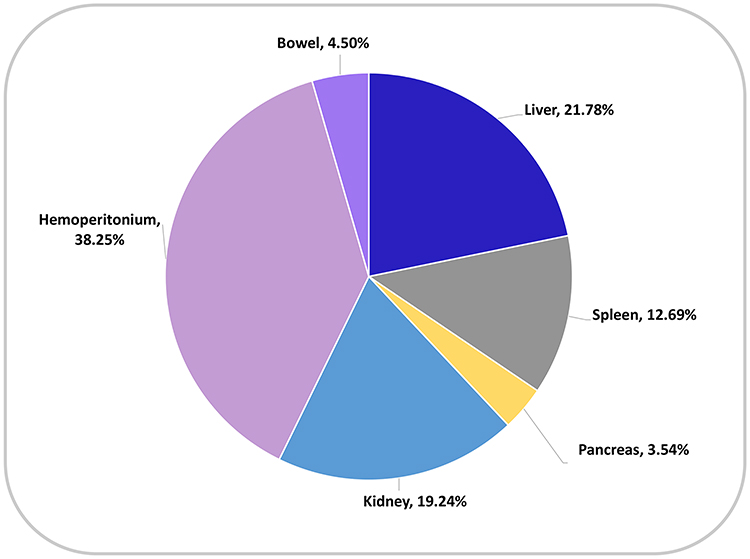 |
Figure 2 Prevalence of abdominopelvic injuries of enrolled trauma patients, according to organ. |
Circulation Stability
In this cohort, 235 (36.84%) participants were “hemodynamically unstable” on arrival at ER. Hypotension (n=437 [68.5%]) was the most common vital sign in patients with altered stability.
Laboratory results
Less than half of the patients (n=268 [42.01%]) had acquired coagulopathies or inherited bleeding disorders (Table 1). Despite TIC, anticoagulant uptake was found in 109 patients (17.08%) and sepsis in 43 (6.74%) (P=0.21); other cardiac hepatic disorders contributed to coagulopathic status. Baseline hemoglobin and reticulocyte levels were obtained for all patients.
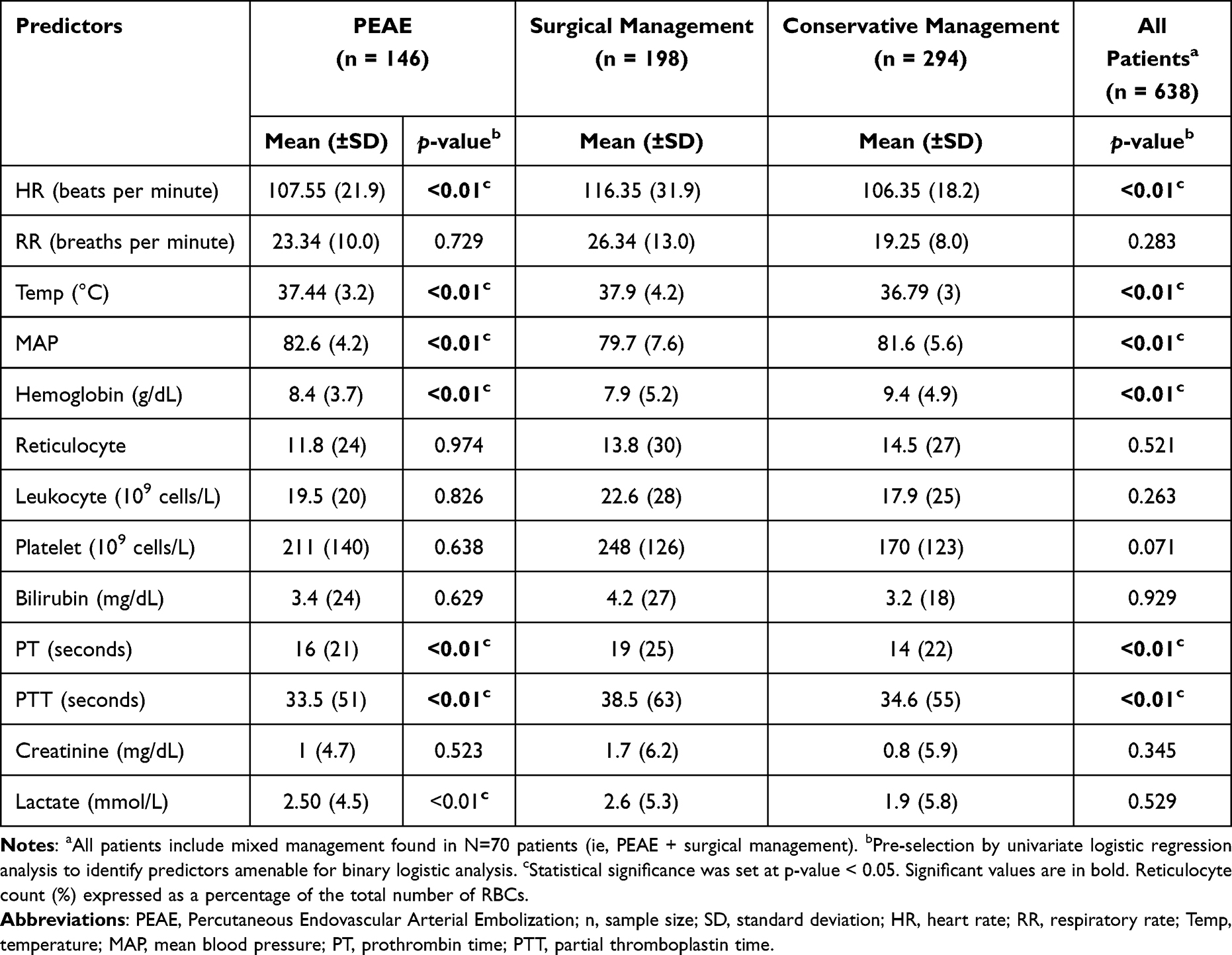 |
Table 1 Laboratory Characteristics of Patients According to Treatment Option |
Independent Pre-Operative PEAE Indices
Heart rate, mean blood pressure, hemoglobin level, and lactic acid level were significant for independent pre-operative indices (p <0.01) (Table 2).
 |
Table 2 Multivariate Logistic Regression for Independent Predictors Associated with Better Survival and Favorable Outcomes for Percutaneous Endovascular Arterial Embolization (n=146) |
Fluid Resuscitation and Allergy Testing
Crystalloid intravenous fluids (normal saline or Ringer’s lactate) were administered for initial volume correction in patients (n=530 [83.07%]; P=<0.005, one-sided t-test). Aggregated data on packed red blood cell transfusions, fresh-frozen plasma, and platelets concentrate were collected (n=189 [29.62%]; P=0.1, one-sided t-test). Paired t-test comparisons showed significantly higher mean pre-intervention with PEAE than post-intervention packed blood products transfusions (4.1 units vs 0.5 units; P<0.0005). Allergic status and related premedication were sub optimally investigated prior to performing PEAE (n=71/146 [48.63%]).
Diagnostic Imaging
The majority of plain radiographs (n=601 [94.20%]) and CT scans (n=408 [63.94%], [89% with intravenous contrast]) were interpreted by a certified radiologists (n=765 [96.8%]). The initial Focused Assessment with Sonography for Trauma (FAST) scans (n=570 [89.34%]) were performed and interpreted by non-radiologists (ie certified emergency physicians) (Figure 3). Tc-99m red blood cell (RBC) scans were not performed at our institution. CT was the most advantageous diagnostic modality for identifying hemorrhage (P=<0.005, one-way ANOVA) and was superior to sonography and fluoroscopy (Figure 4).
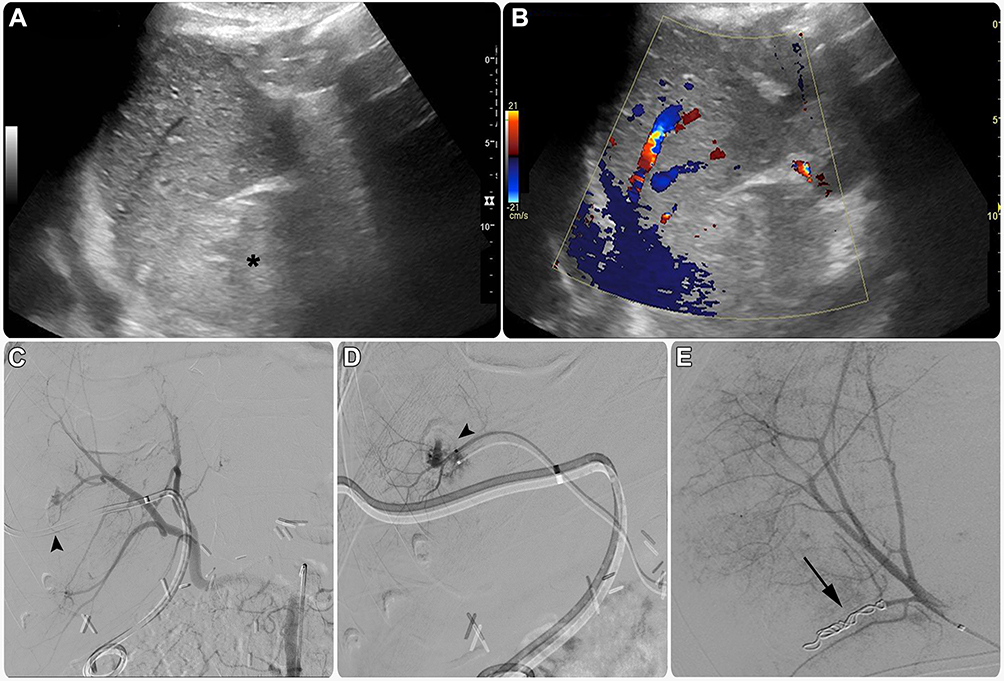 |
Figure 3 Thirty-year-old man underwent emergency surgery to treat Klatskin liver tumor (cholangiocarcinoma), complicated by iatrogenic injury to surrounding vessels. Notes: His hemoglobin level decreased gradually over time, and clinical suspicion of internal bleeding increased. (A) Greyscale and (B) color Doppler ultrasound of the right upper quadrant of abdomen depicted a hematoma at the surgical bed (asterisk). Abdominal computerized tomography scan revealed active intra-hepatic hemorrhage with potential pseudoaneurysm (not shown). (C) Conventional angiography using a selective catheter in the celiac trunk confirmed that there was an active extravasation in the liver (arrowhead). (D) A super-selective microcatheter contrast analysis further characterized the origin of bleeding from a segment (VIl) (arrowhead). (E) Selective embolization was performed with the help of thrombogenic coils (arrow), with an immediate resolution of active extravasation in the final contrast run. |
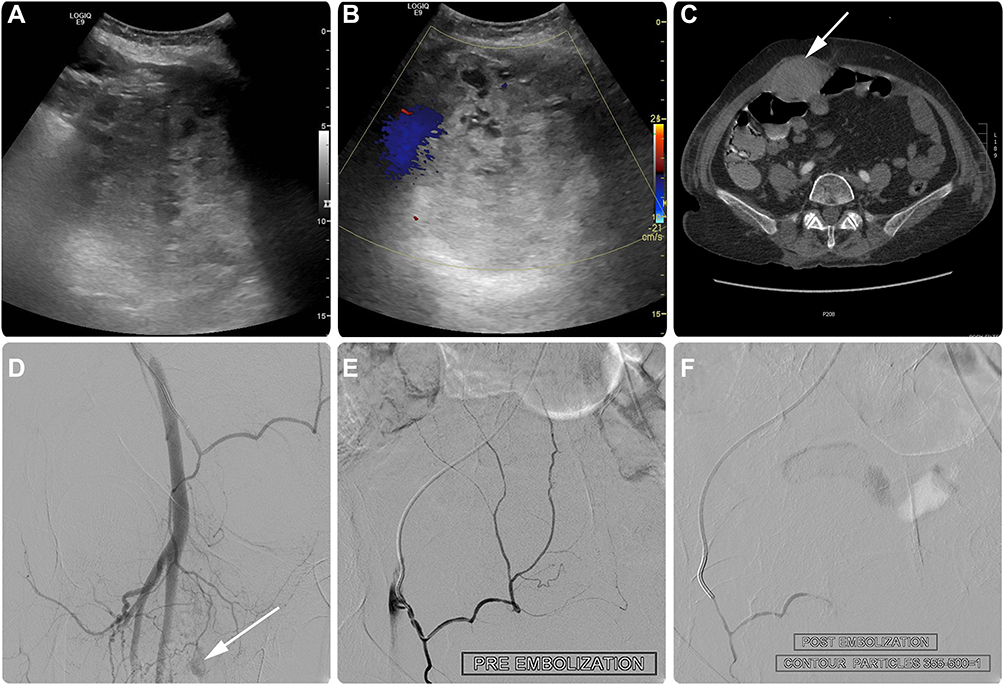 |
Figure 4 Sixty-five-year-old female victim of motor vehicle collision with anterior abdomen query mass. Notes: (A) Greyscale and (B) color Doppler ultrasound of the right lower quadrant of abdomen suspected a hematoma. (C) Enhanced CT confirmed a rapidly growing anterior abdominal wall hematoma (arrow). Despite initial resuscitation with two rescuing red blood cell units, hemoglobin level dropped to 6 g/dL. Conventional selective iliac angiography did not show any visible extravasation (not shown). (D and E) Multi-projection super selection contrast runs of the right inferior epigastric artery, using microwire and microcatheter combination, show hypertrophied right inferior epigastric artery with abnormal venous blush (arrow). “Empirical embolization” was performed using a 0.5 mL (300–500 microns) particulate vial. (F) Post-embolization angiogram revealed complete resolution of hemorrhage. |
Outcomes
No intra-procedural mortality occurred in the interventional suites; however, post-PEAE 90 day mortality was 6.16%. The mean length of hospital stay (LOS), post-PEAE, was 11 days. There were no significant differences among treatment option groups for hospital and intensive care unit LOS or 90 day mortality (Table 3) (Figure 5).
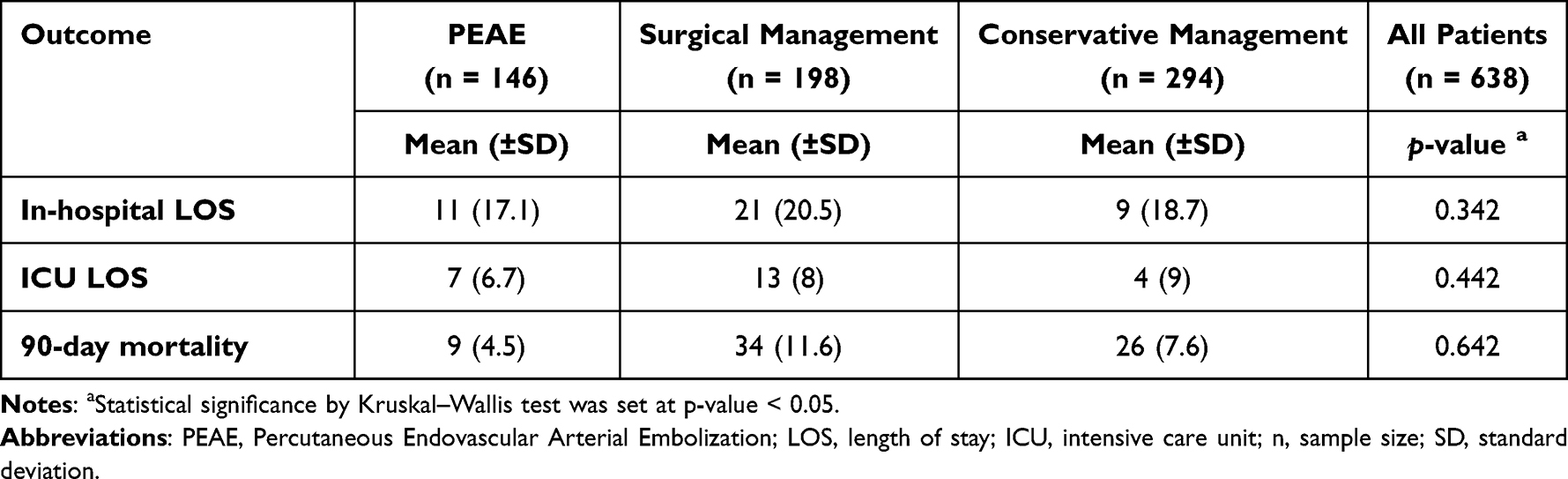 |
Table 3 Patient Outcomes and Survival According to Different Treatment Options |
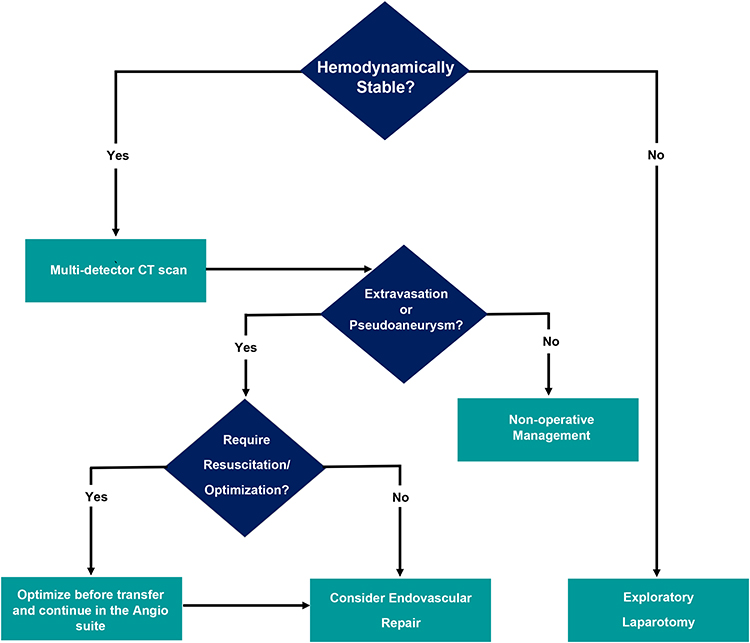 |
Figure 5 Suggested algorithm based on our unicentral data analysis derived from the updated society of interventional radiology guidelines,9,11 which aids pre-operative selection of traumatic abdominopelvic patients amenable for percutaneous endovascular arterial embolization to maximize the likelihood of a favorable outcome. |
Discussion
Worldwide, trauma is a leading cause of millions of deaths per year. This study was conducted at a university center in Saudi Arabia, which experiences a high trauma-related patient population. Globally, MVCs ranked 23rd in mortality rates, and among Saudi nationals, young adults (25% younger than 15 years; 3% older than 65 years) are the most affected group in trauma-related events.15 Similar to the findings of this study, Alharbi et al reported that MVCs were the most prevalent trauma type in Saudi Arabia, and iatrogenic injuries, followed by stab wounds, were the main causes of non-MVC trauma.15
In trauma settings, PEAE therapy constitutes either the sole definitive management or a preoperative adjunct,16 whereby injured vessels can be accessed remotely through the zones of anatomic transition, thus avoiding further injuries/exacerbations secondary to open surgeries.4 Emergent laparotomies are indicated in hemodynamically unstable patients or those who respond transiently to initial resuscitation.4 In this study, a considerable proportion of patients were hemodynamically unstable, with hypotension as the main underlying cause, hemostasis to optimize the vital signs of these patients should be prioritized before PEAE.9,11,13
Selecting endovascular therapy or surgery for trauma management depends upon initial presentation, availability of facilities, hemodynamic status, trauma grade, response to initial therapy, imaging findings, and the interventional radiologists or surgeon’s judgment.4 Currently, feasible PEAE are prioritized over surgery due to lower morbidity and mortality risks and the risk of large blood volume loss and uncontrolled vessel bleeding in surgery (Table 3).4,16
This study presents a thematic algorithm derived from analysis of our aggregated institutional data and the SIR recommendations9,11 to assess trauma patients for their pre-intervention suitability to ensure better survival and favorable procedural outcomes (Figure 5).
In acute trauma, PEAE is a common IR procedure4 for intentional temporary or permanent vascular occlusion using variable embolic materials (eg metallic coils, microvascular plugs, liquid embolic materials, or particles) or by stenting to achieve hemostasis.9 The choice of embolic agent varies based on the target bleeding organ/vessel.4 It is imperative while performing PEAE to prevent the embolic material from traveling to non-target organ tissue, thereby avoiding organ dysfunction due to non-targeted embolization.4,16 Embolization should be done as close as possible to the site of vascular injury (Figures 3 and 4),16 because too proximal embolization may lead to re-bleeding, whereas a distal embolization may cause an infarct.15 Additionally, balloon occlusion may be used in trauma cases for rapid control of exsanguinating hemorrhage where the priority is saving lives.16
Imaging has an important role in the early identification of life-threatening injuries,17 and is critical for patient triaging for operative vs non-operative management. Imaging is recommended before PEAE for localization of injury sites and delineation of arterial anatomy.4 Our results showed that the majority of traumatized victims were imaged with FAST (89.34%) and/or enhanced CT scan (63.94%) at their presentation, which reflects an adequate implementation of the updated SIR9,11 and the American Association for the Surgery of Trauma–World Society of Emergency Surgery18 recommendations on the suitable pre-intervention imaging for traumatized patients.
In the last two years at our center, we have started obtaining Tc-99m RBC scans for trauma victims for limited indications. Tc-99m RBC scans can result in incorrect bleeding localization, which may mislead the subsequent angiographic intervention. Contrast-enhanced CT is preferred as a realistic predictor of positive arteriograms and active hemorrhage. It is superior to Tc-99m RBC scanning for localization of bleeding; and specifically identifies the bleeding pathology, thus facilitating better triage and prognosis prediction of PEAE.19 CT is one of the most effective diagnostic tools for evaluating trauma,17 with a sensitivity of 98% in identifying contrast extravasation and a negative predictive value of 99.6% in diagnosing these injuries.16,20
Another major parameter to determine pre-intervention suitability for traumatized patients is their coagulation profile at presentation.11 Laboratory-defined acquired coagulopathies and inherited bleeding disorders were found in approximately 42% of the study population, which may hinder their suitability for PEAE as a management option (Table 1). Although TIC is a known reason for coagulation derangement,14 anticoagulant medications, sepsis, and cardiac hepatic disorders were other contributors in this study population. It is worth mentioning that target-specific oral anticoagulants which directly inhibit coagulation factor Xa (such as rivaroxaban, edoxaban, apixaban, betrixaban, and darexaban) or thrombin (dabigatran) have been found to be suitable and at least as effective as Vitamin K antagonists with regard to efficacy, but with a lower risk of bleeding.11,21 While oral anticoagulant correction should be based on algorithmic practice, plasma transfusion is the preferred option by anesthesiologists to reverse oral anticoagulants in emergencies compared to commercial prothrombin complex concentrates.22
Pre-selection univariable logistic regression analysis models with a criterion of one explanatory variable at a time revealed that heart rate, temperature, mean blood pressure, hemoglobin level, coagulation indices, and lactic acid level met the selection criterion for multivariable analysis (Table 1). Multivariate analyses, undertaken to account for associated confounders, found that only heart rate, mean blood pressure, hemoglobin level, and lactic acid level were significantly associated with PEAE outcomes based on patient characteristics (p <0.01).
The results of this study are consistent with growing evidence of the predictive ability of serial lactic acid measurement as an independent predictor of poor outcomes in critically ill and traumatized patients. Multiple observational studies, systematic reviews, and meta-analyses in severely ill patients have found hyperlactatemia to be a poor predictor of post-procedural mortality.23–25 This study’s findings add support to the prognostic role of lactic acid in abdominopelvic trauma patients in assessing their suitability for PEAE.
A limited number of papers have considered the effectiveness of PEAE versus other management options in patients with abdominal traumas. A recent retrospective observational study with only 12 patients found imaging confirmed lesions of the internal breast artery (IMA). PEAE was evaluated for efficacy in these patients and a 100% technical success rate was reported. Only 17% of patients were hemodynamically stable, while the remainder required a blood transfusion. We concluded that PEAE is an effective, safe, and efficient management option in comparison to open surgery, avoiding general anesthesia and allowing immediate recovery of the patient. Other studies were recommended with a larger sample of patients to validate their method. This study fills this gap by considerably expanding the sample size and is not restricted to just one vessel.26
It is important to use PEAE appropriately. First, immediate 24-hour access to an interventional angiography suite is necessary. In hospitals without angiography suites, management protocols should involve the postponement of elective procedures if trauma interventions are necessary or transfer the patient to another facility where timely intervention can be performed.9 Second, despite monitored PEAE, anesthetic support should be considered.9 Third, interventional radiologists should be ready to intervene within 60 minutes when a decision to proceed with angiography is made.9 Fourth, assuring the administration of blood products and performing rapid infusions is crucial for active resuscitation.9 Last, PEAE is based on the precise detection of the hemorrhage using contrast-enhanced CT angiography.27
This distinguished study adds to the scanty evidence on pre-procedural characteristics and the suitability of abdominopelvic trauma patients to endure PEAE with favorable outcomes. However, the present study was limited by the retrospective nature of an observational study and possible observer bias due to data derived from medical charts. Descriptive analysis was selected for its usefulness in estimating the morbidity burden with respect to the overall outcomes. Second, intraoperative technical factors were not considered as independent factors because the aim of the study was to determine the influence of preoperative patient characteristics and appropriateness of outcomes, and there was limited availability of intraoperative data in the archival system. Third, despite the gaps that this study bridges in the related literature, only domestic data were used, and the generalizability of the findings is uncertain. Therefore, international studies are required. Finally, the univariate and multivariate logistic regression analysis were performed primarily using a conventional method because the main objective was to identify potentially predictive associations, rather than to test a hypothesis. In addition, we considered the scientific plausibility and clinical meaningfulness of the associated variables.
Conclusion
Despite the recommendations by SIR, 36.84% of trauma patients with imaging detection of hemorrhages suffer from hemodynamic instability at their presentation, and other parameters such as coagulopathy, that would limit the appropriateness of minimally invasive procedures. Apart from hemodynamic stability, blood indices such as hemoglobin and lactic acid levels were independent predictors associated with PEAE outcome. PEAE should only be considered when technically feasible and clinically suitable to improve outcomes. Early recognition and consideration of the most suitable treatment option are essential for optimizing patient outcomes.
Abbreviations
ANOVA, analysis of variance; CT, computerized tomography; ER, emergency room; FAST, Focused Assessment with Sonography for Trauma; ICD-10, International Classification of Diseases 10th Edition; IR, interventional radiology; ISS, Injury Severity Score; KFHU, King Fahad Hospital of the University; LOS, length of hospital stay; MVCs, motor vehicle accidents; PEAE, Percutaneous Endovascular Arterial Embolization; RBC, red blood cell; SIR, Society of Interventional Radiology; SD, standard deviation; TIC, Trauma-Induced Coagulopathy.
Data Sharing Statement
The principal investigator is responsible for sharing the study-related data publicly upon reasonable request from the publishing journal.
Consent to Participate
Given the purely descriptive and observational nature of the study, and in compliance with the Helsinki declaration, informed consent was waived. No identifiable information (image, face, name etc.) of participant is revealed in the submission. Data were collected in anonymously, and analyzed and reported only in aggregate form. In addition, ethical approval was waived by the local Institutional Review Board of Imam Abdulrahman Bin Faisal University (IRB-2022-01-183).
Acknowledgments
The author thanks the Vascular and Interventional Radiology Unit of the Radiology Department at King Fahd Hospital of the University-Imam Abdulrahman Bin Faisal University; Khobar City, Eastern Province, Saudi Arabia.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, and not-for-profit sectors.
Disclosure
The author declares that there are no competing interests.
References
1. Peden M, Scurfield R, Sleet D, et al. World report on road traffic injury prevention. Geneva: World Health Organization; 2004. Available from: http://www.who.int/violence_injury_prevention/publications/road_traffic/world_report/en/.
2. Alghnam S, Alkelya M, Al-Bedah K, Al-Enazi S. Burden of traumatic injuries in Saudi Arabia: lessons from a major trauma registry in Riyadh, Saudi Arabia. Ann Saudi Med. 2014;34:291–296. doi:10.5144/0256-4947.2014.291
3. World Health Organization. Global status report on road safety 2018: summary. Geneva: World Health Organization; 2018. Available from: https://www.who.int/publications/i/item/9789241565684.
4. Jeph S, Ahmed S, Bhatt RD, Nadal LL, Bhanushali A. Novel use of interventional radiology in trauma. J Emerg Crit Care Med. 2017;1:40. doi:10.21037/jeccm.2017.10.04
5. Mahnken AH, Althoff P, Frink M, Viniol S. Interventionelles management peripherer Gefäßverletzungen [Interventional management of peripheral vascular injuries: from the exclusion indication to the procedure of first choice]. Der Unfallchirurg. 2021;124:635–641. German. doi:10.1007/s00113-021-01029-z
6. McCabe S, Maddineni S, Marini C, et al. Vascular and interventional radiology in blunt abdominopelvic trauma-institutional practice and review of the literature. J Trauma Treat. 2016;5:324. doi:10.4172/2167-1222.1000324
7. Stahel PF, Smith WR, Moore EE. Current trends in resuscitation strategy for the multiply injured patient. Injury. 2009;4054:527–535.
8. Gilyard S, Shinn K, Nezami N, et al. Contemporary management of hepatic trauma: what IRs need to know. Semin Intervent Radiol. 2020;37:35–43. doi:10.1055/s-0039-3401838
9. Padia SA, Ingraham CR, Moriarty JM, et al. Society of interventional radiology position statement on endovascular intervention for trauma. J Vasc Interv Radiol. 2020;31:363–369.e2. doi:10.1016/j.jvir.2019.11.012
10. Lopera JE. Embolization in trauma: principles and techniques. Semin Intervent Radiol. 2010;27:14–28. doi:10.1055/s-0030-1247885
11. Patel IJ, Rahim S, Davidson JC, et al. Society of interventional radiology consensus guidelines for the periprocedural management of thrombotic and bleeding risk in patients undergoing percutaneous image-guided interventions—part II: recommendations: endorsed by the Canadian association for interventional radiology and the cardiovascular and interventional radiological society of Europe. J Vasc Interv Radiol. 2019;30(8):1168–1184. doi:10.1016/j.jvir.2019.04.017
12. Vallmuur K, Cameron CM, Watson A, Warren J. Comparing the accuracy of ICD-based severity estimates to trauma registry-based injury severity estimates for predicting mortality outcomes. Injury. 1732–1739;52:32–36. doi:10.1176/ajp.133.1.32
13. Vincent JL, Cecconi M, Saugel B. Is this patient really “(un)stable”? How to describe cardiovascular dynamics in critically ill patients. Crit Care. 2019;23:272. doi:10.1186/s13054-019-2551-1
14. Chang R, Cardenas JC, Wade CE, Holcomb JB. Advances in the understanding of trauma-induced coagulopathy. Blood. 2016;128(8):1043–1049. doi:10.1182/blood-2016-01-636423
15. Alharbi RJ, Lewis V, Mosley I, Miller C. Current trauma care system in Saudi Arabia: a scoping literature review. Accid Anal Prev. 2020;144:105653. doi:10.1016/j.aap.2020.105653
16. Singh A, Kumar A, Kumar P, Kumar S, Gamanagatti S. “Beyond saving lives”: current perspectives of interventional radiology in trauma. World J Radiol. 2017;9:155–177. doi:10.4329/wjr.v9.i4.155
17. Otsuka H, Sato T, Sakurai K, et al. Impact of emergency physicians competent in severe trauma management, surgical techniques, and interventional radiology on trauma management. Acute Med Surg. 2018;5:342–349. doi:10.1002/ams2.359
18. Kobayashi L, Coimbra R, Goes AM
19. Feuerstein JD, Ketwaroo G, Tewani SK, et al. Localizing acute lower gastrointestinal hemorrhage: CT angiography versus tagged RBC scintigraphy. AJR Am J Roentgenol. 2016;207:578–584. doi:10.2214/AJR.15.15714
20. Pillai AS, Srinivas S, Kumar G, Pillai AK. Where does interventional radiology fit in with trauma management algorithm? Semin Interven Radiol. 2021;38:3–8. doi:10.1055/s-0041-1725114
21. Chai-Adisaksopha C, Crowther M, Isayama T, Lim W. The impact of bleeding complications in patients receiving target-specific oral anticoagulants: a systematic review and meta-analysis. J Am Soc Hematol. 2014;124(15):2450–2458.
22. Levy JH, Connors JM, Steiner ME, Douketis J, Spyropoulos AC. Management of oral anticoagulants prior to emergency surgery or with major bleeding: a survey of perioperative practices in North America: communication from the scientific and standardization committees on perioperative and critical care haemostasis and thrombosis of the international society on thrombosis and haemostasis. J Thromb Haemost. 2020;4(4):562–568.
23. Haas SA, Lange T, Saugel B, et al. Severe hyperlactatemia, lactate clearance and mortality in unselected critically ill patients. Intensive Care Med. 2016;42(2):202–210. doi:10.1007/s00134-015-4127-0
24. Zindovic I, Luts C, Bjursten H, et al. Perioperative hyperlactemia is a poor predictor of outcome in patients undergoing surgery for acute type-A aortic dissection. J Cardiothorac Vasc Anesth. 2018;32(6):2479–2484. doi:10.1053/j.jvca.2018.03.030
25. Gemelli M, Di Tommaso E, Chivasso P, et al. Blood lactate predicts mortality after surgical repair of type A acute aortic dissection. J Card Surg. 2022;37(5):1206–1211. doi:10.1111/jocs.16324
26. Corvino F, Giurazza F, Cangiano G, et al. Safety and effectiveness of transcatheter embolization in the treatment of internal mammary artery injuries. Radiol Med. 2018;123(5):369–377. doi:10.1007/s11547-017-0844-5
27. Kinoshita T, Yamakawa K, Matsuda H, et al. The survival benefit of a novel trauma workflow that includes immediate whole-body computed tomography, surgery, and interventional radiology, all in one trauma resuscitation room: a retrospective historical control study. Ann Surg. 2019;269:370–376. doi:10.1097/SLA.0000000000002527
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.