Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Predicting functional remission in patients with schizophrenia: a cross-sectional study of symptomatic remission, psychosocial remission, functioning, and clinical outcome
Authors Valencia M, Fresán A ![]() , Barak Y, Juárez F, Escamilla R, Saracco R
, Barak Y, Juárez F, Escamilla R, Saracco R ![]()
Received 25 April 2015
Accepted for publication 19 June 2015
Published 10 September 2015 Volume 2015:11 Pages 2339—2348
DOI https://doi.org/10.2147/NDT.S87335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Marcelo Valencia,1 Ana Fresán,2 Yoram Barak,3 Francisco Juárez,1 Raul Escamilla,4 Ricardo Saracco4
1Division of Epidemiological and Psychosocial Research, 2Division of Clinical Research, National Institute of Psychiatry Ramón de la Fuente, Mexico City, Mexico; 3Psychiatry Department, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel; 4Schizophrenia Clinic, National Institute of Psychiatry Ramón de la Fuente, Mexico City, Mexico
Background: New approaches to assess outcome in schizophrenia include multidimensional measures such as remission, cognition, psychosocial functioning, and quality of life. Clinical and psychosocial measures have been recently introduced to assess functional outcome.
Objective: The study presented here was designed to examine the rates of symptomatic remission, psychosocial remission, global functioning, and clinical global impressions in a sample of schizophrenia outpatients in order to assess functional remission and to identify predictive factors for functional remission.
Methods: A total of 168 consecutive Mexican outpatients receiving pharmacological treatment at the National Institute of Psychiatry in Mexico City were enrolled in a cross-sectional study. Symptomatic remission was assessed according to the definition and criteria proposed by the Remission in Schizophrenia Working Group using the Positive and Negative Symptom Scale. Psychosocial remission was assessed according to Barak criteria using the Psychosocial Remission in Schizophrenia scale. Functioning was measured with the Global Assessment of Functioning, and clinical outcome with the Clinical Global Impressions (CGI) Scale.
Results: Findings showed that 45.2% of patients fulfilled the symptomatic remission criteria, 32.1% achieved psychosocial remission, and 53% reported adequate functioning. However, the combination of these three outcome criteria – symptomatic, psychosocial remission, and functioning – indicated that 14.9% of the patients achieved our predefined functional remission outcome. The logistic regression model included five predictive variables for functional remission: (1) being employed, (2) use of atypical antipsychotics, (3) lower number of medications, (4) lower negative symptom severity, and (5) lower excitement symptom severity.
Conclusion: The study demonstrated that symptomatic remission, psychosocial remission, and functioning could be achievable goals for a considerable number of patients. The outcome of functional remission was achieved by a minority of patients, less than 15%. New approaches should include multidimensional measures to assess functional outcome in schizophrenia research.
Keywords: Predictors, functional remission, symptomatic remission, psychosocial functioning, clinical outcome, Mexico
Introduction
The model of functional recovery surpasses the traditional medical model of symptomatic remission1 to include the realization of meaningful roles in the community. Thus, “real-life” community functioning is an increasingly important treatment target for schizophrenia. Unfortunately, full functional recovery is rarely attained and even less frequently maintained, even after symptoms have remitted.2 Profound impairments remain obstacles for patients suffering from schizophrenia even after clinical stabilization in the domains of occupational and academic achievement, interpersonal relationships, and independent living.3
Psychotic symptoms and impairments in everyday living are two major concerns in persons suffering from schizophrenia. The integration of pharmacological and psychosocial interventions have made it possible to redefine outcome measures integrating clinical and psychosocial parameters, indicating that therapeutic efforts should be oriented toward achieving symptomatic remission and improving psychosocial functioning.4,5 Thus, the debate on relevant outcomes in the treatment of patients suffering from schizophrenia now focuses on remission, recovery, functional remission, functional outcome, functionality, functional disability, functional impairment, or functional recovery.6–12 At present, there is no consensus on methods and definitions for assessing other outcome domains such as functional status.13 In addition, the emphasis on domains in recent years such as cognition and quality of life14,15 includes using multidimensional measures to assess different areas of functional outcome.16,17
The concept of remission in schizophrenia, as proposed by the Remission in Schizophrenia Working Group (RSWG),1 has been widely accepted and utilized in scientific research since 2005.18 According to this approach, remission of schizophrenia is defined as:
A state in which patients have experienced an improvement in symptoms to the extent that any remaining symptoms are of such low intensity that they no longer interfere significantly with behavior and are below the threshold typically utilized in justifying a diagnosis of schizophrenia.1
It has been demonstrated that remission can be an achievable goal for a considerable number of patients.19,20 Research studies reported that remission rates vary within the ranges of 37%–59%,21 20%–60%,22 17%–88%,13 and 17%–78%.13,21–23 However, the remission criteria used by the research studies13,21–23 did not include factors such as social or vocational functioning which can be considered key domains in functional remission.24 The remission rate variations could be explained because of differences in study design, sample characteristics, and the criteria employed to measure remission.25 Functional outcome domains should go beyond symptomatic improvement.26 For the study reported here, the criteria of the RSWG was utilized to assess symptomatic remission.
Psychosocial remission is a new concept that has been recently introduced2,27 and recommended for measuring impairments.28 Impairments seem to be a core feature of schizophrenia. Psychosocial impairments are expressed in daily living skills (eg, personal hygiene, interest in daily life, family relations), and in various occupational, social, and community settings. These impairments might contribute to disability.29 The Psychosocial Remission in Schizophrenia (PSRS) scale27 utilized in the present study was developed to assess psychosocial impairments. The PSRS scale was designed as an instrument to complement the RSWG criteria,1 since symptomatic and psychosocial remission are considered different domains that do not overlap and might lead to recovery.28 The PSRS scale has been recommended for measuring psychosocial remission.28,30 To date, only one research report, carried out in Israel, has indicated that schizophrenia patients in the community achieved psychosocial remission (31%) or symptomatic remission (37%)2 according to the RSWG criteria.1 A recent study in Hong Kong analyzed psychosocial correlates associated with recovery in an attempt to classify patients with disabilities and test predictors of recovery stages in schizophrenia patients who were in remission. The study was unable to predict combined stages 1 (“overwhelmed by disability”) and 2 (“struggling with disability”). For Stage 3 (“living with disability”), classification accuracy was 75.45% and for Stage 4 (“living beyond disability”), classification accuracy was 75.50%. Logistic regression demonstrated that stages of recovery could be distinguished with reasonable accuracy.31
Functioning is another important contributor to functional remission since it is related to personal, social, and occupational role functioning.32 However, the assessment of functioning is a complicated issue, since there is no consensus on evaluating functioning in schizophrenia and it is unclear what constitutes “appropriate functioning”.33,34
The inability of individuals to meet societal defined roles such as homemaker, worker, student, spouse, family member or friend. In addition, individual’s satisfaction with their ability to meet these roles, are often subsumed under the rubric of social functioning.35
Persons suffering from schizophrenia frequently have significant difficulties in everyday community functioning. It has been estimated that as many as two-thirds of schizophrenia patients are unable to accomplish psychosocial roles, even when psychotic symptoms are in remission.36 Functioning and symptomatic remission can be considered two relevant outcome measures leading to functional remission. It has been considered that there is a consensus that at least remission and the ability to function in the real world should be considered as components of functional remission.37 The bases of definitions of functional remission should include functional outcomes such as psychosocial functioning.20 The Global Assessment of Functioning (GAF) Scale was utilized to measure functioning in the present study. Achieving symptomatic remission and adequate levels of psychosocial functioning might allow patients to function independently in the community. Research indicates that functional remission can be achieved in 10%–68% of people with schizophrenia.10,38–40 Differences have been found in patients who achieved symptomatic versus functional remission: 45% versus 10%,41 49% versus 17%,42 50% versus 20%,43 and 33% versus 21%,44 respectively.
Clinical outcome is another concern because of the relevance of measuring the severity of the illness. Therefore, a patient’s clinical global impression is necessary, whereby the clinician makes a judgment about the total picture of the patient that includes: the illness severity, the patient’s level of distress, and other components of impairment, as well as the impact of the illness on functioning. To assess the diversity of symptoms present in schizophrenia, illness severity was evaluated with the Clinical Global Impressions (CGI) Scale.45 The CGI Scale asks the clinician the following question: “Considering your clinical experience with this particular population, how mentally ill is the patient at this time?”, with the clinician’s response a rating on a seven-point scale ranging from “normal” to “extremely ill”.
Another important consideration refers to research conducted on remission in schizophrenia in different cultural settings. It was found in a study on the Island of Mauritius that 64% of the patients were in complete remission and were independent.46 Achievement of remission according to the RSWG criteria has been reported as 32% in Italy,47 33% in Taiwan,48 27% in Bali,25 87% in India,49 and 31% in Russia.50 Course and outcome appear to be more favorable in developing countries.51 Cultural issues are important, especially as we wanted to compare findings in other cultural settings with the results of the present study.
Several studies have been conducted to identify predictors of remission, and these can be summarized as follows: early treatment response;52 remission status;53 2 weeks of significant response to treatment;54 a 20% symptom reduction at 2 weeks of treatment;55 younger age, shorter duration of illness, shorter length of current episode, being employed, lower Positive and Negative Syndrome Scale (PANSS) general psychopathology and negative scales scores at baseline, and less suicidality;43 educational status, subjective well-being, low score on the PANSS general psychopathology subscale, and side-effects;56 early symptomatic and subjective well-being improvement57 improvement at 2 weeks of 30% in the PANSS total score;58 shorter duration of untreated psychosis (DUP);44,59,60 better premorbid adjustment;59 better functional level at baseline;10,61 lower psychopathology or illness severity at baseline;47,59,62 early symptomatic, functional, or quality of life improvement;33 younger age, lower illness severity at baseline, better functioning level at baseline and early functional remission, early symptomatic, quality of life and medication adherence;33 best premorbid social functioning, duration of psychotic symptoms before to study entry, diagnosis, percentage of time taking antipsychotic medication, global cognition score, and sex.63 Predictors of remission can be considered relevant for the overall outcome of schizophrenia. This assumption is supported by all previous studies that suggest simultaneous assessment of various domains of functional outcome, as the ones measured in the present study.
There is still a search for indicators to assess functional remission and there is yet no consensus on established measures. The current approach is to use multiple domains to assess functional outcome in schizophrenia research.30,64 To assess functional remission in the study reported here, functional remission was defined as a combination of clinical components such as symptomatic remission and illness severity and psychosocial domains such as psychosocial remission and functioning.
The research objectives addressed by this paper are: (a) to examine the rates of symptomatic remission, psychosocial remission, global functioning, and clinical global impression in a sample of schizophrenia outpatients; (b) to assess functional remission as the result of patients fulfilling the symptomatic, psychosocial remission and functioning criteria; (c) to identify predictive factors for functional remission; and (d) to compare assessments in different cultural settings with the results of the reported study.
Materials and methods
Design and participants
The study presented here was a descriptive, observational cross-sectional study. A total of 175 schizophrenia outpatients were referred to the study coordinators. Of those, seven refused to sign the written informed consent (four indicated that they were living far away from the hospital and three argued that they had no time to participate in the study). A final sample of 168 patients participated in the study. Patients who fulfilled the following inclusion criteria were recruited for the study: (a) Diagnostic and Statistical Manual of Mental Disorders: Fourth Edition diagnosis of schizophrenia,65 (b) age 18 years or older, (c) community dwelling (including hostels, sheltered housing, or living with relatives), (d) no psychiatric hospitalization for a minimum of 6 months following discharge from psychiatric hospital, (e) no change in antipsychotic medication in the last 6 months preceding assessment in the study protocol, (f) no a severe and unstable medical disease, and (g) cognitively able to give informed consent. All patients were receiving treatment as usual, which consisted of pharmacological treatment alone, for 6 months or more at the Schizophrenia Clinic of the National Institute of Psychiatry in Mexico City. No other rehabilitation or psychosocial treatment was administered to the patients during the study protocol. The institute belongs to the Coordination of the National Institutes of Health and Hospitals of High Specialty of the Secretary of Health, Mexico. The Scientific Research Committee and the Ethics Committee of the institute approved the study protocol.
Procedures
Patient diagnosis was verified with their clinical chart by the three psychiatrists in charge of referring patients who fulfilled the inclusion criteria to the study protocol. After a detailed description of the study to the participants, written informed consent was obtained. Face-to-face interviews were conducted with all participants in order to endorse research measures. When patients were unable to provide certain specific data during the interview (number and duration of hospitalizations, time elapsed between the manifestations of the disease and seeking psychiatric help), relatives were requested to collaborate providing reliable information.
Measures
The following measures were used in the study.
Psychopathology of psychotic symptoms was evaluated using the PANSS.66 consisting of three subscales: positive (seven items), negative (seven items), and general psychopathology (GPS) (16 items). Each item is rated from 1, “absence of psychopathology”, to 7, “extremely severe”. Symptomatology was measured using the five orthogonal symptom dimensions model (positive, negative, cognitive, excitement, and depression/anxiety factors) since it appears to be more representative of the psychopathological data.67–69
Symptomatic remission was assessed according to the criteria proposed by the RSWG,1 which considers eight chosen items of the PANSS: delusions (P1), conceptual disorganization (P2), hallucinatory behavior (P3), unusual thought content (G9), mannerism and posturing (G5), blunted affect (N1), passive/apathetic social withdrawal (N4), and lack of spontaneity (N6). These represent the core symptoms for schizophrenia that should score on a severity level of mild or less (≤3), each item scoring from 1, “no symptom” to 7, “extremely severe symptoms”. The achievement of symptomatic remission considers two criteria: symptom severity and time remission; for the present study the time criterion was not applicable due to the cross-sectional design of the study. This type of design has been utilized when there have been limits to verifying the time criterion of remission, when the time component was not considered in the design of the study, when patients were considered to have achieved symptomatic remission exclusively on the basis of their remission scores regardless of the time criterion, or when the study was not designed to follow changes in outcome over time.4,23,28,70–75
Psychosocial remission was assessed with the criteria proposed by Barak et al included in the PSRS27 designed to assess psychosocial impairments in the following areas: (1) family relations, (2) understanding and self-awareness, (3) energy, (4) interest in daily life, (5) self-care, (6) activism, (7) responsibility in medical treatment, and (8) use of community services. Severity of impairment for each item was rated from 1, “absent”, to 7, “extreme”. Psychosocial remission was achieved with a score of mild or less (≤3) on the severity level of impairment. The scale has been validated. Acceptable face validity and good inter-rater reliability have been established.2,27
Functioning was assessed with the GAF,65 which measured the combination of symptoms and psychological, social, and occupational functioning on a mental health-illness continuum: level of functioning: 1–10, 11–20, 41–50, 51–60, 91–100, etc. The GAF’s rating is made on a scale from 1 to 100. A total GAF score of ≥60 points was considered as demonstrating adequate functioning.
Illness severity was evaluated with the CGI Scale.45 The CGI Scale was developed to provide a brief assessment of the patient’s clinical functioning that includes knowledge of the patient’s history, symptoms, psychosocial issues, behavior and the impact of the symptoms on the patient’s ability to function. The CGI Scale is rated on a seven-point scale on which 1, “normal, not at all ill”; 2, “borderline mentally ill”; 3, “mildly ill”; 4, “moderately ill”; 5, “markedly ill”; 6, “severely ill”; and 7, “extremely ill”. The psychometric properties of the CGI Scale have been examined and found sufficient.76
For the present study, functional remission was defined when simultaneously achieving the symptomatic and psychosocial remission criteria and having a GAF score of ≥60 that was considered adequate functioning. Patients were classified into two groups: the first group – functionally remitted patients – included patients who achieved symptomatic remission and psychosocial remission and had a GAF score ≥60.77 The second group – non-remitted patients – comprised the remaining patients of the sample who did not meet these three criteria.
Sociodemographic and clinical data were obtained using a structured questionnaire designed exclusively for the study.
Statistical analysis
Demographic and clinical characteristics were determined and completed with frequencies and percentages for categorical variables and with means and standard deviations (SDs) for continuous variables. Skewness and kurtosis were used in order to test normal distribution of the symptomatic and functional dimensions. For the comparison of demographic and clinical characteristics between groups, chi-square tests and independent sample t-tests were used where applicable. Pearson’s correlation coefficient was used to determine the linear association of the GAF score with the PANSS dimensions and the PSRS score. Logistic regression was used with the backward stepwise selection method for the calculation of the likelihood that patients achieve functional remission. The logistic regression model included demographic and clinical characteristics as explanatory variables and functional remission as the outcome. Demographic and clinical characteristics were included in the logistic regression analysis if any statistical significant difference emerged between groups at the initial comparative analyses. The significance level for tests was established at P≤0.05. SPSS Statistics (v 20) software was used to analyze the data.78
Results
Demographic and clinical characteristics of the sample
One hundred and sixty-eight patients were included. Men accounted for 61.9% (n=104) of the sample and the remaining 38.1% (n=64) were women. The mean age of participants was 37.0 (SD =10.3) years and 12.3 (SD =3.4) years of education. The majority of patients were single (n=157, 93.5%) and unemployed (n=97, 57.7%) at the time of the study. The predominant diagnosis among the sample was paranoid schizophrenia (n=124, 73.8%) followed by schizoaffective disorder (n=18, 10.7%); delusional disorder, undifferentiated schizophrenia, residual schizophrenia (n=6, 3.6% each); and disorganized schizophrenia (n=4, 2.4%). The remaining diagnoses (catatonic and simple schizophrenia, undefined psychosis, and schizophreniform disorder) were present in only one subject per diagnosis. Age of illness onset was 23.2 (SD =7.1) years and most of the patients reported a DUP of a year or less (n=127, 75.6%). More than half of the patients (n=106, 63.1%) reported being hospitalized at some point during their disease course, with a mean of 2.3 (SD =2.2, range 1–15) hospitalizations. At the time of their inclusion in the present study all patients were treated by antipsychotic medication, 72.6% (n=122) with atypical antipsychotics and the remaining patients (n=46, 27.4%) with typical antipsychotics. From the review of patients’ clinical records, interviews face-to-face with the patients and their corresponding relatives, and clinician perspective, 97% (n=163) were adequately adherent, four patients (2.4%) were partially adherent, and only one patient (0.6%) was non-adherent to treatment. The mean number of current antipsychotic medications used by the patients was of 2.3 (SD =1.1, range 1–6) (Table 1).
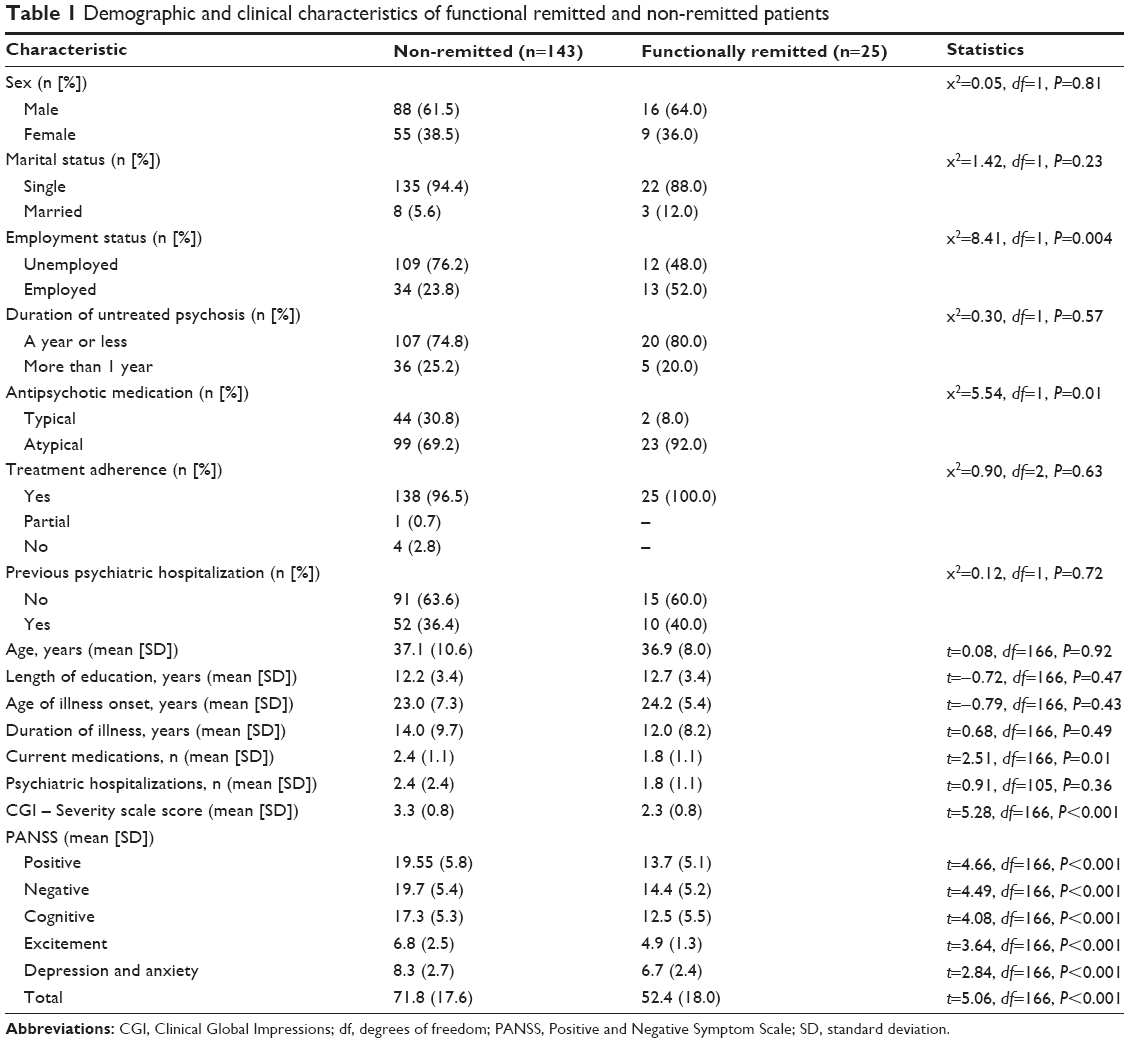 | Table 1 Demographic and clinical characteristics of functional remitted and non-remitted patients |
Symptomatic and psychosocial remission
Symptomatic (PANSS and CGI Scale) and psychosocial dimensions (PSRS and GAF) distributions showed acceptable values of skewness and kurtosis, where none of the values was excessively out of range (skewness range −0.34 to 0.77 and kurtosis range −0.90 to 1.88). The mean CGI – Severity score for the sample was 3.1 (SD =0.9), indicating that patients were “mildly ill”; this was substantiated by the mean total PANSS score (68.9, SD =18.9). The mean GAF score of the sample was 59.8 (SD =8.4), reflecting moderate symptoms and difficulties in functioning, while the PSRS total score was 22.3 (SD =9.1).
Significant associations were found between the GAF scores and the PANSS dimensional scores and the PSRS – positive dimension (r=−0.51, P<0.001), negative dimension (r=−0.60, P<0.001), cognitive dimension (r=−0.55, P<0.001), excitement dimension (r=−0.42, P<0.001), and depression/anxiety dimension (r=−0.26, P=0.001). The association between the GAF score and the PSRS was also significant (r=−0.28, P<0.001).
The symptomatic remission criteria were fulfilled by 45.2% (n=76) of the patients, while 32.1% (n=54) achieved psychosocial remission according to the PSRS total score. In addition, using the cutoff score of 60 for the GAF scale, 53.6% (n=90) of the patients reported adequate functioning.
According to the study’s predefined functional remission (symptomatic and psychosocial remission and a GAF score ≥60), 14.9% (n=25) of the patients were classified as functionally remitted and the remaining 85.1% (n=143) as non-remitted.
Comparing functionally remitted and non-remitted patients
Both groups had similar demographic features, with the exception of employment status, where functionally remitted patients were more frequently employed than non-remitted patients. Regarding clinical features, more functionally remitted patients were treated by atypical antipsychotics, had fewer additional current medications, and exhibited less severe scores on the CGI – Severity scale and in the five PANSS domains than non-remitted patients. The results of the comparison between groups are shown in Table 1.
Predictors of functional remission
Variables included in the logistic regression analyses were: employment status, type of antipsychotic, number of current medications, CGI Scale score and the five domains of the PANSS. All dimensional variables were classified (dummy coding) in auxiliary variables to perform this analysis. The variables were represented by two values, “0” or “1”, based on the mean value of the dimensional variable, where the value “1” was considered the risk/present value. For example, the mean value for the positive PANSS subscale was represented as “1/present” if the patient scored ≥18, and as “0/absent” if the patient scored <18.
The logistic regression equation was capable of correctly classifying 87.5% of the cases. The equation was generally more exact on predicting non-remitted patients (95.8%) than the functionally remitted ones (28.0%). Also, this model was statistically significant according to the Hosmer and Lemeshow79 value (P=0.56) and predicted 42.5% of the variation. The logistic regression model included five predictive variables for functional remission: (1) being employed, (2) use of atypical antipsychotics, (3) lower number of medications, (4) lower negative symptom severity (a score <18 in the PANSS negative dimension), and (5) lower excitement symptom severity (a score <6 in the PANSS excitement dimension) (Table 2).
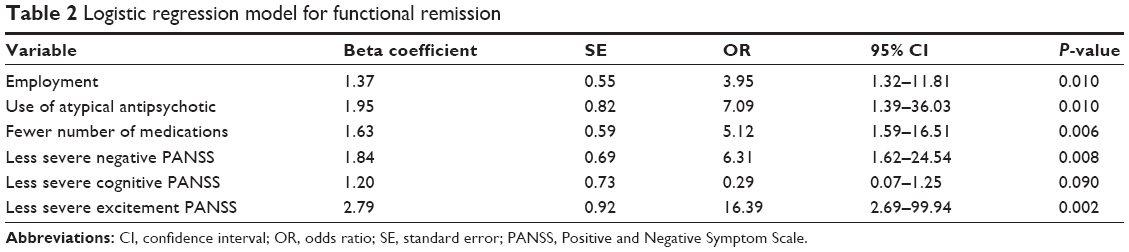 | Table 2 Logistic regression model for functional remission |
Discussion
Recent advances in the treatment of schizophrenia backed by strong scientific support present a more promising long-term outlook for schizophrenia patients than calculated in the 1990s. Evidence-based strategies that include the combination of pharmacological and psychosocial treatments have demonstrated their effectiveness, showing a promising perspective and increased outcome expectations.21,80,81 In the present study, 45.2% of patients fulfilled the RSWG symptomatic remission criteria, 32.1% achieved psychosocial remission, and 53% reported adequate functioning according to the GAF scale. However, the combination of these three outcome criteria, symptomatic and psychosocial remission and functioning, indicated that only a minority of patients (14.9%) achieved our predefined functional remission outcome. The results of this study are in agreement with other studies. Only 7%,4 8%,25 10.2%,28 and 27%84 of schizophrenia patients were reported to have achieved complete (functional) remission in studies designed in a manner comparable to the present survey.4,25,63,75
In the study reported here, predictors of functional remission included being employed, use of atypical antipsychotics, a lower number of medications, lower negative symptom severity, and lower excitement symptom severity. Other studies reported as predictors of functional remission: younger age, employment, a shorter duration of illness, a shorter length of current episode, and a lower PANSS negative and global subscore at admission;43 good social support and higher education;82 female sex, being married, younger age, tertiary education, shorter DUP, lower baseline PANSS negative scores;83 lower PANSS negative symptoms, receiving at least 3 years of psychiatric treatment;62 and negative symptoms, depression, age, sex, verbal memory deficits, and reduced visual acuity.32 It is thus obvious that more work needs to be undertaken before a more coherent set of remission predictors can be crystallized.
Limitations
The reported study has several limitations that should be taken into consideration, some of which may limit the generalizability of our findings. More importantly, the limited capacity of the logistic regression model to predict functional remitters may be related to the lack of inclusion of other relevant variables; functional remission in schizophrenia includes a variety of features ranging from clinically significant biomarkers (eg, pharmacogenetic testing for antipsychotic medications) to sociocultural variables (eg, social environment, premorbid adjustment) that may make a very important contribution to the prediction of functional remission and that were not included in the study. Nevertheless, the variables included in the model reported are clinically meaningful, as all of them have been clearly associated with prognosis in schizophrenia. The cross-sectional nature of this survey precludes identification of probable causes of non-remission. Finally, service delivery models differ significantly between countries and the scarcity of studies from outside Europe or North America makes comparisons difficult.
Conclusion
The results of this study indicate that a minority of patients with stable schizophrenia experienced functional remission. The insistence on complex outcome definitions of functional remission resulted in finding core subgroups of remitted patients. Future research should focus on assessing various clinical and psychosocial domains to determine functional remission in schizophrenia patients.
Functional remission in schizophrenia has been receiving increased attention in first-world countries especially in Europe and the USA. High-quality research could promote and stimulate research in other regions of the world, such as developing countries, in this case, in Latin America. It has been demonstrated that cultural factors influence symptom profile, the course, and the outcome of most psychiatric disorders – in this particular case, schizophrenia. Two collaborative studies, the International Pilot Study of Schizophrenia by the World Health Organization and the Determinants of Outcome of Severe Mental Disorders, demonstrated the importance of cultural factors in schizophrenia.84–86 The results on remission in different cultural settings such as Taiwan,48 India,49 Bali,25 and Italy47 are similar to those found in our study. It seems that the influence of culture on psychopathology is more relevant than racial similarity, historical relations, or geographic proximity in the manifestation of symptoms of schizophrenia when comparing patients of Japan and People’s Republic of China, Korea and People’s Republic of China, and Malta and Libya.87 It has been demonstrated that a better clinical global impression, such as functional remission, is more favorable among non-Western populations.51 This favorable impression in non-Western countries has been explained by factors such as family support, favorable attitudes among family members and the community, a higher level of marriage, styles of interaction, availability of non-stressful employment, and a higher level of supportive workplace colleagues.84,85 When we compared findings in other cultural settings with the results of this study, the importance of cultural factors became clear.
We consider this study to make an important contribution because this is the first time, as far as we are aware, that a relevant issue such as predictors of functional remission has been assessed in Mexican patients with schizophrenia. This might be useful for facilitating decision-making in clinical practice and in future research in Mexico and other countries in Latin America, but also it could be of interest to schizophrenia researchers all over the world. It is well known that research on mental illness is almost nonexistent in Latin America. The present study was carried out at the National Institute of Psychiatry, an institution dedicated to scientific research in mental illness in Mexico. We expect that this research might contribute to the growth of knowledge about functional remission in schizophrenia.
Acknowledgment
This study was conducted and supported as a scientific project, “Symptomatic remission, psychosocial remission and recovery in schizophrenia patients”, by the National Institute of Psychiatry Ramón de la Fuente, Ministry of Health, Mexico (project number: EP114547.0; project coordinator: Marcelo Valencia).
Disclosure
The authors report no conflicts of interest in this work.
References
Andreasen NC, Carpenter WT Jr, Kane JM, Lasser RA, Marder SR, Weinberger DR. Remission in schizophrenia: proposed criteria and rationale for consensus. Am J Psychiatry. 2005;162(3):441–449. | ||
Barak Y, Aizenberg D. Clinical and psychosocial remission in schizophrenia: correlations with antipsychotic treatment. BMC Psychiatry. 2012;12:108. | ||
Best MW, Gupta M, Bowie CR, Harvey PD. A longitudinal examination of the moderating effects of symptoms on the relationship between functional competence and real world functional performance in Schizophrenia. Schizopr Res Cogn. 2014;1(2):90–95. | ||
San L, Ciudad A, Alvarez E, Bobes J, Gilataberte I. Symptomatic remission and social/vocational functioning in outpatients with schizophrenia: prevalence and associations in a cross-sectional study. Eur Psychiatry. 2007;22(8):490–498. | ||
Shrivastava A, Johnston M, Shah N, Bureau Y. Redefining outcome measures in schizophrenia: integrating social and clinical parameters. Curr Opin Psychiatry. 2010;23(2):120–126. | ||
Bai YM, Hsiao CY, Chen KC, et al. The development of a self-reported scale for measuring functionality in patients with schizophrenia – self-reported version of the graphic Personal and Social Performance (SRG-PSP) scale. Schizopr Res. 2014;159(2–3):546–551. | ||
Davidson L, Schnmutte T, Dinzeo T, Andres-Hyman R. Remission and recovery in schizophrenia: practitioner and patient perspectives. Schizopr Bull. 2008;34(1):5–8. | ||
Harvey PD, Strassnig M. Predicting the severity of everyday functional disability in people with schizophrenia: cognitive deficits, functional capacity, symptoms, and health status. World Psychiatry. 2012;11(2):73–79. | ||
Karow A, Moritz S, Lambert M, Schöttle D, Naber D; EGOFORS Initiative. Remitted but still impaired? Symptomatic versus functional remission in patients with schizophrenia. Eur Psychiatry. 2012;27:401–405. | ||
Liberman RP, Kopelowicz A. Recovery from schizophrenia: a concept in search of research. Psychiatr Serv. 2005;56(6):735–742. | ||
Ustun B, Kennedy C. What is “functional impairment”? Disentangling disability from clinical significance. World Psychiatry. 2009; 8(2):82–85. | ||
van Os J, Burns T, Cavallaro R, Leucht S, et al. Standardized remission criteria in Schizophrenia. Acta Psychiatr Scand. 2006:113(2):91–95. | ||
Emsley R, Chiliza B, Asmal L, Lehloenya K. The concepts of remission and recovery in schizophrenia. Curr Opin Psychiatry. 2011; 24(2):114–121. | ||
Brissos S, Dias VV, Balanzá-Martinez V, Carita AI, Figueira ML. Symptomatic remission in schizophrenia patients: relationship with social functioning, quality of life, and neurocognitive performance. Schizophr Res. 2011;129(2–3):133–136. | ||
Weiden P, Zygmunt A. Medication noncompliance in schizophrenia: part I. Assessment. Journal of Practical Psychiatry and Behavioral Health. 1997;3:106–110. | ||
Burns T. Evolution of outcome measures in schizophrenia. Br J Psychiatry. 2007;50:s1–s6. | ||
Yanos PT, Moos H. Determinants of functioning and well-being among individuals with schizophrenia: an integrated model. Clin Psychiatr Rev. 2007;27(1):58–77. | ||
Gorwood P, Peuskens J; European Group On Functional Outcomes, Remission in Schizophrenia. Setting new standards in schizophrenia outcomes: symptomatic remission 3 years before versus after the Andreasen criteria. Eur Psychiatry. 2012;27(3):170–175. | ||
Leucht S, Lasser R. The concepts of remission and recovery in schizophrenia. Pharmacopsychiatry. 2006;39(5):161–170. | ||
Llorca PM, Sacchetti E, Lloyd K, Kissling W, Medori R. Long-term remission in schizophrenia and related psychoses with long-acting risperidone: results obtained in an open-label study with an observation period of 18 months. Int J Clin Pharmacol Ther. 2008;46(1):14–22. | ||
Henry LP, Amminger GP, Harris MG, et al. The EPPIC follow-up study of first-episode psychosis: longer-term clinical and functional outcome 7 years after index admission. J Clin Psychiatry. 2010;71(6):716–728. | ||
Yeomans D, Taylor M, Curri A, et al. Resolution and remission in schizophrenia: getting well and staying well. Adv Psychiatr Treat. 2010;16(2):86–89. | ||
AlAqeel B, Margolese H. Remission in schizophrenia: critical and systematic review. Harv Rev Psychiatr. 2012;20(6):281–297. | ||
Remington G, Kapur S. Remission: what’s in a name? Am J Psychiatry. 2005;162(12):2393–2394. | ||
Kurihara T, Kato M, Reverger R, Tirta GR. Remission in schizophrenia: a community-based 6-year follow-up study in Bali. Psychiatr Clin Neurosci. 2011;65(5):472–482. | ||
Nasrallah HA, Targum SD, Tandon R, McCombs S, Ross R. Defining and measuring clinical effectiveness in the treatment of schizophrenia. Psychiatr Serv. 2005;56(3):273–282. | ||
Barak Y, Bleich A, Aizenberg D. Psychosocial remission in schizophrenia: developing a clinician-rated scale. Compr Psychiatry. 2010;51(1):94–98. | ||
Peuskens J, Gorwood P; EGOFORS Initiative. How are we assessing functioning in schizophrenia? A need for a consensus approach. Eur Psychiatry. 2012;27(6):391–395. | ||
Keefe RS, Poe M, Walker TM, Harvey PD. The relationship of the Brief Assessment of Cognition in Schizophrenia (BACS) to functional capacity and real-world functional outcome. J Clin Exp Neuropsychol. 2006;28(2):260–269. | ||
Figueira M, Brissos S. Measuring psychosocial outcomes in schizophrenia patients. Curr Opin Psychiatry. 2011;24(2):91–99. | ||
Tse S, Davidson L, Chung KF, Yu CH, Ng KL, Tsoi E. Logistic regression analysis of psychosocial correlates associated with recovery from schizophrenia in a Chinese community. Int J Soc Psychiatry. 2015;61(1):50–57. | ||
Viertiö S, Tuulio-Henriksson A, Perälä J, et al. Activities of daily living, social functioning and their determinants in persons with psychotic disorder. Eur Psychiatry. 2012;27(6):409–415. | ||
Lambert M, Karow A, Leucht S, Schimmelmann BG, Naber D. Remission in schizophrenia: validity, frequency, predictors, and patients’ perspective 5 years later. Dialogues Clin Neurosci. 2010;12(3): 393–407. | ||
Leifker FR, Patterson TL, Heaton RK, Harvey PD. Validating measures of real-world outcome: the results of the VALERO expert survey and RAND panel. Schizophr Bull. 2011;37(2):334–343. | ||
Mueser K, Tarrier N, editors. Preface. In Handbook of Social Functioning in Schizophrenia. Boston, MA: Ally and Bacon; 1998:XI–III. | ||
Bellack AS, Green MF, Cook JA, et al. Assessment of community functioning in people with schizophrenia and other severe mental illnesses: a white paper based on an NIMH-sponsored workshop. Schizophr Bull. 2007;33(3):805–822. | ||
Albert N, Bertelsen M, Thorup A, et al. Predictors of recovery from psychosis Analyses of clinical and social factors associated with recovery among patients with first-episode psychosis after 5 years. Schizophr Res. 2011;125(2–3):257–266. | ||
Cannavó D, Concerto C, Battaglia E, et al. Insight and recovery in schizophrenic patients: an observational study. Clin Neuropsychopharmacology. 2013;23(1):S83–S84. | ||
Ciudad A, Bobes J, Alvarez E, San L, Novick D, Gilaberte I. Clinical meaningful outcomes in schizophrenia: remission and recovery. Rev Psiquiatr Salud Ment. 2011;4(1):53–65. English and Spanish. | ||
Valencia M, Caraveo J, Colín R, Verduzco W, Corona F. Symptomatic remission and recovery in patients with schizophrenia. Salud Mental J. 2014;37(1):59–74. | ||
Bobes J, Ciudad A, Alvarez E, San L, Polavieja P, Gilaberte I. Recovery from schizophrenia: results from a 1-year follow-up observational study of patients in symptomatic remission. Schizophr Res. 2009; 115(1):58–66. | ||
Cohen CI, Pathak R, Ramirez PM, Vahia I. Outcome among community dwelling older adults with schizophrenia: results using five conceptual models. Community Ment Health J. 2009;45(2):151–158. | ||
Schennach-Wolff R, Jäger M, Seemüller F, et al. Defining and predicting functional outcome in schizophrenia and schizophrenia spectrum disorders. Schizophr Res. 2009;113(2–3):210–217. | ||
Lambert M, De Marinis T, Pfeil J, Naber D, Schereiner A. Establishing remission and good clinical functioning in schizophrenia: predictors of best outcome with long-term risperidone long-acting injectable treatment. Eur Psychiatry. 2009;25(4):220–229. | ||
Guy W. Clinical global impressions. In: ECDEU Assessment Manual for Psychopharmacology: Revised, 1976. Rockville, MD: National Institute of Mental Health; 1976:217–222. | ||
Murphy HB, Raman AC. The chronicity of schizophrenia in indigenous tropical peoples. Results of a twelve-year follow-up survey in Mauritius. Br J Psychiatry. 1971;118(546):489–497. | ||
Rossi A, Bagalà A, Del Curatolo V, Scapati F, Bernareggi MM, Giustra MG; Risperidone Long-Acting Trial Investigators (R-LAI). Remission in schizophrenia: one-year Italian prospective study of risperidone long-acting injectable (RLAI) in patients with schizophrenia or schizoaffective disorder. Hum Psychopharmacol. 2009;24(7):574–583. | ||
Li CT, Su TP, Chou YH, et al. Symptomatic resolution among Chinese patients with schizophrenia and associated factors. J Formos Med Assoc. 2010;109(5):378–388. | ||
Saravanan B, Jacob KS, Johnson S, Prince M, Bhugra D, David AS. Outcome of first-episode schizophrenia in India: longitudinal study of effect of insight and psychopathology. Br J Psychiatry. 2010; 196(6):454–459. | ||
Mosolov SN, Potapov AV, Ushakov UV, Shafarenko AA, Kostyukova AB. Design and validation of standardized clinical and functional remission criteria in schizophrenia. Neuropsychiatr Dis Treat. 2014;10:167–181. | ||
Murray RM, Jones PB, Susser E, van Os J, Cannon M, editors. The Epidemiology of Schizophrenia. Cambridge: Cambridge University Press; 2003. | ||
Agid O, Kapur S, Arenovich T, Zipursky RB. Delayed-onset hypothesis of antipsychotic action: a hypothesis tested and rejected. Arch Gen Psychiatry. 2003;60(12):1228–1235. | ||
Emsley R, Rabinowitz J, Medori R; Early Psychosis Global Working Group. Remission in early psychosis: Rates, predictors, and clinical and functional outcome correlates. Schizophr Res. 2007; 89(1–3):129–139. | ||
Derks EM, Fleischhacker WW, Boter H, Peuskens J, Kahn RS; EUFEST Study Group. Antipsychotic drug treatment in first-episode psychosis: should patients be switched to a different antipsychotic drug after 2, 4, or 6 weeks of nonresponse? J Clin Psychopharmacol. 2010;30(2):176–180. | ||
Jäger M, Schmauss M, Laux G, et al. Early improvement as a predictor of remission and response in schizophrenia: Results from a naturalistic study. Eur Psychiatry. 2009;24(8):501–506. | ||
Schennach-Wolff R, Seemüller F, Obermeier M, et al. Response and remission of subjective well-being in patients suffering from schizophrenia spectrum disorders. Eur Psychiatry. 2010;26(5):284–292. | ||
Schennach-Wolff R, Jäger M, Obermeier M, et al. Quality of life and subjective well-being in schizophrenia and schizophrenia spectrum disorders: valid predictors of symptomatic response and remission? World J Biol Psychiatry. 2010;11(5):729–738. | ||
Schennach-Wolff R, Seemüller FH, Mayr A, et al. An early improvement threshold to predict response and remission in first-episode schizophrenia. Br J Psychiatry. 2010;196(6):460–466. | ||
Caton CL, Hasin DS, Shrout PE. Predictors of psychosis remission in psychotic disorders that co-occur with substance use. Schizopr Bull. 2006;32(4):618–625. | ||
Gasquet I, Haro JM, Tcherny-Lessenot S, Chartier F, Lépine JP. Remission in the outpatient care of schizophrenia: 3-year results from the Schizophrenia Outpatients Health Outcomes (SOHO) study in France. Eur Psychiatry. 2008;23(7):491–496. | ||
Novick D, Haro JM, Suarez D, Lambert M, Lépine JP, Naber D. Symptomatic remission in previously untreated patients with schizophrenia: 2-year results from the SOHO study. Psychopharmacology (Berl). 2007;191(4):1015–1022. | ||
Lambert M, Schimmelmann BG, Naber D, et al. Prediction of remission as a combination of symptomatic and functional remission and adequate subjective well-being in 2,960 patients with schizophrenia. J Clin Psychiatry. 2006;67(11):1690–1697. | ||
Robinson DG, Woerner MG, McMeniman M, Mendelowitz A, Bilder RM. Symptomatic and functional recovery from a first episode of schizophrenia or schizoaffective disorder. Am J Psychiatry. 2004;161(3):473–479. | ||
Brekke J, Kay DD, Lee KS, Green MF. Biosocial pathways to functional outcome in schizophrenia. Schizophr Res. 2005;80(2–3):213–225. | ||
American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders: Fourth Edition. Washington DC: APA; 1994. | ||
Kay SR, Fiszbein A, Vital-Herne M, Fuentes LS. The Positive and Negative Syndrome Scale – Spanish adaptation. J Nerv Ment Dis. 1990;178(8):510–517. | ||
Fresán A, De la Fuente-Sandoval C, Loyzaga C, et al. A forced five-dimensional factor analysis and concurrent validity of the Positive and Negative Syndrome Scale in Mexican schizophrenic patients. Schizophr Res. 2005;72(2–3):123–129. | ||
Lindenmayer JP, Grochowski S, Hyman RB. Five factor model of schizophrenia: replication across samples. Schizophr Res. 1995;14(3):229–234. | ||
van der Gaag M, Cuijpers A, Hoffman T, et al. The five-factor model of the Positive and Negative Syndrome Scale I: confirmatory factor analysis fails to confirm 25 published five-factor solutions. Schizophr Res. 2006;85(1–3):273–279. | ||
Alenius M, Hammarlund-Udenaes M, Hartvig P, Lindström L. Knowledge and insight in relation to functional remission in patients with long-term psychotic disorders. Soc Psychiatry Psychiatr Epidemiol. 2010;45(5):523–529. | ||
De Hert M, van Winkel R, Wampers M, Kane J, van Os J, Peuskens J. Remission criteria for schizophrenia: evaluation in a large naturalistic cohort. Schizophr Res. 2007;92(1–3):68–73. | ||
Eberhard J, Levander S, Lindström E. Remission in schizophrenia: analysis in a naturalistic setting. Compr Psychiatry. 2009;50(3):200–208. | ||
Fervaha G, Agid O, Takeuchi H, Foussias G, Lee J, Remington G. Clinical and functional outcomes in people with schizophrenia with a high sense of well-being. J Nerv Ment Dis. 2015;203(3):187–193. | ||
Helldin L, Kane JM, Hjärthag F, Norlander T. The importance of cross-sectional remission in schizophrenia for long-term outcome: a clinical prospective study. Schizopr Res. 2009;115(1):67–73. | ||
Mosolov SN, Potapov AV, Ushakov UV. Remission in schizophrenia: results of cross-sectional with 6-month follow-up period and 1-year observational therapeutic studies in an outpatient population. Ann Gen Psychiatry. 2012;11(1):1. | ||
Leught S, Engel RR. The relative sensitivity of the Clinical Global Impressions Scale and the Brief Psychiatric Rating Scale in antipsychotic drug trials. Neuropharmacology. 2006;31(2):406–412. | ||
Lambert M, De Marinis T, Pfeil J, Naber D, Schreiner A. Establishing remission and good clinical functioning in schizophrenia: predictors of best outcome with long-term risperidone long-acting injectable treatment. Eur Psychiatry. 2010;25:220–229. | ||
SPSS Statistics [computer software]. V 20. Armonk, NY: IBM Corporation; 2010. | ||
Hosmer DW, Lemeshow S. Applied Logistic Regression. 2nd ed. New York, NY: John Wiley and Sons; 2000. | ||
Dixon LB, Dickerson F, Bellack AS, et al; Schizophrenia Patient Outcomes Research Team (PORT). The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements. Schizophr Bull. 2010;36(1):48–70. | ||
Valencia M, Fresan A, Juárez F, Escamilla R, Saracco R. The beneficial effects of combining pharmacological and psychosocial treatment on remission and functional outcome in outpatients with schizophrenia. J Psychiatr Res. 2013;47(12):1886–1892. | ||
Dahlan R, Midin M, Sidi H. Remisssion of symptoms among schizophrenia patients receiving assertive community treatment (ACT) in Malaysia: one year follow-up. Sains Malays. 2013;42(3):389–397. | ||
Verma S, Subramanian M, Abdin E, Poon LY, Chong SA. Symptomatic and functional remission in patients with first-episode psychosis. Acta Psychiatr Scand. 2012;126(4):282–289. | ||
Harrison G, Hopper K, Graig T, et al. Recovery from psychotic illness: a 15- and 25-year international follow-up study. Br J Psychiatry. 2001;178:506–517. | ||
Jablensky A, Sartorius N, Ernberg G, et al. Schizophrenia: manifestations, incidence and course in different cultures. A World Health Organization ten-country study. Psychol Med Monogr Suppl. 1992;20:1–97. | ||
World Health Organization. Schizophrenia. An International Follow-up Study. Chichester: John Wiley and Sons; 1979. | ||
Masłowski J. Pathoplastic influences on symptoms of schizophrenia. A comparative study in Libya and Malta. Acta Psychiatr Scand. 1986;73(6):618–623. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.