Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Predialysis hypotension is not a predictor for mortality in long-term hemodialysis patients: insight from a single-center observational study
Authors Huang W ![]() , Hsu C, Hu C
, Hsu C, Hu C ![]() , Yen T
, Yen T ![]() , Weng C
, Weng C ![]()
Received 28 April 2016
Accepted for publication 23 June 2016
Published 24 August 2016 Volume 2016:12 Pages 1285—1292
DOI https://doi.org/10.2147/TCRM.S111635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Wen-Hung Huang,1,2 Ching-Wei Hsu,1,2 Ching-Chih Hu,3 Tzung-Hai Yen,1,2 Cheng-Hao Weng1,2
1Department of Nephrology, Division of Clinical Toxicology, Chang Gung Memorial Hospital, Linkou Medical Center, Gueishan, Taiwan, Republic of China; 2Department of Medicine, Chang Gung University College of Medicine, Taoyuan, Taiwan, Republic of China; 3Department of Hepatogastroenterology and Liver Research Unit, Chang Gung Memorial Hospital, Keelung, Taiwan, Republic of China
Introduction: Predialysis hypotension has been noted to be a predictor of mortality in hemodialysis (HD) patients. Previous studies evaluating the impact of predialysis hypotension on the mortality of HD patients did not exclude patients with diabetes mellitus (DM) or cardiovascular disease.
Methods: Eight hundred and sixty-six patients on maintenance HD were recruited. Clinical parameters were recorded and subjected to the analysis of predictors of predialysis hypotension and mortality.
Results: Multivariate logistic regression analyses indicated that DM (odds ratio [OR]: 0.439, P=0.002), hypertension history (OR: 0.634, P=0.022), Kt/V Daugirdas (OR: 2.545, P=0.001), anuria (OR: 2.313, P=0.002), serum phosphate (OR: 0.833, P=0.010), and serum triglyceride (OR: 1.002, P=0.012) were associated with predialysis hypotension. Multivariate Cox regression analysis showed that age (P<0.001), male sex (P=0.029), anuria (P=0.004), and DM (P=0.011) were associated with higher probability of 24- and 36-month mortality. Predialysis hypotension was not associated with higher probability of 12-, 24-, and 36-month mortality.
Conclusion: Predialysis hypotension is not a predictor of 12-, 24-, and 36-month survival in patients without DM and with higher dialysis adequacy.
Keywords: predialysis hypotension, hemodialysis, mortality
Introduction
Predialysis hypotension had been noted to be a predictor of mortality in hemodialysis (HD) patients.1,2 The causes of predialysis hypotension include heart failure, coronary artery disease (CAD),3,4 diabetes-related severe autonomic neuropathy,5 and uremic autonomic neuropathy.6,7 Autonomic dysfunction and myocardial fibrosis-related heart failure may cause sudden cardiac death in HD patients.8 CAD is the most common cause of morbidity and mortality in HD patients.9 Uremic neuropathy also contributes largely to the morbidity and mortality in patients with renal failure. Previous studies evaluating the impact of predialysis hypotension on the mortality of HD patients did not exclude patients with diabetes mellitus (DM) or cardiovascular disease (CVD). The aim of this study is to further clarify the correlation between predialysis hypotension and mortality in regular long-term HD patients.
Methods
The Institutional Review Board Committee of Chang Gung Memorial Hospital approved the study protocol. Written informed consent was obtained from all patients enrolled in this study. Senior nephrologists reviewed all medical records during the study period, including medical history, laboratory data, and inclusion and exclusion factors. In addition, all individual information was securely protected and was only available to the investigators. Finally, all primary data were collected according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Patients
Study patients were recruited from the three hemodialysis centers of Chang Gung Memorial Hospital, Lin-Kou Medical Center, and Taipei and Taoyuan branches. Only maintenance HD (MHD) patients who were aged 18 years or older and had received HD for at least 6 months were enrolled in this study. Patients with malignancies or obvious infectious diseases, as well as those who had been hospitalized or had undergone surgery within 3 months of the investigation, were excluded. DM was defined by either a physician’s diagnosis, antidiabetic drug treatment, or if two subsequent analyses demonstrated fasting blood glucose levels of >126 mg/dL. Most patients underwent 4 hours of hemodialysis three times a week. Hemodialysis was performed with single-use hollow-fiber dialyzers equipped with modified cellulose, polyamide, or polysulfone membranes. The dialysate used in all cases had a standard ionic composition with a bicarbonate-based buffer. We noted the incidence of CVDs including cerebrovascular disease, CAD, congestive heart failure, and peripheral vascular disease in these patients. Predialysis hypotension was defined as systolic blood pressure (SBP) <100 mmHg by at least two blood pressure measurements.10 Hypertension was defined as the regular use of antihypertensive drugs to control blood pressure or at least two blood pressure measurements of >140/90 mmHg.
Laboratory parameters
All the blood samples were drawn from the arterial end of the vascular access immediately after the initial 2-day interval for HD and were then centrifuged and stored at −80°C until use.
Statistical analysis
Data were analyzed using SPSS, version 12.0 for Windows 95 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was used to test if variables were normally distributed. A P-value of >0.05 was required to assume a normal distribution. Unless otherwise stated, continuous variables were expressed as mean ± standard deviation or median (interquartile range), and categorical variables were expressed as numbers or percentages. χ2 or Fisher’s exact tests were used to analyze the correlation between categorical variables. Comparisons between two groups were performed using the Mann–Whitney U-test and Student’s t-test. Risk factors for predialysis hypotension were assessed by performing univariate logistic regression analysis, and all variables with P<0.1 were included in a multivariate analysis by applying a multiple logistic regression based on forward elimination of data. The data of intact parathyroid hormone, serum ferritin, and high-sensitivity C-reactive protein levels were log-transformed for regression analysis. Risk factors for mortality were assessed by performing univariate Cox regression analysis, and variables with P<0.1 were included in a multivariate analysis by applying a multiple Cox regression based on forward elimination of data.
Results
Subject characteristics
As shown in Table 1, 866 patients were included. The patients on HD were 56.18±13.59 years old, and 440 patients were male (50.8%). The average HD duration was 6.96±5.35 years. One hundred and fifty six patients (18%) had predialysis hypotension.
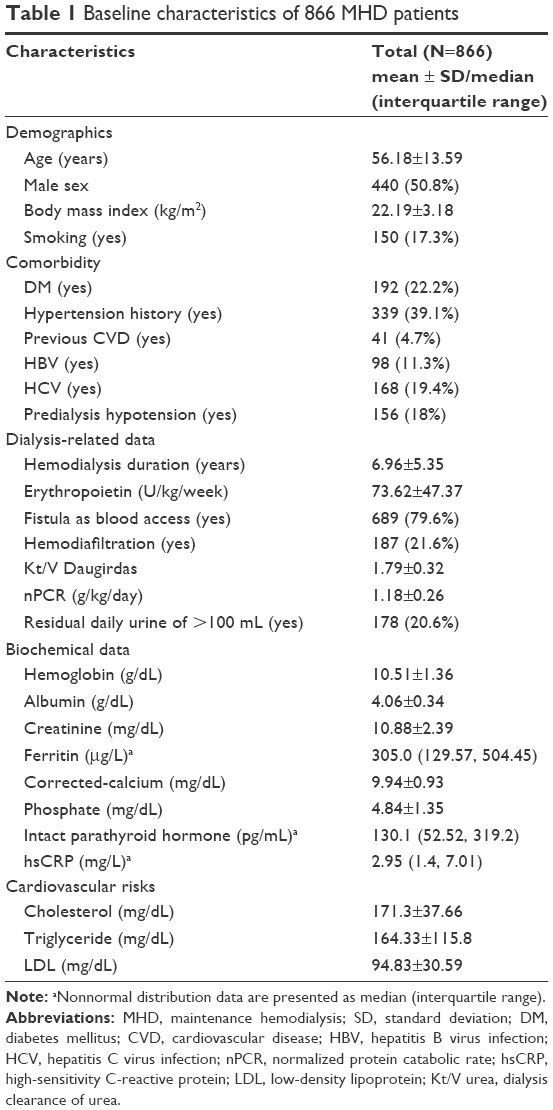 | Table 1 Baseline characteristics of 866 MHD patients |
Comparison of clinical variables between patients with and without predialysis hypotension
A lower proportion of DM (12.8% vs 24.2%, P=0.001) and hypertension history (29.5% vs 41.3%, P=0.007) and higher proportion of anuria (88.5% vs 77.5%, P=0.001) were observed in patients with predialysis hypertension compared with predialysis nonhypotension patients. Furthermore, the predialysis hypotension patients had longer HD duration (8.20±5.88 vs 6.69±5.196 years, P=0.001), higher Kt/V Daugirdas (dialysis clearance of urea) (1.9013±0.35856 vs 1.7769±0.31696, P<0.001), and lower serum level of phosphate (4.579±1.3477 vs 4.902±1.3506, P=0.007) than predialysis nonhypotension patients (Table 2).
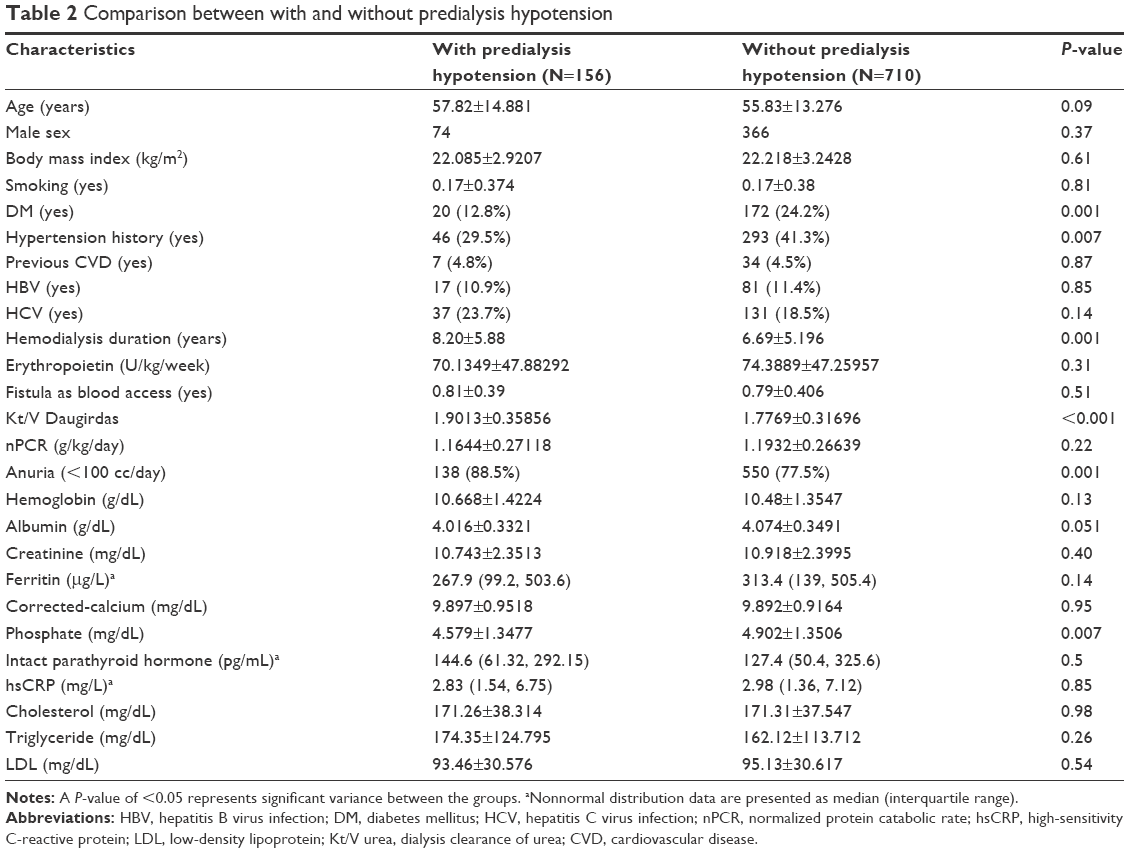 | Table 2 Comparison between with and without predialysis hypotension |
Clinical predictors of pre-dialysis hypotension
Univariate logistic regression identified several clinical variables that were significantly associated with predialysis hypotension (Table 3). Multivariate forward logistic regression analyses of all parameters indicated that DM (odds ratio [OR]: 0.476, 95% confidence interval [CI]: 0.283–0.803, P=0.005), hypertension history (OR: 0.596, 95% CI: 0.40–0.887, P=0.011), Kt/V Daugirdas (OR: 3.031, 95% CI: 1.713–5.363, P<0.001), anuria (OR: 2.204, 95% CI: 1.288–3.772, P=0.004), hemoglobin (OR: 1.178, 95% CI: 1.029–1.349, P=0.018), serum phosphate (OR: 0.826, 95% CI: 0.717–0.952, P=0.008), and serum triglyceride (OR: 1.002, 95% CI: 1.001–1.004, P=0.008) were associated with predialysis hypotension. Multivariate forward logistic regression analyses of parameters with P<0.1 under univariate logistic regression indicated that DM (OR: 0.439, 95% CI: 0.262–0.737, P=0.002), hypertension history (OR: 0.634, 95% CI: 0.430–0.936, P=0.022), Kt/V Daugirdas (OR: 2.545, 95% CI: 1.473–4.396, P=0.001), anuria (OR: 2.313, 95% CI: 1.357–3.942, P=0.002), serum phosphate (OR: 0.833, 95% CI: 0.725–0.957, P=0.010), and serum triglyceride (OR: 1.002, 95% CI: 1.001–1.003, P=0.012) were associated with predialysis hypotension.
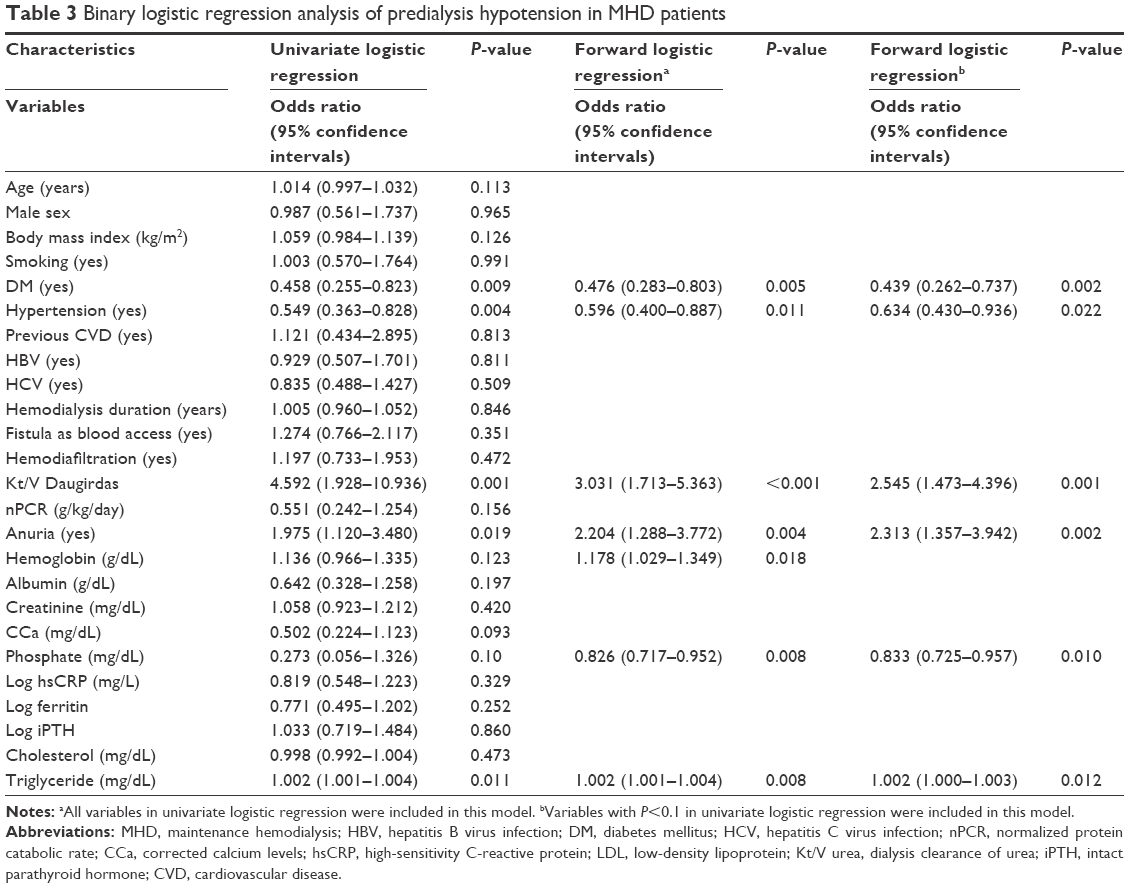 | Table 3 Binary logistic regression analysis of predialysis hypotension in MHD patients |
Clinical predictors of 12 months mortality
Multivariate Cox regression analysis showed that age (P<0.001), body mass index (P=0.003), hepatitis B virus infection (P=0.026), and anuria (P=0.022) were associated with higher probability of 12 months mortality. Hemoglobin (P<0.001), serum albumin (P=0.039), and predialysis hypotension (P=0.011) were associated with lower probability of 12 months mortality (Figure 1).
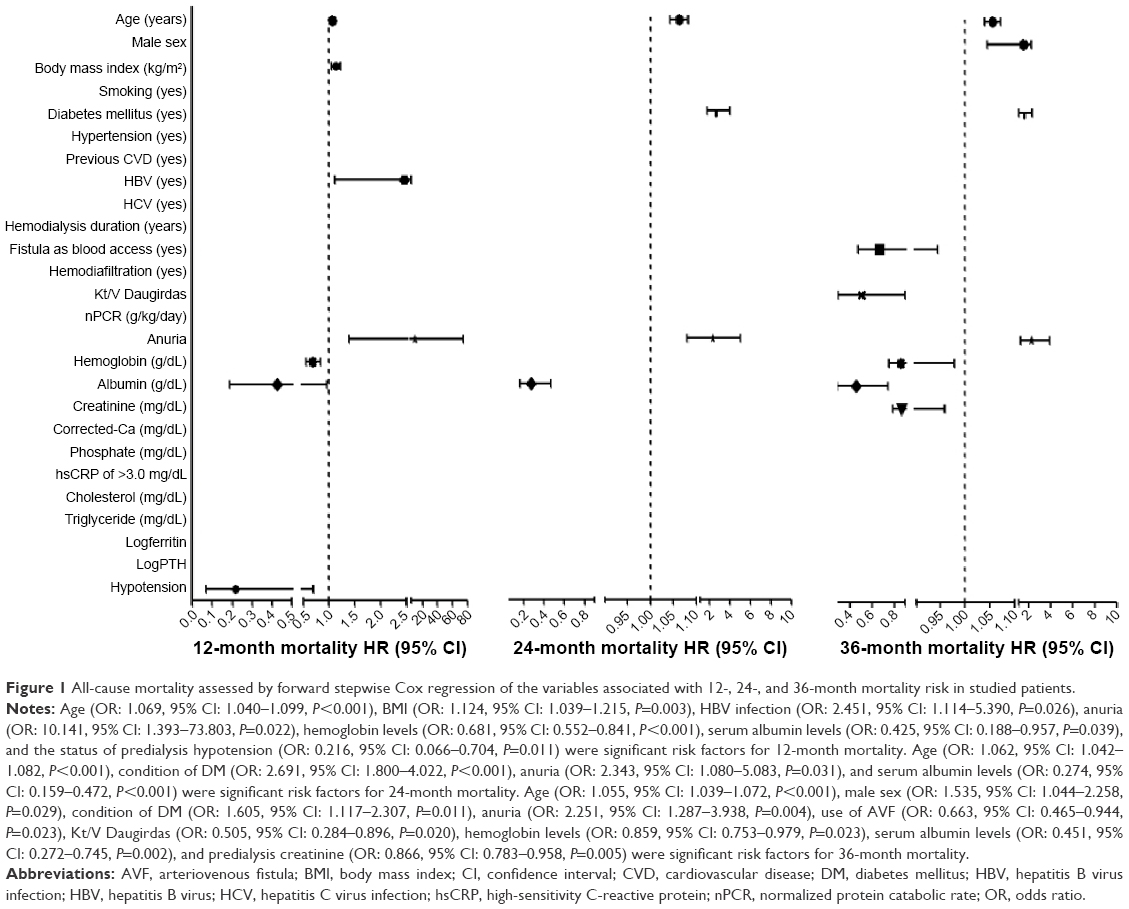 | Figure 1 All-cause mortality assessed by forward stepwise Cox regression of the variables associated with 12-, 24-, and 36-month mortality risk in studied patients. |
Clinical predictors of 24 months mortality
Multivariate Cox regression analysis showed that age (P<0.001), DM (P<0.001), and anuria (P=0.031) were associated with higher probability of 24-month mortality. Serum albumin (P<0.001) was associated with lower probability of 24-month mortality. Predialysis hypotension was not associated with 24 months mortality (Figure 1).
Clinical predictors of 36 months mortality
Multivariate Cox regression analysis showed that age (P<0.001), male sex (P=0.029), anuria (P=0.004), and DM (P=0.011) were associated with higher probability of 36 months mortality. Use of arteriovenous fistula as vascular access (P=0.023), Kt/V Daugirdas (P=0.020), hemoglobin (P=0.023), serum albumin (P=0.002), and predialysis creatinine (P=0.005) were associated with lower probability of 36 months mortality. Predialysis hypotension was not associated with 36 months mortality (Figure 1).
The cumulative survival rate was different between patients with and without predialysis hypotension in 12-month observation (Figure 2A, P=0.045); however, the 24 (Figure 2B, P=0.183) and 36 (Figure 2C, P=0.478) months survival rates were not significantly different between patients with and without predialysis hypotension.
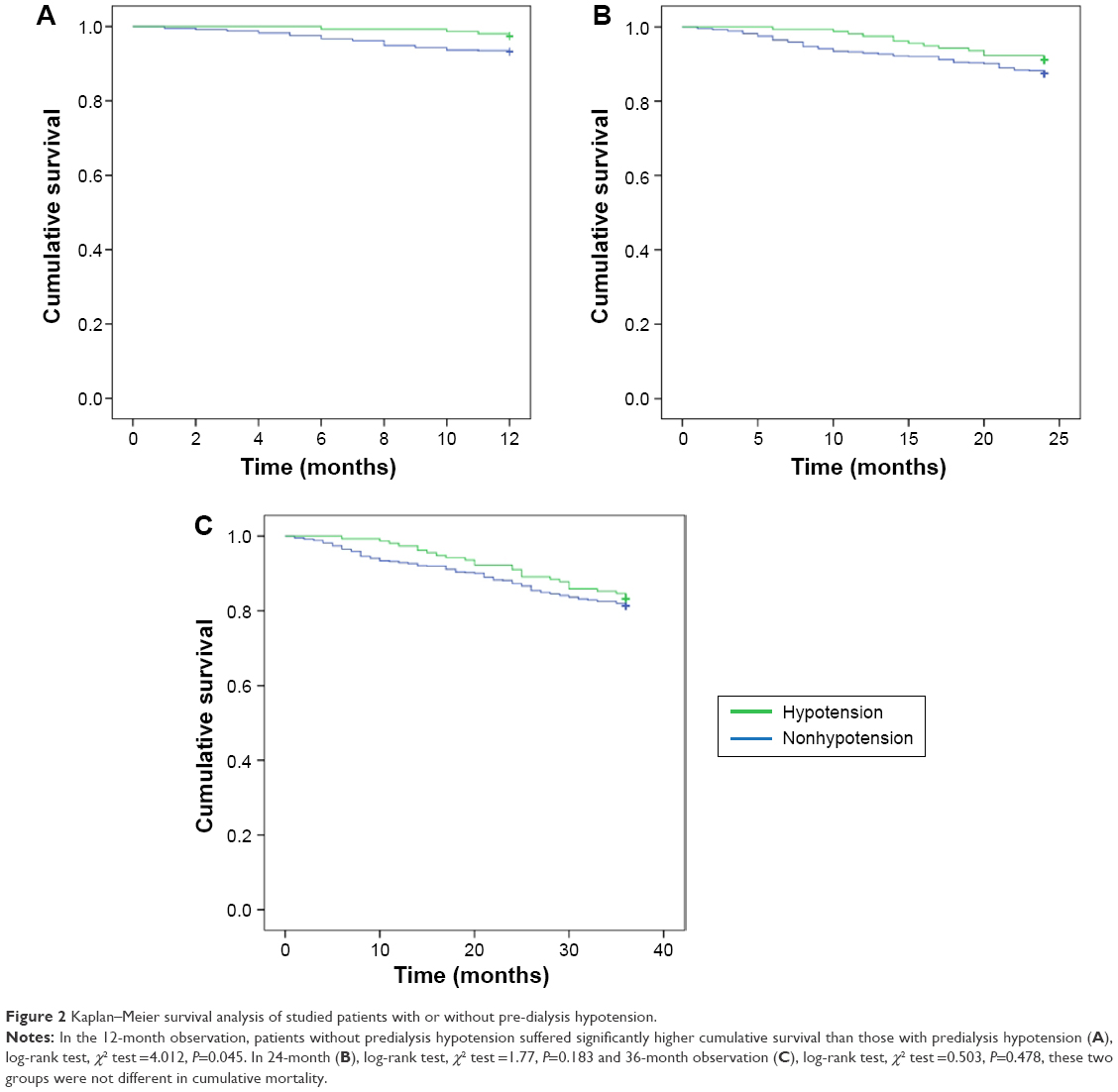 | Figure 2 Kaplan–Meier survival analysis of studied patients with or without pre-dialysis hypotension. |
Discussion
Intradialytic hypotension (IDH) was usually considered as a mortality risk factor. However, observational studies had different results. Tisler et al11 showed that neither frequent IDH nor occasional IDH was associated with mortality. Others found associations between IDH and greater all-cause mortality, a composite outcome of myocardial infarction, stroke, and cardiovascular (CV) mortality.12,13 All patients in this study with predialysis hypotension had nadir SBP <100 mmHg, which was the definition of IDH in many studies. But the results in this study showed that predialysis hypotension was not associated with all-cause 24- and 36-month mortality. Predialysis hypotension was even associated with lower probability of 12-month mortality.
Although mostly asymptomatic or with minimal symptoms, the presence of orthostatic hypotension in the general population increases mortality and the incidence of myocardial infarction, stroke, heart failure, and atrial fibrillation independently.14 Postprandial hypotension has also been noted to be a risk factor for CV mortality in the general population.15 In the present study, predialysis hypotension was not a predictor of all-cause mortality. The reasons behind the opposite results of hypotension in mortality between the general population and HD patients still need further investigation.
Robinson et al2 showed that compared with predialysis SBP of 130–159 mmHg, mortality was 13% higher in facilities that had 20% more patients with SBP of 110–129 mmHg and 16% higher in facilities that had 20% more patients with SBP of >160 mmHg. For patient-level SBP, mortality was elevated at low (<130 mmHg), not high (≥180 mmHg), SBP. The hazard ratio (HR) of SBP <110 mmHg for mortality was elevated (HR: 1.55, 95% CI: 1.39–1.71, P<0.001), compared with BP in the range of 130–139 mmHg. The percentages of CVD, cerebrovascular disease, congestive heart failure, lung disease, peripheral vascular disease, and cancer in patients with predialysis SBP <110 mmHg were significantly higher than the reference group, which had SBP in the range of 130–139 mmHg in the study of Robinson et al.2 In the present study, the patients with predialysis hypotension did not have higher percentage of CVD than those without predialysis hypotension. This might be the reason that our predialysis hypotension patients did not have higher mortality rate than patients without predialysis hypotension. Inaba et al16 also showed that in Japanese HD patients, both low and high BP were associated with all-cause mortality. Zager et al17 demonstrated that predialysis, neither systolic nor diastolic hypertension was associated with an increase in CV mortality. Postdialysis, SBP ≥180 mmHg (relative risk [RR]: 1.96, P<0.015) and diastolic blood pressure ≥90 mmHg (RR: 1.73, P<0.05) were associated with increased CV mortality. Low SBP (SBP <110 mmHg) was associated with increased CV mortality, pre- and postdialysis. The present study is the first to demonstrate that predialysis hypotension was not associated with 24- and 36-month mortality in HD patients.
Predialysis hypotension might result from heart failure,18 diabetic autonomic neuropathy, and uremic autonomic neuropathy.19 However, the present study showed that DM had a negative association with predialysis hypotension and that CVD was not associated with predialysis hypotension. These might be the reasons that our patients with predialysis hypotension did not have higher mortality than those without predialysis hypotension. Higher Kt/V Daugirdas was a predictor of predialysis hypotension in our study. Chan et al20 showed that improved Kt/V Daugirdas from 1.2±0.06 to 2.04±0.08 after 2 months (P=0.02) using nocturnal home HD could lower 24-hour mean arterial pressure (from 102±3 to 90±2 mmHg, P<0.01), total peripheral resistance (from 1,967±235 to 1,499±191 dyne s cm−5, P<0.01), and plasma norepinephrine (from 2.66±0.4 to 1.96±0.2 nmol, P=0.04).20 Others also noted that improved uremia control with longer periods of intermittent dialysis (6–8 hours per session) could lower blood pressure in the absence of any change in extracellular fluid volume or dry weight.21,22
Patients with predialysis hypotension had lower rate of previous hypertension, and previous hypertension history was also a negative predictor of predialysis hypotension. This might also be one of the reasons that predialysis hypotension was not a predictor of mortality. Hypertension is a well-known risk factor of CVDs.23 Hypertension is also a risk factor for heart failure, which is one reason for predialysis hypotension. Therefore, patients in this study with predialysis hypotension had fewer CVDs, and so predialysis hypotension might not be due to heart failure.
Anuria was a predictor of predialysis hypotension in this study. Anuria was also a predictor of 12-, 24-, and 36-month mortality. Anuria impairs both the removal of fluids and the clearance of solutes, resulting in increased morbidity and mortality.24 Residual renal function declines progressively after initiation of HD, and many patients with end-stage renal disease have no residual renal function.25 Predialysis hypotensive patients in this study had significantly longer duration of HD, and this might be the reason that anuria was a predictor of predialysis hypotension.
Limitations
To our knowledge, there are several studies1,2 that discuss the effect of predialysis hypotension on mortality of MHD patients. However, the results are still obscure. This study has several limitations. First, it was designed as a single-center observational study. However, due to the single-center nature of this study, the HD diet and health education are capable of being more consistently monitored. Also, all the patients were selected at random. Second, according to the focus on the association between predialysis hypotension and related variables in discussion, the data about heart function like echocardiography or autonomic dysfunction tests were not gathered. However, in our center, these aforementioned studies were not arranged for all HD patients routinely. Finally, comparing the advantages and disadvantages of predialysis hypotension with regard to mortality is difficult and complicated, particularly in such MHD patients who are at a high risk of chronic comorbidities, such as cerebrovascular disease and CVD, because many factors affect mortality. From these abovementioned points, all possible risk factors correlated with MHD mortality were considered.
Conclusion
Predialysis hypotension is not an adverse predictor for 12-, 24-, and 36-month survival in patients who do not have DM and have higher dialysis adequacy.
Acknowledgments
We thank the members of the Statistic Center in Chang Gung Memorial Hospital and Hemodialysis Center in Chang Gung Memorial Hospital for their invaluable and dedicated assistance. WHH and THY were funded by research grants from the Chang Gung Memorial Hospital, Linkou (CMRPG3D0322, G3D0012) and CHW was funded by research grants from the Chang Gung Memorial Hospital, Linkou (CMRPG5D0081).
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Losito A, Del Vecchio L, Del Rosso G, Malandra R; Gruppo di Studio Dell’Ipertensione Arteriosa, Societa Italiana di Nefrologia. Blood pressure and cardiovascular mortality in dialysis patients with left ventricular systolic dysfunction. Am J Hypertens. 2014;27(3):401–408. | ||
Robinson BM, Tong L, Zhang J, et al. Blood pressure levels and mortality risk among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2012;82(5):570–580. | ||
Schreiber BD. Congestive heart failure in patients with chronic kidney disease and on dialysis. Am J Med Sci. 2003;325(4):179–193. | ||
De Santo NG, Cirillo M, Perna A, et al. The heart in uremia: role of hypertension, hypotension, and sleep apnea. Am J Kidney Dis. 2001;38(4 Suppl 1):S38–S46. | ||
Akmal M. Hemodialysis in diabetic patients. Am J Kidney Dis. 2001;38(4 Suppl 1):S195–S199. | ||
Carreira MA, Nogueira AB, Pena FM, et al. Detection of autonomic dysfunction in hemodialysis patients using the exercise treadmill test: the role of the chronotropic index, heart rate recovery, and R-R variability. PLoS One. 2015;10(6):e0128123. | ||
Krishnan AV, Kiernan MC. Uremic neuropathy: clinical features and new pathophysiological insights. Muscle Nerve. 2007;35(3):273–290. | ||
Chiu DY, Sinha S, Kalra PA, Green D. Sudden cardiac death in haemodialysis patients: preventative options. Nephrology (Carlton). 2014;19(12):740–749. | ||
Afsar B, Turkmen K, Covic A, Kanbay M. An update on coronary artery disease and chronic kidney disease. Int J Nephrol. 2014;2014:767424. | ||
National Kidney F. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266. | ||
Tisler A, Akocsi K, Borbas B, et al. The effect of frequent or occasional dialysis-associated hypotension on survival of patients on maintenance haemodialysis. Nephrol Dial Transplant. 2003;18(12):2601–2605. | ||
Shoji T, Tsubakihara Y, Fujii M, Imai E. Hemodialysis-associated hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int. 2004;66(3):1212–1220. | ||
Stefansson BV, Brunelli SM, Cabrera C, et al. Intradialytic hypotension and risk of cardiovascular disease. Clin J Am Soc Nephrol. 2014;9(12):2124–2132. | ||
Ricci F, De Caterina R, Fedorowski A. Orthostatic Hypotension: Epidemiology, Prognosis, and Treatment. J Am Coll Cardiol. 2015;66(7):848–860. | ||
Zanasi A, Tincani E, Evandri V, Giovanardi P, Bertolotti M, Rioli G. Meal-induced blood pressure variation and cardiovascular mortality in ambulatory hypertensive elderly patients: preliminary results. J Hypertens. 2012;30(11):2125–2132. | ||
Inaba M, Karaboyas A, Akiba T, et al. Association of blood pressure with all-cause mortality and stroke in Japanese hemodialysis patients: the Japan Dialysis Outcomes and Practice Pattern Study. Hemodial Int. 2014;18(3):607–615. | ||
Zager PG, Nikolic J, Brown RH, et al. “U” curve association of blood pressure and mortality in hemodialysis patients. Medical Directors of Dialysis Clinic, Inc. Kidney Int. 1998;54(2):561–569. | ||
Port FK, Hulbert-Shearon TE, Wolfe RA, et al. Predialysis blood pressure and mortality risk in a national sample of maintenance hemodialysis patients. Am J Kidney Dis. 1999;33(3):507–517. | ||
Kersh ES, Kronfield SJ, Unger A, Popper RW, Cantor S, Cohn K. Autonomic insufficiency in uremia as a cause of hemodialysis-induced hypotension. N Engl J Med. 1974;290(12):650–653. | ||
Chan CT, Harvey PJ, Picton P, Pierratos A, Miller JA, Floras JS. Short-term blood pressure, noradrenergic, and vascular effects of nocturnal home hemodialysis. Hypertension. 2003;42(5):925–931. | ||
McGregor DO, Buttimore AL, Lynn KL, Nicholls MG, Jardine DL. A comparative study of blood pressure control with short in-center versus long home hemodialysis. Blood Purif. 2001;19(3):293–300. | ||
Luik AJ, vd Sande FM, Weideman P, Cheriex E, Kooman JP, Leunissen KM. The influence of increasing dialysis treatment time and reducing dry weight on blood pressure control in hemodialysis patients: a prospective study. Am J Nephrol. 2001;21(6):471–478. | ||
Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. Lancet. 2014;383(9921):999–1008. | ||
Pecoits-Filho R, Goncalves S, Barberato SH, et al. Impact of residual renal function on volume status in chronic renal failure. Blood Purif. 2004;22(3):285–292. | ||
Kuno T, Matsumoto K. Clinical benefit of preserving residual renal function in patients after initiation of dialysis. Blood Purif. 2004;22(Suppl 2):67–71. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.