Back to Journals » Clinical Ophthalmology » Volume 20
Precision in Intraocular Lens Calculation for Chinese Cataract Patients with Prior History of Radial Keratotomy
Authors Xiang Y ![]() , Li L, Yu H, Yuan L, Cai M, Zhang L, Hua X, Yuan X
, Li L, Yu H, Yuan L, Cai M, Zhang L, Hua X, Yuan X
Received 19 September 2025
Accepted for publication 16 December 2025
Published 9 January 2026 Volume 2026:20 563896
DOI https://doi.org/10.2147/OPTH.S563896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Bharat Gurnani
Yang Xiang,1,2 Liangpin Li,2 Haiqiang Yu,1,2 Liyun Yuan,2,3 Maoyu Cai,4 Liwei Zhang,5 Xia Hua,6,7,* Xiaoyong Yuan1,2,*
1Clinical College of Ophthalmology, Tianjin Medical University, Tianjin, People’s Republic of China; 2Tianjin Key Laboratory of Ophthalmology and Visual Science, Tianjin Eye Institute, Tianjin Eye Hospital, Tianjin, People’s Republic of China; 3School of Medicine, Nankai University, Tianjin, People’s Republic of China; 4Department of Ophthalmology, The Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China; 5Affiliated Hospital of Yunnan University, The Second Hospital of Yunnan Province, Yunnan Eye Hospital, Kunming, People’s Republic of China; 6Tianjin Aier Eye Hospital, Tianjin University, Tianjin, People’s Republic of China; 7Changsha Aier Eye Hospital, Changsha, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyong Yuan, Clinical College of Ophthalmology, Tianjin Medical University, Tianjin Key Laboratory of Ophthalmology and Visual Science, Tianjin Eye Institute, Tianjin Eye Hospital, No. 4 Gansu Road, Heping District, Tianjin, 300020, People’s Republic of China, Email [email protected] Xia Hua, Tianjin Aier Eye Hospital, 102 Fukang Road, Nankai District, Tianjin, 300191, People’s Republic of China, Email [email protected]
Purpose: To evaluate the predictive accuracy of eight traditional and contemporary intraocular lens (IOL) power calculation formulas in Chinese cataract patients with prior radial keratotomy (RK).
Patients and Methods: RK patients who underwent phacoemulsification with IOL implantation were retrospectively recruited. Refractive prediction errors (RPE)were calculated for eight formulas: Haigis-L, Shammas, Barrett True-K, Camellin Calossi Camellin (CCC), Kane, EVO, Pearl-DGS, and Jin-AI. The study compared RPE, mean absolute error (MAE), median absolute error (MedAE), and percentages of eyes achieving prediction errors within ± 0.25, ± 0.50, ± 0.75, ± 1.0, and ± 2.0 diopters.
Results: This retrospective study analyzed 34 eyes from 21 patients with prior RK surgery. The superior performing IOL power calculation formulas were Jin-AI (MAE = 0.64 D, MedAE = 0.49 D), Barrett True-K (MAE = 0.58 D, MedAE = 0.535 D), and EVO (MAE=0.59 D, MedAE = 0.538 D). These three formulas demonstrated comparable accuracy, with 47.1%, 44.1%, and 44.1% of eyes achieving prediction errors within ± 0.50 D, respectively. The Haigis-L and Pearl-DGS formulas exhibited significantly higher prediction errors in eyes with more than 12 RK incisions.
Conclusion: The Jin-AI, Barrett True-K, and EVO formulas demonstrated superior accuracy for IOL power calculation in Chinese cataract patients with prior RK. The Jin-AI formula, a novel artificial intelligence-based formula derived from Chinese individuals, presents a promising option for post-RK IOL calculation, while external validation studies across diverse ethnic groups are essential.
Keywords: radial keratotomy, cataract, IOL power calculation, refractive prediction errors
Introduction
Radial keratotomy (RK) emerged as a novel refractive surgical technique in the 1980s and early 1990s, gaining widespread adoption globally. However, excimer laser surgeries rapidly superseded RK due to its compromised safety profile and associated complications.1 Epidemiological data reveal that approximately 10% of practicing ophthalmologists performed several hundred thousand RK procedures in the United States alone.2,3 As these patients age, they increasingly develop cataracts, creating a growing population of post-RK eyes requiring cataract extraction and intraocular lens (IOL) implantation.
Accurate IOL power calculation remains fundamental to achieving optimal postoperative visual outcomes.4 Despite significant advances in biometric measurements and IOL formulas, selecting appropriate IOL power for cataract patients with prior RK presents substantial challenges. The distinctive effects of radial corneal incisions induce irregular astigmatism, central corneal flattening, and the discrepancy between anterior corneal curvature and total corneal power, creating three primary complications for IOL power calculation. First, postoperative refraction demonstrates instability characterized by early hyperopic shift and diurnal variations.5,6 Second, instrument errors arise from asymmetric changes in corneal curvature between anterior and posterior surfaces.5,6 Third, formula errors occur due to estimated lens position (ELP) inaccuracies, representing another significant source of calculation error.7 These changes frequently lead to hyperopic surprises in IOL calculation for post-RK eyes.
Over the past two decades, numerous online IOL calculators have been developed to minimize formula errors, with several recent studies comparing formula accuracy.8–12 However, no consensus has emerged from these investigations, and studies from Chinese populations remain limited. Given the increasing expectations of post-RK patients undergoing cataract surgery, advances in this field are critically needed. This study compares the accuracy of eight different IOL power calculation formulas in Northern Chinese cataract patients with prior RK. The eight selected IOL formulas encompass a broad spectrum of algorithmic generations and design philosophies: 1) a traditional theoretical formula (Haigis-L); 2) modern hybrid formulas that combine optical theory with regression or AI, considered current or next-generation standards (Barrett True-K, EVO, Kane, Pearl-DGS, and Jin-AI); and 3) formulas specifically designed for eyes after refractive surgery (Shammas and CCC). This selection allows for a comprehensive evaluation across different technological paradigms.
Materials and Methods
This retrospective case series analyzed patients with a history of RK who underwent uneventful phacoemulsification cataract surgery at Tianjin Eye Hospital between January 2022 and April 2025. This study was approved by the Medical Ethics Committees of Tianjin Eye Hospital (KY-2025036) and was conducted adhering to the tenets of the Helsinki declaration. Informed consent was obtained from all patients prior to study commencement. Exclusion criteria included previous ocular surgery other than RK, severe complications during or after cataract surgery, incomplete medical records, or vision-threatening ocular diseases that could influence postoperative refraction (corneal diseases, glaucoma, uveitis, severe retinopathies, and amblyopia).
Patient demographics and surgical data were extracted from medical records, including age, sex, type and power of implanted IOL. Preoperative biometric measurements comprised axial length (AL), keratometry (K), anterior chamber depth (ACD, measured from epithelium to lens), lens thickness (LT), central corneal thickness (CCT), and white-to-white (WTW) corneal diameter, all obtained using IOL Master 700 (Carl Zeiss Meditec AG, Jena, Germany). All cataract surgeries were performed by a single experienced surgeon (XY Yuan) using a 2.8mm scleral limbal incision to avoid RK wounds. Monofocal aspheric IOLs were implanted in the capsular bag in all cases, specifically Akreos Adapt-AO (10 eyes, Bausch & Lomb, Rochester, NY, USA) or Tecnis ZCB00 (24 eyes, Johnson & Johnson Vision, Santa Ana, CA, USA). IOL power calculations utilized optimized constants from the IOL Con website (https://www.iolcon.org), in which the A constant of Akreos Adapt-AO is 118.5 and the A constant of Tecnis ZCB00 is 119.3.
Formulas
Eight IOL power calculation formulas were evaluated: Haigis-L, Shammas, Barrett True-K, Camellin Calossi Camellin (CCC), Kane, EVO, Pearl-DGS, and Jin-AI. The Haigis-L formula, developed by Dr. Wolfgang in 2008 for patients with previous refractive surgery, corrects for radius error, keratometer index error, and IOL formula error on the basis of the regular Haigis formula.13 The Shammas formula provides an alternative for IOL power calculation after myopic LASIK, particularly when refractive surgery data are unavailable.14 Both formulas are calculated online through the American Society of Cataract and Refractive Surgery website (www.ascrs.org). The Barrett True-K formula, available at https://calc.apacrs.org, predicts ELP and IOL power using AL, K, ACD, LT, and WTW, with or without previous refractive history.15 The CCC formula (https://3ccalculator.lasek.it/index.php), specifically designed by Camellin for IOL power calculation after refractive corneal surgery, incorporates K, ACD, AL, and desired refraction.16 The Kane formula (https://iolformula.com) combines theoretical optics with regression and artificial intelligence (AI) components, using AL, K, ACD, LT, CCT, and biological sex for predictions.17 The EVO formula (www.EVOiolcalculator.com) uses AL, K, and ACD as primary predictors, with LT and CCT as optional parameters.4 The Pearl-DGS Calculator (https://iolcalculator.escrs.org/), an AI formula, predicts theoretical internal lens position using AL, K, ACD, LT, CCT, and biological sex.18 The Jin-AI formula, based on Chinese eyes, incorporates AL, K, ACD, and LT as learning features.19
Methods of Comparison and Adjustments
Postoperative measurements were recorded during follow-up visits at 3–6 months, including uncorrected distance visual acuity, corrected distance visual acuity, manifest refraction, and IOL Master 700 assessments. Analysis and comparison of IOL power prediction accuracy followed guidelines recommended by Wang.20 Refractive prediction error (RPE) was calculated by subtracting the predicted spherical equivalent from the actual postoperative spherical equivalent. Negative RPE values indicated myopic outcomes, while positive values represented hyperopic results. For each formula, the arithmetic mean error (AME) and corresponding standard deviation (SD) were calculated across all patients. Absolute values of arithmetic errors yielded absolute errors, from which mean absolute error (MAE) and median absolute error (MedAE) were derived. The MAE represents the average absolute difference between actual and predicted refractive outcomes and serves as a primary outcome parameter in IOL calculation studies. Since absolute errors do not follow normal Gaussian distribution and MAE is influenced by outliers, MedAE was included to mitigate extreme value effects.21 The percentage of cases falling within ±0.25 diopters (D), ±0.50 D, ±1.00 D, and ±2.00 D was assessed to evaluate refractive outcomes for each formula.
Statistical Analysis
Descriptive statistics, including mean, SD and range, were computed using Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA). Data analysis was performed using the Social Sciences SPSS Statistics for Windows (version 26.0; IBM Corp., Armonk, NY, USA)), and visualizations were generated in GraphPad Prism (version 9.5.1; GraphPad Software, San Diego, CA, USA). Data normality was assessed using the Shapiro–Wilk test. Since most distributions deviated from normality (p < 0.05), nonparametric tests were employed. The Mann–Whitney U-test and Wilcoxon signed-rank test were applied for between-group and paired comparisons, respectively. Continuous variables were summarized as mean ± SD or median and range, as appropriate. Subgroup analysis based on RK incision number (<12, =12, >12) was performed. Bonferroni correction was applied for multiple comparisons. Statistical significance was defined as a two-sided p-value <0.05.
Results
A total of 34 eyes from 21 patients were analyzed in this retrospective study. The cohort had a mean age of 58.56 ± 5.93 years, with 11 of 21 patients being female. Among the 34 eyes examined, 10 eyes (29.4%) presented fewer than 12 RK incisions, 17 eyes (50.0%) had exactly 12 RK incisions, and 7 eyes (20.6%) demonstrated more than 12 RK incisions. Additional demographic and biometric characteristics are presented in Table 1.
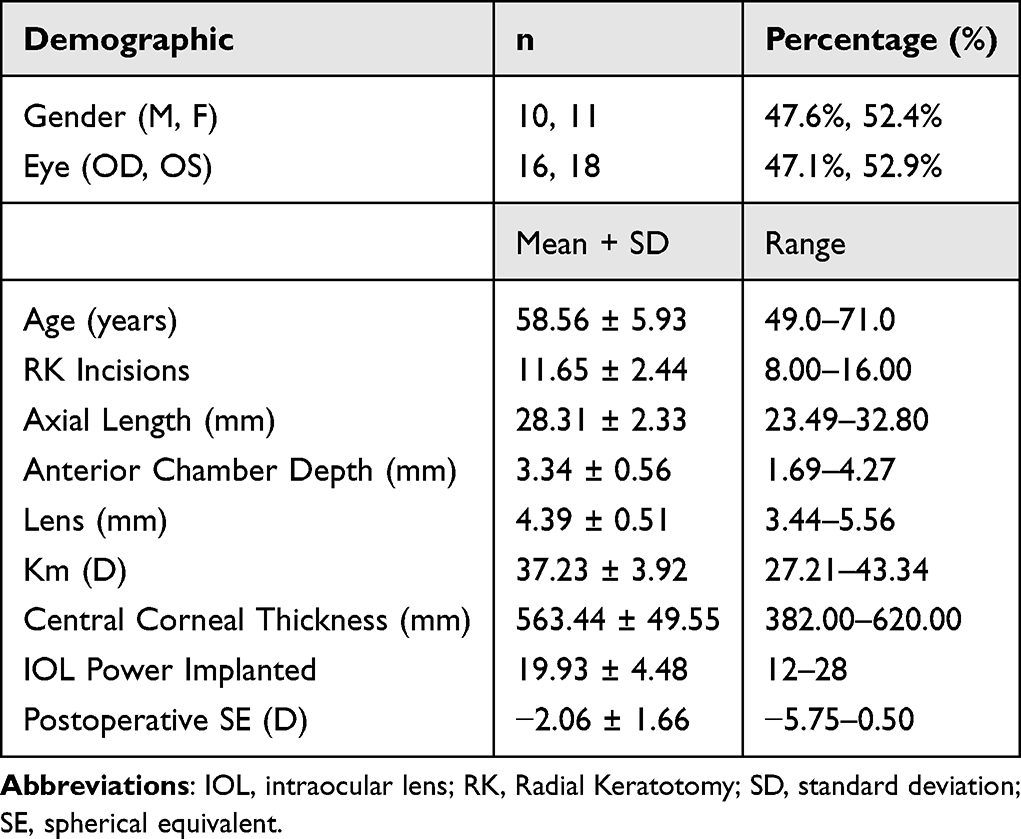 |
Table 1 Demographic and Ocular Characteristics of the Study Population |
Table 2 presents the AME for all eight formulas. The Kane formula exhibited the highest myopic mean error (−1.04D), whereas Shammas achieved the most hyperopic outcomes (0.82D). The Kane, Pearl-DGS, CCC, Barrett True-K, and EVO formulas produced myopic arithmetic mean errors, while the remaining formulas generated hyperopic arithmetic mean errors (Figure 1A). Notably, Barrett True-K and EVO demonstrated arithmetic mean errors within 0.1 D from emmetropia.
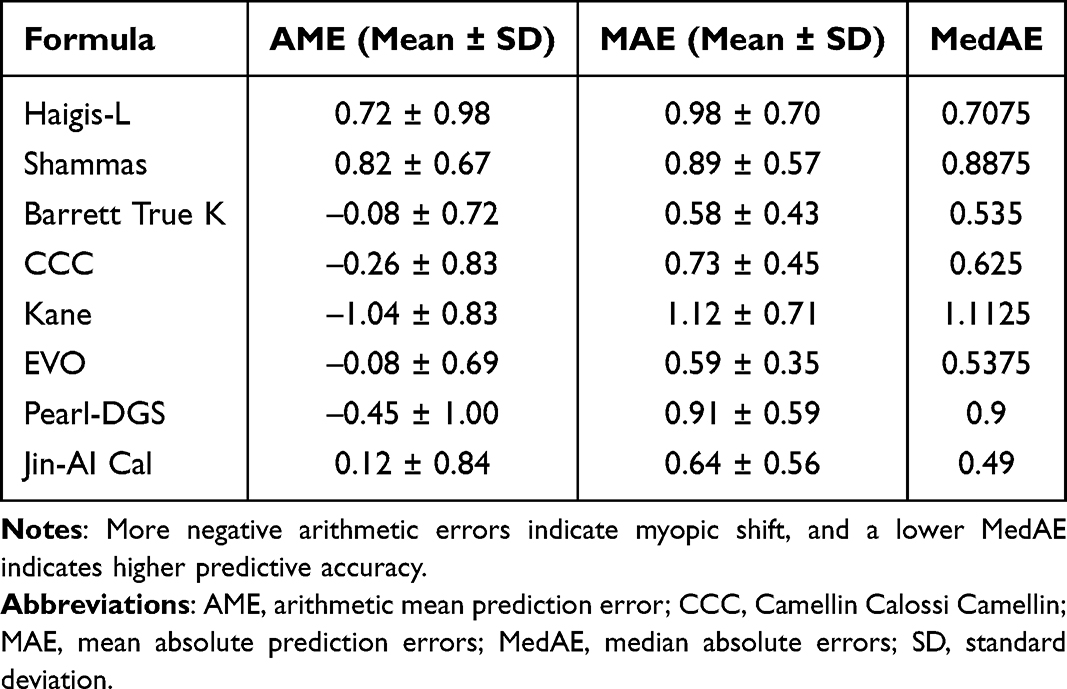 |
Table 2 IOL Prediction Error for Each Formula in Post-RK Eyes |
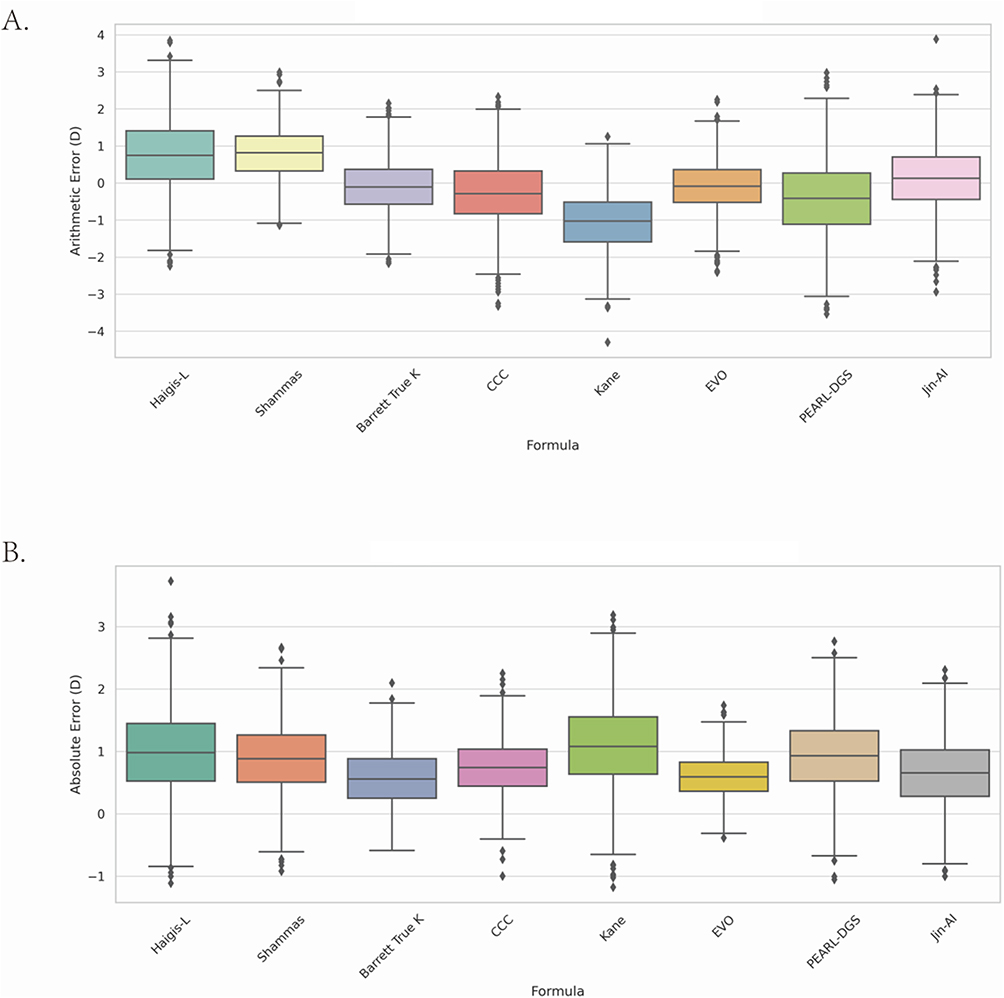 |
Figure 1 (A) This simulated boxplot visualizes arithmetic refractive prediction errors for 8 IOL formulas, reconstructed from mean ± SD data. Each box represents the interquartile range (IQR), and dots represent outliers. Positive values indicate a myopic prediction bias, while negative values reflect a hyperopic shift. (B) Boxplot showing the distribution of absolute refractive prediction errors for 8 IOL power calculation formulas in eyes with prior RK. The horizontal line inside each box indicates the median absolute error (MedAE). A lower and more compact distribution suggests better predictive performance. |
The formula rankings of MAE from lowest to highest (Table 2) were Barrett True-K (0.58D), EVO (0.59D), Jin-AI (0.64D), CCC (0.73D), Shammas (0.89D), Pearl-DGS (0.91D), Haigis-L (0.98D), and Kane (1.12D). Figure 1B displays box and whisker plots of prediction errors for each formula, illustrating the central tendency and variability of prediction bias in post-RK eyes. Statistically significant differences in MAE were observed between multiple formula pairs: Haigis-L versus Shammas (P=0.047), Haigis-L versus Barrett True-K (P=0.08), Haigis-L versus CCC (P=0.013), Haigis-L versus EVO (P=0.001), Haigis-L versus Jin-AI (P=0.001), Barrett True-K versus Pearl-DGS (P=0.045), Kane versus EVO (P=0.01), Kane versus Jin-AI (P=0.01), EVO versus Pearl-DGS (P=0.01), and Jin-AI versus Pearl-DGS (P=0.004). No additional significant differences were identified (Figure 2). Regarding MedAE, the Jin-AI formula achieved the lowest value (0.49 D), followed by Barrett True-K (0.535 D) and EVO (0.5375 D).
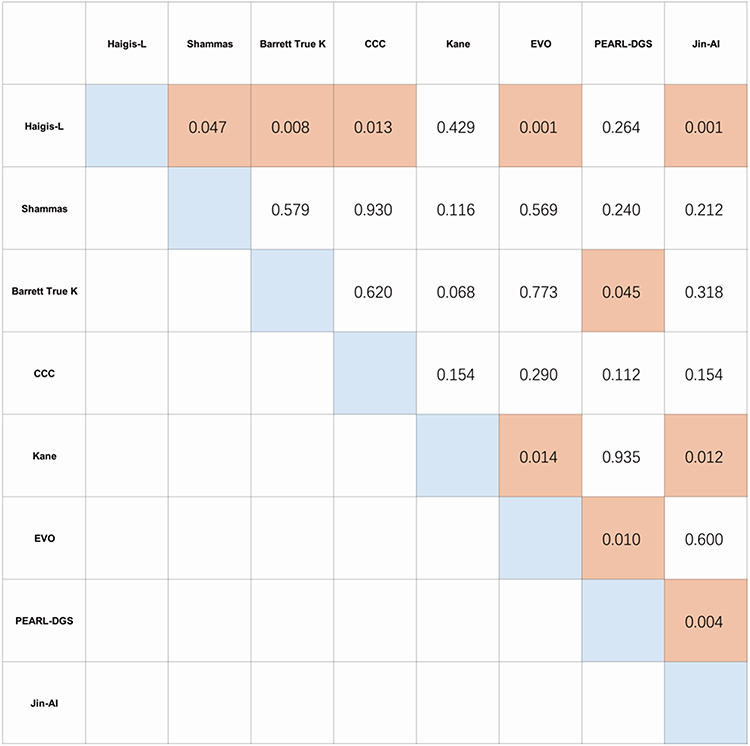 |
Figure 2 A 1:1 statistical comparison of each formula in mean absolute error. Values in gray-shaded boxes indicate statistical significance. |
Prediction accuracy assessment involved calculating the cumulative proportion of eyes achieving RPE within ±0.25 D, ±0.50 D, ±0.75 D, ±1.0 D, and ±2.0 D for each formula (Table 3). The percentage of eyes with RPE within ±0.50 D ranged from 33.5% (Kane) to 57.1% (Jin-AI). Barrett True-K and EVO formulas demonstrated comparable accuracy, with 54.1% of eyes achieving outcomes within ±0.50 D. These metrics are presented as line charts (Figure 3A) and stacked bar charts (Figure 3B). Barrett True-K, EVO, and Jin-AI demonstrated superior accuracy, particularly within the ±0.50 D and ±1.00 D ranges.
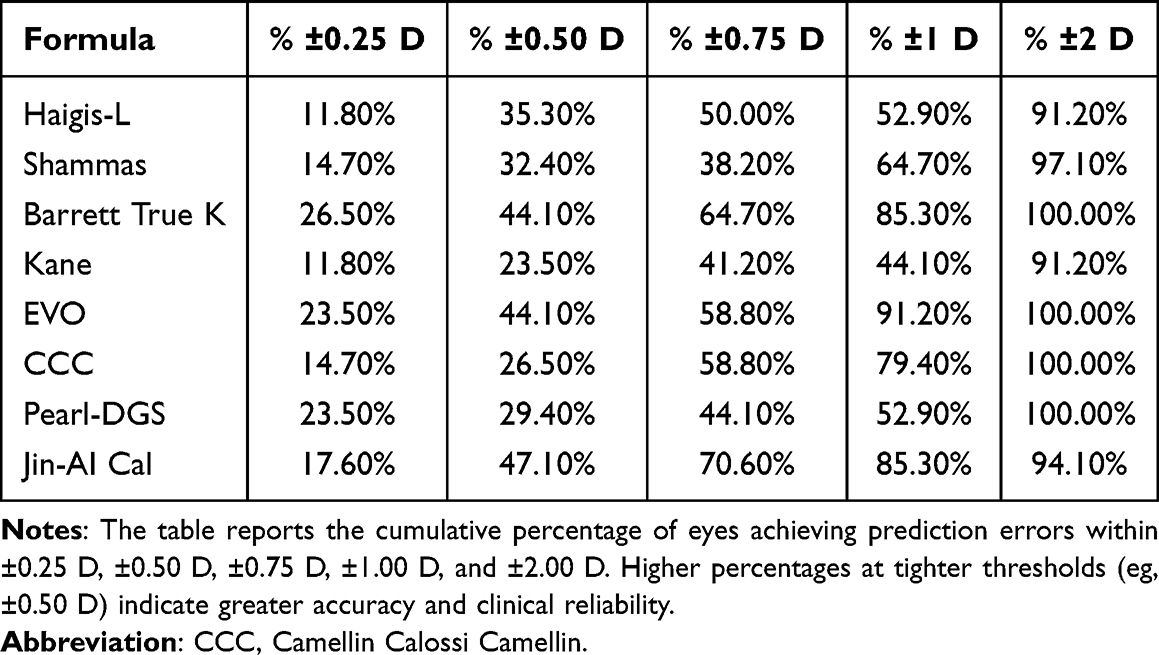 |
Table 3 Percentage of Eyes within Prediction Error Thresholds for Each IOL Formula |
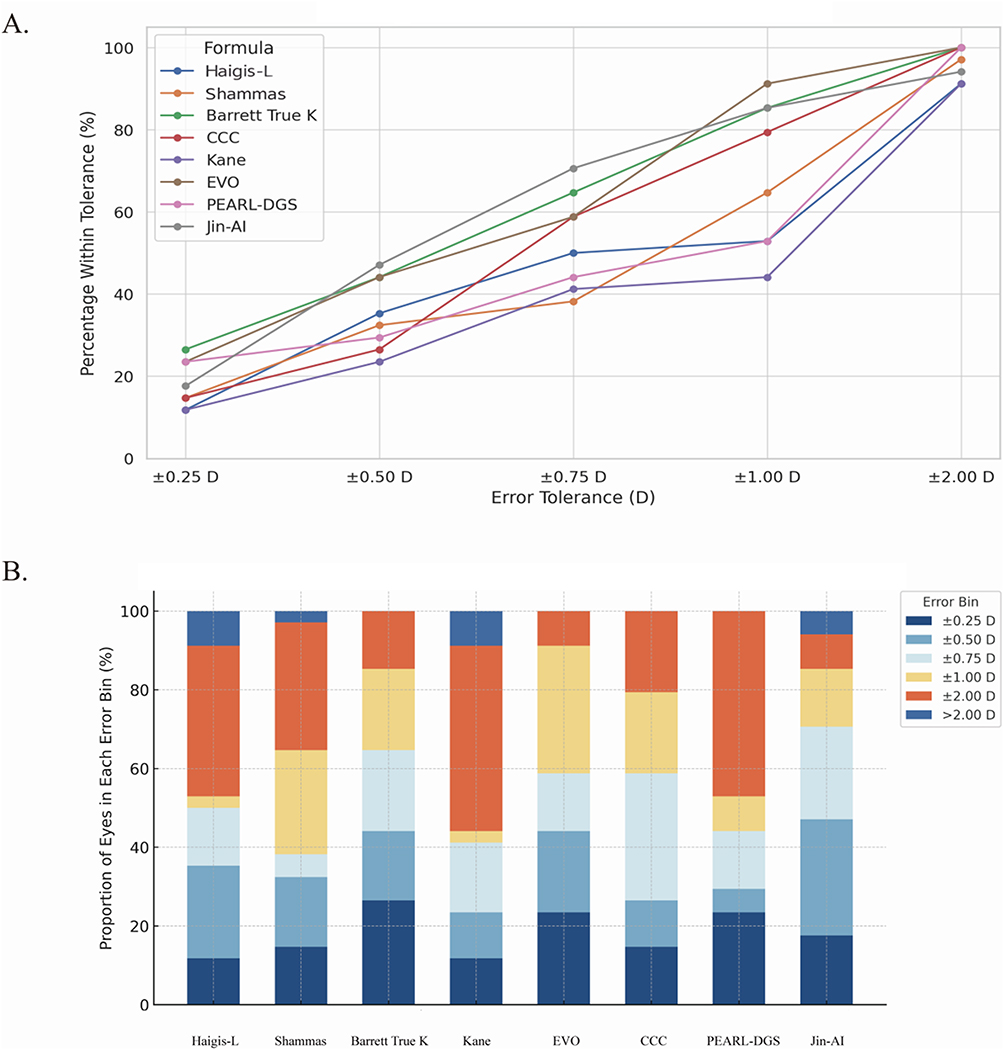 |
Figure 3 (A) Prediction Accuracy of IOL Formulas at Different Refractive Thresholds. Line chart showing the percentage of eyes within specific refractive prediction error thresholds (±0.25 D to ±2.00 D) for 8 IOL power calculation formulas in post-RK patients. Each line represents one formula. A higher curve across tighter thresholds indicates better prediction accuracy. (B) Stacked bar chart illustrating the distribution of refractive prediction errors across six error bins (±0.25 D, ±0.50 D, ±0.75 D, ±1.00 D, ±2.00 D, and >2.00 D) for 8 IOL power calculation formulas in post-RK eyes. Each bar represents the percentage of eyes falling within each prediction error range, with the sum of all bins equal to 100% for each formula. The chart highlights differences in accuracy and extreme outlier rates across formulas. Formulas with taller bars in the lower error bins (eg, Barrett True K, EVO, Jin-AI) demonstrate greater precision, while those with a substantial portion in the >2.00 D bin. |
Subgroup analysis was conducted based on RK incision number, stratifying the cohort into three groups: fewer than 12 incisions, exactly 12 incisions, and more than 12 incisions. Table 4 demonstrates the influence of RK incision number on MAE for each formula. Formulas including Haigis-L and Pearl-DGS exhibited significantly higher prediction errors in eyes with more than 12 incisions (Figure 4).
 |
Table 4 Influence of RK Incision Number on Mean Absolute Error for Each Formula |
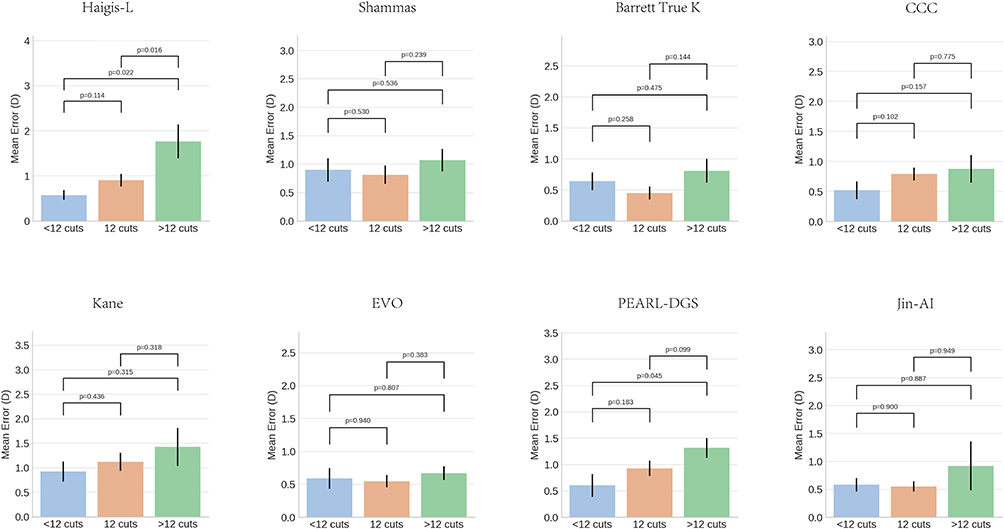 |
Figure 4 Comparison of Mean Absolute Refractive Prediction Errors Among Different RK Incision Groups for Each IOL Formula. Bar charts illustrate the mean absolute prediction errors (Mean ± SD) of each IOL calculation formula, stratified by RK incision number: <12, =12, and >12 cuts. Statistical significance between groups was assessed using the Mann–Whitney U-test, and p-values are shown above the comparisons. Formulas such as Haigis-L and Pearl-DGS demonstrated significantly higher prediction errors in eyes with >12 incisions. |
Discussion
Accurate IOL power calculation represents a fundamental requirement for successful cataract surgery and optimal visual outcomes.22 Despite significant advances in tomographic devices and IOL formulas, achieving appropriate IOL power in patients with prior RK surgery remains a substantial challenge for ophthalmologists worldwide. This study evaluated the predictive accuracy of eight different IOL power calculation formulas in post-RK Chinese eyes. To our knowledge, this represents the first investigation to incorporate the Jin-AI formula, a novel AI-powered formula based on Chinese eyes, when assessing the accuracy of traditional and contemporary IOL power calculation formulas in Chinese cataract patients with prior RK.
The percentage of patients achieving RPE within ±0.50 D holds particular clinical significance. A recent multicenter study from China evaluated eight formulas in 1443 eyes of virgin cataract patients and demonstrated that the percentage of eyes with RPE within ±0.50 D ranged from 73.6% to 84.9%.19 However, formula accuracy declined substantially in cataract patients with prior RK. In our study, the Jin-AI formula demonstrated the highest accuracy, achieving only 47.1% of eyes within ±0.50 D of the target refraction. Additionally, Jin-AI achieved the lowest median absolute error (0.49 D) among all eight traditional and contemporary formulas. The Jin-AI formula, initially reported by Jin, represents a hybrid AI-powered IOL calculation method trained on Chinese eyes, combining a multilayer neural network with Gaussian optical theory.19 Its operation follows a two-stage process: 1. An AI model, constructed as a neural network with three hidden layers and trained using the adaptive moment estimation optimizer on a dataset of Chinese eyes, predicts a patient-specific ELP; 2. This predicted ELP is then input into a standard thin-lens vergence calculation (Gaussian optics) to derive the final IOL power recommendation.19 This formula provides comparable accuracy to newer IOL formulas while demonstrating superior performance compared to third-generation formulas. Their results are in good agreement with our data. Given that current widely-used IOL formulas are based on Caucasian eye data, significant anatomical differences exist between Chinese and Caucasian populations. Jin23 and Wang24 observed that Chinese populations demonstrate significantly lower corneal keratometric index and shallower ACD than the Caucasians. Steeper horizontal keratometry and longer AL in Chinese were also reported compared to Caucasian eyes.25,26 These biometric parameter disparities induce clinically significant variations in IOL power calculation outcomes, necessitating ethnic-specific optimization. The Jin-AI formula presents a promising option for IOL power calculation in Chinese eyes.
In our study, Barrett True-K achieved an impressive MedAE of 0.535 D, the lowest MAE (0.58 D), and the highest percentage of eyes (26.5%) with RPE within ±0.25 D among the eight formulas in cataract patients with prior RK, demonstrating superior accuracy. Several studies support these findings. Curado27 analyzed 52 eyes from 34 patients with cataract and prior RK, investigating the predictive accuracy of seven IOL power methods. They demonstrated that Barrett True-K (MedAE = 0.34 D) achieved a high level of accuracy compared to Holladay 2 (MedAE = 0.44 D), Hoffer Q (MedAE = 0.51 D), ORA (MedAE = 0.53 D), Haigis (MedAE = 0.54 D), SRK/T (MedAE = 0.54 D), and Holladay 1 (MedAE = 0.57 D). Turnbull and Barrett28 reported results from 52 eyes of 34 patients with sequential RK and cataract surgery. Among methods not requiring refractive history, Barrett True-K exhibited superior performance with the lowest MedAE and highest percentage of eyes (69.2%) achieving refractive prediction error within ±0.50 D when compared to Double-K Holladay 1, Potvin-Hill, Haigis, and Haigis with −0.50 D offset. A similar Chinese study10 comparing three formulas (Barrett True-K, Holladay 1 Double-K, Haigis) demonstrated that Barrett True-K achieved the lowest MedAE and highest percentage of eyes within 0.5 D (0.62 D and 46.8%, respectively). However, several studies report divergent findings.29,30 Guo29 reviewed 27 cataract patients after RK and indicated that Barrett True-K demonstrated the largest median absolute error (0.670 D), followed by Kane (0.585 D) and VRF formula (0.580 D), which differed significantly from our results. This discrepancy likely reflects differences in ocular biometric parameters, postoperative follow-up timing, and manifest refraction measurement protocols.
The EVO formula demonstrated comparable accuracy to Barrett True-K in our study. This formula achieved a MAE of 0.59 D with the lowest SD (0.35 D) and highest percentage of eyes (91.2%) achieving refractive prediction error within ± 1.0 D among the eight formulas, indicating high consistency and reliability of this method. The EVO formula maintains validated performance across diverse complex ocular conditions in clinical practice. Maroun31 demonstrated that EVO achieved the lowest MAE and higher percentage of predictions within ±0.50 D for eyes with AL exceeding 26.0 mm compared to Hoffer Q, Holladay 1, Haigis, Barrett Universal II, Kane, Ladas Super formula, and Hill-RBF 3.0. For short eyes (AL ≤22.00 mm), EVO outperformed the special other formulas with which they were compared.32 Although not originally designed for post-RK eyes, EVO demonstrated comparable accuracy in cataract eyes with prior RK due to its inherent stability.11
Camellin developed the CCC formula in 2006 by empirically adjusting two variables (K and ACD) on the basis of the Binkhorst II formula.16 Although the formula was originally devised for IOL calculation following general refractive surgery and proved as a valid option for IOL power calculation in eyes with prior myopic laser vision correction,33 its application following RK remains largely unexplored. A retrospective analysis was conducted on cataract patients with a history of RK by Moshirfar11 and the results indicated CCC formula achieved 46% of eyes scoring within ± 0.50 D, 70% within ± 1 D, and 92% within ± 2 D of the target range. Our results did not entirely align with these findings, with 26.5% of eyes within ±0.50 D, 52.9% within ±1.00 D, and 100% within ±2.00 D of the target range, respectively. Further investigation of its application across different refractive surgery types is necessary to meet clinical requirements.
Increasing numbers of RK incisions proportionally induce corneal surface flattening.34 Subgroup analysis based on RK incision number demonstrated that both Haigis-L and Pearl-DGS formulas exhibited significantly higher prediction errors in eyes with more than 12 incisions. This result is dramatically surprising as the Haigis-L formula does not utilize keratometry readings to estimate ELP, which should theoretically avoid higher error caused by flatter cornea in the post RK eyes. The Pearl-DGS formula represents a thick-lens version of the Haigis formula using AI for back-calculated lens position,18 explaining its similar susceptibility to incision number with Haigis-L formula. Given the limited sample size of seven eyes with more than 12 incisions, this result lacks statistical power for definitive conclusions. Further investigation with large-scale multicenter data and larger subgroup analyses based on RK incision number would inform evidence-based IOL power calculation formula selection.
Several limitations should be acknowledged. First, the relatively uncommon occurrence of cataract patients with prior RK surgery resulted in a small sample size of 34 eyes, which may not fully represent the diverse population of post-RK cataract patients. Additional studies with larger sample sizes are needed to ensure data generalizability and validate these findings. Second, bilateral eye inclusion may introduce between-eye correlation effects. Third, several newer IOL formulas were excluded due to incomplete RK surgery data and technological incompatibility. Given constraints in device availability and efforts to minimize healthcare costs, all parameters were obtained using IOL Master 700, reflecting real clinical scenarios. Furthermore, as the Jin-AI formula shows promising results in our study, its performance in non-Chinese populations remains to be validated. Finally, postoperative follow-up intervals varied among patients due to the retrospective study design.
Conclusion
Despite extensive advances in ocular biometry devices and IOL formulas, accuracy remains concerning for cataract eyes with prior RK surgery. In this Chinese cohort, Jin-AI, Barrett True-K, and EVO formulas demonstrated clinically acceptable and comparable accuracy for IOL power calculation in cataract patients with prior RK. The Jin-AI formula, a novel AI-based formula derived from Chinese individuals, presents a promising option for post-RK IOL calculation. Its real-world accuracy requires further independent validation in larger, prospective, and multi-ethnic populations.
Acknowledgments
The authors thank all participants of this study for sharing their time and experiences.
Funding
This study was funded by Tianjin Metrology Technology Project (No.2025TJMT035) and Tianjin Key Medical Discipline Construction (TJYXZDXK-3-004A-3).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Assessment OP. Radial keratotomy for myopia. American Academy of Ophthalmology. Ophthalmology. 1993;100(7):1103–11.
2. Forstot SL. Radial Keratotomy. Int Ophthalmol Clin. 1988;28(2):116–125.
3. Fu L, Patel BC. Radial keratotomy correction. In: StatPearls. StatPearls Publishing LLC.; 2025.
4. Stopyra W, Langenbucher A, Grzybowski A. Intraocular lens power calculation formulas-a systematic review. Ophthalmol Ther. 2023;12(6):2881–2902. doi:10.1007/s40123-023-00799-6
5. Chavez S, Celikkol L, Feldman ST. Hyperopic shift and myopic regression in a patient 7 years after bilateral refractive keratotomy. J Refract Surg. 1996;12(1):160–162. doi:10.3928/1081-597x-19960101-27
6. Schanzlin DJ, Santos VR, Waring GO, et al. Diurnal change in refraction, corneal curvature, visual acuity, and intraocular pressure after radial keratotomy in the PERK Study. Ophthalmology. 1986;93(2):167–175. doi:10.1016/s0161-6420(86)33765-5
7. Hoffer KJ. Intraocular lens power calculation after previous laser refractive surgery. J Cataract Refract Surg. 2009;35(4):759–765. doi:10.1016/j.jcrs.2009.01.005
8. Dawson VJ, Patnaik JL, Ifantides C, Miller DC, Lynch AM, Christopher KL. Comparison of refractive prediction for intraoperative aberrometry and Barrett True K no history formula in cataract surgery patients with prior radial keratotomy. Acta Ophthalmol. 2021;99(6):e844–e851. doi:10.1111/aos.14688
9. Helaly HA, Elhady AM, Elnaggar OR. Accuracy of traditional and modern formulas for intraocular lens power calculation after radial keratotomy using standard keratometry. Clin Ophthalmol. 2023;17:2589–2597. doi:10.2147/opth.S417336
10. Li M, Wang JD, Zhang JS, Mao YY, Cao K, Wan XH. Comparison of the accuracy of three intraocular lens power calculation formulas in cataract patients with prior radial keratotomy. Eur J Med Res. 2023;28(1):20. doi:10.1186/s40001-023-00998-8
11. Moshirfar M, Sperry RA, Altaf AW, Stoakes IM, Hoopes PC. Predictability of existing IOL formulas after cataract surgery in patients with a previous history of radial keratotomy: a retrospective cohort study and literature review. Ophthalmol Ther. 2024;13(6):1703–1722. doi:10.1007/s40123-024-00946-7
12. Voytsekhivskyy OV. The VRF-L and VRF-GL IOL power calculation methods after radial keratotomy. Eye. 2024;38(15):2947–2954. doi:10.1038/s41433-024-03195-x
13. Haigis W. Intraocular lens calculation after refractive surgery for myopia: haigis-L formula. J Cataract Refract Surg. 2008;34(10):1658–1663. doi:10.1016/j.jcrs.2008.06.029
14. Shammas HJ, Shammas MC. No-history method of intraocular lens power calculation for cataract surgery after myopic laser in situ keratomileusis. J Cataract Refract Surg. 2007;33(1):31–36. doi:10.1016/j.jcrs.2006.08.045
15. Abulafia A, Hill WE, Koch DD, Wang L, Barrett GD. Accuracy of the Barrett True-K formula for intraocular lens power prediction after laser in situ keratomileusis or photorefractive keratectomy for myopia. J Cataract Refract Surg. 2016;42(3):363–369. doi:10.1016/j.jcrs.2015.11.039
16. Camellin M, Calossi A. A new formula for intraocular lens power calculation after refractive corneal surgery. J Refract Surg. 2006;22(2):187–199. doi:10.3928/1081-597x-20060201-18
17. Kane JX, Chang DF. Intraocular lens power formulas, biometry, and intraoperative aberrometry: a review. Ophthalmology. 2021;128(11):e94–e114. doi:10.1016/j.ophtha.2020.08.010
18. Debellemanière G, Dubois M, Gauvin M, et al. The PEARL-DGS formula: the development of an open-source machine learning-based thick IOL calculation formula. Am J Ophthalmol. 2021;232:58–69. doi:10.1016/j.ajo.2021.05.004
19. Lou W, Zhou W, Wu M, Jin H. A new intraocular lens power formula integrating an artificial intelligence-powered estimation for effective lens position based on Chinese eyes. Transl Vis Sci Technol. 2024;13(10):40. doi:10.1167/tvst.13.10.40
20. Wang L, Koch DD, Hill W, Abulafia A. Pursuing perfection in intraocular lens calculations: III. Criteria for analyzing outcomes. J Cataract Refract Surg. 2017;43(8):999–1002. doi:10.1016/j.jcrs.2017.08.003
21. Hoffer KJ, Aramberri J, Haigis W, et al. Protocols for studies of intraocular lens formula accuracy. Am J Ophthalmol. 2015;160(3):403–405.e1. doi:10.1016/j.ajo.2015.05.029
22. Stopyra W. Analysis of accuracy of twelve intraocular lens power calculation formulas for eyes with axial hyperopia. Saudi J Ophthalmol. 2023;37(2):125–130. doi:10.4103/sjopt.sjopt_64_22
23. Jin H, Auffarth GU, Guo H, Zhao P. Corneal power estimation for intraocular lens power calculation after corneal laser refractive surgery in Chinese eyes. J Cataract Refract Surg. 2012;38(10):1749–1757. doi:10.1016/j.jcrs.2012.06.048
24. Wang D, Huang G, He M, Wu L, Lin S. Comparison of anterior ocular segment biometry features and related factors among American Caucasians, American Chinese and mainland Chinese. Clin Exp Ophthalmol. 2012;40(6):542–549. doi:10.1111/j.1442-9071.2011.02746.x
25. Wang SK, Guo Y, Liao C, et al. Incidence of and factors associated with myopia and high myopia in Chinese children, based on refraction without cycloplegia. JAMA Ophthalmol. 2018;136(9):1017–1024. doi:10.1001/jamaophthalmol.2018.2658
26. Hickson-Curran S, Brennan NA, Igarashi Y, Young G. Comparative evaluation of Asian and white ocular topography. Optom Vis Sci. 2014;91(12):1396–1405. doi:10.1097/opx.0000000000000413
27. Curado SX, Hida WT, Vilar CMC, Ordones VL, Chaves MAP, Tzelikis PF. Intraoperative aberrometry versus preoperative biometry for IOL power selection after radial keratotomy: a prospective study. J Refract Surg. 2019;35(10):656–661. doi:10.3928/1081597x-20190913-01
28. Turnbull AMJ, Crawford GJ, Barrett GD. Methods for intraocular lens power calculation in cataract surgery after radial keratotomy. Ophthalmology. 2020;127(1):45–51. doi:10.1016/j.ophtha.2019.08.019
29. Guo ZX, Zheng X, Zhao P, Tian ZY, Wan XH, Li M. The accuracy of VRF intraocular lens power calculation formula in cataract patients after radial keratotomy. Int Ophthalmol. 2025;45(1):278. doi:10.1007/s10792-025-03645-9
30. Patel P, Ashena Z, Vasavada V, et al. Comparison of intraocular lens calculation methods after myopic laser-assisted in situ keratomileusis and radial keratotomy without prior refractive data. Br J Ophthalmol. 2022;106(1):47–53. doi:10.1136/bjophthalmol-2020-317681
31. Maroun A, El Shami M, Hoyek S, Antoun J. Comparison of the accuracy of nine intraocular lens power calculation formulas using partial coherence interferometry. J Fr Ophtalmol. 2023;46(4):341–347. doi:10.1016/j.jfo.2022.09.031
32. Carmona-González D, Castillo-Gómez A, Palomino-Bautista C, Romero-Domínguez M, Gutiérrez-Moreno M. Comparison of the accuracy of 11 intraocular lens power calculation formulas. Eur J Ophthalmol. 2021;31(5):2370–2376. doi:10.1177/1120672120962030
33. Zollet P, Romeo MA, Tripepi D, Vinciguerra P, Vinciguerra R. Camellin-calossi formula for intraocular lens power calculation in patients with previous myopic laser vision correction. J Refract Surg. 2024;40(3):e156–e163. doi:10.3928/1081597x-20240208-02
34. Waring GO, Lynn MJ, McDonnell PJ. Results of the prospective evaluation of radial keratotomy (PERK) study 10 years after surgery. Arch Ophthalmol. 1994;112(10):1298–1308. doi:10.1001/archopht.1994.01090220048022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Outcomes Using a Trifocal Intraocular Lens in Eyes After Previous Laser Corneal Refractive Surgery or Radial Keratotomy: 1-Year of Follow-Up
Vryghem JC, Laouani A, Mansouri M
Clinical Ophthalmology 2025, 19:3089-3102
Published Date: 31 August 2025