Back to Journals » International Medical Case Reports Journal » Volume 19
Precision Balance Rehabilitation in Progressive Multifocal Leukoencephalopathy: A Novel Case Report
Authors Jackson A ![]() , Zampieri C, Gupta M, Heinrichs KI, Elliott J
, Zampieri C, Gupta M, Heinrichs KI, Elliott J
Received 8 November 2025
Accepted for publication 6 April 2026
Published 14 May 2026 Volume 2026:19 578185
DOI https://doi.org/10.2147/IMCRJ.S578185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Adrienne Jackson,1 Cris Zampieri,1 Meera Gupta,1 Kristinn I Heinrichs,2 Joan Elliott1
1Rehabilitation Medicine Department, Clinical Center, National Institutes of Health, Bethesda, MD, USA; 2Bertec® Corporation, Columbus, OH, USA
Correspondence: Adrienne Jackson, National Institutes of Health Clinical Center, 10 Center Drive, MSC 1604, Bethesda, MD, 20892-1604, USA, Tel +1 301 4964733, Email [email protected]
Background and Purpose: Progressive Multifocal Leukoencephalopathy (PML) is a demyelinating disease of white matter, primarily affecting immunocompromised patients. PML survivors often experience disability marked by ataxia and balance deficits. Rehabilitation research for this population is limited. This case report describes the design, application, and efficacy of a balance rehabilitation program for a patient with PML.
Case Description: A 62-year-old male with a history of HIV-associated PML presented with lesions in the left occipital lobe and left cerebellum on MRI. Computerized Dynamic Posturography (CDP) revealed deficits in visual and vestibular sensory integration, limits of stability, and perturbation recovery.
Intervention: The intervention combined CDP-based training with overground and home exercise components. Nine balance training sessions were completed over 5 weeks. Sessions were tailored to the patient’s deficits and progressively adjusted for intensity and focus based on the patient’s performance.
Outcomes: Post-intervention testing demonstrated measurable improvements and reduction of risk for falling in the following outcomes: 1) Mini-Best test 23/28 (pre) increased to 27/28 (post), 2) Sensory Organization Test composite equilibrium score 29 (pre) increased to 51 (post), and 3) Limits of Stability maximal excursion improved by over 20% in the forward and left directions. The patient also reported improvements in balance-related confidence, with an Activities-specific Balance Confidence Scale score that increased from 65.6% (pre) to 69.4% (post).
Discussion: Analysis of posturography data guided the design of a personalized balance intervention integrating CDP, overground training, and home exercise. The patient’s positive response to this targeted, precision approach underscores the potential for meaningful balance improvements in individuals with PML, even in the presence of cerebellar damage.
Keywords: progressive multifocal leukoencephalopathy, postural balance, virtual reality, rehabilitation, cerebellar disorder
Introduction
Progressive Multifocal Leukoencephalopathy (PML) is a viral infection of the central nervous system, resulting in demyelination of the white matter. PML primarily affects immunocompromised patients and is often associated with human immunodeficiency virus (HIV). HIV-associated classic PML is commonly seen when Cluster of Differentiation 4 (CD4) cell counts present below 200 cells/μL.1 At the height of the AIDS pandemic, as many as 5% of people living with HIV developed PML. While often fatal without treatment, the growing prevalence of Antiretroviral Therapy (ART) has increased the 1-year survival rate for patients with HIV and PML from 10% to 50%.2
Depending on the part of the brain affected by PML, long-term survivors may present with cognitive impairments, motor deficits, sensory deficits, limb and gait ataxia, and visual symptoms including visual field deficits such as homonymous hemianopia, blurred vision, or diplopia.1,3–7 Although a handful of cases describe improvements in functional outcomes post-rehabilitation, literature surrounding specific interventions for this population remains sparse.3,4,8 When it comes to the effects of balance rehabilitation, much research has been done in neurological9 and vestibular populations10 however, we found no such studies in PML.
In PML, disruption of white matter pathways involved in sensory processing may contribute to deficits in multisensory integration that impair balance and postural control. Therefore, addressing the components of postural control may serve as a valuable rehabilitation strategy for individuals with PML. Balance deficits have a direct impact on function in an individual’s day-to-day environment.11 Technology such as computerized dynamic posturography (CDP) can precisely identify balance-related impairments that may otherwise be difficult to measure in detail using traditional balance assessments.12 The precision of CDP data combined with the use of virtual-reality affords physical therapists the opportunity to design tailored interventions for patients. CDP can be used as both an assessment and training modality and has been shown to be effective in a variety of patient groups including older adults and people with vestibular13,14 and cerebellar dysfunction.15 In PML, as seen in other cerebellar16 and demyelinating diseases,17 the consolidation of motor learning is largely dependent on high task intensity and number of repetitions. CDP enables repetitive and intensive training through its immersive virtual environment while ensuring patient safety via its harness support system.
This case study describes the use of CDP to quantify and treat subtle impairments in a patient with PML who had plateaued in terms of balance improvements following a traditional rehabilitation program. We developed and assessed the efficacy of a 5-week balance intervention utilizing CDP-based immersive virtual reality training in conjunction with overground dynamic gait training, and a home exercise program.
Case Description
The subject of this case is a 62-year-old male diagnosed with HIV in 2019. He started ART in February 2020, with a CD4 count of < 50 cells/μL (normal range: > 500 cells/μL),18 and was diagnosed with PML in January 2021 (Figure 1). An initial MRI revealed lesions in the left cerebellum and left occipital lobe. His symptoms at the time included slurred speech, hand clumsiness, changes in handwriting, unsteady gait with a history of falls, difficulty swallowing, and binocular diplopia. It should be noted that ART may further alter balance by subtly reducing the ability to detect sensory input, thereby impairing sensory feedback needed for postural control.19
 |
Figure 1 Timeline of diagnosis, disease progression, and rehabilitation interventions. The patient initially completed a traditional program consisting of in-clinic overground therapy and a home exercise program. This was followed by a precision rehabilitation program incorporating CDP. In this phase, CDP assessment results guided the intervention plan, including virtual reality-based training, overground in-clinic therapy, and the home exercise program. |
Before incorporating CDP into his treatment plan, the patient had received traditional outpatient physical therapy for several months, which focused on balance and gait training using a robotic body weight support system, progressive functional strengthening exercises, and a community-based program that included treadmill training and aquatic therapy. Over this period, he showed significant progress, improving from using a two-wheeled walker to walking independently. Despite these improvements, the patient continued to have difficulty utilizing visual-perceptual spatial processing and dual-tasking skills to navigate dynamic environments while maintaining balance.
Although he did not report any falls, the patient expressed concern that these persistent challenges were impacting his quality of life. Specifically, he reported difficulty maintaining balance while navigating his busy outdoor market workplace, particularly when walking on uneven surfaces, avoiding crowds, and carrying items. This prompted his physical therapist to explore alternative treatment approaches to further improve his postural control. To address these ongoing deficits, CDP was introduced to identify subtle impairments in postural control.
CDP assesses the sensory systems underlying balance, including the vestibular, visual, and somatosensory systems. It identifies deficits in these systems and evaluates functional responses to perturbations, such as rapid changes in support surface and the ability to shift one’s weight in multiple directions. By characterizing specific impairments, CDP can inform targeted exercise interventions to improve balance.12 As supported in the literature, CDP serves as a useful clinical tool for guiding the management of balance disorders.13–17
This case study examines the patient’s progress after CDP was added to his existing rehabilitation program. The primary goals when CDP was introduced were to enhance his confidence in his balance and improve his balance skills, particularly in the context of daily activities at home and work.
Initial Assessment
The initial balance assessment included the Mini Balance Evaluation Systems Test (Mini-BEST),20 Activities-Specific Balance Confidence Scale (ABC),21 horizontal dynamic visual acuity (hDVA), and CDP. The NeuroCom InVision software (version 8.4.0) was used for testing minimum perception time and hDVA (NeuroCom, previously Natus, INC; Clackamas, OR). CDP assessments included the Sensory Organization Test (SOT), Motor Control Test (MCT), Adaptation Test (ADT), and Limits of Stability (LOS) conducted on the Bertec Balance Advantage CDP/IVR™® (Bertec Corporation; Columbus, OH). Lower extremity muscle strength and joint range of motion were also assessed and found to be within normal limits. Before any assessments were initiated, the patient provided informed consent to participate in the case study and for the publication of details and images related to his case. The study (13-N-0017: Natural History Study of Progressive Multifocal Leukoencephalopathy) was approved by the National Institutes of Health Institutional Review Board. This case report was conducted under this approved protocol, which permits analysis and publication of de-identified participant data.
The patient scored 65.6% out of 100% on the ABC. His Mini-BEST score of 23/28 declined from his score of 27/28, 2 years prior. Declines were seen across all subscores except Reactive Postural Control, with the greatest decline being a 2-point decrease in Sensory Orientation (6/6, 2 years prior versus 4/6 at initial assessment).
The hDVA is a functional measure of visual acuity during horizontal head motion. It quantifies how much visual acuity is lost during head movements in comparison to the individual’s static visual acuity. Prior to testing hDVA, the prerequisite minimum perception time (the time that it takes for the brain to recognize the image) was assessed at 20 msec. With an average head movement at 85 degrees per second, the patient lost 0.45 logMar in the left eye and 0.67 logMar in the right eye.
The SOT quantifies the relative contributions of the somatosensory, visual, and vestibular systems in maintaining postural control. The test also analyzes the use of balance strategies and the position of the person’s center of gravity (COG). Jacobson et al provides a detailed description of the SOT12 The patient’s composite equilibrium score was 29, which is below age-matched normative values and falls below the established fall-risk threshold of 38.22 Baseline equilibrium scores for conditions 1–3 were at or near normal limits. In contrast, the patient was unable to maintain balance during conditions 4–6, which involve a sway-referenced support surface. Because the patient “fell” on each trial during conditions 4–6, vestibular and visual sensory integration scores were zero. His COG was misaligned, remaining consistently forward of neutral. Strategy analysis indicated a predominant reliance on hip strategies, especially during conditions 4–6, suggesting difficulty using ankle strategies in response to surface perturbations.
The MCT and ADT assess automatic postural control. While perturbations in the Reactive Postural Control section of the Mini-BEST are delivered manually by the physical therapist, the MCT and ADT delivers perturbations via unexpected movements of the CDP forceplate. On the MCT, his postural responses were within normal limits. However, his ADT results were abnormal.
Voluntary, goal-directed postural control was assessed using the LOS Test. During this test, the patient shifts their COG toward the edges of their cone of stability, which is represented by eight targets displayed on an immersive virtual reality screen. He had difficulty maintaining a neutral start position and controlling the translation of his COG toward the targets, particularly in the rightward and backward directions. He visibly struggled with posterior and right-side weight shifting, often unsuccessfully using the hip strategy in attempts to shift his center of gravity.
Intervention
A balance intervention was designed to target the specific deficits that were identified in the baseline assessment: impaired multisensory integration, misaligned COG, inappropriate balance strategy selection, decreased limits of stability (voluntary postural control), deficits in perturbation recovery (automatic postural control), and impaired gaze stabilization. The patient attended nine physical therapy sessions over 5 weeks. Each session consisted of balance training utilizing CDP, overground balance training, and reviewing the home exercise program.
CDP was used to train neutral COG alignment, weight shifting focused on using ankle strategy, perturbation recovery, and sensory re-weighting to optimize the use of vestibular and visual inputs. The immersive virtual environment of the CDP allows the clinician to change the scene, ranging from a blank wall to dynamic visual flow scenes. The COG cursor, target, and gridlines provide visual feedback on movement quality (Figure 2). Given the patient’s marked instability during sway-referenced SOT conditions (4–6), sway-referenced training was introduced early, as soon as the patient demonstrated the ability to identify and maintain neutral alignment. This approach aimed to improve balance when somatosensory input was unreliable. Training progression and parameters are detailed in Appendix A.
 |
Figure 2 (Left) Sway-referenced platform training with an immersive visual flow scene (low central density, medium peripheral density, high contrast) to promote sensory reweighting. Platform motion reduces somatosensory reliability, while the visual environment can be manipulated to challenge visual dependence, increasing reliance on vestibular and visual inputs. The center of gravity (COG) cursor (blue sphere) is controlled by the patient’s weight shifts. Navigable obstacles (static or dynamic) can be added to the scene. The black arc provides real-time feedback to aid in motor planning. (Right) Limits of stability (LOS) training using a customizable elliptical grid with posterior targets. After the patient establishes a neutral starting position (green circle), a “go” cue appears as the target changes from dark to light blue, prompting movement. The COG cursor (yellow cross) reflects real-time position during quiet stance and weight shifting toward the target. Performance goals are used to set and adjust grid boundaries. |
Overground training was designed to promote carryover of CDP-based improvements into functional mobility. Interventions including neuromuscular re-education, core-stability training, vestibulo-ocular reflex training, and weight shifting in static standing, were selected to address impaired postural control, gaze stability, and sensory integration observed during the baseline assessment. These activities were progressively incorporated into dynamic functional tasks such as ambulation and retrieving objects from various heights to challenge balance in real-world conditions.
The home exercise program reinforced clinic-based interventions and targeted the same underlying impairments. Exercises included sit-to-stand transfers for functional strengthening, core stabilization to support postural control, limits of stability training to improve controlled weight shifting, dual-task activities to challenge attentional demands, and metronome-paced VOR exercises to improve gaze stabilization. Exercise difficulty was progressed at each visit to align with the patient’s improving balance and sensory integration. Details of overground and home exercises are in Appendix A.
Outcomes
Mini-BEST and ABC
Improvements were seen in the total Mini-BEST score, as well as the sensory organization and anticipatory postural control subscores. The patient’s confidence in maintaining his balance during functional tasks improved, meeting one of his personal goals (Figure 3).
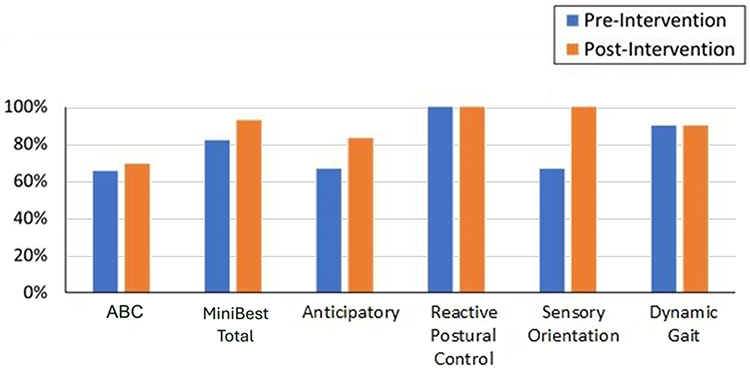 |
Figure 3 Activities-specific Balance Confidence (ABC) Scale and Mini Balance Evaluation Systems Test (Mini-BEST) total and subscale scores (anticipatory, reactive postural control, sensory orientation, and dynamic gait) at baseline and post-intervention. The ABC scale showed slight improvement. Mini-BEST scores improved primarily in the anticipatory and sensory orientation subscales, while reactive postural control and dynamic gait remained unchanged. |
Sensory Organization Test
An increase in the patient’s Mini-BEST Sensory Orientation subscore was consistent with his SOT results showing improvement in use of visual and vestibular information for postural control (Figure 4). The SOT composite equilibrium score, also shown in Figure 4, increased from 29 to 51 post-intervention, suggesting a reduction in risk of fall (ROF). He demonstrated the greatest improvement on the sway-referenced conditions (C4–C6). He completed 7/9 trials on C4–C6 without losing his balance, compared to 0/9 trials on the initial assessment. Trial times (i.e., time to fall) improved between baseline and post-intervention. During the post-intervention assessment, the patient demonstrated increased use of ankle strategies to maintain balance during C4–C6. In contrast, at baseline, he was unable to employ appropriate balance strategies and fell almost immediately following the initiation of force plate motion. Additionally, there was a slight improvement in the patient’s COG position (see Supplemental Figure 1 for additional details).
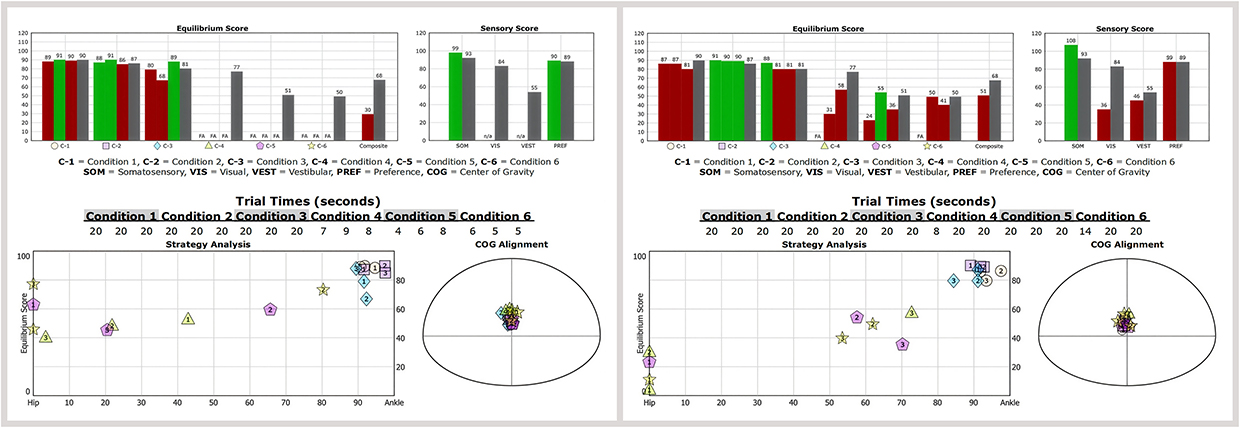 |
Figure 4 Sensory Organization Test (SOT) results at baseline (left) and post-intervention (right) with equilibrium scores for each of the six conditions (“FA” = fall), sensory score ratios, trial times, strategy analysis, and center of gravity (COG) alignment at the start of each trial. Gray bars indicate age-based normative values; green bars indicate values within norms; red bars indicate values outside norms. At baseline, balance was not maintained following force plate motion, with short trial durations. Trial times increased from baseline to post-intervention. Strategy analysis indicated greater reliance on hip strategy at baseline and increased use of ankle strategy post-intervention. COG alignment was slightly forward at baseline and improved marginally post-intervention. |
Automatic Postural Control
The patient scored 6/6 on the Reactive Postural Control section of the Mini-BEST post-intervention (Figure 3). On the MCT, post-intervention latency times showed a slight increase from 152 msec to 159 msec. The patient demonstrates a persistent weight bearing bias to the left, which was difficult to correct with coaching. This asymmetrical alignment contributed to the observed increase in composite latency times.23,24
ADT results post-intervention showed improvement for the toes-up condition (Figure 5), reflecting improved ability to centrally adapt to perturbations that occur in that direction. Figure 5 also shows a decrease in variability of raw data traces in the toes-down conditions post-intervention, which indicates more consistent control of postural sway to maintain quiet standing as the force plate is returned to the start position.
 |
Figure 5 Adaptation Test (ADT) results at baseline (left) and post-intervention (right). Gray bars represent age-adjusted normative data, green indicates scores within normal range and red represents abnormal performance. Center of gravity (COG) tracings are color-coded by trial. Post-intervention, performance in the toes up condition improved toward age-matched norms. In the toes down condition, sway energy remained elevated but declined progressively across trials (versus irregular baseline performance). Recovery responses, reflected in the COG tracings, appeared more consistent post-intervention. |
Voluntary Postural Control
LOS performance improvements were corroborated by a one-point increase in his Mini-BEST anticipatory subscore. His post-intervention COG traces shown in Figure 6 illustrate improvements in directional control and maximal excursion in several directions. Directional control increased more than 10% in five out of eight target directions and his maximum excursion increased by over 20% in the forward and left directions as reflected in more distinct traces. Deficits remained in his ability to move backward. His ability to maintain a neutral starting position improved following intervention.
 |
Figure 6 Limits of Stability (LOS) tracings and scores for eight directions at baseline (left) and post-intervention (right). Measures include reaction time (RT), movement velocity (MVL), endpoint excursion (EPE; initial movement reflecting confidence), maximum excursion (MXE; maximal safe COG displacement reflecting true stability limits), and directional control (DCL; movement accuracy toward the target). Post-intervention measures improved in the forward and lateral directions, while limitations remained for backwards movements. |
Patient-Reported Outcome Measures: Adherence and Balance Confidence
The patient attended all sessions and demonstrated high adherence to the home exercise program. His feedback guided adjustments to the exercise plan. He was highly motivated and supported by his partner.
In addition to an increase in his ABC score, his subjective remarks described greater ease in walking up inclines and stairs, and through busy areas.
“I gained strength and confidence to overcome fears walking in crowds and walking near children. The best example at home was my ability to come down stairs more naturally. I remember my cousin watching me as I descended the stairs and he said, wow, look at you!”
The patient’s partner reported that the patient had become less likely to grab on to household objects for stability, a motor behavior that was common prior to the intervention.
Discussion
The objective of this case report was to develop and assess the efficacy of a 5-week balance intervention for a 62-year-old patient with HIV-related PML. Our intervention integrated CDP-based training, overground training, and targeted home exercises. Over nine sessions, the patient showed meaningful improvements in voluntary and automatic postural responses, sensory organization, and balance confidence. Our results support the fundamental role of precision rehabilitation in optimizing function for individuals living with a disability.25
The patient’s most recent MRI showed stable lesions, notably in the left occipital lobe and left cerebellum. Deficits in processing visual cues and relaying visual information necessary for maintaining balance are consistent with occipital lobe damage.26 Cerebellar dysfunction is reflected by increased postural sway, difficulties in sensory integration, and instability in goal-directed movements.27 Given the cerebellum’s crucial role in motor learning, it was historically postulated that individuals with cerebellar damage may get limited benefit from physical therapy.28 However, more recent literature suggests the contrary.29 While research specifically examining neurological and functional deficits in PML remains limited, evidence from related neurological populations provides supportive insights into mechanisms of sensory integration and motor learning. These findings should be interpreted with caution when applied to PML, given differences in underlying pathology. Our findings align with this broader body of literature and highlight the importance of applying neuroplasticity-based, data-driven, and targeted intervention strategies.
Improvements seen in the post-intervention assessments suggest a decrease in ROF. The patient initially scored 65.6% on the ABC, which is associated with an increased ROF. Post-intervention, his score improved to 69.4%, which is above the predictive fall cut-off score of 67%.30 His SOT composite score improved from 28 points pre-intervention to 51 points post-intervention, exceeding the minimum detectable change (MDC) of 6.52 points.14 This increase in his score placed him above the 38-point threshold considered to be the cutoff for increased ROF.21 Improvements in the patient’s responses to toes-up rotational perturbations on the ADT also suggest a decrease in ROF.31 The patient’s score on the Mini-BEST, although not below the fall cut score of 16/2832 on initial assessment, increased from 23/28 to 27/28, indicating an improvement beyond the minimal important change (MIC) of 4 for Mini-BEST.33 Last, the patient’s and his partner’s subjective descriptions of the patient’s mobility and motor behaviors post-treatment further suggest a decreased ROF. The patient described greater ease in walking up inclines and through busy areas. His partner also observed that the patient became less likely to grab on to household objects for stability, a motor behavior that is commonly seen in individuals with a history of falls or poor balance.34
During the course of the intervention, deficits in the patient’s ability to maintain his balance in the immersive virtual environment of the CDP prompted assessment of his hDVA. The patient’s acuity loss (left DVA loss 0.189, right DVA loss 0.202) was greater than that of healthy older adults.35 This likely contributed to his inability to maintain his balance within the community. To address these deficits, evidenced-based vestibulo-ocular reflex (VOR) exercises were incorporated into his intervention plan.36 Unfortunately, we were unable to perform a post-intervention DVA assessment due to unforeseen circumstances.
The individualized approach to developing a successful and precise balance training program was based on assessment results. CDP identified specific postural control deficits and offered the physical therapist specific rehabilitation targets. Individuals with mild to moderate balance deficits may be able to compensate, at least partially, during conventional balance testing because of the ability of the visual system to “anchor” vertical and horizontal reference points.37 Training in the CDP allows the clinician to eliminate these anchors and better control the visual environment. CDP has been shown to be more sensitive in detecting balance deficits than traditional clinical assessments.24,38
A three-pronged training approach was utilized: CDP training with immersive virtual reality, overground functional training, and a customized home exercise program. A multimodal approach to balance training has been shown to be effective in other neurological disorders.39,40 David et al and Keshner et al highlighted the usefulness of combining forceplate and virtual reality–based interventions with functional activities.13,41 Additionally, regularly practicing motor skills with a customized home exercise program is crucial and has been consistently shown to improve outcomes.42,43 The balance training program was developed and supervised by a team of three physical therapists specializing in neurological rehabilitation. This collaborative approach led to improved problem solving through the sharing of knowledge. Although the value of intradisciplinary practice in physical therapy is rarely discussed in the literature, the benefits should be considered, particularly in complex cases.
There are barriers to replicating this method of assessment and training. The cost and training required for the use of CDP technology may limit its utilization in the clinic. Additionally, hesitancy to use new technology by both patients and clinicians can hinder integration into routine care.44 Insurance limitations on the number of physical therapy visits may be another barrier. In this case, the patient was able to show meaningful improvement after only nine visits. However, patients with cerebellar dysfunction may require longer episodes of care.45,46 Single-subject study designs such as this case inherently limit generalizability and causal inference. However, research in neurological and balance rehabilitation is challenging due to heterogeneity in patient populations, impairments, and inconsistencies in reporting training variables.47 In this context, baseline and repeated assessments in a single-subject design allow clinicians to develop targeted interventions and systematically document outcomes.48,49 Although the absence of a control condition or baseline stability phase prevents definitive attribution of observed improvements to the intervention, establishing such controls in rehabilitation settings can be challenging due to ethical concerns (eg, withholding treatment), variability in patient presentation, and the need for individualized interventions. Long-term follow-up assessments would allow evaluation of the durability of improvements; however, this was not possible due to unforeseen patient circumstances.
Conclusions
CDP identified specific balance deficits that conformed with neurological lesions in a patient with PML that would not have been evident with conventional clinical tests alone. The detailed balance assessment allowed for the development of a personalized and precise balance intervention integrating CDP, overground training, and home exercise. Over nine sessions, the patient showed meaningful improvements. Given the single-case design, these findings should be interpreted cautiously and do not establish causality. Rather, this case highlights the potential utility of a precision-based rehabilitation approach and suggests that balance improvements may be achievable in individuals with PML despite cerebellar involvement. Further research with larger, controlled studies and follow-up assessments is needed to confirm the durability and specificity of the outcomes.
Acknowledgment
The authors thank Yolanda L. Jones, NIH Library Editing Services, for manuscript editing assistance. The authors also acknowledge the contributions of Zeynep Erdemir for the design and preparation of the graphical illustrations presented in this work. This research was supported [in part] by the Intramural Research Program of the National Institutes of Health (NIH). The contributions of the NIH author(s) are considered Works of the United States Government. The findings and conclusions presented in this paper are those of the author(s) and do not necessarily reflect the views of the NIH or the US Department of Health and Human Services.
Disclosure
Dr. Jackson, Dr Zampieri, Ms. Gupta, and Dr. Elliott are employed by the NIH. Dr. Heinrichs is employed by Bertec, the company that produces the CDP/IVR™ device. Dr. Heinrichs’ role in this study was limited to providing subject matter expertise in data interpretation and program design. They did not conduct any testing or intervention and received no financial compensation for this project.
References
1. Berger JR, Pall L, Mark AS, Berger JR, Kedar S. Progressive multifocal leukoencephalopathy: recent advances in diagnosis and treatment. J Neuroophthalmol. 2015;35(3):296–12. doi:10.1097/WNO.0000000000000271
2. Lima MA, Bernal-Cano F, Clifford DB, Gandhi RT, Koralnik IJ. Clinical outcome of long-term survivors of progressive multifocal leukoencephalopathy. J Neurol Neurosurg Psychiatry. 2010;81(11):1288–1291. PMID: 20710013; PMCID: PMC3077967. doi:10.1136/jnnp.2009.179002
3. Aye SL, Triveldi Y, Bolgarina Z, et al. The prognosis of progressive multifocal leukoencephalopathy in HIV/AIDS patients undergoing highly active antiretroviral treatment: a systematic review. Cureus. 2023. doi:10.7759/cureus.45155
4. Naro A, Billeri L, Lauria P, et al. Toward improving functional recovery in AIDS-associated progressive multifocal leukoencephalopathy: a single case pilot study on a novel neuromodulation approach. Innov Clin Neurosci. 2022;19(1–3):15–18.
5. Sudhakar P, Bachman DM, Mark AS, Berger JR, Kedar S. Progressive multifocal leukoencephalopathy: recent advances and a neuro-ophthalmological review. J Neuroophthalmol. 2015;35(3):296–305. doi:10.1097/WNO.0000000000000271
6. Bernard-Valnet R, Koralnik IJ, Du Pasquier R. Advances in treatment of progressive multifocal leukoencephalopathy. Ann. Neurol. 2021;90(6):865–873. doi:10.1002/ana.26198
7. Anand P, Hotan GC, Vogel A, Venna N, Mateen FJ. Progressive multifocal leukoencephalopathy: a 25-year retrospective cohort study. Neurology. 2019;6(6):e618.
8. Moreh E, Israel S, Korem M, Meiner Z. Rehabilitation outcome of progressive multifocal leukoencephalopathy in HIV-positive patients: a report of two cases. Disabil Rehabil. 2017;39(18):1893–1896. doi:10.1080/09638288.2016.1211754
9. Lai C, Chen H, Liou T, Li W, Chen S. Exercise interventions for individuals with neurological disorders. Am J Phys Med Rehabil. 2019;98(10):921–930. doi:10.1097/PHM.0000000000001247
10. Burzynski J, Sulway S, Rutka JA. Vestibular rehabilitation: review of indications, treatments, advances, and limitations. Curr Otorhinolaryngol Rep. 2017;5(3):160–166. doi:10.1007/s40136-017-0157-1
11. Horak FB. Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age Ageing. 2006;35(2):ii7–ii11. doi:10.1093/ageing/afl077
12. Jacobson GP, Newman GW, Kartush JM. Handbook of Balance Function Testing. London: Singular Publishing Group Inc. San Diego; 1997.
13. David EA, Shahnaz N. Dynamic posturography after computerized vestibular retraining for stable unilateral vestibular deficits. Acta Oto-Laryngologica. 2023;143(5):396–401. doi:10.1080/00016489.2023.2208615
14. Grove CR, Whitney SL, Hetzel SJ, Heiderscheit BC, Pyle GM. Effect of repetitive administration of a next-generation sensory organization test in adults with and without vestibular dysfunction. Otol Neurotol. 2021;42(3):Article3. doi:10.1097/MAO.0000000000002950
15. Croarkin E, Shrader J, Shahim P, Yonter S, Toro C, Zampieri C. Rehabilitation of high-level dynamic balance skills in an individual with significant nonprogressive cerebellar atrophy: case report. ARRCT. 2025;7:100500. doi:10.1016/j.arrct.2025.100500
16. Lanza G, Casabona J, Bellomo M, et al. Update on intensive motor training in spinocerebellar ataxia: time to move a step forward? J Int Med Res. 2019;48(2):1–15.
17. García-Muñoz C, Cortes-VegaMD. Effectiveness of vestibular training for balance and dizziness rehabilitation in people with multiple sclerosis: a systematic review and meta-analysis. J Clin Med. 2020;9:1–16. doi:10.3390/jcm9020590
18. Giorgi JV, Detels R. T lymphocyte subsets and HIV: the era of HAART. J Am Med Assoc. 1989;261(7):935–939. doi:10.1001/jama.1989.03420070059031
19. Bauer LO, Ceballos NA, Shanley JD, Wolfson LI. Sensorimotor dysfunction in HIV/AIDS: effects of antiretroviral treatment and comorbid psychiatric disorders. AIDS. 2005;19(5):495–502. doi:10.1097/01.aids.0000162338.66180.0b
20. Franchignoni F, Horak F, Godi M, Nardone A, Giordano A. Using psychometric techniques to improve the balance evaluation systems test: the mini-BESTest. J Rehabil Med. 2010;42(4):323–331. PMID: 20461334; PMCID: PMC3228839. doi:10.2340/16501977-0537
21. Powell LE, Myers AM. The Activities-specific Balance Confidence (ABC) scale. J Gerontol Series A. 1995;50A(1):M28–M34. doi:10.1093/gerona/50A.1.M28
22. Whitney SL, Marchetti GF, Schade AI. The relationship between falls history and computerized dynamic posturography in persons with balance and vestibular disorders. Arch Phys Med Rehabil. 2006;87(3):402–407. doi:10.1016/j.apmr.2005.11.002
23. Kolářová B, Janura M, Svoboda Z, Kolář P, Tečová D, Elfmark M. Postural control strategies and balance-related factors in individuals with traumatic transtibial amputations. Sensors. 2021;21(21):7284. doi:10.3390/s21217284
24. Harro CC, Kelch A, Hargis C, DeWitt A. Comparing balance performance on force platform measures in individuals with parkinson’s disease and healthy adults. Parkinson’s Dis. 2018;2018:1–12. doi:10.1155/2018/6142579
25. French MA, Roemmich RT, Daley K, et al. Precision rehabilitation: optimizing function, adding value to health care. Arch Phys Med Rehabil. 2022;103(6):1233–1239. doi:10.1016/j.apmr.2022.01.154
26. Rehman A, Al Khalili Y. Neuroanatomy, occipital lobe. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
27. Marsden JF. Cerebellar ataxia. Handbook Clin Neurol. 2018;159:261–281. doi:10.1016/B978-0-444-63916-5.00017-3
28. Horak FB, Diener HC. Cerebellar control of postural scaling and central set in stance. J Neurophysiol. 1994;72(2):479–493. doi:10.1152/jn.1994.72.2.479
29. Keller JL, Bastian AJ. A home balance exercise program improves walking in people with cerebellar ataxia. Neurorehabil Neural Repair. 2014;28(8):770–778. doi:10.1177/1545968314522350
30. Lajoie Y, Gallagher SP. Predicting falls within the elderly community: comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparing fallers and non-fallers. Arch Gerontol Geriatr. 2004;38(1):11–26. doi:10.1016/s0167-4943(03)00082-7
31. Wolfson L, Whipple R, Derby CA, et al. A dynamic posturography study of balance in healthy elderly. Neurology. 1992;42(11):2069. doi:10.1212/wnl.42.11.2069
32. Yingyongyudha A, Saengsirisuwan V, Panichaporn W, Boonsinsukh R. The Mini-Balance Evaluation Systems Test (Mini-BESTest) demonstrates higher accuracy in identifying older adult participants with history of falls than do the BESTest, Berg Balance Scale, or timed up and go test. J Geriatric PhysTher. 2016;39(2):64–70. doi:10.1519/jpt.0000000000000050
33. Godi M, Franchignoni F, Caligari M, Giordano A, Turcato AM, Nardone A. Comparison of reliability, validity, and responsiveness of the mini-BESTest and Berg Balance Scale in patients with balance disorders. Physical Ther. 2013;93(2):158–167. doi:10.2522/ptj.20120171
34. Northridge ME, Nevitt MC, Kelsey JL, Link B. Home hazards and falls in the elderly: the role of health and functional status. Am J Public Health. 1995;85(4):509–515. doi:10.2105/ajph.85.4.509
35. Riska KM, Hall CD. Reliability and Normative Data for the Dynamic Visual Acuity Test for Vestibular Screening. Otol Neurotol. 2016;37(5):545–552. doi:10.1097/mao.0000000000001014
36. Tramontano M, Russo V, Spitoni GF, et al. Efficacy of vestibular rehabilitation in patients with neurologic disorders: a systematic review. Arch Phys Med Rehabil. 2021;102(7):1379–1389. doi:10.1016/j.apmr.2021.03.011
37. Basford JR, Chou LS, Kaufman KR, et al. An assessment of gait and balance deficits after traumatic brain injury. Arch Phys Med Rehabil. 2003;84(3):343–349. doi:10.1053/apmr.2003.50034
38. Melillo F, Di Sapio A, Martire S, Malentacchi M, Matta M, Bertolotto A. Computerized posturography is more sensitive than clinical Romberg Test in detecting postural control impairment in minimally impaired Multiple Sclerosis patients. Mult Scler Relat Disord. 2017;14:51–55. doi:10.1016/j.msard.2017.03.008
39. Brichetto G, Piccardo E, Pedullà L, Battaglia MA, Tacchino A. Tailored balance exercises on people with multiple sclerosis: a pilot randomized, controlled study. Mult Scler J. 2015;21(8):1055–1063. doi:10.1177/1352458514557985
40. Ahmed MM, Mosalem DM, Alfeeli AK, Baqer AB, Soliman DY. Relationship between gait parameters and postural stability in early and late Parkinson’s Disease and visual feedback-based balance training effects. Open Access Maced J Med Sci. 2017;5(2):207–214. PMID: 28507630; PMCID: PMC5420776. doi:10.3889/oamjms.2017.051
41. Keshner EA, Lamontagne A. The untapped potential of virtual reality in rehabilitation of balance and gait in neurological disorders. Front Virtual Reality. 2021;2. doi:10.3389/frvir.2021.641650
42. Shumway-Cook A, Gruber W, Baldwin M, Liao S. The effect of multidimensional exercises on balance, mobility, and fall risk in community-dwelling older adults. Physical Ther. 1997;77(1):46–57. doi:10.1093/ptj/77.1.46
43. Costa SN, Ferreira LHB, Bento PCB. Effects of home-based exercise programs on mobility, muscle strength, balance, and gait in community-Dwelling older adults: a systematic review and meta-analysis. J Aging Phys Act. 2023;31(4):693–704. PMID: 36623512. doi:10.1123/japa.2022-0221
44. Hatami Kaleshtari M, Ciobanu I, Lucian Seiciu P, Georgiana Marin A, Berteanu M. Towards a model of rehabilitation technology acceptance and usability. Int J Soc Sci Hum. 2016;6(8):612–616. doi:10.7763/ijssh.2016.v6.720
45. Miyai I, Ito M, Hattori N, et al. Cerebellar ataxia rehabilitation trial in degenerative cerebellar diseases. Neurorehabil Neural Repair. 2012;26(5):515–522. doi:10.1177/1545968311425918
46. Ilg W, Synofzik M, Brotz D, Burkard S, Giese MA, Schols L. Intensive coordinative training improves motor performance in degenerative cerebellar disease. Neurology. 2009;73(22):1823–1830. doi:10.1212/WNL.0b013e3181c33adf
47. Hoppes CW, Anson ER, Carender WJ, et al. Type, dose, and outcomes of physical therapy interventions for unilateral peripheral vestibular hypofunction: protocol for a systematic review. Syst Rev. 2023;12(1):164. doi:10.1186/s13643-023-02328-9
48. Lin DJ, Stein J. Stepping closer to precision rehabilitation. JAMA Neurol. 2023;80(4):339–341. doi:10.1001/jamaneurol.2023.0044
49. Willingham TB, Stowell J, Collier G, Backus D. Leveraging emerging technologies to expand accessibility and improve precision in rehabilitation and exercise for people with disabilities. Int J Environ Res Public Health. 2024;21(1):79. doi:10.3390/ijerph21010079
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.