Back to Journals » Clinical Ophthalmology » Volume 20
Precise Epithelium Removal for Ectatic Corneas Technique in Corneal Collagen Crosslinking (PERFECT-CXL): Technique Description and Clinical Outcomes
Authors Desilets J ![]() , Agarwal K, Hatch KM
, Agarwal K, Hatch KM
Received 26 January 2026
Accepted for publication 8 July 2026
Published 15 July 2026 Volume 2026:20 595025
DOI https://doi.org/10.2147/OPTH.S595025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Jeffrey Desilets,1 Kanika Agarwal,1 Kathryn M Hatch2
1Comprehensive Ophthalmology Service, Massachusetts Eye and Ear, Boston, MA, USA; 2Cornea and Refractive Surgery Service, Massachusetts Eye and Ear, Boston, MA, USA
Correspondence: Jeffrey Desilets, Massachusetts Eye and Ear, 110 Hartwell Ave, Lexington, MA, 02421, USA, Email [email protected]
Purpose: To describe clinical outcomes of a hybrid collagen crosslinking technique, Precise Epithelium Removal for Ectatic Corneas Technique Collagen Crosslinking (PERFECT-CXL) using tomography-guided hybrid partial central epithelium removal with peripheral epithelial disruption in keratoconus.
Patients and Methods: A retrospective chart review of all previously untreated eyes that underwent PERFECT-CXL for keratoconus (KCN) by one surgeon from June 2018 to January 2023 at a single, tertiary care center. PERFECT-CXL utilizes a two-stage epithelial approach involving diffuse, across the entire cornea, roughening with an Ultracell LASIK Disc in order to create epithelial microerosions, followed by 45 minutes of loading with hypo-osmolar 0.146% riboflavin. After loading, epithelial debridement of an approximately 4– 5mm zone is performed, centered over the cone, based on Pentacam tomographic localization, and the cornea is treated with pulsed UV-A irradiation. This hybrid method aims to optimize oxygen availability and targeted biomechanical stabilization while also aiming to promote faster visual recovery and an earlier return to contact lens wear. In this retrospective chart review, 362 eyes underwent PERFECT-CXL, of which 150 were previously untreated non-contact lens wearing keratoconic eyes. Outcomes measured at 6 months, 1, 2 and 3 years post-operatively included best spectacle-corrected visual acuity (BSCVA), maximum keratometry (Kmax), and treatment-associated complications.
Results: At six months, one, two, and three years post-op, BSCVA was stable in 97.5% (n = 120), 95.7% (n = 93), 94.2% (n = 69), and 94.9% (n = 39) of eyes, respectively. At one, two, and three years post-op, 80.3% (n = 117), 88.2% (n = 93), 84.1% (n = 69), and 84.6% (n = 39) of eyes experienced stabilization in Kmax, respectively. Of patients not lost to follow-up, 1.3% (2/150) demonstrated progression requiring retreatment within three years. There were no instances of treatment-associated complications.
Conclusion: Preliminary, retrospective results suggest that PERFECT-CXL can be a safe and effective technique in halting progression of KCN and can be utilized in various stages of keratoconus.
Keywords: corneal ectasia, keratoconus, corneal collagen crosslinking, Dresden protocol, hybrid partial epithelium-off with peripheral disruption crosslinking technique
Introduction
Corneal crosslinking (CXL) is a minimally invasive procedure that halts or slows progression of corneal ectatic disorders, including keratoconus (KCN) and post-refractive ectasia, by improving the biomechanical properties of the corneal stroma.1–3 In CXL, the cornea is photosensitized with riboflavin and irradiated using ultraviolet A (UV-A) light (370 nm), together generating excited riboflavin triplets and reactive oxygen species. This reaction mediates cross-linking between collagen fibers in the stroma, ultimately leading to increased mechanical rigidity of the ectatic cornea.2–4
The Dresden protocol, involving an epithelium-off approach, was the first technique to be described in 2003 by Wollensak et al and was the only approved technique by the Federal Drug Administration (FDA) in the United States until Epioxa epithelium-on CXL in October 2025.5 In the Dresden technique, debridement of a central 7–9 mm zone of epithelium is first performed, followed by stromal loading of 0.1% riboflavin-5-phosphate in 20% dextran T-500 every 2 min for 30 min. UV-A is then administered at an irradiance of 3.0 mW/cm2 for 30 minutes to achieve a total surface dose of 5.4 J/cm2, with additional riboflavin applied every 5 min during irradiation.
Since the introduction of epithelium-off CXL, various modifications have been tested to maximize treatment efficacy, safety, comfort and healing time.2,3 Modifications to the Dresden technique aim to address issues associated with epithelium removal, such as patient discomfort, poor epithelial healing, persistent corneal haze, and infection.2 Additionally, contact lens-dependent patients may experience prolonged periods of time before being able to resume use or undergo refitting. Nevertheless, epithelial removal may be integral to the efficacy of the Dresden protocol technique because an intact epithelium impacts stromal riboflavin absorption and this absorption depends on the formulation, UV-A penetration, and oxygen availability.3,6 Although superior in terms of patient comfort with reduced risk or complications, some studies suggest that epithelium-on or transepithelial CXL (t-CXL) has been less effective at halting progression of ectasia when compared to epi-off crosslinking.7–10 Epithelium-on techniques vary and lack an established standardized approach. Because of this, the efficacy can vary significantly between study designs. Moreover, various modifications to t-CXL, including use of iontophoresis systems and chemical enhancers (eg, ethylenediaminetetraacetic acid (EDTA), benzalkonium chloride (BAK), and trometamol) have also been attempted with mixed success.11–13 Notwithstanding, t-CXL still has the strong advantage of faster recovery, including return to contact lens wear within one week if desired. t-CXL requires a shorter course of postoperative steroids due to reduced risk of visually significant stromal haze because of the technique and quicker recovery.14 Proposed techniques of partial de-epithelialization attempt to garner the advantages and avoid the concerns of both epi-on and epi-off crosslinking.15–19
In view of 1) maintaining effectiveness of crosslinking and 2) minimizing risks associated with epithelium removal employed in the Dresden technique with quick return to contact lens use when desired, we describe a hybrid epithelium-off CXL protocol, termed Precise Epithelium Removal for Ectatic Corneas Technique-CXL (PERFECT-CXL). This hybrid technique involves several modifications to the Dresden technique—including a tomography-guided, partial central de-epithelization with peripheral epithelial disruption and modified UV light treatment—with the goal of optimizing safety and healing time with biomechanical efficacy.
Materials and Methods
Surgical Technique
PERFECT-CXL is an off-label hybrid partial central epithelium-off CXL technique with peripheral epithelial disruption (Table 1). After anesthesia, the epithelium is roughened at the slit lamp to create dense punctate epithelial erosions (PEEs) (Figure 1). A sponge is then placed on the cornea and is loaded with one drop of non-viscous riboflavin 0.146% (GLAUKOS, Aliso Viejo, CA, USA) every minute and swirled every 5 minutes for a total load time of 45 minutes (Figure 2). The patient is then examined at the slit lamp to ensure an even limbus-to-limbus load. Additional loading for approximately 5 min is sometimes required and performed if the loading was not even or there is insufficient riboflavin in the stroma. After ensuring limbus-to-limbus uniform loading at the slit lamp, the ultrasound pachymetry is measured. If the pachymetry is less than 400 microns, nonviscous riboflavin is applied for every 30 seconds for 2–3 minutes until the pachymetry is greater than 400 microns, as a means of intraoperative pachymetric adjustment. Epithelium removal is then guided by the patient’s tomography (Oculus Pentacam); a 4–5 mm zone of epithelium centered at the cone is removed using an Epi-Clear™ (Orca Surgical, Israel) Epi-Bowman Keratectomy (EBK) or 57 blade while at the slit-lamp (Figure 3). If the pachymetry is greater than 500 microns in eyes that were preoperatively under 500 (suggesting edema during the loading process), application of alternating viscous 0.1% and non-viscous riboflavin every 20 seconds for 3 minutes is performed (after epithelium removal) until the pachymetry is less than 500 but greater than 400 microns, as a continued means of intraoperative pachymetric adjustment. Repeat ultrasound pachymetry is measured and is confirmed to be between 400–500 microns. In this way, the viscous 0.1% riboflavin in dextran is reserved as a deturgescent agent for eyes exceeding the 500µm threshold during loading. Afterwards, the patient is then placed under the KXL system (GLAUKOS) and the cornea is irradiated with UV-A light for a total irradiation time of 15 minutes, delivered over a 30-minute period using 15-second on/off pulses, resulting in a total fluence of 2.7 J/cm2. The light is manually blocked during the 15 second intervals with a tegaderm dressing on its opaque backing during the 30 min UVA treatment. One drop of non-viscous riboflavin 0.146% is administered at 10 and 20 minutes. One drop of artificial tear is given every 2.5 minutes except at minute 10 and 20 when riboflavin is applied instead. After completion of UV-A treatment, one drop of prednisolone acetate, ofloxacin, and diclofenac are administered, and a bandage contact lens is applied.
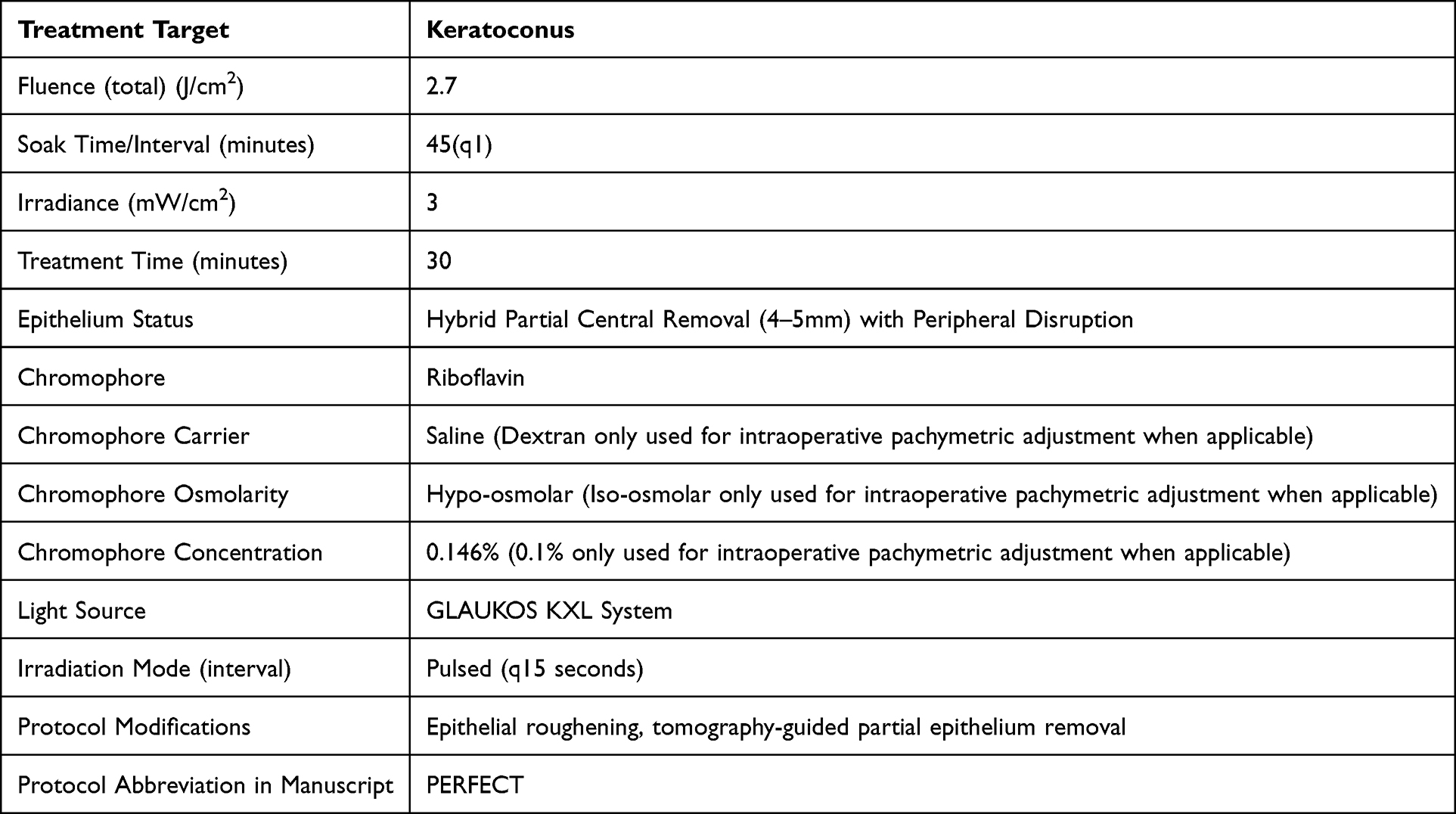 |
Table 1 PERFECT Corneal Crosslinking Methodology |
 |
Figure 1 Roughening of the Epithelium to Induce Punctate Epithelial Erosions. |
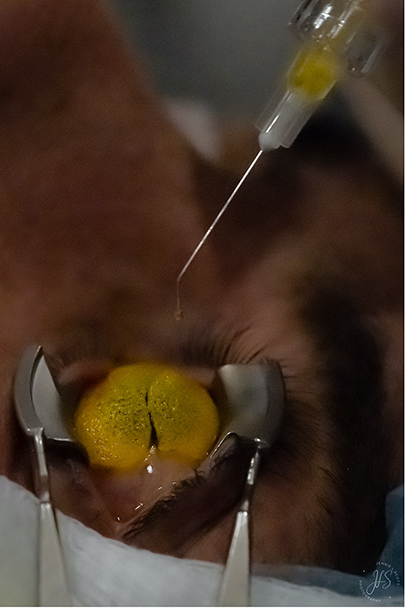 |
Figure 2 Application of Non-Viscous Riboflavin. |
 |
Figure 3 Topography-Guided Partial Epithelium Removal. |
Data Collection
A single-center, retrospective chart review of keratoconic eyes treated with PERFECT-CXL spanning from June 1, 2018 through January 1, 2023 was performed. This study was approved by the Massachusetts Eye and Ear Institutional Review Board and is in accordance with the tenets of the Declaration of Helsinki and HIPAA regulations. Three hundred and sixty-two eyes that underwent the procedure were identified. Only previously untreated eyes with KCN were included. Patients lost to follow-up within 6 months after CXL were excluded. Patients were also excluded once they initiated contact lens use to eliminate any confounding effect they might have on keratometry measurements. One hundred and fifty eyes in 89 patients that met the inclusion criteria were ultimately analyzed. Outcomes assessed included best spectacle-corrected visual acuity (BSCVA), maximum keratometry (Kmax), and treatment-associated complications (eg delayed epithelial healing [>1 week], persistent haze [>1 month], endothelial decompensation, and infection). Outcomes were assessed at 6 months, 1, 2 and 3 years postoperatively.
Results
Three hundred and sixty-two eyes that underwent PERFECT-CXL between June 2018 and January 2023 were analyzed and 150 were included in the study. Two hundred and twelve eyes were excluded for the following reasons: history of prior CXL, ectasia other than KCN, loss to follow-up after CXL, or use of contact lenses. Among the 150 eyes included in the study, 110 (73.3%) were from male subjects. This was a nonconsecutive cohort. The average age of the subjects was 28 years, with a 48-year range from 14 to 62 years old. All patients included were not wearing contact lenses for at least one month prior to being seen in the office and did not wear them for the duration of the study.
BSCVA and Kmax were measured and recorded preoperatively, and at 6 months, 1-, 2-, and 3- year intervals. Stable BSCVA was defined as within 2 lines of preoperative Snellen visual acuity. At 6 months, 1-, 2-, and 3-year intervals, 120, 93, 69 and 39 eyes were analyzed, respectively. At 6 months, 1-, 2-, and 3-year intervals, BSCVA was stable in 97.5%, 95.7%, 94.2%, 94.9%, respectively (Figure 4).
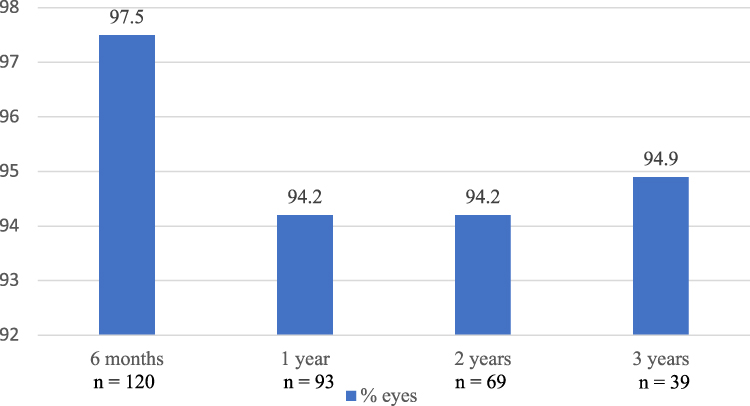 |
Figure 4 Percent of Eyes with Stable BCVA Defined as No Loss Greater than 2 Lines. |
Stable Kmax was defined as a change of less than 1 D from preoperative Kmax. At 6 months, 1 year, 2 years and 3 years, 80.3% (94/117), 88.2% (82/93), 84.1% (58/69), and 84.6% (33/39) of eyes experienced stabilization in Kmax, respectively (Figure 5). Mean Kmax changes were +0.40D, (SD 1.94, n = 117), −0.11D (SD 1.65, n = 93), −0.32D (SD 2.00, n = 69), and no change (0.00 D) (SD 1.52, n = 39) at 6 months, 1, 2, and 3 years, respectively (Table 2).
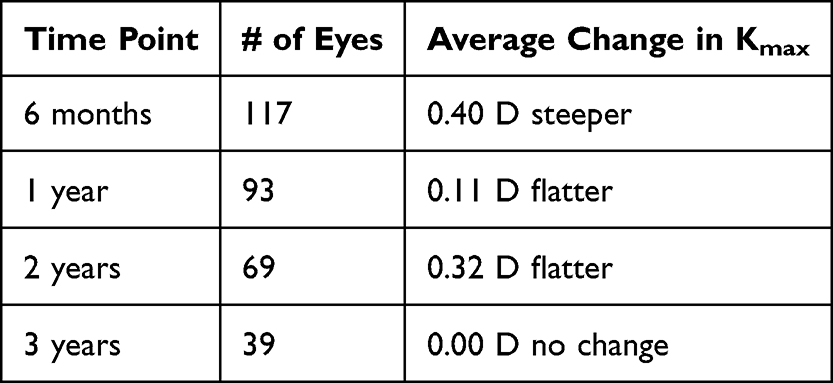 |
Table 2 Average Change in Kmax |
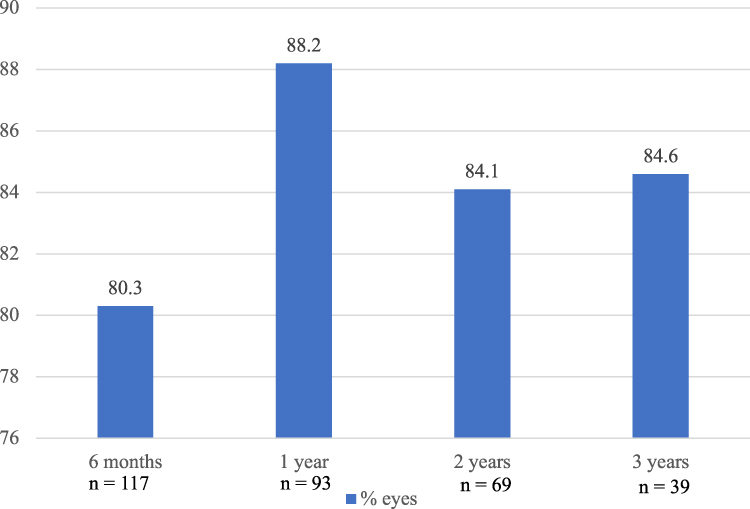 |
Figure 5 Percent of Eyes with Stable Kmax Defined as No Increase Greater than 1.0 Diopters. |
For eyes of patients not lost to follow-up, 1.3% (2/150) showed signs of tomographic progression, worsening subjective vision symptoms and/or reduction of BSCVA, and/or increase in astigmatism within 3 years after PERFECT CXL which required retreatment. The two patients who underwent retreatment were a 19 year-old male with grade 2 KCN and a 16 year-old female with grade 1 KCN with a positive family history of KCN. Both of these subjects self-reported ongoing eye rubbing. There were no cases of treatment-associated complications, including no instances of visually significant haze, delayed epithelial healing greater than 1 week, secondary infections, or endothelial decompensation.
Discussion
The hybrid CXL protocol, PERFECT-CXL, employs a tomography-guided manual de-epithelization technique intended to minimize the risks associated with complete epithelium removal during crosslinking. While de-epithelization in the Dresden protocol allows for improved riboflavin diffusion, oxygen diffusion, and UV penetration,3 debridement of a relatively large area of epithelium carries significant risks, including pain, poor epithelial healing, persistent corneal haze, and infection.2 Our protocol involves a two-step approach to epithelial disruption comprised 1) diffuse, partial disruption of epithelium using gentle mechanical disruption to induce dense punctate epithelial erosions (PEEs), 2) debridement of a relatively small 4–5mm zone of epithelium overlying the ectatic cone after riboflavin loading followed by 3) application of pulsed UV light. This technique utilizes a smaller total area of denuded epithelium than in s-CXL, which provides a theoretical basis to improve safety, minimize discomfort, expedite healing, and accelerate visual recovery.20 Smaller epithelial defects may also allow for contact lens wearers to typically resume use within 7 days and return to daily activities as quickly as possible.
Although various approaches have been described for epithelial removal—including mechanical debridement using a blade, alcohol-assisted debridement, and laser-assisted debridement– these approaches may entail additional risks. Mechanical debridement with a blade can result in Bowman’s membrane defects and stromal dehydration. Alcohol-assisted debridement can induce stromal dehydration along with inflammation and keratocyte loss. Lastly, laser-assisted techniques carry a risk of corneal haze.21 When compared to other types of mechanical removal, epithelial debridement using EBK has been shown to result in reduced patient discomfort and faster epithelial healing in CXL.21
The complication rate associated with s-CXL has been reported to be approximately 3–4%, so risk-reducing alternative techniques are desired.10,22 The epithelial preparation technique employed in PERFECT-CXL showed no complications in our cohort including delayed epithelial healing, corneal haze, infectious keratitis, persistent corneal edema, and endothelial decompensation. While future studies will be needed to quantify this effect, we noticed that patients are able to recover quickly from the procedure, perhaps due to the faster healing time from limited epithelial debridement. They were able to routinely return to baseline contact lens wear within 7–10 days of the procedure if desired. By contrast, many patients cannot tolerate their regular contact lenses until 1–2 months after s-CXL, with some studies illustrating that the actual time back to RGP use after s-CXL can be as long as 2.53 months on average.23 In this way, PERFECT-CXL fosters a patient-centered approach to cross-linking.
PERFECT-CXL is designed to improve CXL safety without sacrificing the efficacy of halting KCN progression. Of particular importance for CXL clinical outcome studies are the two- and three-year timepoints, as eyes that exhibit stability at one year may ultimately progress after additional follow-up.24 Ultimately, after 3 years of follow-up, only 2 eyes (1.3%) demonstrated signs of progression and underwent retreatment. Even prior s-CXL studies report progression rates of approximately 7–8% at 12 and 36 months.22,25 In fact, Koller et al found that even when eyes with a pre-op Kmax higher than 58.00 D (those at highest risk for progression) were excluded from their study, the rate of progression was still around 3% after just one year.
At every time point examined within the study, less than 6% of patients demonstrated fluctuation in BSCVA and less than 20% of patients had fluctuating Kmax compared to their baseline. Sometimes, a single metric was worse within a larger clinical picture that still suggested stability. Additionally, a patient who was unstable at one visit may also improve to the stable range at the following visit. In this way, the eyes included in these percentages deemed as “unstable” were not necessarily progressing. Kmax was used as a primary endpoint because it has historically been used for this purpose in FDA clinical trials assessing the efficacy of CXL.26 However, Kmax alone is arguably an imperfect measurement of progression. While studies have demonstrated that Kmax is among the most repeatable parameters used to discern ectatic progression,27 Kmax becomes more inaccurate with more advanced disease, and single variables (like Kmax) used to detect progression often show poor correlation with each other in comparison to parameters that aggregate several variables into one measurement (D-index, KPI, etc).28 Altogether, only 2 eyes (1.3%) demonstrated worsening of vision with corresponding increased steepening/progression on tomography that was consistently reproducible across office visits to warrant retreatment in our study.
There were two FDA-approved riboflavin formulations used for CXL in this study: iso-osmolar riboflavin 0.1% in 20% dextran (viscous) and hypo-osmolar riboflavin 0.1% in saline (non-viscous). Iso-osmolar, viscous riboflavin is traditionally used in the Dresden technique in de-epithelialized corneas.3,5,29 Hypoosmolar riboflavin is typically reserved for corneas with a thickness of less than 400mm and is used to “swell” the cornea after loading with viscous prior to UVA treatment. Compared to the single, large epithelial defect created in s-CXL, our technique involves creating dense punctate epithelial erosions (PEEs), or “roughened” epithelium prior to riboflavin loading. In the setting of PEEs, iso-osmolar, viscous riboflavin is unable to successfully penetrate the epithelium without prior creation of a full epithelial defect. Conversely, hypo-osmolar, non-viscous riboflavin yields a more even load due to its ability to penetrate areas of roughened epithelium and subsequently diffuse across the stroma. The generally favorable results seen in our cohort suggest successful CXL can be performed by utilizing the other type of FDA-approved riboflavin applied in the protocol. Moreover, although endothelial cell density was not directly assessed in our study, use of hypoosmolar riboflavin may have the unintended benefit of better protecting the endothelium during PERFECT-CXL in patients with thinner corneas.30,31
PERFECT-CXL allows for customized centration of the epithelial defect in accordance with each eye’s unique tomography with centration over the cone which may allow for a deeper crosslinking effect over the patient’s cone. Studies have shown that the biomechanical abnormalities observed in KCN are heterogeneously distributed across the cornea, with a greater degree of abnormality observed at or near the cone.32,33 By employing an approach wherein partial epithelial disruption is performed diffusely, followed by creation of a zone of complete epithelial debridement centered at the ectatic cone, the PERFECT-CXL technique allows for treatment of the entire cornea, but with greater treatment focus directed specifically at the cone with the goal to create an increased effect in this area. Although cone debridement occurs after riboflavin loading (and therefore does not affect the amount of riboflavin penetration), complete removal of the epithelium overlying the cone should result in greater stromal UV-A penetration and oxygen diffusion within the area.3 This reasoning is supported by a small number of studies that have reported favorable results with customized approaches to CXL.15–20,34 Seiler et al and Mazzotta et al reported more Kmax flattening and epithelial healing with delivery of graded UV-A dosing based on cone topography.18,34 In addition to employing tomography-guided CXL, Cassagne et al reported success with a technique in which de-epithelization was also focused on the cone. Notably, their technique did not involve partial de-epithelization at the periphery and follow up was restricted to only one year postoperatively.20
The effectiveness of PERFECT-CXL may also be bolstered by the mode of UV-A delivery used. Herein, we report use of non-continuous or “pulsed” UV-A irradiation as part of our protocol. Although s-CXL employs continuous UV-A irradiation, there is preclinical35 and clinical36 evidence to suggest pulsed UV-A administration may improve crosslinking of collagen. Studies have demonstrated that aerobic mechanisms are integral to riboflavin-mediated CXL.4,37 Yet, oxygen becomes depleted within 10–15 seconds of irradiation, at which point crosslinking proceeds through anaerobic mechanisms entirely.4 By applying pulsed UV-A irradiation in PERFECT-CXL, oxygen is permitted to re-diffuse into the stroma between light exposures, allowing for greater participation of aerobic mechanisms during CXL.36 It should be noted that this aerobic advantage of pulsed irradiation needs to be weighed against the potential reduced effect from reduced total fluence (2.7J/cm2), as compared to the Dresden protocol (5.4J/cm2).
Our study carries several limitations including a nonconsecutive cohort and less follow-up at longer periods of time postoperatively. This includes the possibility of attrition bias as the sample size decreased from 150 to 39 eyes over the 3-year period. Complications were holistically evaluated rather than using standardized safety outcomes. This study did not directly compare outcomes of PERFECT-CXL to other CXL techniques, including s-CXL, as a control group. While these initial results are promising, we look forward to prospective comparative validation with inferential statistical analysis in future studies. Because only keratoconic patients were included, the results of this study may also not be generalizable to other corneal ectatic disorders. In the future, alignment tools could be incorporated to increase the precision of the partial central epithelium removal only at the tomographic center of the cone; this could reduce potential surgeon-dependent variability in the technique. While using a “pulsed” irradiation technique provided the aerobic benefits described previously, pulsing has a theoretical risk of lower biomechanical efficacy from the reduced total fluence as compared to the Dresden protocol (2.7 compared to 5.4 J/cm2). It can also be noted that the efficacy and consistency of blocking UV-A radiation manually on timed intervals with tegaderm dressing has not yet been formally examined.
In conclusion, our study provides promising preliminary, retrospective results to suggest that PERFECT-CXL can be a safe and efficacious technique for the stabilization of KCN. The technique could be considered as an alternative approach to s-CXL in various stages of keratoconus.
Ethics Approval
This study was found to be IRB Exempt by the Massachusetts Eye and Ear Institutional Review Board on 9/12/24 (Protocol #: 2021P002770) and is in accordance with the tenets of the Declaration of Helsinki and HIPAA regulations. Patient informed consent to review medical records was waived.
Funding
There was no public or private financial support received for this study.
Disclosure
Dr Kathryn Hatch reports personal fees from Glaukos and EpiON; she is a co-founder of Tilleron, outside the submitted work. The authors declare that there are no conflicts of interest, including any financial/proprietary interests for this work.
References
1. Saad S, Saad R, Jouve L, et al. Corneal crosslinking in keratoconus management. J Fr Ophtalmol. 2020;43(10):1078–10. doi:10.1016/j.jfo.2020.07.002
2. Pasha H, Palazzolo L, Prakash G, Jhanji V. Update on corneal collagen crosslinking for ectasia. Curr Opin Ophthalmol. 2021;32(4):343–347. doi:10.1097/ICU.0000000000000765
3. Wu D, Lim DKA, Lim BXH, et al. Corneal cross-linking: the evolution of treatment for corneal diseases. Front Pharmacol. 2021;12:686630. doi:10.3389/fphar.2021.686630
4. Kamaev P, Friedman MD, Sherr E, Muller D. Photochemical kinetics of corneal cross-linking with Riboflavin. Invest Ophthalmol Vis Sci. 2012;53(4):2360. doi:10.1167/iovs.11-9385
5. Wollensak G, Spörl E, Seiler T. Behandlung von Keratokonus durch Kollagenvernetzung. Der Ophthalmologe. 2003;100(1):44–49. doi:10.1007/s00347-002-0700-3
6. Ng SM, Hawkins BS, Kuo IC. Transepithelial versus epithelium-off corneal crosslinking for progressive keratoconus: findings from a cochrane systematic review. Am J Ophthalmol. 2021;229:274–287. doi:10.1016/j.ajo.2021.05.009
7. Al Fayez MF, Alfayez S, Alfayez Y. Transepithelial versus epithelium-off corneal collagen cross-linking for progressive keratoconus: a prospective randomized controlled trial. Cornea. 2015;34(Supplement 10):S53–S56. doi:10.1097/ICO.0000000000000547
8. Li W, Wang B. Efficacy and safety of transepithelial corneal collagen crosslinking surgery versus standard corneal collagen crosslinking surgery for keratoconus: a meta-analysis of randomized controlled trials. BMC Ophthalmol. 2017;17(1):262. doi:10.1186/s12886-017-0657-2
9. Rush SW, Rush RB. Epithelium-off versus transepithelial corneal collagen crosslinking for progressive corneal ectasia: a randomised and controlled trial. Br J Ophthalmol. 2017;101(4):503–508. doi:10.1136/bjophthalmol-2016-308914
10. Nath S, Shen C, Koziarz A, et al. Transepithelial versus epithelium-off corneal collagen cross-linking for corneal ectasia. Ophthalmology. 2021;128(8):1150–1160. doi:10.1016/j.ophtha.2020.12.023
11. Wen D, Song B, Li Q, et al. Comparison of epithelium-off versus transepithelial corneal collagen cross-linking for keratoconus: a systematic review and meta-analysis. Cornea. 2018;37(8):1018–1024. doi:10.1097/ICO.0000000000001632
12. Buzzonetti L, Petrocelli G, Valente P, et al. Iontophoretic transepithelial collagen cross-linking versus epithelium-off collagen cross-linking in pediatric patients: 3-year follow-up. Cornea. 2019;38(7):859–863. doi:10.1097/ICO.0000000000001965
13. Arance-Gil Á, Villa-Collar C, Pérez-Sanchez B, Carracedo G, Gutiérrez-Ortega R. Epithelium-Off vs. transepithelial corneal collagen crosslinking in progressive keratoconus: 3 years of follow-up. J Optom. 2021;14(2):189–198. doi:10.1016/j.optom.2020.07.005
14. Ng SM, Ren M, Lindsley KB, Hawkins BS, Kuo IC. Transepithelial versus epithelium-off corneal crosslinking for progressive keratoconus. Cochrane Database Syst Rev. 2021;3(3):CD013512. doi:10.1002/14651858.CD013512.pub2
15. Hashemi H, Miraftab M, Hafezi F, Asgari S. Matched comparison study of total and partial epithelium removal in corneal crosslinking. J Refract Surg. 2015;31(2):110–115. PMID: 25735044. doi:10.3928/1081597X-20150122-06
16. Galvis V, Tello A, Carreno NI, et al. Corneal cross-linking (with a Partial Deepithelization) in keratoconus with five years of follow-up. Ophthalmol Eye Dis. 2016;8:17–21. PMID: 27199574; PMCID: PMC4869599. doi:10.4137/OED.S38364
17. Razmjoo H, Rahimi B, Kharraji M, Koosha N, Peyman A. Corneal haze and visual outcome after collagen crosslinking for keratoconus: a comparison between total epithelium off and partial epithelial removal methods. Adv Biomed Res. 2014;3:221. PMID: 25538907; PMCID: PMC4260293. doi:10.4103/2277-9175.145677
18. Seiler TG, Fischinger I, Koller T, Zapp D, Frueh BE, Seiler T. Customized Corneal Cross-linking: one-Year Results. Am J Ophthalmol. 2016;166:14–21. PMID: 26944278. doi:10.1016/j.ajo.2016.02.029
19. Frigelli M, Ariza Gracia MA, Aydemir ME, et al. Predicting the effects of customized corneal cross-linking on corneal geometry. Invest Ophthalmol Vis Sci. 2025;66(12):51. PMID: 40985801; PMCID: PMC12468094. doi:10.1167/iovs.66.12.51
20. Cassagne M, Pierné K, Galiacy SD, Asfaux-Marfaing MP, Fournié P, Malecaze F. Customized topography-guided corneal collagen cross-linking for keratoconus. J Refract Surg. 2017;33(5):290–297. doi:10.3928/1081597X-20170201-02
21. Shetty R, Nagaraja H, Pahuja NK, Jayaram T, Vohra V, Jayadev C. Safety and efficacy of Epi-Bowman keratectomy in photorefractive keratectomy and corneal collagen cross-linking: a pilot study. Curr Eye Res. 2015;1–7. doi:10.3109/02713683.2015.1045082
22. Koller T, Mrochen M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract Refract Surg. 2009;35(8):1358–1362. doi:10.1016/j.jcrs.2009.03.035
23. Mandathara PS, Kalaiselvan P, Rathi VM, Murthy SI, Taneja M, Sangwan VS. Contact lens fitting after corneal collagen cross-linking. Oman J Ophthalmol. 2019;12(3):177–180. doi:10.4103/ojo.OJO_43_2018
24. Caporossi A, Mazzotta C, Paradiso AL, Baiocchi S, Marigliani D, Caporossi T. Transepithelial corneal collagen crosslinking for progressive keratoconus: 24-month clinical results. J Cataract Refract Surg. 2013;39(8):1157–1163. doi:10.1016/j.jcrs.2013.03.026
25. Lenk J, Herber R, Oswald C, Spoerl E, Pillunat LE, Raiskup F. Risk factors for progression of keratoconus and failure rate after corneal cross-linking. J Refract Surg. 2021;37(12):816–823. doi:10.3928/1081597X-20210830-01
26. Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK; U.S. Crosslinking Study Group. U.S. multicenter clinical trial of corneal collagen crosslinking for treatment of corneal ectasia after refractive surgery. Ophthalmology. 2017;124(10):1475–1484. doi:10.1016/j.ophtha.2017.05.036
27. Neuhann S, Schuh A, Krause D, et al. Comparison of variables measured with a Scheimpflug device for evaluation of progression and detection of keratoconus. Sci Rep. 2020;10(1):19308. doi:10.1038/s41598-020-76020-6
28. Shajari M, Steinwender G, Herrmann K, et al. Evaluation of keratoconus progression. Br J Ophthalmol. 2019;103(4):551–557. doi:10.1136/bjophthalmol-2017-311651
29. Stojanovic A, Zhou W, Utheim TP. Corneal collagen cross-linking with and without epithelial removal: a contralateral study with 0.5% hypotonic riboflavin solution. Biomed Res Int. 2014;2014:1–9. doi:10.1155/2014/619398
30. Hafezi F, Mrochen M, Iseli HP, Seiler T. Collagen crosslinking with ultraviolet-A and hypoosmolar riboflavin solution in thin corneas. J Cataract Refract Surg. 2009;35(4):621–624. doi:10.1016/j.jcrs.2008.10.060
31. Raiskup F, Spoerl E. Corneal cross-linking with hypo-osmolar riboflavin solution in thin keratoconic corneas. Am J Ophthalmol. 2011;152(1):28–32.e1. doi:10.1016/j.ajo.2011.01.016
32. Scarcelli G, Besner S, Pineda R, Yun SH. Biomechanical characterization of keratoconus corneas ex vivo with brillouin microscopy. Invest Ophthalmol Vis Sci. 2014;55(7):4490. doi:10.1167/iovs.14-14450
33. Scarcelli G, Besner S, Pineda R, Kalout P, Yun SH. In vivo biomechanical mapping of normal and keratoconus corneas. JAMA Ophthalmol. 2015;133(4):480. doi:10.1001/jamaophthalmol.2014.5641
34. Mazzotta C, Moramarco A, Traversi C, Baiocchi S, Iovieno A, Fontana L. Accelerated corneal collagen cross-linking using topography-guided UV-A energy emission: preliminary clinical and morphological outcomes. J Ophthalmol. 2016;2016:1–10. doi:10.1155/2016/2031031
35. Aldahlawi NH, Hayes S, O’Brart DPS, Akhbanbetova A, Littlechild SL, Meek KM. Enzymatic resistance of corneas crosslinked using riboflavin in conjunction with low energy, high energy, and pulsed UVA irradiation modes. Invest Ophthalmol Vis Sci. 2016;57(4):1547. doi:10.1167/iovs.15-18769
36. Peyman A, Nouralishahi A, Hafezi F, Kling S, Peyman M. Stromal demarcation line in pulsed versus continuous light accelerated corneal cross-linking for keratoconus. J Refract Surg. 2016;32(3):206–208. doi:10.3928/1081597X-20160204-03
37. Richoz O, Hammer A, Tabibian D, Gatzioufas Z, Hafezi F. The biomechanical effect of corneal collagen cross-linking (CXL) with riboflavin and UV-A is oxygen dependent. Trans Vision Sci Technol. 2013;2(7):6. doi:10.1167/tvst.2.7.6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Epi-On vs Epi-Off Corneal Cross-Linking in Corneal Ectasia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Nughays RO, Bazayd AS, Alshamekh LA, Alshammari RA, Alanazi MA, Dahlan HY, Alsubhi JA, Alshammri SG, AlQurashi NA, Aldajani AH, Alrammah AH, Alenezi MN, Almutairi AA, Alomayri AF, Alghamdi S
Clinical Ophthalmology 2025, 19:1531-1541
Published Date: 8 May 2025