Back to Journals » Risk Management and Healthcare Policy » Volume 18
Precautionary Recommendation System in Risk Management: A FMEA-Based Approach
Authors Narlı M ![]()
Received 22 August 2025
Accepted for publication 7 October 2025
Published 23 October 2025 Volume 2025:18 Pages 3437—3447
DOI https://doi.org/10.2147/RMHP.S557778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Müfide Narlı
Faculty of Engineering, Cukurova University, Adana, Turkey
Correspondence: Müfide Narlı, Email [email protected]
Purpose: FMEA (Failure Mode and Effects Analysis), a widely used tool in risk management, lacks systematic guidance on selecting the type of precaution. This study introduces a rule-based FMEA. Although the Risk Priority Number (RPN), widely used in the literature, expresses the risk level quantitatively, it is insufficient for guiding the appropriate type of precaution. The proposed rule-based model uses a multi-dimensional rule system that considers numerical parameters (probability, severity, detectability, and RPN) and contextual variables.
Material and Methods: The model, structured according to the Occupational Health and Safety precaution hierarchy, defines six precaution classes: elimination, substitution, engineering measures, training, administrative measures, and personal protective equipment (PPE). The model’s theoretical consistency, sensitivity, and practical applicability were tested in a neonatal intensive care unit (NICU).
Results: The FMEA method identified 24 failure modes related to infections. Scenario-based sensitivity analyses revealed that contextual variables significantly influenced the recommended precautions. Administrative and training measures were the most frequently recommended, while PPE was consistently recommended for exposure-related risks. Expert evaluation indicated 95.8% agreement with the model outputs.
Conclusion: These findings indicate that the development of a rule-based system can serve as a repeatable and explainable decision-support tool, especially in high-risk settings such as healthcare, which is the study’s most distinctive contribution.
Keywords: FMEA, RPN, risk control measures, rule-based decision model, decision support system
Introduction
Efficient management of complex system errors is critical for occupational health, safety, and service quality. In this context, Failure Mode and Effects Analysis (FMEA) is a proactive risk analysis method widely used to identify potential failure modes in processes, evaluate the effects of these failures, and plan appropriate preventive measures.1,2 However, although the Risk Priority Number (RPN) calculation provided by FMEA is often helpful in determining the magnitude of the risk, it provides limited systematic guidance on which precaution type should be implemented.
Although fuzzy logic, multi-criteria decision-making (MCDM), and artificial intelligence-based approaches have been integrated to fill this gap in the literature, subjective judgments and practitioner experience continue to be effective in the recommendation generation process.3,4 Especially in healthcare settings, the effects of contextual variables such as human factors and exposure on risk management decisions have not been systematically modeled to a sufficient degree. This situation highlights a significant methodological limitation regarding the consistency and repeatability of precautionary measures.
To overcome these limitations, this study proposes a rule-based, multi-dimensional decision support model integrated with the FMEA. The developed model systematically recommends the most appropriate precaution type for each failure mode, taking into account the RPN value, severity, occurrence, detectability, human factors, and exposure status. It classifies precautions into six categories: elimination, substitution, PPE and engineering controls, training, and administrative measures, according to the occupational health and safety precaution hierarchy.5,6 The model’s validity was tested through a sample FMEA application implemented in a neonatal intensive care unit (NICU); the sensitivity of the proposed measures to contextual variables and their compatibility with healthcare team members were analyzed in detail. The results demonstrate that the model serves as a decision support tool that is both theoretically and practically applicable and generalizable.
The FMEA method is a risk assessment tool of industrial origin that has been widely used in the healthcare sector in recent years. Its application in healthcare significantly contributes to patient safety, medication management, and cost-effectiveness analysis.3,7–9 The adaptation of FMEA as a proactive approach in healthcare services gained momentum with the adoption of risk analysis standards by.10 The study by Spath (2003) detailed how FMEA steps can be applied clinically in perioperative solutions, creating one of the first guides for healthcare professionals.8 In the literature, FMEA applications aim to identify high-risk areas based on RPN values and to assign risk classes accordingly. However, the stages of developing precautions, creating action plans, and evaluating outcomes have often been overlooked or assessed subjectively. This has been identified as a significant deficiency that limits the scope of FMEA applications.11 This study aims to address this gap by systematically developing a precautionary recommendation framework that incorporates specific rules and considers relevant contextual variables.
Rule-based systems are structures where decisions are determined by predefined rules, typically based on logical constructs such as “IF-THEN” or “OR-AND”. These systems form the fundamental components of expert knowledge systems.12 Expert systems are not limited to rule sets; they encompass a broader framework that includes an inference engine, knowledge base, and user interface. Conversely, rule-based systems are built solely on rules, as they do not incorporate classical machine learning or inference options.
The systematic literature review conducted by Papadopoulos (2022) emphasized that rule-based clinical decision support systems (CDSS) have key advantages, including explainability, transparency, and flexibility.12 In this context, combining the benefits of these systems with FMEA-based risk management processes enables the development of a systematic and assessable precautionary recommendation framework. However, it has also been noted that most of these systems have not been adequately tested in actual clinical environments and that there are gaps in the evaluation processes of decision-making mechanisms.
The success of rule-based CDSSs depends directly on the accuracy and clarity of their knowledge representation methods. In this context, Silva et al (2023) noted that these methods offer advantages in terms of ease of use and understandability, especially in clinical settings. The study highlighted that representing clinical rules with these two methods facilitates the intuitive and effective operation of the systems.13
The effectiveness of CDSS rules relies on their accuracy and structural factors, such as reusability, management, and interoperability. A recent systematic review found that ontologies are widely utilized in structuring medical knowledge and decision rules. However, they have limitations in CDSS rule management and customization processes. This highlights the need for robust rule management mechanisms to ensure the development and sustainability of decision support systems.14
Haas, Maier, and Rothgang (2021) highlighted the issues of explainability and reliability in the early prediction of in-hospital mortality risk among emergency and intensive care patients. They developed two rule-based risk prediction models that use demographic data and clinical information available during patient admission. The study concluded that the models, particularly the comprehensive model, demonstrated high performance with 98% accuracy, and the generated rules were both explainable and clinically assessable. This research demonstrates that rule-based structures can be effectively used in healthcare for decision support and data interpretation and shows the potential for similar methods to be applied across various risk assessment scenarios.15
In recent years, artificial intelligence (AI)-based diagnostic support systems have increasingly appeared in the CCDS literature. For example, Zhang16 applied AI as a diagnostic CCDS in a scenario study, demonstrating its potential to assist decision-makers in clinical processes. In addition, the literature review conducted by Scenario et al17 emphasized that the use of AI-based decision support systems in healthcare has been steadily expanding.
Studies using rule-based FMEA methods in industrial applications are also noteworthy. For example, Karatuğ, Ceylan, and Arslanoğlu (2024) developed a rule-based FMEA model that utilizes fuzzy logic based on expert opinions to evaluate risks in scrubber systems used in the maritime sector. The study identified the highest-risk components, and systematic measures were recommended.18
This study presents a structured approach to the FMEA method, with a focus on precaution suggestions. The rule-based model provides recommendations not only based on the RPN value but also on contextual variables, including failure type, human factors, and exposure. The model aims to present precaution decisions within a more systematic and transparent framework, providing a structured and auditable basis to enhance current practices and improve the consistency of risk management decisions in healthcare.
Materials and Methods
This study was conducted in 2024 in a level 4 Neonatal Intensive Care Unit (NICU) affiliated with a university hospital. This study team comprised senior nurses working in the NICU (each with more than 20 years of professional experience), the charge nurse, and a faculty member responsible for the clinical management of the NICU. Their expertise contributed to the identification of failure modes, FMEA scoring, and the evaluation of the rule-based model outputs.
A total of 24 failure modes related to infection risks in the NICU were identified. For each failure mode, severity (S), occurrence (O), detectability (D), and contextual variables such as human factors and exposure were defined. The decision support system was developed using Python, and failure mode inputs were entered manually. For each of these factors (S, O, D), the system generates rule-based recommendations based on the inputs. These recommendations were organized according to the occupational health and safety precautions hierarchy, which includes six precaution classes: elimination, substitution, engineering, training, administrative, and PPE.
The workflow of the study followed five stages:
Identifying infection-related failure modes in the NICU with team input and literature
Defining and scoring of FMEA parameters (S, O, D) and calculation of the RPN
Generating precaution recommendations through the rule-based model
Validating recommendations with scenario-based sensitivity analyses
Comparing system outputs with team evaluations to assess agreement
In this study, the  value for each failure mode (i) was calculated using the traditional FMEA approach as the product of the Severity (
value for each failure mode (i) was calculated using the traditional FMEA approach as the product of the Severity ( ), Probability (
), Probability ( ), and Detectability (
), and Detectability ( ) scores, as shown in Equation (1). However, the decision structure of the model was not based solely on this RPN score. The developed rule-based system used the RPN value as a primary indicator. Nevertheless, it evaluated final precaution decisions in light of additional factors, such as contextual variables (human factor, exposure), parameter thresholds (eg, high severity, low detectability), and systemic variation. In this way, the model extends beyond the one-dimensional RPN threshold-based decision structures often seen in classical FMEA applications, offering a multidimensional, explainable system for precautionary recommendations.
) scores, as shown in Equation (1). However, the decision structure of the model was not based solely on this RPN score. The developed rule-based system used the RPN value as a primary indicator. Nevertheless, it evaluated final precaution decisions in light of additional factors, such as contextual variables (human factor, exposure), parameter thresholds (eg, high severity, low detectability), and systemic variation. In this way, the model extends beyond the one-dimensional RPN threshold-based decision structures often seen in classical FMEA applications, offering a multidimensional, explainable system for precautionary recommendations.

This study developed a model using a multi-criteria rule set to analyze failure modes systematically and recommend precautions for each risk. The decision rules that form the foundation of the model are explained below.
Notations
 : Input vector representing the i-th failure mode
: Input vector representing the i-th failure mode
 : Risk Priority Number of the i-th failure mode
: Risk Priority Number of the i-th failure mode
 : The set of recommended preventive actions for the i-th failure mode
: The set of recommended preventive actions for the i-th failure mode
 : Type of failure cause (1=human factor, 0=other)
: Type of failure cause (1=human factor, 0=other)
 : Exposure status (1=present, 0=absent)
: Exposure status (1=present, 0=absent)
 : Power set of all possible preventive actions
: Power set of all possible preventive actions
Input Definition
The model represents each failure mode with the following vector.

Where:



 : Type of failure {1=human related, 0=not human related}
: Type of failure {1=human related, 0=not human related}
 : Exposure condition {1=present, 0=absent}
: Exposure condition {1=present, 0=absent}
Rule-Based Decision Model
The model’s basic output is the recommended measures for each failure mode. In addition to the RPN value, the decision algorithm operates based on specific decision rules for each failure mode.
Rule 0:  , for each failure mode, is calculated as shown in equation (1) by multiplying the parameter scores based on the traditional FMEA method. This approach enables a quantitative risk assessment by evaluating the severity of the failure, its likelihood of occurrence, and detectability [1,2].
, for each failure mode, is calculated as shown in equation (1) by multiplying the parameter scores based on the traditional FMEA method. This approach enables a quantitative risk assessment by evaluating the severity of the failure, its likelihood of occurrence, and detectability [1,2].
Rule 1-Low Risk Monitoring Recommendation: Failure modes with an RPN of 100 or less are considered low risk. However, limited and low-level precautions may be necessary due to certain contextual factors (eg, exposure or failure caused by human behavior).

Rule 2-Active Measures for Higher Risk: Failure modes with an RPN value above 100 are too risky to manage with “monitoring”. An active measure must be developed for such risks. According to the AIAG & VDA (2019) guide, monitoring is only valid at low risk levels.17

Rule 3-Risk Classification: This rule categorizes failure modes into four classes based on risk levels. This classification, determined by the RPN value, serves as the foundation for developing specific precautions for each risk group.2,19

Rule 4-Medium Risk Measures: Medium-risk situations can be managed through behavioral or administrative actions, as human factors are primarily responsible for them. If the error stems from a human factor, “training” is recommended; if it results from a system failure, “administrative” measures are advised. Additionally, when there is exposure, the use of PPE becomes mandatory.10

Rule 5-High Risk Requires Technical Controls: Implementing technical measures is crucial for high-risk failure modes. These risks should be managed at the system level using engineering solutions, rather than solely relying on behavioral methods. Additional precautions, such as training or PPE, should be added if human factors or physical exposures are involved. The ISO 45001:2018 standard supports these layered strategies in occupational health and safety management systems.

Rule 6-High Control Strategy: This rule defines the order of measures starting from the closest and most effective to the source.5,20

Rule 7-Substitution When Elimination is Not Possible: This additional rule supports rule 6. If eliminating the hazard is impossible and the system has ruled out this option, substitution should be the next priority. This allows the use of less hazardous substances or processes, especially in environments with physical, chemical, or biological hazards. As a result, effective and proactive risk reduction can be achieved.



Rule 8-Critical Conditions Trigger Rule 6: This rule mandates the application of Rule 6 in specific situations. When severity is high and detectability is low, or when  exceeds the specified threshold, measures must be chosen strictly by the priority order outlined in Rule 6. These conditions indicate that the risk has exceeded acceptable limits and requires interventions focused on the source. Each
exceeds the specified threshold, measures must be chosen strictly by the priority order outlined in Rule 6. These conditions indicate that the risk has exceeded acceptable limits and requires interventions focused on the source. Each  represents a high-risk class, where evaluation begins with elimination and substitution.
represents a high-risk class, where evaluation begins with elimination and substitution.



Rule 9-Engineering Control Enforcement: This rule applies in scenarios where the severity is very high but the error is relatively easy to detect. In such cases, the rule structure should activate engineering controls, which are more effective and permanent measures to mitigate the risk at its source. The model evaluates the following special conditions and makes engineering intervention mandatory.2,5




Rule 10-Training vs Administrative: If the source of the failure mode is related to human behavior (T₁ = 1), the system recommends direct training measures. Otherwise (T₁ = 0), organizational or administrative controls are preferred. This distinction enables targeted intervention to reduce accidents caused by human factors.10

Rule 11-PPE Decision Based on Exposure: If exposure exists (eg, biological, chemical, or physical risk), PPE is required under legal and occupational standards. When there is no exposure, PPE is not advised.5


Action Set Definition: The model developed in this study defines a decision function to identify the appropriate action set for each failure mode. Action set A is the comprehensive set that includes all action types the system can apply. This set:

Decision Function: The model recommends one or more suitable measures for each failure mode  . These recommendations are based on the established rules and the risk parameters associated with the failure mode.
. These recommendations are based on the established rules and the risk parameters associated with the failure mode.

Here,  is the power set that includes all subsets of the measure set. That is, the decision function can choose zero or more types of measures from the set (A) for each failure mode. However, this study is designed to recommend only one measure. This approach facilitates the development of holistic measures based on the combined effect of multiple risk factors.
is the power set that includes all subsets of the measure set. That is, the decision function can choose zero or more types of measures from the set (A) for each failure mode. However, this study is designed to recommend only one measure. This approach facilitates the development of holistic measures based on the combined effect of multiple risk factors.
Findings and Discussion
This study identified 24 different failure modes through risk analysis using the FMEA method in a university hospital’s neonatal intensive care unit. The identified failure modes were categorized into five main processes, based on the functional integrity and analytical traceability of each process. By defining these processes, possible failure sources were examined more systematically. According to the traditional FMEA method, the RPN value for each failure mode was calculated by multiplying the scores of the S, O, and D parameters. The rule-based decision support model developed in this study systematically recommends appropriate precaution types for each failure mode, taking into account the RPN value and contextual factors such as human factors and exposure.
Table 1 presents the basic risk parameters for each failure mode, the computed RPN values, and the precautionary measures suggested by the model.
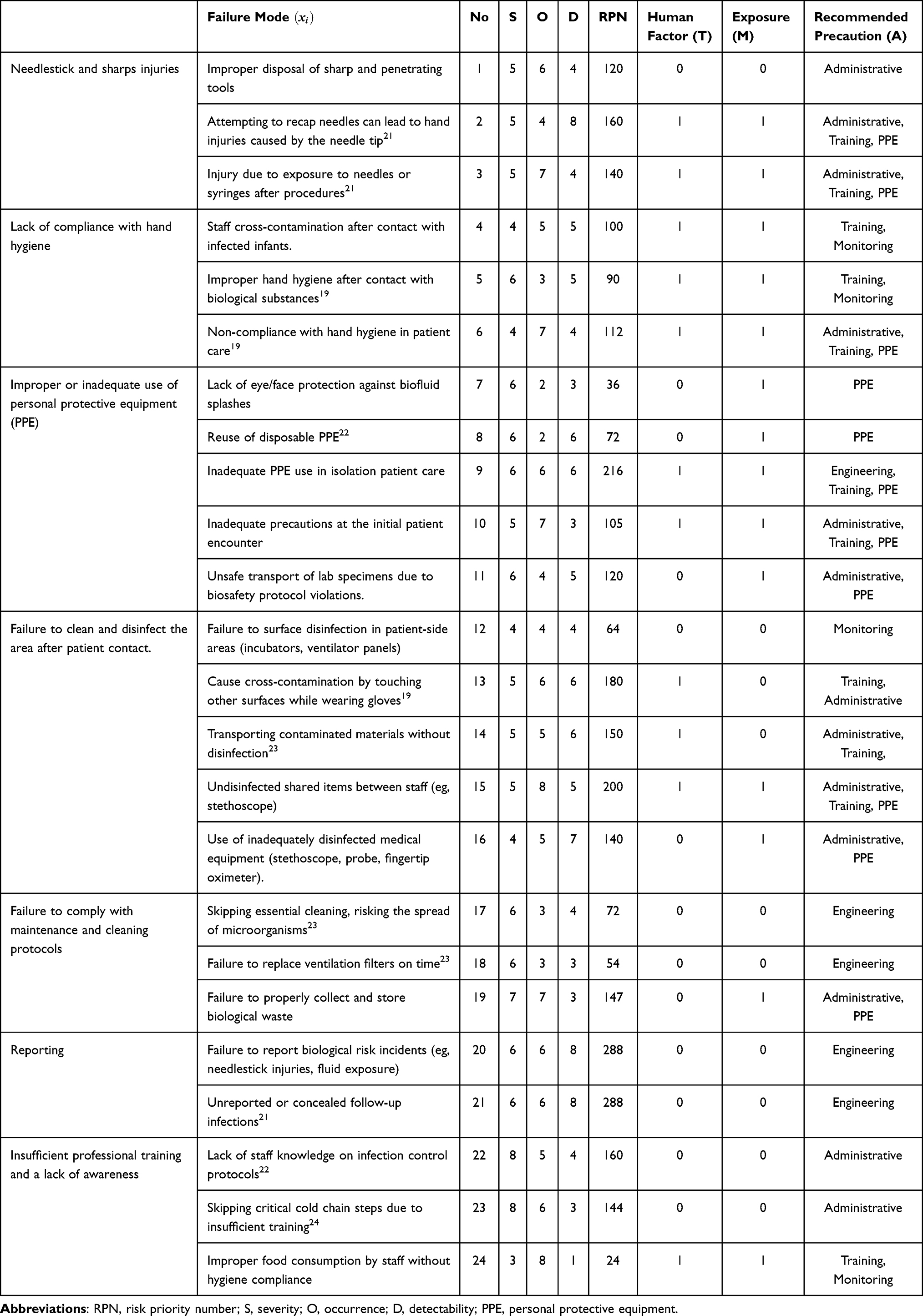 |
Table 1 Risk Parameters, RPN Values, and Recommended Precaution Types for Failure Modes |
Training and administrative measures are the most commonly recommended precautions, especially in the medium-risk group ( . The model suggested at least one precaution for each failure mode, with no gaps in any decision. Additionally, a structural harmony was observed between the measures proposed by the model and the contextual risk indicators. This demonstrates that the model efficiently reflects a multidimensional, condition-based risk management approach, not relying solely on
. The model suggested at least one precaution for each failure mode, with no gaps in any decision. Additionally, a structural harmony was observed between the measures proposed by the model and the contextual risk indicators. This demonstrates that the model efficiently reflects a multidimensional, condition-based risk management approach, not relying solely on  . It was noted that administrative and training measures were primarily recommended, supporting the idea that human factors and systemic deficiencies are the primary causes of most failure modes. Moreover, PPE was systematically recommended in cases of exposure to hazardous materials. No failure modes fell into the critical risk class, indicating that none of the failure types reached the extreme
. It was noted that administrative and training measures were primarily recommended, supporting the idea that human factors and systemic deficiencies are the primary causes of most failure modes. Moreover, PPE was systematically recommended in cases of exposure to hazardous materials. No failure modes fell into the critical risk class, indicating that none of the failure types reached the extreme  value. Since critical risk thresholds were not surpassed, aggressive elimination and substitution measures were not suggested at any risk level. Engineering measures were rarely recommended. Table 2 provides a comparative overview of the frequency of different measure types based on
value. Since critical risk thresholds were not surpassed, aggressive elimination and substitution measures were not suggested at any risk level. Engineering measures were rarely recommended. Table 2 provides a comparative overview of the frequency of different measure types based on  values and risk class intervals.
values and risk class intervals.
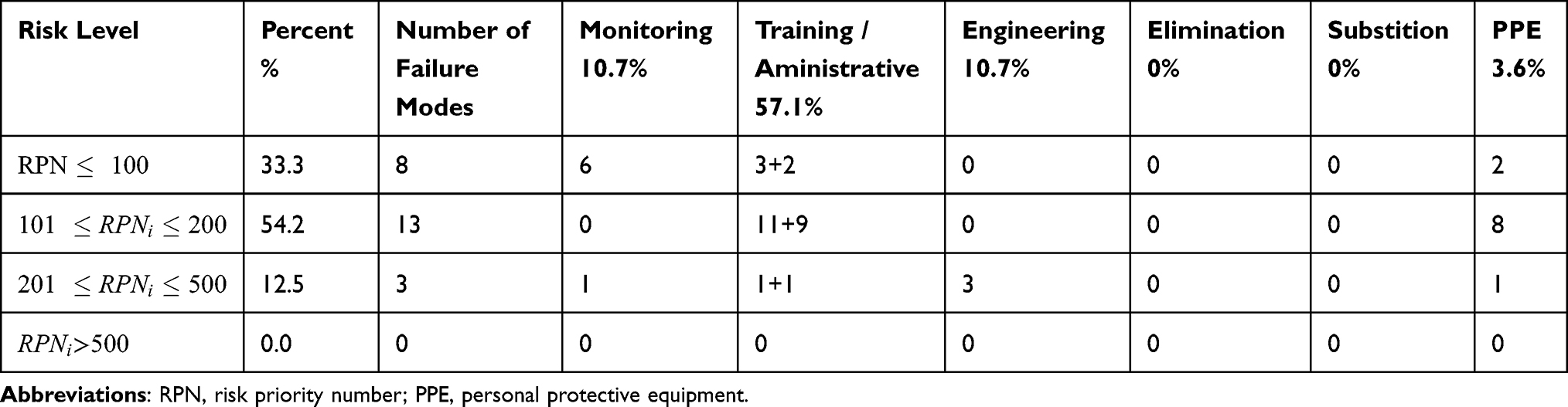 |
Table 2 Distribution of Recommended Precaution Types by Risk Level |
The model outputs in Table 1 are made more numerically traceable with the data in Table 2. In the sample, as shown in Table 2, no failure mode was identified for the critical risk level RPN > 500; therefore, no precautions are recommended for this range.
Scenario-based calculations were conducted using contextual variables such as “Human Factor” and “Impact of Exposure” to assess the model’s sensitivity in its recommendations. The four scenarios below indicate whether each failure mode is system- or human-based and if the risk is related to exposure. In this context, the model recalculated the recommended precautions for each scenario, and the results are shown in Table 3. Four scenarios were defined to evaluate the model’s sensitivity to these variables, considering whether the failure mode was caused by human factor (T) and the exposure content (M).
Scenario 1 (No Human Factor – No Exposure): (T = 0, M = 0) Situations that are system-based and lack exposure.
Scenario 2 (Human Factor – No Exposure): (T = 1, M = 0): Situations involving human factor without exposure.
Scenario 3 (No Human Factor – With Exposure): (T = 0, M = 1): System-based situations involving exposure.
Scenario 4 (Human Factor – With Exposure): (T = 1, M = 1): Situations that are both human-based and with exposure.
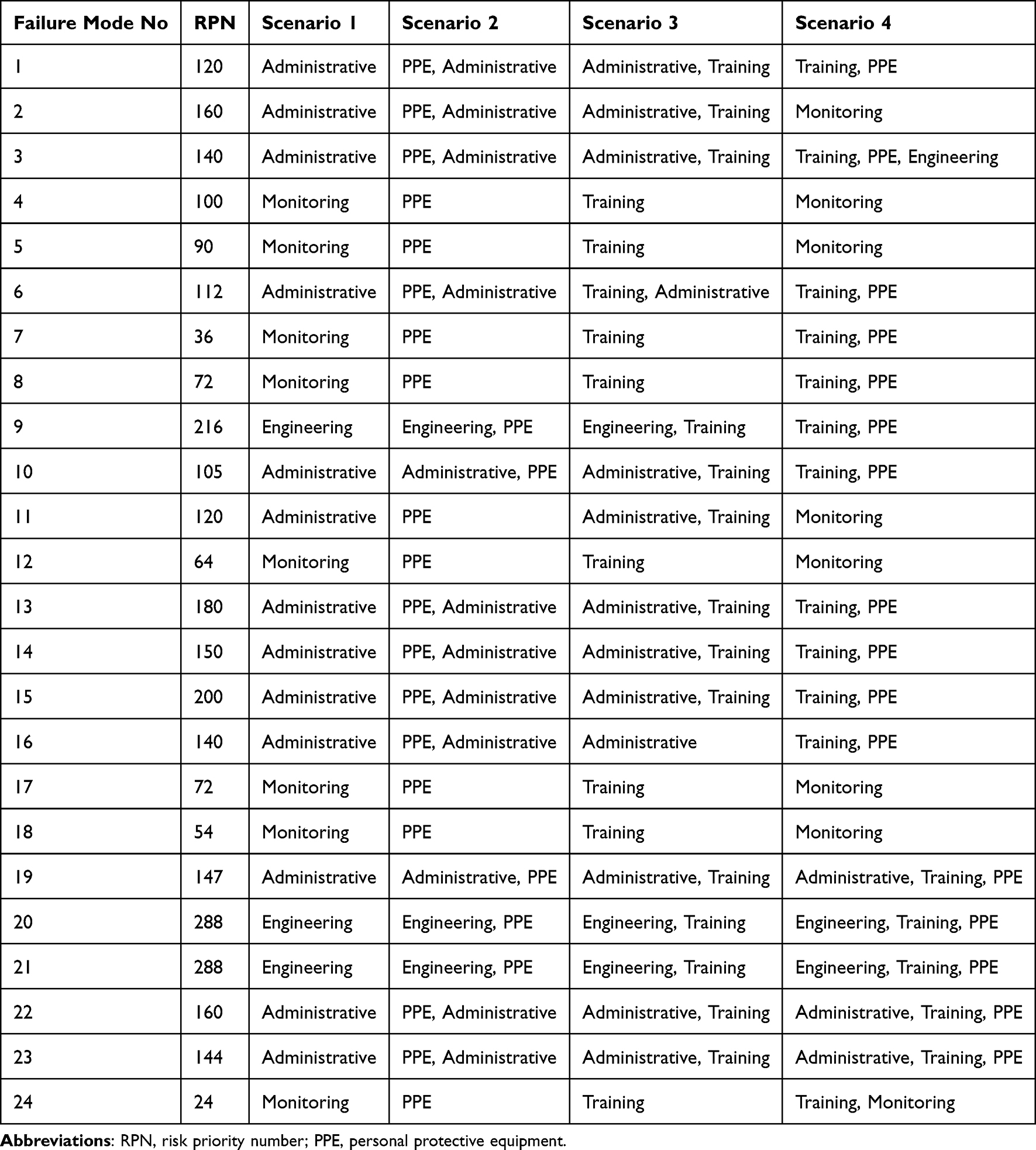 |
Table 3 Comparison of Recommendations Across All Scenarios |
The results demonstrate that the model responds sensitively to contextual variables. Significant differences were observed in recommended measures, especially for failure modes at medium risk levels. Only administrative measures are recommended for some failure modes when T and M values are zero. However, when T = 1, training and administrative measures are recommended together for the same failure mode. When exposure (M=1) is present, using PPE for that failure often becomes a prominent recommendation and is added to the measures set. When both variables are active simultaneously (T=1, M=1), the model recommends combining training, administrative, and PPE measures. In about 70% of failure modes, the recommended measures vary depending on the scenario. Especially in failure modes sensitive to human factors, behavioral factors directly influence the model’s decision-making structure. Additionally, despite having a fixed RPN value, the variations in measure sets across different scenarios show that the model relies not only on quantitative scores but also on contextual logic rules.
The validity of the model was tested not only with theoretical concepts but also through expert evaluation. In this context, experienced team members working in the intensive care unit, selected because of their many years of service in this unit, assessed the precautions suggested by the model for each failure mode. The team of three members contributing to the study was asked to rate each recommendation using a three-dimensional scale. This validation process served as an independent and systematic check of the model’s practical applicability.
As a result of the evaluation, the findings presented in Table 1 classified a total of 24 failure modes, with the model’s suggested precautions for 19 failure modes as “Appropriate”. Four failure modes were evaluated as “Partially Appropriate”, where the recommendations could be improved with minor corrections. One failure mode was classified as “Not Appropriate”, in which the recommended precautions were insufficient, contextually inappropriate, or ineffective.
Expert team evaluations and model recommendations were 95.8% in agreement. This high level of compliance indicates that the developed decision support model effectively integrates predefined rules and practical expert knowledge in healthcare. The findings demonstrate that the model is stable with respect to parametric variables, sensitive to critical threshold values, and provides flexible and customizable suggestions based on contextual variables.
Therefore, it was concluded that the developed model has strong potential as a proactive, systematic, and explainable decision-support tool in healthcare. Furthermore, the model significantly aids in objectifying and automating FMEA processes, helping to reduce inconsistencies in human-related decision-making.
Although expert evaluations and scenario-based analyses supported the findings of this study, they remain limited by their reliance on a theoretical framework. The novelty of the lies in its ability to incorporate contextual variables, such as human factors and exposure, into the precaution selection process, which has often been overlooked in traditional FMEA applications. To further establish the reliability and generalizability of the proposed system, confirmatory applications in real-world clinical and industrial settings are required. Such validations would not only strengthen the credibility of the results but also demonstrate the model’s practical applicability across diverse environments.
Conclusion
In this study, a rule-based decision model was integrated into the FMEA-based risk assessment approach, and the precaution types recommended for each failure mode were systematically determined. Designed to eliminate subjectivity in precaution-type selection, a common issue in FMEA applications highlighted in the literature, this model considers the RPN value in conjunction with failure effects, severity, detectability, and exposure status.
The model classifies risk control measures into six main categories: elimination, substitution, engineering controls, training, administrative controls, and personal protective equipment (PPE), establishing a hierarchy among these measures. This framework enables proactive intervention in high-severity and difficult-to-detect failures, helping to avoid resource waste in low-risk situations. Furthermore, behavioral and process-based strategies are included, and training and/or administrative measures are recommended for human-factor-related cases.
The model, tested through a sample FMEA application, delivered successful results in both theoretical consistency and practical applicability with its recommended precaution based on failure mode characteristics. The proposed system can be viewed as a generalizable decision support tool in clinical settings, such as NICUs, and in high-risk environments, including industrial, laboratory, and production processes. Overall, the study makes a clear contribution to risk management by enhancing the consistency, objectivity, and explainability of precaution selection in high-risk settings.
However, the study has limitations, as the findings are primarily based on theoretical analyses and expert evaluations. To further establish the reliability and generalizability of the model, confirmatory applications in real-world clinical and industrial settings are required.
Future research could expand by integrating this model with artificial intelligence and learning systems, making it more dynamic through training with large data sets, and creating specific sub-versions tailored to sectoral needs. Additionally, testing the model with different user groups across various institutional settings and supporting it with user-friendly software interfaces will significantly enhance risk management.
Ethics Statement
According to the Çukurova University Scientific Research and Publication Ethics Directive (Çukurova Üniversitesi Bilimsel Araştırma ve Yayın Etiği Yönergesi, Senate Decision dated 13.02.2018, No. 03/03), ethics approval is only required for biomedical, clinical, or survey-based studies involving human or animal data (Articles 5/b, 5/c, and 8/c, 8/g). Since this study is theoretical and does not include human participants, patient data, employee data, or animal subjects, it is exempt from requiring ethics approval under this directive. The necessary administrative permissions were obtained from the relevant institutional authorities and can be provided upon request.
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (2013 revision).
Disclosure
The author declares no conflicts of interest.
References
1. Stamatis DH. Failure Mode and Effect Analysis: FMEA From Theory to Execution. Quality Press; 2003.
2. International Electrotechnical Commission (IEC). IEC 60812:2018 – failure modes and effects analysis (FMEA and FMECA). 2018. Available from: https://webstore.iec.ch/.
3. Kunac DL, Reith DM. Identification of priorities for medication safety in neonatal intensive care. Drug Safety. 2005;28(3):251–261. doi:10.2165/00002018-200528030-00006
4. Yi L, Chen Y, Hu R, Hu J, Pan W. Application of healthcare failure mode and effect analysis in controlling surgical instrument packaging defects. Sci Rep. 2022;12(1):19708. doi:10.1038/s41598-022-24282-7
5. National Institute for Occupational Safety and Health (NIOSH). Hierarchy of controls. Centers for disease control and prevention (CDC). 2015. Available from: https://www.cdc.gov/niosh/topics/hierarchy/.
6. International Organization for Standardization (ISO). ISO 45001:2018 - Occupational health and safety management systems — requirements with guidance for use. 2018. Available from: https://www.iso.org/home.html.
7. Vecchia M, Sacchi P, Marvulli LN, et al. Healthcare application of failure mode and effect analysis (FMEA): is room in the infectious disease setting? A scoping review. In: Healthcare. Vol. 13. Multidisciplinary Digital Publishing Institute; 2025:82.
8. Spath PL. Using failure mode and effects analysis to improve patient safety. AORN J. 2003;78(1):15–37. doi:10.1016/S0001-2092(06)61343-4
9. Najar AV, Ghane H, Ebrahimipour H, Nouri GA, Dadpour B. Identifying priorities for medication safety in the neonatal intensive care unit via failure mode and effect analysis. Iranian J Neonatol. 2016;7(2).
10. The Joint Commission. Framework for conducting a root cause analysis and action plan. 2017. Available from: https://jointcommission.new-media-release.com/2017_annual_report/.
11. Liu HC, Zhang LJ, Ping YJ, Wang L. Failure mode and effects analysis for proactive healthcare risk evaluation: a systematic literature review. J Evaluation Clin Pract. 2020;26(4):1320–1337. doi:10.1111/jep.13317
12. Papadopoulos P, Soflano M, Chaudy Y, Adejo W, Connolly TM. A systematic review of technologies and standards used to develop rule-based clinical decision support systems. Health Technol. 2022;12(4):713–727. doi:10.1007/s12553-022-00672-9
13. Silva B, Hak F, Guimarães T, Manuel M, Santos MF. Rule-based system for adequate clinical decision support. Procedia Comput Sci. 2023;220:880–885. doi:10.1016/j.procs.2023.03.119
14. Jing X, Min H, Gong Y, et al. Ontologies applied in clinical decision support system rules: systematic review. JMIR Med Informatics. 2023;11:e43053. doi:10.2196/43053
15. Haas O, Maier A, Rothgang E. Rule-based models for risk estimation and analysis of in-hospital mortality in emergency and critical care. Front Med. 2021;8:785711. doi:10.3389/fmed.2021.785711
16. Zhang Y, Chen Y, Li K, Jiang W, Zhang BC. Artificial intelligence system application in military lung metastasis: experience from a rare case. Risk Manag Healthcare Policy. 2021;Volume 14:2825–2829. doi:10.2147/RMHP.S315152
17. Secinaro S, Calandra D, Secinaro A, Muthurangu V, Biancone P. The role of artificial intelligence in healthcare: a structured literature review. BMC Med Inf Decis Making. 2021;21(1):125. doi:10.1186/s12911-021-01488-9
18. Karatuğ Ç, Ceylan BO, Arslanoğlu Y. A risk assessment of scrubber use for marine transport by rule-based fuzzy FMEA. Proc Institution Mech Engineers Part M. 2024;238(1):114–125.
19. Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Lancet. 2000;356(9238):1307–1312. doi:10.1016/S0140-6736(00)02814-2
20. AIAG & VDA. Failure Mode and Effects Analysis (FMEA) Handbook. Automotive Industry Action Group & Verband der Automobilindustrie; 2019. Available from https://www.aiag.org/training-and-resources/manuals/details/FMEAAV-1.
21. Berríos-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, Kelz RR; CDC. Healthcare Infection Control Practices Advisory Committee. Centers for disease control and prevention guideline for preventing surgical site infection, 2017. JAMA Surg. 2017;152:784–791. doi:10.1001/jamasurg.2017.0904
22. Stone PW, Larson E, Kawar LN. A systematic audit of economic evidence linking nosocomial infections and infection control interventions: 1990-2000. Am J Infect Control. 2002;30(3):145–152. doi:10.1067/mic.2002.121099
23. Rosenthal VD, Bijie H, Maki DG, et al. International nosocomial infection control consortium (INICC) report, data summary of 36 countries, for 2004-2009. Am J Infect Control. 2012;40(5):396–407. doi:10.1016/j.ajic.2011.05.020
24. Chudleigh J, Fletcher M, Gould D. Infection control in neonatal intensive care units. J Hosp Infect. 2005;61(2):123–129. doi:10.1016/j.jhin.2005.02.017
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.