Back to Journals » Clinical and Experimental Gastroenterology » Volume 7
Potentiated clinoptilolite: artificially enhanced aluminosilicate reduces symptoms associated with endoscopically negative gastroesophageal reflux disease and nonsteroidal anti-inflammatory drug induced gastritis
Authors Potgieter W, Samuels CS, Snyman J, Laurens I
Received 8 July 2013
Accepted for publication 27 January 2014
Published 1 July 2014 Volume 2014:7 Pages 215—220
DOI https://doi.org/10.2147/CEG.S51222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Wilna Potgieter, Caroline Selma Samuels, Jacques Renè Snyman
Department of Pharmacology, School of Medicine, Faculty of Health Sciences, University of Pretoria, Pretoria, Gauteng, South Africa
Purpose: The cation exchanger, a potentiated clinoptilolite (Absorbatox™ 2.4D), is a synthetically enhanced aluminosilicate. The aim of this study was to evaluate the possible benefits of a potentiated clinoptilolite as a gastroprotective agent in reducing the severity of clinical symptoms and signs associated with 1) endoscopically negative gastroesophageal reflux disease (ENGORD) and 2) nonsteroidal anti-inflammatory drug (NSAID) medication.
Methods and patients: Two randomized, double-blind, placebo-controlled, pilot studies, the ENGORD and NSAID studies, were conducted. After initial negative gastroscopy, a total of 25 patients suffering from ENGORD were randomized to receive either placebo capsules or 750 mg Absorbatox twice daily for 14 days. The NSAID study recruited 23 healthy patients who received orally either 1,500 mg Absorbatox or placebo three times daily, plus 500 mg naproxen twice daily. Patients underwent gastroscopic evaluation of their stomach linings prior to and on day 14 of the study. Gastric biopsies were obtained and evaluated via the upgraded Sydney system, whereas visible gastric events and status of the gastric mucosa were evaluated via a 0–3 rating scale. During both studies, patients recorded gastric symptoms in a daily symptom diary.
Results: In the ENGORD study, patients who received the potentiated clinoptilolite reported a significant reduction (P≤0.05) in severity of symptoms including reduction in heartburn (44%), discomfort (54%), and pain (56%). Symptom-free days improved by 41% compared to the group who received placebo (not significant). This was over and above the benefits seen with the proton pump inhibitor. In the NSAID study, the reduction in gastric symptom severity was echoed in the group who received the potentiated clinoptilolite. Treatment with the potentiated clinoptilolite resulted in significant prevention (P≤0.05) of mucosal erosion severity as graded by the gastroenterologist.
Conclusion: Absorbatox is a nonabsorbable aluminosilicate with potential gastroprotective benefits as it protected against ENGORD symptoms and NSAID-induced gastric events. The exact mechanism of action is not clear but may be due to its binding to hydrogen ions and biologically active amines and nitrates.
Keywords: cation exchanger, gastro-protective agent, endoscopy, zeolite
Introduction
Gastrointestinal related disturbances
Dyspepsia-associated symptoms significantly reduce patients’ quality of life; this is in spite of many acid-reducing and other gastroprotective agents being used as either prescription- or self-medication. Heartburn is a debilitating disease that not only influences the quality of life of patients, but also has a great impact on health system costs. It has been shown that up to 81% of patients suffering from heartburn may be diagnosed positively with gastroesophageal reflux disease (GORD).1 Patients suffering from GORD can either be classified as being endoscopically negative or positive after upper gastrointestinal endoscopic evaluation. Patients with endoscopically negative GORD (ENGORD) experience heartburn symptom severity and decrements in their quality of life comparable to patients with erosive esophagitis.2 Patients suffering from occasional heartburn usually self-medicate with antacids for symptomatic relief. The aim of therapy is to improve quality of life of patients suffering from heartburn manifesting from GORD.3 Treatment regimens usually depend on the severity and intensity of symptoms.4 The use of proton pump inhibitors (PPIs) has become the gold standard in practice with the majority of patients responding well to treatment (ie, with or without erosive esophagitis).5 The “treat as needed” approach with PPIs is suitable for younger patients who suffer from nonerosive esophagitis. These patients may not experience heartburn on a daily basis and require a PPI only when experiencing episodes of heartburn.
PPIs reduce the symptoms of dyspepsia commonly associated with nonsteroidal anti-inflammatory drug (NSAID) treatment. They also diminish ulcer formation in these patients using NSAIDs; however, they have the potential to result in drug–drug interactions, especially in patients taking multiple agents for comorbid conditions, and may also impact negatively on the health status of some vulnerable patients purely because of the reduction in intragastric pH, increasing the vulnerability of the mucosa. Some evidence suggests an association between protracted PPI use and osteoporosis as well as lung infections.6,7 There is, therefore, a need for safer, affordable, and more accessible (self-medication) products able to protect at-risk patients against suffering GORD- and NSAID-induced dyspepsia without drug–drug interactions with no effect on intestinal flora.
The many uses of hydrated aluminosilicate crystals in both industry and agriculture are attributable to their three-dimensional structure, which endows them with specific physicochemical properties including: ion exchange capacity, adsorbent nature, size exclusion frame work, as well as catalytic properties.8–12 Additionally, they have been claimed to exhibit diverse biological activities, which may include uses such as adjuvant therapy to anticancer therapy, adjuvant for vaccines, treatment of heartburn, and as antidiarrheal agents.11 Various studies have shown that hydrated aluminosilicates have no toxic effects both in humans and in animals.13–18
Absorbatox™ (Absorbatox (Pty) Ltd, Centurion, Gauteng, South Africa), the specific clinoptilolite used in this research, is a designer product able to exchange specific types of molecules. It may also bind biologically active amines such as luminal excreted amines in the stomach, which are associated with gastric acid stimulation such as histamine. Furthermore, it is an ion exchange agent, which makes it a possible substance to reduce gastric pH and provide symptomatic relief of heartburn.19
The aim of this study was therefore to investigate, in two different but related conditions, the gastroprotective efficacy of the potentiated clinoptilolite: 1) relieving clinical symptoms such as heartburn, discomfort, and pain in patients suffering from ENGORD (acidic reflux in a nonresistant mucosa) and 2) protecting the gastric mucosa by limiting the NSAID-induced erosions and ulcer formation (NSAID-related inhibition of normal protective prostaglandins resulting in a vulnerable mucosa).
Material and methods
Absorbatox
Absorbatox is a synthetically enhanced hydrated aluminosilicate that falls under the zeolite family. It is a unique aluminosilicate crystal with properties differentiating it from other aluminosilicates, due to its patented process resulting in a higher cation exchange capacity and specific size exclusion frame (through manipulating the pore size); ie, higher than what can be achieved by only soaking it in brine. These clinoptilolite crystals so achieved have a well-defined, microporous, crystalline structure, which carries an excessive negative charge, usually compensated for by cations.20 Void spaces within the frameworks, 3 to 10 Å in diameter, are capable of hosting cations, water, or other organic molecules, which can then be selectively exchanged for other species depending on charge and affinity.21
ENGORD study
A double-blind, randomized, placebo-controlled (two parallel arms) trial was performed. Approval was obtained from the Ethics Committee of the University of Pretoria. A total of 25 patients over the age of 18 years old who had been suffering from heartburn at least three times a week for a period of at least 3 months and who, after endoscopy, were diagnosed with ENGORD, were enrolled after signing informed consent. Patients with peptic ulcer disease, erosive esophagitis (lesion according to the Los Angeles classification system22), mucosal breaks due to use of NSAIDs, Barrett’s esophagitis, those using concomitant medication, smoking, and pregnant or lactating females were excluded before enrollment. Selected patients had to be otherwise healthy with no concomitant diseases and had to be on a stable diet for the period of the study.
Treatment was randomized by means of computer-generated randomization numbers. Twenty-five adult (18 years and older) patients, after endoscopy who were diagnosed with ENGORD, were enrolled to receive either placebo or active clinoptilolite capsules (750 mg) three times daily for a period of 14 days. Placebo and active capsules were identical and manufactured by Absorbatox (Pty) Ltd. Thirteen patients were randomized to receive Absorbatox and 12 to receive placebo. Patients were assessed on number of heartburn episodes, discomfort, pain, symptom-free days, and use of rescue medication by means of questionnaires and a visual analog scale. All was documented in a patient diary. These questionnaires were simplified from the literature and patients had only to indicate the number of episodes of heart burn per day or rescue medication used (reflective in the evening, counting the night as the next day); all other aspects were scored on a 100 mm visual analog scale line indicating the severity of heart burn or indigestion specified as discomfort and pain.23,24 Patients were trained as how to score by the same investigator upon recruitment. PPI (Nexiam: esomeprazole 20 mg, Astra Zeneca, London, UK) was provided as rescue medication as part of on-demand therapy for all patients.
Statistical analyses were done by means of an unpaired t-test at 95% confidence interval (Gaussian distribution of all data was confirmed).
NSAID study
In this 14-day, double-blind, placebo-controlled, pilot study, 23 healthy nonsmoking volunteers over the age of 18 years (18–24 years) were enrolled. Approval to conduct the study was granted by the Ethics Committee of the University of Pretoria. Persons with existing peptic ulcers, those using NSAID medication, PPIs, histamine-2 receptor antagonist, sucralfate, or any other medication except oral contraception at the time of enrollment, and pregnant or breast feeding females were excluded. All volunteers had to be healthy and were screened by physical examination to confirm their health status before commencing the study. They had to follow a standard diet for the duration of the study and had to abstain from alcohol use for the duration of the study (14 days). Volunteers were randomized to receive orally either 1,500 mg active clinoptilolite (n=11) or placebo (n=12) three times daily, plus 500 mg naproxen (Aspen Pharmacare; Durban, South Africa) twice daily 1–2 hours before or after the study treatment to eliminate the possibility of drug interactions. Active clinoptilolite and placebo were packed in identical indistinguishable capsules by the manufacturer, Absorbatox (Pty) Ltd. Naproxen has been used as a comparator NSAID in evaluating the clinical benefits of COX-2 inhibitors such as rofecoxib and meloxicam.23,24 NSAIDs such as naproxen are known to cause nonsymptomatic mucosal breaks in almost 80% of patients in a short exposure period of 14 days.24 The COX-2 inhibitors have significantly fewer of these, mostly asymptomatic ulcers/erosions, hence the selection of naproxen as offending drug (NSAID causing ulceration) in this pilot study.24
All healthy volunteers underwent gastroscopic evaluation of their stomach linings prior to and on day 14 of the study to evaluate gastric events and the status of the gastric mucosa. They also had a physical examination by a clinician prior to both procedures and at a 1-week follow-up at end of the study. No abnormalities were detected on recruited volunteers.
Gastric biopsies were taken from each patient at the first gastroscopy (day 0) and on the last day of treatment (ie, day 14 gastroscopy). An independent histopathologist evaluated the biopsies by means of the upgraded Sydney system, taking into account activity, inflammation, Helicobacter pylori presence, atrophy, and intestinal metaplasia. Visual endoscopic evaluation of gastric mucosa was done by an independent gastroenterologist. The severity of gastric erosions was scored by means of a 0–3 rating scale: 0= none; 1= erosion size ≤1 mm; 2= erosion size 2–5 mm; 3= erosion size ≥5 mm.
Both of these researchers were blinded to the drug treatment arms. Patients also completed a daily symptom diary.
Statistical analyses were done by means of Wilcoxon signed-rank test.
Results
ENGORD study
A total of five out of 25 patients did not complete the study successfully. Three patients did not return on their scheduled visits, of which two received placebo and one received potentiated clinoptilolite, and two patients gave notice of withdrawal without reason (both received potentiated clinoptilolite). Data from a total of ten patients in each group were analyzed. Results are summarized in Table 1. Treatment with potentiated clinoptilolite significantly reduced the number of heartburn episodes (44% reduction), discomfort (54% reduction), and pain (56% reduction) in patients with ENGORD (P<0.05) when compared to the placebo group. The average symptom-free days during the study period was reported to be 41% less in the potentiated clinoptilolite treated group when compared to the placebo group, however, this was not significant. It was reported that seven patients in the placebo group and six in the group receiving the potentiated clinoptilolite used rescue medication (PPI) at some stage during the 14-day study period. Adverse events are summarized in Table 2.
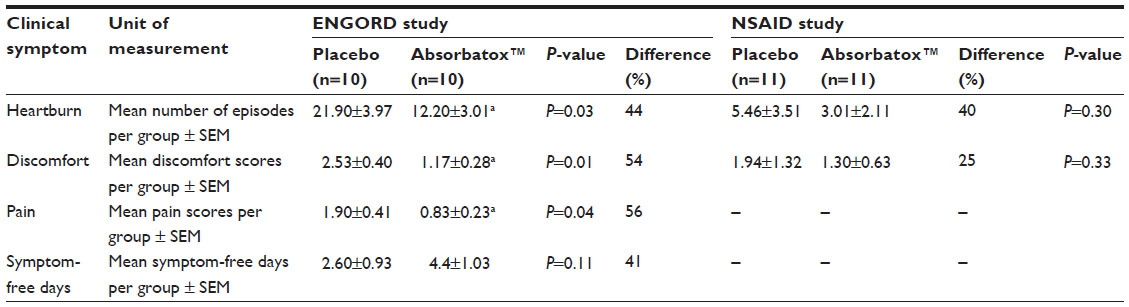 | Table 1 Severity of clinical symptoms recorded in a daily symptom diary for 14 consecutive days by volunteers participating in the ENGORD and NSAID pilot studies |
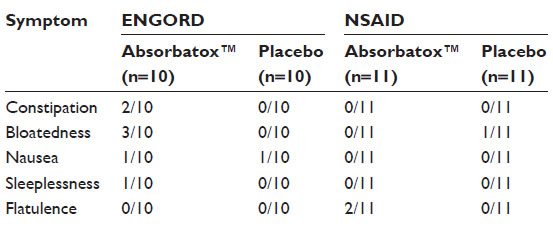 | Table 2 Indicating side effects reported by volunteers during both studies |
NSAID study
Of the 23 enrolled healthy volunteers, one volunteer in the placebo group did not complete the study due to unexplained personal reasons. Twenty-two patients completed the study. Biopsy analysis revealed no significant difference in the severity of gastritis or presence of H. pylori when comparing the diagnosis obtained for the two treatment groups prior to and after the study period (data not shown). However, there was a visibly significant increase in erosion severity in the group that received placebo (0.05±0.05 before and 0.77±0.30 after; P=0.03; Wilcoxon signed-rank test). It was found that the increase in erosion severity in the potentiated clinoptilolite treated group was 44% less when compared to that of the placebo treated group (0.05±0.05 before and 0.45±0.20 after; P=0.06; Wilcoxon signed-rank test) (Figure 1). Typical NSAID-induced erosions were visible in the placebo treated group at the end of the study (Figure 2).
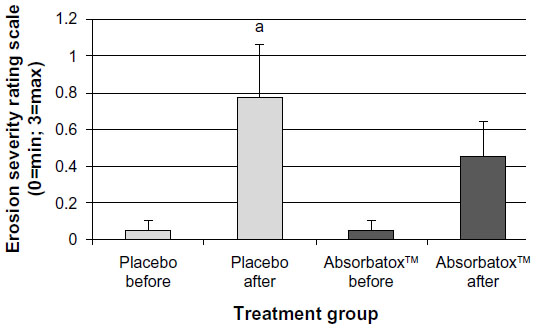 | Figure 1 Erosion severity induced by naproxen in the placebo and Absorbatox™ treated groups. |
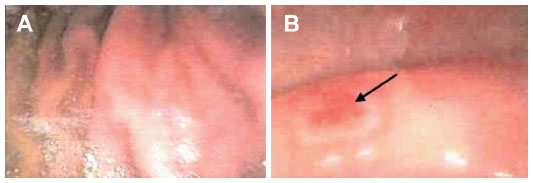 | Figure 2 (A) Normal stomach lining of volunteer after first endoscopic evaluation; (B) endoscopic image taken after the study period. |
Furthermore, data obtained from the volunteers’ symptom diary cards exhibited that the potentiated clinoptilolite resulted in superior prevention of discomfort of heartburn and dyspepsia associated with NSAID use when compared to the placebo treated group, however, this was not statistically significant (Table 1). Pertaining to adverse events, two volunteers that received the potentiated clinoptilolite experienced flatulence and one volunteer in the placebo group complained of bloatedness (Table 2).
Discussion
The results of the ENGORD study indicate the potential for use of the potentiated clinoptilolite in the treatment of non-complicated GORD. Results obtained from this study demonstrate overall clinical improvement in several of the study outcome scores; including heartburn, discomfort, and pain. The exact mechanism of action of the potentiated clinoptilolite was not elucidated in this study, but may be ascribed to hydrogen ion trapping, and enzyme and amine binding properties.
The main outcome in the NSAID study was achieved in that the potentiated clinoptilolite resulted in gastroprotection, thereby reducing the severity of erosions induced by naproxen. Heartburn and discomfort symptom reduction echoed the findings of the ENGORD study. It is possible that the effect is due to simple binding of the offending H+ ions and pepsin (confirmed in vitro) on the gastric mucosa.20 It is also possible that the potentiated clinoptilolite binds to amines such as histamine (confirmed in vitro), thereby limiting the extent of collateral tissue damage. The cation exchange on the luminal surface of the stomach has an intricate balance and the relative concentrations on the surface of either sodium or hydrogen determines the secretion of the other (autoregulation). Cation exchangers such as this activated clinoptilolite may actually function like a regulator of this system by donating sodium and capturing hydrogen and by so doing reduce the impact of free hydrogen on the surface without effecting the pH.25
It has further been suggested that intraluminal enterobacteria play a significant role in the pathogenesis and lesion formation of gastrointestinal damage induced by NSAIDs.26,27 Antibacterial and antiviral properties of the potentiated clinoptilolite may also be responsible for the reduction of gastric events.28–30
Although the sample sizes of both studies were small, the magnitude of effect is evidence of efficacy and therefore warrants evaluation in a larger Phase III study. Activated clinoptilolite is a nonabsorbable substance with potential benefit in reducing GORD-associated clinical symptoms and protecting against NSAID-induced erosions. Activated clinoptilolite is effective by possibly binding the offending H+ ions and binding to biologically active substances such as histamine.
Conclusion
Absorbatox is a nonabsorbable aluminosilicate with potential gastroprotective benefits as it protected against ENGORD symptoms and NSAID-induced gastric events. The exact mechanism of action is not clear but may be due to its binding to hydrogen ions and biologically active amines and nitrates.
Acknowledgments
The authors would like to thank Dr Johan van Den Bogaerde, Gastroenterologist at Unitas Hospital, Centurion, Gauteng, South Africa, for performing and evaluating endoscopies and AMPATH/Drs Du Buisson, Bruinette, Kramer Inc. Pretoria Anatomical Pathology, Pretoria, Gauteng, South Africa for evaluating gastric biopsies.
Disclosure
Study finance was provided by Absorbatox (Pty) Ltd. The authors report no other conflicts of interest in this work.
References
Müller-Lissner S, Klauser A. [Diseases of the esophagus. Modern functional evaluations]. Internist Berl. 1990;31(2):85–93. German. | |
Tack J, Fass R. Review article: approaches to endoscopic-negative reflux disease: part of the GERD spectrum or a unique acid-related disorder? Aliment Pharmacol Ther. 2004;19 Suppl 1:28–34. | |
Dimenäs E, Carlsson G, Glise H, Israelsson B, Wiklund I. Relevance of norm values as part of the documentation of quality of life instruments for use in upper gastrointestinal disease. Scand J Gastroenterol Suppl. 1996;221:8–13. | |
van Pinxteren B, Numans ME, Bonis PA, Lau J. Short-term treatment with proton pump inhibitors, H2-receptor antagonists and prokinetics for gastro-oesophageal reflux disease-like symptoms and endoscopy negative reflux disease. Cochrane Database Syst Rev. 2006;(3):CD002095. | |
Rang HP, Dale MM, Ritter JM, et al. Rang and Dale’s Pharmacology. 6th ed. London: Churchill Livingstone Elsevier; 2004. | |
Mazziotti G, Canalis E, Giustina A. Drug-induced osteoporosis: mechanisms and clinical implications. Am J Med. 2010;123(10):877–884. | |
Hermos JA, Young MM, Fonda JR, Gagnon DR, Fiore LD, Lawler EV. Risk of community-acquired pneumonia in veteran patients to whom proton pump inhibitors were dispensed. Clin Infect Dis. 2012;54(1):33–42. | |
Flanigan EM. Molecular sieve zeolite technology – the first twenty-five years. In: Rees LVC, editor. Proceedings of the Fifth International Conference on Zeolites, Naples, Italy, 2–6 June 1980. London: Heyden; 1980:760–780. | |
Sersale R. Natural zeolites: processing, present and possible applications. Stud Surf Sci Catal. 1985;24:503–512. | |
Naber JE, de Jong KP, Stork WHJ, Kuipers HPCE, Post MFM. Industrial applications of zeolite catalysts. Stud Surf Sci Catal. 1994;84:2197–2219. | |
Garces JM. Observations on zeolite applications. In: Treacz MMJ, Marcus BK, Misher ME, Higgens JB, editors. Proceedings of the 12th International Conference on Zeolites. Warrendale: Materials Research Society; 1999:551–566. | |
Colella C. Natural zeolites in environmentally friendly processes and applications. Stud Surf Sci Catal. 1999;125:641–655. | |
Rodríguez-Feuntes G, Denis AR, Barrios Álvarez MA, Colarte AI. Antacid drug based on purified natural clinoptilolite. Microporous Mesoporous Mater. 2006;94(1–3):200–207. | |
Kyriakis SC, Papaioannou DS, Alexopoulos C, Polizopoulouc Z, Tzikaa ED, Kyriakisa CS. Experimental studies on safety and efficacy of the dietary use of a clinoptilolite-rich tuff in sows: a review of recent research in Greece. Microporous Mesoporous Mater. 2002;51(1):65–74. | |
Olver MD. Effect of feeding clinoptilolite (zeolite) on the performance of three strains of laying hens. Br Poult Sci. 1997;38(2):220–222. | |
Rodríguez-Fuentes G. Enterex: anti-diarrheic drug based on purified natural clinoptilolite. Zeolites. 1997;19(5–6):441–448. | |
Pond WG, Yen JT, Crouse JD. Tissue mineral element content in swine fed clinoptilolite. Bull Environ Contam Toxicol. 1989;42(5):735–742. | |
Gloxhuber C, Potokar M, Pittermann W, et al. Zeolithe A – A phosphate substitute for detergents: toxicological investigation. Food Chem Toxicol. 1983;21(2):209–220. | |
Breck DW. Crystalline molecular sieves. J Chem Educ. 1964;41(12):678–689. | |
Seetharam G, Saville BA. L-Dopa production from tyrosinase immobilized on zeolite. Enzyme Microb Technol. 2002;31(6):747–753. | |
Pavelić K, Hadzija M, Bedrica L, et al. Natural zeolite clinoptilolite: new adjuvant in anticancer therapy. J Mol Med (Berl). 2001;78(12):708–720. | |
Nasseri-Moghaddam S, Razjouyan H, Nouraei M, et al. Inter- and intra-observer variability of the Los Angeles classification: a reassessment. Arch Iran Med. 2007;10(1):48–53. | |
Choi HK, Seeger JD, Kuntz KM. Effects of rofecoxib and naproxen on life expectancy among patients with rheumatoid arthritis: a decision analysis. Am J Med. 2004;116(9):621–629. | |
Speight TM, Holford NHG. Avery’s Drug Treatment. 4th ed. Auckland: Adis International Limited; 1997. | |
Allen A, Garner A. Mucus and bicarbonate secretion in the stomach and their role in mucosal protection. Gut. 1980;21(3):249–262. | |
Lanas A, Scarpignato C. Microbial flora in NSAID-induced intestinal damage: a role for antibiotics? Digestion. 2006;73 Suppl 1:136–150. | |
Chan FKL, Graham DY. Prevention of non-steroidal anti-inflammatory drug gastrointestinal complications – review and recommendations based on risk assessment. Aliment Pharmacol Ther. 2004;19(10):1051–1061. | |
Takai K, Ohtsuka T, Senda Y, et al. Antibacterial properties of antimicrobial-finished textile products. Microbiol Immunol. 2002;46(2):75–81. | |
Vezirov AN, Sadykhova FE. [Comparative characteristics of the adsorption properties of natural sorbents in relation to influenza viruses]. Gig Sanit. 1982;(9):90–91. Russian. | |
Goncharuk EI, Shirobokov VP, Salata OV. [Principles of sorption purification of sewage water contaminated by bacteria and viruses]. Gig Sanit. 1990;(7):18–20. Russian. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.