Back to Journals » Clinical Interventions in Aging » Volume 20
Potentially Inappropriate Medication and Associated Factors Among Older Patients with HIV/AIDS: A Multicenter Cross-Sectional Study
Authors Li J, Hong D, Dong J, Zhao Q, Wang H ![]()
Received 4 February 2025
Accepted for publication 19 July 2025
Published 30 July 2025 Volume 2025:20 Pages 1155—1164
DOI https://doi.org/10.2147/CIA.S519649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Jia Li,1 Dongsheng Hong,2 Jiankun Dong,1 Qingwei Zhao,2 Hongmei Wang1
1Department of Pharmacy of the First Affiliated Hospital, and Department of Social Medicine of School of Public Health, Zhejiang University School of Medicine, Hangzhou, 310058, People’s Republic of China; 2Department of Clinical Pharmacy, Zhejiang Provincial Engineering Center for Innovative Drug Clinical Research and Application, Zhejiang Provincial Key Laboratory of Traditional Chinese Medicine for Clinical Evaluation and Translational Research, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310006, People’s Republic of China
Correspondence: Hongmei Wang, Department of Pharmacy of the First Affiliated Hospital, and Department of Social Medicine of School of Public Health, Zhejiang University School of Medicine, Hangzhou, 310058, People’s Republic of China, Tel +86 0571 88208222, Email [email protected] Dongsheng Hong, Department of Clinical Pharmacy, Zhejiang Provincial Engineering Center for Innovative Drug Clinical Research and Application, Zhejiang Provincial Key Laboratory of Traditional Chinese Medicine for Clinical Evaluation and Translational Research, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310006, People’s Republic of China, Tel +86 13857180186, Email [email protected]
Purpose: This study sought to characterize the prevalence, patterns, and associated risk factors for Potentially Inappropriate Medication use among older patients living with HIV/AIDS. The ultimate goal of this study is to inform strategies to increase medication safety in this vulnerable population.
Patients and Methods: Using the 2023 American Geriatrics Society Beers Criteria, we performed a comprehensive retrospective analysis of medication use patterns among HIV/AIDS patients aged ≥ 65 years, drawing data from 21 hospitals across eight Chinese cities between 2019 and 2023. The analytical framework incorporated descriptive statistics, negative binomial regression for trend analysis, and multivariable logistic regression to evaluate PIM prevalence and identify associated risk factors.
Results: The analysis included 2,642 patients (80.28% male; median age 71 years, IQR: 67~75). The PIM prevalence was 23.20% (613/2,642) in the cohort, with medications contraindicated in older adults constituting the largest category (51.87%), followed by disease-related PIMs (19.88%) and medications requiring cautious use (27.80%). Type 3 PIMs demonstrated a consistent and statistically significant downward trend throughout the study period (P< 0.001). Conversely, using a single PIM exhibited a statistically significant upward trajectory (P=0.020). In multivariate modeling, polypharmacy emerged as the strongest predictor of PIM use (adjusted OR=9.05, 95% CI: 7.20~11.38), followed by hospitalization (adjusted OR=1.38, 95% CI: 1.05~1.80), with consistent associations observed across the 65~84 year age range (all P< 0.05).
Conclusion: The substantial and increasing burden of PIM use among elderly patients living with HIV/AIDS underscores the urgent need for enhanced medication oversight. Targeted intervention strategies should prioritize patients with polypharmacy, those requiring hospitalization, and those with specific age demographics.
Keywords: potentially inappropriate medications, HIV/AIDS, beers criteria, polypharmacy, elderly patients
Introduction
China faces significant demographic challenges due to its rapidly aging population, characterized by a continuous increase in the number of residents aged 65 years and older. Concurrently, the proportion of elderly individuals living with human immunodeficiency virus (HIV) continues to rise.1,2 According to the Chinese Center for Disease Control and Prevention, by the end of 2022, mainland China reported 1.223 million people living with HIV/AIDS (acquired immunodeficiency syndrome), with a notable increase in elderly patients since 2008. The national prevalence among the elderly population reached 1.68% (95% CI: 1.00%~2.79%).3 The “graying” of the HIV epidemic presents unique challenges globally and in China, as older PLWH experience a higher burden of age-related comorbidities, leading to complex polypharmacy and an elevated risk of drug–drug interactions (DDIs).4 Particularly concerning are interactions between antiretroviral medications and drugs commonly prescribed for chronic conditions, such as statins, antidepressants, and proton pump inhibitors. Age-related physiological changes, such as altered renal and hepatic function, further impact pharmacokinetics and pharmacodynamics, predisposing older PLWH to incorrect dosing and potentially inappropriate prescribing.5
Potentially inappropriate medication (PIM) refers to medications where the potential risks outweigh the expected clinical benefits, particularly when safer, more effective therapeutic alternatives exist for the same condition.6,7 PIMs are strongly associated with adverse health outcomes, potentially leading to clinical deterioration, increased risk of hospital readmission, and elevated mortality rates among older adults.8 Elderly individuals living with HIV often manage multiple chronic conditions requiring complex medication regimens, significantly complicating the achievement of optimal pharmacotherapy.9 Furthermore, PIMs contribute to increased healthcare system burden through adverse drug reactions and elevated readmission rates.10 In China, PIM is a growing concern in the general elderly population, with studies reporting prevalence rates of 10% to 30% in community-dwelling older adults.11,12 However, data on PIM among older patients living with HIV/AIDS in China are scarce, with no prior multicenter studies examining this issue.
Given these concerns, we conducted a multicenter cross-sectional study of HIV/AIDS patients aged 65 years and older utilizing the 2023 American Geriatrics Society Beers Criteria to assess PIM prevalence and associated risk factors. This study aims to provide evidence-based recommendations for improving medication safety and quality of care for older patients living with HIV/AIDS.
Methods
Study Design and Data Source
Drawing from the Chinese Hospital Prescription Analysis Cooperative Project (CHPACP), we conducted a retrospective analysis of prescription patterns among HIV/AIDS patients aged ≥65 years across 21 hospitals in eight Chinese cities from 2019 to 2023.12–14 This project aims to analyze hospital prescription data in China and the database for this project has been widely used.15 This well-established pharmacoepidemiological database employs systematic random sampling, collecting prescription data from two nonconsecutive Monday-to-Friday periods per quarter, totaling 10 working days, to ensure representative temporal coverage. Each prescription record contains comprehensive data, including prescription identifiers, institutional codes, prescription dates, clinical department affiliations, patient demographics (age and sex), diagnostic information, and detailed medication records (including generic names, formulations, dosages, frequencies and routes of administration, and medication costs). Inclusion Criteria: (1) Diagnosis includes HIV/AIDS, regardless of clinical disease stage; (2) Age ≥65 years, no gender restrictions. Exclusion Criteria: (1) Prescriptions missing patient age or gender; (2) Prescriptions with unclear diagnostic information. The study protocol was approved by the Institutional Review Board of the First Affiliated Hospital, Zhejiang University School of Medicine (Ethics approval: 2024–0807-Fast) and registered with the Chinese Clinical Trial Registry (ChiCTR2400089432). Recognizing the sensitive nature and vulnerability of the elderly HIV/AIDS population, we implemented comprehensive privacy protection protocols, ensuring complete anonymization of all patient data throughout collection and analysis. This study adheres to the reporting guidelines for observational studies (Table S1).
Definition of Potentially Inappropriate Medication and Polypharmacy
Assessment of PIM use was conducted according to the 2023 American Geriatrics Society Beers Criteria, which categorizes PIMs into four distinct domains: medications explicitly contraindicated in older adults; medications that may exacerbate existing conditions through drug‒disease or drug‒syndrome interactions; medications requiring cautious use in the geriatric population; and clinically significant drug‒drug interactions that warrant avoidance. In accordance with the established literature, polypharmacy was operationally defined as the concurrent use of five or more medications. In our study, “1 PIM” means using a single PIM, “2 PIM” means using two distinct Potentially Inappropriate Medications, “3–6 PIM” menas using multiple PIMs from three to six agents, and “Total PIM” means using at least one PIM.
Statistical Analysis
Statistical analyses were conducted via R software (version 4.3.2). Descriptive statistics are presented as medians (interquartile ranges) for continuous variables and frequencies (percentages) for categorical variables. Temporal trends in PIM incidence were evaluated via negative binomial regression models, which were selected after confirming overdispersion (θ range: 3.42~28.76, all P < 0.001). Model fit was assessed via Pearson χ²/df ratios (range: 0.82~1.31). Confidence intervals (95%) for temporal trends were derived from the asymptotic properties of regression coefficients, with standard errors computed using the inverse of the Fisher information matrix. The overall trend represents the relative percentage change from 2019 to 2023, computed by dividing the absolute change (2023 value minus 2019 value) by the 2019 baseline value and multiplying by 100.14 To elucidate patterns potentially obscured in aggregate analyses, we performed stratified analyses by PIM quantity (single, double, and ≥3 medications). Factors associated with PIM use were identified through univariate and multivariate logistic regression modeling. All analyses employed two-sided tests with significance established at P < 0.05.
Results
Overview of the Research Subjects
The study population comprised 2,642 elderly patients living with HIV/AIDS, of whom 2,121 (80.28%) were male and 521 (19.72%) were female. The median age was 71 years (interquartile range [IQR]: 67~75 years). Medication analysis revealed a median of 2 medications per patient (IQR: 1~3), with 481 patients (18.21%) meeting the criteria for polypharmacy. In terms of disease burden, 1,220 patients (46.18%) had ≤5 concurrent diagnoses, whereas 1422 (53.82%) had >5 diagnoses. The detailed baseline characteristics are presented in Table 1.
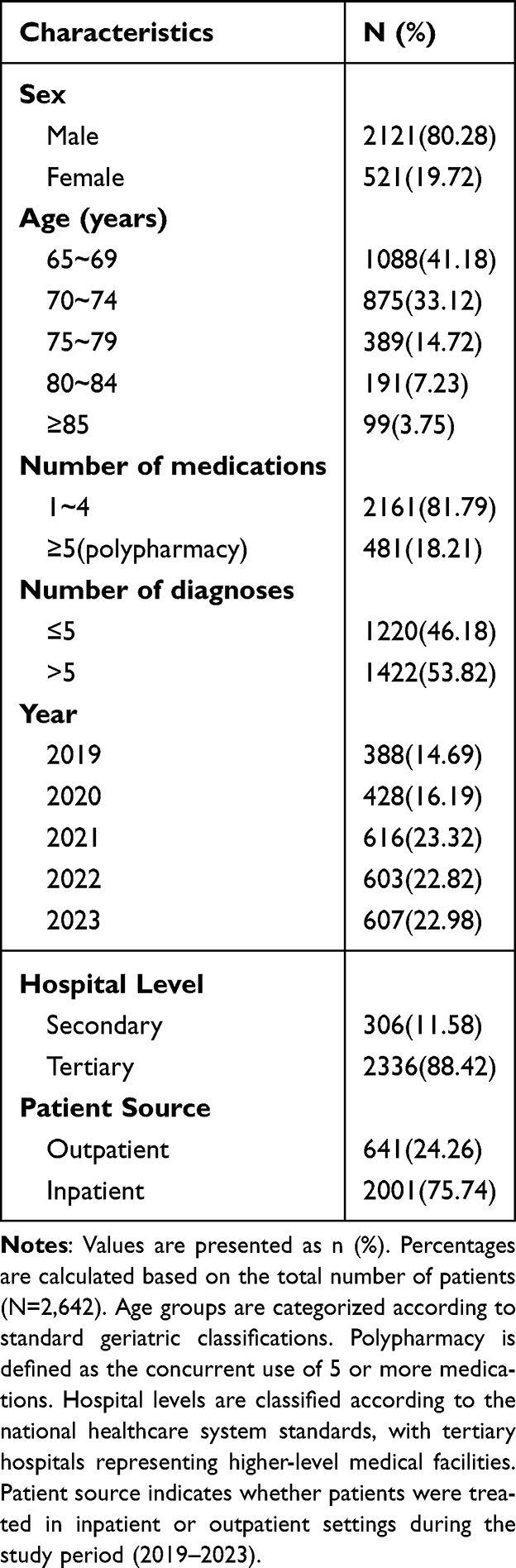 |
Table 1 Demographic and Clinical Characteristics of the Study Population (N=2,642) |
Overall Prevalence and Temporal Trends of Potentially Inappropriate Medication Use
The overall prevalence of PIM use was 23.20% (613/2,642; 95% CI: 21.62%~24.78%). Among the identified PIMs, the most frequent category was medications contraindicated in older adults (51.87%, 95% CI: 48.52%~55.22%), followed by medications requiring cautious use (27.80%, 95% CI: 24.84%~30.76%) and drug‒disease or drug‒syndrome interactions (19.88%, 95% CI: 17.26%~22.50%). Clinically significant drug‒drug interactions were relatively rare (0.47%, 95% CI: 0.01%~0.93%). Detailed data are presented in Table 2.
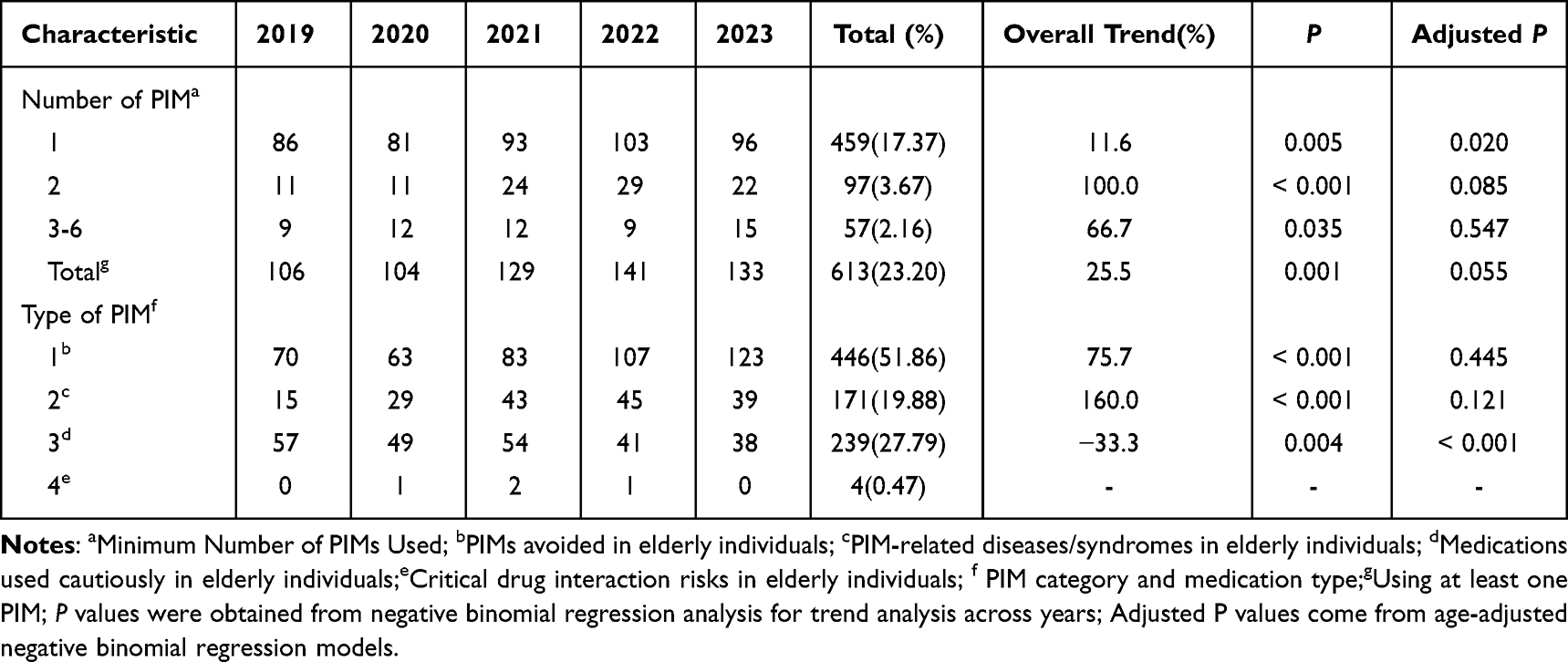 |
Table 2 Potentially Inappropriate Medications (PIMs) Occurrence and Trends from 2019–2023 |
Temporal trend analysis, conducted via negative binomial regression (validated by overdispersion testing), initially showed significant increases in unadjusted PIM use across multiple categories. However, after adjusting for age, the interpretation changed. Type 3 PIM (medications to be used with caution) showed a significant overall reduction of 33.3% from 2019 to 2023 (P=0.004), with age-adjusted significance maintained (P< 0.001). Year-over-year analysis revealed variable patterns, including decreases of 14.0% in 2020 and 24.1% in 2022, alongside increases of 10.2% in 2021. In contrast, using a single PIM demonstrated an overall increasing trend of 11.6% (P = 0.005), but the difference remained significant after age adjustment (P = 0.020), with notable year-over-year increases of 14.8% in 2021 and 10.8% in 2022. The contrast between observed growth in raw frequencies and the impact of age adjustment is particularly evident in total PIMs, where age adjustment changed the interpretation from a significant increasing trend (25.5%, P = 0.001) to a non-significant trend (P = 0.055). Detailed data are presented in Tables 2 and 3.
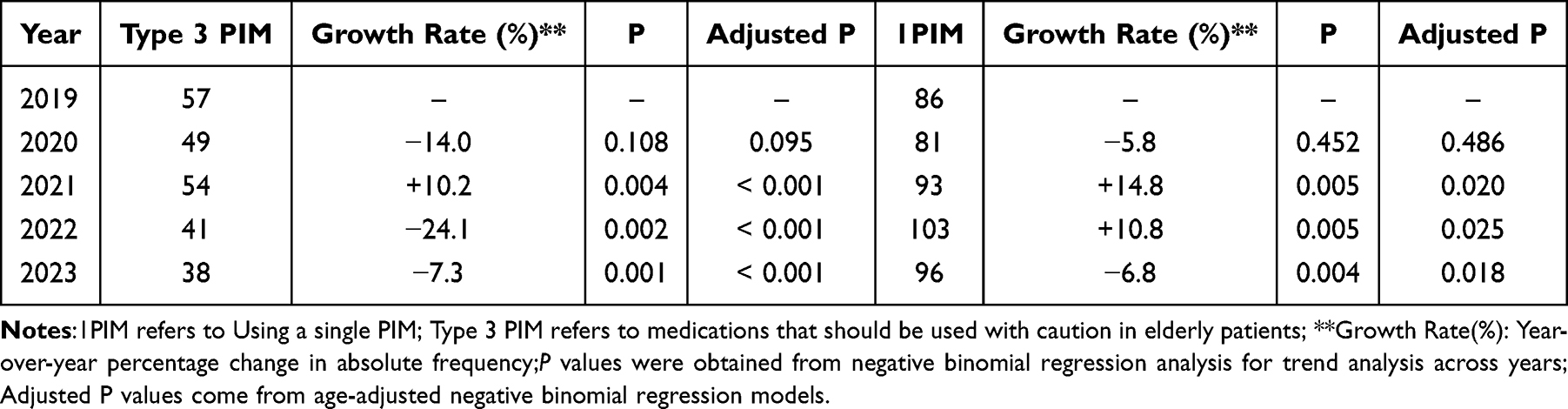 |
Table 3 Comparative Temporal Trends of PIM 1 and Type 3 PIM from 2019 to 2023 |
Patterns of Potentially Inappropriate Medication Use by Category
Detailed analysis of PIM categories (Table 4) revealed distinct patterns of inappropriate medication use. Among the PIMs that should be avoided in older adults, gastrointestinal medications were most prevalent (27.91%), followed by cardiovascular and antithrombotic agents (8.60%), central nervous system medications (4.88%), endocrine system medications (4.19%), analgesics (3.37%), and antihistamines (1.74%). In the category of drug‒disease or drug‒syndrome interactions, delirium-related medications constituted the largest proportion (12.56%), followed by medications associated with heart failure (6.40%), medications linked to fall or fracture risk (0.58%), syncope-related medications (0.23%), and medications affecting dementia or cognitive function (0.23%). Among the medications requiring cautious use, trimethoprim-sulfamethoxazole combinations were the most common (15.35%), followed by diuretics (11.40%), sodium‒glucose cotransporter-2 inhibitors (1.86%), and antidepressants (0.23%). Potentially clinically significant drug‒drug interactions were observed in 0.47% of cases, primarily involving combinations of antiepileptics, antidepressants, antipsychotics, benzodiazepines, benzodiazepine receptor agonist hypnotics, and opioids.
 |
Table 4 Potentially Inappropriate Medications Among Older Patients with HIV/AIDS |
Risk Factors for Potentially Inappropriate Medication Use
Analysis of risk factors for PIM use (Table 5) revealed several significant associations. Univariate logistic regression revealed that age (P<0.001), sex (P=0.021), number of medications (P<0.001), and treatment setting (P<0.001) were significant predictors. These variables were subsequently included in a multivariate logistic regression model, which identified polypharmacy, age, and treatment setting as independent risk factors for PIM use. Polypharmacy emerged as the strongest independent predictor, with patients taking ≥5 medications showing a substantially greater risk of PIM use than those taking 1~4 medications (adjusted OR=9.05, 95% CI: 7.20~11.38; P<0.001). Age demonstrated a significant but nonlinear association with PIM use. Compared with patients aged ≥85 years, all the other age groups presented increased risk, with the highest risk observed in the 80~84 years age group (adjusted OR=3.68, 95% CI: 1.79~7.57; P<0.001). Additionally, inpatients demonstrated a greater likelihood of PIM use than outpatients did (adjusted OR=1.38, 95% CI: 1.05~1.80, P=0.021).
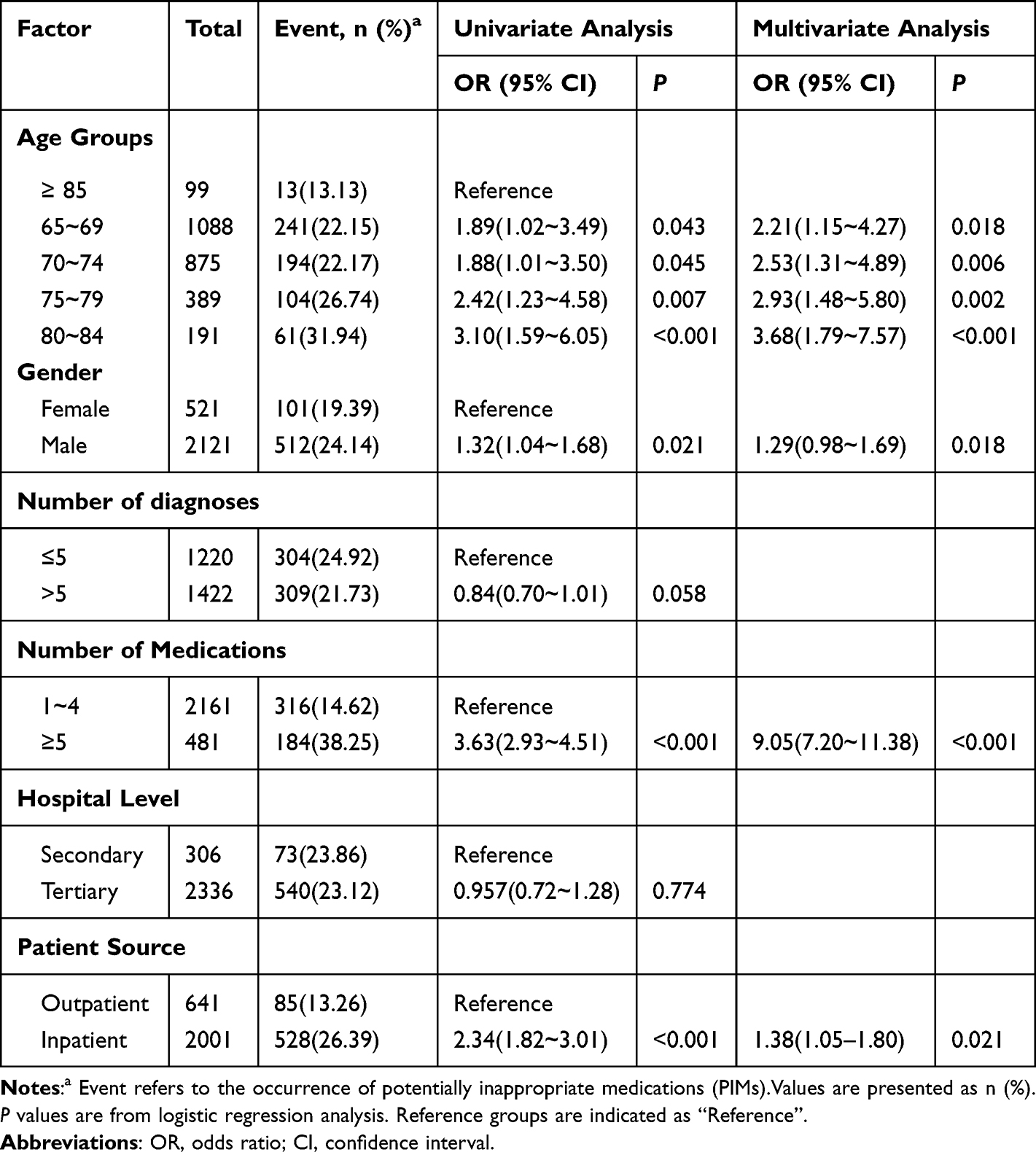 |
Table 5 Associated Factors of Potentially Inappropriate Medications Among Older Patients with HIV/AIDS |
Discussion
This multicenter cross-sectional study, encompassing 21 hospitals across eight Chinese cities, represents the first systematic evaluation of PIM patterns and associated risk factors among older patients living with HIV/AIDS in China. Our findings revealed an overall PIM prevalence of 23.20% among elderly HIV/AIDS patients. This prevalence falls within the range of 10% to 30% reported in the general elderly population in China, but is lower than the hospital-based studies of older PLWH in Spain (29.4%).11,12,16 However, this diverges significantly from a study of the American general elderly population, which reported PIM rates as high as 34.4%.10 These comparisons suggest that while PIMs are a pervasive issue across aging populations, the centralized HIV care model in China—characterized by standardized ART regimens, stringent drug interaction monitoring, and integrated comorbidity management—may partially mitigate polypharmacy risks compared to fragmented healthcare systems.17 Nevertheless, the unique challenges of HIV, including chronic inflammation, immune dysregulation, and high rates of multimorbidity, amplify susceptibility to PIM-related complications such as ART-associated hepatotoxicity and CYP3A4-mediated interactions.18 Negative binomial regression analysis, after age adjustment, demonstrated a significant 33.3% reduction in Type 3 PIMs (medications requiring cautious use) from 2019 to 2023 (P < 0.001), despite notable annual fluctuations. Conversely, using a single PIM exhibited an overall significant increase of 11.6% (P = 0.020), particularly in 2021 (14.8%) and 2022 (10.8%). The observed increase in single PIM use might be partially related to healthcare disruptions during the COVID-19 pandemic. Age adjustment altered the interpretation of total PIM trends, highlighting the influence of demographic shifts on PIM utilization. These contrasting trends between PIM categories underscore the complex interplay of factors influencing medication safety in this population and the need for ongoing monitoring and targeted interventions.
Understanding the patterns of PIM use among elderly patients living with HIV/AIDS has significant clinical and public health implications.19–21 With advances in antiretroviral therapy, HIV/AIDS has evolved into a chronic condition with substantially improved life expectancy. In China, the proportion of elderly HIV/AIDS patients continues to rise, reaching a national prevalence of 1.68% (95% CI: 1.00%~2.79%) by the end of 2022.3 This population faces not only challenges related to HIV infection but also multiple age-related chronic conditions, significantly complicating medication management. PIMs are closely associated with adverse health outcomes. Studies have demonstrated that inappropriate medication use can significantly increase the risk of adverse drug reactions, rehospitalization, and mortality among older patients. These risks may increase further in elderly patients with compromised immune function, such as those with HIV/AIDS. This is attributable to their distinctive clinical profile, encompassing chronic inflammation, immune suppression, and complex antiretroviral therapy (ART) regimens, which collectively elevate their susceptibility to drug-drug interactions and adverse drug reactions compared to the general elderly population. For instance, ART-associated toxicities and polypharmacy exacerbate the risk of PIM-related complications, such as gastrointestinal and cardiovascular events, which are less prevalent among HIV-negative elderly individuals.21 In cases of polypharmacy, drug interactions can potentially lead to more severe health complications from a health economics perspective, PIMs may substantially increase healthcare resource consumption.22,23 A systematic assessment of PIMs not only aids in identifying high-risk medication patterns but also provides evidence-based grounds for developing targeted intervention strategies, which optimizes healthcare resource allocation and reduce unnecessary medical expenditures.24 Therefore, it is critically important to conduct an in-depth investigation into the prevalence, influencing factors, and evolutionary trends of PIMs among elderly HIV/AIDS patients. Such research is essential for improving medication safety, enhancing quality of life, and reducing the healthcare burden in this vulnerable population. Moreover, this comprehensive understanding provides the necessary foundation for developing targeted prevention and intervention strategies.25
In our analysis of PIM patterns, medications that should be avoided in older adults constituted the largest category (51.87%), with gastrointestinal medications being the most prevalent (27.91%). Notably, the inappropriate use of proton pump inhibitors (PPIs) is particularly prominent, likely reflecting the common gastrointestinal symptoms in HIV/AIDS patients.26 Previous studies have demonstrated that HIV infection can directly damage the gastrointestinal mucosa, while antiretroviral therapy may also induce gastrointestinal discomfort, potentially leading clinicians to favor the prescription of PPIs.27 However, substantial evidence suggests that long-term PPI use carries significant health risks. Meta-analyses have shown strong associations between prolonged PPI use and increased fracture risk (OR=1.26, 95% CI: 1.16~1.36), vitamin B12 deficiency (OR=1.83, 95% CI: 1.36~2.46), and gut microbiota dysbiosis.28 These risks may be amplified in elderly HIV/AIDS patients with compromised immune function and reduced physiological reserve. Our findings also revealed high utilization rates of medications associated with delirium (12.56%) and heart failure (6.40%), highlighting the complex challenges in medication management for this population. The high proportion of delirium-related medications suggests potential overprescription in clinical practice, particularly given that elderly HIV patients already face an elevated risk of delirium, and certain medications used to treat delirium may paradoxically exacerbate cognitive dysfunction.29,30 Additionally, the frequent use of heart failure-related medications underscores the prevalence of cardiovascular complications in this population, attributable to both the chronic inflammatory state associated with HIV infection and the cardiac toxicity of antiviral medications.31,32
Multivariate regression analysis revealed three key independent predictors of PIM use: polypharmacy was the strongest risk factor (adjusted OR=9.05, 95% CI: 7.20~11.38), followed by inpatient status (adjusted OR=1.38, 95% CI: 1.05~1.80) and age between 65~84 years. This finding align with Tian et al’s study on age-related PIM prevalence among the general elderly population in China. For most older adults, prescription medications are generally well-accepted and may improve medication adherence. However, in individuals aged 80 years and older, the benefits of prescribing are limited, with no significant reduction in mortality, likely attributable to poorer baseline health.33 This observation may reflect enhanced prescribing caution among clinicians for the oldest-old population while also highlighting the need to further explore the nonlinear relationship between age and inappropriate medication use.
These findings have several important clinical implications. Priority should be given to patients with polypharmacy, and systematic medication reviews should be implemented to assess therapeutic necessity and optimize prescription regimens.34,35 Enhanced medication stewardship programs are needed for inpatient care, incorporating more stringent prescription review protocols. Age-stratified monitoring and intervention strategies should be developed to address heterogeneous medication risks across different age groups.36,37
This study has several notable limitations. The absence of an HIV-negative control cohort limits our ability to compare PIM prevalence directly with the general elderly population. Future studies should incorporate such a cohort to elucidate HIV-specific PIM risks. The CHPACP database does not systematically record several critical HIV clinical parameters, including viral load measurements, CD4+ T-cell counts, or duration of HIV infection since diagnosis. This limitation prevents us from conducting the comprehensive HIV disease characterization. The absence of key clinical parameters, particularly renal function indices, may have resulted in the underestimation of PIM prevalence in specific high-risk populations. The cross-sectional nature of our study limits causal inference. Our analysis did not include traditional Chinese medicines, potentially affecting the comprehensiveness of medication safety assessment in this population. Furthermore, while our age criterion of ≥65 years aligns with the Beers criteria, it may not capture medication safety patterns in the emerging cohort of HIV/AIDS patients aged 50–64 years. To address this gap in future research, we propose developing a customized screening tool specifically calibrated for HIV-positive patients in this younger elderly cohort. The development of culturally appropriate assessment tools that integrate both western and traditional Chinese medicines is also needed to increase the ecological validity of medication safety evaluations in this population.
Conclusions
This study reveals a prevalence (23.20%) of PIM use among older Chinese patients living with HIV/AIDS, with several substantial risk factors. Polypharmacy emerged as the most potent independent risk factor for PIM use, with additional considerable associations observed for inpatient treatment setting and specific age groups within the elderly population. These findings underscore the complexity of medication management in this vulnerable population and emphasize the need for geriatric-focused medication practices to inform the development of targeted intervention strategies for optimizing pharmacotherapy.
Data Sharing Statement
This study was preregistered in the Chinese Clinical Trial Registry (ChiCTR2400089432). Summary data used in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was reviewed and approved by the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (approval number: 2024-0807-Fast). The study was conducted in strict accordance with the ethical principles of the Declaration of Helsinki. This study applied retrospective data for evaluation, without involving personal privacy or commercial interests, and was exempted by the ethics committee from obtaining informed consent from patients.
Acknowledgments
We thank the Chinese Hospital Prescription Analysis Collaboration Group (CHPACP) for their assistance with our research. We thank all participating hospitals and staff members for their support in data collection and execution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any external funding.
Disclosure
The authors declare no conflicts of interest. They are responsible for the content and writing of the article and have approved the final manuscript for submission. All authors agree to be accountable for the accuracy and integrity of the work.
References
1. Laybohr Kamara I, Wang L, Guo Y, et al. Spatial-temporal heterogeneity and determinants of HIV prevalence in the Mano River Union countries. Infect Dis Poverty. 2022;11(1):116. doi:10.1186/s40249-022-01036-1
2. Xing J, Y-g L, Tang W, et al. HIV/AIDS epidemic among older adults in China during 2005–2012: results from trend and spatial analysis. Clinl Infect Dis. 2014;59(2):e53–e60. doi:10.1093/cid/ciu214
3. Dou Z, Luo Y, Zhao Y, Zheng X, Han M. Trends in Mortality and Prevalence of Reported HIV/AIDS Cases - China, 2002-2021. China CDC Wkly. 2023;5(42):943–947. doi:10.46234/ccdcw2023.177
4. Livio F, Marzolini C. Prescribing issues in older adults living with HIV: thinking beyond drug-drug interactions with antiretroviral drugs. Ther Adv Drug Saf. 2019;10:2042098619880122. doi:10.1177/2042098619880122
5. Sun C, Li J, Liu X, et al. HIV/AIDS late presentation and its associated factors in China from 2010 to 2020: a systematic review and meta-analysis. AIDS Res Ther. 2021;18(1):96. doi:10.1186/s12981-021-00415-2
6. Levy HB. Polypharmacy reduction strategies: tips on incorporating American geriatrics society beers and screening tool of older people’s prescriptions criteria. Clin Geriatr Med. 2017;33(2):177–187. doi:10.1016/j.cger.2017.01.007
7. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
8. McCarthy C, Moriarty F, Wallace E, Smith SM. Barbara Clyne for the SST. The evolution of an evidence based intervention designed to improve prescribing and reduce polypharmacy in older people with multimorbidity and significant polypharmacy in primary care (SPPiRE). J Comorb. 2020;10:2235042X20946243. doi:10.1177/2235042X20946243
9. Mohamed MR, Ramsdale E, Loh KP, et al. Associations of polypharmacy and inappropriate medications with adverse outcomes in older adults with cancer: a systematic review and meta-analysis. Oncologist. 2020;25(1):e94–e108. doi:10.1634/theoncologist.2019-0406
10. Clark CM, Guan J, Patel AR, et al. Association between potentially inappropriate medications prescription and health-related quality of life among US older adults. J Am Geriatr Soc. 2024;72(9):2807–2815. doi:10.1111/jgs.18957
11. Fu M, Wushouer H, Nie X, Shi L, Guan X, Ross-Degnan D. Potentially inappropriate medications among elderly patients in community healthcare institutions in Beijing, China. Pharmacoepidemiol Drug Saf. 2020;29(8):923–930. doi:10.1002/pds.5064
12. Lou G, Yu Z, Chen L, Zhou Y, Zhang L. Trends in prescriptions for insomnia in a province in China between 2015 and 2019. Front Psychiatry. 2022;13:915823. doi:10.3389/fpsyt.2022.915823
13. Yu L, Chen X, Yu Z. Trends of antidementia drugs use in outpatients with Alzheimer’s disease in six major cities of China: 2012-2017. Int Clin Psychopharmacol. 2019;34(6):312–316. doi:10.1097/YIC.0000000000000278
14. Yu L, Zhu W, Zhu X, Lu Y, Yu Z, Dai H. Anti-seizure medication prescription in adult outpatients with epilepsy in China, 2013-2018. Front Neurol. 2021;12:649589. doi:10.3389/fneur.2021.649589
15. Yu L, Ding K, Luo L, Yu Z. Prescribing trends of glaucoma drugs in six major cities of China from 2013 to 2017. PLOS ONE. 2020;15(1):e0227595. doi:10.1371/journal.pone.0227595
16. Fernandez-Fradejas J, Delgado-Silveira E, Gonzalez-Burgos E, Alvarez-Diaz AM, Velez-Diaz-Pallares M. Potentially inappropriate prescriptions and potential prescription omissions in older people living with HIV. HIV Med. 2024;25(5):587–599. doi:10.1111/hiv.13616
17. Kim TW, Walley AY, Ventura AS, et al. Polypharmacy and risk of falls and fractures for patients with HIV infection and substance dependence. AIDS Care. 2018;30(2):150–159. doi:10.1080/09540121.2017.1384532
18. Morley KI, Ferris JA, Winstock AR, Lynskey MT. Polysubstance use and misuse or abuse of prescription opioid analgesics: a multi-level analysis of international data. Pain. 2017;158(6):1138–1144. doi:10.1097/j.pain.0000000000000892
19. Falutz J, Kirkland S, Guaraldi G. Geriatric syndromes in people living with HIV associated with ageing and increasing comorbidities: implications for neurocognitive complications of hiv infection. Curr Top Behav Neurosci. 2021;50:301–327. doi:10.1007/7854_2019_119
20. Blanco JR, Morillo R, Abril V, et al. Deprescribing of non-antiretroviral therapy in HIV-infected patients. Eur J Clin Pharmacol. 2020;76(3):305–318. doi:10.1007/s00228-019-02785-z
21. Marzolini C, Livio F. Prescribing issues in elderly individuals living with HIV. Expert Rev Clin Pharmacol. 2019;12(7):643–659. doi:10.1080/17512433.2019.1627200
22. Jungo KT, Streit S, Lauffenburger JC. Utilization and spending on potentially inappropriate medications by US older adults with multiple chronic conditions using multiple medications. Arch Gerontol Geriatr. 2021;93:104326. doi:10.1016/j.archger.2020.104326
23. Sarma P, Cassidy R, Corlett S, Katusiime B. Ageing with HIV: medicine optimisation challenges and support needs for older people living with HIV: a systematic review. Drugs Aging. 2023;40(3):179–240. doi:10.1007/s40266-022-01003-3
24. Contreras-Macias E, Gutierrez-Pizarraya A, Morillo-Verdugo R. Influence of polypharmacy in the simultaneous presence of high pharmacotherapeutic complexity, drug interactions and non-adherence to medication in patients with HIV infection. Project 3-HIT. Enferm Infecc Microbiol Clin. 2023;41(6):342–347. doi:10.1016/j.eimce.2022.09.007
25. McNicholl IR, Gandhi M, Hare CB, Greene M, Pierluissi E. A pharmacist-led program to evaluate and reduce polypharmacy and potentially inappropriate prescribing in older HIV-positive patients. Pharmacotherapy. 2017;37(12):1498–1506. doi:10.1002/phar.2043
26. Yu S, Zhang Y, Yao Y, Cao H. Migraine treatment and healthcare costs: retrospective analysis of the China Health Insurance Research Association (CHIRA) database. J Headache Pain. 2020;21(1):53. doi:10.1186/s10194-020-01117-2
27. Kosana P, Wu K, Tassiopoulos K, et al. Polypharmacy is associated with slow gait speed and recurrent falls in older people with HIV. Clin Infect Dis. 2024;78(6):1608–1616. doi:10.1093/cid/ciad782
28. Rostom A, Moayyedi P, Hunt R. Canadian association of gastroenterology consensus G. Canadian consensus guidelines on long-term nonsteroidal anti-inflammatory drug therapy and the need for gastroprotection: benefits versus risks. Aliment Pharmacol Ther. 2009;29(5):481–496. doi:10.1111/j.1365-2036.2008.03905.x
29. Winston A, Underwood J. Emerging concepts on the use of antiretroviral therapy in older adults living with HIV infection. Curr Opin Infect Dis. 2015;28(1):17–22. doi:10.1097/QCO.0000000000000117
30. Tian L, Ding P, Kuang X, Ai W, Shi H. The association between sleep duration trajectories and successful aging: a population-based cohort study. BMC Public Health. 2024;24(1):3029. doi:10.1186/s12889-024-20524-7
31. Collaborators GBDCoD. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2.
32. Petoumenos K, Worm SW, Fontas E, et al. Predicting the short-term risk of diabetes in HIV-positive patients: the data collection on adverse events of anti-HIV Drugs (D:A:D) study. J Int AIDS Soc. 2012;15(2):17426. doi:10.7448/IAS.15.2.17426
33. Tian F, Chen Z, Wu J. Prevalence of polypharmacy and potentially inappropriate medications use in elderly Chinese patients: a systematic review and meta-analysis. Front Pharmacol. 2022;13:862561. doi:10.3389/fphar.2022.862561
34. Fialova D, Laffon B, Marinkovic V, et al. Medication use in older patients and age-blind approach: narrative literature review (insufficient evidence on the efficacy and safety of drugs in older age, frequent use of PIMs and polypharmacy, and underuse of highly beneficial nonpharmacological strategies). Eur J Clin Pharmacol. 2019;75(4):451–466. doi:10.1007/s00228-018-2603-5
35. Greene M, Steinman MA, McNicholl IR, Valcour V. Polypharmacy, drug-drug interactions, and potentially inappropriate medications in older adults with human immunodeficiency virus infection. J Am Geriatr Soc. 2014;62(3):447–453. doi:10.1111/jgs.12695
36. Madhombiro M, Musekiwa A, January J, Chingono A, Abas M, Seedat S. Psychological interventions for alcohol use disorders in people living with HIV/AIDS: a systematic review. Syst Rev. 2019;8(1):244. doi:10.1186/s13643-019-1176-4
37. Salahudeen MS. Deprescribing medications in older people: a narrative review. Drugs Today. 2018;54(8):489–498. doi:10.1358/dot.2018.54.8.2856495
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.