Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Potential Use of Novel Image and Signal Processing Methods to Develop a Quantitative Assessment of the Severity of Acute Radiation Dermatitis in Breast Cancer Radiotherapy
Authors Kondziołka J ![]() , Wilczyński S
, Wilczyński S ![]() , Michalecki Ł
, Michalecki Ł
Received 11 January 2022
Accepted for publication 18 March 2022
Published 22 April 2022 Volume 2022:15 Pages 725—733
DOI https://doi.org/10.2147/CCID.S354320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Joanna Kondziołka,1 Sławomir Wilczyński,1 Łukasz Michalecki2
1Department of Basic Biomedical Science, Faculty of Pharmaceutical Sciences in Sosnowiec, Medical University of Silesia, Katowice, Poland; 2University Clinical Center of the Medical University of Silesia, Katowice, Poland
Correspondence: Sławomir Wilczyński, Email [email protected]
Abstract: More than 95% of patients who undergo radiotherapy report symptoms of radiation dermatitis, which is a side effect of this therapy. Erythema, edema, dry and moist desquamation intensify with each fraction of irradiation and can significantly reduce a patient’s quality of life. Therefore, an effective skin care procedure is needed for skin that has been exposed to ionizing radiation in order to avoid unplanned treatment interruptions. The methods that are currently used to assess the severity of an acute radiation reaction are based on visual scales (RTOG, EORTC, NCI CTCAE, LENT-SOMA). Because the assessment is made subjectively, the results depend on the researchers, their experience and perceptiveness. Until now, several studies have been carried out to check the possibility of using an objective methods like hyperspectral imaging, thermal imaging, laser Doppler flowmetry, dielectric and electrochemical methods, reflection spectrophotometry and Courage-Khazaka Multi-skin instrument to radiation-induced dermatitis assessment. Unfortunately, due to various limitations that occurred in the research, none of these techniques was successfully implement as alternative for visual assessment. The continuous development of technology enables researchers to access new techniques that might constitute useful diagnostic and cognitive tools. Infrared thermal imaging, hyperspectral imaging and reflectance spectroscopy are examples of the visual techniques that have been used for many years in various fields of medicine, including dermatology and chronic wound or burn care. They provide information on the skin parameters, such as the temperature, concentration and distribution of chromophores (eg, hemoglobin and melanin), saturation or perfusion changes. The aim of this study is to review the available literature on the use of imaging methods in the clinical assessment of skin with lesions of various origins, evaluation of their suitability for the assessment of radiation reaction and consideration the possibility of creating a quantitative scale for assessing severity of acute radiation dermatitis.
Keywords: infrared thermal imaging, hyperspectral imaging, reflectance spectroscopy, breast cancer, radiodermatitis, algorithm
Introduction
According to the data provided by WHO, there were more than 19.2 million cases of cancer in 2020. Breast cancer is the most common malignant neoplasm that accounts for approximately 2.3 million cases and is also the most common cancer death in the female group of patients (almost 690,000 deaths).1 The cause of the occurrence of neoplastic changes are not clearly defined but based on state of the current knowledge, it is a result of the interaction of various risk factors such as environmental, exogenous and endogenous factors as well as individual factors (genetic predisposition) that increase the risk of getting the disease. The most frequently mentioned causes of cancer include smoking, alcohol abuse, a high fat diet and a lack of physical activity.2,3
The choice of the treatment method depends on the patient’s performance status, the clinical stage of the neoplastic disease, the histopathological diagnosis, the biological subtype of the neoplasm and any coexisting diseases. The diagnostic and therapeutic plan is developed by a Multidisciplinary Team.4,5
Radiotherapy (RT) is one of the basic methods that is used to treat patients with neoplastic disease in addition to surgical and systemic treatment (chemotherapy, hormone therapy, immunotherapy). Approximately 50% of patients with various types of cancer will undergo RT as part of their treatment. Ionizing radiation treatment is most often used as part of adjuvant treatment in patients with breast cancer after a radical mastectomy or breast conserving surgery (BCS).6,7 Planning the radiotherapy is a multi-stage process that requires the involvement of a team of specialists and the use of technologically advanced medical equipment. Quality control procedures are used to prepare the radiotherapy plan and treatment delivery in order to ensure the safe implementation of the treatment plan in accordance with international standards.7,8
The aim of radiotherapy is to deposit the prescribed dose of ionizing radiation in the indicated area while limiting the maximum dose in normal tissues (heart, lungs, contralateral breast). Breast RT uses both external beam irradiation and brachytherapy (irradiation using a radiation source that is placed inside the treated area). Depending on the stage of the neoplastic disease, the scope of the surgical treatment and the postoperative pathomorphological diagnosis, the irradiated area may include the chest wall, the breast, the tumor bed and the regional lymphatic system (supraclavicular area, axillary fossa).7,9
A standard course of RT usually last for four to five weeks (five fractions per week) and consists of 25–28 fractions of single doses 1.8–2.0 Gy, which is enhanced by an additional boost of 10–16Gy to the tumor bed after a lumpectomy. In recent years, many institutes have introduced hypofractionation regimens in which a single dose >2.0 Gy is delivered in 15–18 sessions. This treatment reduces the time of exposure to ionizing radiation with the same clinical results as conventionally fractionated RT, which makes it easier for patients to complete the course of RT.8–10
Despite the undeniable advantages of radiotherapy, which include its loco-regional control, high efficiency and safety profile, more than 95% of patients report side effects that may significantly reduce their quality of life. These radiation-associated side effect such as erythema, edema, dry and moist desquamation, itching, soreness or even necrosis are known as radiodermatitis (RD).11–13
The early symptoms refer to the place that has been directly exposed to ionizing radiation and are called acute radiation dermatitis (ARD). They can occur in as little as during the first four weeks of radiotherapy and then increase with each fraction. The late side effects of RT can appear months or even years after the course of RT and is called chronic radiation dermatitis.14,15
In the first stage, ARD is manifested by redness of varying severity along with the dry or wet desquamation of the epidermis. Exfoliation of the epidermis reveals a defect in the cells of the basal layer of the epidermis as well as in the sebaceous and sweat glands in the dermis. Wet exfoliation is accompanied by serous exudate and a loss of the dermis. Late RD is manifested as changes in vascularity (telangiectasia), dermis atrophy, changes in pigmentation (poikiloderma, hyper- or hypopigmentation), fibrosis, ulceration or necrosis. The severity of chronic radiodermatitis depends on the total radiation dose, the size of the irradiated area and the individual predisposition of patient.14,16,17
The severity of skin changes also depends on many other factors, including the type and energy of the radiation, the total dose, the duration of therapy, the power and number of fractional doses as well as the sensitivity of the irradiated cells and the individual predisposition of patients. The assessment of the skin condition is based on the subjective assessment of the oncologist and is most often presented using a visual scale. In the case of ARD, the most commonly used scales are The European Organization for Research and Treatment of Cancer (EORTC), the Radiation Therapy Oncology Group (RTOG) and the five-point scale of the National Cancer Institute – Common Terminology Criteria for Adverse Events (NCI CTCAE, version 5).18,19 The Late Effects on Normal Tissue – Subjective, Objective Management and Analytic (LENT-SOMA) scale is used to determine the severity of chronic RD.20 A comparison of most commonly used scales is presented in Table 1.
 |
Table 1 A Comparison of the Scales That are Used to Determine the Severity of Acute and Chronic RD18–20 |
Visual assessment of the condition of the skin depends on many factors but the most important of which are experience and perceptiveness of researcher. Due to the lack of objective methods of assessing ARS, which do not allow to quantify the physiological skin parameters, several studies have been carried out using alternative quantitative methods. Kitajima et al used the Multi-skin Instrument (Courage + Khazaka Corporation) to assess the condition of the skin during radiotherapy. It allows to check the surface temperature of the skin, the level of hydration and the intensity of melanin and erythema. The results of these preliminary studies indicate that corneometer, mexameter and skin-thermometer measurements can be an objective tool to improve the accuracy of skin assessment.18 Sanchis et al used the technique of laser Doppler flowmetry (LDF) to measure cutaneous blood flow in patients with breast cancer undergoing RT. The results of this study indicate that measurements with LDF could be useful and objective method to assess RD.21 Research has also been carried out using thermal imaging techniques to assess radiodermatitis. Obtained by Maillot et al results confirm the increase in local skin temperature during the development of the radiation-induced inflammatory, however, due to the limitations of this study, further research is needed on this issue.22 Abdlaty et al conducted a pilot study to use hyperspectral imaging to assess the erythema that develops during skin cancer treatment with radiation therapy. The obtained results indicate that HSI allows for the quantification of oxygenation and perfusion of the skin subjected to radiotherapy and can be approached to objectively assess the severity of erythema.23
Despite numerous studies using various measurement techniques, at present researchers do not have at their disposal a standardized method allowing for an objective assessment of the degree of the severity of the radiation reaction. Further research on this topic is necessary because only repeated measurements and sensitive techniques will allow for early identification of RD lesions, their prevention and effective treatment.
Materials and Methods
In order to analyze the suitability of the imaging methods that are used to assess the intensity of a radiation reaction, the research was conducted in the PubMed electronic database, which was searched for any articles that were published between 1991 and 2021. The search was conducted until December 5, 2021. The language of the articles was limited to English and the databases that were used had the appropriate filters. The following keywords were searched in various combinations in order to optimize the search results in accordance with the topic of this article: infrared thermal imaging, thermography, hyperspectral imaging, reflectance spectroscopy, skin, wound care, and diagnosis. All of the articles that were cited in these narrative review were also screened in order to identify any other potential studies in their reference lists.
Results
During the online search, the articles were screened by their titles and abstracts. A total of 39 articles were considered to be relevant and were selected for a full-text reading. A scan of the literature and citations of the included studies yielded 18 more articles for a full-text reading. Among the 57 papers that were considered for the present review, 17 did not have any relevant data for the planned narrative review and were excluded. The remaining 40 articles, among which were reviews, case studies, randomized controlled trials, the content was evaluated and selected for the data analysis.
Discussion
Infrared Thermal Imaging
Because changes in the skin temperature are one of the earliest observed disease symptoms of organisms infrared thermal imaging (IRT) analysis can be one of the basic diagnostic and cognitive tools. IRT enables information about the physiological and pathological processes that take place in the human body to be obtained by analyzing the temperature gradient, its change over time and its distribution in a given area. Importantly, it is a non-invasive and non-contact analysis, which is absolutely harmless, does not cause any side effects, and therefore can be used for prolonged or repeated diagnostics.24,25 The basis of IRT is the fact that the temperature that is measured on the body surface depends on the temperature of the internal organs and the tissues under the skin. Since lesions very often change the heat flux that is emitted by diseased tissue, it causes changes in the temperature of the surrounding tissues, including the skin. In the case of a thermographic analysis, it is important that the reference point is an area of the patient’s skin that has not been affected by the disease because body temperature depends on many factors, including age or gender, thanks to which differences in its values can be observed during the measurements.26
IRT has been used in many areas of medicine. One of the oldest uses was for diagnosing breast cancer. In the 1950s, Lawson conducted research that proved its usefulness for diagnosing benign neoplastic changes in the breast.27 In later years, numerous studies were conducted that confirmed the usefulness of thermography in diagnosing the early stage of breast cancer. Although thermography cannot show the morphological structure of the breast, it does illustrate the thermal changes and changes in the blood vessels in tissues, which are usually the first symptoms of a developing neoplastic disease.28 Because of the development of technology and temperature measurement standards (ISO, ASTM – Table 2) that define the specifications for measuring devices, including their minimum requirements, equipment calibration and the practical aspects of taking the measurements, thermography is increasingly used in medicine. IRT is currently used in practice, among others, in dentistry to assess the condition of the periodontium in patients with leukemia, to assess inferior alveolar nerve deficits or to screen for endodontic diseases in the oral cavity.29–31 It is used to diagnose pneumonia and also supports diagnosing thyroid diseases.32 In cardiology, it can be used to monitor the circulation or heart during cardiac surgery, while in allergology, it supports diagnosing respiratory and food allergies.33–35 It was also found that a thermal imaging analysis can be an effective tool for diagnosing peripheral vascular disorders.28
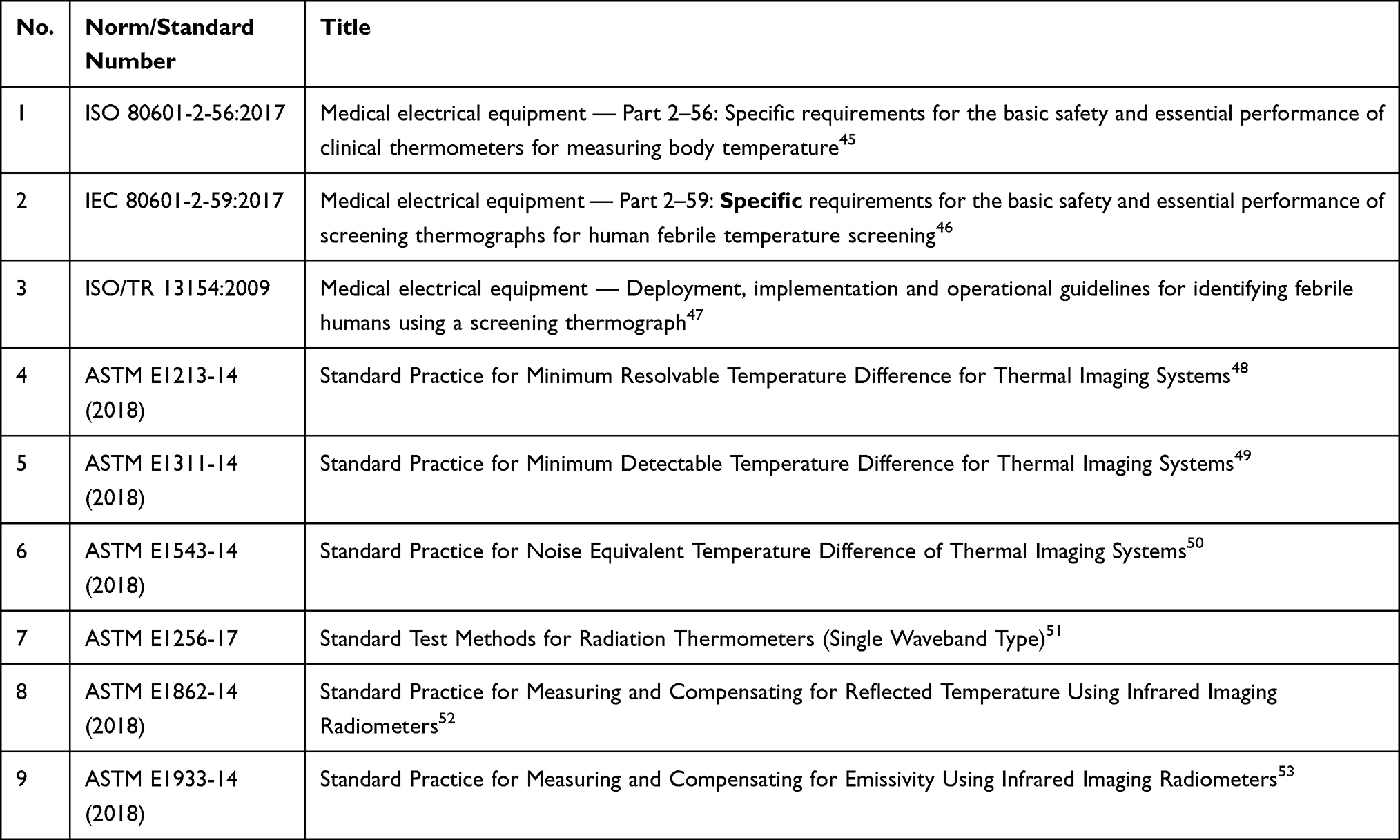 |
Table 2 Summary of the Basic Standards for a Thermal Imaging Analysis |
IRT is also a useful technique for imaging the skin temperature distribution in diabetics.36 The studies that were conducted by Bagavathiappan et al confirmed that thermal imaging can be used to detect diabetic neuropathy while the studies that were conducted by Aliahmad et al confirmed the usefulness of IRT for evaluating the healing status of diabetes-related foot ulcers.37,38 Because most skin disorders cause inflammation that is manifested by changes in temperature, IRT can be considered to be a suitable technique to use to evaluate it. Vargas et al used the thermography method to diagnose leprosy and to evaluate the effectiveness of the treatment.39 In the case of dermatological diseases, thermal imaging has been used in studies of psoriasis, inter alia, for the early diagnosis of psoriatic arthritis.40 According to the studies of Thomas et al, IRT can also be used to optimize the application of a laser during laser-based skin treatment such as depilation or treating vascular lesions.41 Numerous studies have been conducted to confirm the usefulness of thermography for treating burns. This technique can be used to assess the depth of the burns as well as to qualify patients who require early surgery. The effectiveness of sprayed and poured cooling agents was also compared for the initial cooling management of extensive burns.25,42–44
The development of computer technologies, the use of high-resolution detectors and the development of measurement standards have made thermography increasingly popular in the scientific community. Because thermal imaging cameras are widely available and easy to use, the techniques can be used by both scientific laboratories and medical centers.
Hyperspectral Imaging
Hyperspectral imaging (HSI), which is derived from standard digital photography, is an increasingly popular method of imaging using visible light. This technique uses three wavelength ranges that correspond to the red, green and blue channels to record an image that consists of many individual photos that are recorded at a strictly defined wavelength.54 Because of the high spectral resolution, the recorded data is presented as a two-dimensional map of the reflection spectra, which enables a quantitative analysis of a given object by, eg, color measurement or qualitative by, eg, identifying chemical compounds. The obtained set of images is called a hypercube and its analysis can be used to determine the concentration of tissue chromophores.55 It is important to keep in mind that these reflectance spectra of the skin can be affected by different factors such as the melanin concentration, the thickness of the epidermis, the oxygen saturation of the blood in the dermis or blood volume.55
Taking pictures with a hyperspectral camera is non-invasive and non-contact causes no side effects, and therefore it is used more frequently in various fields of medicine, especially in dermatology.56 This technique enables, inter alia, the differences in the absorption of visible light radiation by the chromophores in the skin such as hemoglobin and melanin to be analyzed, which makes it possible to determine their distribution and concentration in a given area of the skin.57
The studies that were conducted by Chin et al and Shah et al indicated that HSI analysis can be used to visualize and quantify changes in oxygenation and perfusion in the areas of the skin that have been exposed to ionizing radiation. Such an assessment is possible immediately after irradiation before any visible skin lesions appear, which can be a useful tool for the immediate assessment of the condition of patients who have had radiation accidents.58,59 Several studies have been conducted on the use of hyperspectral methods to control and evaluate the healing process of chronic wounds. Until now, these processes have been monitored by a visual inspection, which is a subjective method the result of which depends on the experience and perception of the examiners. The studies that were conducted by Calin et al showed that HSI enables the different types of tissue that are present in the injured area to be identified, which enables an objective wound characterization to be made.60 The research proved that hyperspectral imaging enables the tissue saturation and hydration as well as the observation of blood flow to be determined, and therefore it can be used for the local detection of changes in perfusion and oxygenation, which are extremely important in open wound healing.54,60 Yudovsky et al used hyperspectral methods to control and evaluate the healing process of diabetic foot ulcerations, which occur as a complication in 15–25% of patients with type 1 and type 2 diabetes. What is also important is that HSI can be used to assess the risk of ulceration as early as during screening and not during the months of observation as is the case today.55 The case report presented by McCarthy et al indicated that HSI might also be an effective method for determining the depth of a burn, which potentially enable a decision about early surgical intervention.61
HSI has also been used with oncology patients. The research of Kho et al indicated the possibility of using HSI as a safe and precise tool for determining the margin of safety during BCS.62
Diffuse Reflectance
Diffuse reflectance (DR), which uses radiation with a wavelength of 250–2500 nm, has found wide application in analyzing various surfaces and materials.63,64 A reflectometer measures the absorption and transmission of the emitted radiation and determines its reflectance. Using the obtained data and the optical properties of a surface, it is possible to obtain information on the structure of the tested sample or on the concentration of chromophores.
DR is widely used in many fields of technology and pharmacy, and it has also been used in medicine to study the properties of the skin. By measuring reflectance, quantitative data on the melanin and hemoglobin content of the skin can be obtained, which might be useful in detecting acute and chronic inflammations that are caused by various factors, eg, an infection or irritation. The studies that were conducted by Yudovsky et al showed that a method that uses reflectance measurement can be a useful tool for monitoring changes in the blood supply and melanin concentration in the skin as well as for analyzing the epidermal thickness, which is associated with the normal aging process of the skin and is caused by external factors (UV radiation) and disease states (ulceration, cancer).65,66 The results of a study conducted by Kollias et al in 1995 showed that diffuse reflectance spectroscopy enabled the erythema that is caused by an irritant (sodium lauryl sulfate) to be evaluated. DR enables the apparent concentration of oxyhemoglobin to be assessed. Studies have confirmed that irritant-induced inflammation primarily involves the capillaries and the superficial arterial plexus.67 Additionally, the research that was conducted by Riordan et al indicated that DR can be used to design an algorithm for detecting erythema in skin with varying pigmentations.68 As was shown by a pilot study that was conducted by Tzeng et al, reflectance can also be used to diagnose or evaluate the skin of psoriasis patients without having to perform a histopathology examination, which is invasive.69 DR was also used by Hsu et al to assess the severity of keloid scars. That research indicated that this technique can be used to objectively evaluate the alignment direction of collagen bundles in scars as well as to quantify the concentration of collagen, water content and oxygen saturation in order to monitor the response to the therapeutic interventions.70
Conclusion
Considering that a visual assessment of most dermatological changes is a subjective evaluation by the researcher, the lack of standardization and comparability of the results due to the inter-individual differences and personal changes in research teams, in many cases, such an analysis does not reflect the actual state of the patient, which prevents the precise planning of further treatment. In the case of RD, an appropriate assessment of the developing inflammation is of essential importance in enabling clinicians and researchers to provide effective patient care. The appropriate start of the treatment can in many cases determine the possibility of completing the course of radiotherapy.
As can be seen from the summary presented in Table 1, the scales that are used to determine the intensity of the radiation reaction are based solely on a visual evaluation, and thus depend on the subjective assessment of the researchers, which depends on their experience, perceptiveness and the information that is obtained from a patient during a follow-up visit. Therefore, depending on the physician and the institute in which the therapy is performed, there may be discrepancies in assessing the severity of the side effects of RT. This makes it difficult to assess the effectiveness of the treatments given to patients and to compare the effectiveness of the active ingredients and care preparations that are analyzed in studies that are conducted by various institutes.
Therefore, it is important to develop and implement objective methods for assessing the condition of the skin that has been affected by RD using numerical data that is independent of the researcher. For this purpose, imaging methods, which have been gaining popularity for many years and are increasingly being used in dermatological diagnostics, can be useful for both clinical research and medical care.
As the analysis shows, the above-mentioned methods have been used for years to determine the temperature of the skin (IRT), erythema and to analyze wounds, including those associated with burns (HSI, DR), which makes them perfectly suitable to dealing with the problem of ARD. Using HSI and DR, it is possible to determine the concentration and distribution of hemoglobin and melanin in the skin. In the case of RD, which is manifested by erythema and pigmentation changes, these chromophores will be the basic parameter that indicates the development and severity of the ARD. Analyzing them will also be useful for monitoring a patient’s recovery after RT. In the case of RD, which is an inflammation reaction of the skin, the data that is obtained from the thermal imaging analysis would be also useful. Temperature changes, which are usually the first observed symptoms of a disease, indicate the development of a reaction. Therefore, it seems reasonable to combine these three techniques and to supplement the data that is obtained with observations according to the visual methods in order to create an algorithm for quantifying the severity of the ARD. The use of imaging methods is also supported by the increasing availability of equipment such as hyperspectral cameras, thermal imaging cameras and diffuse reflectometers, which means that the methods can be widely used. Each of these methods is non-invasive, non-contact and safe for patients, so they can safely be used as a diagnostic tool during the follow-up visits during radiotherapy and after its completion. However, it should be noted that HSI and DR are relatively young techniques that are continuously being researched in various fields of medicine, and that therefore they require standards for the methods for specific applications be established and developed.
Until now, several studies have been carried out to check the possibility of using new objective methods to assess the severity of the radiation reaction. Researchers focused on methods such as thermal imaging, laser Doppler flowmetry, dielectric and electrochemical methods, reflection spectrophotometry and used Courage-Khazaka Multi-skin instrument equipped with different probes like skin-thermometer, corneometer and mexameter. The results obtained from all these studies indicate that instrumental methods, including optical techniques, can be used to assess the changes taking place in the skin exposed to radiation, and therefore they can be an alternative to visual assessment. Unfortunately, due to various limitations that occurred in the studies, including too small research groups, it was not possible to develop and validate a final method that could successfully replace visual evaluation so further researches are required.
Because of the development of technology and the widespread availability of the equipment, these imaging techniques can be a valuable diagnostic and cognitive tool in evaluating RD and determining the effective skin care procedure.
Funding
This study was financially supported by the Medical University of Silesia, grants no. PCN-1-013/K/0/O and PCN-2-114/N/0/O.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization [homepage on the Internet]. Fact sheets: breast cancer; 2021. Available from: https://gco.iarc.fr/today/data/factsheets/cancers/39-All-cancers-fact-sheet.pdf.
2. Lewandowska AM, Rudzki M, Rudzki S, Lewandowski T, Laskowska B. Environmental risk factors for cancer - review paper. Ann Agric Environ Med. 2018;26(1):1–7. doi:10.26444/aaem/94299
3. Sun YS, Zhao Z, Yang ZN, et al. Risk factors and preventions of breast cancer. Int J Biol Sci. 2017;13(11):1387–1397. doi:10.7150/ijbs.21635
4. Blackwood O, Deb R. Multidisciplinary team approach in breast cancer care: benefits and challenges. Indian J Pathol Microbiol. 2020;63(5):105–112. doi:10.4103/IJPM.IJPM_885_19
5. Saini KS, Taylor C, Ramirez AJ, et al. Role of the multidisciplinary team in breast cancer management: results from a large international survey involving 39 countries. Ann Oncol. 2011;23(4):853–859.
6. Warrier S, Tapia G, Goltsman D, Beith J. An update in breast cancer screening and management. Womens Health. 2015;12(2):229–239. doi:10.2217/whe.15.105
7. McDonald ES, Clark AS, Tchou J, Zhang P, Freedman GM. Clinical diagnosis and management of breast cancer. J Nucl Med. 2016;57(Suppl 1):9S–16S. doi:10.2967/jnumed.115.157834
8. Mutebi M, Anderson BO, Duggan C, et al. Breast cancer treatment: a phased approach to implementation. Cancer. 2020;126(Suppl 10):2365–2378. doi:10.1002/cncr.32910
9. Haussmann J, Corradini S, Nestle-Kraemling C, et al. Recent advances in radiotherapy of breast cancer. Radiat Oncol. 2020;15(1):71. doi:10.1186/s13014-020-01501-x
10. Whelan TJ, Pignol JP, Levine MN, et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med. 2010;362(6):513–520. doi:10.1056/NEJMoa0906260
11. Kišonas J, Venius J, Sevriukova O, et al. Application of reflectance confocal microscopy for early diagnosis of radiation-induced acute dermatitis in radiosensitive patient: case study. Radiat Prot Dosimetry. 2018;182(1):93–97. doi:10.1093/rpd/ncy135
12. White J, Joiner MC. Toxicity from radiation in breast cancer. In: Small W, Woloschak GE, editors. Radiation Toxicity: A Practical Guide. (Cancer Treatment and Research V.128). New York: Springer Science + Media Business; 2006:65–110.
13. Lee J, Park W, Choi DH, et al. Patient-reported symptoms of radiation dermatitis during breast cancer radiotherapy: a pilot study. Qual Life Res. 2017;26(7):1713–1719. doi:10.1007/s11136-017-1526-4
14. Spałek M. Chronic radiation-induced dermatitis: challenges and solutions. Clin Cosmet Investig Dermatol. 2016;9(9):473–482. doi:10.2147/CCID.S94320
15. Seité S, Bensadoun RJ, Mazer JM. Prevention and treatment of acute and chronic radiodermatitis. Breast Cancer. 2017;9:551–557. doi:10.2147/BCTT.S149752
16. Robijns J, Laubach HJ. Acute and chronic radiodermatitis: clinical signs, pathophysiology, risk factors and management options. J Egypt Women Dermatol Soc. 2018;15(1):2–9. doi:10.1097/01.EWX.0000529960.52517.4c
17. Singh M, Alavi A, Wong R, Akita S. Radiodermatitis: a review of our current understanding. Am J Clin Dermatol. 2016;17(3):277–292. doi:10.1007/s40257-016-0186-4
18. Kitajima M, Mikami K, Noto Y, et al. Quantitative assessment of radiodermatitis through a non-invasive objective procedure in patients with breast cancer. Mol Clin Oncol. 2019. doi:10.3892/mco.2019.1948
19. Rosenthal A, Israilevich R, Moy R. Management of acute radiation dermatitis: a review of the literature and proposal for treatment algorithm. J Am Acad Dermatol. 2019;81(2):558–567. doi:10.1016/j.jaad.2019.02.047
20. Marcenaro M, Sacco S, Pentimalli S, et al. Measures of late effects in conservative treatment of breast cancer with standard or hypofractionated radiotherapy. Tumori. 2004;90(6):586–591. doi:10.1177/030089160409000609
21. Sanchis GA, González BL, Carazo SJL, et al. Evaluation of acute skin toxicity in breast radiotherapy with a new quantitative approach. Radiother Oncol. 2016;122(1):54–59.
22. Maillot O, Leduc N, Atallah V, et al. Evaluation of acute skin toxicity of breast radiotherapy using thermography: results of a prospective single-centre trial. Cancer Radiother. 2018;22(3):205–210. doi:10.1016/j.canrad.2017.10.007
23. Abdlaty R, Doerwald-Munoz L, Farrell TJ, Hayward JE, Fang Q. Hyperspectral imaging assessment for radiotherapy induced skin-erythema: pilot study. Photodiagnosis Photodyn Ther. 2021;33:102195. doi:10.1016/j.pdpdt.2021.102195
24. Usamentiaga R, Venegas P, Guerediaga J, Vega L, Molleda J, Bulnes FG. Infrared thermography for temperature measurement and non-destructive testing. Sensors. 2014;14(7):12305–12348. doi:10.3390/s140712305
25. Lahiri BB, Bagavathiappan S, Jayakumar T, Philip J. Medical applications of infrared thermography: a review. Infrared Phys Technol. 2012;55(4):221–235. doi:10.1016/j.infrared.2012.03.007
26. Baic A, Plaza D, Lange B, et al. The Use of thermal imaging in the evaluation of temperature effects of radiotherapy in patients after mastectomy-First study. Sensors. 2021;21(21):7068. doi:10.3390/s21217068
27. Lawson R. Implications of surface temperatures in the diagnosis of breast cancer. Can Med Assoc J. 1956;75(4):309–311.
28. Bagavathiappan S, Saravanan T, Philip J, et al. Infrared thermal imaging for detection of peripheral vascular disorders. J Med Phys. 2009;34(1):43–47. doi:10.4103/0971-6203.48720
29. Păunică SC, Dumitriu A, Mogoş M, Georgescu O, Mogoş I. The evaluation of the periodontium in patients with leukemia using thermographic imaging. Hematology. 2009;14(6):341–346. doi:10.1179/102453309X12473408860505
30. Mouli PE, Kumar SM, Senthil B, Parthiban S, Malarvizhi AE, Karthik R. Application of thermography in dentistry - A review. J Dent Med Sci. 2012;1(1):39–43.
31. Komoriyama M, Nomoto R, Tanaka R, et al. Application of thermography in dentistry-visualization of temperature distribution on oral tissues. Dent Mater J. 2003;22(4):436–443. doi:10.4012/dmj.22.436
32. Damião CP, Montero JRG, Moran MBH, et al. Application of thermography in the diagnostic investigation of thyroid nodules. Endocr J. 2021;68(5):573–581. doi:10.1507/endocrj.EJ20-0541
33. Clark AT, Mangat JS, Tay SS, et al. Facial thermography is a sensitive and specific method for assessing food challenge outcome. Allergy. 2007;62(7):744–749. doi:10.1111/j.1398-9995.2007.01363.x
34. Okada Y, Kawamata T, Kawashima A, Hori T. Intraoperative application of thermography in extracranial-intracranial bypass surgery. Neurosurgery. 2007;60(4Suppl 2):
35. Siebert J, Keita L, Kaczmarek M, Anisimowicz L, Rogowski J, Narkiewicz M. Application of intraoperative thermography in coronary artery bypass grafting without extracorporeal circulation - clinical report. Med Sci Monit. 2001;7(4):766–770.
36. Ring F. Thermal imaging today and its relevance to diabetes. J Diabetes Sci Technol. 2010;4(4):857–862. doi:10.1177/193229681000400414
37. Bagavathiappan S, Philip J, Jayakumar T, et al. Correlation between plantar foot temperature and diabetic neuropathy: a case study by using an infrared thermal imaging technique. J Diabetes Sci Technol. 2010;4(6):1386–1392. doi:10.1177/193229681000400613
38. Aliahmad B, Tint AN, Poosapadi Arjunan S, et al. Is Thermal imaging a useful predictor of the healing status of diabetes-related foot ulcers? A pilot study. J Diabetes Sci Technol. 2018;13(3):561–567. doi:10.1177/1932296818803115
39. Vargas JVC, Brioschi ML, Dias FG, et al. Normalized methodology for medical infrared imaging. Infrared Phys Technol. 2009;52(1):42–47. doi:10.1016/j.infrared.2008.11.003
40. Ismail E, Capo A, Amerio P, Merla A. Functional-thermoregulatory model for the differential diagnosis of psoriatic arthritis. Biomed Eng Online. 2014;13(1):162. doi:10.1186/1475-925X-13-162
41. Thomas RA, Donne KE, Clement M, et al. Optimized laser application in dermatology using infrared thermography. Proc. SPIE 4710, Thermosense, XXIV, 2002:424–435. doi:10.1117/12.459592
42. Zhu WP, Xin XR. Study on the distribution pattern of skin temperature in normal Chinese and detection of the depth of early burn wound by infrared thermography. Ann NY Acad Sci. 1999;888:300–313. doi:10.1111/j.1749-6632.1999.tb07964.x
43. Renkielska A, Nowakowski A, Kaczmarek M, et al. Static thermography revisited-an adjunct method for determining the depth of the burn injury. Burns. 2005;31(6):768–775. doi:10.1016/j.burns.2005.04.006
44. Thatcher JE, Squiers JJ, Kanick SC, et al. Imaging techniques for clinical burn assessment with a focus on multispectral imaging. Adv Wound Care. 2016;5(8):360–378. doi:10.1089/wound.2015.0684
45. International Organization of Standarization [homepage on the Internet]. Available from: https://www.iso.org/standard/67348.html.
46. International Organization of Standarization [homepage on the Internet]. Available from: https://www.iso.org/standard/69346.html.
47. International Organization of Standarization [homepage on the Internet]. Available from: https://www.iso.org/standard/69347.html.
48. ASTM International [homepafe on the Internet]. Available from: https://www.astm.org/e1213-14r18.html.
49. ASTM International [homepafe on the Internet]. Available from:https://www.astm.org/e1311-14r18.html.
50. ASTM International [homepafe on the Internet]. Available from:https://www.astm.org/e1543-14r18.html.
51. ASTM International [homepafe on the Internet]. Available from:https://www.astm.org/e1256-17.html.
52. ASTM International [homepafe on the Internet]. Available from:https://www.astm.org/e1862-14r18.html.
53. ASTM International [homepafe on the Internet]. Available from:https://www.astm.org/e1933-14r18.html.
54. Saiko G, Lombardi P, Au Y, Queen D, Armstrong D, Harding K. Hyperspectral imaging in wound care: a systematic review. Int Wound J Epub. 2020;17(6):1840–1856. doi:10.1111/iwj.13474
55. Yudovsky D, Nouvong A, Pilon L. Hyperspectral imaging in diabetic foot wound care. J Diabetes Sci Technol. 2010;4(5):1099–1113. doi:10.1177/193229681000400508
56. Chen YM, Lai KL, Chen HH, et al. Hyperspectral imaging for skin assessment in systemic sclerosis: a pilot study. Rheumatology. 2020;59(11):3201–3210. doi:10.1093/rheumatology/keaa067
57. Koprowski R, Wilczyński S, Wróbel Z, Błońska-Fajfrowska B. Calibration and segmentation of skin areas in hyperspectral imaging for the needs of dermatology. Biomed Eng Online. 2014;13(1):113. doi:10.1186/1475-925X-13-113
58. Chin MS, Freniere BB, Lo YC, et al. Hyperspectral imaging for early detection of oxygenation and perfusion changes in irradiated skin. J Biomed Opt. 2012;17(2):026010. doi:10.1117/1.JBO.17.2.026010
59. Shah SA, Bachrach N, Spear SJ, et al. Cutaneous wound analysis using hyperspectral imaging. Biotechniques. 2003;34(2):408–413. doi:10.2144/03342pf01
60. Calin MA, Coman T, Parasca SV, Bercaru N, Savastru R, Manea D. Hyperspectral imaging-based wound analysis using mixture-tuned matched filtering classification method. J Biomed Opt. 2015;20(4):046004. doi:10.1117/1.JBO.20.4.046004
61. McCarthy M, Prete VI, Oh S, et al. The use of visible-light hyperspectral imaging in evaluating burn wounds: a Case Report. J Burn Care Res. 2021;42(4):825–828. doi:10.1093/jbcr/irab003
62. Kho E, de Boer LL, Van de Vijver KK, et al. Hyperspectral imaging for resection margin assessment during cancer surgery. Clin Cancer Res. 2019;25(12):3572–3580. doi:10.1158/1078-0432.CCR-18-2089
63. Cooksey CC, Allen DW, Tsai BK. Reference data set of human skin reflectance. J Res Natl Inst Stand Technol. 2017;122:1–5. doi:10.6028/jres.122.026
64. Bydlon TM, Nachabé R, Ramanujam N, Sterenborg HJ, Hendriks BH. Chromophore based analyses of steady-state diffuse reflectance spectroscopy: current status and perspectives for clinical adoption. J Biophotonics. 2014;8(1–2):9–24. doi:10.1002/jbio.201300198
65. Yudovsky D, Pilon L. Rapid and accurate estimation of blood saturation, melanin content, and epidermis thickness from spectral diffuse reflectance. Appl Opt. 2010;49(10):1707–1719. doi:10.1364/AO.49.001707
66. Yudovsky D, Pilon L. Retrieving skin properties from in vivo spectral reflectance measurements. J Biophotonics. 2011;4(5):305–314. doi:10.1002/jbio.201000069
67. Kollias N, Gillies R, Muccini JA, Uyeyama RK, Phillips SB, Drake LA. A single parameter, oxygenated hemoglobin, can be used to quantify experimental irritant-induced inflammation. J Invest Dermatol. 1995;104(3):421–424. doi:10.1111/1523-1747.ep12666001
68. Riordan B, Sprigle S, Linden M. Testing the validity of erythema detection algorithms. J Rehabil Res Dev. 2001;38(1):13–22.
69. Tzeng SY, Guo JY, Yang CC, et al. Portable handheld diffuse reflectance spectroscopy system for clinical evaluation of skin: a pilot study in psoriasis patients. Biomed Opt Express. 2016;7(2):616–628. doi:10.1364/BOE.7.000616
70. Hsu CK, Tzeng SY, Yang CC, et al. Non-invasive evaluation of therapeutic response in keloid scar using diffuse reflectance spectroscopy. Biomed Opt Express. 2015;6(2):390–404. doi:10.1364/BOE.6.000390
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.