Back to Journals » International Journal of Women's Health » Volume 18
Postpartum Spontaneous Coronary Artery Dissection Involving the Left Main Coronary Artery: A Case Report
Authors Jing H, Zong A, Gong X, Zhang L
Received 5 September 2025
Accepted for publication 9 February 2026
Published 3 March 2026 Volume 2026:18 565542
DOI https://doi.org/10.2147/IJWH.S565542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Hongchang Jing, Aifen Zong, Xiujun Gong, Linlin Zhang
Department of Cardiology, The People’s Hospital of Huantai County (The 9th People’s Hospital of Zibo), Zibo, 256400, People’s Republic of China
Correspondence: Linlin Zhang, Department of Cardiology, The People’s Hospital of Huantai County (The 9th People’s Hospital of Zibo), No. 2198 Huantai Avenue, Suo Town, Huantai County, Zibo City, Shandong Province, 256400, People’s Republic of China, Tel +86 18505338537, Email [email protected]
Introduction: Postpartum spontaneous coronary artery dissection (PSCAD) is a non-iatrogenic coronary artery wall separation typically occurring within weeks of childbirth and resulting in vessel occlusion and heart attack. This report presents a case of PSCAD involving the left main (LM) coronary artery.
Case Presentation: A 27-year-old woman was admitted to emergency care due to sudden chest pain lasting for 1.5 hours. Coronary angiography suggested complete occlusion of the LM coronary artery, and she was urgently transferred to a provincial-level hospital. A 3.0 × 22-mm Endeavor Resolute stent was implanted in the proximal LM and left anterior descending coronary arteries. Postoperatively, mechanical circulatory support was provided using veno-arterial extracorporeal membrane oxygenation (VA-ECMO), an intra-aortic balloon pump (IABP), intermittent continuous renal replacement therapy, and non-invasive ventilation. The clinical symptoms of the patient improved temporarily. However, after withdrawal of the IABP and VA-ECMO, the patient’s symptoms worsened, and she died while awaiting heart transplantation.
Conclusion: We report a rare case of PSCAD involving the LM coronary artery with the aim of enhancing clinicians’ understanding of PSCAD and providing insights for treatment approaches.
Keywords: postpartum spontaneous coronary artery dissection, acute coronary syndrome, percutaneous coronary intervention
Introduction
Postpartum spontaneous coronary artery dissection (PSCAD) is a non-iatrogenic cause of coronary artery wall separation, and the associated obstruction of the coronary artery involves intramural hematomas or intimal tears.1 PSCAD is a rare form of acute coronary syndrome (ACS), accounting for up to 43% of all cases of pregnancy-associated acute myocardial infarction (AMI) and is more common in young mothers.1 Due to the absence of traditional coronary heart disease (CHD) risk factors, it is routinely misdiagnosed.1
Compared with SCAD not associated with pregnancy, pregnancy-associated SCAD occurs in younger patients and is associated with a worse prognosis. This is especially true for PSCAD, which is thought to result from hormonally mediated weakening of the coronary arterial wall combined with abrupt hemodynamic and shear stress changes that occur during and after delivery, predisposing the patient to intimal disruption or intramural hematoma formation.2 SCAD most commonly affects the left anterior descending (LAD) and left main (LM) coronary arteries.3 LM-SCAD is considered very serious and carries significant acute risks, including high morbidity and mortality, often requiring urgent intervention (percutaneous coronary intervention [PCI]/coronary artery bypass grafting [CABG]) rather than conservative care. Additionally, in LM-SCAD, intravascular ultrasound (IVUS) or optical coherence tomography (OCT) is essential in cases with ambiguous or complex lesions, because intravascular imaging allows precise identification of the true lumen, intramural hematoma, and dissection extent, thereby enabling accurate diagnosis and guidance of safe management when angiographic findings are inconclusive.4
There is currently no clear consensus on the treatment of PSCAD, and conservative treatment should be the cornerstone for patients. However, if a patient experiences LM-SCAD or shock, urgent intervention with PCI/CABG is required.4 This report presents a case of PSCAD involving the LM coronary artery with the aim of informing future development of more accurate and effective diagnostic and treatment strategies for this condition.
Case Presentation
A 27-year-old woman was admitted to emergency care at 2:19 AM on April 6, 2023, with sudden chest pain lasting 1.5 hours. The patient had no history of smoking, alcohol consumption, or substance abuse, thereby excluding common risk factors for coronary artery disease, and had undergone a cesarean section 1 week previously. Approximately 1.5 hours prior to admission, she developed chest pain after coughing while drinking water, accompanied by back pain, profuse diaphoresis, and restlessness. The symptoms persisted without relief. Electrocardiography (Figure 1) indicated sinus rhythm, with bow-shaped ST-segment elevation of approximately 0.05–0.2 mV, fused with T waves, in leads I, augmented vector left (aVL), augmented vector right (aVR), and V1–V6, and ST-segment depression of approximately 0.05–0.1 mV in leads II, III, and augmented vector foot (aVF). On physical examination, her blood pressure (BP) was 96/50 mmHg, and her heart rate was 90 beats per minute, with low and muffled sound and no murmurs detected. Laboratory testing revealed a high-sensitivity troponin T level of 12.3 ng/L, a D-dimer level of 3.17 mg/L, and an N-terminal pro-B-type natriuretic peptide (NT-proBNP) level of 24.53 pg/mL. Transthoracic echocardiography demonstrated a left atrial diameter of 35 mm, a left ventricular diameter of 49 mm, a right atrial diameter of 40 mm, and a right ventricular diameter of 18 mm. The interventricular septal thickness measured 10 mm; the ascending aortic root diameter was 30 mm; and the main pulmonary artery diameter was 28 mm. The left ventricular ejection fraction (LVEF) was 52% as calculated by the Simpson method with reduced motion of the anterior wall. No pericardial effusion was detected. Color Doppler ultrasonography of the lower extremity veins was unremarkable. Chest computed tomography (CT) revealed widening of the main pulmonary artery (Figure 2). CT angiography (CTA) revealed no evidence of aortic dissection or fibromuscular dysplasia (FMD) (results not presented).
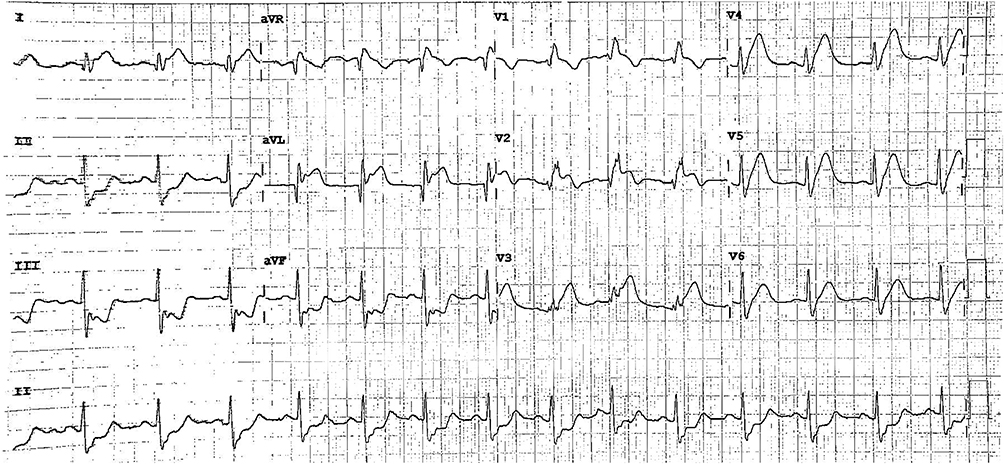 |
Figure 1 Electrocardiography indicated a sinus rhythm, with the ST segments of leads I, aVL, aVR, and V1-V6 exhibiting a bow-like elevation of approximately 0.05–0.2 mV, and a ST segment depression of approximately 0.05–0.1 mV in leads II, III and aVF. |
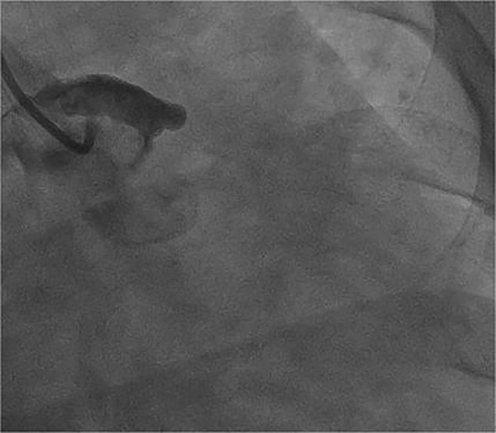 |
Figure 2 CAG suggested that the LM was completely occluded, with an anterior flow of TIMI grade 0. |
Coronary angiography (CAG) suggested complete occlusion of the left main (LM) coronary artery (Figure 2), whereas the right coronary artery showed no significant stenosis and normal antegrade flow with Thrombolysis in Myocardial Infarction (TIMI) grade 3. An attempt to advance a Runthrough guidewire across the occlusion into the distal LAD or left circumflex branch was unsuccessful. Due to the cardiogenic shock, suspected LM coronary artery occlusion, and limitations in operator skill and available mechanical support in our institution, the patient was urgently transferred to a provincial-level hospital. After admission, continuous intraoperative monitoring, including electrocardiography, invasive arterial blood pressure measurement, and oxygen saturation measurement, was instituted. After routine skin preparation and draping, intravenous heparin (50 mg) was administered. Vascular access was obtained via the right femoral artery, through which an XB3.5 guiding catheter was advanced to the ostium of the left coronary artery. CAG then demonstrated complete occlusion of the LM coronary artery. A SION guidewire was advanced successfully into the distal LAD, followed by advancement of a Finecross microcatheter beyond the LM occlusion. Contrast injection confirmed that the guidewire was positioned within the true lumen of the LAD. Thrombus aspiration was performed using an EXPORT AP aspiration catheter. Predilation of the occluded segment was carried out with a 2.0 × 20-mm balloon and a 2.5 × 15-mm Quantum Maverick balloon. Subsequently, a 3.0 × 22-mm Endeavor Resolute stent was deployed from the LM to the proximal LAD. Post-dilation was performed using a 4.0 × 12-mm Quantum Maverick non-compliant balloon. Repeat CAG showed no residual in-stent stenosis, with restoration of TIMI grade 3 flow. The right femoral arterial sheath was then exchanged, and an intra-aortic balloon pump (IABP) was advanced along the guidewire to the appropriate position and connected to the counterpulsation console, functioning normally. The IABP external tubing was secured, and the puncture site was dressed with a pressure bandage. The patient was transferred to the intensive care unit in extremely critical condition. Close monitoring of vital signs, electrocardiography, blood pressure, and puncture-site complications was continued.
Subsequent laboratory testing, including thyroid function evaluation, completion of rheumatologic and immunologic panels, detection of antiphospholipid and anti–β2-glycoprotein I antibodies, and testing for lupus anticoagulant, produced negative results. Follow-up echocardiography demonstrated a marked reduction in LVEF to 14%. Postoperatively, mechanical circulatory support was initiated with veno-arterial extracorporeal membrane oxygenation (VA-ECMO), continuous renal replacement therapy (CRRT), and noninvasive ventilation (NIV). The patient’s chest tightness improved, and both VA-ECMO and IABP were discontinued on April 26. After withdrawal of these forms of support, the patient experienced recurrent episodes of chest tightness and dyspnea. On May 4, echocardiography revealed a persistently reduced LVEF of 15%, with thinning of the interventricular septum, anterior wall, and lateral wall, and severely diminished wall motion. The patient’s NT-proBNP level increased to 11,307 pg/mL, and her troponin I level was 75 pg/mL. The patient’s family elected to transfer her to Shenzhen Hospital for evaluation for heart transplantation. She ultimately died from progressive heart failure in mid-May.
Discussion
Pregnancy-associated SCAD is a rare cause of ACS with an incompletely understood pathogenesis but a main cause of pregnancy-associated AMI.1 Because these patients typically lack traditional CHD risk factors, SCAD related to pregnancy is frequently misdiagnosed. PSCAD typically occurs within the first month or even within the first week after delivery and differs from atherosclerosis-induced AMI in several ways. PSCAD most commonly affects the LAD and LM coronary arteries,5 possibly due to differences in coronary artery anatomy and hemodynamics. Additionally, the LAD coronary artery has more branches, making it more susceptible to higher cardiac torsional forces. Data from the Mayo Clinic SCAD Registry indicate that, compared with cases of non–pregnancy-associated SCAD, patients with PSCAD are younger and have a higher risk of ST-segment elevation MI, malignant arrhythmias, cardiogenic shock, and sudden death.6 Prior studies have also confirmed that pregnancy-related SCAD is associated with an increased likelihood of LM coronary artery involvement. For example, a systematic review reported that SCAD-involved vessels in addition to the LM coronary artery are commonly observed (78%) in pregnancy-related SCAD, with the LAD coronary artery being the most frequently affected vessel (68%) and both LAD and left circumflex coronary artery involvement present in 33% of patients.4 In the present case, the patient had no risk factors such as gestational hypertension, diabetes, or hyperlipidemia and no family history of CHD. The disease occurred 1 week postpartum, with an abrupt onset and limited opportunity for intervention. CAG showed no abnormality in the right coronary artery, a finding inconsistent with atherosclerotic coronary disease and consistent with prior observations reported by Tweet et al.6
PSCAD is considered a multifactorial condition but its exact pathogenesis remains to be elucidated. In contrast to non-pregnancy-associated SCAD, in which approximately 50% of patients have FMD, PSCAD is less frequently associated with FMD or other extracoronary vascular abnormalities.6 This observation suggests that pregnancy-related hormonal and hemodynamic changes may play a more significant role in the development of PSCAD. Elevated estrogen levels promote the expression of matrix metalloproteinases, leading to degradation of the extracellular matrix and thinning of arterial walls, whereas lower estrogen levels may exert the opposite effects.7 Progesterone may further contribute by reducing collagen synthesis and increasing production of mucopolysaccharides, resulting in medial thickening.8 Moreover, the occurrence of PSCAD in the early postpartum period raises the possibility that prolactin may also be involved in its pathogenesis.9 Hemodynamic changes during pregnancy,10 including increased blood volume and cardiac output, may increase coronary artery shear stress and predispose patients to intimal disruption and intramural hematoma formation. Additional factors, such as intense physical exertion, blunt chest trauma, or repetitive coughing or sneezing, have also been implicated as potential triggers.11 In the present case, the patient had just experienced her first singleton pregnancy. CTA showed no evidence of aortic dissection or FMD, and screening for autoimmune diseases was negative. The clinical presentation was therefore mostly attributed to pregnancy-related hormonal fluctuations and hemodynamic stress leading to increased coronary arterial vulnerability, with cough serving as a triggering event. Although hormone-related SCAD also has been reported in association with oral contraceptive use, postmenopausal hormone therapy, and infertility treatments, the available data remain limited, and the precise role of sex hormones in the pathogenesis of SCAD remains unclear.7,8
Given that the clinical manifestations of SCAD are similar to those of ACS, CAG remains the most informative approach for the diagnosis of SCAD. According to the 2018 ESC Scientific Statement on SCAD,12 CAG results are categorized into four types: Type I represents the classical angiographic radiolucent “flap and linear double lumen” often associated with contrast hold-up; Type II is characterized by a long diffuse and smooth stenosis predominantly located in mid-to-distal segments; Type III involves focal or lumen stenosis, with a length less than 20 mm, similar to local stenosis caused by atherosclerotic lesions; and Type IV corresponds to total occlusion of the coronary artery, clinically presenting as acute ST-segment elevation MI. Most SCAD cases can be diagnosed angiographically. However, in cases of diagnostic uncertainty or when PCI is being considered, further examination with IVUS or OCT can provide critical information.13 In the present case, the patient presented with AMI complicated by cardiogenic shock and did not undergo further evaluation with IVUS or OCT.
Currently no clear consensus on the treatment of PSCAD has been reached, and no significant difference has emerged in the management of PSCAD versus non–pregnancy-associated SCAD. Conservative treatment should be the cornerstone of therapy for most patients.14,15 However, given the risk of recurrence, extended hospital observation periods and follow-ups are recommended. The optimal antithrombotic strategy remains uncertain. Available evidence suggests that conservative management should involve single antiplatelet therapy or, in some cases, no antithrombotic therapy,16 and thrombolysis is contraindicated in SCAD.12 In patients with LM coronary artery involvement, ongoing chest pain, hemodynamic instability, proximal vessel occlusion with TIMI flow grades 0–1 or refractory ventricular arrhythmia, revascularization with PCI or CABG should be considered.14,17 Furthermore, dual antiplatelet therapy is necessary after stent implantation. However, the use of more potent antiplatelet agents, including newer P2Y12 inhibitors and intravenous antiplatelet drugs, is generally discouraged.18 Mechanical circulatory support has been reported to be beneficial in SCAD complicated by cardiogenic shock, although its use should be carefully individualized.14 In the present case, CAG revealed complete occlusion of the LM coronary artery, prompting emergency PCI and initiation of mechanical circulatory support with an IABP and VA-ECMO. With this support, the patient’s clinical symptoms improved temporarily. However, after removal of the IABP and cessation of VA-ECMO, despite fluctuating improvement, her status deteriorated overall, with persistently elevated NT-proBNP levels. These findings suggest that early initiation and prolonged use of mechanical circulatory support may be beneficial in selected SCAD patients with LM coronary artery involvement or cardiogenic shock.
Several important limitations in the presented case should be considered. First, intravascular imaging with IVUS or OCT was not performed, which limited precise characterization of the coronary pathology, including identification of the true lumen and delineation of the presence and extent of intramural hematoma or dissection. Second, coronary CTA results were not obtained prior to intervention, limiting noninvasive evaluation of the coronary anatomy and lesion extent. Consequently, we cannot be certain whether the findings in this case reflect extensive SCAD involving the LM coronary artery versus a primary LM coronary artery occlusion. Finally, genetic testing for underlying connective tissue disorders were not conducted, limiting assessment of potential predisposing conditions and underlying etiology.
Conclusion
We report a rare case of PSCAD involving the LM coronary artery. Because young women experiencing this condition usually lack traditional risk factors for CHD, its diagnosis is challenging. This report aims to enhance clinicians’ awareness of PSCAD and to provide insights into its management. For women with a history of SCAD who are pregnant or considering pregnancy, multidisciplinary collaboration between cardiology and obstetrics is essential, and patients should be counseled regarding the risk of recurrence prior to conception.
Abbreviations
AMI, acute myocardial infarction; aVF, augmented vector foot; aVL, augmented vector left; aVR, augmented vector right; BP, blood pressure; CAG, coronary angiography; CHD, coronary heart disease; CT, computed tomography; CTA, computed tomography angiography; CABG, coronary artery bypass grafting; CRRT, continuous renal replacement therapy; FMD, fibromuscular dysplasia; IVUS, intravascular ultrasound; IABP, intra-aortic balloon pump; LM, left main; LVEF, left ventricular ejection fraction; NIV, non-invasive ventilator; NT-proBNP, N-terminal pro-B-type natriuretic peptide; OCT, optical coherence tomography; PCI, percutaneous coronary intervention; PSCAD, postpartum spontaneous coronary artery dissection; SCAD, spontaneous coronary artery dissection; VA-ECMO, veno-arterial extracorporeal membrane oxygenation.
Data Sharing Statement
The datasets generated and analyzed during the present study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the People’s Hospital of Huantai County.
Consent for Publication
Written informed consent was obtained from the patient’s family for the publication of potentially identifiable images or data presented in this article.
Funding
This study did not receive any funding in any form.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Offen S, Yang C, Saw J. Spontaneous coronary artery dissection (SCAD): a contemporary review. Clin Cardiol. 2024;47(6):e24236. doi:10.1002/clc.24236
2. Igbokwe N, Gomersall J, Ugwoke SP, Esmonde S. Pregnancy-associated spontaneous coronary artery dissection: multidisciplinary management, challenges and literature review. BMJ Case Rep. 2021;14(12):e244851. doi:10.1136/bcr-2021-244851
3. Merlo AC, Rosa GM, Porto I. Pregnancy-related acute myocardial infarction: a review of the recent literature. Clin Res Cardiol. 2022;111(7):723–6. doi:10.1007/s00392-021-01937-5
4. Morosato M, Gaspardone C, Romagnolo D, et al. Left main spontaneous coronary artery dissection: clinical features, management, and outcomes. JACC Cardiovasc Interv. 2025;18(8):975–983. doi:10.1016/j.jcin.2025.01.427
5. Elkayam U, Jalnapurkar S, Barakkat MN, et al. Pregnancy-associated acute myocardial infarction: a review of contemporary experience in 150 cases between 2006 and 2011. Circulation. 2014;129(16):1695–1702. doi:10.1161/CIRCULATIONAHA.113.002054
6. Tweet MS, Hayes SN, Codsi E, Gulati R, Rose CH, Best PJM. Spontaneous coronary artery dissection associated with pregnancy. J Am Coll Cardiol. 2017;70(4):426–435. doi:10.1016/j.jacc.2017.05.055
7. Dang YP. The Correlation Between EMMPRIN-Mediated Metalloproteinases in the Uterus and Vascular Tissue Matrix of Pregnant Rats and the Mechanism of Estrogen and Progesterone Response. Hubei: Huazhong University of Science and Technology; 2013.
8. Mori R, Macaya F, Giacobbe F, et al. Association between hormone therapy and short-term cardiovascular events in women with spontaneous coronary artery dissection. Rev Esp Cardiol. 2023;76(3):165–172. doi:10.1016/j.recesp.2022.06.012
9. Turley TN, Kosel ML, Bamlet WR, et al. Susceptibility locus for pregnancy-associated spontaneous coronary artery dissection. Circ Genom Precis Med. 2021;14(4):e003398. doi:10.1161/CIRCGEN.121.003398
10. Zeven K. Pregnancy-associated spontaneous coronary artery dissection in women: a literature review. Curr Ther Res Clin Exp. 2023;98:100697. doi:10.1016/j.curtheres.2023.100697
11. Saw J, Aymong E, Sedlak T, et al. Spontaneous coronary artery dissection: association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv. 2014;7(5):645–655. doi:10.1161/CIRCINTERVENTIONS.114.001760
12. Adlam D, Alfonso F, Maas A, Vrints C. European Society of Cardiology, acute cardiovascular care association, SCAD study group: a position paper on spontaneous coronary artery dissection. Eur Heart J. 2018;39(36):3353–3368. doi:10.1093/eurheartj/ehy080
13. Zhang QQ, Wu S, Yan H. Progress in the study of spontaneous coronary artery dissection. Internal Med J Critical Care. 2023;29(1):61–64.
14. Pristera N, Chaudhury P, Van Iterson EH, Cho LS. Spontaneous coronary artery dissection: principles of management. Cleve Clin J Med. 2021;88(11):623–630. doi:10.3949/ccjm.88a.20162
15. Ahmed SA, Mohamed AH, Waberi MM, et al. A multivessel spontaneous coronary artery dissection presented with an acute coronary syndrome that was conservatively managed. A case report. Radiol Case Rep. 2023;18(7):2381–2384. doi:10.1016/j.radcr.2023.03.044
16. Cerrato E, Giacobbe F, Quadri G, et al. Antiplatelet therapy in patients with conservatively managed spontaneous coronary artery dissection from the multicentre DISCO registry. Eur Heart J. 2021;42(33):3161–3171. doi:10.1093/eurheartj/ehab372
17. Ahmed SA, Karataş M, Öcal L, Mohamud MA, Abdi IA, Hassan MO. A 28-year-old male with spontaneous coronary artery dissection complicated by apical thrombus and acute ischemic stroke: an interesting case. Radiol Case Rep. 2023;18(1):246–249. doi:10.1016/j.radcr.2022.10.001
18. Luong C, Starovoytov A, Heydari M, Sedlak T, Aymong E, Saw J. Clinical presentation of patients with spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2017;89(7):1149–1154. doi:10.1002/ccd.26977
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.