Back to Journals » Clinical Interventions in Aging » Volume 15
Postoperative Physical Therapy to Prevent Hospital-acquired Pneumonia in Patients Over 80 Years Undergoing Hip Fracture Surgery—A Quasi-experimental Study
Authors Ståhl A, Westerdahl E ![]()
Received 10 June 2020
Accepted for publication 31 July 2020
Published 1 October 2020 Volume 2020:15 Pages 1821—1829
DOI https://doi.org/10.2147/CIA.S257127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Anna Ståhl,1,2 Elisabeth Westerdahl3
1Department of Physiotherapy, Örebro University Hospital, Örebro, Sweden; 2Department of Knowledge-Driven Management, Health Care Administration, Region Örebro County, Örebro, Sweden; 3University Health Care Research Center, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
Correspondence: Elisabeth Westerdahl
Associate Professor, Physiotherapist, University Health Care Research Center, Örebro University Hospital, Örebro SE-701 85, Sweden
Tel +46 19 602 41 49
Email [email protected]
Background: Hip fracture requiring surgical fixation is a common condition with high mortality and morbidity in the geriatric population. The patients are usually frail, and vulnerable to postoperative complications and delayed recovery. Few studies have investigated physical therapy methods to prevent hospital-acquired pneumonia (HAP) after hip fracture surgery.
Objective: To explore whether an intensified physical therapy regimen can prevent HAP and reduce hospital length of stay in patients aged 80 and older, following hip fracture surgery.
Patients and Methods: The inclusion criterion was patients aged 80 or older who had undergone hip fracture surgery at Örebro University Hospital, Sweden during eight months in 2015– 2016 (the “physical therapy group”) (n=69). The study has a quasi-experimental design with a historical control group (n=64) who had received routine physical therapy treatment. The physical therapy group received intensified postoperative physical therapy treatment, which included daily supervised early mobilization and coached deep breathing exercises with positive expiratory pressure (PEP). The patients were instructed to take deep breaths, and then exhale through the PEP-valve in three sessions of 10 deep breaths, at least four times daily. Early mobilization to a sitting position and walking was advised as soon as possible after surgery.
Results: There was a significantly lower incidence of HAP in the physical therapy group; 2/69 (3%, 95%CI: 1– 10) compared to the historical control group 13/64 (20%, 95%CI: 12– 32%) (p=0.002). Patients in the physical therapy group had a significantly shorter length of stay than the control group (10.6± 4 vs 13.4± 9 days, p=0.022).
Conclusion: Intensified physical therapy treatment after hip fracture surgery may be of benefit to reduce the incidence of HAP in patients over 80 years; however, the results need to be confirmed in randomized controlled trials.
Keywords: breathing exercises, hospital-acquired infection, mobilization, physical therapy, postoperative, prevention
Introduction
Hip fracture surgery has become an increasing health issue and is one of the leading causes for hospital admission in the aging population.1,2 Pneumonia is considered a serious complication after geriatric hip fracture surgery, with increased risk of readmission and mortality.3,4 Age over 80 years has been associated with an increased risk of pneumonia.5 An incidence of pneumonia of approximately 4–5% after hip fracture surgery has been described in a retrospective cohort study by the American College of Surgeons3 and in a Canadian cohort.6
Hospital-acquired pneumonia (HAP) is defined as pneumonia that occurs 48 h or more after admission and should not have appeared to be incubating at the time of admission.7 The pneumonia may arise from surgical or other treatment interventions or regardless of cause within the health-care system. Besides basic hygiene and rational use of antibiotics, there is a lack of proven preventive interventions to reduce the incidence of HAP.8,9 A comprehensive pulmonary rehabilitation program in elderly patients (≥65 years) undergoing hip fracture surgery in China has been shown to reduce the incidence of postoperative pneumonia.5 Otherwise, there is, to authors’ knowledge, limited scientific evidence for effective nonpharmacological rehabilitation strategies to prevent HAP after hip fracture surgery. There are published US10 and European11 guidelines for treatment of HAP, with recommendations on HAP diagnosis, treatment, and prevention. These guidelines primarily focus on pharmacological strategies and most on the literature on prevention of HAP have focused primarily on mechanically ventilated patients.
Early mobilization and deep breathing exercises are sometimes recommended as a complement to antibiotics for treatment of community-acquired pneumonia,12 but the effect of such nonpharmacological interventions regarding prevention of HAP has not been sufficiently evaluated.13 Early mobilization is considered an important factor for avoiding postoperative complications and for achieving as high a functional level as possible in older patients after hip surgery.14 Delayed mobilization to walking following hip fracture has long been considered to increase the risk of pneumonia and increased length of hospital stay.15
Early mobilization, especially if walking is achieved, can accelerate functional recovery and reduce the length of stay among patients following surgery for hip fracture.14,16 Chest physical therapy including deep breathing exercises is often recommended to surgical patients to increase lung volumes, change the breathing pattern, improve oxygenation, and facilitate secretion mobilization. To the authors knowledge, there are no studies that have assessed whether physical therapy interventions with deep breathing exercises and early mobilization can prevent care-related pneumonia in elderly patients who have undergone hip fracture surgery.
The aim of this study was to explore whether intensified postoperative physical therapy including deep breathing exercises and early mobilization can prevent HAP and reduce length of stay in patients aged 80 and older following hip fracture surgery.
Patients and Methods
Study Design and Patients
The design was a prospective, quasi-experimental study, including a physical therapy treatment group (n=69) and a historical control group (n=64). The inclusion criterion was patients aged 80 or older who had undergone surgery for hip fracture at the Department of Orthopedic Surgery at Örebro University Hospital, Örebro, Sweden. To be included, patients further needed to understand instructions and be able to perform physical therapy-administered breathing exercises and mobilization. Patients with a diagnosis of pneumonia on arrival at the hospital were not included. Other exclusion criteria were previous surgical procedures (thoracic and abdominal), impaired ability to swallow, impaired cough reflex, impaired consciousness, trauma to the thorax or head or immunosuppression.
Patients in both groups received standardized preoperative physical therapy information and daily postoperative physical therapy as conventionally used at the clinic. The ordinary physical therapy entailed passive and active bed exercises, leg range of motion exercises, sitting at the edge of the bed and ambulation. Early mobilization was implemented according to ordinary routines in connection with meals and toilet visits on an individual basis, depending on patient's health status and nursing staff levels. Normally no chest physical therapy techniques including breathing exercises were provided. The physical therapy group received additional intensified treatments including deep breathing exercises and mobilization, as described below.
The patients were consecutively enrolled in the study during an eight-month period from September 2015 to May 2016. Informed consent was obtained from each patient after receiving both verbal and written information about the study. In cases where patients were unable to decide for themselves whether to participate in the study because of cognitive impairment or confusion, a next of kin was asked on the patient’s behalf. The physical therapist on the ward enrolled the patients who met the inclusion criteria, either on admission to hospital or on the first available postoperative weekday. The study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Ethical Review Board in Uppsala, Sweden (2015/291).
Clinical Setting
The setting was the Department of Orthopedic Surgery, which consists of two hospital wards for patients with a variety of orthopedic diagnoses. There are four physical therapists who work on weekdays and are on call on Saturdays, as well as on certain days during major holidays. Patients can also be postoperatively treated at a Department of Rehabilitation facility for patients requiring extended hospital care before discharge, with one physical therapist on duty during weekdays.
Physical Therapy Group
The physical therapy group received intensified in-hospital treatments including deep breathing exercises and early mobilization, in addition to standard physical therapy conventionally used at the clinic, which mainly consists of mobility exercises for the lower extremities and mobilization according to ability. The study responsible physical therapist (AS) did not participate in the intervention; rather, the ward’s regular physical therapists carried out the intervention in conjunction with other health-care personnel. The staff received both oral and written information concerning the study before it began and were further briefed from time to time over the course of the study.
Early mobilization was defined as transfer from lying in bed to sitting on the edge of the bed with the feet on the floor/sitting in a chair, and standing and walking as early as possible after surgery, preferably as soon as the day after the surgery, with focus on an upright body position on at least four occasions during the day. Patients received repeated daily information from the physical therapist about the importance of rising to a sitting position, sitting in a chair, and walking as soon as possible after the surgery. The patient’s individual ability to move decided the progression of mobilization. The patients were assisted by the physical therapist at least once a day on weekdays; on other occasions, a ward assistant nurse or nurse helped the patient with deep breathing exercises and mobilization. The staff recorded the occasions on which breathing exercises and mobilization were carried out, and assessed frequency of mobilization according to a study-specific schedule that was kept in the patient’s room.
Patients were instructed to perform four daily sessions of deep breathing with positive expiratory pressure (PEP) using a PEP-valve (Mini-PEP; Dolema AB, Täby, Sweden), expiratory target pressure 10–15 cmH2O achieved by use of resistance nipple diameters of 0.3–0.4 cm. The pressure was titrated according to standard pragmatic clinical practice, and not measured by a manometer for each individual patient. Patients who were unable to manage this device instead received a PEP breathing mask (PEP/RMT; Wellspect Health Care, Mölndal, Sweden) or a PEP blow bottle device (a bottle filled with 10 cmH2O and a 40–50 cm plastic tube, 1 cm internal diameter). The physical therapist instructed the patients to take deep breaths, hold their breath for two seconds and then exhale through the valve in three sets of 10 deep breaths, with 30–60 seconds of rest between each set, at least four times daily.
The study did not include any follow-up, the intervention ended when the patients were discharged from the hospital.
Historical Control Group
The historical control group comprised patients aged 80 and older who had undergone hip fracture surgery at Örebro University Hospital the year before (n=64). Patients who met the criteria were identified by assistance of secretaries at the Department of Orthopedic Surgery. The patients had received standard physical therapy as conventionally used at the clinic, which mainly consisted of postoperative lower extremity exercises and mobilization based on ability. The patients were most often seen by the physical therapist once a day. Breathing exercises were not included as a routine procedure in this standard treatment.
Demographic Data
The following variables were noted from the medical records: age, gender, dementia, multimorbidity, living situation and mobilization ability prior to admission. The following surgical data were recorded; fracture type, cause of fracture, site of accident, delay prior to surgery, type of surgery, duration of surgery, postoperative blood transfusion and postoperative confusion.
Physical therapy treatments that the patients received during hospitalization were assessed as date of first physical therapy session, number of daily sessions noted in the medical record, and type of physical therapy.
Assessment of Mobilization
For assessment of mobilization ability of the patients in the physical therapy group, the cumulated ambulation score (CAS)17,18 tool was used each day during the first postoperative week, every seventh day during prolonged hospitalization, and at discharge. The assessment was made by the ward-treating physical therapist. The CAS is a reliable17 and valid predictor of number of bed days, time to discharge, 30-day mortality, and postoperative medical complications in older patients with hip fracture.18 The tool describes the patient’s ability to carry out three activities—to rise from lying in bed to sitting at the edge of the bed and return to lying; sitting to standing to sitting in a chair with armrests; and walking at least three meters. Assistive devices of various types may be used. Each activity is assessed on a 3-point scale from 0 to 2, where 0=incapable of performing the activity, despite human assistance and verbal instructions; 1=can perform the activity, assisted by one or more people and/or with verbal instructions; 2=can perform the activity, safely and without verbal instructions or human assistance or supervision. This results in a daily total score between 0 and 6: the higher the score, the more independent the patient.
Outcome Measures
Primary outcome was the number of days in hospital, defined as the number of days from admission to discharge from the hospital.
Secondary outcomes were incidence of HAP (ie, the number of HAP cases that arose during hospitalization), and data concerning discharge. “HAP” was defined as pneumonia with onset 48 h or later after admission to hospital, where a diagnosis code was indicated in the medical records or where pneumonia was described explicitly in the medical records by a physician at the Department of Orthopedic Surgery at discharge. The physicians were not informed which patients were included in the study, but no regular blinding was performed in this quasi-experimental design. Data were obtained from the patients’ medical records by the principal investigator (AS), who was unblinded. Patients with a primary or secondary diagnosis of pneumonia (J12*–J18*), classified according to the Swedish version of the International Statistical Classification of Diseases and Related Health Problems, tenth revision (ICD-10-SE), in the discharge summary in the medical records, were included. The principal investigator manually reviewed the medical records to distinguish between HAP and community-acquired pneumonia. Only data from patients diagnosed with HAP was registered.
Sample Size Calculation and Statistical Analysis
A sample size calculation showed that a group size of 64 patients in each group with a power of 0.80 was needed to demonstrate a difference of one hospital day between groups, given that the standard deviation (SD) was ±two hospital days. In order to make up for possible withdrawals, an additional five patients were included in the physical therapy group.
For comparisons between groups, the chi-squared test was used for categorical data, the Mann–Whitney U-test for data on the ordinal level, and the independent t-test for continuous variables. Statistically significant differences were defined as p<0.05. Statistical analysis of quantitative data was carried out using Statistical Package for the Social Sciences (SPSS; version 23 for Windows; IBM Corp, Armonk, NY, USA).
Results
During the study period, 176 patients, aged 80 and older, with the diagnosis of hip fracture were treated at the Department of Orthopedic Surgery. Of these, 69 patients, mean age 89±5 years, were included in the physical therapy group. The main reasons for not including patients in the study were inoperable hip fracture, multitrauma, a verified diagnosis of pneumonia on admission to hospital, and/or no physical therapist available to include patients in the study on certain weekends. Other reasons included a poor general condition or impaired cognitive function severe enough to preclude informed consent to participate, or next of kin not available to provide consent for inclusion.
Demographic data for the physical therapy group and the historical control group is presented in Table 1. There were no significant differences between groups concerning gender, age, multimorbidity, or mobilization ability prior to hospitalization. However, there was a significant difference regarding a dementia diagnosis and the living situation prior to hospitalization (Table 1). The occurrence of fractures, and factors associated with surgery are presented in Table 2. The duration of surgery was longer in the physical therapy group and more patients in the control group had postoperative confusion; otherwise, there were no significant differences between the two groups.
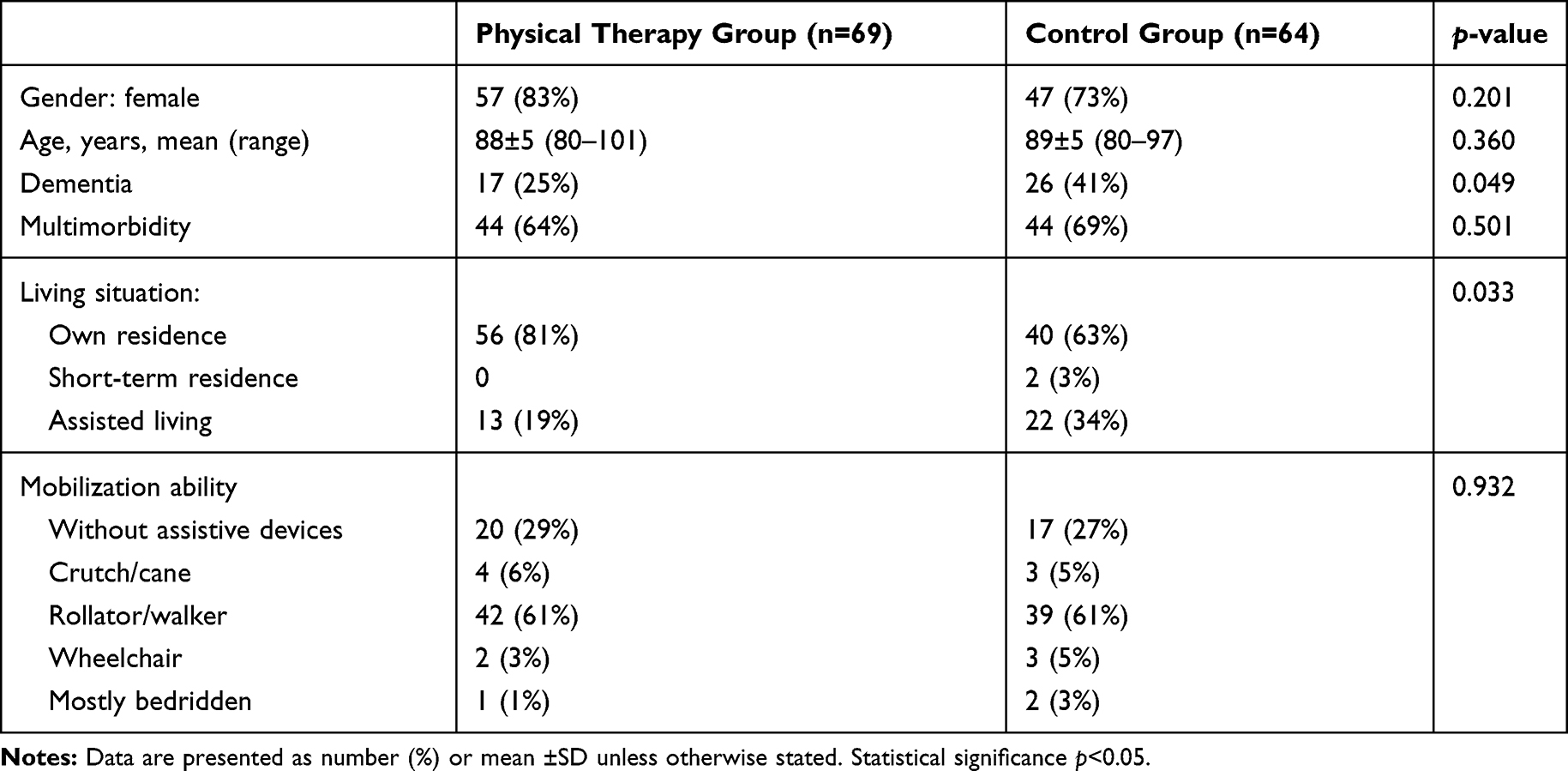 |
Table 1 Demographic Data of Included Patients Undergoing Hip Fracture Surgery |
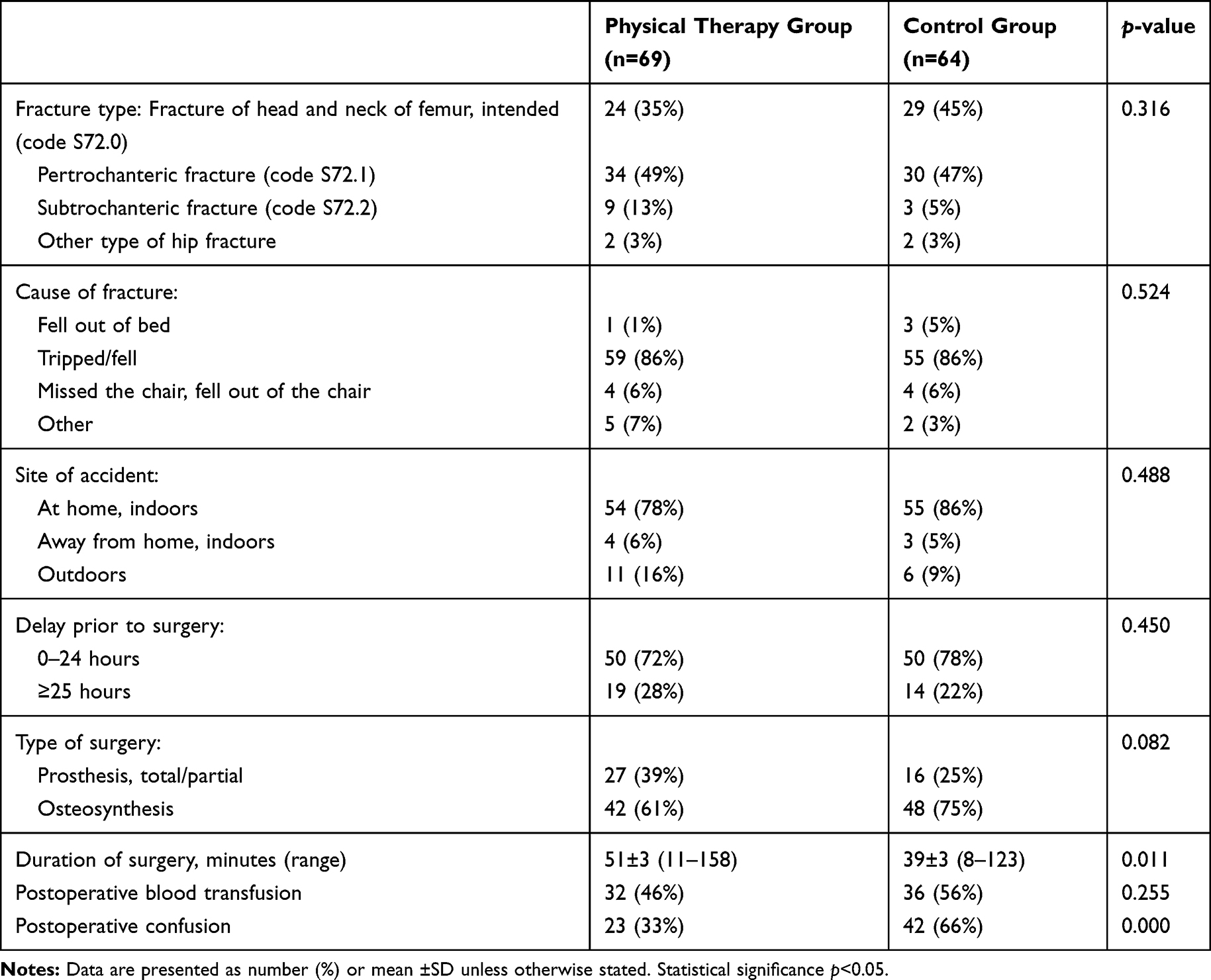 |
Table 2 Hip Fracture Types and Surgical Procedures |
Patients in the physical therapy group had a significantly shorter length of stay than the patients in the control group (11±4 (range 4–22) vs 13±9 (range 3–52) days, p=0.022). There was a significantly lower incidence of HAP in the physical therapy group; 2/69 (3%, 95%CI: 1–10) compared to the historical control group 13/64 (20%, 95%CI: 12–32) (p=0.002). Of the patients developing HAP, two patients in the physical therapy group, both men, had dementia or postoperative confusion. In the control group, nine women and four men developed HAP, four of the 13 patients were diagnosed with dementia, and 11 of the patients experienced postoperative confusion. Data concerning discharge are presented in Table 3.
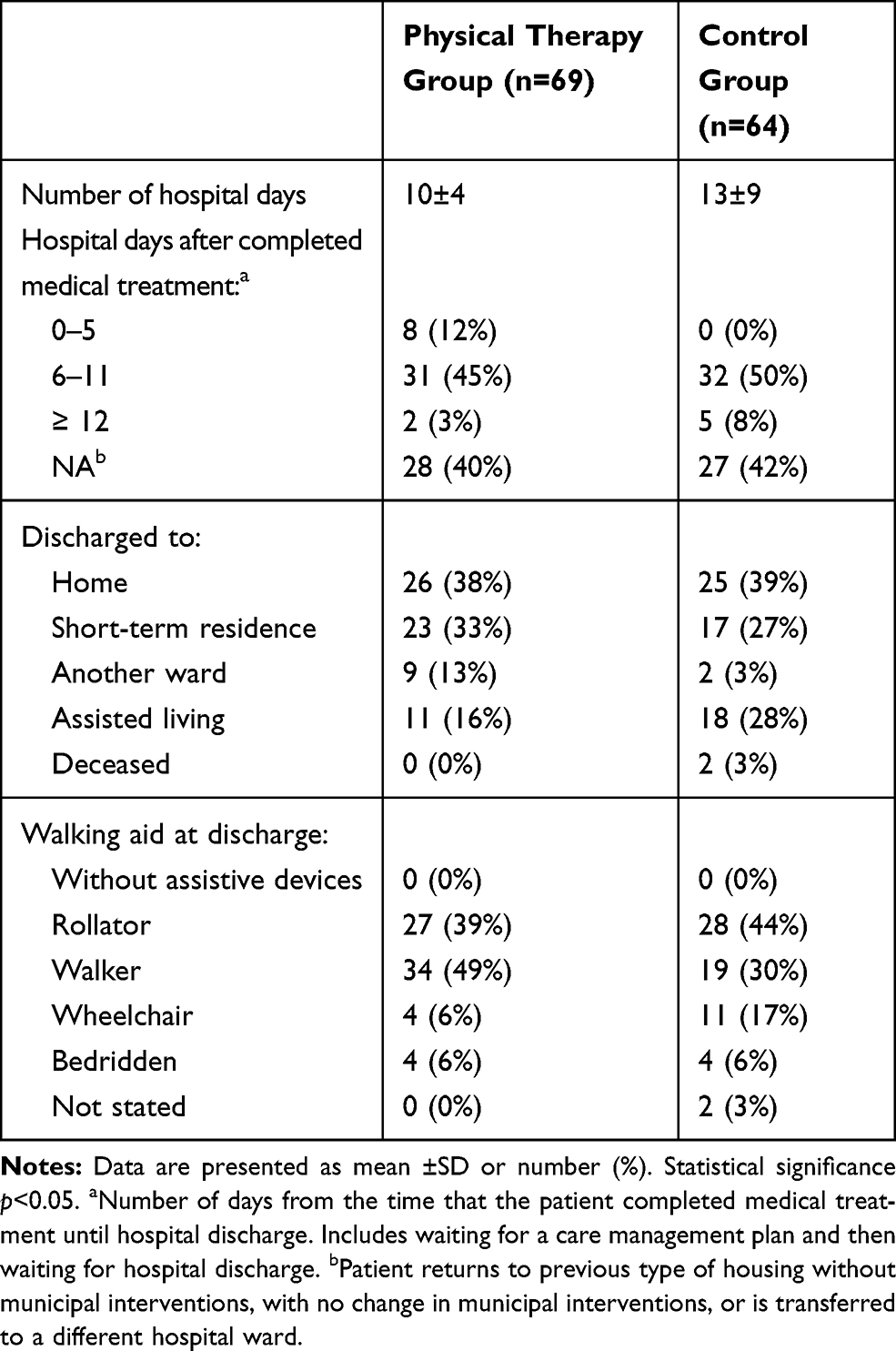 |
Table 3 Data on Discharge from Hospital |
For assessment of postoperative mobilization ability in the physical therapy group, the CAS was used at inclusion and at discharge. No data were available on the historical control group. More patients had a higher score at discharge showing a progress of being more independent in mobilization activities without assistance from the staff compared to the early postoperative period (Table 4).
 |
Table 4 Mobilization Activity in the Physical Therapy Group (n=69), According to the Cumulated Ambulation Score (CAS) Tool, at Inclusion and Discharge |
All patients needed assistance from at least one person for mobilization during the first postoperative days. Obstacles to mobilization that were noticed were severe pain, nausea, fatigue, or that the patient was confused and had problems cooperating, as well as staff shortage/lack of time. In some patients up to three health-care personnel were needed to assist during mobilization, which could result in patients not being mobilized as often as desirable because the staff did not always have time. At time of discharge, all patients were mobilized at least to sitting on the edge of the bed and six patients were completely independent in all transfers.
In the physical therapy group, some of the patients were incapable of completing the recommended sessions/repetitions of deep breathing exercises (three sessions of 10 deep breaths at least four times daily); instead, they performed the breathing exercises as many times as they were able. This was not documented, but noticed to be particularly pertinent during the first postoperative days.
Discussion
The current study suggests that intensified physical therapy, including early mobilization and daily recommended deep breathing exercises, has the potential to prevent HAP and reduce the length of hospital stay in octogenarians following hip fracture surgery. However, the results are based on nonrandomized data with considerable risk of bias, and the sample of included patients was small. The risk of cardiorespiratory death persists longer than 30 days after hip fracture surgery,19 which indicates the need for continued follow-up after discharge from hospital.
Early mobilization of patients undergoing hip fracture surgery is a widely practiced component of postoperative care to improve functional recovery and the rate of recovery compared to the pre-fracture ambulatory status.20,21 Intensive acute hospital physical therapy aimed to improve functional outcomes, increased independence, progression of gait aid (eg, from frame to crutches), and increased distance walked has been shown to be safe and to reduce hospital length of stay after isolated hip fracture.22 Prolonged bedrest has a negative effect on the entire body and can lead to conditions such as muscle atrophy and weakness, reduced joint mobility, insulin resistance, increased risk of thrombosis and impaired respiration, all of which increase the risk of impaired oxygenation, atelectasis and secretion stagnation.23 Despite knowing of the risks of prolonged bedrest, a number of hospitalized patients spend most of their time lying in bed, including patients who are able to get up independently. Factors that may prevent or impede postoperative patient mobilization include patients’ general state of health, degree of pain, type of anesthesia during surgery, urinary catheter, and various types of drainage.14,24
Failing to mobilize has been demonstrated to increase the risk of postoperative complications. In a study by Kenyon-Smith et al,20 bedbound patients had a complication rate of 52%, whereas mobilized patients had a complication rate of 36%. Other factors, such as postoperative delirium and preoperative health, are likewise important to consider and can adversely affect outcomes after hip fracture surgery.20,25 In the present study, all patients in the physical therapy group who contracted HAP had dementia or postoperative confusion. This becomes significant in view of the fact that in the control group, 85% had dementia or confusion.
The sample was too small to evaluate mortality. Earlier prediction models for in-hospital mortality after hip fracture surgery identified age, timing of surgery, male sex, congestive heart failure, pulmonary circulation disease, renal failure, weight loss and fluid and electrolyte disorders as essential predictors.26
Independent risk factors for a complicated course during hospitalization are increased age, delirium risk according to frailty scores, and higher American Society of Anesthesiologists (ASA) scores.27 The median postoperative day of diagnosis for pneumonia has been reported to be the fourth day following geriatric hip fracture surgery.28 The risk of hip fracture increases with rising age and a high percentage of hip fractures occur in women.29 Hip fractures are usually multifactorial in origin and reflect an increased tendency to fall, and loss of protective reflexes and muscle strength.29,30 In a previous Swedish cohort study, male sex emerged as a risk factor for developing pneumonia after hip fracture; the authors’ explanation for this was that the men had poorer health status with higher comorbidity before the surgery compared to the women.31 By contrast, in the present study, fewer men than women developed HAP, but considering that the sample was so small, in total 15 patients, no conclusions could be drawn.
Appropriate treatment for pain and basic hygiene measures are cornerstones in preventive efforts to reduce the occurrence of HAP. Cassidy et al32 and Kazaure et al33 have shown that implementation of standardized clinical protocols to prevent postoperative pneumonia in patients in the surgery department substantially reduces the number of cases of pneumonia after general surgery. Both clinical protocols included breathing exercises, elevation of head-end of bed to a sitting position, mobilization to get out of bed, and oral hygiene.32,33
The aging process entails a reduction in the elasticity of the lungs, chest wall mobility, and respiratory muscle strength, which can lead to impaired ventilation, impaired cough reflex, and consequently, difficulty in clearing mucus, which increases the risk of pneumonia.14,34 Other factors that increase the risk of pneumonia with aging are changes in the immune system, worsened nutritional status, and swallowing difficulties.34,35
Chest physical therapy may involve different breathing techniques; in this study it was chosen to advise patients to take deep breaths using a PEP device. Positive expiratory pressure is a technique that provides resistance to exhalation.36 The pressure can be achieved by using the lips, or with various assistive devices.36 It is important to emphasize a correct breathing technique, and this can be difficult especially for older patients with possible cognitive impairments. Three different devices, the PEP valve, the PEP mask, or a ”blow bottle”, were administrated to the patients in order to find the most suitable equipment for each individual patient; because of this, it may be difficult to generalize the results. The main purpose of postoperative deep breathing exercises is to increase lung volumes, change the breathing pattern, improve oxygenation, and facilitate secretion mobilization. The method is used by physical therapists in many different medical conditions to prevent various pulmonary complications, such as atelectasis, pneumonia, stagnation of secretions, and carbon dioxide retention. There is no evidence of the effect of breathing exercises in patients who already have pneumonia.37 Making a clinical diagnosis of HAP is often complicated due to the high proportion of old and frail patients who present with vague symptoms.34 Diagnostic criteria include fever, productive cough, cultures of respiratory secretions, impaired respiratory function, inflammatory markers, and X-ray-verified pulmonary infiltrates.8,9 In this study, HAP was defined as pneumonia with onset 48 h or later after hospital admission, indicated by a diagnosis code in the medical records or described explicitly by a physician in the medical records.
There are several significant limitations in this study. The results of this current study should be seen as preliminary, since this was a nonrandomized, single-center study with historical controls. Confounding factors as well as differences between groups at baseline can cause a high risk of bias as the difference in length of hospital stay between groups could be because of the difference in these baseline factors, and not because of the treatment. The current unadjusted analysis cannot exclude this possibility.
Although there was a significantly lower incidence of pneumonia in the physical therapy group, the sample size was small and the patients and physical therapists in the physical therapy group were not blinded. Given the use of a historical control group, rather than a parallel group comparison, it is important to be aware of the risk of unknown possible differences between groups that could have influenced the results.
Further limitations were that the mobilization was based on patient performance, and was not standardized. It is possible that factors other than the physical therapy treatment could have affected the results. Early mobilization is also important for the prevention of venous thrombosis, pressure ulcers, and other infections besides pneumonia, but these outcomes were not the focus of the present study.
The event of a hip fracture may result in significant functional impairment, but may also be life-threatening because of the risk of complications. Factors related to the preoperative status, time to surgery, the operation itself, medications, and postoperative care may have changed and improved over time, which cannot be ignored in the present study design with historical controls.
Pneumonia is one of the most common health-care-associated infections and it is associated with high morbidity and mortality.8 Despite development of methods for lung-protective perioperative management and pharmacological treatments, HAP may arise postoperatively in patients of all ages.8 A 2015 systematic review by McAuley et al38 found only two high-quality randomized controlled studies where interventions were taken to prevent HAP in non-intensive care patients and both studies included stroke patients. Beneficial effects from manual turning and passive mobilization in addition to standard treatment were found in one of these included studies.38 Although HAP is an important issue for older hip surgery patients, this is a relatively neglected research area in this patient group.
Conclusions
A more comprehensive physical therapy treatment including early mobilization and deep breathing exercises after hip fracture surgery may be of benefit to reduce the incidence of HAP in octogenarians. Parallel-group, randomized trials are needed to further verify current study findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Smith T, Pelpola K, Ball M, Ong A, Myint PK. Pre-operative indicators for mortality following hip fracture surgery: a systematic review and meta-analysis. Age Ageing. 2014;43(4):464–471. doi:10.1093/ageing/afu065
2. Ali AM, Gibbons CE. Predictors of 30-day hospital readmission after hip fracture: a systematic review. Injury. 2017;48(2):243–252. doi:10.1016/j.injury.2017.01.005
3. Bohl DD, Sershon RA, Saltzman BM, Darrith B, Della Valle CJ. Incidence, Risk Factors, and Clinical Implications of Pneumonia After Surgery for Geriatric Hip Fracture. J Arthroplasty. 2018;33(5):1552–1556. doi:10.1016/j.arth.2017.11.068
4. Lv H, Yin P, Long A, et al. Clinical characteristics and risk factors of postoperative pneumonia after hip fracture surgery: a prospective cohort study. Osteoporosis Int. 2016;27(10):3001–3009. doi:10.1007/s00198-016-3624-5
5. Chang SC, Lai JI, Lu MC, et al. Reduction in the incidence of pneumonia in elderly patients after hip fracture surgery: an inpatient pulmonary rehabilitation program. Medicine. 2018;97(33):e11845. doi:10.1097/MD.0000000000011845
6. Sheehan KJ, Sobolev B, Guy P, et al. Feasibility of administrative data for studying complications after hip fracture surgery. BMJ Open. 2017;7(4):e015368. doi:10.1136/bmjopen-2016-015368
7. Monegro AF, Regunath H. Hospital Acquired Infections. Treasure Island (FL): StatPearls; 2020.
8. Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111.
9. Burton LA, Price R, Barr KE, et al. Hospital-acquired pneumonia incidence and diagnosis in older patients. Age Ageing. 2016;45(1):171–174. doi:10.1093/ageing/afv168
10. American Thoracic S. Infectious Diseases Society of A. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416.
11. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociacion Latinoamericana del Torax (ALAT). Eur Respir J. 2017;50(4):3. doi:10.1183/13993003.00711-2017
12. Spindler C, Stralin K, Eriksson L, et al. Swedish guidelines on the management of community-acquired pneumonia in immunocompetent adults–Swedish Society of Infectious Diseases 2012. Scand J Infect Dis. 2012;44(12):885–902. doi:10.3109/00365548.2012.700120
13. Curtis LT. Prevention of hospital-acquired infections: review of non-pharmacological interventions. J Hosp Infect. 2008;69(3):204–219. doi:10.1016/j.jhin.2008.03.018
14. Sanguineti VA, Wild JR, Fain MJ. Management of postoperative complications: general approach. Clin Geriatr Med. 2014;30(2):261–270. doi:10.1016/j.cger.2014.01.005
15. Kamel HK, Iqbal MA, Mogallapu R, Maas D, Hoffmann RG. Time to ambulation after hip fracture surgery: relation to hospitalization outcomes. J Gerontol a Biol Sci Med Sci. 2003;58(11):1042–1045. doi:10.1093/gerona/58.11.M1042
16. Oldmeadow LB, Edwards ER, Kimmel LA, Kipen E, Robertson VJ, Bailey MJ. No rest for the wounded: early ambulation after hip surgery accelerates recovery. ANZ J Surg. 2006;76(7):607–611. doi:10.1111/j.1445-2197.2006.03786.x
17. Kristensen MT, Andersen L, Bech-Jensen R, et al. High intertester reliability of the cumulated ambulation score for the evaluation of basic mobility in patients with hip fracture. Clin Rehabil. 2009;23(12):1116–1123. doi:10.1177/0269215509342330
18. Foss NB, Kristensen MT, Kehlet H. Prediction of postoperative rehabilitation in hip fracture morbidity, mortality and patients: the cumulated ambulation score. Clin Rehabil. 2006;20(8):701–708. doi:10.1191/0269215506cre987oa
19. Khan SK, Rushton SP, Shields DW, et al. The risk of cardiorespiratory deaths persists beyond 30 days after proximal femoral fracture surgery. Injury. 2015;46(2):358–362. doi:10.1016/j.injury.2014.02.024
20. Kenyon-Smith T, Nguyen E, Oberai T, Jarsma R. Early Mobilization Post-Hip Fracture Surgery. Geriatr Orthop Surg Rehabil. 2019;10:2151459319826431. doi:10.1177/2151459319826431
21. Ko Y. Pre- and Perioperative Risk Factors of Post Hip Fracture Surgery Walking Failure in the Elderly. Geriatr Orthop Surg Rehabil. 2019;10:2151459319853463. doi:10.1177/2151459319853463
22. Kimmel LA, Liew SM, Sayer JM, Holland AE. HIP4Hips (High Intensity Physiotherapy for Hip fractures in the acute hospital setting): a randomised controlled trial. Med J Australia. 2016;205(2):73–78. doi:10.5694/mja16.00091
23. Brower RG. Consequences of bed rest. Crit Care Med. 2009;37(10 Suppl):S422–S428. doi:10.1097/CCM.0b013e3181b6e30a
24. Siu AL, Penrod JD, Boockvar KS, Koval K, Strauss E, Morrison RS. Early ambulation after hip fracture: effects on function and mortality. Arch Intern Med. 2006;166(7):766–771. doi:10.1001/archinte.166.7.766
25. Rizk P, Morris W, Oladeji P, Huo M. Review of Postoperative Delirium in Geriatric Patients Undergoing Hip Surgery. Geriatr Orthop Surg Rehabil. 2016;7(2):100–105. doi:10.1177/2151458516641162
26. Endo A, Baer HJ, Nagao M, Weaver MJ. Prediction Model of In-Hospital Mortality After Hip Fracture Surgery. J Orthop Trauma. 2018;32(1):34–38. doi:10.1097/BOT.0000000000001026
27. Folbert EC, Hegeman JH, Gierveld R, et al. Complications during hospitalization and risk factors in elderly patients with hip fracture following integrated orthogeriatric treatment. Arch Orthop Trauma Surg. 2017;137(4):507–515. doi:10.1007/s00402-017-2646-6
28. Bohl DD, Samuel AM, Webb ML, et al. Timing of Adverse Events Following Geriatric Hip Fracture Surgery: A Study of 19,873 Patients in the American College of Surgeons National Surgical Quality Improvement Program. Am J Orthop (Belle Mead NJ). 2018;47:9.
29. LeBlanc KE, Muncie HL, LeBlanc LL. Hip fracture: diagnosis, treatment, and secondary prevention. Am Fam Physician. 2014;89(12):945–951.
30. Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: A review of the literature. Maturitas. 2013;75(1):51–61. doi:10.1016/j.maturitas.2013.02.009
31. Ekstrom W, Samuelsson B, Ponzer S, Cederholm T, Thorngren KG, Hedstrom M. Sex effects on short-term complications after hip fracture: a prospective cohort study. Clin Interv Aging. 2015;10:1259–1266. doi:10.2147/CIA.S80100
32. Cassidy MR, Rosenkranz P, McCabe K, Rosen JE, McAneny D. I COUGH: reducing postoperative pulmonary complications with a multidisciplinary patient care program. JAMA Surg. 2013;148(8):740–745. doi:10.1001/jamasurg.2013.358
33. Kazaure HS, Martin M, Yoon JK, Wren SM. Long-term results of a postoperative pneumonia prevention program for the inpatient surgical ward. JAMA Surg. 2014;149(9):914–918. doi:10.1001/jamasurg.2014.1216
34. Janssens JP, Krause KH. Pneumonia in the very old. Lancet Infect Dis. 2004;4(2):112–124. doi:10.1016/S1473-3099(04)00931-4
35. Fung HB, Monteagudo-Chu MO. Community-Acquired Pneumonia in the Elderly. Am J Geriatr Pharmac. 2010;8(1):47–62. doi:10.1016/j.amjopharm.2010.01.003
36. Fagevik Olsen M, Lannefors L, Westerdahl E. Positive expiratory pressure - Common clinical applications and physiological effects. Respir Med. 2015;109(3):297–307. doi:10.1016/j.rmed.2014.11.003
37. Yang M, Yan Y, Yin X, et al. Chest physiotherapy for pneumonia in adults. Cochrane Database Syst Rev. 2013;1(2):CD006338.
38. McAuley SM, Price RJG, Phillips G, Marwick CA, McMurdo MET, Witham MD. Interventions to prevent non-critical care hospital acquired pneumonia - a systematic review. Eur Geriatr Med. 2015;6(4):336–340. doi:10.1016/j.eurger.2015.03.007
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.