Back to Journals » Patient Preference and Adherence » Volume 20
Postoperative Oropharyngeal Muscle Training Compliance in Obstructive Sleep Apnea: Growth Mixture Model
Received 3 December 2025
Accepted for publication 26 March 2026
Published 7 April 2026 Volume 2026:20 581913
DOI https://doi.org/10.2147/PPA.S581913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Xue-Mei Zhao,1 Wei-Gang Zhao2
1Department of Otolaryngology-Head and Neck Surgery, the First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China; 2Department of Geriatric, the First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China
Correspondence: Wei-Gang Zhao, Department of Geriatric, the First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, No. 17 of Lujiang Road, Luyang District, Hefei, Anhui, 230001, People’s Republic of China, Email [email protected]
Purpose: To explore developmental trajectories of oropharyngeal muscle training adherence and their influencing factors in postoperative adult patients with obstructive sleep apnea (OSA).
Patients and Methods: This study was a prospective longitudinal observational study. Using convenience sampling, adult OSA patients who were hospitalized and underwent surgery at the First Affiliated Hospital of University of Science and Technology of China from October 2023 to January 2025 were selected as the study subjects. A total of 215 patients were enrolled, with 11 lost to follow-up during the postoperative periods of 4 weeks, 8 weeks, and 12 weeks, resulting in a final analysis sample size of 204 cases. Using the General Information Questionnaire, Oropharyngeal Muscle Training Adherence Questionnaire, Self-Management Questionnaire for Adult Obstructive Sleep Apnea Patients, General Self-Efficacy Scale, and Epworth Sleepiness Scale, patients’ oropharyngeal muscle training adherence levels were assessed at 1 week, 4 weeks, 8 weeks, and 12 weeks after adult OSA surgery. A latent variable growth mixture model was applied to identify adherence development trajectories, and multivariate logistic regression analysis was used to examine the influencing factors of different trajectory categories.
Results: Three oropharyngeal muscle training adherence development trajectories were identified in adult OSA patients post-surgery: the Low-start Sustained Increase Group, the Moderate Gradual Decline Group, and the Moderate Rapid Decline Group. Multivariate logistic regression analysis identified self-management scores and GSES as significant independent predictors of trajectory group membership, with ESS also showing predictive value for certain trajectory comparisons (p < 0.05).
Conclusion: There is significant heterogeneity in postoperative oropharyngeal muscle training (OMT) adherence trajectories among adult OSA patients. Identifying these distinct patterns enables the stratification of patients for tailored interventions. Healthcare providers should prioritize individuals showing declining adherence for early, targeted support.
Keywords: obstructive sleep apnea, oropharyngeal muscle training, adherence patterns, growth mixture modeling, daytime sleepiness
Introduction
Obstructive sleep apnea (OSA) is a prevalent disorder associated with breathing difficulties during sleep, marked by repeated occurrences of apnea and hypopnea. This condition results in disturbances to normal sleep patterns and a reduction in blood oxygen levels. This condition can subsequently trigger various serious complications such as cardiovascular diseases and cognitive dysfunction, significantly impairing patients’ quality of life and overall health.1 The pathogenesis of OSA is primarily associated with anatomical narrowing of the upper airway, neuromuscular dysfunction, and abnormal ventilatory control.2 Surgery can address anatomical pathology abnormalities to treat OSA, but patients with neurological or muscular factors, particularly severe cases, may experience suboptimal postoperative outcomes or recurrence, as maintaining upper airway patency is inseparable from neuromuscular regulation.3 In recent years, with deepening understanding of OSA, Oropharyngeal myofunctional therapy (OMT) has emerged as a crucial postoperative adjuvant treatment,4 playing a significant role in improving respiratory function and preventing disease recurrence.
Oropharyngeal muscle training (OMT) holds multifaceted value in clinical practice, with its application scope extending beyond postoperative management of obstructive sleep apnea (OSA) to functional recovery following various upper airway surgeries, such as rehabilitation after head and neck tumor resection.5,6 Notably, OMT serves not only as an economical, safe, and noninvasive treatment option for mild-to-moderate OSA patients,7 but also as a crucial adjunctive approach during postoperative recovery.8
Treatment adherence reflects patients’ conformity to medical recommendations and rehabilitation plans.9 Sustained adherence is crucial for therapeutic outcomes.10 Grounded in Social Cognitive Theory (SCT), which emphasizes the reciprocal interaction among personal factors, behavioral capabilities, and environmental influences, we conceptualize OMT adherence as a self-regulated behavior requiring sustained self-regulation.11,12 However, while previous studies have examined cross-sectional adherence rates, longitudinal trajectory analyses identifying distinct adherence patterns in postoperative adult OSA patients remain scarce. Based on SCT13 and the Self-Management Framework,14 we hypothesized a priori that self-efficacy, self-management capability, and baseline disease severity (ESS)—reflecting symptom burden and motivational capacity—would significantly influence adherence trajectories. This study aims to explore the dynamic patterns of postoperative OMT adherence and the influencing factors in adult patients with OSA, thereby providing scientific evidence for the implementation of precision intervention strategies.
Subjects and Methods
Research Subjects
Adult OSA patients who were hospitalized and underwent surgery in the Department of Otolaryngology at the First Affiliated Hospital of University of Science and Technology of China (Anhui Provincial Hospital) between October 2023 and January 2025, and met the inclusion and exclusion criteria, were selected as study subjects. Inclusion criteria: (1) Meeting the diagnostic criteria for adult obstructive sleep apnea established by the Sleep Medicine Committee of the Chinese Medical Doctor Association;15 (2) Aged between 18 and 60 years; (3) Scheduled for upper airway surgery during hospitalization; (4) Patients or their legally authorized representatives have understood and signed the informed consent form. Exclusion criteria: (1) Presence of psychological or mental disorders; (2) Diagnosis of asthma; (3) Inability to comprehend or comply with the postoperative oropharyngeal muscle function exercise regimen, such as failure to complete preoperative or postoperative scale assessments.
Sample size was estimated using Kendall’s method (5–10 times the number of independent variables).16 Considering 16 independent variables and a 20% non-response rate, the target sample size was 192–200 participants. The final sample of 204 participants was divided into 3 trajectory classes (range: 69–88 per class), exceeding the minimum recommendation of 20–30 observations per class for growth mixture modeling. This study received approval from the Medical Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (Approval No.: XJS2023-2-17 (HL)). All participants provided informed consent voluntarily and signed the informed consent form.
Oropharyngeal Muscle Training
All adult OSA patients who met the criteria underwent upper airway surgery under general anesthesia, primarily Uvulopalatopharyngoplasty (UPPP), after completing preoperative examinations and ruling out surgical contraindications.
Training Protocol: The training protocol remained consistent for all participants. The assigned nurse sent oropharyngeal muscle training videos and conducted one-on-one demonstrations. The specific protocol included: (1) Tongue exercises: comprising pressing the tongue tip firmly against the anterior hard palate and sliding, as well as suctioning the entire tongue backward and upward; (2) Soft palate and pharyngeal muscle training: such as sustaining the “a” sound, cheek puffing, and swallowing exercises. Training frequency and duration: Patients were required to complete training twice daily, with each session lasting 15–20 minutes. Training compliance was assessed through participant self-reporting.
Patient Education and Supervision: Prior to discharge, specially trained nurses provided standardized education including instructional videos and one-on-one demonstrations to ensure proper exercise technique. Structured telephone follow-ups at 4, 8, and 12 weeks served dual purposes: (1) adherence monitoring (addressing barriers and reinforcing exercise importance), and (2) data collection regarding training completion. Compliance was assessed exclusively via self-reporting, where patients recorded daily exercise completion.
Survey Instruments
General Information Questionnaire
Demographic data: gender, age, occupation, education level, marital status, smoking history, alcohol consumption history, etc. Disease characteristic data: BMI, AHI, history of hypertension, history of diabetes, and other disease-related information.
Oropharyngeal Muscle Training Compliance Questionnaire
To evaluate the implementation of the intervention content for the study subjects. Currently, there is limited literature on OMT training adherence. This study referenced the research by Song17 to calculate adherence by determining the weekly OMT training rate (actual weekly OMT sessions/planned weekly OMT sessions × 100%).
Self-Management Behavior Questionnaire for Patients with Obstructive Sleep Apnea
The Self-Management Behavior Questionnaire for Patients with Obstructive Sleep Apnea was developed by Dong18 in 2014 to assess OSA patients’ self-management levels in areas including lifestyle, treatment, knowledge/skills, and psychological aspects. The questionnaire comprises 4 dimensions: lifestyle management (9 items), treatment management (6 items), knowledge/skills management (3 items), and psychological management (3 items), totaling 21 items. It employs a Likert 5-point scoring scale ranging from “fully achieved (5 points)” to “completely unachievable (1 point)”. The total score ranges from 21 to 105 points, calculated by summing all item scores, with higher scores indicating better patient self-management levels. A score below 63 indicates a general level, 63–84 represents an intermediate level, and above 84 denotes a good level. The total questionnaire and all dimensions achieved Cronbach’s α coefficients, content validity, and test-retest reliability above 0.724. In this study, the questionnaire’s Cronbach’s α coefficient was 0.715.19
General Self-Efficacy Scale (GSES)
The GSES is a classic psychological assessment tool for evaluating individual self-efficacy, originally developed by Schwarzer et al20 in 1981. The Chinese version was translated and revised by scholars including Wang et al21 in 2001, consisting of 10 items scored on a 4-point Likert scale. The response options are “Not at all true” (1 point), “Hardly true” (2 points), “Moderately true” (3 points), and “Exactly true” (4 points). The total score ranges from 10 to 40 points, with higher scores indicating stronger self-efficacy. 10–20 points: Low confidence, may easily doubt one’s abilities when facing stress. 20–30 points: Relatively high confidence, capable of handling daily challenges effectively. A score of 30–40 indicates particularly high self-confidence, with a greater tendency to proactively confront challenges and believe in one’s ability to solve problems. The scale demonstrates internal consistency reliability (Cronbach’s α) typically ranging between 0.76–0.90, with test-retest reliability of 0.67–0.73, making it suitable for measuring overall self-efficacy.21
Epworth Sleepiness Scale (ESS)
The ESS scale was developed by Johns22 and translated into Chinese by Chung et al23 in Hong Kong, China. It employs a semi-quantitative approach to assess patients’ daytime sleepiness and holds significant value in OSA patient evaluation.24 The scale scores patients’ sleepiness levels in eight common daily scenarios, with each item rated from 0 to 3 points (0 indicating never, 1 indicating rarely, 2 indicating sometimes, and 3 indicating frequently), yielding a total score of 24 points. A total score ≥9 suggests the presence of daytime sleepiness, with higher scores indicating more severe sleepiness. Peng et al25 conducted reliability and validity assessments of the ESS scale, with results showing a Cronbach’s α coefficient of 0.814, test-retest reliability of 0.679, and item reliabilities ranging from 0.473 to 0.698. Copyright and Disclaimer : The Epworth Sleepiness Scale was used with permission from Mapi Research Trust. This study used a published version of the scale. Mapi Research Trust and the copyright holder are not liable for any consequences arising from the use of this version.
Data Collection Methods
Studies have shown that oropharyngeal muscle training, which is similar to strength and tension improvements in weight training, requires at least three months to achieve muscle remodeling effects, and may require even longer to enhance training outcomes.26 The selection of 1 week post-operation (T0) as the baseline for the initial assessment was primarily based on the following considerations: by this time, patients have typically passed the most acute phase of surgery (eg., significant pain and edema), have initially resumed oral feeding, and possess the physical condition to commence basic oropharyngeal muscle training.27 Moreover, assessments conducted at this stage can more accurately reflect the patient’s baseline status at the onset of rehabilitation. Subsequent follow-up assessment points were set at 4 weeks (T1), 8 weeks (T2), and 12 weeks (T3) post-operation. With approval from hospital administrators, the researchers screened eligible patients based on hospital medical records. After explaining the study purpose and follow-up procedures through face-to-face interviews, baseline data collection commenced upon obtaining signed informed consent forms. Upon reaching the follow-up time, conduct the follow-up survey via phone or WeChat during 16:00–17:00 (specific time to be coordinated with the patient). For patients visiting the outpatient clinic for re-examination, collected data through face-to-face interviews.
Statistical Methods
Statistical analyses were performed using IBM SPSS Statistics (version 27.0) and Mplus (version 8.11). Continuous data are presented as mean ± standard deviation, and categorical data as frequencies and percentages. To identify heterogeneous trajectories of OMT adherence in adult OSA patients after surgery, we applied growth mixture modeling (GMM). Model fit was assessed using the Akaike information criterion (AIC), Bayesian information criterion (BIC), and sample-size adjusted BIC (aBIC), with lower values indicating better fit. The optimal number of latent classes was determined by selecting the model with the lowest BIC, supplemented by the significant LMR-LRT and BLRT (p < 0.05). Classification accuracy was evaluated by entropy, where values closer to 1 indicate clearer class separation; entropy ≥ 0.8 corresponds to >90% accuracy. After identifying the trajectory classes, interclass differences in baseline characteristics were compared using the chi-square test for categorical variables and one-way ANOVA for continuous variables. Variables showing a univariate association with class membership (p < 0.05) were entered into a multivariable logistic regression model to identify independent predictors of trajectory class membership. A two-tailed p-value < 0.05 was considered statistically significant. Missing data were handled using Full Information Maximum Likelihood (FIML) estimation, which utilizes all available data points under the Missing At Random (MAR) assumption. To assess potential bias from attrition, we compared baseline characteristics between participants who completed all assessments (completers, n=204) and those lost to follow-up (dropouts, n=11) using chi-square tests and t-tests. No significant differences were found in age, gender, BMI, or baseline ESS scores (all p > 0.05), suggesting minimal selection bias affecting trajectory classification.
Results
General Information of the Survey Subjects
This study initially enrolled 215 adult OSA patients postoperatively, aged 19–66 (36.78±8.84) years. Follow-up assessments were completed for 204 participants at all three time points (4, 8, and 12 weeks), with 11 lost to follow-up. Reasons for loss included: 3 cases with changed contact information, 4 cases refusing to participate in follow-up, and 4 cases with poor compliance who failed to complete follow-up. The overall loss-to-follow-up rate was 5.1%.
Identification and Determination of Postoperative Oropharyngeal Muscle Training Adherence Trajectories in Adults with OSA
We employed GMM to analyze the trajectory of OMT adherence at four postoperative time points in adult patients with OSA, sequentially fitting between 1 to 5 latent classes. The model fit indices indicated that upon increasing the number of classes to three, the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and adjusted Bayesian Information Criterion (aBIC) values continued to decrease. Both the LMRT and the BLRT achieved statistical significance (p < 0.01), while the entropy value was 0.98, indicating high classification accuracy. However, when the number of latent classes was increased to four, neither LMRT nor BLRT reached statistical significance (p > 0.05), indicating that further increasing the number of classes did not substantially enhance model fit. To ensure model stability, we performed sensitivity analyses using 100 random starting values, with all solutions consistently converging to the same three-class model. See Table 1.
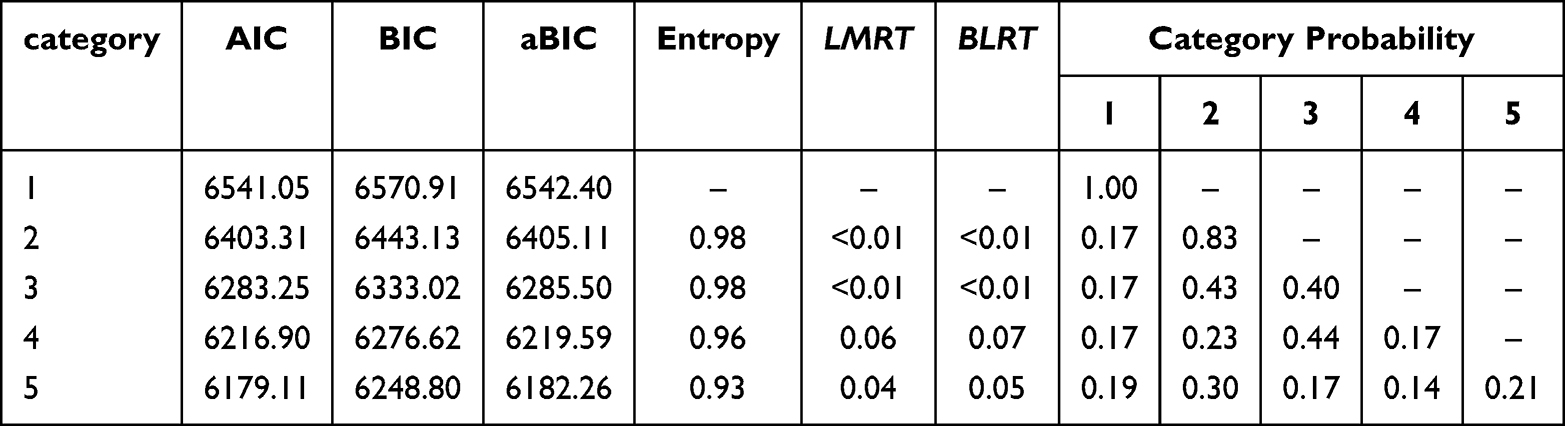 |
Table 1 Model Fit Indices for the Developmental Trajectory of OMT Adherence in Adult OSA Patients After Surgery (n=204) |
Three distinct trajectories of OMT adherence were identified among postoperative adult patients of OSA (Figure 1), characterized as follows: (1) Low-start Sustained Increase Group (17%): Starting from a low baseline (intercept I = 33.24), adherence showed a significant increasing trend (slope S = 7.85, p < 0.05). (2) Moderate Gradual Decline Group (43%): Beginning with a moderate baseline (I = 53.81), adherence demonstrated a significant gradual decline (S = −8.85, p < 0.05). (3) Moderate Rapid Decline Group (40%): Also starting from a moderate baseline (I = 53.42), adherence exhibited a significant and steeper decline over time (S = −9.41, p < 0.05).
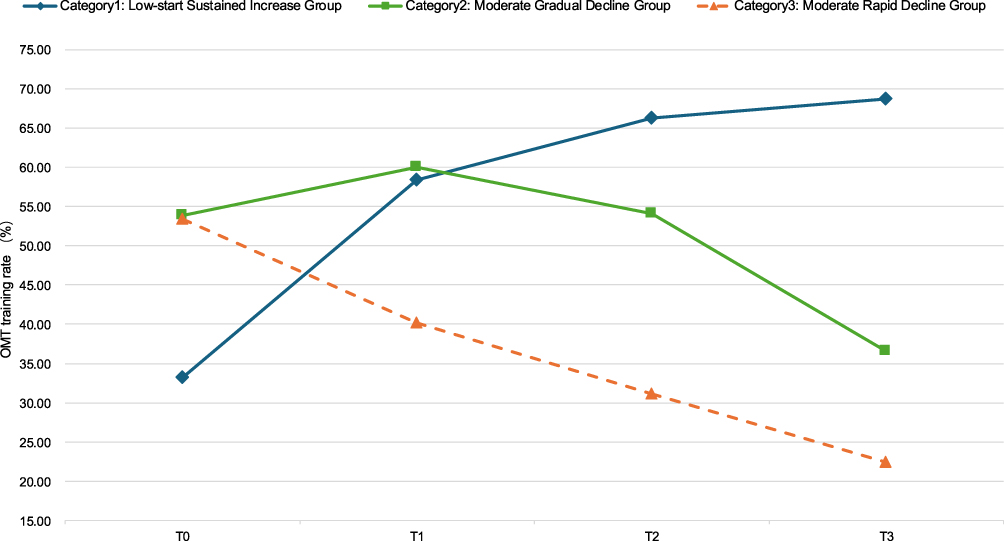 |
Figure 1 Developmental trajectories of latent variable growth mixture modeling for OMT adherence in adults with OSA after surgery. Note: T0 represents the baseline (1 week postoperatively), while T1, T2, and T3 correspond to 4, 8, and 12 weeks after adult OSA surgery, respectively. |
Identification of Predictive Factors for Developmental Trajectory Categories of Postoperative Oropharyngeal Muscle Training Compliance in Adults with OSA
Comparison of Baseline Characteristics Across Adherence Trajectory Groups
Baseline characteristics differed significantly among the three OMT adherence trajectory groups. Specifically, the AHI, self-management scores, ESS scores, GSES scores, and disease duration showed statistically significant variation (p < 0.05). See Table 2.
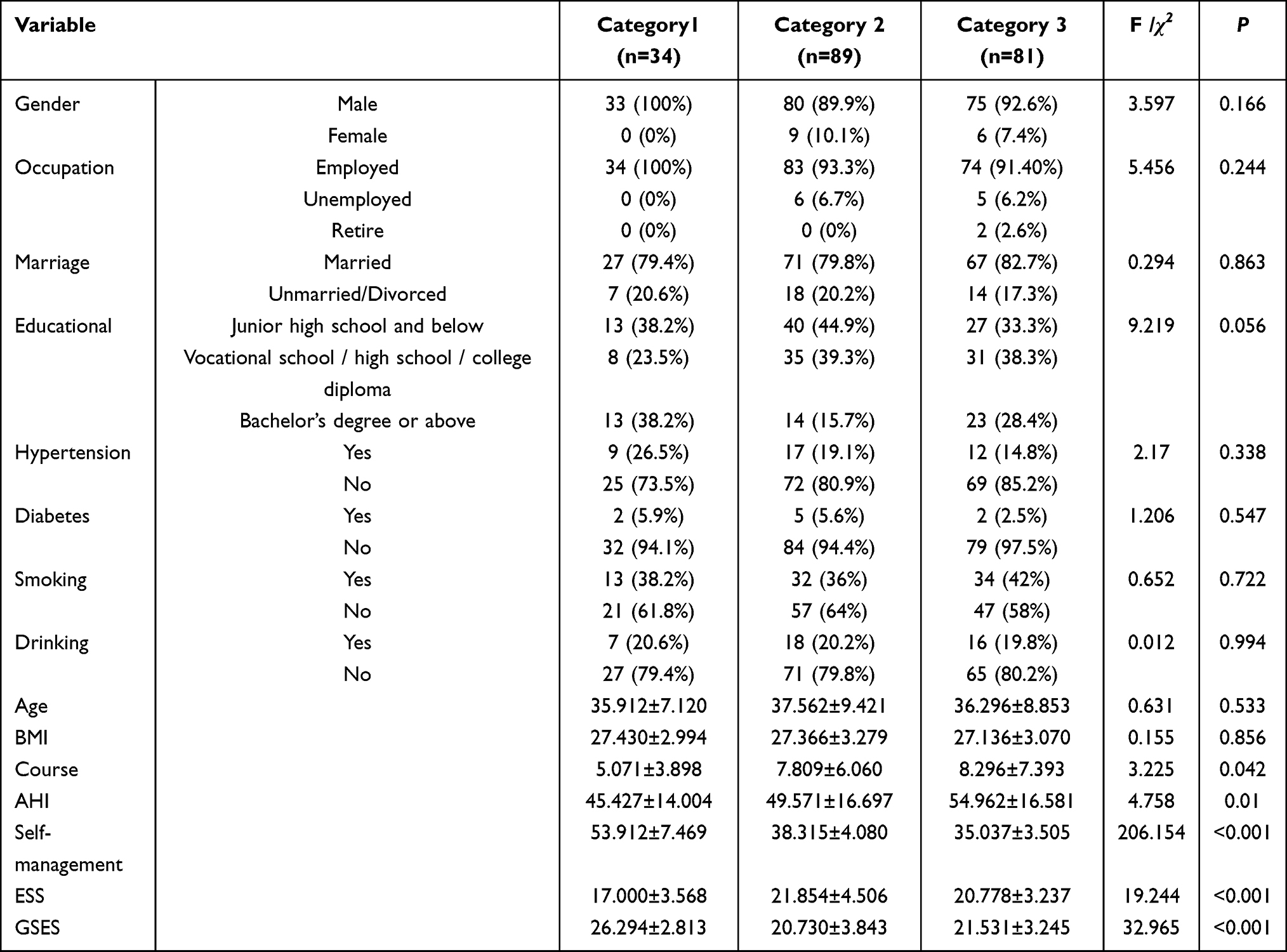 |
Table 2 Univariate Analysis Results of Patients in Each Trajectory Category (n=204) |
Independent Predictors of Trajectory Group Membership
To identify independent factors associated with trajectory group membership, variables significant in univariate analyses (p < 0.05) were entered into a multivariate logistic regression model, with continuous variables included as raw scores. Using the “Low-start Sustained Increase Group” (Category 1) as the reference, the analysis identified self-management ability score and GSES score as significant independent predictors of trajectory classification (all p < 0.05), with ESS score also showing predictive value in one comparison group (p < 0.05). The full results of the multivariate logistic regression are presented in Table 3.
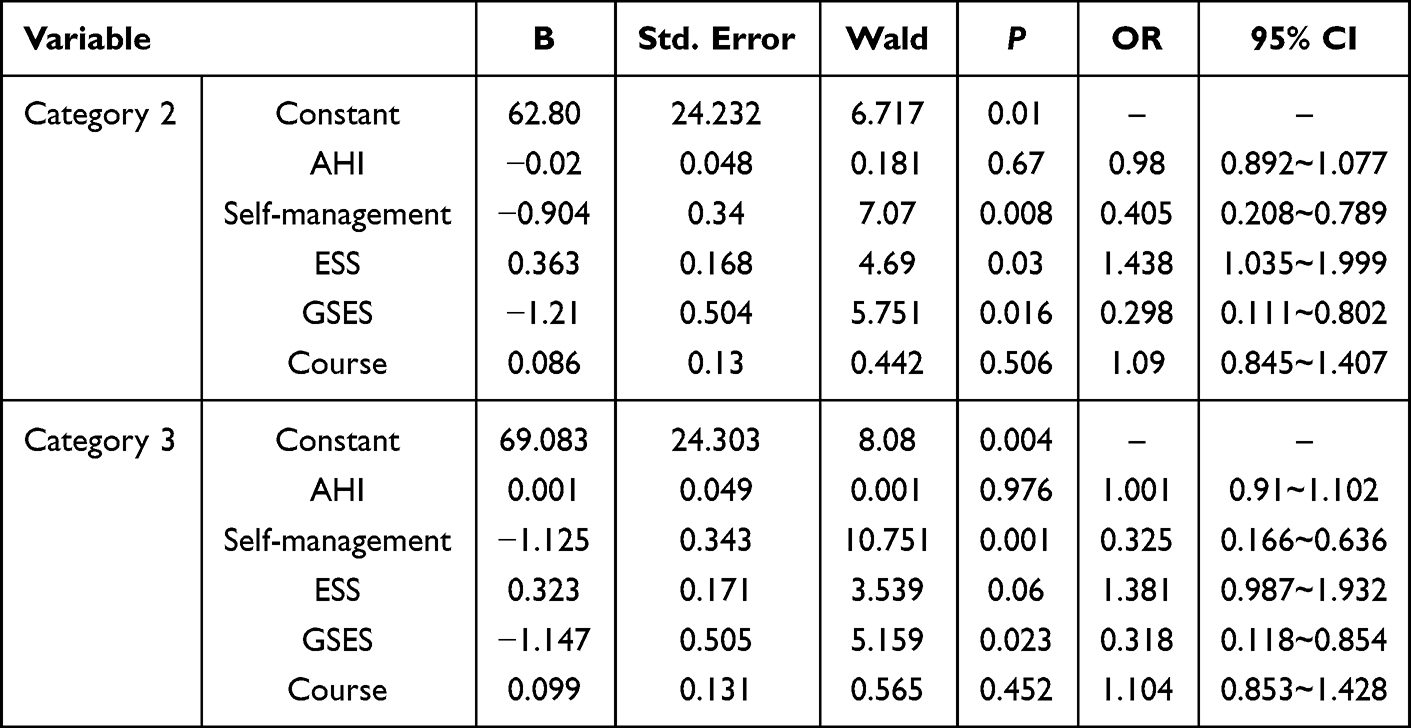 |
Table 3 Results of Multivariate Logistic Regression Analysis on Developmental Trajectory Categories of OMT Adherence in Adult OSA Patients After Surgery (n=204) |
Discussion
The Trajectory of Postoperative OMT Adherence Changes in Adult OSA Patients Exhibits Three Potential Categories
Trajectory Patterns of Postoperative OMT Adherence This study employed Growth Mixture Modeling (GMM) to characterize the longitudinal trajectories of postoperative oropharyngeal muscle training (OMT) adherence in adult OSA patients, identifying three distinct latent classes. Category 1 (17%): Low-start Sustained Increase Group (improving from 33% to 69%). These “late bloomers” successfully adapted to therapy after initial difficulties, suggesting that early struggles do not necessarily predict long-term failure. Category 2 (43%): Moderate Gradual Decline Group (peaking at 60%, then declining to 37%). As the largest subgroup, this pattern reflects typical “intervention fatigue”, underscoring the need for booster education to prevent complete dropout. Category 3 (40%): Moderate Rapid Decline Group (dropping to 22%). These high-risk patients require immediate intensive interventions (eg., motivational interviewing, family supervision) or consideration of alternative therapies within the first postoperative month. Notably, while the overall cohort exhibited a general declining trend, the identification of Category 1 reveals a subgroup capable of behavioral adaptation, offering a target for positive reinforcement strategies.
Unlike prior OMT studies that characterized adherence as a uniform linear decline over time,28,29 the present study identified three distinct trajectory patterns, revealing significant heterogeneity in postoperative OMT adherence that challenges the traditional single-population assumption. This finding suggests that aggregating adherence data into mean trends may mask critical subgroup differences, potentially explaining the inconsistent efficacy reports in previous trials that treated adherence as a homogenous construct. The finding that 83% of patients (Categories 2 and 3) struggled with sustained adherence highlights the critical need for risk-stratified interventions in postoperative OMT management. The identification of distinct phenotypes—particularly the 40% rapid decline group—enables early risk stratification within the first postoperative month, facilitating timely resource allocation and personalized intervention strategies.
The Impact of Self-Management and General Self-Efficacy on OMT Adherence in Adult OSA Patients After Surgery
The results demonstrated that both self-management scores and general self-efficacy showed significant negative correlations with declining adherence trajectories, indicating that patients with stronger self-management abilities and higher self-efficacy levels maintained more stable long-term treatment adherence. This finding aligns closely with existing literature emphasizing the central role of self-regulation theory in chronic disease management.30 Specifically, self-efficacy—defined as an individual’s belief in their ability to control behaviors—not only directly influences patients’ self-management practices but also indirectly enhances long-term adherence by mitigating the mediating pathway of self-regulatory fatigue.31,32 As a core construct of social cognitive theory, self-efficacy exerts direct effects on health management behaviors by shaping motivation levels, goal setting, and persistence behaviors.33 Patients with high self-efficacy are more inclined to adopt proactive self-regulation strategies, such as regular monitoring of physiological indicators, strict adherence to prescribed medications, and maintaining a healthy lifestyle. This aligns with findings from multiple studies. For instance, in hypertension management, enhanced self-efficacy significantly improves patients’ daily weight monitoring and standardized medication behaviors;34 in remote heart failure management, increased self-efficacy is directly associated with improved adherence to daily weight measurements.35 Furthermore, the enhancement of self-management capabilities is often achieved through structured educational interventions,36,37 as demonstrated in the Rerkasem et al38 study. The 12-week personalized exercise therapy and self-management support program significantly improved health-related quality of life in patients with multiple comorbidities by systematically training their problem-solving skills and resource utilization abilities.
Daytime Sleepiness Severity Affects OMT Compliance in Adult OSA Patients Postoperatively
As one of the core symptoms of adult OSA, the severity of daytime sleepiness shows a significant association with patients’ postoperative rehabilitation compliance.39 This study quantified the degree of daytime sleepiness using baseline Epworth Sleepiness Scale (ESS) scores and found that increased ESS scores were associated with a higher risk of decreased compliance with postoperative oropharyngeal muscle training (OMT) in adult OSA patients. This suggests that daytime sleepiness is not merely a pathophysiological manifestation of OSA, but may also influence OMT compliance by affecting patients’ cognitive function and behavioral motivation. 28 The negative correlation between daytime sleepiness severity and postoperative compliance may involve multiple mechanisms: First, the functional inhibition of thalamocortical circuits caused by chronic sleep fragmentation can impair patients’ ability to sustain attention to training instructions;40 Second, the prefrontal cortical morphological alterations (such as reduced sulcal depth in the right middle frontal gyrus) commonly observed in high ESS score populations may compromise executive function, hindering the regular implementation of training plans.41
In clinical practice, risk stratification based on ESS scores helps identify high-risk populations with poor adherence. Strengthening follow-up and supervision for such patients can more effectively enhance their adherence levels, improve long-term adherence maintenance, and promote patient recovery.
Potential Biological Mechanisms (Hypothesized)
While the observed trajectory heterogeneity is empirically robust, we acknowledge that the underlying physiological mechanisms remain speculative and require further validation. Hall et al42 and Amanda et al43 found that individual differences in neurocognitive functions can influence key processes of behavioral regulation, which may serve as potential intrinsic mechanisms underlying the observed variations in patients’ adherence patterns. These neurocognitive differences may explain why some patients (Category 1) successfully adapt to therapy while others (Category 3) rapidly discontinue despite similar baseline characteristics.
This theoretical perspective provides a potential framework for understanding adherence heterogeneity; however, these interpretations represent post-hoc hypotheses generated to explain observed patterns rather than empirically tested causal relationships. Future studies are recommended to incorporate prospective neurocognitive function assessments (eg., executive function testing, attentional capacity evaluation) to validate these proposed mechanisms and strengthen the theoretical foundation for personalized interventions.
Clinical Implications: Operationalizing Trajectory-Based Interventions
The identified adherence trajectories can be operationalized into specific, actionable nursing protocols through risk-stratified care pathways: For the Moderate Rapid Decline Group (Category 3, 40%): High-risk patients require immediate intensive intervention within the first postoperative month, including increased follow-up frequency (weekly contacts), structured motivational interviewing, family involvement in supervision, and early consideration of alternative therapeutic options (eg., CPAP therapy) if adherence remains suboptimal. For the Moderate Gradual Decline Group (Category 2, 43%): This largest subgroup represents a critical intervention window. Enhanced support should be provided around 4 weeks postoperatively (the peak adherence point), including booster education sessions, barrier assessment, and telehealth follow-up to slow the downward trend and prevent complete dropout. For the Low-start Sustained Increase (Category 1, 17%): These patients require maintenance support focusing on positive feedback to reinforce proactive behaviors and prevent late-stage decline.
This trajectory-guided approach facilitates efficient resource allocation, allowing healthcare providers to prioritize intensive interventions for the 40% rapid decline group while providing maintenance support for successful adapters, thereby optimizing limited nursing resources in postoperative care settings.
Limitations
This study has several limitations. First, training adherence was assessed primarily through patient self-reports. Although entries were verified during telephone follow-ups, this method remains susceptible to recall bias and social desirability bias, potentially leading to systematic overestimation of adherence, particularly in the “Sustained Increase” group. Such measurement limitations may result in misclassification of trajectory membership, where true non-adherers could be erroneously categorized within moderate-decline trajectories, thereby diluting between-group differences. Future studies should incorporate objective verification methods (eg., wearable sensors, electronic training loggers, or app-based monitoring) to validate self-reported data and confirm trajectory stability.
Second, as a single-center study conducted at a tertiary hospital, our findings may have limited external validity and generalizability to community settings or different surgical practices. The homogeneity of our sample—sourced from a single institution with specific postoperative care protocols—might artificially inflate trajectory stability estimates and could introduce selection bias toward patients with higher health literacy or socioeconomic status who can maintain complex rehabilitation regimens. Multi-center collaborations involving diverse clinical settings (eg., community hospitals, different geographic regions) are warranted to validate these adherence patterns across broader populations.
Third, while we identified distinct trajectories, this study mainly examined baseline influencing factors; future research could incorporate time-varying covariates (eg., symptom changes, motivational fluctuations) to dynamically understand the underlying mechanisms driving transitions between trajectory classes. Future multi-center validation incorporating objective adherence monitoring is warranted to confirm these findings and refine trajectory-based clinical protocols.
While the sample size was adequate for identifying trajectories via GMM (n=34~89 per class), the multinomial logistic regression analyses should be interpreted with caution. The smallest trajectory class (Category 1, n=34) relative to the number of predictors (16 covariates) results in a low events-per-variable ratio (EPV ≈ 2.1), which may lead to unstable estimates and wide confidence intervals for this specific subgroup comparison. Future studies with larger sample sizes are warranted to confirm these predictor associations.
Conclusion
In conclusion, this study identified distinct postoperative OMT adherence trajectories and highlighted patient self-management capacity and self-efficacy as pivotal factors influencing these patterns in adult OSA. Crucially, early identification of declining adherence—particularly within the first postoperative month—enables dynamic risk stratification and redirection into tailored care pathways. Specifically, detecting rapid decline should trigger immediate intensive nursing interventions and early consideration of alternative therapies, while recognizing gradual decline allows for timely booster education to prevent complete dropout.
Data Sharing Statement
The datasets that were utilized and/or examined in the present study can be obtained from the corresponding author upon a reasonable request.
Ethical Approval
All procedures conducted in studies that included human participants adhered strictly to the ethical standards set forth by the relevant institutional and/or national research committee, such as the specific name of the institute or committee involved. Additionally, these procedures were in alignment with the principles outlined in the 1964 Helsinki Declaration, along with its subsequent amendments, or followed comparable ethical standards that govern research practices. It is essential to ensure that all research involving human subjects complies with these established ethical guidelines to safeguard participants’ rights and welfare.
Acknowledgments
We acknowledge all the study participants for their cooperation.
Funding
No funding was received for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gottlieb DJ, Punjabi NM. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389–11. doi:10.1001/jama.2020.3514
2. Gleeson M, McNicholas WT. Bidirectional relationships of comorbidity with obstructive sleep apnoea. Eur Respir Rev. 2022;31(164):210256. 10.1183/16000617.0256-2021
3. Cozowicz C, Memtsoudis SG. Perioperative management of the patient with obstructive sleep apnea: a narrative review. Anesth Analg. 2021;132(5):1231–1243. doi:10.1213/ANE.0000000000005444
4. Li W-Y, Masse J-F, Sériès F. Myofunctional therapy for obstructive sleep apnoea. Australian Dental Journal. 2024;69(Suppl S1):S63–S67. doi:10.1111/adj.13058
5. Yang W, Nie W, Zhou X, et al. Review of prophylactic swallowing interventions for head and neck cancer. Int J Nurs Stud. 2021;123:104074. doi:10.1016/j.ijnurstu.2021.104074
6. Starmer HM, McCarroll L, Goldsmith T, et al. One-year swallowing outcomes in a head and neck cancer cohort: the impact of adherence to swallowing exercises and feeding tube use. Dysphagia. 2025. doi:10.1007/s00455-025-10918-z
7. Rueda JR, Mugueta-Aguinaga I, Vilaró J, Rueda-Etxebarria M. Myofunctional therapy (oropharyngeal exercises) for obstructive sleep apnoea. Cochrane Database Syst Rev. 2020;11(11):CD013449.
8. Wu C, Lu Z, Chen L, et al. Effects of orofacial myofunctional therapy on postoperative outcomes of upper airway surgery for adults with severe obstructive sleep apnea. J Clin Otorhinolaryngol Head Neck Surg. 2022;36:916–920.
9. Mir TH. Adherence versus compliance. HCA Healthcare J Med. 2023;4(2):219–220. doi:10.36518/2689-0216.1513
10. Lettieri MJ, Warren WA, Walter RJ, et al. Correlation between positive airway pressure and medication adherence: the healthy user effect. J Clin Sleep Med. 2024;20(7):1087–1092. doi:10.5664/jcsm.11092
11. Ewulu AR, Singh R, Roberson KB, Masicampo EJ, Feldman SR. Toward a better understanding of treatment adherence: incorporating accountability explicitly into the social cognitive theory of adherence behavior. J DermatolTreat. 2024;35(1):2351493. doi:10.1080/09546634.2024.2351493
12. Neumannova K, Hobzova M, Sova M, et al. Pulmonary rehabilitation and oropharyngeal exercises as an adjunct therapy in obstructive sleep apnea: a randomized controlled trial. Sleep Med. 2018;52:92–97. doi:10.1016/j.sleep.2018.03.022
13. Graf AS, Cohn TJ, Syme ML. Social cognitive theory as a theoretical framework to predict sexual risk behaviors among older adults. Clin Gerontol. 2021;44(3):331–344. doi:10.1080/07317115.2020.1825584
14. Mashola MK, Korkie E, Mothabeng DJ. Development of a pain self-management intervention framework for people with spinal cord injury. Afr J Prim Health Care Fam Med. 2023;15(1):e1–e12. 10.4102/phcfm.v15i1.4039
15. The Anesthesia & Pain Special Committee of Chinese Sleep Research Society. Expert consensus on preoperative screening and evaluation of adult patients with obstructive sleep apnea. Chinese J Anesthesiol. 2021;41(12):1414–1420.
16. Malone HE, Nicholl H, Coyne I. Fundamentals of estimating sample size. Nurse Res. 2016;23(5):21–25. doi:10.7748/nr.23.5.21.s5
17. Song C, Zhang C, Yang J, et al. Research progress on exercise compliance in patients with chronic obstructive pulmonary disease. J Chinese General Practice Nurs. 2020;18(36):5063–5066.
18. Dong W. The Effect of Nursing Intervention on Self-Management and Quality of Life in Patients with Obstructive Sleep Apnea [dissertation]. Xinxiang: Xinxiang Medical University, 2014.
19. Dong W. Yu G.Influence of nursing intervention on self management and quality of life of patients with obstructive sleep apnea hypopnea syndrome. Chinese Clinical Nursing. 2015;7(04):292–295.
20. Tikac G, Unal A, Altug F. Regular exercise improves the levels of self-efficacy, self-esteem and body awareness of young adults. Sports Med Phys Fitness. 2022;62(1):157–161.
21. Wang C, Hu Z, Liu Y. Evidences for reliability and validity of the chinese version of general self efficacy scale. Chin J Appl Psychol. 2001;(01):37–40.
22. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
23. Chung KF. Use of the Epworth sleepiness scale in Chinese patients with obstructive sleep apnea and normal hospital employees. J Psychosom Res. 2000;49(5):367–372. doi:10.1016/S0022-3999(00)00186-0
24. Hu Y-C, Jin Z. Evaluation of the epworth sleepiness scale in diagnosis of obstructive sleep apnea-hypopnea syndrome. Int J Respirat. 2010;30(15):936–938.
25. Peng L, Li J, Sun J, et al. Reliability and validity of the simplified Chinese version of Epworth sleepiness scale. Zhonghua Er Bi Yan Hou Tou jing Wai Ke Za Zhi. 2011;46(1):44–49.
26. Clauw DJ. Diagnosing and treating chronic musculoskeletal pain based on the underlying mechanism(s). Best Pract Res Clin Rheumatol. 2015;29(1):6–19. doi:10.1016/j.berh.2015.04.024
27. Sheen D, Abdulateef S. Uvulopalatopharyngoplasty. Oral Maxillofac Surg Clin North Am. 2021;33(2):295–303. doi:10.1016/j.coms.2021.01.001
28. Atilgan E, Kunter E, Algun ZC. Are oropharyngeal exercises effective in Obstructive Sleep Apnea Syndrome? J Back Musculoskelet Rehabil. 2020;33(2):209–216. doi:10.3233/BMR-171101
29. O’Connor-Reina C, Ignacio Garcia JM, Rodriguez Ruiz E, et al. Myofunctional therapy app for severe apnea-hypopnea sleep obstructive syndrome: pilot randomized controlled trial. JMIR mHealth and uHealth. 2020;8(11):e23123. doi:10.2196/23123
30. Liu Y, Zhang L, Jin Z, Zhang L, Song Y, He L. Association of longitudinal body mass index trajectories with phenotypic age acceleration: a cross-sectional study based on growth mixture modeling. Geroscience. 2025;47(4):5937–5949. doi:10.1007/s11357-025-01681-y
31. Smith PJ, Whitson HE, Merwin RM, O’Hayer CV, Strauman TJ. Engineering virtuous health habits using emotion and neurocognition: flexibility for lifestyle optimization and weight management (EVEN FLOW). Front Aging Neurosci. 2023;15:1256430. doi:10.3389/fnagi.2023.1256430
32. Masadeh AB, Saleh AM. The effect of a diabetes self-management mobile application on self-efficacy, self-care agency, and self-care management among patients with type 1 diabetes mellitus. Creative Nurs. 2023;29(3):286–294. doi:10.1177/10784535231211693
33. Woreta GT, Zewude GT, Józsa K. The mediating role of self-efficacy and outcome expectations in the relationship between peer context and academic engagement: a social cognitive theory perspective. Behav Sci. 2025;15(5):681. 10.3390/bs15050681
34. Egele VS, Klopp E, Stark R. How valid is bandura’s social cognitive theory to explain physical activity behavior? Eur J Investig Health Psychol Educ. 2025;15(2):20.
35. Hermansson-Borrebaeck R, Fors A, Bengtsson U, Kjellgren K, Calling S, Midlöv P. Self-efficacy in hypertension management using e-health technology: a randomized controlled trial in primary care. J Clin Hypertens. 2025;27(1):e14981. doi:10.1111/jch.14981
36. Cuppen S, van Leunen M, Henken T, et al. Association of technology-related skills and self-efficacy with willingness to participate in heart failure telemonitoring: cross-sectional observational study. JMIR Form Res. 2025;9:e68992. doi:10.2196/68992
37. Asmat K, Dhamani K, Froelicher ES, Gul R. A patient-centered self-management intervention to improve glycemic control, self-efficacy and self-care behaviors in adults with type 2 diabetes mellitus: a spirit compliant study protocol for randomized controlled trial. Diabetes Metab Syndr Obes. 2023;16:225–236. doi:10.2147/DMSO.S385715
38. Rerkasem A, Nantakool S, Kulprachakarn K, et al. The effect of standard compression adjuvant with a tailored exercise training program on health-related quality of life outcomes in treating adults with venous leg ulcer: a randomized controlled trial. Int J Low Extrem Wounds. 2023.
39. Pérez-Carbonell L, Mignot E, Leschziner G, Dauvilliers Y. Understanding and approaching excessive daytime sleepiness. Lancet. 2022;400(10357):1033–1046. doi:10.1016/S0140-6736(22)01018-2
40. Xie Y, Zhao M, Guo Y, Tian P, Liu S, Xing H. Excessive daytime sleepiness and gait disturbances in patients with Parkinson’s disease. Front Aging Neurosci. 2025;17:1626247. doi:10.3389/fnagi.2025.1626247
41. Wang L, Zhang C, Wang B, et al. Decreased cortical sulcus depth in parkinson’s disease with excessive daytime sleepiness. Clin Neuroradiol. 2025;35(2):279–286. doi:10.1007/s00062-024-01482-4
42. Hall PA, Marteau TM. Executive function in the context of chronic disease prevention: theory, research and practice. Prev Med. 2014;68:44–50. doi:10.1016/j.ypmed.2014.07.008
43. Szabo-Reed AN, Martin LE, Savage CR, Washburn RA, Donnelly JE. Pre–post intervention exploring cognitive function and relationships with weight loss, intervention adherence and dropout. Health Psychol Behav Med. 2023;11(1):2162528. doi:10.1080/21642850.2022.2162528
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.