Back to Journals » Cancer Management and Research » Volume 11
Postoperative morbidity and mortality after neoadjuvant chemotherapy versus upfront surgery for locally advanced gastric cancer: a propensity score matching analysis
Authors Wu L, Ge L, Qin Y, Huang M, Chen J, Yang Y, Zhong J ![]()
Received 1 February 2019
Accepted for publication 31 May 2019
Published 3 July 2019 Volume 2019:11 Pages 6011—6018
DOI https://doi.org/10.2147/CMAR.S203880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Liucheng Wu,1 Lianying Ge,2 Yuzhou Qin,1 Mingwei Huang,1 Jiansi Chen,1 Yang Yang,1 Jianhong Zhong3
1Department of Gastrointestinal Surgery, Affiliated Tumor Hospital of Guangxi Medical University, Nanning, Guangxi Autonomous Region 530021, People’s Republic of China; 2Department of Endoscopy, Affiliated Tumor Hospital of Guangxi Medical University, Nanning, Guangxi Autonomous Region 530021, People’s Republic of China; 3Department of Hepatobilliary Surgery, Affiliated Tumor Hospital of Guangxi Medical University, Nanning, Guangxi Autonomous Region 530021, People’s Republic of China
Background: Cohort studies have shown that neoadjuvant chemotherapy (NAC) is not associated with increased risk of postoperative complications and mortality as compared to upfront surgery (SURG).
Objective: The aim of this study was to compare postoperative morbidity and mortality after NAC with SURG.
Patients and methods: Patients who underwent gastrectomy with D2 lymphadenectomy for advanced gastric cancer (GC) between 2010 and 2017 were selected. The impact of neoadjuvant chemotherapy on surgical safety was investigated by using propensity score matching.
Results: Three hundred and seventy-seven patients were included. After propensity score matching, 86 patients in each group were matched. The percentage of patients with one or more complications was 10.5% in NAC group and 15.1% in SURG group (P=0.361), there was no mortality developed in either group. The total blood loss was significantly more in the NAC group than that in the SURG group (320.79 vs 243.37 ml, P<0.04). In univariate and multivariate of the matched cohort, sex, age (<70), BMI (<24), ASA grade, surgical procedure (open vs laparoscopy), gastrectomy extent, cTNM and Charlson index comorbidity were not associated with postoperative complications (all P>0.05).
Conclusion: This study showed that postoperative morbidity and mortality were similar for NAC group and SURG group.
Keywords: gastric cancer, surgery, postoperative morbidity, propensity score, neoadjuvant chemotherapy
Introduction
Nearly one million new patients are diagnosed with gastric cancer (GC) annually, and it is the third leading cause of cancer-related deaths worldwide.1 GC is often diagnosed in a locally advanced stage because early-stage GC is often asymptomatic.2 The 5-year survival rate is only 25–30% for advanced-stage GC patients.3 In an effort to improve this poor prognosis, different therapeutic practices, including the effects of adding chemoradiotherapy and the use of targeted therapies, have been studied and applied to improve survival. To date, several randomized controlled trials (RCTs) have appraised the effectiveness of neoadjuvant chemotherapy (NAC), and the benefit of NAC in GC has been recommended in both the European Society of Medical Oncology (ESMO) and American National Comprehensive Cancer Network (NCCN) guidelines.4–8 The rationale for NAC is downstaging of the primary tumor, improving rates of R0 resection and treating micrometastatic disease that may be present in a relatively high proportion of GC patients.9
Few studies have investigated the impact of NAC on surgical safety,5,10,11 while surgery performed in the MAGIC and FNCLCC-FFCD RCTs did not include a proper D2 lymphadenectomy in the majority of patients, and many patients had lower esophagus cancer instead of only GC.4,12 Thus, there is still a lack of evidence that a proper radical surgery (gastrectomy with D2 lymphadenectomy) can be safely performed following NAC.
The purpose of the present study was to compare the postoperative morbidity and mortality following NAC versus upfront surgery (SURG) for advanced-stage GC. Since patient characteristics may vary significantly between two different cohorts because the choice of treatment can be confounded by abounding factors, the true significance of the outcomes will not be apparent if there are no appropriate matches of patients to cohorts. In addition, propensity score matched (PSM) analysis delivers the possibility of reducing the impact of selection bias in retrospective studies. This method was used in this study to investigate the surgical safety of advanced-stage GC patients following NAC compared with that of patients undergoing SURG. We also wished to identify the risk factors that may predict postoperative complications after NAC in GC patients.
Materials and methods
Patients
The prospectively collected records of all patients at the Department of Gastrointestinal Surgery, Affiliated Tumor Hospital of Guangxi Medical University (Nanning, China) between 2010 and 2017 with histologically proven GC were retrospectively reviewed. The study data were collected and managed using Research Electronic Data Capture (REDCap) hosted at the Department of Gastrointestinal Surgery, Affiliated Tumor Hospital of Guangxi Medical University.13 Only patients who underwent curative surgery were included in this study. The exclusion criteria included stages I and IV disease, emergency operation, hybrid procedures and palliative treatment intent. Preoperative clinical tumor-node-metastasis (cTNM) staging and postoperative pathological tumor-node-metastasis (pTNM) staging were based on the 7th American Joint Committee on Cancer (AJCC) staging system.14 PSM was used to match the two groups on a 1:1 basis. The ethical approval and informed consent were waived by the Institutional Review Board. The reason for the waiver of ethical approval and informed consent by the Institutional Review Board is because the patient data was extracted from our database without patient identifiers.
Surgical procedure
All surgeries were performed by surgeons experienced in both laparoscopic and open gastrectomy. Patients received total, proximal or distal gastrectomy, depending on the anatomic location of the tumor. D2 lymphadenectomy was performed in all patients according to the guidelines of the Japanese Gastric Cancer Association. During total gastrectomy, spleen-preserving No. 10 lymph node dissection and omentectomy were performed. Multivisceral resection was performed when necessary. Reconstruction of the gastrointestinal passage was performed according to the surgeon’s preference.
Outcomes
Information on diagnostics, comorbidity, intraoperative data, adverse events, and reinterventions was retrieved from the database. Comorbidity was measured by the Charlson comorbidity index score, which uses certain diseases with different weights for each one.15 Surgical complications occurring during the hospital stay or within 30 days of discharge were considered in this study. The presence of saliva or gastrointestinal contents in the drain or during repeat laparotomy or by a contrast swallow test was defined as anastomotic leakage. A pancreatic fistula was diagnosed by any measurable drain output on or after postoperative day 3 with an amylase level 3 times higher than the serum level. Inflammation and/or prolonged fever with positive findings on computed tomography on the abdomen showed complicated fluid collection, and those requiring antibiotic therapy were defined as having “intra-abdominal infection”. Positive results obtained from bacterial culture of purulent discharge from the wound were diagnosed as a wound infection. The details of complications were documented and categorized based on the Clavien–Dindo classification system.16,17 Postoperative mortality was defined as death from any cause within the first 30 days after surgery or at any time during the initial hospitalization.
Statistical methods
Patient characteristics were summarized using descriptive statistics or contingency tables. We used Student’s t-test and chi-squared test to compare variables between the NAC group and the SURG group. PSM was used to minimize the effects of confounding influences of measured covariates on the assessed outcome between the 2 groups (NAC vs SURG). The PSM is a conditional probability of having a particular exposure given a set of baseline measured covariates.18,19 The PSM was estimated with the use of a nonparsimonious multivariable logistic-regression model with the group as the dependent variable and all the baseline characteristics outlined in Table 1 as covariates.20 Matching was performed with the use of a 1:1 matching protocol without replacement (nearest algorithm), with a caliper width equal to 0.10 of the standard deviation of the logit of the propensity score. Standardized differences were estimated for all the baseline covariates before and after matching to assess before matching imbalance and after matching balance.21 Standardized differences of less than 0.1 for a given covariate indicated a relatively small imbalance.21
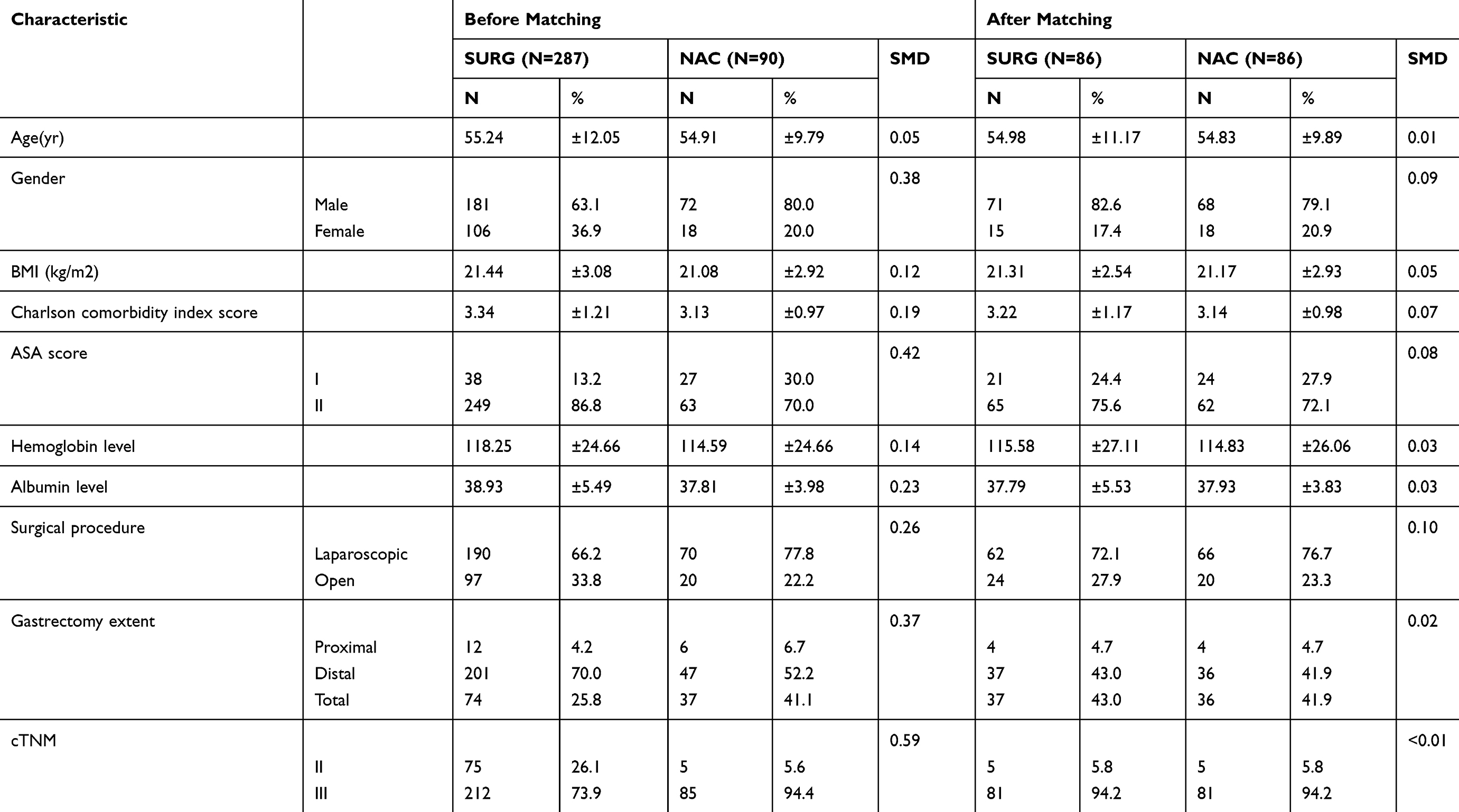 |
Table 1 Clinicopathological characteristics of GC in patients in the NAC and SURG groups |
All P-values are two-sided and have not been adjusted for multiple testing. All the statistical analyses were performed using R software, version 3.5.1.
Results
Clinicopathological characteristics of patients
Between 2010 and 2017, a total of 607 patients with histologically proven gastric cancer underwent curative gastrectomy. A total of 377 patients were included in the study (Figure 1). The NAC group contained 90 patients, and the SURG group contained 287 patients. Patient characteristics are shown in Table 1. The differences in baseline characteristics between the NAC group and the SURG group were statistically significant across sex, BMI (body mass index), Charlson comorbidity index score, ASA score, hemoglobin level, albumin level, surgical procedure, gastrectomy extent, and cTNM variates before adjusting; however, all the differences were eliminated after adjusting with the PSM (Table 1).
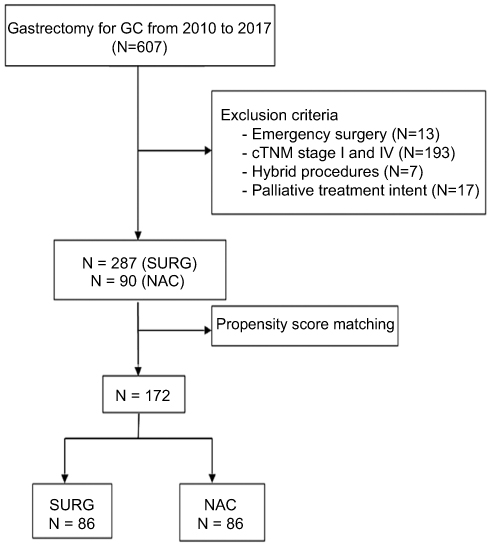 |
Figure 1 Flowchart. Abbreviations: GC, gastric cancer; NAC, neoadjuvant chemotherapy; SURG, surgery. |
Intraoperative findings
The total blood loss was significantly higher in the NAC group than in the SURG group (320.79 vs 243.37 ml, P<0.04); however, other variables, such as operative time, number of harvested lymph nodes, and multiorgan resection, did not differ significantly between these two groups (P>0.05, Table 2).
 |
Table 2 Intraoperative outcomes |
Postoperative outcomes
In the SURG and NAC groups, postoperative complications occurred in 13 (15.1%) and 9 (10.5%) patients, respectively, P=0.361. The incidence of anastomotic leakage, duodenal stump leakage, pancreatic leakage, gastroparesis, bowel obstruction, intra-abdominal bleeding, abdominal infection, wound infection/dehiscence, anastomotic bleeding and other complications were not significantly lower in the SURG group than in the NAC group (all P>0.05, Table 3). There were no mortalities in either group.
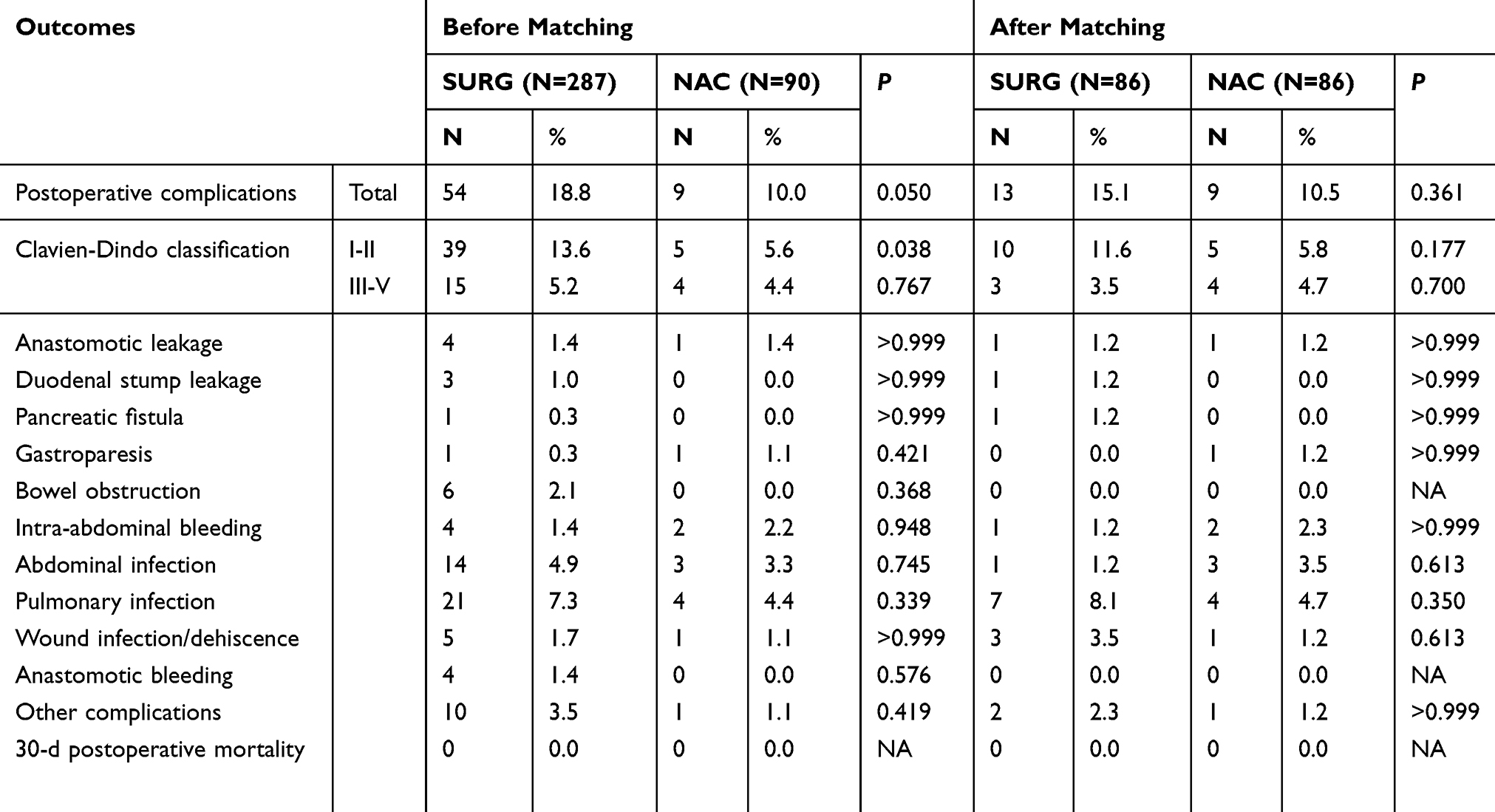 |
Table 3 Perioperative outcomes and morbidity |
Risk factors associated with postoperative complications
Both the univariate analysis and multivariate analysis showed that sex, age (<70), BMI (<24), ASA grade, surgical procedure (open vs lap), gastrectomy extent, cTNM and Charlson comorbidity index score were not related to postoperative complications (all P>0.05, Table 4).
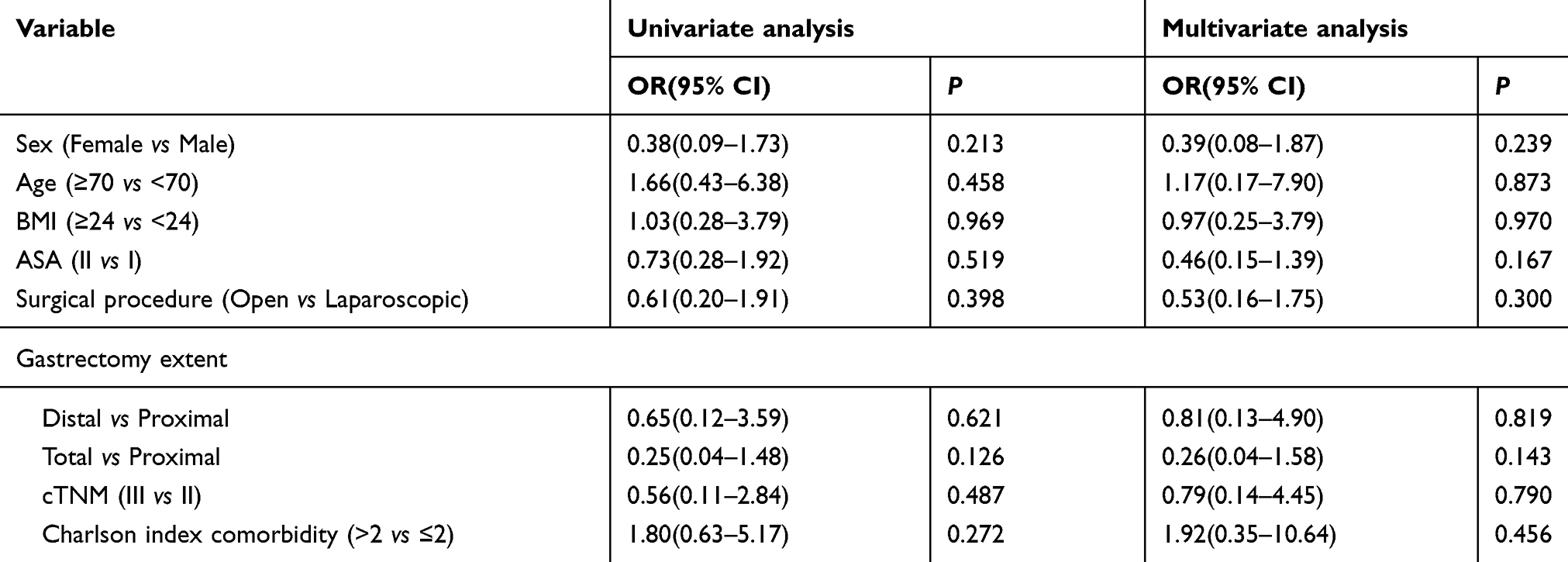 |
Table 4 Univariate and multivariate analyses of risk factors associated with overall complications |
Discussion
The goals of NAC for advanced GC are to treat micrometastasis and to improve curative resection (R0) with D2 lymphadenectomy. In addition, NAC provides in vivo testing, better tolerability and compliance with chemotherapy in the preoperative setting compared with the postoperative setting. Many reports of the effectiveness of NAC have been reported, and surgeons are seeing a greater number of patients who have undergone NAC. However, the essential problems of NAC are its negative effect on wound healing and immunocompetence. Consequently, more postoperative complications could occur. However, only a few studies have investigated the morbidity and mortality of surgery after NAC.5,10,11,22 Therefore, there is still a lack of evidence that proper radical surgery (gastrectomy with D2 lymphadenectomy) can be safely performed following NAC.
We did not observe a significant influence of NAC on postoperative morbidity and mortality in this study. Postoperative morbidity was 12.8%, with no deaths occurring in our study. These findings are comparable to previous studies; several trials reported morbidity rates of 14.3–46.8% and mortality rates of 0–5.6%;4,12,23 however, in these trials, D2 lymphadenectomy was recommended in the “Study Treatment” protocol but not described in the results or was performed less than 50% of patients.4,12,23 Observational studies where more than 90% of patients had a proper D2 lymphadenectomy also reported similar complication rates, while the morbidity rate was between 10.0–38.0%, and the mortality rate was between 0.7–1.4%.24 However, these observational studies suffer from baseline imbalance, where some clinicians tend to recommend NAC for stage III GC. Several East Asian low-volume population studies that have investigated the effect of NAC on postoperative complications found that NAC did not increase postoperative morbidity and mortality compared with surgery alone, but NAC regimens in these studies are rarely applied in modern clinical settings because of newer NAC regimens (capecitabine, oxaliplatin, docetaxel, S-1).25,26 In our study, all the patients had D2 lymphadenectomy, and the NAC regimens were popular in Asian countries. With PSM overcoming selection bias, our results are likely to be more reliable and generalizable than those of previous studies.
Although we observed no increasing risk of anastomotic leakage and duodenal dump leakage with NAC, it could be that patients who underwent NAC had much more severe consequences than patients who had upfront surgery. This possible disadvantage is currently outweighed by the benefit of NAC over upfront surgery.
Factors that might influence postoperative mortality and morbidity in patients undergoing gastrectomy for GC include age greater than 70 years, multiorgan resection, and comorbidities. While both comorbidity and age variables were included and equalized in our study, the patients’ mean age was approximately 55 years, so the safety profile of NAC for older patients (>70) is still unanswered; future investigations are warranted to determine the safety and effectiveness of NAC for older patients.
We observed significantly more blood loss in the NAC group, which was completely expected because of NAC-induced fibrosis. Increased complications are expected if more blood loss occurred during surgery. But the incidence of complication does not increase in the NAC group, the possible reason is that more blood loss occurred because of tissue fibrosis surrounding lymph nodes after NAC, not from major vessel injuries or major organ injuries. We also evaluated the impact of sex, age, BMI, ASA grade, surgical procedure, gastrectomy extent, cTNM, and Charlson comorbidity index score on our patients, and no associations were found between them and postoperative complications. These results suggest that NAC is safe and feasible even in high-risk patients.
Sarcopenia was shown to be associated with toxicity in GC patients who had NAC,27 and it is well-recognized that frail and sarcopenic patients are susceptible to severe outcomes from a complication.28 In the clinical setting, we see that some sarcopenic patients’ health status greatly improved after NAC, but we still could not recommend NAC for sarcopenic patients because of the lack of data from this study.
The complication rate in the SURG group was higher than that in the NAC group (15.1% and 10.5%, respectively, P=0.361), and the reason for this higher complication rate in the SURG group is unclear. One possible explanation is that patients who were recommended to have NAC and were able to complete their NAC could have been physically stronger and fitter, and therefore a complication is less likely to occur.
The strength of the present study is the dataset with detailed information on postoperative complications. Although this study spanned from 2010 to 2017, surgery techniques were consistent in our institution during this period. Since the NAC regimens in our study varied slightly over time, the risk attributable to any specific regimen is unlikely. Our surgical team consisted of six surgeons who were experienced in both open and laparoscopic gastrectomy for GC, so individual surgeon bias was unlikely to influence the resultant surgical complications.
Despite the strength mentioned above, some limitations of the present study should be acknowledged. First, this is a single-center retrospective study, and selection bias may have influenced the outcomes. Second, the patients were not randomized into the two groups. Although two quite similar groups were reached with a validated matching model, the role of the treatment segment in an analysis is always a concern.
In summary, NAC for GC has been strongly recommended in guidelines without strong evidence about its impact on surgical safety in patients who receive a complete extended (D2) lymphadenectomy. This study is the first PSM analysis to demonstrate that NAC can be safely administered to patients without increasing postoperative morbidity and mortality rates. Concerns about the possible increase of postoperative complications should not deter the use of NAC in advanced-stage GC patients.
Acknowledgments
This work is supported by the National Natural Science Foundation of China (81760521), the Graduate Course Construction Project of Guangxi Medical University (YJSA2017014), and 'Guangxi BaGui Scholars' Special Fund.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. doi:10.3322/caac.21208
2. Russo A, Li P, Strong VE. Differences in the multimodal treatment of gastric cancer: east versus west. J Surg Oncol. 2017;115(5):603–614. doi:10.1002/jso.24597
3. Allemani C, Weir HK, Carreira H, et al. Global surveillance of cancer survival 1995-2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet. 2015;385(9972):977–1010. doi:10.1016/S0140-6736(14)62038-9
4. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11–20. doi:10.1056/NEJMoa055531
5. Schuhmacher C, Gretschel S, Lordick F, et al. Neoadjuvant chemotherapy compared with surgery alone for locally advanced cancer of the stomach and cardia: european organisation for research and treatment of cancer randomized trial 40954. J Clin Oncol. 2010;28(35):5210–8. doi:10.1200/JCO.2009.26.6114
6. Oki E, Emi Y, Kusumoto T, et al. Phase II study of docetaxel and S-1 (DS) as neoadjuvant chemotherapy for clinical stage III resectable gastric cancer. Ann Surg Oncol. 2014;21(7):2340–2346. doi:10.1245/s10434-014-3594-9
7. Yoshikawa T, Sasako M, Yamamoto S, et al. Phase II study of neoadjuvant chemotherapy and extended surgery for locally advanced gastric cancer. Br J Surg. 2009;96(9):1015–1022. doi:10.1002/bjs.v96:9
8. Kosaka T, Akiyama H, Makino H, et al. Preoperative S-1 and docetaxel combination chemotherapy in patients with locally advanced gastric cancer. Cancer Chemother Pharmacol. 2014;73(2):281–285. doi:10.1007/s00280-013-2350-3
9. Bonavina L, Soligo D, Quirici N, et al. Bone marrow-disseminated tumor cells in patients with carcinoma of the esophagus or cardia. Surgery. 2001;129(1):15–22. doi:10.1067/msy.2001.109503
10. Fujitani K, Ajani JA, Crane CH, et al. Impact of induction chemotherapy and preoperative chemoradiotherapy on operative morbidity and mortality in patients with locoregional adenocarcinoma of the stomach or gastroesophageal junction. Ann Surg Oncol. 2007;14(7):2010–2017. doi:10.1245/s10434-006-9198-2
11. Valenti V, Hernandez-Lizoaín JL, Beorlegui MC, et al. Morbidity, mortality, and pathological response in patients with gastric cancer preoperatively treated with chemotherapy or chemoradiotherapy. J Surg Oncol. 2011;104(2):124–129. doi:10.1002/jso.v104.2
12. Ychou M, Boige V, Pignon J-P, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol. 2011;29(13):1715–1721. doi:10.1200/JCO.2010.33.0597
13. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009. doi:10.1016/j.jbi.2008.08.010
14. Washington K, Murray DR, Gow KW, et al. 7th edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol. 2010;17(12):3077–3079. doi:10.1245/s10434-010-1022-3
15. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
16. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
17. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
18. Rubin DB. Using propensity scores to help design observational studies: application to the tobacco litigation. Health Serv Outcomes Res Methodol. 2001;2(3–4):169–188. doi:10.1023/A:1020363010465
19. Rosenbaum PR. The central role of the propensity score in observational studies for causal effects. In: Rubin DB, editor. Matched Sampling for Causal Effects. Cambridge University Press: Cambridge; 2006:170–184.
20. Ali A, Husain A, Love TE, et al. Heart failure, chronic diuretic use, and increase in mortality and hospitalization: an observational study using propensity score methods. Eur Heart J. 2006;27(12):1431. doi:10.1093/eurheartj/ehi890
21. Normand SLT, Landrum MB, Guadagnoli E, et al. Validating recommendations for coronary angiography following acute myocardial infarction in the elderly: a matched analysis using propensity scores. J Clin Epidemiol. 2001;54(4):387–398. doi:10.1016/S0895-4356(00)00321-8
22. Li ZY, Shan F, Zhang L-H, et al. Complications after radical gastrectomy following FOLFOX7 neoadjuvant chemotherapy for gastric cancer. World J Surg Oncol. 2011;9:110. doi:10.1186/1477-7819-9-110
23. Nio Y, Kuroki M, Kuroki M, Badran A, Hachimine K, Kinugasa T. A randomized consent design trial of neoadjuvant chemotherapy with tegafur plus uracil (UFT) for gastric cancer–a single institute study. Anticancer Res. 2004;24(3b):1879–1887.
24. Ahn HS, Jeong S-H, Son YG, et al. Effect of neoadjuvant chemotherapy on postoperative morbidity and mortality in patients with locally advanced gastric cancer. Br J Surg. 2014;101(12):1560–1565. doi:10.1002/bjs.2014.101.issue-12
25. Fan CG, Li GL. [Effect of neoadjuvant chemotherapy on the postoperative pulmonary infection of patients with advanced gastric cancer]. Zhonghua Wei Chang Wai Ke Za Zhi. 2011;14(7):503–505.
26. Zhao Wen-He, Wang SF, Ding W, et al. Apoptosis induced by preoperative oral 5′-DFUR administration in gastric adenocarcinoma and its mechanism of action. World J Gastroenterol. 2006;12(9):1356–1361. doi:10.3748/wjg.v12.i9.1356
27. Tan BHL, Brammer K, Randhawa N, et al. Sarcopenia is associated with toxicity in patients undergoing neo-adjuvant chemotherapy for oesophago-gastric cancer. Eur J Surg Oncol. 2015;41(3):333–338. doi:10.1016/j.ejso.2014.11.040
28. Wagner, D., DeMarco MM, Amini N, Buttner S, Segev D, Gani F and Pawlik TM. Role of frailty and sarcopenia in predicting outcomes among patients undergoing gastrointestinal surgery. World J Gastrointest Surg. 2016;8(1):27–40. doi:10.4240/wjgs.v8.i1.27
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.