Back to Journals » Vascular Health and Risk Management » Volume 21
Postoperative Acute Refractory Hypoxemia After Acute Type A Aortic Dissection Surgery: Supporting the Two-Hit Mechanism of Transfusion-Related Acute Lung Injury. A Retrospective Cohort Study
Authors Afolabi MO ![]() , Li J, Wang J, Abass MAJ, Lin A, Debora A, Madzikatire TB, Wang J
, Li J, Wang J, Abass MAJ, Lin A, Debora A, Madzikatire TB, Wang J
Received 5 June 2025
Accepted for publication 6 September 2025
Published 16 September 2025 Volume 2025:21 Pages 797—811
DOI https://doi.org/10.2147/VHRM.S544999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Harry Struijker-Boudier
Mariam Omotolani Afolabi,1 Jiannan Li,1 Jian Wang,2 Mashud Akinfemi Junior Abass,2 AiLing Lin,1 Asta Debora,3 Tinotenda Blessing Madzikatire,4 Jue Wang1
1Department of Cardiac Surgery, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325035, People’s Republic of China; 2Department of Wound Healing, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China; 3Department of Radiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China; 4Department of Hepatobiliary Surgery, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China
Correspondence: Jue Wang, Email [email protected]
Background: Acute type A aortic dissection (ATAAD) surgery is often complicated by postoperative acute refractory hypoxemia (ARH). Multiple risk factors contribute to ARH, and perioperative blood transfusion is a potential risk factor. This study investigates the association between perioperative blood product transfusion and ARH in ATAAD surgical patients.
Methods: This retrospective cohort study included 282 patients who underwent surgical repair of ATAAD between 2015 and 2020. Perioperative blood product transfusion volumes, postoperative oxygenation indices, laboratory and radiological findings were analyzed. The primary outcome, ARH, was defined as moderate-to-severe hypoxemia (P/F ≤ 200 mmHg) within 72 hours postoperatively. Multivariate logistic regression was used to identify risk factors for ARH, confounders were adjusted for, and platelet transfusion association was further evaluated.
Results: Acute refractory hypoxemia occurred in 35.8% of the total patient cohort. At baseline, ARH patients had significantly higher BMI and a high prevalence of hypertension and coronary artery disease. Marfan syndrome was significantly more prevalent in the non-ARH group. Platelet transfusion was administered in 81.2% of patients, and a significantly higher frequency of ARH patients received platelet transfusion [p=0.013; Adjusted OR 95% CI; 3.43 (1.54– 7.63)]. A synergistic effect was observed between high preoperative C-reactive protein (CRP) and platelet transfusion in the resulting ARH [p < 0.001; adjusted OR 95% CI: 16.06 (3.02– 85.50)]. After multivariate logistic regression analysis, platelet transfusion, high CRP, brachiocephalic trunk involvement, and prolonged hypothermic circulatory arrest time were independent risk factors for postoperative ARH after ATAAD surgery. ARH patients required a significantly longer duration of mechanical ventilation.
Conclusion: Platelet transfusion was independently associated with risk of postoperative ARH, supporting a potential TRALI-like mechanism. Findings suggest that in high-risk ATAAD surgery, the synergistic effect of preoperative systemic inflammation and platelet transfusion may contribute to lung injury compatible with the “two-hit” model. This potential pathway requires further investigation.
Keywords: acute type A aortic dissection, ATAAD, postoperative hypoxemia, acute refractory hypoxemia, blood transfusion, platelet transfusion, TRALI, two-hit hypothesis
Graphical Abstract:

Introduction
Patients undergoing surgical repair of acute type A aortic dissection (ATAAD) are at an increased risk of postoperative hypoxemia, which is associated with high mortality rates and prolonged mechanical ventilation in the cardiac intensive care unit (CCU). Acute refractory hypoxemia is a severe form of respiratory failure characterized by persistently low arterial oxygen despite an increase in the fraction of inspired oxygen (P/F ratio ≤ 200 mmHg). Literature indicates a 45% prevalence of moderate to severe ARH due to acute respiratory distress syndrome (ARDS), along with a 48% mortality rate in the ICU.1
Perioperative High-volume transfusion is a recognized risk factor for postoperative hypoxemia in ATAAD surgery.2,3 While the effect of RBC transfusion on postoperative hypoxemia has been extensively reported in ATAAD surgery,4 platelet transfusion remains less well-defined. Perioperative Utilization of platelets in patients undergoing surgery with CPB is often influenced by the potential risk of bleeding due to platelet dysfunction, platelet consumption during CPB, and hemodilution-induced thrombocytopenia in cardiac surgery patients.5 Notably, since patients receiving blood transfusions are likely to receive a combination of other blood product components, completely isolating the effects of platelets in analysis is challenging.
A two-hit mechanism commonly explains the pathophysiology of transfusion-related pulmonary dysfunction; the first is pre-existing systemic inflammation, such as that induced by surgical trauma and aortic dissection itself, which primes the pulmonary endothelium for the second hit, occurring upon infusion of blood products containing donor antibodies, bioactive lipids, and platelet-derived inflammatory mediators that activate neutrophils and proinflammatory cytokines. Platelets are especially immunoreactive due to their inflammatory effector properties.6,7 Platelet transfusion introduces a combination of several pathways that result in neutrophil dominance; activated platelets induce the release of proinflammatory cytokines (TNF-α and TGF-β) and the formation of neutrophil extracellular traps (NETs). Ceramide accumulation in stored platelets modulates neutrophil apoptosis, leading to prolonged neutrophil activity. These trigger a cascade of fulminant neutrophil-mediated vascular endothelial damage, lung tissue injury, and pulmonary edema.
Kapur et al reported that CRP, a marker of systemic inflammation, and antibodies present in transfused blood products synergistically increase the accumulation of neutrophils and inflammatory cytokines (IL-2, MIP-2) in the lungs, resulting in acute lung injury characterized by noncardiogenic pulmonary edema.8
The objective of the current study was twofold; firstly, we aimed to identify the perioperative risk factors associated with postoperative ARH after surgical repair of ATAAD; second, we further investigated the relationship between platelet transfusion and ARH, including the analysis of a potential dose-dependent relationship. Given the observed association of platelet transfusion and postoperative ARH, we hypothesized that systemic inflammation related to the ATAAD disease process, and extensive surgery, interact with platelet transfusion, resulting in acute lung injury presenting as ARH, consistent with a TRALI-like “two-hit” mechanism.
What is Known
- Acute refractory hypoxemia (ARH) is a common complication following acute type A aortic dissection (ATAAD) surgery.
- Blood product transfusion is a recognized risk factor for Transfusion-related acute lung injury (TRALI) and adverse outcomes in cardiac surgery.
What this Study Adds
- This retrospective study identified an independent association between platelet transfusion and the development of ARH in patients who underwent ATAAD surgery.
- The platelet transfusion decisions were not based on preprocedural platelet levels but rather on intraoperative bleeding (measured by hemoglobin drop).
- The combined effect of systemic inflammation (measured by preprocedural CRP levels) and platelet transfusion was associated with increased risk of postoperative acute refractory hypoxemia, supporting the two-hit mechanism.
Methods
Flowchart of Study Design (Figure 1)
 |
Figure 1 Flowchart of study design. |
Study Design and Patients
We conducted a retrospective cohort study approved by the institutional review board on patients who underwent surgical repair of ATAAD at the First Affiliated Hospital of Wenzhou Medical University between January 2015 to December 2020. The study was conducted according to the ethical principles and clinical guidelines set out by the Declaration of Helsinki. Informed consent was waived due to the study design.
Our Inclusion criteria were as follows: (i) Patients with a confirmed diagnosis of ATAAD who underwent surgical repair, (ii) Patients with available ABG reports within 72 hours postoperatively (iii) Patients with complete perioperative data.
Patients were excluded if they had incomplete medical records, died intraoperatively or within 24 hours postoperatively, or had pre-existing pulmonary disease. To ensure that ARH cases reflect inflammatory lung injury rather than volume overload, we excluded TACO cases, defined as hypoxemia with high postoperative BNP (> 300 pg/mL) combined with the presence of pleural effusion or pulmonary edema on chest X-ray in transfused patients.9
Surgical Procedure
The surgical procedure in this cohort follows total aortic arch replacement with stent Graft using Sun’s procedure10 in 259 cases and hemiarch replacement with artificial graft in 9 cases. Proximal surgery was selected according to clinical judgement for each case. General anesthesia was initiated, and the patients were placed in a supine position with the shoulders back and elevated. A median sternotomy was performed, and the thoracic cavity was entered layer by layer. The right axillary artery (or femoral in some patients for easier access in emergent cases) was dissected and cannulated to establish cardiopulmonary bypass. The diameter of the ascending aorta and aortic arch was directly visualized and measured with calipers. The size and location of the tear and the presence of retrograde dissection were identified and noted. The aortic sinus and annulus diameter were measured, and based on previous echocardiography results, aortic and other valves were assessed for the presence of regurgitation. Involvement of aortic branches and extent of dissection was visualized and noted.
Cardiopulmonary bypass was initiated, and cooling was performed. The ascending aorta was cross-clamped and opened, and blood cardioplegia (4:1) was administered directly through the coronary ostia to induce cardiac arrest. This was supplemented with Retrograde perfusion via the coronary sinus, at the surgeon’s discretion. The ascending aorta was transected (above coronary ostia) and the proximal aortic sinus was repaired by approximating the inner and outer layers, and left and right non-coronary junctions were resuspended. The aortic sinus layers were then reinforced with interrupted sutures using a patch. Deep hypothermic circulatory arrest and selective cerebral perfusion was initiated, the aortic arch was opened, and a well-sized, case-specific intraoperative stent graft was placed in the descending thoracic aorta, with the distal end of the artificial graft first anastomosed to the descending aorta, and lower body perfusion was restored. The left common carotid artery, subclavian artery, and brachiocephalic artery were sequentially anastomosed. Finally, the aortic root was anastomosed to the artificial graft. The heart was de-aired, and the aortic cross clamp was released. Cardiac massage was performed for subsequent spontaneous cardiac recovery. The patients were rewarmed to a rectal temperature of 36 degrees C. Hemodynamic stability was achieved, and cardiopulmonary bypass was discontinued. Pericardial and mediastinal drainage tubes were placed. Hemostasis was ensured, and surgical instruments and sponges were counted and confirmed. The sternum was closed with steel wires, and the thoracic cavity was closed layer by layer.
Blood Transfusion and Laboratory Measurements
The decision to initiate blood product transfusion was made by the cardiac surgeon and anesthesiologist, in accordance with the 2021 STS/SCA/AmSECT/SABM clinical practice guideline on patient blood management. Indications for blood transfusion were guided by a series of ABGs measured throughout the procedure and included compromised oxygen delivery or hemoglobin levels falling below threshold (7.0g/dL), evidence of ongoing surgical blood loss, or hemodynamic instability. The difference between preoperative and immediate postoperative hemoglobin level was calculated, and the resulting hemoglobin drop (∆Hb) was used as a surrogate marker to quantify intraoperative blood loss. To account for intraoperative RBC transfusion, ∆Hb was corrected for, using the Landefeld equation, where 1 unit of packed RBC was assumed to increase Hb level by 1g/dL.11 Patients were further classified into minimal (<1g/dl), moderate (1-<2g/dl), significant (2.0-<3g/dL) and severe blood loss (≥3g/dL) to assess the potential association of blood loss in the decision to transfuse blood products and its association with ARH in our cohort.
Our hospital’s blood bank laboratory records platelet transfusions in pooled platelet units administered, rather than standardized apheresis units. Each pooled unit contains 0.45–0.85*1011 platelets while an apheresis unit contains 3*1011 platelets. Therefore, one apheresis unit equals approximately 4–6 pooled units.12 Hence, while the number of units may appear astonishingly elevated compared to studies that used apheresis-based data, the actual dose is equivalent therapeutically. This study analyzed platelet transfusion volume with the original pooled units data as recorded. Preoperative hematologic parameters were recorded and inflammatory markers including CRP, Fibrinogen, D-dimer were considered as baseline indicators of systemic inflammatory status.13
Data Collection
Diagnostic Data for Acute Type A Aortic dissection, demographics, intraoperative and postoperative components were independently extracted from the hospital’s electronic database, and imaging studies were obtained from the current picture archiving and communication system (PACS). The PaO2 and FiO2 levels in all available ABGs taken within 72 hours post-surgery were examined, and the lowest PF ratio was recorded for analysis. Patient demographic, clinical characteristics, laboratory markers, anatomical abnormalities, aortic branch involvement, and dissection tear location were obtained. Data was last updated on December 31, 2020. Informed consent was waived due to the retrospective nature of the study; however, patients’ identities were anonymized for confidentiality.
Study Outcomes and Objectives
The primary outcome of interest was postoperative acute refractory hypoxemia (ARH), defined as PF ratio ≤200mmHg (moderate to severe hypoxemia) within 72hours postoperatively, and perioperative blood product transfusion was the exposure of interest. Secondary outcomes were defined as postoperative need for ECMO, duration of ventilation, CCU and hospital stay, laboratory markers (troponin, CRP, BNP, lactate), neurological complications (postoperative paraplegia, transient and permanent neurological deficits), pleural effusion, radiographic findings (mild inflammatory infiltrates, unilateral or bilateral), and incidence of pneumonia post-surgery.
Statistical Analysis
Baseline characteristics between the two groups were summarized using descriptive statistics, the distribution of continuous variables was assessed for skewness, and based on the distribution, continuous variables with normal distribution were reported as mean ± Standard deviation and median and interquartile range (IQR) for skewed data. Categorical variables were expressed as frequencies (%). Univariate logistic regression was used to analyze the association of perioperative variables with the primary outcomes. Chi-square test was used for categorical variables, independent sample t-test and Mann–Whitney U-tests for continuous variables. ARH was further analyzed in relation to transfusion volumes of each blood product (RBC, Platelets, FFP, and Whole blood) and postoperative outcomes. Differences between patients with and without ARH, and between transfusion volume groups were analyzed. A multivariate Logistic regression analysis was conducted to adjust for potential confounders and identify the independent predictors of ARH. Statistically significant variables (p <0.05) from the univariate analysis were included in the multivariable analysis. Sequential multivariable models (models I–III) were constructed to evaluate the contribution of different variable clusters and adjust for potential confounding, including clinically relevant variables in the unadjusted, partially adjusted (models I–II), and the fully adjusted model (model III). Variables included in the model were age, gender, BMI, Hypertension, Diabetes Mellitus (model II), and Preoperative lactate, Preoperative D-dimer, aortic branches involvement, complex surgery, CPB time, MAP during CPB, RBC transfusion volume, plus variables in model II (model III). Model performance was assessed by evaluating discrimination, calibration, and stability. Discrimination was quantified using the area under the receiver operating characteristic curve (AUC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. To assess the risk of overfitting in the final multivariable model, we calculated the events per variable (EPV) ratio. Multicollinearity was evaluated using variance inflation factors (VIFs); a VIF value below 5 was considered indicative of no significant multicollinearity among the predictors. We reported the unadjusted OR and 95% CI in model I. Adjusted Odds ratios, 95% CI, and corresponding p-values were reported in the results. Statistical significance was defined as p < 0.05. All statistical analysis was performed using SPSS Statistics Version 29.0 and GraphPad Prism, Version 8.2.0 (GraphPad, Inc).
According to our analysis of the extent of missing data for all variables, we found that <20% of baseline variables had missing data with no clear pattern. Using SPSS Statistics Version 29.0, 20 imputed datasets were created, with predictive mean matching used for continuous variables and logistic regression for categorical variables. Multiple imputation was used because it is the most appropriate imputation model under the missing at random (MAR) assumption, as seen in our dataset, to minimize potential bias. However, data related to the primary endpoint (postoperative ABGs) and key exposure (transfusion history) were handled by complete case analysis to ensure diagnostic and exposure accuracy, detailed in the exclusion criteria and shown in Figure 1.
Results
Baseline and Intraoperative Characteristics
A total of 282 patients who underwent ATAAD surgery under cardiopulmonary bypass were included in this study. The patients were divided into two groups according to whether or not they developed the primary endpoint, postoperative ARH. At baseline, a significantly higher BMI was observed in ARH patients (p <0.001). ARH patients had a high prevalence of comorbidities, including hypertension (p<0.001) and coronary artery disease (p =0.022) at baseline. A higher prevalence of Marfan syndrome was observed in the non-ARH group (p =0.004). There was no statistically significant difference in age between the two groups. Preoperative CRP and troponin levels were significantly higher in the ARH group (p=0.001 and p=0.008, respectively). No statistically significant differences were observed in preoperative hemoglobin, platelet, and coagulation profiles. Only 6 patients received Ulinastatin for its anti-inflammatory effect, and the difference observed in the two groups was not significant (Table 1).
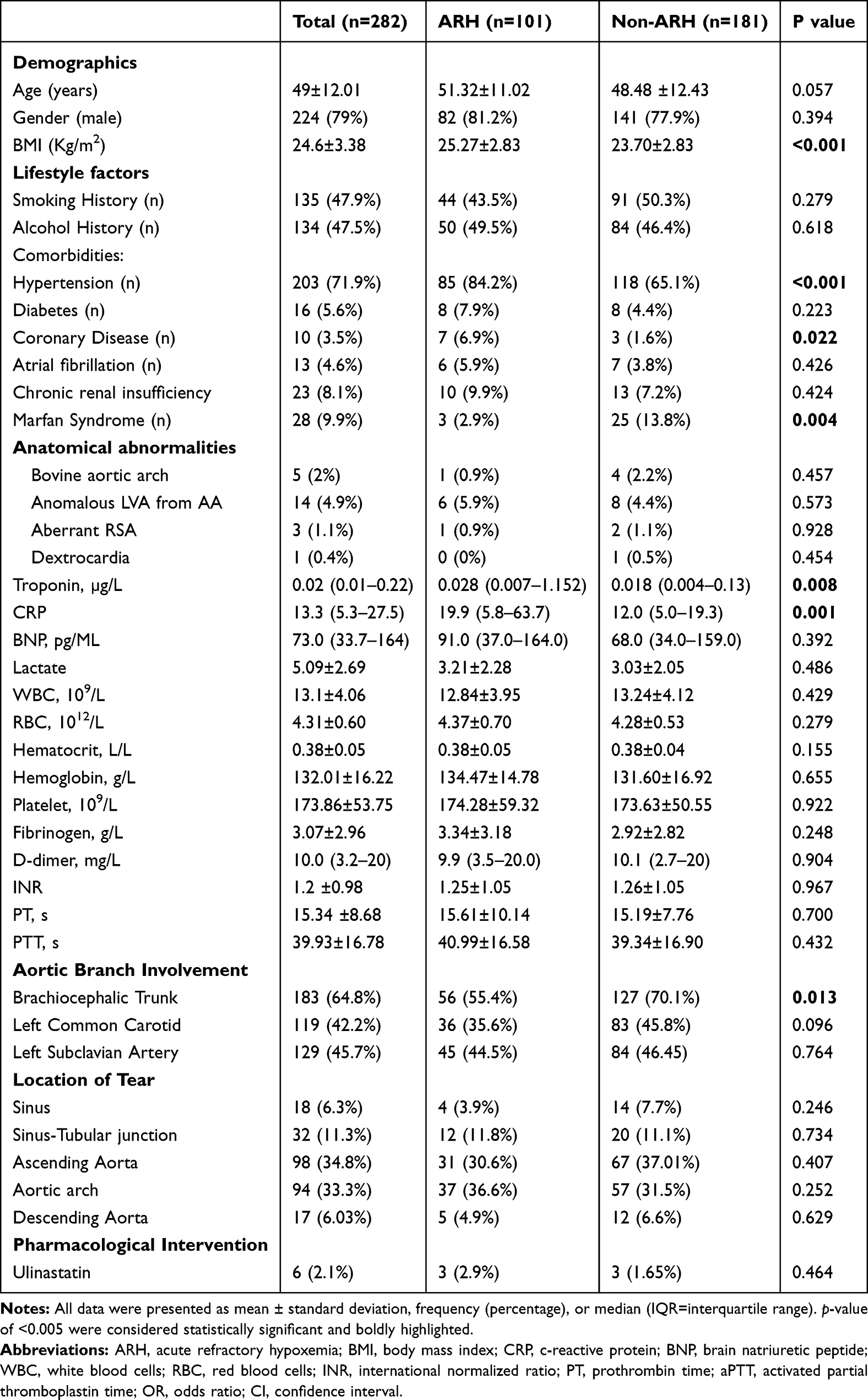 |
Table 1 Baseline Characteristics Comparison Between ARH and Non-ARH |
We observed a higher incidence of ARH in patients who underwent Bentall and ascending proximal surgical procedures (p<0.001). A higher hypothermic circulatory arrest time was observed in the ARH group (p=0.011). ARH patients received higher units of platelet transfusion on average (p=0.013) (Table 2). No significant association was observed between ARH and RBC, FFP, and whole blood transfusion in this cohort (Figure 2).
 |
Figure 2 Comparison of Blood product transfusion between ARH and non-ARH patients. Only platelet transfusion was statistically significant. Patients who developed ARH received higher volumes of platelet transfusion than the non-ARH group. No significant difference was observed with RBC, FFP, and whole blood transfusion. |
 |
Table 2 Intraoperative Variables |
Blood Product Transfusion, Systemic Inflammation, and Platelet Transfusion Volume Association
In the overall cohort, 229 (81.2%) patients received platelet transfusions. Patients with severe blood loss (∆Hb ≥3) were more likely to receive RBC transfusion (p=0.022), higher frequencies of platelet and FFP transfusions were observed in patients with severe blood loss, and whole blood was less frequently transfused in the overall patient cohort (Table 3). Platelet transfusion was strongly associated with a high frequency of ARH in patients who had high preprocedural CRP levels (≥50mg/L) compared to patients who did not receive platelet transfusion (p<0.001, Adjusted OR: 16.07, 95% CI: 3.02–85.50) (Table 4). No significant association was observed between preoperative low platelet count and platelet transfusion (Table 5). ARH was significantly associated with medium and high-volume platelet transfusion [p=0.023 and p=0.006, respectively] (Table 6).
 |
Table 3 Frequency of Blood Product Transfusion Based on the Severity of Blood Loss in Patients Who Underwent ATAAD Surgery |
 |
Table 4 Exploratory Subgroup Analysis of the Combined Effect of Preprocedural CRP Levels and Platelet Transfusion on Risk of Postoperative ARH After ATAAD Surgery |
 |
Table 5 Exploratory Subgroup Analysis of Platelet Transfusion in Association with Baseline Platelet Levels and Intraoperative Blood Loss |
 |
Table 6 Exploratory Subgroup Analysis of Blood Loss and Dose-Dependent Association of Platelet Transfusion with ARH in ATAAD Patients |
Outcomes
There was no significant difference in 30-day mortality between the two groups. ARH patients required a longer duration of mechanical ventilation postoperatively (p=0.008) and higher levels of CRP (p=0.005). Post-operative outcomes are presented in Table 7 and Figure 3.
 |
Figure 3 Incidence of postoperative complications in Acute Refractory hypoxemia (ARH) and Non-ARH group; TND (Transient Neurological Deficits include confusion, seizure, agitation, and delirium), PND (Permanent Neurological Dysfunction includes Stroke and COMA confirmed via CT / MRI), MII (mild inflammatory infiltrates on postoperative chest-X-ray). |
 |
Table 7 ARH and Postoperative Outcomes |
Predictors of Postoperative ARH After ATAAD Surgery
In the multivariate regression analysis, preoperative CRP [p<0.001; OR 95% CI: 1.022 (1.011–1.033)], platelet transfusion [p=0.030; OR 95% CI: 1.024 (1.002–1.046)], brachiocephalic trunk involvement [p=0.010; OR 95% CI: 0.426 (0.257–0.830)], and hypothermic circulatory arrest time [p=0.019 OR 95% CI: 1.045 (1.007–1.085)] were identified as the independent risk factors of ARH after adjusting for potential confounders (Table 8). The final adjusted model contained 19 predictor variables for 101 outcome events, yielding an events per variable (EPV) ratio of 5.32, which meets the minimum acceptable threshold of 5. Although below the ideal threshold of 10, it is supported by the model’s strong overall performance. The prediction model demonstrated good discriminatory ability for predicting ARH with an AUC of 0.80 (95% CI: 0.75–0.85; p<0.001). Calibration of the final regression model was satisfactory between predicted probabilities and observed outcomes as indicated by the Hosmer-Lemeshow goodness-of-fit test (χ² = 8.696, df = 8, p = 0.37). Multicollinearity, assessed by variance inflation factors (VIFs) among the final multivariate model, indicates no significant multicollinearity among the predictors (mean VIF = 1.5; range 1.07–2.81).
 |
Table 8 Multivariate Analysis of Independent Risk Factors for Acute Refractory Hypoxemia (ARH) in Patients Who Underwent Surgical Repair of ATAAD |
Discussion
ARH following ATAAD surgery is a common complication in the cardiac ICU. Recent studies identified high BMI, preoperative hypoxemia, WBC count, CPB time, deep hypothermic circulatory arrest time, preoperative and intraoperative inflammatory response, time from symptom onset to surgery ≤72h, preoperative renal insufficiency, and high volume of blood transfusion as independent risk factors for postoperative hypoxemia.14–17 In our study, we examined the risk factors for postoperative ARH and further expanded our findings to identify that platelet transfusion, among other blood products in combination with systemic inflammation, was significantly associated with ARH.
Due to the likelihood of significant hemorrhage in ATAAD surgery, substantial volumes of transfusion are often required. Complications associated with blood transfusion in cardiac surgery include postoperative hypoxemia, prolonged mechanical ventilation, acute lung injury, pneumonia, increased mortality, and, most frequently, acute kidney injury (AKI).18–20 Our study is the first to analyze the specific association of platelet transfusion and postoperative ARH. High volumes of blood transfusion are reported to be significantly related to the risk of hypoxemia after ATAAD surgery; however, transfusion was comprehensively analyzed, without isolating blood product components.3,16 In our study, we observed transfusion of >20 units (>3.3 to 5 apheresis units) of platelets to be independently associated with the risk of ARH.
In the present study, we defined ARH as PF ratio ≤200mmHg, based on the oxygen index component of the Berlin criteria for ARDS diagnosis, however we did not require the radiological presence of bilateral infiltrates or specific exclusion of cardiogenic pulmonary edema in our diagnostic criteria because patients undergoing aortic surgery may have overlapping presentations on chest imaging, and the presence of preexisting comorbidities make it challenging too differentiate the origin of pulmonary edema.21 Therefore, we aimed to primarily identify clinically relevant hypoxemia, regardless of ARDS status and only 8 patients met the full modified Belin’s diagnostic criteria for ARDS in our cohort.2,22
Independent risk factors for postoperative ARH in our study include high preoperative CRP, high volume transfusion, brachiocephalic trunk involvement in the dissection and hypothermic circulatory arrest time. The findings of this study indicate that ARH outcome may be improved by a more careful use of platelet transfusion. As mentioned, higher volumes of platelet transfusion had a strong independent association with postoperative ARH, especially with inflammation. In a recent study on risk factors for acute respiratory dysfunction (ARD) following ATAAD surgery, they did not find a significant association between blood product transfusion and postoperative hypoxemia.15 This might be explained by their specific exclusion of patients who received massive volumes of transfusion, potentially omitting patients at high risk of TRALI. In our study, we included high volume transfusion cases, but to reflect the inflammatory pathophysiology of TRALI, we excluded possible cases of TACO defined as hypoxemia in combination with the presence of pulmonary edema or pleural effusion on chest imaging and high BNP level >300pg/mL.9,23 Notably, we also found that preoperative inflammatory markers like CRP had a strong association with postoperative ARH, suggesting that preoperative CRP could serve as a biomarker for identifying patients at high risk for postoperative ARH.
In our study, the TRALI-like mechanism reflects a mechanistic hypothesis rather than a clinical diagnosis. We suggest that the occurrence of ARH is related to the contribution of platelet transfusion to lung injury through a similar immunoinflammatory pathway seen in TRALI. TRALI is defined as the acute onset of hypoxemia (P/F ≤ 300 mmHg or SpO2 < 90% on room air) occurring within 6 hours of transfusion.24 Multiple studies have identified platelets as a trigger for TRALI development. The significant role of platelets in amplifying inflammatory lung injury under primed conditions (first hit) has been extensively defined.25,26 In our study, we found that patients with elevated preoperative CRP who also received platelet transfusions had significantly higher rates of postoperative ARH, supporting the two-hit model of lung injury. Systemic inflammatory response marked by high CRP levels, among other inflammatory markers, including interleukin 6 (IL-6), and D-dimer, is a recognized risk factor in the pathogenesis of hypoxemia in ATAAD.13 Similarly, in our study, we found that preoperative CRP was significantly elevated in the ARH group, and this association remained significant after multivariate logistic regression analysis. (p<0.001). The two-hit model of TRALI is characterized by pre-existing inflammation and transfusion synergistically resulting in acute lung injury. Bioactive lipids and immune mediators in transfused platelets contribute to antibody-mediated neutrophil and complement activation, followed by the release of inflammatory cytokines, and subsequent pulmonary endothelial damage and hypoxemia. While the two-hit model served as a conceptual framework to explain the pathogenesis of acute lung injury, in the context of postoperative ARH, this model, as suggested by Middelburg and van der Bloom, may lead to under-identification of other modifiable risk factors, because TRALI pathogenesis is “multicausal”.27 Based on the several potential limitations of our study, we cannot infer direct causality between ARH and platelet transfusion. Firstly, utilization of platelet transfusion did not specifically follow any pre-established institutional protocols or guidelines, except for the generalized blood transfusion protocol, and possible confounders may have been missed. Secondly, our study is a single-center retrospective observational study with a relatively smaller sample size, particularly the low number of patients with ARH (n=101), which resulted in a moderate events per variable (EPV) ratio of 5.3 (below the conservative threshold of 10); however, the model’s overall discriminatory power and calibration suggest that the findings are robust. Future studies with larger cohorts are needed to validate these results. Thirdly, our ARH definition was based on the P/F ratio, which was informed by previous validated studies is a reliable but solitary metric, we did not apply full Berlin criteria, which include radiographic confirmation and timing. Lastly, the exact timing of the hypoxemia after transfusion was not accounted for. We propose that future studies can confirm the TRALI mechanism with a 6-hour cutoff duration for diagnosis, and prospective randomization using a platelet transfusion guideline can provide more insight.
Conclusion
In patients undergoing ATAAD surgery, ARH is a significant complication with a strong association with platelet transfusion, increased preoperative CRP levels, and hypothermic circulatory arrest time. Patients who developed postoperative ARH required a longer duration of mechanical ventilation and had more postoperative complications.
Ethics Approval
According to the Regulations and Rules of “Ethical Reviews for Biomedical Research Involving Human Subjects” (2023) the National Health Commission of PRC (People’s republic of China), “Declaration of Helsinki” of WMA, and “International Ethical Guidelines for Human Biomedical Research” of CIOMS, this project was approved by Ethics committee in clinical research (ECCR) of the First Affiliated Hospital of Wenzhou Medical University. Due to the retrospective nature of the study, informed consent was waived by the ECCR. All Patient data were anonymized to ensure privacy and confidentiality.
Acknowledgments
Graphical Abstract. Platelet transfusion may contribute to acute lung injury in postoperative ATAAD patients. 101 (35.8%) of patients developed postoperative ARH. First hit: systemic inflammation, second hit was platelet transfusion. Created in BioRender. Afolabi, M. (2025) https://BioRender.com/ scbwhcu.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 2021 New Medical Talent in Zhejiang Province (HCZP[2021]No.40) and the Wenzhou Science and Technology Bureau Self-funded Projects (2021Y1307).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Huang X, Zhang R, Fan G, et al. Incidence and outcomes of acute respiratory distress syndrome in intensive care units of mainland China: a multicentre prospective longitudinal study. Crit Care. 2020;24(1):515. doi:10.1186/s13054-020-03112-0
2. Wang Y, Xue S, Zhu H. Risk factors for postoperative hypoxemia in patients undergoing Stanford A aortic dissection surgery. J Cardiothorac Surg. 2013;8:1–7. doi:10.1186/1749-8090-8-118
3. Sheng W, Yang H-Q, Chi Y-F, et al. Independent risk factors for hypoxemia after surgery for acute aortic dissection. Saudi Med J. 2015;36(8):940. doi:10.15537/smj.2015.8.11583
4. Zhou R, Qian D, Li H, et al. Clinical presentation and in-hospital outcomes of intraoperative red blood cell transfusion in non-anemic patients undergoing elective valve replacement. Front cardiovasc med. 2022;9:1053209. doi:10.3389/fcvm.2022.1053209
5. Bilgin YM, van de Watering LMG, Versteegh MIM, et al. Postoperative complications associated with transfusion of platelets and plasma in cardiac surgery. Transfusion. 2011;51(12):2603–2610. doi:10.1111/j.1537-2995.2011.03200.x
6. Middleton EA, Weyrich AS, Zimmerman GA. Platelets in pulmonary immune responses and inflammatory lung diseases. Physiol Rev. 2016;96(4):1211–1259. doi:10.1152/physrev.00038.2015
7. Tariket S, Sut C, Hamzeh-Cognasse H, et al. Transfusion-related acute lung injury: transfusion, platelets and biological response modifiers. Exp Rev Hematol. 2016;9(5):497–508. doi:10.1586/17474086.2016.1152177
8. Kapur R, Kim M, Rondina MT, et al. Elevation of C-reactive protein levels in patients with transfusion-related acute lung injury. Oncotarget. 2016;7(47):78048–78054. doi:10.18632/oncotarget.12872
9. Zhou L, Giacherio D, Cooling L, et al. Use of B‐natriuretic peptide as a diagnostic marker in the differential diagnosis of transfusion‐associated circulatory overload. Transfusion. 2005;45(7):1056–1063. doi:10.1111/j.1537-2995.2005.04326.x
10. Sun LZ, Ma W-G, Zhu J-M, et al. Sun’s procedure for chronic type A aortic dissection: total arch replacement using a tetrafurcate graft with stented elephant trunk implantation. Ann Cardiothorac Surg. 2013;2(5):665–666. doi:10.3978/j.issn.2225-319X.2013.09.20
11. Nuis R-J, Rodés-Cabau J, Sinning JM, et al. Blood transfusion and the risk of acute kidney injury after transcatheter aortic valve implantation. Circulation. 2012;5(5):680–688. doi:10.1161/CIRCINTERVENTIONS.112.971291
12. Liumbruno G, Bennardello F, Lattanzio A, et al. Recommendations for the transfusion of plasma and platelets. Blood Transfus. 2009;7(2):132. doi:10.2450/2009.0005-09
13. Duan XZ, Xu Z-Y, Lu F-L, et al. Inflammation is related to preoperative hypoxemia in patients with acute Stanford type A aortic dissection. J Thorac Dis. 2018;10(3):1628–1634. doi:10.21037/jtd.2018.03.48
14. Liu N, Zhang W, Ma W, et al. Risk factors for hypoxemia following surgical repair of acute type A aortic dissection. Interact Cardiovasc Thorac Surg. 2016;24(2):251–256. doi:10.1093/icvts/ivw272
15. Möller CM, Ellmauer -P-P, Zeman F, et al. Postoperative acute respiratory dysfunction and the influence of antibiotics after acute type A aortic dissection surgery: a retrospective analysis. PLoS One. 2021;16(2):e0246724. doi:10.1371/journal.pone.0246724
16. Wang Y, Xue S, Zhu H. Risk factors for postoperative hypoxemia in patients undergoing Stanford A aortic dissection surgery. J Cardiothorac Surg. 2013;8:118. doi:10.1186/1749-8090-8-118
17. Yu W, Liang Y, Gao J, et al. Study on risk factors and treatment strategies of hypoxemia after acute type a aortic dissection surgery. J Cardiothorac Surg. 2024;19(1):273. doi:10.1186/s13019-024-02775-y
18. Xie Q, Li C, Zhong Y, et al. Blood transfusion predicts prolonged mechanical ventilation in acute Stanford type A aortic dissection undergoing total aortic arch replacement. Front cardiovasc med. 2022;9:832396. doi:10.3389/fcvm.2022.832396
19. Sheng W, Xia W, Niu Z, et al. Incidence of acute kidney injury and risk factors of prognosis in patients with acute Stanford type A aortic dissection. Ann Thoracic Cardio Surg. 2023;29(5):249–255. doi:10.5761/atcs.oa.22-00242
20. Lin C-Y, Wu M-Y, Tseng C-N, et al. Delayed sternal closure for intractable bleeding after acute type A aortic dissection repair: outcomes and risk factors analyses. J Cardiothorac Surg. 2022;17(1):184. doi:10.1186/s13019-022-01946-z
21. Sanfilippo F, Palumbo GJ, Bignami E, et al. Acute respiratory distress syndrome in the perioperative period of cardiac surgery: predictors, diagnosis, prognosis, management options, and future directions. J Cardiothorac Vasc Anesth. 2022;36(4):1169–1179. doi:10.1053/j.jvca.2021.04.024
22. Song X-C, Nie S, Xiao J-L, et al. Risk factors and long-term prognosis for postoperative hypoxemia in patients with acute type A aortic dissection: a retrospective observational study. Medicine. 2022;101(50):e32337. doi:10.1097/MD.0000000000032337
23. Klanderman RB, Bosboom JJ, Migdady Y, et al. Transfusion-associated circulatory overload-a systematic review of diagnostic biomarkers. Transfusion. 2019;59(2):795–805. doi:10.1111/trf.15068
24. Vlaar APJ, Toy P, Fung M, et al. A consensus redefinition of transfusion-related acute lung injury. Transfusion. 2019;59(7):2465–2476. doi:10.1111/trf.15311
25. Zeeuw van der Laan EAN, van der Velden S, Porcelijn L, et al. Evaluation of platelet responses in Transfusion-Related Acute Lung Injury (TRALI). Transfus Med Rev. 2020;34(4):227–233. doi:10.1016/j.tmrv.2020.08.002
26. McVey MJ, Kim M, Tabuchi A, et al. Acid sphingomyelinase mediates murine acute lung injury following transfusion of aged platelets. Am J Physiol Lung Cell Mol Physiol. 2017;312(5):L625–L637. doi:10.1152/ajplung.00317.2016
27. Middelburg RA, van der Bom JG. Transfusion‐related acute lung injury not a two‐hit, but a multicausal model. Transfusion. 2015;55(5):953–960. doi:10.1111/trf.12966
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.