Back to Journals » Clinical Ophthalmology » Volume 16
Postnatal Growth Trajectories and Neurodevelopmental Outcomes Following Bevacizumab Treatment for Retinopathy of Prematurity
Authors Zhang DL ![]() , Yoon HH, deRegnier RAO, Arzu J, Rahmani S
, Yoon HH, deRegnier RAO, Arzu J, Rahmani S
Received 15 June 2022
Accepted for publication 4 August 2022
Published 20 August 2022 Volume 2022:16 Pages 2713—2722
DOI https://doi.org/10.2147/OPTH.S378520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
David L Zhang,1 Hawke H Yoon,1,2 Raye-Ann O deRegnier,3 Jennifer Arzu,4 Safa Rahmani1,2
1Department of Ophthalmology, Northwestern University Feinberg School of Medicine, Chicago, IL, USA; 2Division of Ophthalmology, Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL, USA; 3Division of Neonatology, Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL, USA; 4Division of Preventive Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL, USA
Correspondence: Safa Rahmani, Division of Ophthalmology, Ann & Robert H. Lurie Children’s Hospital of Chicago, 225 E. Chicago Ave, Chicago, IL, 60611, USA, Tel +1 312 227-6180, Fax +1 312 227-9411, Email [email protected]
Purpose: To investigate the postnatal growth and neurodevelopment of infants with retinopathy of prematurity (ROP) treated with intravitreal bevacizumab (IVB).
Patients and Methods: This was a retrospective comparative study. A total of 262 infants were divided among three study groups: 22 treated with intravitreal bevacizumab, 55 treated with laser, and 185 with ROP that resolved without treatment. Infants with nonviable course or hydrocephalus, a source of non-physiologic weight gain, were excluded. Neurodevelopment was assessed with Bayley III scores at 17– 28 months if available and presence of hearing loss or cerebral palsy. Weekly weight, height, and head circumference from birth through 50 weeks postmenstrual age (PMA) were modeled to determine differences in growth trajectories following treatment.
Results: Comparison of postnatal growth curves from the time of treatment to 50 weeks PMA showed no significant differences in growth trajectories between groups after adjusting for the corresponding growth parameters at birth. Comparison of Bayley scores in patients with available data (n = 120) showed no significant differences. There was an increased risk of cerebral palsy in the IVB group after logistic regression adjusting for baseline confounders, but this did not retain statistical significance after applying the false discovery rate correction for multiple testing.
Conclusion: To our knowledge, this is the first large retrospective study to examine longitudinal growth in infants treated with IVB compared to controls. There were no significant differences in postnatal growth or neurodevelopmental outcomes between groups, which overall continue to support the safety of bevacizumab treatment for ROP.
Keywords: pediatric retina, ROP, laser, bevacizumab, neurodevelopment, growth
Introduction
Retinopathy of prematurity (ROP) is a leading cause of childhood blindness characterized by neovascularization of the immature retina that can progressively lead to retinal detachment. The pathogenesis of ROP is thought to involve two phases, a hyperoxic phase followed by a hypoxic phase.1 In phase one, excess oxygen exposure due to the extrauterine environment or supplemental oxygen causes downregulation of growth factors and termination of retinal blood vessel growth. During this phase, vascular endothelial growth factor (VEGF), an essential factor in angiogenesis, is suppressed. In phase two, increasing metabolic demands of the maturing retina cause hypoxic ischemia, upregulated VEGF, and subsequent vasoproliferation.
The current most widely accepted treatment for ROP is peripheral laser ablation, which has shown to improve visual, structural, and refractive outcomes.2 However, laser photocoagulation is destructive to the retina, and more recent studies on the use of anti-VEGF agents have shown that intravitreal bevacizumab (IVB) monotherapy is an effective treatment for ROP.3 The use of IVB as a primary treatment has quickly gained popularity because it does not require general anesthesia, is more easily tolerated by sicker babies, and allows further development of peripheral retinal vessels before possible laser treatment is needed.
However, due to the anti-angiogenic effects of anti-VEGF agents, concern has risen regarding the systemic effects of IVB injection in premature infants.4 The presence of bevacizumab in the systemic circulation after intravitreal injection has been observed for as long as 8 weeks after injection, while serum levels of VEGF were suppressed for the same duration.5
Systemic VEGF plays a key role in organogenesis and neural tube development6,7 and may have a neuroprotective effect during periods of hypoxic cerebral injury, the most common known cause of cerebral palsy.8 VEGF-mediated angiogenesis has also been shown to affect adipose tissue growth and function, contributing to weight gain and insulin resistance.9 Furthermore, the interplay between VEGF and IGF-1 has prompted interest in postnatal growth rate as a prognostic factor in developing ROP.10–13 The potential consequences of anti-VEGF therapy on these physiological processes are not completely understood. The goal of this study is to investigate the postnatal growth and neurodevelopment of preterm infants treated with IVB for ROP.
Patients and Methods
Subjects and Grouping
This study was approved by the institutional review boards of Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University in Chicago, Illinois. All procedures adhered to the tenets of the Declaration of Helsinki.
All the patients screened for ROP at Ann & Robert H. Lurie Children’s Hospital of Chicago and Prentice Women’s Hospital from 2008 to 2019 were identified. Inclusion criteria included infants with ROP that resolved without treatment (group 0), infants with ROP treated with laser photocoagulation (group 1), and infants with ROP treated with initial bevacizumab monotherapy (group 2). Indications for treatment were type I ROP as defined by the Early Treatment for Retinopathy of Prematurity study.2 Infants with nonviable course, infants who were transferred or lost to follow up before growth and neurodevelopment could be measured, and infants with hydrocephalus, which is a source of non-physiologic weight gain, were excluded. Baseline characteristics, hospital course, and systemic comorbidities were recorded and compared between groups.
Neurodevelopmental Outcomes Assessment
In patients with sufficient follow-up and available data, the Bayley Scales of Infant and Toddler Development-III scores at 17–28 months of age were used as a representation of neurodevelopmental outcomes. Poor neurodevelopmental outcomes were defined as Bayley III composite scores <85 in cognitive, language, or motor domains. Severe neurodevelopmental impairment was defined as a Bayley III composite score <70 in any domain. The presence or absence of hearing loss or cerebral palsy at the latest follow-up was also recorded and compared between groups as a separate proxy for neurodevelopmental outcomes.
Growth Outcomes Assessment
Weekly weight, height, and head circumference measurements from birth through 50 weeks postmenstrual age (PMA) were recorded, statistically modeled, and compared between groups to examine changes in growth trajectory over time. The mean weight, height, and head circumferences of each treatment group were also plotted against a standard, the Fenton preterm growth chart, to qualitatively examine growth trends over time by gender.
Statistical Analysis
Statistical analysis was performed using R software version 4.1.0 within RStudio version 1.4.1717 (R Core Team, Vienna, Austria). P-values were adjusted using the Benjamini–Hochberg procedure to control the false discovery rate (adjusted q < 0.05 for statistical significance) for the neurodevelopmental outcome assessment.
Demographic characteristics, baseline clinical data, and neurodevelopmental outcomes were expressed as frequency and percentage for categorical variables, and median and interquartile ranges (IQR) for continuous variables due to skewed distributions. Statistical significance (unadjusted p < 0.05) and clinical importance were used to identify clinical characteristics as potential confounders. Differences across treatment types were assessed using Pearson’s chi-squared or Fisher’s exact test for categorical variables such as hearing loss, and Kruskal–Wallis test for continuous measures including Bayley scores. We used logistic regression to examine differences in cerebral palsy outcome by treatment type, adjusting for birth weight, gestational age, presence of intraventricular hemorrhage (IVH), and Apgar score at 5 minutes.
Mixed-effects modeling was used to examine changes in weight, height, and head circumference beginning from the earliest time of treatment. To model the non-linear relationship of time with height and head circumference, we introduced a quadratic term for time. The models of weight, height, and head circumference included a time-by-treatment-type interaction to assess differences in the changes in growth measures over time across treatment groups. The models were adjusted for initial birth weight, height, and head circumference, respectively.
Results
Patient Characteristics
A total of 262 patients (144 males and 118 females) were included in the final analysis. A flowchart showing inclusion and exclusion of patients is shown in Figure 1. Among these patients, 185 had ROP that resolved without treatment (Group 0), 55 had ROP treated with laser (Group 1), and 22 had ROP treated with bevacizumab (Group 2). Median PMA at treatment was 36.3 weeks in the bevacizumab group (IQR 35.3–38.1) and 38.3 weeks in the laser group (IQR 35.1–41.6); there was no statistically significant difference in the time of treatment using the Mann–Whitney U-test (p = 0.06).
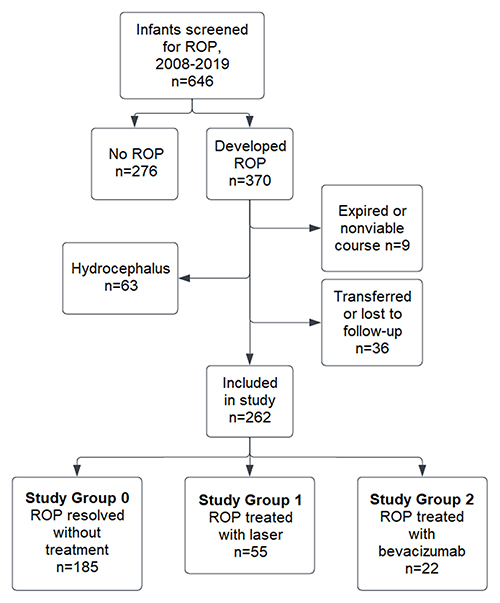 |
Figure 1 Flowchart showing inclusion and exclusion of patients during the study period. |
Table 1 shows the demographics and baseline comorbidities of each group. The IVB group had younger median gestational age (24.9 weeks, IQR 24.0–25.9) than the laser group (25.1 weeks, IQR 24.5–25.3) and untreated group (26.1 weeks, IQR 25.3–28.0). The IVB group also had lower birth weight (672.5 g, IQR 547.5–771.2) compared to the laser group (740.0 g, IQR 642.5–825.0) and untreated group (870.0 g, IQR 720.0–1080.0). Additionally, postnatal steroid use was higher in the IVB group (16/22, 73%) compared to laser (31/55, 56%) and untreated (86/185, 46%) groups. Finally, Apgar score at 5 minutes was found to be different between groups, with a median score of 6 in the IVB group (IQR 4–7), 6 in the laser group (IQR 5–8), and 7 in the untreated group (IQR 5.5–8).
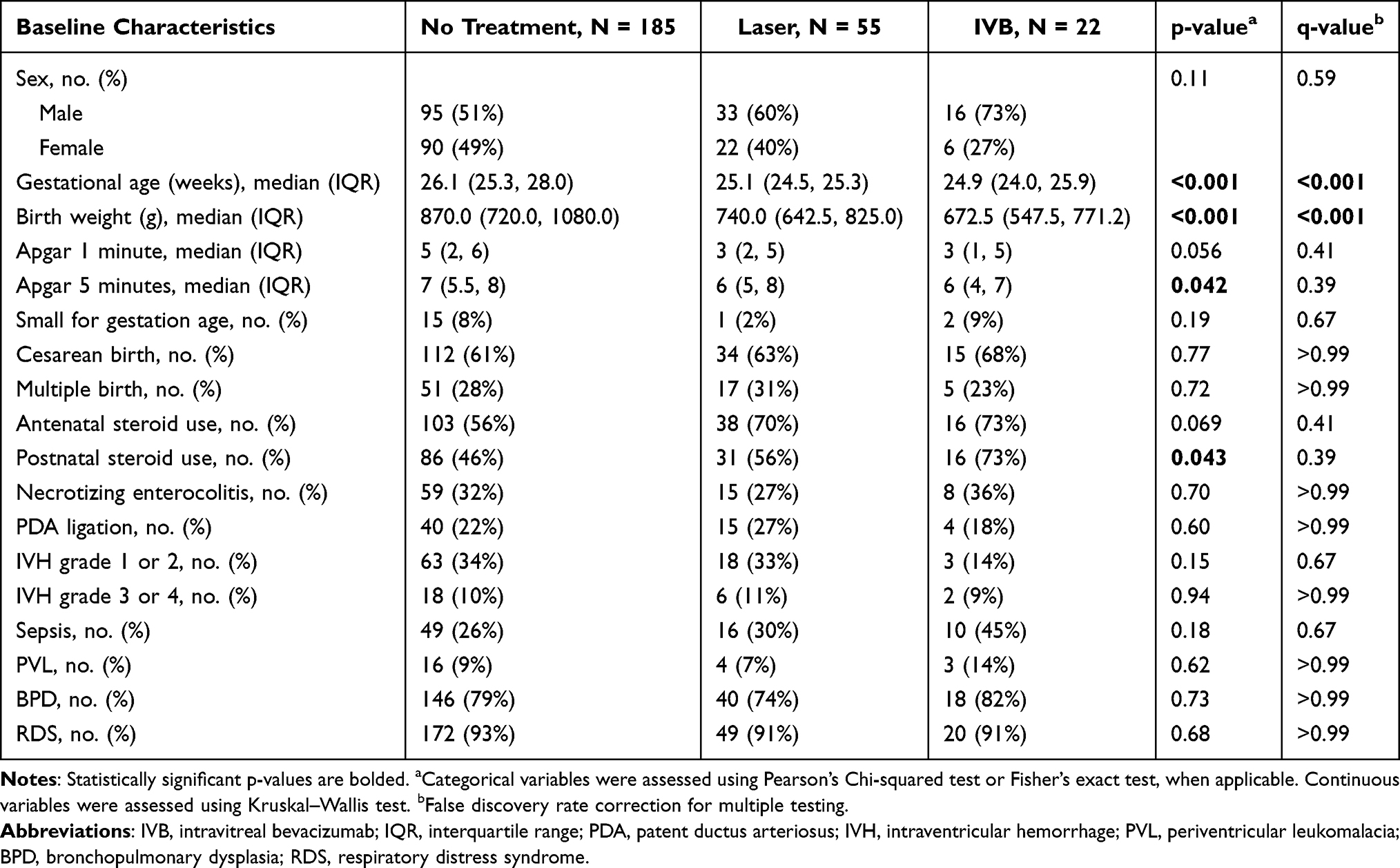 |
Table 1 Baseline Demographics and Systemic Risk Factors of All Included Study Participants |
Neurodevelopmental Outcomes
A total of 120 patients had available Bayley scores in the 17–28-month range: 12 treated with IVB, 31 treated with laser, and 77 without treatment. Baseline characteristics of this subset of patients are described in Table 2. Comparison of the Bayley III composite scores (Table 3) using the Kruskal–Wallis test with false discovery rate correction showed no significant differences in cognitive, language, or motor domains (q-value >0.99). Similarly, the frequency of poor neurodevelopmental outcomes, defined as a Bayley III score <85, was not significantly different across the groups in cognitive, language, or motor domains (q > 0.99). Finally, there were no differences in severe neurodevelopmental impairment, defined as any Bayley III score <70 (q >0.99).
 |
Table 2 Baseline Demographics and Systemic Risk Factors for Participants with Bayley Scores |
 |
Table 3 Comparison of Neurodevelopmental Outcomes Across Treatment Type Based on Bayley III Scores Collected at 17–28 Months |
The presence of hearing loss and cerebral palsy were also compared between groups (Table 4). There was no significant difference in the presence of hearing loss between groups (q > 0.99). Notably, the presence of cerebral palsy was significantly higher in the group treated with IVB (unadjusted p = 0.015); this statistical significance was retained after logistic regression adjusting for BW, GA, IVH, postnatal steroid use, and Apgar score at 5 minutes (OR 3.67, 95% CI 1.01–12.9, p = 0.043). However, after applying the false discovery rate correction for multiple testing, this finding failed to achieve significance (q > 0.99).
 |
Table 4 Association of Other Neurodevelopmental Measures with Treatment Status |
Postnatal Growth Outcomes
Figure 2 shows comparisons of weight, height, and head circumference trajectories following treatment with laser or bevacizumab. Individual growth measurements each week from birth through 50 weeks PMA were graphed on a scatter plot and converted into prediction lines using mixed-effects models. The time period of interest began from the earliest age at bevacizumab or laser treatment, which was 32 weeks PMA. Comparison of growth rates prior to treatment showed no significant differences in weight, height, and head circumference.
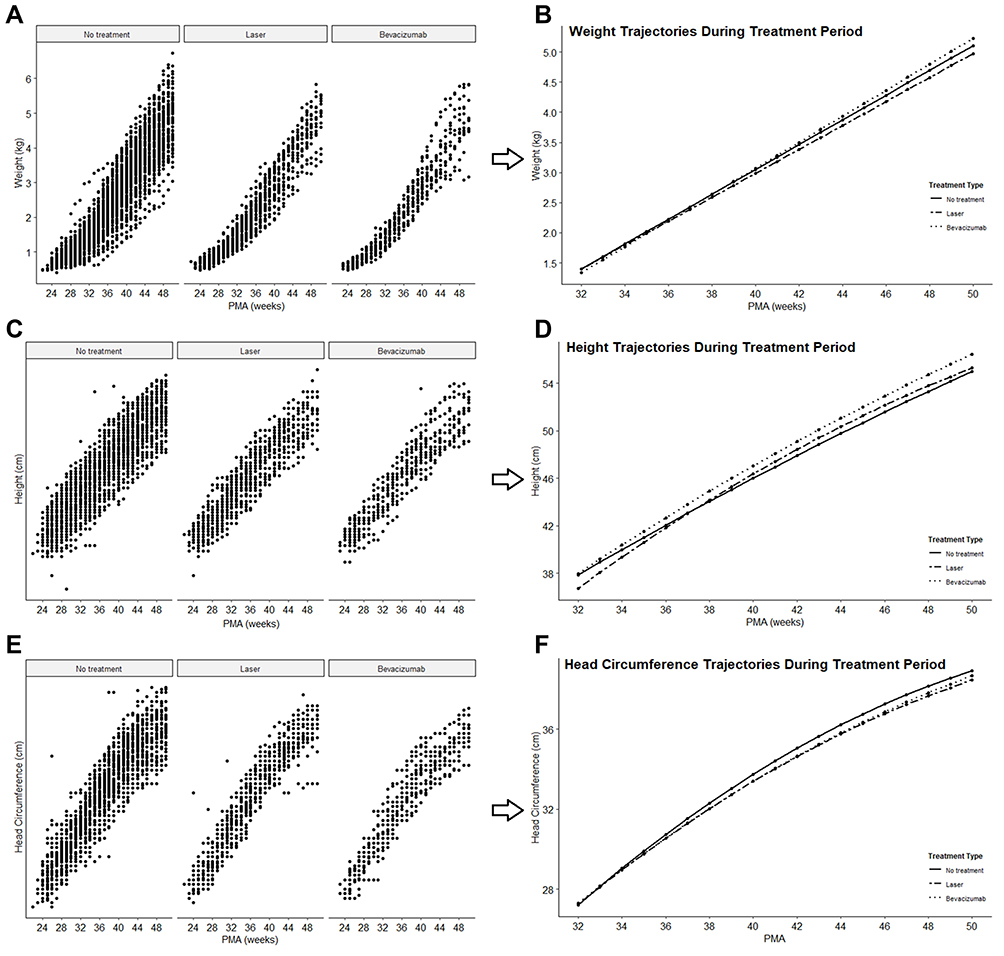 |
Figure 2 Postnatal growth trajectories during time period of ROP treatment and subsequent weeks of growth. Individual growth data from birth through 50 weeks PMA were plotted (A, C and E) and converted into prediction lines using mixed effects models (B, D and F). (B) Weight trajectories were not significantly different between groups after adjusting for initial birth weight. (D) Height trajectory for the bevacizumab group was not significantly different from the other study groups after adjusting for initial height at birth. Incidentally, the laser group showed a statistically different height trajectory compared to the untreated group. (F) Head circumference trajectories were not significantly different between groups after adjusting for initial head circumference at birth. |
Comparison of weight trajectories after treatment, adjusted for initial birth weight, showed no significant difference in the bevacizumab group (p = 0.31) or the laser group (p = 0.38) compared to the untreated group. The proportion of variance explained by the model in total (fixed and random effects), R2, was 98%. Comparison of height trajectories after treatment, adjusted for initial height at birth, showed no significant difference in the bevacizumab group compared to the untreated group (p = 0.42, R2= 95%). Incidentally, statistically significant differences were detected in the trajectory of the laser group compared to the untreated group (p = 0.01). Finally, comparison of head circumference trajectories, adjusted for initial head circumference at birth, showed no significant difference in growth across groups (bevacizumab vs untreated p = 0.23, laser vs untreated p = 0.44, R2= 96%).
Plotting of mean growth measures per week on the Fenton preterm growth chart qualitatively demonstrated percentile deterioration in weight, height, and head circumference from birth through 50 weeks PMA, regardless of sex or treatment status. At birth, mean weight in both sexes began around the 50th percentile range, then fell to the 10th percentile in males and 20th percentile in females. Mean height also began around the 50th percentile in both sexes, then fell to <3rd percentile in males and 3–10th percentile in females. Finally, mean head circumference at birth began around the 50th percentile and fell to 3–10th percentile in males; in females, head circumference deteriorated to 10th percentile over weeks 28–40 and recovered to the 30th percentile by 50 weeks PMA.
Discussion
The purpose of this study was to analyze postnatal growth and neurodevelopmental outcomes in a large single-center cohort of premature babies treated with IVB for ROP. To our knowledge, this is the first large retrospective study to compare longitudinal growth trends in infants treated with IVB to those who were treated with laser and untreated. The findings in this study were two-fold: our analysis of growth outcomes shows no difference in growth rates in weight, height, and head circumference over time in the IVB-treated group; in addition, we found no significant differences in Bayley III scores at 17–28 months between treatment groups.
Although VEGF has been shown to play a key role in neurodevelopment,7 previous studies have largely found no detriment to neurodevelopmental outcomes in infants treated with IVB.14–20 Bayley III scores have been the most commonly used metric to quantify neurodevelopment, and our analysis corroborates the majority of previous studies.
Several studies have found a higher risk of neurodevelopmental disability in infants treated with IVB,21–23 but concerns with selection bias and baseline inequalities limit the generalizability of results.24,25 A meta-analysis of eight studies conducted by Tsai et al showed no increased risk of severe neurodevelopmental impairment after IVB treatment, except for a minor difference in motor performance, the clinical effects of which are uncertain.26 In contrast, another meta-analysis of thirteen studies conducted by Kaushal et al found significantly increased odds of cognitive impairment, defined by Bayley III score <85, associated with IVB.27 Nevertheless, due to the low quality of evidence of studies used in both meta-analyses, there is consensus that further randomized control trials are needed to better understand systemic safety.
One additional concern of systemic IVB exposure is the potential risk of cerebral palsy, as suggested by Morin et al,21 who found increased odds of composite severe neurodevelopmental disability (which included cerebral palsy) in infants treated with IVB. Several subsequent studies have investigated the frequency of cerebral palsy and have not found an association.16,17,28 In our analysis, statistical analysis found an increased risk of cerebral palsy in the IVB group, even after adjusting for baseline confounders by logistic regression. However, this result was ultimately not statistically significant after false discovery rate correction, suggesting that this finding was likely a false-positive result in the setting of multiple testing.
It has been suggested that cerebral palsy is a movement disorder that is present from birth rather than a postnatal developmental disorder.14 However, even in the absence of a genetic component, postnatal neurologic insults such as infection, trauma, sepsis, kernicterus, or hypoxia-ischemia can precipitate CP.29 VEGF suppression could also theoretically fall into this category, as VEGF has been suggested to have a neuroprotective effect in hypoxic-ischemic brain injury.8 Despite the high probability of a false-positive result in our study evidenced by the statistical correction, we ultimately could not fully exclude the possibility of cerebral palsy risk with IVB treatment, and further studies are needed to better understand their association.
Physical growth is another key measure of postnatal development, which is heavily influenced by VEGF activity.6 In animal models, suppression of VEGF has shown context-dependent effects on insulin resistance and reduced weight gain, even with intravitreal injection.9 In humans, Kong et al30 measured weekly body weight gain from birth to 60 days in 24 infants treated with laser, 0.25 mg IVB, or 0.625 mg IVB. After adjusting for gestation age, sex, and birth weight, they found no significant differences in body weight at 60 days post treatment between groups. Due to the small sample size of that study, definite conclusions are limited but are consistent with the results of the present analysis.
Growth rate, the change in growth over time, is a more sensitive indicator of growth than a single measurement,30 and absolute growth rate during the first year of life is not significantly different between the two sexes.31 Comparison of growth trajectories in the weeks prior to treatment showed similar growth rates between groups, supporting the consistent growth trends among all preterm infants in this retrospective study. There were additionally no overall differences in PMA at the time of treatment between the IVB and laser groups. It is possible that earlier or later individual ages at the time of treatment may affect the impact of IVB or laser on subsequent growth; however, the time of treatment is dictated by ROP severity, which can be confounded by risk factors that also affect postnatal growth.
Intravitreal bevacizumab can escape from the eye into the systemic circulation and has been detected within serum as early as one to two days after intravitreal injection, with correspondingly suppressed serum VEGF levels up to eight weeks after treatment.5,30 Comparison of growth trends between treatment groups shows no significant differences in weight, height, or head circumference changes in the bevacizumab group compared to the laser and untreated groups up to 50 weeks PMA, which is up to 18 weeks after the earliest time of treatment in our sample. The incidental finding of height trajectory differences in the laser group compared to the untreated group may be due to the statistical growth model used; random variation within the data may cause a slightly different shape when fitting the prediction line and adding a quadratic term for time. Reassuringly, there was no significant difference between the IVB group and the laser group or the untreated group.
Additionally, comparison of mean growth measures to an established standard, the Fenton preterm growth chart, demonstrated deterioration in growth curve percentile regardless of sex and treatment status and is a known consequence of preterm birth.31 Despite the potential of catch-up growth in these preterm infants, postnatal growth continues to lag behind their term counterparts, even into adolescence and adulthood. The significance of impaired growth has a variety of metabolic consequences and systemic complications such as hypertension and insulin resistance.32 Overall, postnatal growth has been shown to be a prognostic factor associated with ROP and is an important consideration when investigating systemic outcomes; our results reassuringly did not find an impact of systemic bevacizumab exposure on these measures.
Limitations of this study include its retrospective nature; analysis of baseline characteristics and comorbidities has shown that, like previously published studies, infants treated with IVB have historically been smaller and sicker. These baseline differences can be adjusted for in statistical calculations but may not necessarily reflect real-life clinical consequences of using anti-VEGF agents in a vulnerable patient population. IVB treatment was generally for sicker children with anesthesia concerns or those with more posterior disease, and the choice of IVB versus laser treatment was not randomized due to the retrospective nature of this study. The proportion of patients with available Bayley scores was also higher in the IVB (55%) and laser (56%) groups compared to the untreated group (42%), which may have reflected selection bias for sicker patients that required more long-term follow-up. Despite this, there were no significant differences in Bayley scores between groups. Our limited sample size of IVB-treated patients may also limit the generalizability of neurodevelopmental findings, particularly our findings on cerebral palsy risk. Nevertheless, our robust comparison groups and novel analysis of growth outcomes provide additional data to the current literature surrounding systemic safety of IVB.
Conclusion
In all, anti-VEGF treatment for ROP has been shown to have comparable short-term efficacy to laser photocoagulation3,33 and has increased in usage due to greater ease of administration, decreased destruction of the peripheral retina, and lower risk of myopia.34 Studies on the systemic effects of these agents have been largely reassuring, but the lower quality of available evidence still warrants caution and investigation regarding their long-term effects on developing infants. Our results show no significant differences in postnatal growth, Bayley scores, hearing loss, and cerebral palsy compared to ROP infants receiving laser or no treatment. Further prospective, randomized studies will be needed to determine if anti-VEGF treatment for ROP indeed has clinically significant systemic consequences.
Ethics Statement
This study has obtained ethics approval from the institutional review boards of Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University in Chicago, Illinois. Written informed consent was waived due to the retrospective nature of the study, and the privacy of participants was ensured by anonymizing the data and securely storing all data in a private location.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen J, Smith LEH. Retinopathy of prematurity. Angiogenesis. 2007;10:133–140. doi:10.1007/s10456-007-9066-0
2. Good WV, Flynn JT, Flach AJ, Cibis GW, Raab EL, Beauchamp GR. Final results of the Early Treatment for Retinopathy of Prematurity (ETROP) randomized trial. Trans Am Ophthalmol Soc. 2004;102:233–250.
3. Mintz-Hittner HA, Kennedy KA, Chuang AZ. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364:603–615. doi:10.1056/NEJMoa1007374
4. Quinn GE, Darlow BA. Concerns for development after bevacizumab treatment of ROP. Pediatrics. 2016;137. doi:10.1542/peds.2016-0057
5. Wu WC, Lien R, Liao PJ, et al. Serum levels of vascular endothelial growth factor and related factors after intravitreous bevacizumab injection for retinopathy of prematurity. JAMA Ophthalmol. 2015;133:391–397. doi:10.1001/jamaophthalmol.2014.5373
6. Gerber HP, Hillan KJ, Ryan AM, et al. VEGF is required for growth and survival in neonatal mice. Development. 1999;126:1149–1159. doi:10.1242/dev.126.6.1149
7. James JM, Gewolb C, Bautch VL. Neurovascular development uses VEGF-A signaling to regulate blood vessel ingression into the neural tube. Development. 2009;136:833–841. doi:10.1242/dev.028845
8. Feng Y, Rhodes PG, Bhatt AJ. Neuroprotective effects of vascular endothelial growth factor following hypoxic ischemic brain injury in neonatal rats. Pediatr Res. 2008;64:370–374. doi:10.1203/PDR.0b013e318180ebe6
9. Sun K, Asterholm IW, Kusminski CM, et al. Dichotomous effects of VEGF-A on adipose tissue dysfunction. Proc Natl Acad Sci USA. 2012;109:5874–5879. doi:10.1073/pnas.1200447109
10. Hellstrom A, Perruzzi C, Ju M, et al. Low IGF-I suppresses VEGF-survival signaling in retinal endothelial cells: direct correlation with clinical retinopathy of prematurity. Proc Natl Acad Sci USA. 2001;98:5804–5808. doi:10.1073/pnas.101113998
11. Lin L, Binenbaum G. Postnatal weight gain and retinopathy of prematurity. Semin Perinatol. 2019;43:352–359. doi:10.1053/j.semperi.2019.05.008
12. Binenbaum G, Tomlinson LA, De Alba Campomanes AG, et al. Validation of the postnatal growth and retinopathy of prematurity screening criteria. JAMA Ophthalmol. 2020;138:31–37. doi:10.1001/jamaophthalmol.2019.4517
13. Binenbaum G, Bal S, Ying GS, Tomlinson L. Association of weight gain acceleration with risk of retinopathy of prematurity. JAMA Ophthalmol. 2019;137:1301–1305. doi:10.1001/jamaophthalmol.2019.3447
14. Fan YY, Huang YS, Huang CY, et al. Neurodevelopmental outcomes after intravitreal bevacizumab therapy for retinopathy of prematurity: a prospective case-control study. Ophthalmology. 2019;126:1567–1577. doi:10.1016/j.ophtha.2019.03.048
15. Chang YS, Chen YT, Lai TT, et al. Involution of retinopathy of prematurity and neurodevelopmental outcomes after intravitreal bevacizumab treatment. PLoS One. 2019;14:1–12. doi:10.1371/journal.pone.0223972
16. Rodriguez SH, Peyton C, Lewis K, et al. Neurodevelopmental outcomes comparing bevacizumab to laser for type 1 ROP. Ophthalmic Surg Lasers Imaging Retina. 2019;50:337–343. doi:10.3928/23258160-20190605-01
17. Kennedy KA, Mintz-Hittner HA; BEAT-ROP Cooperative Group. Medical and developmental outcomes of bevacizumab versus laser for retinopathy of prematurity. J AAPOS. 2018;22:61–65.e1. doi:10.1016/j.jaapos.2017.10.006
18. Lien R, Yu MH, Hsu KH, et al. Neurodevelopmental outcomes in infants with retinopathy of prematurity and bevacizumab treatment. PLoS One. 2016;11:e0148019. doi:10.1371/journal.pone.0148019
19. Ahmed K, Ali AS, Delwadia N, Greven MA. Neurodevelopmental outcomes following intravitreal bevacizumab with laser versus laser photocoagulation alone for retinopathy of prematurity. Ophthalmic Surg Lasers Imaging Retina. 2020;51:220–224. doi:10.3928/23258160-20200326-03
20. Araz-Ersan B, Kir N, Tuncer S, et al. Preliminary anatomical and neurodevelopmental outcomes of intravitreal bevacizumab as adjunctive treatment for retinopathy of prematurity. Curr Eye Res. 2015;40:585–591. doi:10.3109/02713683.2014.941070
21. Morin J, Luu TM, Superstein R, et al. Neurodevelopmental outcomes following bevacizumab injections for retinopathy of prematurity. Pediatrics. 2016;137:e20153218. doi:10.1542/peds.2015-3218
22. Arima M, Akiyama M, Fujiwara K, et al. Neurodevelopmental outcomes following intravitreal bevacizumab injection in Japanese preterm infants with type 1 retinopathy of prematurity. PLoS One. 2020;15:1–7. doi:10.1371/journal.pone.0230678
23. Natarajan G, Shankaran S, Nolen TL, et al. Neurodevelopmental outcomes of preterm infants with retinopathy of prematurity by treatment. Pediatrics. 2019;144:e20200056A. doi:10.1542/peds.2018-3537
24. Blair MP, Shapiro MJ, Berrocal AM; Ad Hoc Group Concerning Neurodevelopment and antiVEGF. Re: good: bevacizumab for retinopathy of prematurity: treatment when pathology is embedded in a normally developing vascular system (Ophthalmology. 2016;123:1843–1844). Ophthalmology. 2017;124:e74–e75. doi:10.1016/j.ophtha.2017.05.007
25. Rodriguez SH, Blair MP, Shapiro MJ, et al. Neurodevelopmental outcomes of preterm infants with retinopathy of prematurity by treatment. Pediatrics. 2020;145:2018–2020. doi:10.1542/peds.2020-0056A
26. Tsai CY, Yeh PT, Tsao PN, Chung YCE, Chang YS, Lai TT. Neurodevelopmental outcomes after bevacizumab treatment for retinopathy of prematurity: a meta-analysis. Ophthalmology. 2021;128:877–888. doi:10.1016/j.ophtha.2020.11.012
27. Kaushal M, Razak A, Patel W, Pullattayil AK, Kaushal A. Neurodevelopmental outcomes following bevacizumab treatment for retinopathy of prematurity: a systematic review and meta-analysis. J Perinatol. 2021;41:1225–1235. doi:10.1038/s41372-020-00884-9
28. Raghuram K, Isaac M, Yang J, et al. Neurodevelopmental outcomes in infants treated with intravitreal bevacizumab versus laser. J Perinatol. 2019;39:1300–1308. doi:10.1038/s41372-019-0420-z
29. Odding E, Roebroeck ME, Stam HJ. The epidemiology of cerebral palsy: incidence, impairments and risk factors. Disabil Rehabil. 2006;28:183–191. doi:10.1080/09638280500158422
30. Kong L, Bhatt AR, Demny AB, et al. Pharmacokinetics of bevacizumab and its effects on serum VEGF and IGF-1 in infants with retinopathy of prematurity. Investig Ophthalmol Vis Sci. 2015;56:956–961. doi:10.1167/iovs.14-15842
31. Casey PH, Kraemer HC, Bernbaum J, et al. Growth patterns of low birth weight preterm infants: a longitudinal analysis of a large, varied sample. J Pediatr. 1990;117:298–307. doi:10.1016/S0022-3476(05)80551-7
32. Euser AM, De Wit CC, Finken MJJ, Rijken M, Wit JM. Growth of preterm born children. Horm Res. 2008;70:319–328. doi:10.1159/000161862
33. Hwang CK, Hubbard GB, Hutchinson AK, Lambert SR. Outcomes after intravitreal bevacizumab versus laser photocoagulation for retinopathy of prematurity: a 5-year retrospective analysis. Ophthalmology. 2015;122:1008–1015. doi:10.1016/j.ophtha.2014.12.017
34. Geloneck MM, Chuang AZ, Mintz-Hittner HA, et al. Refractive outcomes following bevacizumab monotherapy compared with conventional laser treatment: a randomized clinical trial. JAMA Ophthalmol. 2014;132:1327–1333. doi:10.1001/jamaophthalmol.2014.2772
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.