Back to Journals » Clinical Ophthalmology » Volume 20
Posterior Capsule Rupture and Vitreous Loss in Cataract Surgery: A Retrospective Analysis from a Swiss Tertiary Center
Authors Spitznagel T ![]() , Somfai GM
, Somfai GM ![]() , Turgut F, Kang P, Katz T, Ernst SCK, Hornberger U, Becker MD, Heussen F
, Turgut F, Kang P, Katz T, Ernst SCK, Hornberger U, Becker MD, Heussen F ![]() , Ramsauer M
, Ramsauer M ![]()
Received 5 November 2025
Accepted for publication 12 March 2026
Published 3 April 2026 Volume 2026:20 577514
DOI https://doi.org/10.2147/OPTH.S577514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Bharat Gurnani
Tahm Spitznagel,1,2 Gábor Márk Somfai,1– 3 Ferhat Turgut,1– 4 Paul Kang,5 Toam Katz,6,7 Sophie-Christin Kornelia Ernst,1,2,8 Ute Hornberger,1,2 Matthias Dieter Becker,1,2,9 Florian Heussen,10 Michaela Ramsauer1,2
1Department of Ophthalmology, Stadtspital Zürich, Zurich, Switzerland; 2Spross Research Institute, Zurich, Switzerland; 3Department of Ophthalmology, Semmelweis University, Budapest, Hungary; 4Gutblick Research, Pfäffikon, Switzerland; 5University of Arizona Mel and Enid Zuckerman College of Public Health, Tucson, AZ, USA; 6EuroEyes, Zurich, Switzerland; 7Department of Ophthalmology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany; 8Department of Ophthalmology, Basel University Hospital, Basel, Switzerland; 9Department of Ophthalmology, Heidelberg University Hospital, Heidelberg, Germany; 10Department of Ophthalmology, Inselspital, Bern University Hospital, Bern, Switzerland
Correspondence: Michaela Ramsauer, Department of Ophthalmology, Stadtspital Zürich, Birmensdorferstrasse 497, Zürich, 8063, Switzerland, Email [email protected]
Purpose: To determine the incidence of posterior capsule rupture (PCR) and vitreous loss (VL) during cataract surgery in a Swiss tertiary care center. Furthermore, we aimed to evaluate preoperative risk factors associated with PCR/VL, including pseudoexfoliation (PEX), age, type of anesthesia, and the Triemli Cataract Score (TCS), a locally implemented preoperative risk assessment tool for surgical complexity.
Methods: This retrospective single-center cohort study included all phacoemulsification and refractive lens exchange procedures performed at Stadtspital Zürich between January 2021 and late August 2024. Data were retrieved from the Dendrite clinical database of the TCS and supplemented through manual chart review and surgical reports for identification of intraoperative complications. Univariable and multivariable logistic regression analyses were performed to evaluate associations between preoperative factors and the occurrence of PCR and/or VL.
Results: A total of 2’ 719 eyes were included in the study. PCR and/or VL occurred in 52 eyes (1.9%), including 45 cases of PCR (5 with concomitant VL) and 7 additional cases of isolated VL due to zonulolysis. In univariate analysis, PEX and a TCS ≥ 3 were significantly associated with an increased risk of PCR and/or VL (OR 2.72; p=0.003 and OR 2.38; p=0.002, respectively), while topical (vs. general) anesthesia was associated with a reduced risk (OR 0.51, p=0.019). In multivariate analysis, only PEX remained an independent risk factor (OR 2.38; p=0.013). The association between TCS ≥ 3 and PCR/VL just missed statistical significance (OR 1.79; p=0.057).
Conclusion: The rate of PCR and/or VL during cataract surgery at a Swiss tertiary care center is comparable to international statistics. PEX is a strong and independent predictor for these complications; although the predictive power of TCS did not reach statistical significance in multivariable analysis, the observed trend suggests that risk-based preoperative scores such as the TCS may support risk-stratification and surgical planning in clinical practice.
Keywords: surgical complications, triemli cataract score, phacoemulsification, risk factors
Introduction
Cataract surgery is one of the most frequently performed and safest surgical procedures in Ophthalmology. Nevertheless, posterior capsular rupture (PCR), often accompanied by vitreous loss (VL), remains the most common serious intraoperative complication and can significantly affect postoperative outcomes.1–3 In some cases, PCR leads to further surgical interventions, increased healthcare costs, prolonged recovery, and even long-term visual impairment.4
The integrity of the posterior capsule is widely recognized as a key indicator of surgical safety and quality in cataract surgery.2,3,5 Despite advances in phacoemulsification techniques, instrumentation, and surgical training, the incidence of PCR and/or VL has remained relatively stable over the past decade, with rates of approximately 1.1% and 2.1% reported in large multicenter studies.1,5–8
Numerous studies have identified a range of preoperative factors associated with an increased risk of PCR or VL, including advanced age, pseudoexfoliation (PEX), brunescent cataracts, small pupils, zonular instability, high axial length, and poor patient cooperation.6–9 Furthermore, surgeon experience is also considered a critical factor, with higher complication rates observed in procedures performed by trainees (3.2–5.1% PCR rate).4,10
To address these risks, several structured preoperative assessment tools have been developed, such as the Muhtaseb score and the updated Cataract Complexity Stratification Score.11 In addition to these internationally established scores, some institutions have developed customized systems tailored to their specific clinical settings. Such a recent example is the Triemli Cataract Score (TCS), a modified system adapted from the Muhtaseb et al Score and the New Zealand Cataract Risk Stratification (NZCR) scoring system11–15 The TCS was developed at the Department of Ophthalmology, Stadtspital Zürich (formerly called “Stadtspital Triemli”) and tailored to the specific needs of a Swiss public hospital setting. To estimate surgical complexity, it incorporates ocular, anatomical, and patient-related factors, such as pseudoexfoliation, pupil size, axial length, cataract density and systemic or behavioural conditions that could complicate surgery. The TCS classifies patients into “routine,” “complex,” or “highly complex” surgical categories and supports case assignment and counseling. By systematically identifying high-risk cases preoperatively, such tools facilitate safer case allocation and structured surgical training, ultimately enhancing patient safety and the quality of surgical training. A concise summary of the TCS risk factors is included in the Table S1.
To our knowledge, there is limited real-world data from Switzerland assessing the frequency of PCR and VL in a high-volume tertiary care setting, especially in correlation with risk stratification tools. This study retrospectively evaluates the incidence of PCR and VL during cataract surgery at Stadtspital Zürich. In addition, it explores the relationship between preoperative factors such as the TCS and the occurrence of intraoperative complications.
Materials and Methods
This retrospective, single-center clinical study was conducted at the Department of Ophthalmology at the public City Hospital Zurich, Switzerland. The study period included all cataract procedures performed between January 2021 and late August 2024. Ethical approval was obtained from the Cantonal Ethics Committee Zurich, Switzerland (2023–01867). The study was conducted in adherence with the Declaration of Helsinki and all federal state laws of Switzerland. All patients provided written general consent for the further use of their health-related data for research.
Inclusion and Exclusion Criteria
Eligible cases included all patients who underwent phacoemulsification cataract surgery or refractive lens exchange at Stadtspital Zürich during the above-mentioned study period. Only patients with complete datasets were considered for the analysis. In addition, only procedures performed exclusively by experienced cataract surgeons were included, namely senior attending physicians and the head of department, of whom each had performed over 250 cataract surgeries yearly. Exclusion criteria were congenital cataracts, cataracts with lens dislocation, combined surgeries (additional pars plana vitrectomy or glaucoma surgery), inexperienced surgeons (defined as having performed fewer than 250 yearly cataract surgeries based on institutional records prior to the study period), secondary IOL implantations or surgeries with other severe complications leading to blindness (eg. suprachoroidal hemorrhage), that were not associated with PCR/VL. Furthermore, patients with either missing or denied written general consent for the further use of health-related data for research were excluded (Figure 1).
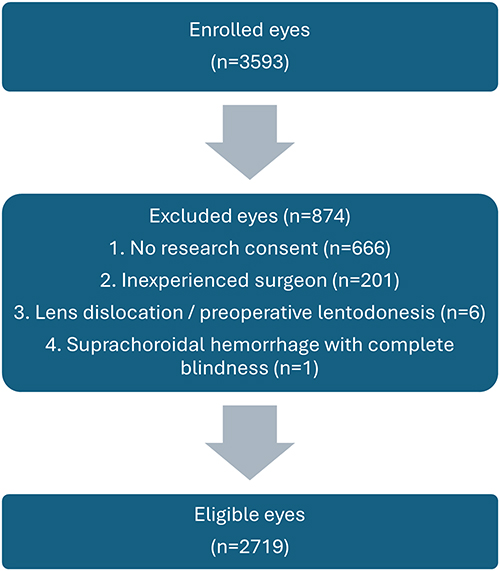 |
Figure 1 Flowchart of patient exclusion showing 2’719 eligible eyes out of 3’593. |
Endpoints
The primary endpoint was the intraoperative incidence of PCR and/or VL, as documented by the operating surgeon in standardized digital reports. Secondary endpoints included the influence of potential risk factors such as the TCS, age, PEX and the type of anesthesia.
Data Collection and Database Description
Data from cataract surgeries performed between January 2021 and late August 2024 were collected utilizing the Intellect database (Dendrite Clinical Systems, Reading, United Kingdom), which serves as a fully auditable platform for clinical data management. Since appointing the Dendrite system, a comprehensive database was built, including all patients who provided written consent and underwent ophthalmic surgery at our hospital. This database captured demographic details, preoperative and perioperative parameters, clinical follow-up notes and health questionnaire responses completed by the patients. Therefore, this approach allowed for more streamlined and accurate data handling.
All data entries were carefully reviewed and curated by a data manager and quality assurance team from our study center to ensure consistency and data integrity.
Intraoperative complications were systematically categorized based on the surgical report, including iris trauma, zonular dialysis, PCR, VL, anterior capsular tear, hemorrhage, and other specified events or a combination thereof.
Statistical Analysis
Demographics and clinical characteristics were reported for those with and without PCR/VL, using medians and interquartile ranges for continuous variables and frequencies and percentages for categorical variables. Medians and interquartile ranges were appropriate, as indicated by statistically significant Shapiro–Wilk assessments, which determined normality. Univariate logistic regression was used to assess the independent associations between each demographic and clinical characteristic and the odds of PCR/VL. Covariates with p < 0.20 were entered into a second model, where backward variable selection determined the covariates most associated with PCR/VL. All p-values were 2-sided, and p<0.05 was considered statistically significant. All data analyses were conducted using STATA version 18 (StataCorp, College Station, TX, USA).
Results
A total of 2’719 eyes were included in the analysis (Table 1). The median age of the cohort was 73.5 years. Among the patients, 1’337 male (49.2%) and 1’382 female (50.8%) underwent cataract surgery. Of the total eyes operated, 1’370 were right eyes (50.4%) and 1’349 were left eyes (49.6%). In total, 52 eyes (1.9%) experienced PCR and/or VL during cataract surgery. PCR occurred in 45 eyes, including 5 eyes with concomitant VL. 7 additional eyes showed isolated VL secondary to zonulolysis.
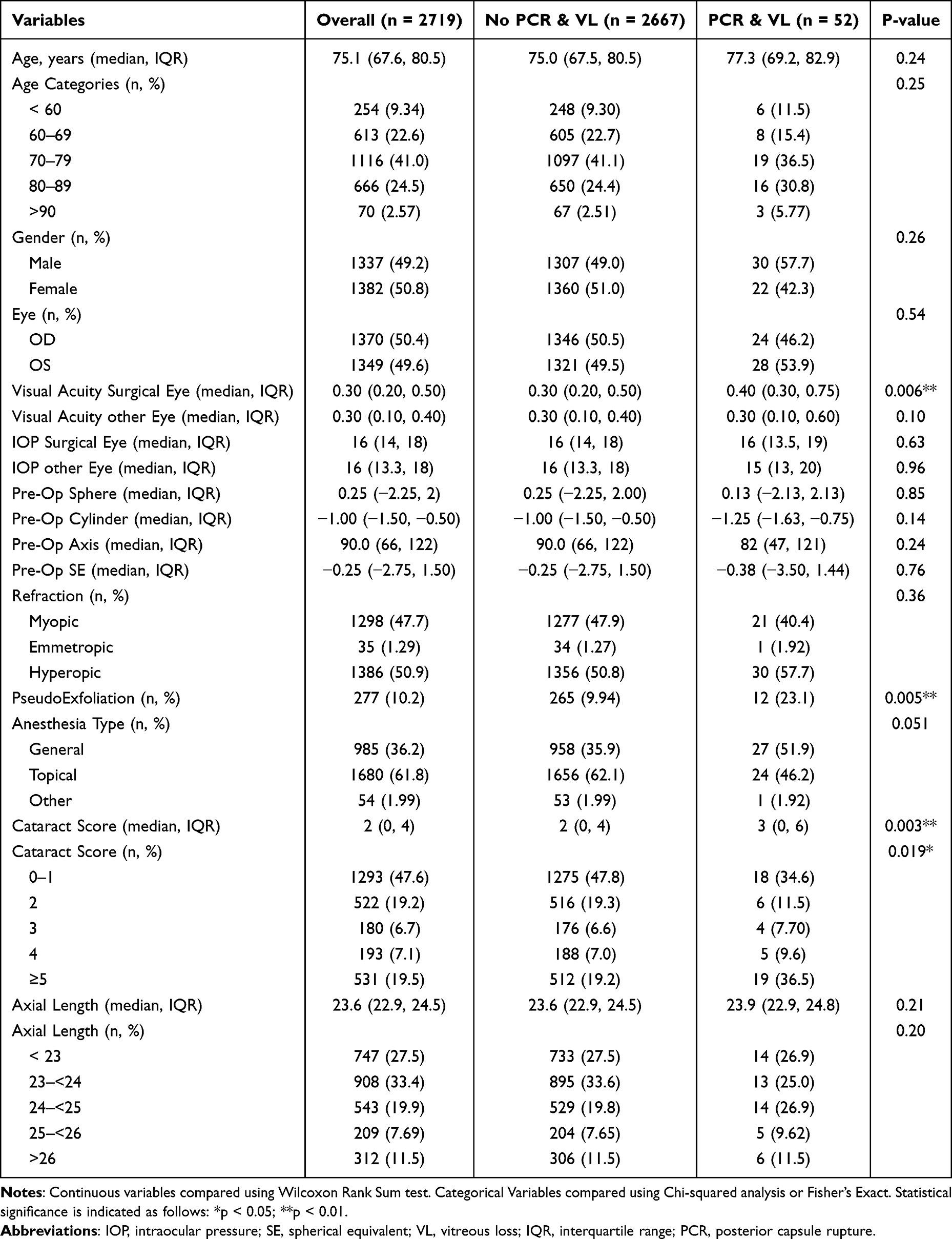 |
Table 1 Baseline Characteristics of the Study Patients |
In univariate analysis, several factors showed a statistically significant association with intraoperative complications (Table 2). Notably, eyes with PEX had a significantly increased risk of PCR/VL compared to eyes without PEX (OR 2.72, 95% CI 1.40–5.24; p = 0.003). The TCS ≥ 3 was also strongly associated with higher complication rates (OR 2.38, 95% CI 1.37–4.14; p = 0.002). Furthermore, topical anesthesia appeared to be protective, with a significantly lower complication rate compared to general anesthesia (OR 0.51, 95% CI 0.29–0.89; p = 0.019).
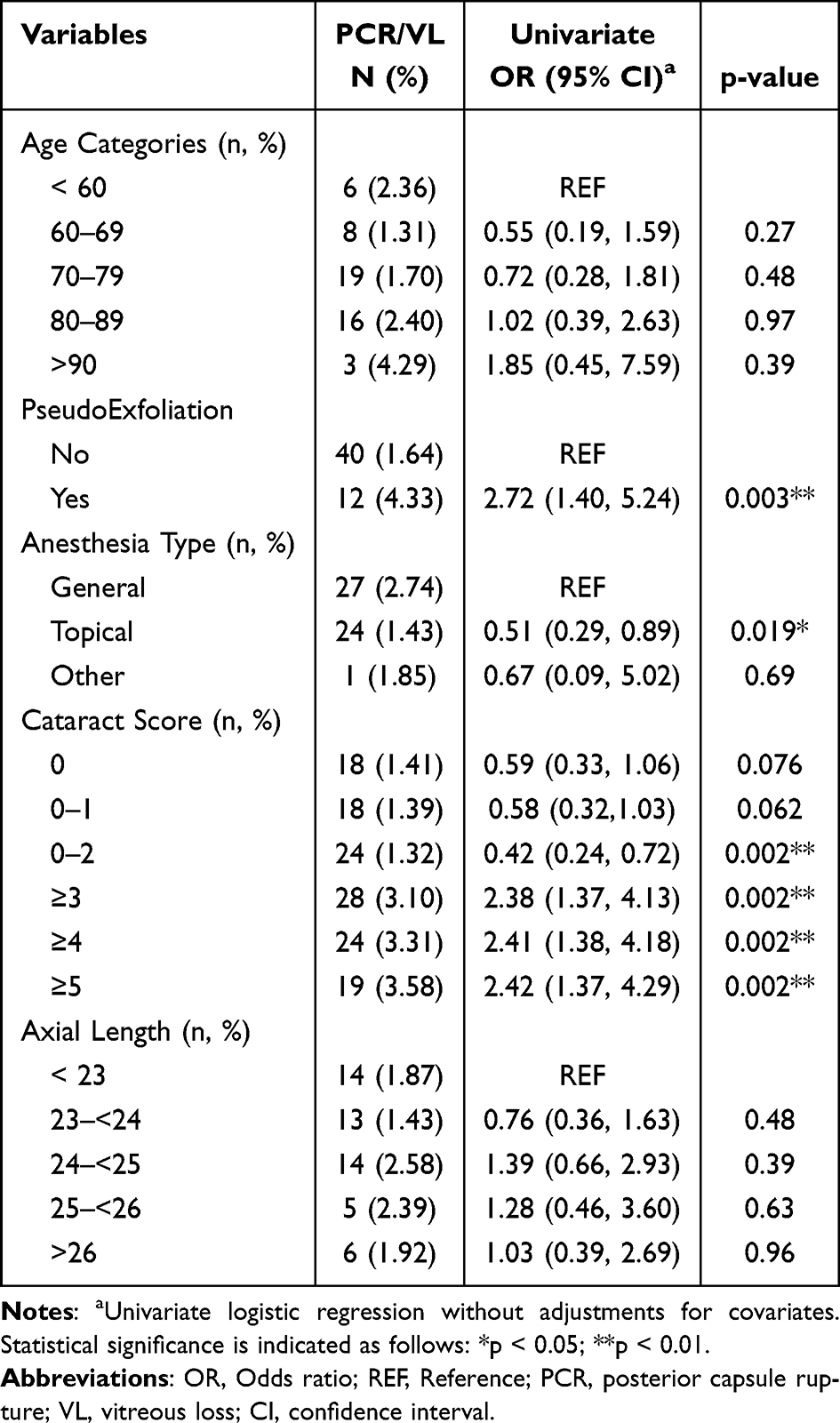 |
Table 2 Univariate Logistic Regression Analysis of Preoperative Risk Factors Associated with PCR and/or VL |
In the multivariate model (Table 3), which included variables with p < 0.20 in the univariate analysis, PEX remained an independent predictor of PCR/VL (OR 2.38, 95% CI 1.19–4.72; p = 0.013). The association between TCS ≥3 and intraoperative complications persisted but did not reach formal statistical significance (OR 1.79, 95% CI 0.98–3.25; p = 0.057). The protective effect of topical anesthesia was no longer significant after adjustment (OR 0.65, 95% CI 0.36–1.17; p = 0.15).
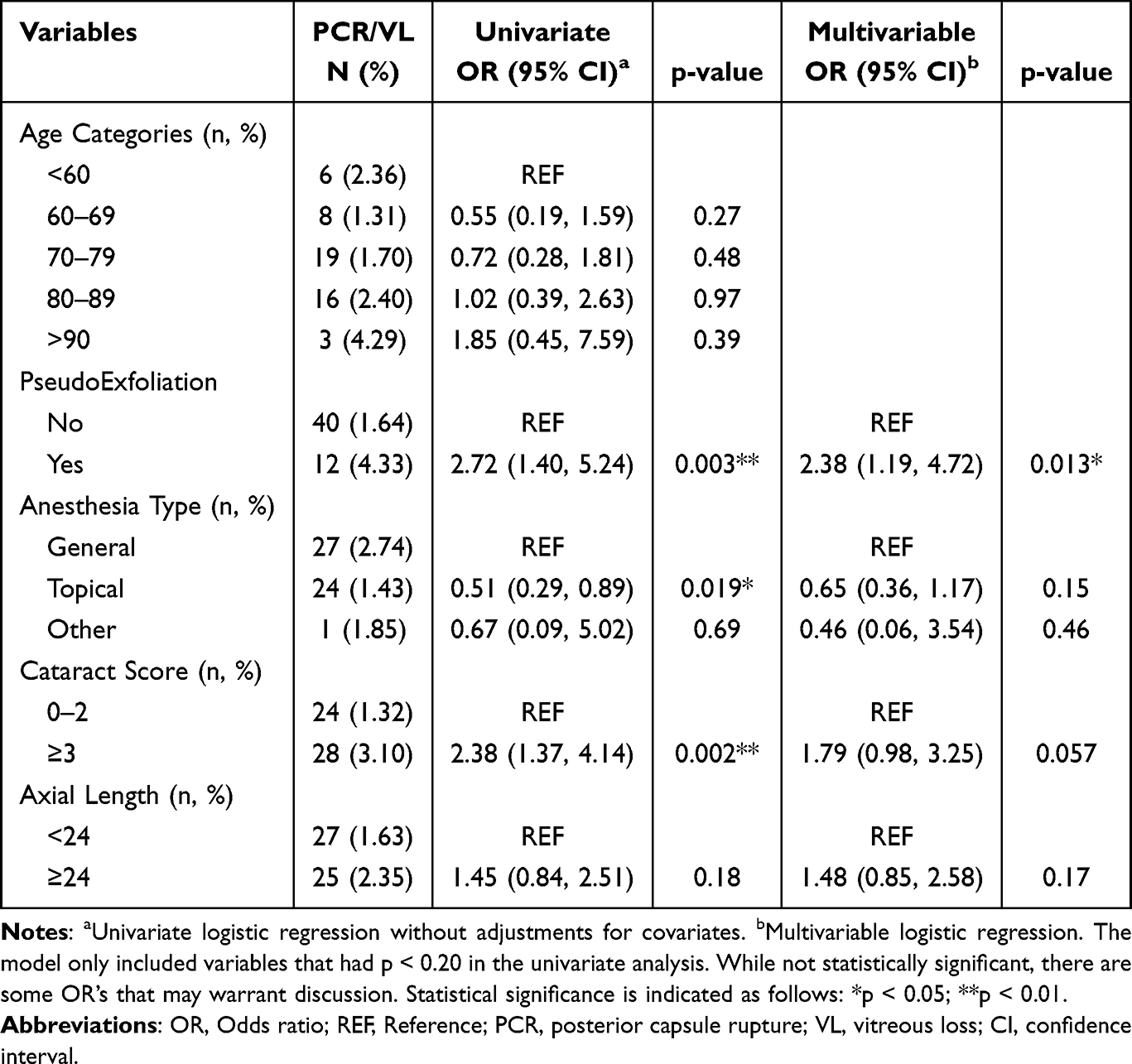 |
Table 3 Multivariate Logistic Regression Analysis of Independent Risk Factors for PCR and/or VL |
Patient age, including higher age categories (>80 or >90 years), did not show a significant association with PCR/VL in either uni- or multivariate analysis. Similarly, axial length was not a significant predictor of intraoperative complications.
Discussion
In this retrospective single-center study, performed at a large Swiss public hospital, the overall incidence of PCR and/or VL during cataract surgery was 1.9%. This rate is in line with international benchmarks from high-volume institutions and reflects a high standard of surgical care in the context of a publicly funded tertiary care setting.1,5,6,8 Despite advancements in surgical techniques and equipment, these complications remain a key factor for surgical safety and quality of care in cataract surgery.
While many established risk factors for PCR and VL have been described previously, the present study provides real-world benchmark data from a large Swiss public tertiary center within a clinical setting that has been underrepresented in the literature thus far. Our findings confirm the clinical significance of PEX as an independent risk factor for intraoperative complications.16,17 Even after adjustment for other covariates, eyes with visible PEX had more than double the odds of developing PCR and/or VL. This observation is consistent with prior reports and likely reflects underlying zonular weakness associated with PEX pathology. In contrast, other factors that have been highlighted in the literature, such as advanced age or increased axial length, did not reach statistical significance in our cohort. This may be due to differences in patient demographics or case selection.
As a secondary and exploratory analysis, we evaluated the association between a locally adapted risk stratification system, the TCS, and intraoperative complications. The TCS was previously introduced at our institution to support surgical planning and case allocation. While a TCS ≥ 3 was associated with a higher complication rate in univariate analysis, the association did not reach statistical significance in the multivariate model (p = 0.057). This may in part reflect the inclusion of multiple individual risk factors, such as PEX, small pupils, or poor visibility that are already embedded in the score itself. Importantly, the present study was not designed to formally assess or validate the predictive performance of the TCS. Therefore, the observed trends should be interpreted as hypothesis-generating rather than confirmatory. While these findings provide contextual insights into the potential role of structured preoperative risk stratification tools in routine clinical practice, further prospective and multicenter studies are required to evaluate their predictive capacity and clinical utility.
The increased risk of complications associated with procedures performed under general anesthesia, as observed in the univariate analysis, is likely attributable to the fact that more complex cases are preferentially scheduled for general rather than local anesthesia. However, in the multivariate analysis, no definite association could be established between the type of anesthesia and the occurrence of complications.
Several studies have indicated an increased risk of PCR and/or VL in older patients (over 80 or 90 years of age).6,18 While the point estimate in our study (odds ratio: 1.85 in patients over 90 years) suggests a potentially elevated risk, the wide confidence interval (0.45–7.59) does not allow for a definitive conclusion, likely due to the small sample size in this age group and the low event rate.
It is important to point to the several limitations of the study. First, its retrospective design may introduce documentation bias, particularly with respect to the accurate reporting of intraoperative events. To mitigate this risk, intraoperative complications were identified based on standardized digital surgical reports and were additionally cross-checked by manual review of operative notes and clinical records.
Second, as novice surgeons were excluded, heterogeneity in surgical experience was maintained among the study population. More detailed assessment of surgical hierarchy or learning curves was not feasible due to limitations in the available retrospective data; therefore, surgeon-specific variables were not explored in detail. Third, our dataset did not permit stratified analyses of postoperative visual outcomes or postoperative complications such as endophthalmitis, as these data are not included in our registry due to the fact that the majority of patients are referred back to their private ophthalmologist following an uneventful initial postoperative follow-up visit. Thus, potential differential effects of PCR and/or VL on visual prognosis across clinically relevant subgroups (eg, by age, preexisting ocular pathology etc.) and other postoperative complications could not be evaluated. Such analyses would have offered a deeper understanding of the broader clinical relevance of these intraoperative complications. Finally, the relatively low number of intraoperative complication events may have limited statistical power and increase the risk of Type II error, particularly in multivariable analyses.
Despite its limitations, this study contributes meaningful real-world data on the incidence and risk factors of intraoperative complications in cataract surgery within a high-volume, public Swiss tertiary care center. The identification of PEX as a significant risk factor reinforces the importance of careful preoperative assessment, and the exploratory analysis of the TCS highlights the potential benefit of structured, patient-specific risk stratification tools in routine surgical planning and the training of cataract surgeons.
Conclusion
In conclusion, PCR and VL remain clinically relevant intraoperative complications, occurring in approximately 1.9% of cataract surgeries.1,5,6,8 Our findings highlight the importance of thorough preoperative risk assessment, particularly regarding PEX, and support the integration of structured risk stratification approaches into everyday surgical decision-making. Future prospective and multicenter studies are required to further evaluate the role and clinical utility of the TCS to link intraoperative complications with postoperative visual and refractive outcomes.
Funding
This study was supported by the Werner H. Spross Stiftung zur Förderung der Augenheilkunde, Zurich, Switzerland.
Disclosure
Dr Gábor Somfai reports personal fees from Abbvie, Bayer, Carl Zeiss, Roche, and Apellis, outside the submitted work. Dr Michaela Ramsauer reports non-financial support from Refractive Surgery Alliance, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Day AC, Donachie PH, Sparrow JM, Johnston RL. The Royal College of Ophthalmologists’ National Ophthalmology Database study of cataract surgery: report 1, visual outcomes and complications. Eye. 2015;29(4):552–8. doi:10.1038/eye.2015.3
2. Jaycock P, Johnston RL, Taylor H, et al. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye. 2009;23(1):38–49. doi:10.1038/sj.eye.6703015
3. Mahmud I, Kelley T, Stowell C, et al. A proposed minimum standard set of outcome measures for cataract surgery. JAMA Ophthalmol. 2015;133(11):1247–1252. doi:10.1001/jamaophthalmol.2015.2810
4. Ti SE, Yang YN, Lang SS, Chee SP. A 5-year audit of cataract surgery outcomes after posterior capsule rupture and risk factors affecting visual acuity. Am J Ophthalmol. 2014;157(1):180–185.e1. doi:10.1016/j.ajo.2013.08.022
5. Johnston RL, Taylor H, Smith R, Sparrow JM. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: variation in posterior capsule rupture rates between surgeons. Eye. 2010;24(5):888–893. doi:10.1038/eye.2009.195
6. Narendran N, Jaycock P, Johnston RL, et al. The Cataract National Dataset electronic multicentre audit of 55,567 operations: risk stratification for posterior capsule rupture and vitreous loss. Eye. 2009;23(1):31–37. doi:10.1038/sj.eye.6703049
7. Segers MHM, Behndig A, van den Biggelaar FJHM, et al. Risk factors for posterior capsule rupture in cataract surgery as reflected in the European Registry of quality outcomes for cataract and refractive surgery. J Cataract Refract Surg. 2022;48(1):51–55. doi:10.1097/j.jcrs.0000000000000708
8. Lundström M, Behndig A, Kugelberg M, Montan P, Stenevi U, Thorburn W. Decreasing rate of capsule complications in cataract surgery: eight-year study of incidence, risk factors, and data validity by the Swedish National Cataract Register. J Cataract Refract Surg. 2011;37(10):1762–1767. doi:10.1016/j.jcrs.2011.05.022
9. Day AC, Donachie PH, Sparrow JM, Johnston RL; Royal College of Ophthalmologists’ National Ophthalmology Database. The Royal College of Ophthalmologists’ National Ophthalmology Database study of cataract surgery: report 2, relationships of axial length with ocular copathology, preoperative visual acuity, and posterior capsule rupture. Eye. 2015;29(12):1528–1537. doi:10.1038/eye.2015.198
10. Jeang LJ, Liechty JJ, Powell A, et al. Rate of posterior capsule rupture in phacoemulsification cataract surgery by residents with institution of a wet laboratory course. J Acad Ophthalmol. 2022;14(1):e70–e73. doi:10.1055/s-0042-1744270
11. Muhtaseb M, Kalhoro A, Ionides A. A system for preoperative stratification of cataract patients according to risk of intraoperative complications: a prospective analysis of 1441 cases. Br J Ophthalmol. 2004;88(10):1242–1246. doi:10.1136/bjo.2004.046003
12. Kim BZ, Patel DV, Sherwin T, McGhee CNJ. The Auckland Cataract Study: assessing preoperative risk stratification systems for phacoemulsification surgery in a teaching hospital. Am J Ophthalmol. 2016;171:145–150. doi:10.1016/j.ajo.2016.09.003
13. Sjoberg DD, Whiting K, Curry M, Lavery JA, Larmarange J. Reproducible summary tables with the gtsummary package. R J. 2021;13(1):570–580. doi:10.32614/RJ-2021-053
14. Kaiser KP, Turgut F, Ernst SCK, et al. Implementation of a modified risk stratification score in cataract surgery at a Swiss public hospital. Clin Ophthalmol. 2025;19:3307–3316. doi:10.2147/OPTH.S544354
15. Nderitu P, Ursell P. Updated cataract surgery complexity stratification score for trainee ophthalmic surgeons. J Cataract Refract Surg. 2018;44(6):709–717. doi:10.1016/j.jcrs.2018.04.036
16. Vazquez-Ferreiro P, Carrera-Hueso FJ, Rodriguez LB, Diaz-Rey M, Barrios MAR, Jornet JEP. Determinants of the risk of intraoperative complications in phacoemulsification among patients with pseudoexfoliation. Saudi J Ophthalmol. 2021;35(1):5–8. doi:10.4103/1319-4534.325774
17. Lumme P, Laatikainen LT. Risk factors for intraoperative and early postoperative complications in extracapsular cataract surgery. Eur J Ophthalmol. 1994;4(3):151–158. doi:10.1177/112067219400400304
18. Berler DK. Intraoperative complications during cataract surgery in the very old. Trans Am Ophthalmol Soc. 2000;98:127–130.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.