Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Post-Market Observational Study of Injectable PLLA Microspheres for Facial Rejuvenation
Authors Bertossi D, Camporese A, Kefalas N, Massidda E, Papagni MF, Patalano M II, Quartucci S, Renga MM, Santorelli A, Sciuto C, Trocchi G
Received 17 February 2026
Accepted for publication 21 April 2026
Published 13 May 2026 Volume 2026:19 589929
DOI https://doi.org/10.2147/CCID.S589929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Anne-Claire Fougerousse
Dario Bertossi,1 Alessandra Camporese,2 Nicola Kefalas,3 Enrico Massidda,4 Marco Francesco Papagni,5 Mariagrazia Patalano II,6 Sandro Quartucci,7 Monica MR Renga,5 Adriano Santorelli,8 Chantal Sciuto,9 Gloria Trocchi10
1Section of Oral and Maxillofacial Surgery, Department of Surgical Sciences, University of Verona, Verona, Italy; 2International School of Aesthetic Medicine, Fondazione Internazionale Fatebenefratelli, Rome, Italy; 3Private Practice, Turin, Italy; 4Master in Regenerative and Anti-Aging Aesthetic Medicine, Università Niccolò Cusano, Rome, Italy; Italian Society of Aesthetic Medicine (SIME), Sardinia, Italy; 5Agorà, Italian Society of Aesthetic Medicine, Milan, Italy; 6Studio Mariagrazia Patalano, Private Practice, Messina, Italy; 7Saba Clinic, Rome, Italy; 8Adriano Santorelli & Partners, Private Practice, Naples, Italy; 9Studio Sciuto, Private Practice, Rome, Italy; Studio Sciuto, Private Practice, Dubai, United Arab Emirates; Agorà, Italian Society of Aesthetic Medicine, Milan, Italy; 10Outpatient Service of Aesthetic Medicine and Psychophysical Wellbeing, Isola Tiberina Hospital – Gemelli Isola, Rome, Italy; Italian Society of Aesthetic Medicine (SIME), Rome, Italy
Correspondence: Dario Bertossi, Section of Oral and Maxillofacial Surgery, Department of Surgical Sciences, University of Verona, Piazzale L.A. Scuro 10, Verona, 37134, Italy, Email [email protected]
Purpose: Facial aging and dermal conditions may negatively influence the quality of life, leading patients to seek aesthetic procedures to restore a more satisfying appearance. This post-market observational study investigates the efficacy and safety of PLLA microspheres (PLLA-LASYNPRO™) in patients affected by chrono-and photoaging and other facial skin conditions.
Patients and Methods: Ninety-five adult patients affected by chronoaging, photoaging and skin conditions such as oily and acne-prone skin, rosacea, or scarring, were treated with PLLA-based injectable). The patients assessed treatment outcomes through a questionnaire during the sessions and after the end of the treatment. 2D and 3D images were taken for documentation. Physicians assessed the treatment efficacy through the Global Aesthetic Improvement Scale (GAIS) between sessions and at the 6 months follow-up. Adverse events (AEs) were evaluated immediately after the procedure and after 6 months.
Results: All treated patients demonstrated visible improvement in facial appearance, with 100% showing GAIS enhancement as assessed by physicians and strong concordance from patient self-evaluations, where satisfaction was reported by 94.7% of respondents, although only 56 patients returned the follow-up questionnaire. Improvements were already present after the first session in 60% of the participants, noted in skin texture, firmness, and elasticity, with progressive enhancement over time. Only mild, transient AEs were reported, such as short-term swelling or localized discomfort, all resolving spontaneously without complications or nodular formation.
Conclusion: PLLA-LASYNPRO™ proved to be a safe, effective, and well-tolerated injectable bio-regenerator. The treatment achieved high levels of patient satisfaction and compliance, producing natural, gradual, and sustained aesthetic improvements in skin quality and facial contour, particularly in the middle and lower face. A medical infographic summarizes a study on PLLA microspheres for treating chrono- and photoaging and other facial conditions. The workflow includes: Population (95 adults with various skin conditions), PLLA Treatment (injectable sessions), Assessment (GAIS, patient questionnaires) and a 6-Month Follow-Up (adverse events monitoring). Key outcomes: 94.7% patient satisfaction, 100% GAIS improvement at 6 months and 60% improvement after the first session. No nodules or ischemic events were reported, only mild transient adverse effects like swelling, resolving in 2-3 days. Conclusion: PLLA-LASYNPRO™ is a safe, effective and well-tolerated bio-regenerator, achieving high patient satisfaction and compliance.Infographic summarizing PLLA microspheres study results: satisfaction, GAIS improvement and safety outcomes.
Keywords: poly-L-lactic acid, PLLA, collagen stimulation, regenerative aesthetics, facial rejuvenation, real-world evidence, skin quality
Introduction
Facial aging is a complex and multifactorial biological process driven by both intrinsic and extrinsic factors. Intrinsic aging results from genetically programmed cellular senescence and hormonal changes, while extrinsic factors such as ultraviolet (UV) radiation, oxidative stress, environmental pollution, and lifestyle habits further accelerate tissue degeneration.1,2 Together, these mechanisms lead to profound structural and functional alterations in the skin and subcutaneous tissues. Progressive dermal thinning, collagen and elastin degradation, decreased fibroblast activity, and impaired extracellular matrix turnover result in loss of elasticity, hydration, and volume.3 Concurrently, fat redistribution, skeletal resorption, and ligament laxity contribute to the gradual loss of facial contour, culminating in the visible signs of aging such as wrinkles, skin laxity, and volume depletion.4 Traditional aesthetic medicine has largely focused on compensating for these changes through mechanical volumetric restoration, primarily employing hyaluronic acid–based fillers or other implantable materials.5,6 While effective for immediate correction, these fillers do not address the fundamental biological decline underlying the aging process. In recent years, however, the concept of regenerative aesthetics has emerged, emphasizing skin health and quality improvement through stimulation of the body’s intrinsic regenerative mechanisms.7,8 This paradigm shift reflects the growing patient demand for natural-looking, long-lasting results that enhance the structural and functional integrity of the skin rather than simply masking aging-related deficits. Regenerative treatments aim to activate fibroblasts, induce neocollagenesis and neoelastogenesis, and promote balanced dermal remodelling, thereby restoring both the appearance and vitality of the skin.9,10
Among the various biostimulatory agents introduced for regenerative purposes, poly-L-lactic acid (PLLA) has demonstrated robust and reproducible efficacy in stimulating collagen synthesis and improving dermal thickness.11 PLLA is a synthetic, biodegradable, and biocompatible polymer that acts as a scaffold to induce fibroblast proliferation and gradual collagen deposition over time,12,13 resulting in progressive volumisation and skin texture enhancement with long-lasting effects.14 Despite its clinical success, earlier PLLA formulations presented practical limitations, including delayed onset of aesthetic improvement, complex reconstitution requirements, and potential adverse events such as papule or nodule formation related to uneven particle distribution.15,16 These challenges have prompted the development of next-generation PLLA-based systems with optimized physical and handling properties. PLLA-LASYNPRO™ represents an innovative advancement in this field, designed to overcome the limitations of traditional PLLA formulations while maximizing regenerative efficacy.17 It is an injectable biostimulator composed of PLLA microspheres suspended within a proprietary carrier system that ensures uniform particle dispersion, improved injectability, and enhanced biocompatibility.18 The formulation rationale of PLLA-based injectable lies in its ability to deliver controlled, predictable collagen stimulation and tissue regeneration while minimizing the risk of adverse reactions19 lowering the pro-inflammatory cascade associated with earlier formulations This mechanism supports a controlled, multidimensional regenerative response characterized by coordinated collagen deposition, elastin remodeling, and increased dermal density. Overall, PLLA-based injectable should be framed as an evidence-backed evolution of PLLA technology, enabling predictable tissue integration and addressing critical limitations of earlier generations. By refining polymer uniformity and optimizing particle–carrier interaction, PLLA-LASYNPRO™ supports a reproducible regenerative cascade. These biological effects are supported by activation of key pathways involved in tissue repair and remodeling.20 PLLA-based injectabletherefore ensures homogeneous tissue integration contributing to improved dermal elasticity, thickness, and overall facial contour.21 From a regenerative perspective, PLLA-based injectable aligns with the principles of modern aesthetic medicine by addressing both structural and biological aspects of skin aging. Rather than acting solely as a volumetric filler, it functions as a biological activator and restoring tissue functionality.17,21 Given these mechanistic properties, evaluating the real-world clinical performance of PLLA-based injectable becomes essential to understand how this multidimensional regenerative profile translates into patient outcomes.
The present real-world, post-market study was designed to evaluate the efficacy, safety, and patient satisfaction associated with PLLA-LASYNPRO™ for facial aesthetic rejuvenation in adult subjects. By assessing clinical outcomes under routine practice conditions, this investigation aims to provide valuable insights into the performance of JULÄINE™ (Nordberg Medical AB, Huddinge, Sweden), a PLLA-based injectablemedical device, in everyday aesthetic settings and to contribute to the growing body of evidence supporting regenerative injectables as a cornerstone of next-generation facial rejuvenation therapies.
Materials and Methods
Data Collection Design
This real-world evidence study was performed in different clinics in Italy, between June 2024 and April 2025. The aim of the study was to investigate the efficacy, safety and level of satisfaction in patients who underwent an aesthetic facial rejuvenation procedure with the PLLA-based injectable through a questionnaire provided to patients and physicians. Physicians assessed the occurrence of AEs immediately after every session and at the 6-month follow-up visit. The observational study was designed prospectively, with patients being informed of the participation in the study. Surveys were standardized across centers and developed specifically for this study.
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and applicable regulatory requirements.
Inclusion and Exclusion Criteria
The study included 95 patients (85 females and 10 males) above 18 years old. The skin type of each patient was categorized according to the Fitzpatrick Skin Phototype Classification.22 Patients in this study presented different skin conditions including chrono-and photoaging, bad skin quality and scarring. Patients’ baseline characteristics are reported in Table 1. All patients gave informed consent after an exhaustive explanation of the procedure and its potential adverse events (AEs).
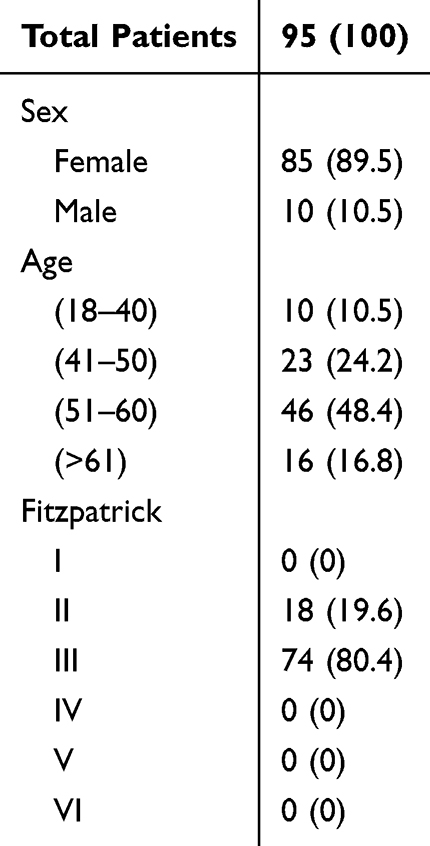 |
Table 1 Patients’ Baseline Characteristics |
Treatment Protocol
JULÄINE™, the new injectable medical device used in this study, is a PLLA-based injectablebio-regenerator containing highly uniform microspheres to smoothen wrinkles and tighten the skin. Each vial, containing a dry powder of 150 mg of poly-L-lactic acid microspheres, 45 mg of sodium carboxymethylcellulose and 145 mg of non -pyrogenic mannitol was reconstituted with 5 mL of saline solution, according to manufacturer’s instructions, and used immediately. 1 to 4 mL (average 2.44 mL) were used for each patient’s side. The product was placed in the superficial subcutaneous layer and/or in the deep dermis, using a 25-gauge cannula and following a retrograde linear fanning technique. Injections were performed through skin perforations at different entry points. The injection is divided in 5–6 vectors in a fanning fashion for each entry point, depositing 0.4–0.5 mL per vector. This technique ensures an even distribution of the product in a broader anatomical area, not focusing only on the single wrinkle or depression. The most frequent entry points are depicted in Figure 1: for the middle-third area the entry point is just below the zygomatic arch, in the lateral malar; in the perioral area and nasolabial folds it is located 1 cm laterally from the oral commissure; for the medial and lateral mandibular points it is in the lower-third region. The treatment comprised 2 to 3 sessions, 6 to 8 weeks apart. All patients received a follow-up 6 months after the initial session.
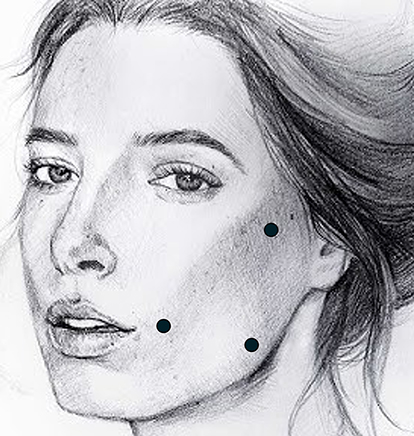 |
Figure 1 Typical entry points for PLLA-LASYNPRO™ injection. Black dots indicate the most frequently used injection entry points for cannula insertion during treatment. |
Patients’ Survey
Patients were provided a survey to evaluate their previous knowledge and expectations from the aesthetic treatments. Satisfaction of the procedure outcomes was evaluated after the first treatment and at the follow-up visit.
Physicians’ Survey
Physicians evaluated the efficacy of the treatment with a Global Aesthetic Improvement Scale (GAIS) before the second and third sessions and at the 6 months follow-up. The results were graded as “much improved”, “improved”, “no change”, and “worse”. GAIS evaluation was performed by the patient’s practitioner and not blinded due to the nature of the study. Patients evaluated during the three assessment timepoints were 94, 90 and 73. To better compare the pre- and post- treatment conditions, rigorous positioning protocols were used to take imaging, ensuring consistency and facilitating comparisons. To evaluate wrinkles depth, Vectra H1, VISIA and ANTERA imaging system were used to provide a qualitative analysis. Adverse events were assessed by physicians immediately after the treatment and at the 6 months follow-up.
Both patients’ and physicians’ survey responses were collected and percentage of respondents were calculated on the basis of the total number of answers.
Statistical Analysis
Categorical variables were summarized as percentages. Differences in the distribution of Global Aesthetic Improvement Scale (GAIS) scores across timepoints (before session 2, before session 3, and 3 months after the last treatment) were assessed using the chi-square (χ2) test. Given the ordinal nature of GAIS, a test for trend across ordered categories was also performed to evaluate changes over time. Additionally, responder rates (defined as GAIS scores of 1–2) were compared between timepoints using tests for proportions. All tests were two-sided, and a p-value < 0.05 was considered statistically significant. Analyses were conducted using aggregated data.
Adverse Events
Adverse events (AEs) were assessed by the patients at the intermediate and final timepoints, rating the amount of pain during the treatments and the duration of the swelling after the treatment. Physicians recorded immediate AEs after injection and evaluated the presence of nodules or ischemic events after treatments.
Imaging Assessment
Pictures of the patients were taken before the initial treatment, after the first session, second session and after 6 months from the first infiltration. Rigorous positioning protocols were followed before image capture to ensure consistency and facilitate accurate comparison between pre-and post-treatment conditions. Additional imaging was performed with VISIA to perform skin analysis, ANTERA for the measurement of wrinkles and texture and with digital dermatoscope for skin assessment. A pinch test was performed to qualitatively assess the skin firmness by picture.
Results
Adult participants of both sexes spontaneously asking for a treatment were treated with PLLA-based injectable in different facial areas. Initially, 114 subjects answered to the first survey evaluating their knowledge of available collagen-stimulating options and their expectations about the treatment. Of these, 95 subjects proceeded to be enrolled in the study. The study participants were then asked to fill a questionnaire about initial satisfaction and adverse events before the second treatment. At the final timepoint, 6 months after the initial treatment, subjects were asked to give a final assessment on the treatment and 56 returned the questionnaires.
Subjects were asked about their knowledge and expectations regarding aesthetic treatments before the first treatment, and to evaluate their knowledge and experience with biostimulation treatments, collagen stimulation and their potential benefits. A small proportion of subjects was not aware of this type of treatments (11.4%), whereas 28.1% of subjects already heard of it, 25.4% had a good knowledge and 35.1% had a very good knowledge (Figure 2A). Among respondents, 14.9% of subjects never had experience with aesthetic treatments, 12.3% never had them but investigated this aspect, 37.7% had experience but without a regular treatment rhythm and 35.1% had them several times per year (Figure 2B). Regarding aesthetic treatment results, the majority of respondents (91.2%) stated that what they valued most was to achieve a natural result, while a minority reported that they valued most quickly visible results (2.6%) or long-lasting results, up to 24 months (6.1%) (Figure 2C). The preferred aim of the treatment was to improve skin quality (31.8%), achieve a firmer skin structure (25.2%), have a younger look (24%), contour the face (14%), or appear more attractive (5%) (Figure 2D).
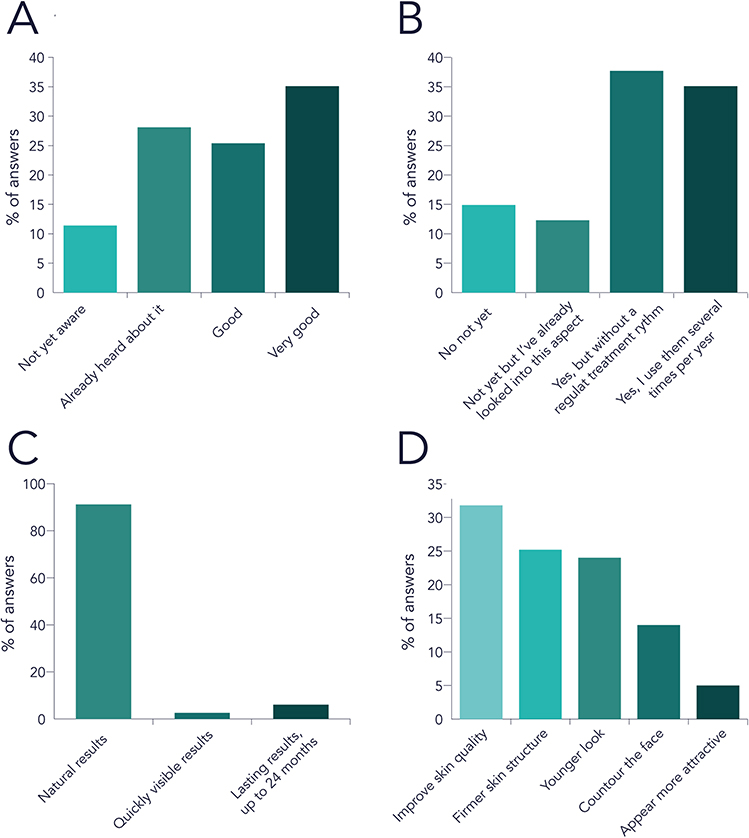 |
Figure 2 Survey regarding previous knowledge and experience with aesthetic treatments and expectations on aesthetic treatments. (A) Self-reported level of knowledge about biostimulation treatments and collagen stimulation; (B) Previous experience with aesthetic treatments; (C) Key factors considered important when choosing aesthetic treatments; (D) Desired outcomes from aesthetic treatments. Data were normalized by the percentage of answers. |
The most common treatment was performed at the nasolabial fold (31.8% of total treatments), followed by cheeks (14.6% of treatments), marionettes (9.6%), malar area (9.1%), lower third (7.6%), pre-jowl (7.1%), oral area (7.1%), middle third (6.1%), zygomatic area (3%), temporal area (2%), auricular area (1.5%) and chin (0.5%). In many cases, more areas were covered within the same treatment session.
Eight weeks after the first injection, most subjects rated the experience as satisfying (36.1%) or very satisfying (53.6%), with only 8.2% reporting a neutral impression and 2.1% a not-so-good one (Figure 3A). Early visible changes were reported by the majority: 38.8% noticed improved skin feel, 19.8% better elasticity, and 30.6% improved tone, while only 10.7% did not yet perceive differences (Figure 3B). Importantly, no patient intended to discontinue the treatment at this stage, with 83.5% resolute about continuing and 16.5% still undecided (Figure 3C). Effects were considerable on skin quality, wrinkle presence and nasolabial fold depth eight weeks after the second treatment (Figure 3D).
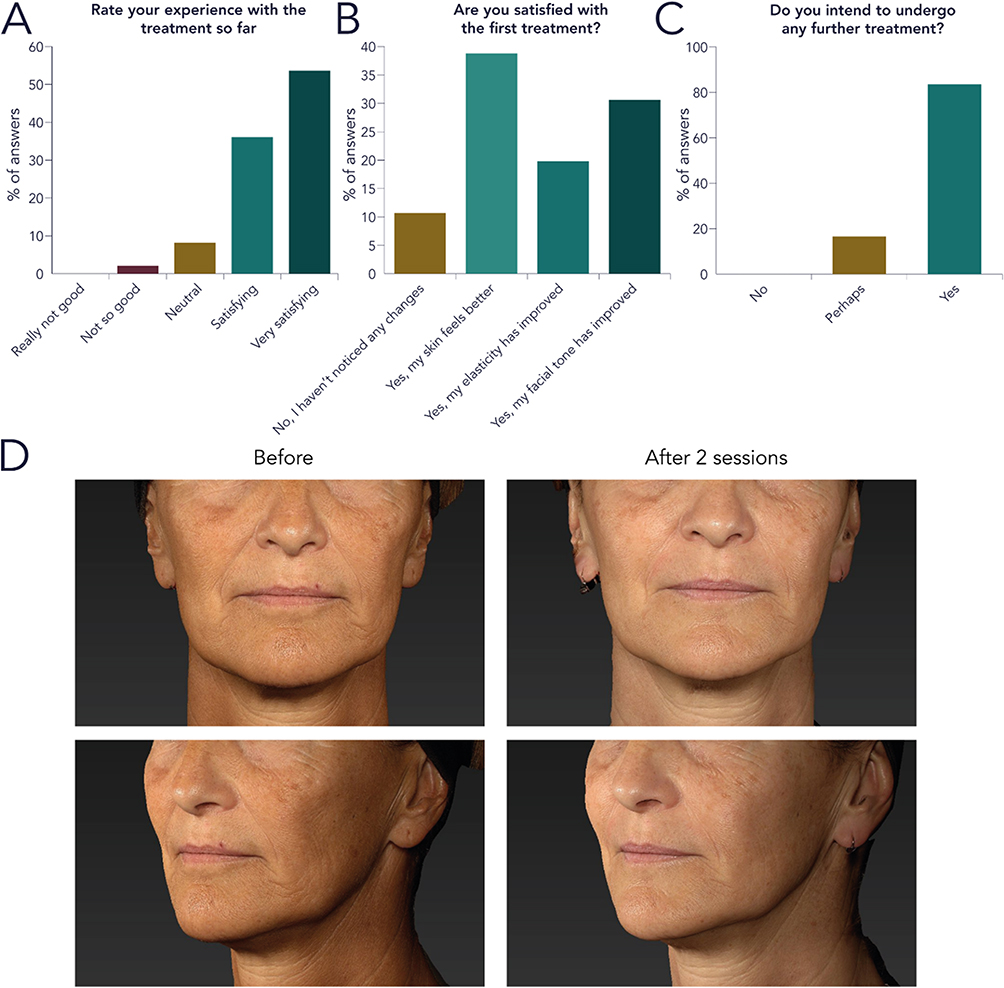 |
Figure 3 Subjects’ impression after the first treatment regarding experience, satisfaction and willingness to proceed (A–C). Data were normalized by the percentage of answers. Pictures of before and after treatment after two sessions (D). |
Treatment results showed a consistent quantitative improvement across sessions. After the first treatment, 59.6% of patients were rated as improved (Figure 4A). This proportion increased to 74.4% after the second session, with 20% assessed as “much improved” (Figure 4B). At the 6-month follow-up, all participants demonstrated objective improvement, with almost 85% rated as “improved” or better on GAIS (Figure 4C). A statistically significant shift in GAIS distribution was observed across timepoints (χ2-test, p < 0.001), with a significant trend toward improved outcomes after repeated treatment sessions and at 3-month follow-up. The proportion of responders (GAIS 1–2) increased from 1.1% to 37.0%, while patients reporting no improvement (GAIS 4) decreased from 38.3% to 0%. These findings confirm the progressive and sustained bio-regenerative effect of the treatment over time (Figure 4D). In particular, central compartments were replenished, contributing to an overall younger appearance (Figure 4E). Skin quality was assessed by VISIA software, indicating an overall improvement of texture and evenness (Figure 4F). Skin wrinkles were further analysed by Antera 3D camera, showing an improved skin texture after 6 months (Figure 4G). The treatment also led to less visible capillaries, improvement in photoaging and tissue re-densification, as assessed by a digital dermatoscope (Figure 4H).
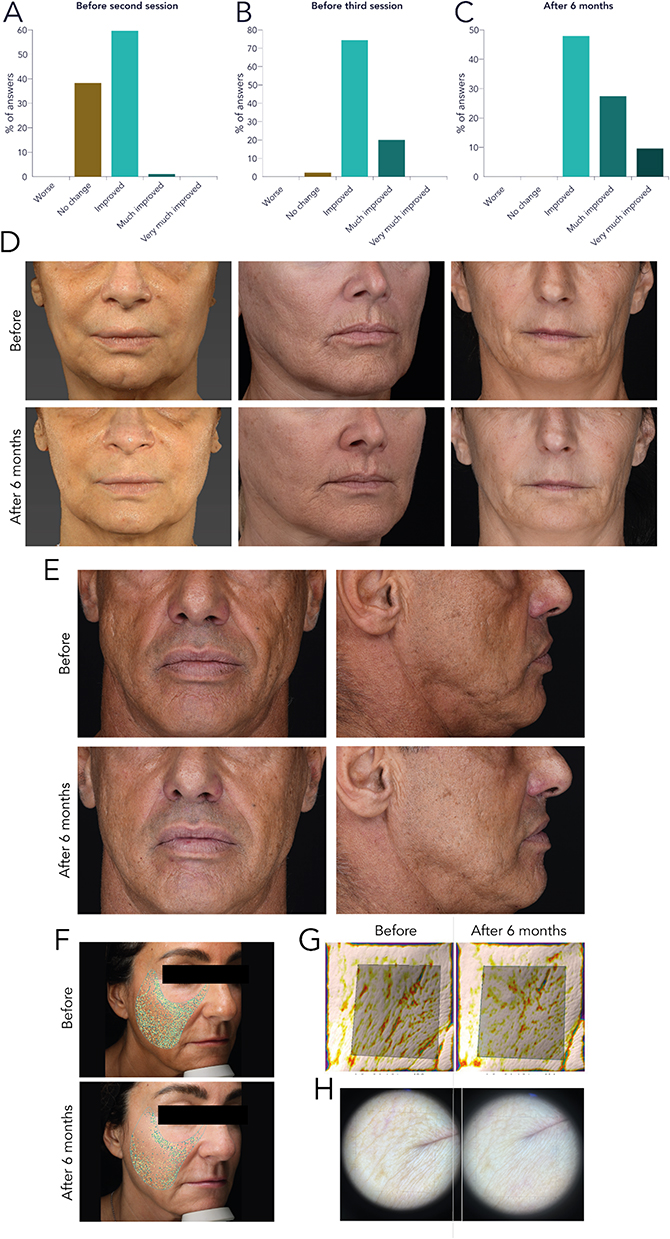 |
Figure 4 Physicians GAIS assessment after the first (A) second (B) and third session (C). Data were normalized by the percentage of answers. Pictures of the treatment effect before and after three sessions (D). Frontal and lateral view of the treatment effect on central compartments (E). Skin quality assessment with VISIA software (F) Antera 3D camera (G) and digital dermatoscope (H). |
Interestingly, the treatment with PLLA-LASYNPRO™ significantly enhances the skin’s elasticity, reducing laxity. These improvements are significantly visible during the pinch test (Figure 5A) and movement, such as smiling and lowering the chin (Figure 5B).
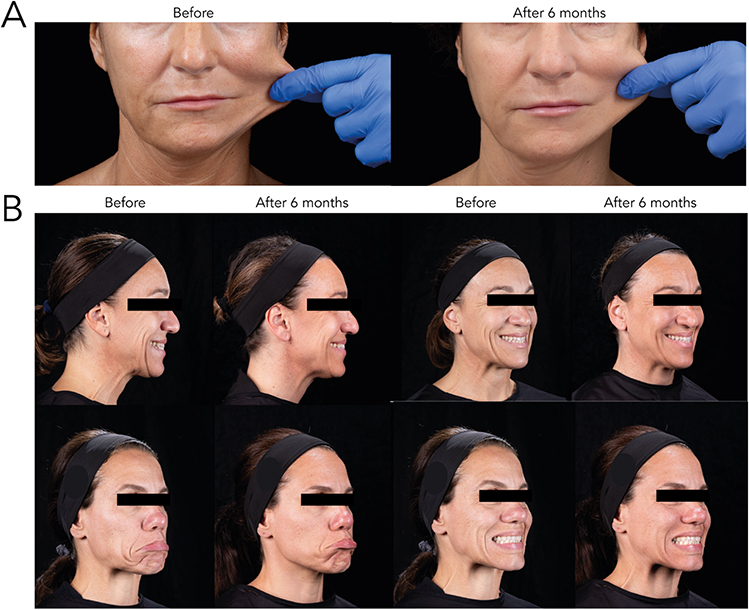 |
Figure 5 Before and after pictures showed improved skin elasticity at the 6-month follow-up. Pinch test (A) and results during exaggerated facial expressions (B). |
At the 6-month final follow-up, overall satisfaction remained high. Most respondents rated the experience as very good (64.3%) or good (30.4%), while 5.4% considered it “not good”, mainly due to limited visible results (Figure 6A). Nevertheless, all participants reported being at least quite satisfied with the outcome, with 35.7% very satisfied, 42.9% satisfied, and 21.4% quite satisfied (Figure 6B). When compared to other aesthetic treatments, 42.3% found PLLA-based injectable to provide better results and 19.2% significantly better, while 32.7% considered it comparable and only 5.8% found it less satisfactory (Figure 6C). Regarding retreatment, 21.4% would certainly repeat the procedure, 46.4% would probably repeat it, and 25% were still evaluating it, while 7.1% preferred other treatments (Figure 6D).
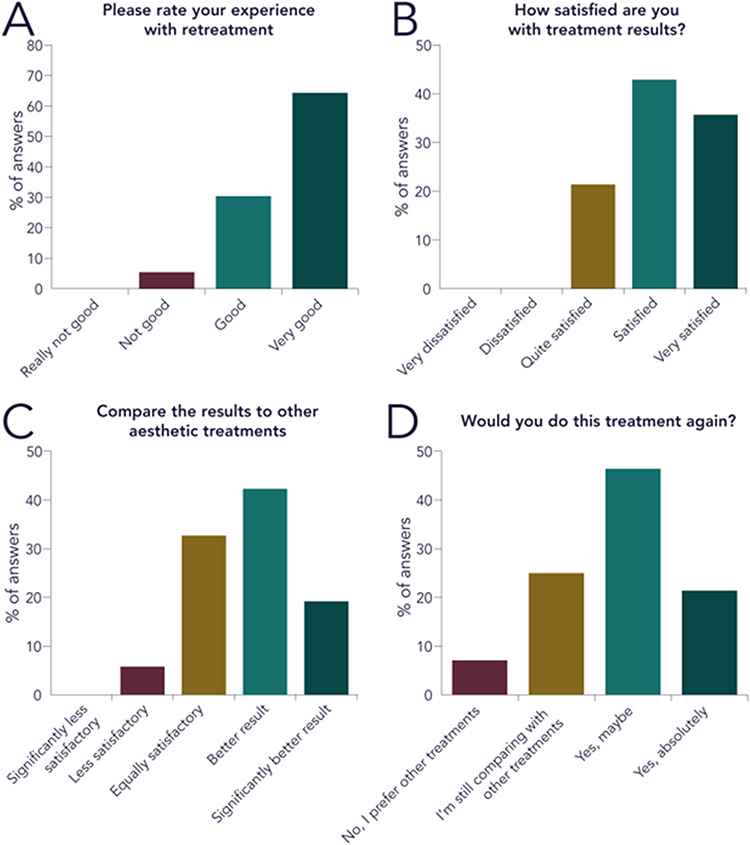 |
Figure 6 Final satisfaction survey from the subjects at the 6 months follow-up, assessing the overall experience (A), results (B), comparison to other aesthetic treatments (C) and willingness to repeat the procedure (D). Data were normalized by the percentage of answers. |
Subjects were asked to evaluate the level of pain and swelling after the first injection and after the last treatment. 30.9% of subjects reported to have experienced no pain during the first treatment, 38.1% experienced light pain, 29.9% moderate and 1% strong pain (Figure 7A). When asked if they experienced swollen face after treatment, 16.5% of respondents did not experience any swell. The rest of the participants did but for 41.2% it resolved after 1–2 days, for 34% after 2–3 days and for 8.2% after more than 5 days (Figure 7B). No adverse event was severe or lasted up to the subsequent follow-up. At the 6-month follow-up the percentage of subjects that did not experience any pain lowered to 16.7%, with 38.9% experiencing mild, 44.4% moderate and 1.9% intense pain over the past treatments (Figure 7C). The pain was not to be associated to the product itself, but rather to the treated area and to the physician’s handling.
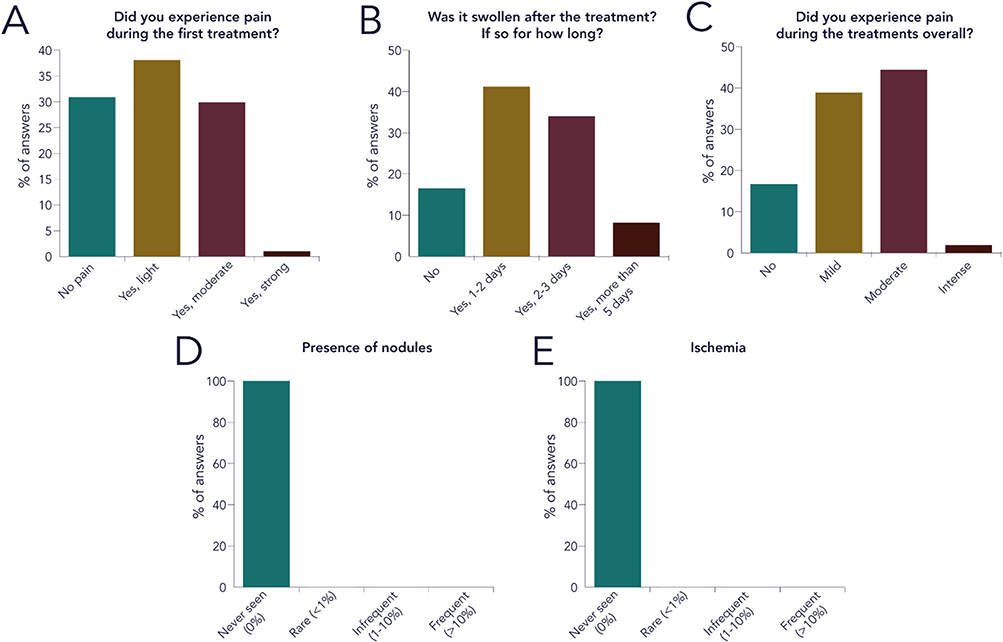 |
Figure 7 Adverse events (AEs) assessment by patients after the first session (A and B) and after the final treatment (C). Physician AEs assessment regarding the presence of nodules of ischemia at the 6-month follow-up (D and E). Data were normalized by the percentage of answers. |
Physicians reported visible AEs after the procedure (immediate AEs) and during the 6-month follow-up visit (late AEs). The immediate reactions can be associated with the technical procedure, with swelling (short duration, less than 2–3 days) being the most common. Most of patients did not show any sign of immediate AEs. At the 6-month follow-up visit physicians evaluated the presence of nodules or ischemia, common AEs associated with injectable fillers. No patient experiences either of them (Figure 7D and E).
Discussion
The results of this real-world study demonstrate that treatment with PLLA-based injectable is an effective and well-tolerated option for facial rejuvenation, offering progressive and natural improvements in skin quality, elasticity, and overall facial appearance. The physical and instrumental assessments consistently confirmed significant enhancement of dermal parameters, supporting the regenerative capacity of PLLA-based injectable Improvements were already evident after the first session, with nearly 60% of patients showing clinical enhancement, and continued to increase throughout the follow-up, reaching universal improvement after six months. Objective analyses using VISIA and Antera 3D technologies corroborated these findings, revealing improved skin texture, reduced wrinkle depth, and increased evenness. Although the findings indicate a strong effect of PLLA-based injectable on facial rejuvenation, some limiting factors must be taken into account. The study was designed as a post-market observational setup, therefore without the presence of a control group, limiting the possibility of a direct comparison. The number of participants that answered the survey was lower at every timepoint, resulting in less than half of the original number answering at the final follow-up evaluation. These limitations however are inevitable in the context of a post-market observational study, even though results are in line with previous PLLA injectables studies. These data in fact align with previous evidence on the use of PLLA-based injectable, where it was demonstrated its effect on fibroblast migration, ECM synthesis and ultimately skin remodelling both in vitro and ex vivo.20 A notable strength of PLLA-based injectable lies in its rapid reconstitution and ease of injection, which simplify the clinical procedure and enhance practitioner handling.18 The optimized carrier system ensures uniform microsphere dispersion, contributing to predictable outcomes and reduced risk of local complications. The streamlined preparation process represents a significant advancement over earlier PLLA formulations, which often required complex reconstitution protocols and longer waiting times before injection. These improvements facilitate treatment integration into routine aesthetic practice and increase physician compliance and patient throughput without compromising safety.
Patient-reported outcomes further confirmed the treatment’s effectiveness and acceptability. The majority of subjects perceived visible improvements in skin quality, elasticity, and firmness within eight weeks, with satisfaction scores increasing progressively over time. By the end of the study, 94.7% of respondents rated the treatment experience as “good” or “very good”, and more than two-thirds expressed willingness to repeat the treatment. These results reflect both the aesthetic efficacy and the high level of patient compliance and satisfaction, which are key factors in long-term treatment adoption and clinical success. The preference for natural and gradually evolving results expressed by participants aligns with the regenerative aesthetic paradigm, emphasizing subtle, authentic rejuvenation rather than abrupt volumetric correction.
The safety profile observed in this study was favourable, with no severe or long-lasting adverse events reported throughout the six-month follow-up. The most common reactions were mild to moderate swelling, resolving spontaneously within a few days and transient pain at the injection site. The pain was mostly linked to the site of the injected area and to the experience of the clinician performing the injection, suggesting a dependence on the site and operator rather than a role of the device itself. Importantly, no cases of nodules, papules, or ischemic events were observed, underscoring the high biocompatibility of the formulation and the benefit of improved particle dispersion within the carrier matrix. The absence of serious complications supports the rationale behind PLLA-based injectable formulation, designed to minimize inflammatory clustering and ensure controlled, homogeneous tissue integration of the PLLA microspheres.17,18,20 The lack of papules or nodules could be linked to the different action PLLA-based injectable exerts on regeneration. Conventional fillers rely on collagen deposition after a localized inflammatory response, therefore eliciting the body response with fibroblasts mobilization and collagen deposition. However, this pathway is often linked to the formation of nodules or papules in the injection areas, due to the inflammation reaction.23 The different neocollagenesis process promotes a gentler body response, avoiding unfavourable outcomes. Although it is expected, later follow-up reports are required to prove the absence of nodules and papules emergence. This property allows the use of The lack of papules or nodules could be linked to the different action PLLA-based injectable exerts on regeneration in novel delicate areas such as the perioral area, where PLLA formulations are extensively diluted or not normally used.
From a clinical perspective, these findings reinforce the concept that PLLA-based injectable acts not merely as a volumetric filler but as a regenerative stimulator, triggering biological remodelling processes that restore dermal architecture and functionality. The progressive nature of results and their maintenance over time attest to sustained collagen, elastin and other ECM components secretion activity and tissue renewal.20 These results align well with previous studies on collagen deposition and nasolabial folds improvement, where results were evaluated via cutaneous strain elastography and ultrasonographic assessment.21 However, more studies are required to fully assess the potential of this treatment. In any case, the product’s ease of preparation, favourable safety profile, and high patient satisfaction position it as a valuable regenerative injectable for facial rejuvenation.
Conclusions
In conclusion, PLLA-LASYNPRO™ demonstrated clinically meaningful, progressive, and long-lasting improvements in skin quality and facial appearance under real-world clinical conditions. The treatment was easy to prepare and inject, ensuring high physician usability and consistent delivery. No severe adverse events were observed, confirming an excellent safety and tolerability profile. Patient feedback indicated strong satisfaction and compliance, with most subjects reporting visible improvements and willingness to undergo repeated treatments. These findings support its use as an effective and reliable tool in regenerative aesthetics, bridging the gap between traditional fillers and biologically active skin rejuvenation therapies.
Data Sharing Statement
The authors confirm that no further data beyond those presented in the manuscript are available for sharing. All data supporting the findings of this study are fully presented within the manuscript.
Ethics Approval and Informed Consent
The data included in our manuscript derive from post-marketing clinical use of a CE-marked medical device, under routine clinical practice by qualified physicians. According to Article 74(1) of Regulation (EU) 2017/745 (MDR) and the Italian national guidance issued by the National Coordination Centre for Ethics Committees (22 August 2022), the collection of Post-marketing data within the normal conditions of use of a CE-marked device does not constitute a clinical investigation and therefore does not require prior approval by an Ethics Committee, as no additional invasive or burdensome procedures are performed. This study does not involve investigational products, off-label manipulation, or deviations from standard clinical care.
Consent for Publication
Written consent for publication was obtained from all patients whose clinical images were included in this manuscript. Patients signed a specific authorization allowing the use of their images for scientific publication purposes. Copies of the signed consent forms can be provided to the journal editorial office upon request.
Acknowledgments
Medical writing assistance was provided by Osmosia, medical writing and consultancy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Nordberg Medical provided financial support exclusively for manuscript submission and publication-related costs and had no role in the study design, data collection, data analysis, interpretation of results, or manuscript preparation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Farage MA, Miller KW, Elsner P, Maibach HI. Intrinsic and extrinsic factors in skin ageing: a review. Int J Cosmet Sci. 2008;30(2):87–13. doi:10.1111/j.1468-2494.2007.00415.x
2. Kohl E, Steinbauer J, Landthaler M, Szeimies R-M. Skin ageing. J Eur Acad Dermatol Venereol. 2011;25(8):873–884. doi:10.1111/j.1468-3083.2010.03963.x
3. Langton AK, Sherratt MJ, Griffiths CEM, Watson REB. Review article: a new wrinkle on old skin: the role of elastic fibres in skin ageing. Int J Cosmet Sci. 2010;32(5):330–339. doi:10.1111/j.1468-2494.2010.00574.x
4. Coleman SR, Grover R. The anatomy of the aging face: volume loss and changes in 3-dimensional topography. Aesthetic Surg J. 2006;26(1_Supplement):S4–9. doi:10.1016/j.asj.2005.09.012
5. Bravo B, Correia P, Euzébio Gonçalves Junior J, Sant’Anna B, Kerob D. Benefits of topical hyaluronic acid for skin quality and signs of skin aging: from literature review to clinical evidence. Dermatologic Therapy. 2022;35(12):e15903. doi:10.1111/dth.15903
6. Cui Y, Wang F, Voorhees JJ, Fisher GJ. Rejuvenation of aged human skin by injection of cross-linked hyaluronic acid. Plastic Reconstructive Surg. 2021;147(1S–2):43S. doi:10.1097/PRS.0000000000007620
7. Zarbafian M, Fabi SG, Dayan S, Goldie K. The emerging field of regenerative aesthetics—where we are now. Dermatologic Surg. 2022;48(1):101. doi:10.1097/DSS.0000000000003239
8. Goldie K. The evolving field of regenerative aesthetics. J Cosmet Dermatol. 2023;22(S1):1–7. doi:10.1111/jocd.15556
9. Mehta-Ambalal SR. Neocollagenesis and neoelastinogenesis: from the laboratory to the clinic. J Cutaneous Aesthetic Surg. 2016;9(3):145. doi:10.4103/0974-2077.191645
10. Haddad S, Galadari H, Patil A, Goldust M, Salam SA, Guida S. Evaluation of the biostimulatory effects and the level of neocollagenesis of dermal fillers: a review. Int J Dermatol. 2022;61(10):1284–1288. doi:10.1111/ijd.16229
11. Christen M-O. Collagen stimulators in body applications: a review focused on Poly-L-Lactic acid (PLLA). Clin Cosmet Invest Dermatol. 2022;15(June):997–1019. doi:10.2147/CCID.S359813
12. Zhu W, Dong C. Poly-L-Lactic acid increases collagen gene expression and synthesis in cultured dermal fibroblast (Hs68) through the TGF-β/Smad pathway. J Cosmet Dermatol. 2023;22(4):1213–1219. doi:10.1111/jocd.15571
13. Kim S-A, Kim H-S, Jung J-W, Suh S-I, Ryoo Y-W. Poly-L-Lactic acid increases collagen gene expression and synthesis in cultured dermal fibroblast (Hs68) through the P38 MAPK pathway. Ann Dermatol. 2019;31(1):97–100. doi:10.5021/ad.2019.31.1.97
14. Haykal D, Haddad A, Cartier H, Avelar L. Poly-L-Lactic acid in aesthetic dermatology: a decade beyond volume restoration toward regenerative biostimulation. Aesthetic Surg J. 2025;45(10):1065–1072. doi:10.1093/asj/sjaf121
15. Lowe NJ, Maxwell CA, Lowe P, Shah A, Patnaik R. Injectable Poly-l-Lactic acid: 3 years of aesthetic experience. Dermatologic Surg. 2009;35(s1):344–349. doi:10.1111/j.1524-4725.2008.01061.x
16. Janjua TA. Role of massage in preventing formation of papules and nodules after injecting Poly-L-Lactic acid. JAMA Facial Plastic Surg. 2014;16(6):457. doi:10.1001/jamafacial.2014.1173
17. Bertossi D, Cavallini M, Camporese A, et al. First insights on the upcoming role of next-generation PLLA-LASYNPRO in aesthetic and regenerative medicine: a survey of experts-the PLLA-LASYNPRO rationale. Facial Plast Surg. 2026. PMID: 41760129. doi:10.1055/a-2764-3062
18. Kubik P, Gruszczyński W, Filipowska M. Comparative analysis of reconstitution and solubility of two Poly-L-Lactic acid fillers for medical applications. Polymers. 2025;17(13):1778. doi:10.3390/polym17131778
19. Serrano-Coronado M, Rallo PC, Toral FR, Tirado CC, Ribé Subirà A, Páez Ruiz V. Clinical perspectives on the safety profile of Poly-L-Lactic Acid (Juläine): results from a national survey. J Cosmet Dermatol. 2025;24(9):e70439. doi:10.1111/jocd.70439
20. Geara J, Luo L, Parlak O, Sommar P, Landén NX. Poly-
21. Urdiales-Gálvez F, Benítez PA, Díaz I. Clinical outcomes of an innovative Poly-L-Lactic acid (LASYNPRO) in facial rejuvenation: prospective, multicenter Spanish study. J Cosmet Dermatol. 2026;25(2):e70753. doi:10.1111/jocd.70753
22. Gupta V, Sharma VK. Skin typing: fitzpatrick grading and others. Clin Dermatol. 2019;37(5):430–436. doi:10.1016/j.clindermatol.2019.07.010
23. Kleinfelder RE, Glick BP. Complications of non-hyaluronic fillers. Dermatological Rev. 2020;1:55–57. doi:10.1002/der2.26
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.