Back to Journals » International Medical Case Reports Journal » Volume 19
Post-Diphtheritic Myocarditis with Right Ventricular Thrombus: A Rare Cardiac Complication
Authors Mohamed HH ![]() , Adan HAA
, Adan HAA ![]() , Ahmed AH, Abdirahman AM
, Ahmed AH, Abdirahman AM ![]() , Shafici A
, Shafici A ![]()
Received 9 December 2025
Accepted for publication 27 June 2026
Published 9 July 2026 Volume 2026:19 580819
DOI https://doi.org/10.2147/IMCRJ.S580819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Hussein Hassan Mohamed,1 Hassan Adan Ali Adan,1 Abdiaziz Hussein Ahmed,1 Abdishakur Mohamed Abdirahman,1 Ahmed Shafici2
1Department of Emergency Medicine, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2Department of Cardiology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Hussein Hassan Mohamed, Department of Emergency Medicine, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia, Email [email protected]
Background: Myocarditis is a serious consequence of diphtheria; however, the occurrence of a subsequent right ventricular (RV) thrombus is exceedingly rare. We provide an uncommon case of post-diphtheritic myocarditis complicated by a right ventricular thrombus and secondary pneumonia, emphasizing its effective multi-modal therapy and subsequent recovery.
Case Presentation: A 19-year-old female arrived at our emergency department with acute dyspnea and chest pain two weeks after a 3-day hospitalization for pharyngeal diphtheria at Galkacyo Regional Hospital. Laboratory analyses revealed increased Troponin I (2615 ng/L), CK (511 U/L), and severely high NT-proBNP (33,349.0 pg/mL). Chest radiography verified the presence of simultaneous right lower lobe pneumonia. Electrocardiography revealed low-voltage QRS complexes, whereas echocardiogram indicated worldwide hypokinesia (LVEF 40– 45%) and a movable hypoechoic mass at the right ventricular apex, strongly suggesting the presence of a right ventricular thrombus.
Management and Outcome: The patient was admitted to a designated ICU bed and commenced on broad-spectrum antibiotics, guideline-recommended heart failure pharmacotherapy (metoprolol, furosemide, empagliflozin), and therapeutic anticoagulation with subcutaneous enoxaparin. She was released on a two-month regimen of oral anticoagulation. Five-month serial follow-up demonstrated total clearance of the right ventricular thrombus, a fully normalized ejection fraction, and complete remission of all symptoms.
Conclusion: This case demonstrates that patients continue to be susceptible to toxin-induced myocarditis and intracardiac thrombosis even in the convalescent phase. It highlights Virchow’s Triad in post-diphtheritic conditions and illustrates that timely heart failure treatment, along with a systematic 2-month anticoagulation protocol, can result in remarkable myocardial healing and total thrombus clearance.
Keywords: diphtheria, myocarditis, right ventricular thrombus, cardiac complication
Introduction
Acute infectious diphtheria is transmitted by Corynebacterium diphtheriae, a bacterium that generates a potent exotoxin that can inflict harm on numerous organ systems.1 The exotoxin primarily targets peripheral nerves and myocardial tissue by inhibiting cellular protein synthesis. It specifically destroys Schwann cells, resulting in segmentary demyelination and subsequent polyneuropathy. In Somalia and other regions with low vaccination coverage, randomized cases and isolated epidemics persist, despite extensive worldwide vaccination campaigns.2 Rapid administration of diphtheria antitoxin (DAT) is essential to neutralize circulating toxin prior to cell entrance, as the exotoxin binds irreversibly to tissue receptors. Nevertheless, the timely acquisition of DAT continues to be a significant challenge in resource-limited environments as a result of global supply shortages and distribution challenges. Myocarditis is a systemic complication that is both frequent and lethal, affecting up to 25% of patients and substantially increasing the risk of mortality. Myocarditis, which frequently results in heart failure, life-threatening arrhythmias, and aberrant cardiac conduction, typically manifests two to three weeks following the initial infection. This condition is caused by direct myocardial injury from the diphtheritic toxin.3 The development of right ventricular (RV) thrombus is an extremely rare and uncommon complication, although left ventricular dysfunction is a pervasive and anticipated consequence of this toxin. This case, which pertains to a 19-year-old Somali woman, contributes substantial value to the current body of literature by documenting this uncommon clinical finding and emphasizing its clinical significance in contemporary medical practice.
Presentation of the Case
A 19-year-old female presented to the Emergency Department of the Mogadishu Somali–Turkish Training and Research Hospital with deteriorating dyspnea and central chest discomfort. It is important to mention that she was diagnosed with pharyngeal diphtheria two weeks anterior to this presentation and was admitted to Galkacyo Regional Hospital for three days of acute management. She was transferred to our facility for advanced cardiac assessment and diagnostic evaluation after experiencing progressive shortness of breath and bilateral lower limb edema following her initial discharge. Upon her arrival at our Emergency Department, her vital signs were as follows: a pulse of 88 beats per minute, a blood pressure of 98/60 mmHg, a temperature of 36.7°C, an oxygen saturation of 95% on room air, and a random blood sugar of 99 mg/dL. A profound hypoxemia accompanied by mild metabolic alkalosis was indicated by an elevated pH of 7.47, PCO2 of 45.2 mmHg, PO2 of 38 mmHg, and HCO3 of 33 mmol/L in the arterial blood gas analysis. A white blood cell count of 4.83x109/L and a normal international normalized ratio (INR) were observed during laboratory investigations. Nevertheless, the patient exhibited significant biomarkers of myocardial injury and hemodynamic stress, such as a 33 U/L aspartate aminotransferase (AST), a 511 U/L creatine kinase (CK), a 2615 ng/L troponin I level, and a 33,349.0 pg/mL N-terminal pro-B-type natriuretic peptide (NT-proBNP) level. Chest radiography (Figure 1) demonstrated a minor pleural effusion and heightened density in the right lower lobe, concurrent with a blunting of the costophrenic angle, which is indicative of right lower lobe pneumonia. Multimodal diagnostic imaging was promptly initiated. In the limb leads, electrocardiography (Figure 2) revealed low-voltage QRS complexes, normal sinus rhythm, and nonspecific ST–T wave alterations, which are indicative of diffuse myocardial inflammation. The left ventricular dimensions were normal, but the ejection fraction was reduced to 40–45%, and there was diffuse global hypokinesia, as demonstrated by transthoracic echocardiography (Figures 3–8). A mobile, hypoechogenic mass affixed to the apical region was observed, raising strong diagnostic suspicion of an intracardiac thrombus or a cardiac blood cyst, despite the fact that the right ventricle was normal in size. The pericardium was normal, the heart valves and septa were intact, and the estimated pulmonary artery systolic pressure was 20 mmHg. The patient was diagnosed with post-diphtheritic myocarditis that was exacerbated by a secondary right ventricular thrombus and concurrent secondary pneumonia, as determined by the clinical history, laboratory findings, and imaging.
 |
Figure 1 The chest X-ray showed that the right lower lobe was consolidated and that there was a little pleural effusion. |
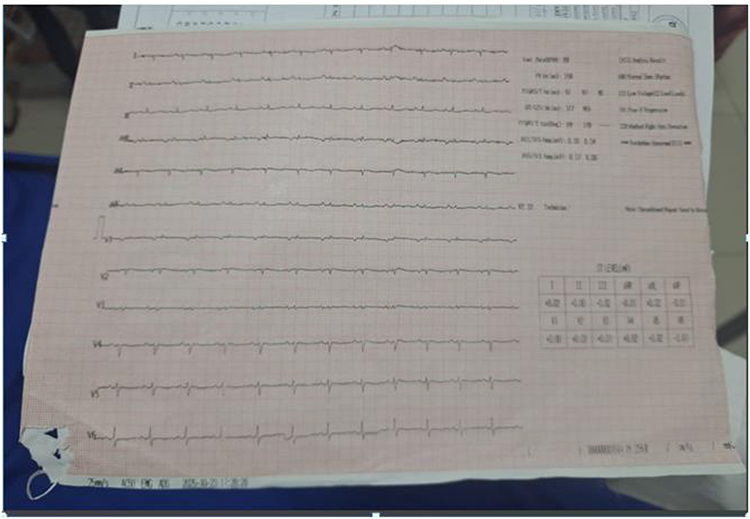 |
Figure 2 The ECG showed sinus rhythm with nonspecific ST-T alterations and low-voltage complexes. |
 |
Figure 3 Assessment of right ventricular outflow tract (RVOT) and tricuspid valve view. |
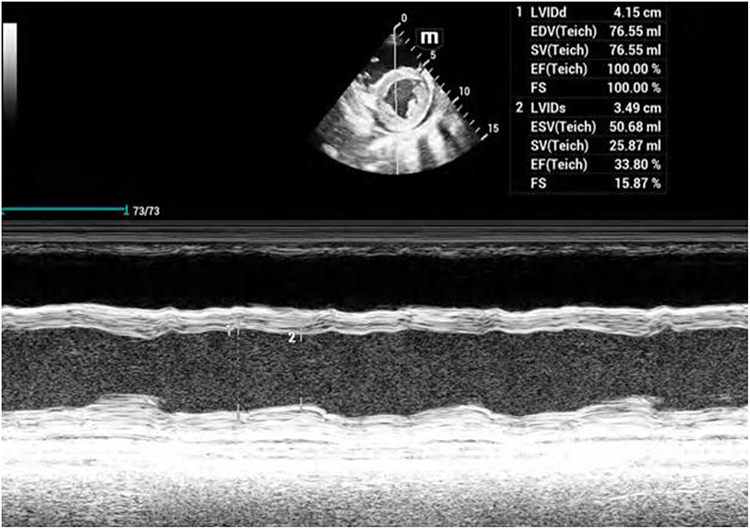 |
Figure 4 M-mode ECHO graph of the left ventricle as a parasternal short-axis view. |
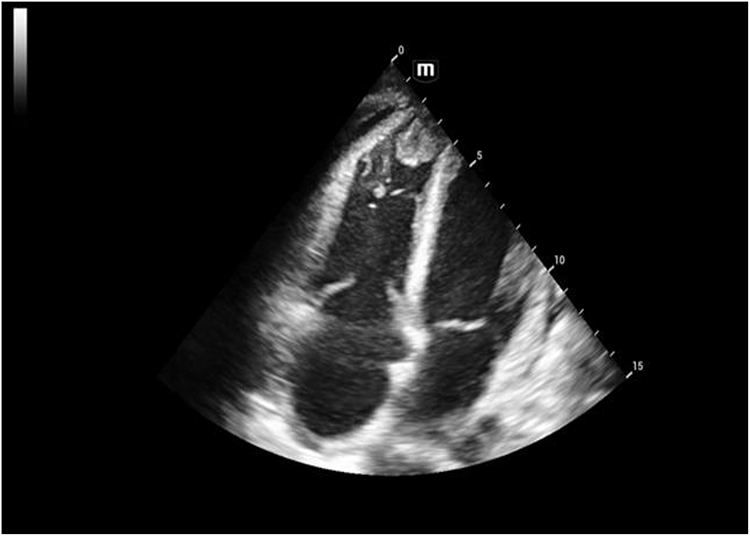 |
Figure 5 Apical four-chamber view echocardiography with right apex thrombus. |
 |
Figure 6 The apical one-chamber view shows a right ventricular thrombus at the apex. |
 |
Figure 7 The two-chamber view shows a right ventricular thrombus at the apex. |
 |
Figure 8 Apical four-chamber view echocardiography with right apex thrombus by measurement. |
Subsequently, the patient was confined to an isolated bed in the Intensive Care Unit (ICU) for specialized care and continuous cardiac monitoring. A therapeutic regimen of oral Metoprolol succinate (Beloc) 25 mg once daily (titrated according to blood pressure thresholds), intravenous Furosemide (Lasix) 40 mg three times daily for fluid optimization, oral Empagliflozin (Jardiance) 10 mg once daily (adjusted according to hemodynamic tolerance), and therapeutic anticoagulation with subcutaneous Enoxaparin (Clexane) 0.6 mL twice daily was initiated in conjunction with broad-spectrum antibiotic coverage for pneumonia. Despite the initial recommendation for a CT thorax angiography on the first day to further characterize the mobile right ventricular apical mass, it was ultimately not performed due to the patient’s acute clinical status and the high pre-test probability of an RV thrombus in the setting of acute post-diphtheritic myocarditis. The patient was safely discharged after clinical stabilization and the resolution of the acute respiratory symptoms. They were treated with a planned 2-month course of oral anticoagulation therapy and optimized guideline-directed medical therapy for heart failure. The patient’s recovery was exceptional, as evidenced by the complete resolution of lower limb edema, chest pain, and dyspnea during serial clinical and echocardiographic follow-up at 5 months post-discharge. The patient was entirely asymptomatic. The complete disappearance of the right ventricular apical thrombus was confirmed by repeated transthoracic echocardiography, and her left ventricular ejection fraction had considerably improved to normal limits. These findings indicate a favorable midterm prognosis and excellent myocardial recovery.
Discussion
Myocarditis affects approximately 10–25% of patients, making it a significant systemic complication of diphtheria and accounting for nearly half of all related fatalities. The diphtheritic exotoxin is responsible for the pathophysiology, as it impedes protein synthesis within myocardial cells, resulting in tissue necrosis and conduction disturbances, including heart block.4 Clinical cardiac symptoms typically manifest within 1–2 weeks of infection and seem to be directly correlated with the total toxic burden in the body. Echocardiography frequently reveals global hypokinesia and a substantially reduced ejection fraction, while electrocardiogram (ECG) findings frequently manifest as low-voltage QRS complexes and nonspecific ST–T wave alterations;5 these findings are diagnostic. In the case of our patient, who experienced progressive dyspnea and lower limb edema after an initial three-day stay at Galkacyo Regional Hospital, the pervasive hypokinesia and ejection fraction of 40–45% were definitive indicators of toxin-mediated myocardial injury. The novel and most remarkable aspect of this case is the development of a right ventricular (RV) thrombus, which significantly contributes to the existing literature. Although diphtheritic myocarditis is frequently associated with left ventricular dysfunction and heart failure, the occurrence of an intracardiac thrombosis in the right ventricle is exceedingly uncommon. Virchow’s Triad provides a comprehensive explanation for this complication, which is the result of a precise combination of factors. These factors include direct endocardial and endothelial injury caused by the circulating cytotoxic exotoxin, profound intraventricular blood stasis resulting from severe global ventricular dysfunction, and a systemic hypercoagulable state induced by concurrent diphtheria and secondary pneumonia.6 The presence of a mobile, hypoechogenic 1.2×1.4 cm mass in the RV apex presents a critically high risk for life-threatening pulmonary embolism, necessitating immediate and aggressive therapeutic anticoagulation in conjunction with optimized guideline-directed medical therapy (GDMT) for heart failure. In order to resolve this issue, the patient was administered a comprehensive regimen that included metoprolol succinate (Beloc), intravenous furosemide (Lasix), and empagliflozin (Jardiance) in an isolated ICU bed. Initially, subcutaneous enoxaparin (Clexane) 0.6 mL twice daily was administered to accomplish rapid, predictable anticoagulation. This was followed by a planned 2-month course of oral anticoagulation upon discharge. Despite the initial recommendation for a cardiac CT thorax angiography to exclude rare differentials such as a cardiac blood cyst, it was ultimately omitted due to the patient’s acute clinical fragility and the overwhelmingly high pre-test probability of an RV thrombus. Although differential diagnoses such as viral, toxic, or idiopathic dilated cardiomyopathy were taken into account, the evident temporal correlation with pharyngeal diphtheria and the significantly elevated troponin I levels (2615 ng/L) strongly suggest a diphtheritic origin. Ultimately, the selection of a 2-month anticoagulation window was highly successful. At the 5-month follow-up, the patient exhibited exceptional recovery, with complete resolution of the thrombus, normalized ejection fraction, and complete remission of all heart failure symptoms. This outcome demonstrates that the prognosis of this rare condition is significantly altered by prompt, targeted intensive supportive care.
Limitation
The absence of advanced cardiovascular imaging, specifically Cardiac Magnetic Resonance Imaging (CMR) and Cardiac Computed Tomography (CT) angiography, is a significant limitation of this case report. This restriction hinders our capacity to non-invasively characterize myocardial tissue and definitively differentiate the right ventricular mass from rare etiologies such as a cardiac blood cyst. Furthermore, although our 5-month follow-up study effectively demonstrated complete thrombus resolution and substantial myocardial recovery, our results are limited by the absence of long-term, multi-year tracking to assess the possibility of late-onset conduction disturbances or recurrence. Lastly, these observations are an isolated case report that pertains to a singular clinical scenario that was managed within a particular healthcare setting. Consequently, they cannot be broadly generalized to much larger patient populations.
Conclusion
The present case highlights the necessity of cardiac monitoring in diphtheria patients, even post apparent recovery. In places like Somalia, where not everyone is fully vaccinated, doctors should keep an eye out for heart problems. Early echocardiography and cardiac biomarker assessment can identify myocarditis and avert life-threatening occurrences, such as the formation of intracardiac thrombus.
Ethics Approval and Consent to Participate
The Ethics Committee of Mogadishu Somali Türkiye Training and Research Hospital in Mogadishu, Somalia, looked over and approved this case report. The committee does not provide case reports, formal approval, or reference numbers; hence, there is no ethics approval number. The study adhered to both the Declaration of Helsinki’s rules and the institutional ethical standards.
Consent for Publication
The patient has provided written consent for the public release of the case data and images. All personal information and other information that could give away the patient’s identity have been taken out to preserve their privacy.
Author Contributions
All authors made significant contributions to the reported work, including the conception, study design, execution, data acquisition, analysis, and interpretation; participated in drafting, revising, or critically reviewing the article; gave final approval for the version to be published; agreed on the journal to which the article has been submitted; and accepted accountability for all aspects of the work.
Funding
We declare that we have not received any financial support.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Ilyas S, Khan I, Yousafzai ZA, Kamran Amin Q, Rahman Z, Bilal M. Diphtheria-associated myocarditis: clinical profiles and mortality trends in a tertiary care hospital in Pakistan. Cureus. 2024;16(3):e56744. PMID: 38650814; PMCID: PMC11033218. doi:10.7759/cureus.56744
2. Jean Simon D, Kondo Tokpovi VC, Dianou K, et al. Regional, subregional, and country-level full vaccination coverage in children aged 12–23 months for 34 countries in sub-Saharan Africa: a global analysis using demographic and health survey data. BMJ Glob Health. 2025;10(3):e018333. PMID: 40090697; PMCID: PMC11911682. doi:10.1136/bmjgh-2024-018333
3. Singh S, Gupta N, Saple P. Diphtheritic myocarditis: a case series and review of literature. J Fam Med Prim Care. 2020;9(11):5769–8. PMID: 33532430; PMCID: PMC7842443. doi:10.4103/jfmpc.jfmpc_1396_20
4. Collier RJ. Effect of diphtheria toxin on protein synthesis: inactivation of one of the transfer factors. J Mol Biol. 1967;25(1):83–98. PMID: 4291872. doi:10.1016/0022-2836(67)90280-x
5. Kole AK, Roy R, Kar SS. Cardiac involvement in diphtheria: a study from a tertiary referral infectious disease hospital. Ann Trop Med Public Health. 2012;5(4):302. doi:10.4103/1755-6783.102031
6. Jiang XJ, Zhang WY. Myocarditis complicated by massive right ventricular thrombus and extensive pulmonary embolism: a case report. Front Surg. 2022;9:924366. PMID: 36051705; PMCID: PMC9424664. doi:10.3389/fsurg.2022.924366
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.