Back to Journals » International Medical Case Reports Journal » Volume 18
Porto Sinusoidal Vascular Disorder: A Case Report
Authors Abdullahi NM ![]() , Ahmed MA, Yusuf MA, Warsame HA
, Ahmed MA, Yusuf MA, Warsame HA ![]()
Received 1 November 2024
Accepted for publication 25 February 2025
Published 1 March 2025 Volume 2025:18 Pages 289—293
DOI https://doi.org/10.2147/IMCRJ.S502206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Naima Mukhtar Abdullahi,1,* Mohammed AM Ahmed,1 Mohamed Abdulahi Yusuf,2,3 Hawa Ali Warsame4,*
1Department of Medicine, Faculty of Medicine and Surgery, Mogadishu University, Mogadishu, Somalia; 2Department of Internal Medicine and Gastroenterology, Alami Specialist Hospital, Mogadishu, Somalia; 3Department of Internal Medicine, Somali National University, Mogadishu, Somalia; 4Department of Medicine, Faculty of Medicine and Surgery, Salaam University, Mogadishu, Somalia
*These authors contributed equally to this work
Correspondence: Naima Mukhtar Abdullahi; Hawa Ali Warsame, Email [email protected]; [email protected]
Background: Porto sinusoidal vascular disease (PSVD) is an unusual vascular disorder defined by raised portal venous pressure without cirrhosis or other common causes of liver pathology. The disease pathogenicity is not well understood.
Case Report: We report a rare case of Porto Sinusoidal Vascular Disorder (PSVD). This patient presented with hematemesis and melena several times, despite having no prior history of chronic disease. An endoscopic evaluation revealed 4 cords of oesophageal varices. The exact cause of portal hypertension was not identified despite the patient undergoing MRI, liver biopsy, abdominal and hepatic sonography, and other required laboratory tests. This patient was performed band ligation and received beta blockers, proton pump inhibitors and whole blood transfusion.
Conclusion: This case highlights the complexity of the diagnosing and managing of PSVD. Despite the patient receiving symptomatic treatment, he still has pancytopenia due to splenomegaly and needs close monitoring and flow-up.
Keywords: porto sinusoidal vascular disease, idiopathic non-cirrhotic portal hypertension, splenomegaly, pancytopenia, trans-jugular intrahepatic portosystemic shunt
Introduction
Porto sinusoidal Vascular Disorder (PSVD) previously known as Idiopathic non-cirrhotic portal hypertension (INCPH) is a vascular condition characterized by increased blood pressure in the portal vein system without the presence of cirrhosis. The exact cause of PSDV is not yet fully known. Many theories on the development of PSDV have been proposed, signifying limited understanding of the disease process. The aetiology of PSVD is unidentified; however, there are theories related to the disease that can be classified into five categories: long term exposure to toxins and drugs, immunological disorders, chronic infections, clotting issues and hereditary disorders.
This case involved a patient who presented with the sudden onset of hematemesis (vomiting blood) and melena (black, tarry stool), despite having no known prior history of chronic disease. After ruling out all other potential causes, he was diagnosed with Porto Sinusoidal Vascular Disorder (PSVD). The patient was managed with band ligation, beta-blockers, proton pump inhibitors, and blood transfusion. Although he remains stable, he continues to have pancytopenia due to moderate splenomegaly.
Case Presentation
A 28-year-old Somalian male patient presented with hematemesis (vomiting of blood) and melena (black, tarry stool) in October 2023. The patient has no related past medical history. Endoscopic evaluation revealed 4 cords of oesophageal varices. Abdominal sonography and hepatic duplex assessment showed a normal liver size with a coarse parenchymal texture, fine periportal fibrosis, and multiple scattered, well-defined hypoechoic focal lesions, the largest measuring about 17.7 × 16.5mm. The spleen was enlarged, measuring about 16.3cm. Initial management included band ligation for a torn cord observed during endoscopy, terlipressin Injection 1 mg, propranolol tab 40mg and blood transfusion due to pancytopenia.
During the investigation of the illness, a stool test was performed to rule out schistosomiasis as a potential cause of portal hypertension. The stool analysis had a negative result. Schistosomiasis is endemic in Somalia, Sudan, Yemen, and Egypt, and more people in those nations require chemotherapy to prevent the disease.
Further evaluation with high-field MRI showed chronic parenchymal liver changes, with the right hepatic lobe not exceeding 10cm and preferential enlargement of the lobe. The posterior aspect of the right hepatic lobe (segments 7–8) showed faint bright signal on T1 pre-contrast images, with corresponding faint heterogeneous enhancement in the early phases of the dynamic study, but without definite delayed washout or restricted diffusion. The left hepatic lobe segment 2 had two adjacent subcapsular, well-defined lesions, the largest measuring 6.5mm, showing faint bright signal on T2 without significant diffusion restriction. On dynamic post-contrast images, these nodules demonstrated corresponding enhancement throughout the dynamic study with no related washout (Figure 1). Liver biopsy was performed, and microscopic examination of the prepared slides revealed intact architecture. The slides showed 10 enclosed portal areas with mild expansion due to fibrosis, without any inflammatory infiltrate, plasma cells, or interface hepatitis. The parenchyma showed one-cell-thick plates without focal necrosis or parenchymal rosetting. There was no evidence of steatosis, cholestasis, or hemosiderosis, and no PAS-D globules or other storage material was detected. Additionally, no granulomas were found (not seen).
 |
Figure 1 High-field MRI, the right hepatic lobe is less than 10 cm in size, indicating chronic liver parenchymal abnormalities. There is no delayed washout or restricted diffusion in the posterior region of the right lobe (segments 7–8), which shows a weak bright signal on T1-weighted pre-contrast images and faint heterogeneous enhancement in the early dynamic phases. There are two contiguous subcapsular lesions in the left hepatic lobe (segment 2), the largest of which is 6.5 mm in size. On T2-weighted pictures, these lesions exhibit a weak, bright signal that gets stronger throughout the course of the dynamic study without showing any signs of washout. |
Laboratory examinations revealed normal liver function tests, including AST, ALT, bilirubin, serum albumin, and alkaline phosphatase immunological investigations including alpha-fetoprotein (AFP), HCV antibody, HBS antigen, anti-mitochondrial antibody (AMA), and anti-smooth muscle (ASMA), were mostly negative, except for a weak positive result of ASMA and a weak positive of speckled antinuclear antibody pattern (ANA). The complete blood count showed anaemia, leukopenia, and thrombocytopenia. The coagulation profile, including prothrombin time (PT) and INR, were normal.
The patient received elective management during his course of illness (Table 1), and doctors recommended regular follow-up.
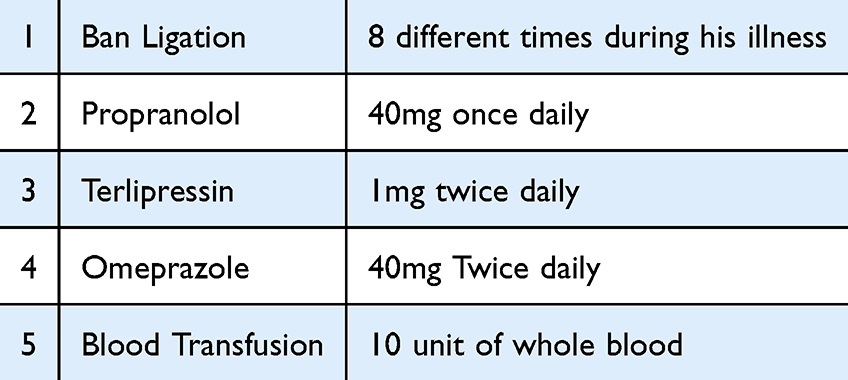 |
Table 1 Management of the Patient Summarized Table |
Above the pathological test and excluded all possibility of portal hypertension in the patient diagnosed with PSVD.
Discussion
This case involves a young male who presented with hematemesis and melena at different times, without any relevant past medical history or chronic illness. Initial endoscopy revealed four cords of oesophageal varices, along with slight splenomegaly and pancytopenia.
PSVD is a rare disease characterized of intrahepatic portal hypertension in the absence of cirrhosis or other causes of liver disease and splanchnic venous thrombosis.
The aetiology of PSVD is unknown; however, many theories on the development of PSVD have been proposed, signifying limited understanding of the disease process. Theoretically, the aetiology of PSVD can be divided in five categories: chronic infections, exposure to medication or toxins, genetic disorders, thrombophilia, and immunological disorders. Multifactorial aetiology can also be encountered.
Differentiating between schistosomiasis and porto-sinusoidal vascular disease (PSVD) is essential due to their overlapping clinical features, particularly in regions where schistosomiasis is prevalent (Table 2).
 |
Table 2 Comparison Between Schistosomiasis and Porto Sinusoidal Vascular Diseases |
Schistosoma species are the parasites that cause schistosomiasis. Hepatosplenic schistosomiasis, which is typified by portal hypertension and periportal fibrosis, can result from a persistent infection. Patients may exhibit maintained liver function, esophageal varices, and splenomegaly. Periportal fibrosis is frequently seen in imaging examinations without notable liver parenchymal abnormalities. According to histopathological analysis, schistosome eggs are deposited in the portal veins, causing granulomatous inflammation and fibrosis.1
Schistosoma infection is traditionally confirmed by the presence of parasite eggs in tissue, urine, or faeces. However, ova found by parasitological testing and biopsy frequently do not show active infection in the case of Schistosoma liver disease. Coming from sub-Saharan Africa, it has potential susceptibility of one of the causes is schistosomiasis, although he had stool test which back negatively;2 however, one of the main causes of portal hypertension PH is schistosomiasis, a neglected tropical illness that is common in low-to-middle-income nations. The disease affects over 290 million people globally, primarily in areas with poor sanitation, where contact with contaminated freshwater promotes transmission. People who live in poverty and lack proper sanitation are more likely to come into touch with unprotected natural freshwater sources, which is where the disease is spread.3
Like this patient, the most common presenting sign of Porto sinusoidal vascular diseases (PSVD) is gastric or oesophageal variceal bleeding with preserved liver function.4 The patient in this case exhibited splenomegaly without any evidence of liver cirrhosis or liver pathology. Splenomegaly can be the primary clinical manifestation of INCPH.5 Our patient’s clinical manifestations included splenomegaly and pancytopenia, while liver function remained normal.
The primary complication of the disease is gastrointestinal bleeding due to the rupture of esophago-gastric varices.6 In this patient, esophago-gastric varices were the initial sign of the illness, and this sequence continued subsequently.
The primary goals in treating acute variceal bleeding are to control the bleeding, prevent early rebleeding, and manage complications, especially infections. Combining endoscopic techniques (band ligation or sclerotherapy) with vasoactive drugs can control bleeding in up to 90% of patients. Antibiotic prophylaxis should be started as soon as possible.7,8
There are currently no medications tailored to PSVD that can stop the disease’s progression. Rather, it is advisable to think about treating related systemic illnesses or stopping esophago-gastric varices.9 In this patient, esophago-gastric varices were the initial sign of the illness medications that lead to PSVD. Treating portal hypertension-related problems in patients with PSVD and indicators of the condition is currently advised; this recommendation is taken from the guidelines for patients with cirrhosis.9 Porto sinusoidal vascular disorder Patients with oesophageal varices are treated according to guidelines for cirrhosis, which includes primary prophylaxis with non-selective b-blockers (NSBB) and variceal ligation in case of intolerance or contraindication to NSBB. Trans-jugular intrahepatic portosystemic shunt has shown equally good results as in cirrhotic patients. Indications for liver transplantation are the same as in cirrhosis.10 Similarly, the management for ascites and hepatic encephalopathy is identical to those in cirrhotic patients.11
Non-selective beta-blockers and band ligation are equally effective in preventing the first bleeding episode, with rubber band ligation preferred for patients who cannot tolerate beta-blockers.7,8, During the first episode of this patient’s illness, along with band ligation, he was also treated with a non-selective β-adrenergic antagonist and Terlipressin injection to control the bleeding episodes from oesophageal varices.
Ligated-site ulcers are often small and go away on their own in a month. According to research, patients who received a PPI following elective EVL saw significantly fewer post-banding ulcers on follow-up endoscopies than those who did not receive (owner). The possibility that PPIs could reduce the risk of bleeding following EVL has been investigated in several trials. The use demonstrated that using PPIs before EVL decreases the likelihood that the varices would come loose early, speeds up the healing process, and minimises the size of the ulcer by halting acid production.12
The patient was prescribed a proton pump inhibitor (PPI) for suspected gastritis and peptic ulcer disease prior to the confirmation of his diagnosis. PPIs were also given to help with the healing process following endoscopic variceal band ligation.
A trans-jugular intrahepatic portosystemic shunt (TIPS) is a valid option for patients with uncontrolled variceal bleeding despite medical and endoscopic treatment.13
Our patient has mild splenomegaly and pancytopenia. Therefore, his doctors recommend close follow-up and considering TIPS as a prophylactic measure or in case of relapse.
Patients with severe hypersplenism may consider splenectomy or partial splenic embolization. These interventions have been shown to increase platelet counts; however, their advantages have never been shown to exceed their hazards. Thus, these interventions should be reserved for rare patients with intractable symptoms associated with hypersplenism, such as repeated splenic infarcts or spontaneous bleeding events.9
In this case, the patient is presently under ongoing medical monitoring. Presenting with significant pancytopenia and splenomegaly, the possibility of a splenectomy as a future therapeutic intervention may be explored in the event of severe hypersplenism or spontaneous bleeding episodes refractory to medical therapy, which is fatal.
Ethical Approval and Informed Consent
Institutional approval is not necessary for publication; therefore, informed written consent was obtained from the patient for using their information and publishing the case report, provided that identifying data remains anonymous.
Funding
The authors have not declared any specific grants for this research from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Nakhleh RE. The Pathological Differential Diagnosis of Portal Hypertension. Clinical Liver Disease. 2017;10(3):57–62. doi:10.1002/cld.655
2. EMRO.WHO. EMRO.WHO, 2023. Available from: http://www.emro.who.int/.
3. Veiga ZST, Fernandes FF, Guimarães L, Piedade J, Pereira GHS. Natural History of Hepatosplenic Schistosomiasis (HSS) Non–Cirrhotic Portal Hypertension (NCPH): influence of Gastrointestinal Bleeding and Decompensation in Prognosis. Trop Med Infect Dis. 2023;8(3):145. doi:10.3390/tropicalmed8030145
4. Feiz VCBC, Gastric Varices in Absence of Splenic Vein Thrombosis: a Rare Entity of Idiopathic Non-Cirrhotic Portal Hypertension. Cureus. 2017;9:1179.
5. Ziarkiewicz-Wroblewska B, Gornicka B, Wroblewski T, et al. Idiopathic portal hypertension: a case report. Med Sci Monit. 2004;2004:69–72.
6. Gioia S, Nardelli S, Ridola L. Causes and Management of Non-cirrhotic Portal Hypertension. PMC. 2020;22:1–8.
7. Dagher L, Burroughs A. Variceal bleeding and portal hypertensive gastropathy. Eur J Gastroenterol Hepatol. 2001;13(1):81–88. doi:10.1097/00042737-200101000-00017
8. de Franchis R, Dell’Era A, Iannuzzi F. Diagnosis and treatment of portal hypertension. Digestive Liver Dis. 2004;36(12):789–798. doi:10.1016/j.dld.2004.08.001
9. Jin SJ, Choi WM. Porto-Sinusoidal Vascular Disease: a Concise Updated Summary of Epidemiology, Pathophysiology, Imaging, Clinical Features, and Treatments. Korean J Radiol. 2023;24(1):31–38. doi:10.3348/kjr.2022.0668
10. Barisic-Jaman M, Milosevic M, Pastrovic F, Skrtic A, Grgurevic I. Porto-sinusoidal vascular disease: a new definition of an old clinical entity. Clin Exp Hepatol. 2023;9(4):297–306. doi:10.5114/ceh.2023.133107
11. Kmeid M, Liu X, Ballentine S, Lee H. Idiopathic Non-Cirrhotic Portal Hypertension and Porto-Sinusoidal Vascular Disease: review of Current Data. Gastroenterol Res. 2021;14(2):49–65. doi:10.14740/gr1376
12. Lodato F, Azzaroli F, Di Girolamo M, et al. Proton Pump Inhibitors in cirrhosis: tradition or evidence based practice? World J Gastroenterol. 2008;14(19):2980–2985. doi:10.3748/wjg.14.2980
13. Fiordaliso M, Pala B, Marincola G, et al. A Narrative Review on Non-Cirrhotic Portal Hypertension: not All Portal Hypertensions Mean Cirrhosis. Diagnostics. 2023;13(20). doi:10.3390/diagnostics13203263.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.