Back to Journals » Risk Management and Healthcare Policy » Volume 15
Population Attributable Risks of Potential Modifiable Factors for Atrial Fibrillation in China: A National Survey
Authors Nie Z, Xu H, Chen C, Gan Y, Chen G, Wang C, Yue W, Yan F, Feng Y, Lu Z ![]()
Received 28 January 2022
Accepted for publication 4 June 2022
Published 14 June 2022 Volume 2022:15 Pages 1215—1224
DOI https://doi.org/10.2147/RMHP.S360285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Zhiqiang Nie,1,2,* Hongbin Xu,2,* Chen Chen,3,* Yong Gan,2 Guo Chen,1 Chao Wang,2 Wei Yue,4 Feng Yan,5 Yingqing Feng,1 Zuxun Lu2
1Department of Cardiology, Hypertension Research Laboratory, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, 510080, People’s Republic of China; 2Department of Social Medicine and Health Management, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 3Department of Respiratory, Pediatric Intensive Care Unit, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, Guangzhou, People’s Republic of China; 4Department of Neurology, Tianjin Huanhu Hospital, Tianjin, People’s Republic of China; 5Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zuxun Lu, School of Public Health, Tongji Medical College, No. 13 Hangkong Road, Wuhan, 430030, People’s Republic of China, Email [email protected] Yingqing Feng, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, No. 106 Zhongshan Two Road, Yuexiu District, Guangzhou, 510080, People’s Republic of China, Email [email protected]
Background: There is an association between atrial fibrillation (AF) and overall mortality as well as mobility. It is not known, however, what the preventable burden of AF in China is. This study aims to identify what proportion of the burden of AF may be avoided by modifiable risk factors.
Methods: As part of the China National Stroke Screening and Prevention Project, 726,451 adults aged ≥ 40 years were enrolled in a representative cross-sectional study. The following seven factors have been categorized as modifiable risk factors for AF: body mass index, smoking, alcohol consumption, physical inactivity, hypertension, diabetes mellitus, and dyslipidemia. In order to calculate population-attributable risks (PARs), odds ratios (ORs) were calculated for selected risk factors.
Results: The crude ORs increased with age (ORs ranged from 1.92 to 4.02). A total of 18,736 cases of prevalent AF have been identified. The overall prevalence of AF was 2.6%. The crude ORs increased with age (ORs range 1.92– 4.03). The adjusted ORs and the corresponding confidence intervals (CIs) for these seven modifiable factors were 1.16 (95% confidence interval [CI]: 1.12– 1.19), 1.56 (95% CI: 1.49– 1.62), 2.15 (95% CI: 2.02– 2.28), 2.07 (95% CI: 2.01– 2.14), 2.71 (95% CI: 2.62– 2.79), 2.10 (95% CI: 2.02– 2.19), 2.52 (95% CI: 2.44– 2.60), and 3.32 (95% CI: 3.18– 3.48), respectively. Accordingly, 59.3% of all cases of AF could be explained by having these modifiable risk factors, among which hypertension accounted for the greatest share.
Conclusion: In China, hypertension is the leading preventable cause of AF, and more than half of these cases can be prevented through improving those modifiable risk factors.
Keywords: atrial fibrillation, risk factors, population attributable risk, odds ratio, hypertension
Introduction
Atrial fibrillation (AF) is a most common persistent cardiac arrhythmia, is an important prognostic indicator for stroke, heart failure, cardiovascular and all-cause mortality.1 AF posed significant challenges to patients, physicians, and healthcare systems globally. Approximately 33.3 million people worldwide were affected, resulting in roughly 195,300 deaths in 2015.2 It was estimated that the age-standardized prevalence of AF in adults ranged between 2% and 4%, with an increase of 2.3 times.3, AF has now become a considerable healthcare cost burden as well as a critical public health issue in China.4
In sight of the enormous burden of AF in China, AF prevention is a pressing concern in this region. Primary prevention strategies are restricted by an unclear pathophysiology5 and several non-modifiable risk factors of AF (eg, gender, age, genetic background).6 Nonetheless, various modifiable risk factors, including obesity,7 smoking,8 alcohol intake,9 physical activity,10 diabetes,11 hypertension,12 dyslipidemia,13 obstructive sleep apnea,14 which may serve as prevention or intervention targets. The approaches to AF prevention vary according to geographical regions15 or demographic characteristics (eg, age, gender), which require an accurate risk assessment based on the - factors mentioned above.
It is estimated that 62% to 88% of coronary heart disease or heart failure events could be prevented if a variety of risk factors are maintained.16,17 By contrast, it remains unclear what risks of AF are potentially avoidable by relevant risk factors, especially in China. In order to tailor targeted strategies for the prevention and control of AF, it is also essential to identify which risk factors tend to occur simultaneously and can be reduced altogether in the population. With limited epidemiologic literature available, our study aimed to investigate the importance of potentially modifiable risk factors via using a population attributable risk (PAR) model in a nationally representative sample of the population, which could better enhance policy makers’ awareness of the identification of priority areas for effective and customized management strategies for preventing AF.
Methods
Study Design and Population
The data presented here are derived from the China National Stroke Screening and Prevention Project (CNSSPP), conducted in 31 provinces (except Tibet) in Mainland China between October 2014 and November 2015. Additional details on the design and rationale of the study have been published previously.18 Briefly, a nationally representative hospital-based sample was created using a stratified, multistage cluster sampling procedure. Chinese adults aged 40 and older were included in the study. In each project area, structured face-to-face interviews conducted by trained neurologists or physicians from community hospitals, resulting in a response rate of 85%. This study was carried out in accordance with the Declaration of Helsinki and was approved by the local ethics committee (Ethics Committee of Xuanwu Hospital and Capital Medical University). The participants provided informed consent prior to participating in the study. All investigations were conducted in accordance with institutional guidelines.
Outcome Definition
AF was defined by either evidence based on a self-reported history of persistent AF (asked as “Has a doctor or other health professional ever informed you that you suffered from atrial fibrillation?”) or with an electrocardiograph (ECG). All ECGs were reviewed by board certified cardiologists who confirmed the diagnosis of AF.
Data Collection
AF risk profiles were compared among seven geographical regions, including northeastern, northern, eastern, central, southern, northwestern, and southwestern (Figure 1). Individual-level covariates were demographic variables (age, sex, location, economic development, family history of stroke, stroke), and modifiable risk factors (body mass index (BMI), cigarette smoking, alcohol consumption, physical inactivity, hypertension, diabetes mellitus, dyslipidemia). Age was divided by 10-year categories as follows: ≥80, 70–79, 60–69, 50–59, 40–49 yrs. Comparatively, the elderly were defined as ≥60 years old, and the young as <60 years old.19 Economic development of regions was classified as Less-developed, Middle-developed, and developed in 2014 based on the tertials of per capita disposable household income. The definition of a stroke family history is the occurrence of stroke in the participant’s parents, brothers, or sisters. According to the World Health Organization (WHO) MONICA Project, Stroke is defined as a combined result of a previous medical diagnosis that was verified by the medical records and the judgment of a neurologist or physician.
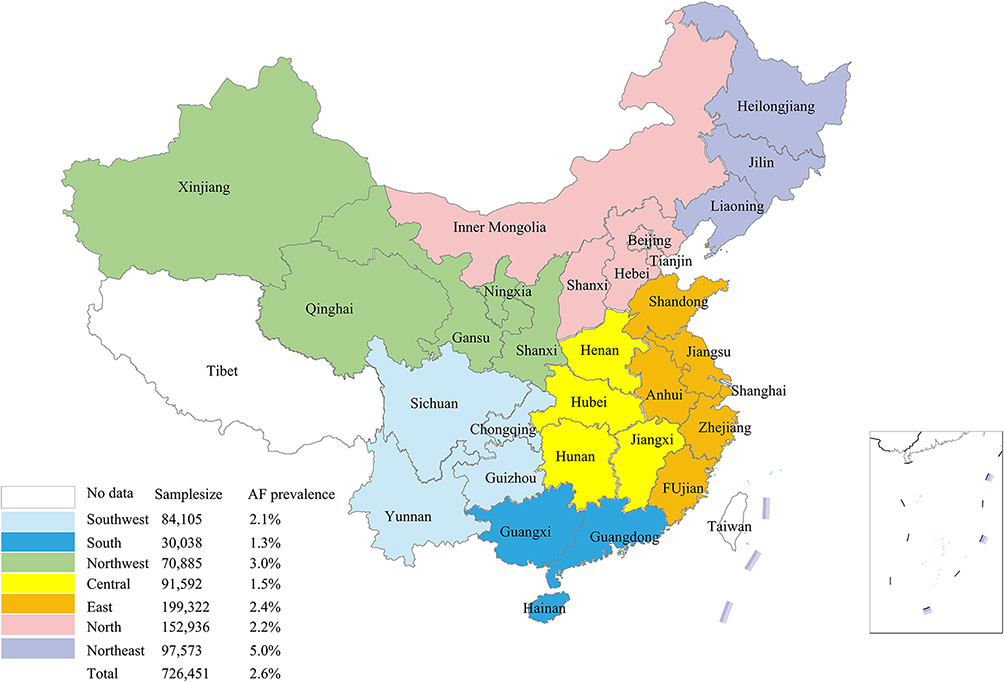 |
Figure 1 Participants and prevalence of atrial fibrillation from different geographical regions. |
Assessment of Risk Factors
BMI (in kg/m2) was divided into three groups (<25, 25 to 30, and >30 kg/m2) based on the WHO recommendations for measuring obesity (normal weight, overweight, and obese). Smoking was defined as anyone who has smoked more than 100 cigarettes in their lifetime. Participants who consumed at least one alcoholic beverage per week (beer, wine, and liquor) for at least one year were considered alcohol drinkers. Based on self-reports, the definition of physical activity is “≥3 times per week for at least 30 minutes each time”. Hypertension was defined as a current resting systolic blood pressure (SBP)≥140 mmHg, and/or a diastolic blood pressure (DBP)≥90 mmHg, by a self-reported hypertension, or the current use of antihypertensive agents. Type 2 diabetes was defined as fasting plasma glucose (FPG) levels of ≥7.0 mmol/L and/or non-FPG amounts ≥11.1 mmol/L in multiple examinations or the use of insulin or oral hypoglycemic agents. Dyslipidemia was defined as fasting TG ≥2.26 mmol/L and/or HDL-C <1.04 mmol/L and/or LDL-C >4.14 mmol/L and/or TC≥6.22 mmol/L, or current use of lipid-lowering medications.
Statistical Analysis
This study was reported in accordance with STROBE reporting guidelines (Supplementary Checklist). All continuous variables were classified according to their central tendency and variability. For categorical factors, percentages were utilized to describe the distributions. Due to the hierarchical structure of the data (geographical region), intra-class correlation coefficients (ICCs) were calculated to evaluate intra-observer repeatability. The ICC was less than 6%, suggesting that hierarchical-level variation was responsible for only a small proportion of variance in AF risk estimation. Then, the crude and adjusted main effects were estimated through using univariate and multivariable logistic regression models.
Population-attributable risks (PARs) were calculated to determine the possible impact of altering risk profiles on the incidence of AF. An approach to multivariable estimation of PAR for each risk factor, as well as combinations of risk factors, was described by Yusuf et al20 and Qaddoura et al.14 Odds ratios (ORs) were estimated using multivariable logistic regressions. PARs were estimated for seven modifiable risk factors, after adjusting for age, sex, location, economic development, family history of stroke, and stroke. PAR% can be interpreted as the percentage by which the prevalence of AF could be lowered among all individuals with AF if the given exposure was abolished, assuming that the observed association is causal.
Missing data were not imputed since less than 1% of the data for any predictor variable were missing from the dataset. The data were analyzed using SAS (Version 9.4; SAS Institute Inc, Cary, NC, USA) and R (Version 3.2.5; R Foundation for Statistical Computing, Vienna, Austria). All statistical tests were two-sided, and p< 0.05 was considered statistically significant.
Results
After the primary data cleaning, a total of 726,451 residents (386,975 women and 339,476 men) were included. Figure 1 illustrates the geographical variation in the sample size and prevalence of AF across the seven major geographical regions in China. Descriptive characteristics of the cases are summarized in Table 1. The proportion of patients with AF varied according to their demographics and risk factors. The mean age of these participants was 57.2±11.4 years. Among the AF patients, approximately 33.0% were 60–69 years old, 25.0% were 50–59 years old, and 7.0% were 80 years old or older. AF patients who were more likely to be female, in a middle-developed economic region, with a family history of stroke, with a history of stroke, with overweight or obesity, with current smoking, with current alcohol consumption, with physical inactivity, with hypertension, with diabetes mellitus, and with dyslipidemia (p<0.001).
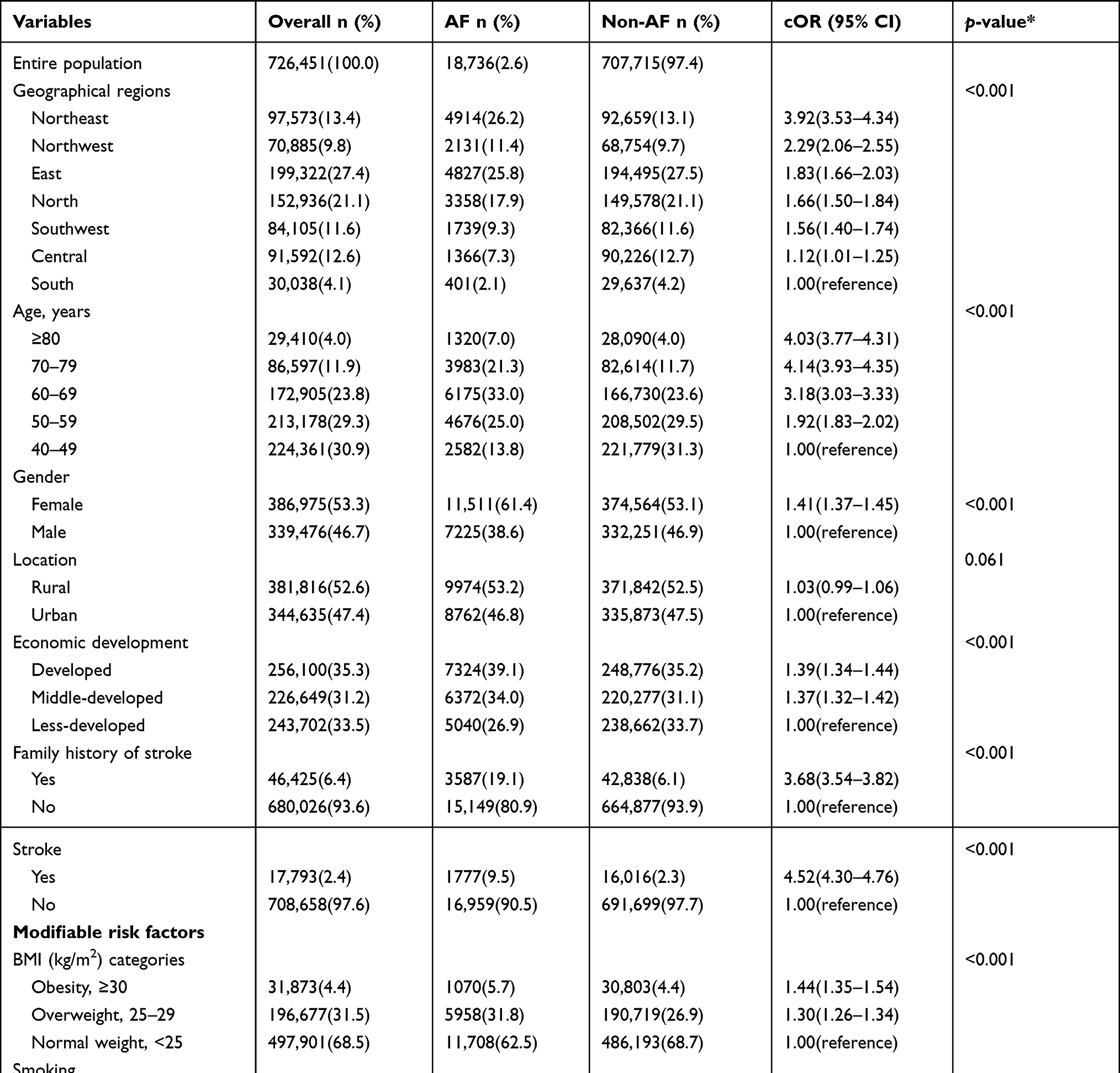 |
Table 1 Characteristics of the Study Participants |
Association of seven modifiable risk factors with AF, BMI, smoking, alcohol consumption, physical inactivity, hypertension, diabetes mellitus, and dyslipidemia is reported in Figure 2. After adjusting for age, gender, economic development, family history of stroke, and stroke, the results demonstrate that AF were significantly associated with these seven modifiable factors. The adjusted odds ratio (aOR) of overweight or obesity in patients with AF was 1.16 (95% CI: 1.12–1.19). Smoking was associated with an increased risk of AF (aOR=1.56, 95% CI: 1.49–1.62). Moreover, a high proportion of patients with AF had other modifiable risk factors including alcohol consumption (aOR=2.15, 95% CI: 2.02–2.28), physical inactivity (aOR=2.07, 95% CI: 2.01–2.14), hypertension (aOR=2.71, 95% CI: 2.62–2.79), diabetes mellitus (aOR=2.10, 95% CI: 2.02–2.19), and dyslipidemia (aOR=3.32, 95% CI: 3.18–3.48).
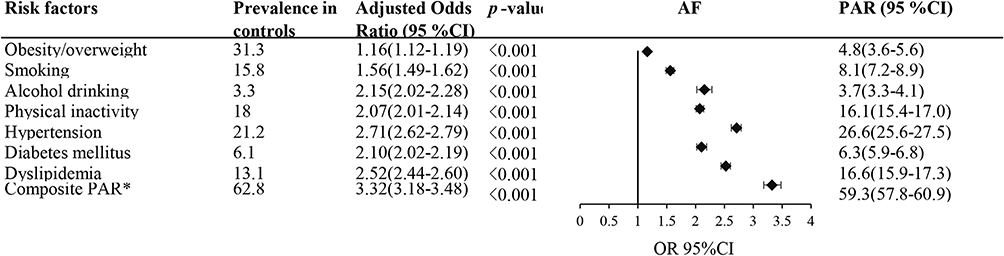 |
Figure 2 Multivariable analysis of prevalence of modifiable risk factors, Odds ratio for modifiable risk factors. Abbreviations: aOR, adjusted odds ratio; AF, atrial fibrillation; PAR, population-attributable risk. Note: *Composite PAR includes all seven risk factors. |
An analysis of the independent effects of seven separate risk factors on AF susceptibility was carried out in a stepwise manner. The most significant contributor to prevalent AF was hypertension, which constituted 22.0% of the entire sample, accounting for 26.6% (95% CI: 25.6–27.5%) (Figure 2). Dyslipidemia and physical inactivity are responsible for 16.6% and 16.1% of all AF cases, respectively. Obesity and overweight, smoking, alcohol consumption, and diabetes mellitus accounted for 4.8–8.1% of total AF cases. In this cohort, alcohol consumption represented the smallest proportion of the AF burden (3.7%) (Figure 3). Combining all seven risk factors, the PAR was 59.3% (57.8–60.9%) for all AF cases.
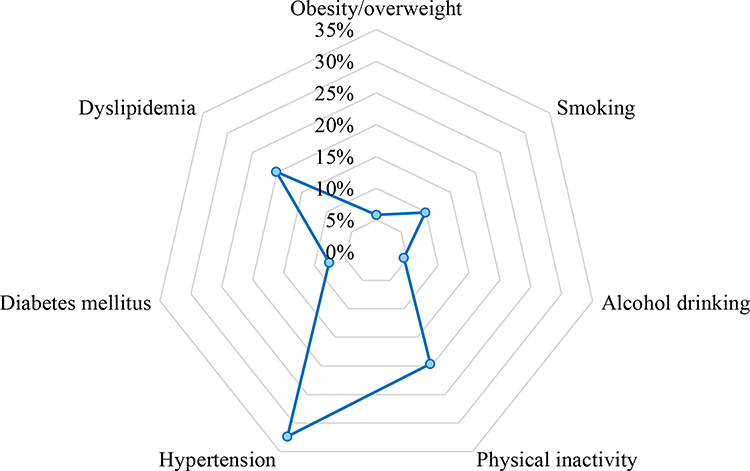 |
Figure 3 The percentage of total population population-attributable risk. |
These associations were robust, with the similar importance rank and approximate effect sizes for all subtypes of regions, sex, and age groups. However, smoking only explains 4.9% and hypertension only explains 15.6% of total AF cases in the South of China; smoking accounted for 10.0% and alcohol consumption for 7.3% of total AF cases in males; and hypertension explained 32.2% of total AF cases in the elderly. (Supplement Figures S1–S4).
Discussion
PAR and Prevalence
The seven potentially modifiable risk factors contributed to approximately two thirds of the PAR for AF cases in China. Comparing to other risk factors, hypertension, dyslipidemia, and physical inactivity played a greater role in the prevalence of AF. There were, however, some discrepancies between the Northeast and the South (smoking and hypertension), between females and males (smoking and alcohol consumption), and between the elderly and the young (hypertension). Despite the risk factors were clustered and unevenly distributed across the geographical regions, the overall contribution of those seven risk factors to AF risk was consistent in all populations, which shows that general approaches to prevention of AF can be similar, but population-specific refinement of programs may be necessary. This study provided insights into AF epidemiology that may help to develop population-based healthcare strategies in China.
A previous study based on the Framingham cohort concluded that cigarette smoking, diabetes mellitus, hypertension, and prevalent coronary heart disease together explained 44% of the AF burden for men and 58% for women.21 Within a U.S cohort of middle-aged adults, 56.5% of AF cases could be explained by ≥1 borderline or elevated risk factors, of which elevated blood pressure ranked highest.22 These findings were consistent with those of the present study.
It was also found that the overall prevalence of AF in China was 2.6%. Previously, the reported prevalence rate ranged from 0.77% to 3.5% based on China national data published in the decade 2004–2014.23–25 The prevalence in our study (2.6%) was higher than the prevalence obtained in a previous study (0.77%), and was close to that reported by Li et al23 in 2013 (1.57%). The differences were most likely to be attributable to the different years, sizes of the population samples, and geographical regions. Therefore, including a large sample size and a complete geographic coverage of the areas will therefore make the findings more reliable. Additionally, the results of our study suggested that the prevalence of AF was associated with increasing age, female, a higher level of economic development, and family history of stroke and stroke, which is consistent with the findings of previous studies.4,26–28
Modifiable Risk Factors
Participants with overweight or obesity, current cigarette smoking, current alcohol consumption, physical inactivity, with hypertension, with diabetes mellitus, with dyslipidemia had higher ORs of AF ranging from 1.16 to 2.71. In this study, we observed significant detrimental effects of those seven modifiable cardiovascular risk factors as contributing to the development and progression of AF. Several epidemiological studies have reported a strong and independent relationship between these risk factors and AF in recent years.
In a U.S biracial middle-aged cohort, excess body weight and weight changes in excess of 5% were associated with an increased risk of AF.29 Furthermore, a prospective cohort study, ARIC study reported that obesity/overweight accounted for approximately 18% of incident AF cases and 12.7% of the PAR.22 It was reported in A U.S prospective observational cohort study that overweight or obesity was the cause of an alarmingly high PAR (12.1%) among older women.30 A randomized controlled study in Australia found that weight reduction and intensive risk factor management were associated with a reduction in AF symptom severity.31
Previous studies have shown that cigarette smoking was significantly associated with an increased risk of AF. According to data from a Netherlands cohort study, smoking in the past and currently was equally associated with an increased risk of AF (relative risk range 1.49–1.51),32 and the risk of AF is reduced by approximately 36% for those who quit smoking.
Alcohol consumption has been linked to AF. The Framingham Heart Study showed heavy alcohol intake (more than three drinks per day, > 36 grams of alcohol per day) greatly increased the risk of AF.33 A large meta-analysis conducted recently found that even one daily drink was statistically significant for increasing the risk of AF. Overall, this represents an increase of approximately 10% in the risk of atrial fibrillation.9
Numerous observational studies have suggested that higher levels of physical activity could reduce the risk of premature AF. For instance, a Norwegian cohort study have indicated that physical activity was associated with AF in a J-shape pattern.10 As observed in a U.S middle-aged biracial cohort, attaining an ideal level of physical activity at study baseline provided some protection against future AF risk.7
Historically, hypertension has been recognized as one of the major risk factors for AF. The ARIC study showed that hypertension accounted for approximately 22% of AF incidents and 24.5% of PARs.22 Similar results were reported from an observational study conducted on postmenopausal women, in which an elevated systolic or diastolic blood pressure was responsible for almost one-third of the PAR of incident AF.30
Several meta-analyses have recently revealed that diabetes increases the risk of developing AF by 0.28 to 0.39. A clear dose-response relationship has been demonstrated between increasing levels of blood glucose and the risk of AF.34,35 In a Danish nationwide cohort study, the risk was more pronounced among young diabetic patients with a more than two-fold increase in risk.11 Both the ARIC study and the study by Perez et al demonstrated that only 3% of incident AF was attributable to diabetes.22,30 However, the PAR of diabetes has increased over time despite improvements in treatment.36
There was conflicting evidence regarding the occurrence of dyslipidemia in relation to AF status was inconsistent. Although many studies have indicated inverse associations between AF and increase in TC or LDL,37,38 these associations are not significant in some studies.13
In summary, AF is amenable to lifestyle intervention: maintaining a healthy body weight, quitting smoking, and participating in physical activity constitute a coherent public health message targeted at reducing the prevalence of AF. Further, the identification of probable modifiable risk factors of AF and the formulation of effective preventive strategies may be a substantial factor in promoting community health and reducing health care expenses.
Strengths and Limitations
To our knowledge, this is the largest study to date evaluating the PAR of major and modifiable risk factors for the association of AF with 726,451 individuals. From a public health perspective, our research highlights the substantial potential for reducing AF risk via primary prevention strategies. Additionally, data collection and management were carefully controlled. Investigators were trained and evaluated through an examination at the beginning of the program. A professional quality controller team was allocated at each survey site. Standard protocols and vigorous quality control programmes were implemented to ensure the quality of data collected.
The present study, however, also had some limitations. First, as an observational study, regardless of the presence of many confounders, residual confounding cannot be excluded. Second, all participants were older than 40 years, so these findings cannot be generalized to younger individuals. The prevalence of AF, however, increases with age, rising from ∼0.5% at 40–50 years, to ∼10% or more at 80 years.39 Third, the AF event was partly based on self-reports, and the numbers may have been underestimated or overstated. In order to minimize bias in the incidence of AF, we only included the data collected from physicians who self-reported the diagnosis. AS well, in our study, AF was diagnosed based on a single electrocardiogram, instead of ambulatory electrocardiogram monitoring. Furthermore, our data on some risk factors, including physical inactivity, cigarette smoking, and alcohol consumption, were gathered from participant self-reports, which might be subject to recall bias. In previous studies, however, it has been found that self-reported AF was reliable and could be used interchangeably or in conjunction with ECG results to confirm the diagnosis.40,41 Finally, the researchers also acknowledged that their ability to correctly classify subtypes of AF was limited, and hence they did not distinguish between subtypes of AF in the AF outcome. In sight of the fact that AF subtypes have not detected any differences in the magnitude of the associations, the hypothesis seems reasonable.20 Additionally, the outcome definition is based on self-reported history of persistent AF. It may be an overestimation of the AF prevalence.
Conclusions
In conclusion, modifiable risk factors contribute significantly to the total PAR of AF. The findings from this study may help develop better prevention and management plans for AF.
Abbreviations
AF, atrial fibrillation; aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; DBP, diastolic blood pressure; ECG, electrocardiograph; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; ICC, intraclass correlation coefficient; LDL-C, low-density lipoprotein cholesterol; ORs, odds ratios; PARs, population-attributable risks; SBP, systolic blood pressure; TG, triglyceride.
Data Sharing Statement
The datasets generated in this study and the protocol are available from the corresponding author on reasonable request.
Ethics Statement
Our study was performed according to the declaration of Helsinki and approved by the Ethics Committee of Xuanwu Hospital Institutional Review Board, Capital Medical University (Beijing, China). Informed Consent was obtained from the participants of the study subjects. All investigations were performed in accordance with institutional guidelines.
Author Contributions
ZXL and YQF conceived and designed the research. YG, GC, CW, WY, and FY performed the research and collected data. ZQN analyzed the data and wrote the manuscript. HBX and CC revised the manuscript critically for important intellectual content. LZX and FYQ provided advices and supervision of the work. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Guangdong Province [2020A1515010743], the National Social Science Foundation of China [18ZDA085], Science and Technology Planning Project of Guangdong Province (2019B020230003; 2018B090944002; 2020B1111170011), and Guangdong peak project (DFJH201802).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Hindricks G, Potpara T, Dagres N, et al. ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42:373–498.
2. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
3. Kjerpeseth LJ, Igland J, Selmer R, et al. Prevalence and incidence rates of atrial fibrillation in Norway 2004–2014. Heart. 2020;107:201–207. doi:10.1136/heartjnl-2020-316624
4. Guo Y, Tian Y, Wang H, Si Q, Wang Y, Lip GY. Prevalence, incidence, and lifetime risk of atrial fibrillation in China: new insights into the global burden of atrial fibrillation. Chest. 2015;147(1):109–119.
5. Schnabel RB, Aspelund T, Li G, et al. Validation of an atrial fibrillation risk algorithm in whites and African Americans. Arch Intern Med. 2010;170(21):1909–1917. doi:10.1001/archinternmed.2010.434
6. Johansen OE, Tveit A. Understanding modifiable risk factors for new onset atrial fibrillation: the knowledge gap is closing. AME Med J. 2017;2:178. doi:10.21037/amj.2017.12.01
7. Huxley RR, Misialek JR, Agarwal SK, et al. Physical activity, obesity, weight change, and risk of atrial fibrillation: the atherosclerosis risk in communities study. Circ Arrhythm Electrophysiol. 2014;7(4):620–625. doi:10.1161/CIRCEP.113.001244
8. Sabzwari SRA, Garg L, Lakkireddy D, Day J. Ten lifestyle modification approaches to treat atrial fibrillation. Cureus. 2018;10(5):45.
9. Larsson SC, Drca N, Wolk A. Alcohol consumption and risk of atrial fibrillation: a prospective study and dose-response meta-analysis. J Am Coll Cardiol. 2014;64(3):281–289. doi:10.1016/j.jacc.2014.03.048
10. Morseth B, Graff-Iversen S, Jacobsen BK, et al. Physical activity, resting heart rate, and atrial fibrillation: the Tromsø Study. Eur Heart J. 2016;37(29):2307–2313. doi:10.1093/eurheartj/ehw059
11. Pallisgaard JL, Schjerning A-M, Lindhardt TB, et al. Risk of atrial fibrillation in diabetes mellitus: a nationwide cohort study. Eur J Prev Cardiol. 2016;23(6):621–627. doi:10.1177/2047487315599892
12. Brandes A, Smit MD, Nguyen BO, Rienstra M, Van Gelder IC. Risk factor management in atrial fibrillation. Arrhythm Electrophysiol Rev. 2018;7(2):118. doi:10.15420/aer.2018.18.2
13. Allan V, Honarbakhsh S, Casas J-P, et al. Are cardiovascular risk factors also associated with the incidence of atrial fibrillation? Thromb Haemost. 2017;117(05):837–850. doi:10.1160/TH16-11-0825
14. Qaddoura A, Kabali C, Drew D, et al. Obstructive sleep apnea as a predictor of atrial fibrillation after coronary artery bypass grafting: a systematic review and meta-analysis. Canad J Cardiol. 2014;30(12):1516–1522. doi:10.1016/j.cjca.2014.10.014
15. Liu S, Li Y, Zeng X, et al. Burden of cardiovascular diseases in China, 1990–2016: findings from the 2016 global burden of disease study. JAMA Cardiol. 2019;4(4):342–352. doi:10.1001/jamacardio.2019.0295
16. Hozawa A, Folsom AR, Sharrett AR, Chambless LE. Absolute and attributable risks of cardiovascular disease incidence in relation to optimal and borderline risk factors: comparison of African American with white subjects–Atherosclerosis Risk in Communities Study. Arch Intern Med. 2007;167(6):573–579. doi:10.1001/archinte.167.6.573
17. Folsom AR, Yamagishi K, Hozawa A, Chambless LE. Absolute and attributable risks of heart failure incidence in relation to optimal risk factors. Circ Heart Fail. 2009;2(1):11–17. doi:10.1161/CIRCHEARTFAILURE.108.794933
18. Tan X, Zhang Y, Shao H. Healthy China 2030, a breakthrough for improving health. Glob Health Promot. 2019;26(4):96–99. doi:10.1177/1757975917743533
19. Murray CJ, Ezzati M, Flaxman AD, et al. GBD 2010: design, definitions, and metrics. Lancet. 2012;380(9859):2063–2066. doi:10.1016/S0140-6736(12)61899-6
20. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. doi:10.1016/S0140-6736(04)17018-9
21. Benjamin EJ, Levy D, Vaziri SM, D’Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA. 1994;271(11):840–844. doi:10.1001/jama.1994.03510350050036
22. Huxley RR, Lopez FL, Folsom AR, et al. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123(14):1501–1508. doi:10.1161/CIRCULATIONAHA.110.009035
23. Li Q, Wu H, Yue W, et al. Prevalence of stroke and vascular risk factors in china: a nationwide community-based study. Sci Rep. 2017;7(1):6402. doi:10.1038/s41598-017-06691-1
24. Li Y, Wu YF, Chen KP, et al. Prevalence of atrial fibrillation in China and its risk factors. Biomed Environ Sci. 2013;26(9):709–716. doi:10.3967/0895-3988.2013.09.001
25. Zhang X, Zhang S, Li Y, et al. Association of obesity and atrial fibrillation among middle-aged and elderly Chinese. Int J Obes. 2009;33(11):1318–1325. doi:10.1038/ijo.2009.157
26. Chei CL, Raman P, Ching CK, et al. Prevalence and risk factors of atrial fibrillation in Chinese elderly: results from the Chinese longitudinal healthy longevity survey. Chin Med J. 2015;128(18):2426–2432. doi:10.4103/0366-6999.164918
27. Diener HC, Aisenberg J, Ansell J, et al. Choosing a particular oral anticoagulant and dose for stroke prevention in individual patients with non-valvular atrial fibrillation: part 1. Eur Heart J. 2017;38(12):852–859. doi:10.1093/eurheartj/ehv643
28. Madhavan M, Graff-Radford J, Piccini J, Gersh B. Cognitive dysfunction in atrial fibrillation. Nat Rev Cardiol. 2018;15(12):744–756. doi:10.1038/s41569-018-0075-z
29. Wanahita N, Messerli FH, Bangalore S, Gami AS, Somers VK, Steinberg JS. Atrial fibrillation and obesity—results of a meta-analysis. Am Heart J. 2008;155(2):310–315. doi:10.1016/j.ahj.2007.10.004
30. Perez MV, Wang PJ, Larson JC, et al. Risk factors for atrial fibrillation and their population burden in postmenopausal women: the Women’s Health Initiative Observational Study. Heart. 2013;99(16):1173–1178. doi:10.1136/heartjnl-2013-303798
31. Abed HS, Wittert GA, Leong DP, et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA. 2013;310(19):2050–2060. doi:10.1001/jama.2013.280521
32. Heeringa J, Kors JA, Hofman A, van Rooij FJ, Witteman JC. Cigarette smoking and risk of atrial fibrillation: the Rotterdam Study. Am Heart J. 2008;156(6):1163–1169. doi:10.1016/j.ahj.2008.08.003
33. Djousse L, Levy D, Benjamin EJ, et al. Long-term alcohol consumption and the risk of atrial fibrillation in the Framingham Study. Am J Cardiol. 2004;93(6):710–713.
34. Tadic M, Cuspidi C. Type 2 diabetes mellitus and atrial fibrillation: from mechanisms to clinical practice. Arch Cardiovasc Dis. 2015;108(4):269–276. doi:10.1016/j.acvd.2015.01.009
35. Aune D, Feng T, Schlesinger S, Janszky I, Norat T, Riboli E. Diabetes mellitus, blood glucose and the risk of atrial fibrillation: a systematic review and meta-analysis of cohort studies. J Diabetes Complications. 2018;32(5):501–511. doi:10.1016/j.jdiacomp.2018.02.004
36. Schnabel RB, Yin X, Gona P, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386(9989):154–162. doi:10.1016/S0140-6736(14)61774-8
37. Knuiman M, Briffa T, Divitini M, et al. A cohort study examination of established and emerging risk factors for atrial fibrillation: the Busselton Health Study. Eur J Epidemiol. 2014;29(3):181–190. doi:10.1007/s10654-013-9875-y
38. Lopez FL, Agarwal SK, Maclehose RF, et al. Blood lipid levels, lipid-lowering medications, and the incidence of atrial fibrillation: the atherosclerosis risk in communities study. Circ Arrhythm Electrophysiol. 2012;5(1):155–162. doi:10.1161/CIRCEP.111.966804
39. Heeringa J, van der Kuip DA, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006;27(8):949–953. doi:10.1093/eurheartj/ehi825
40. Psaty BM, Manolio TA, Kuller LH, et al. Incidence of and risk factors for atrial fibrillation in older adults. Circulation. 1997;96(7):2455–2461. doi:10.1161/01.CIR.96.7.2455
41. Soliman EZ, Howard G, Meschia JF, et al. Self-reported atrial fibrillation and risk of stroke in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study. Stroke. 2011;42(10):2950–2953. doi:10.1161/STROKEAHA.111.621367
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.