Back to Journals » Vascular Health and Risk Management » Volume 21
Poor Sleep Pattern Might Increase the Prevalence of Abdominal Aortic Calcification in US Adults: Data from the NHANES (2013-2014)
Authors Chen Y ![]() , Xu S
, Xu S ![]() , Duan M, Shen L
, Duan M, Shen L
Received 8 April 2025
Accepted for publication 13 July 2025
Published 31 July 2025 Volume 2025:21 Pages 571—579
DOI https://doi.org/10.2147/VHRM.S532476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roland Asmar
Yunqing Chen,1 Shiyong Xu,2 Mingxia Duan,2 Liang Shen2
1Department of Infectious Diseases, Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China; 2Department of Cardiology, Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China
Correspondence: Liang Shen, Affiliated Hospital of Jiaxing University, No. 1882 Zhonghuan South Road, Jiaxing, Zhejiang, People’s Republic of China, Tel +86 18868042552, Email [email protected]
Background: Abdominal aortic calcification (AAC) is a reliable predictor of cardiovascular events. Sleep is an essential component of cardiovascular health. This study aimed to assess the association between sleep patterns (including sleep duration, trouble sleeping, and sleep disorders) and the risk of AAC.
Methods: A total of 2801 participants from the 2013 to 2014 National Health and Nutrition Examination Survey (NHANES) 2013– 2014 cycle were included in the study. AAC score was assessed using the Kauppila scoring system. Sleep patterns were defined according to the overall sleep score, which was calculated based on the sleep duration, self-reported trouble sleeping, and sleep disorders. Weighted multivariable linear regression models were used to analyze the association between sleep patterns and AAC.
Results: AAC prevalence was higher in older age groups, smokers, those with hypertension or diabetes, and those with less physical activity, lower eGFR, or higher levels of total 25-hydroxyvitamin D, serum uric acid, and serum calcium. Compared with the healthy sleep pattern group, participants in the poor sleep pattern group had a higher prevalence of AAC (odds ratio [OR] = 1.664, 95% CI: 1.286– 2.152) and a higher prevalence of severe AAC (OR = 2.179, 95% CI: 1.539– 3.087). After adjusting for potential confounders, the poor sleep pattern group remained significantly associated with a higher risk of AAC (OR = 1.657, 95% CI: 1.235– 2.222) and severe AAC (OR = 2.374, 95% CI: 1.616– 3.488).
Conclusion: Sleep patterns were related to the risk of AAC in middle-aged and elderly populations. Poor sleep patterns may increase AAC prevalence.
Keywords: abdominal aortic calcification, NHANES, sleep pattern, cardiovascular event
Introduction
Cardiovascular disease (CVD) is the leading cause of mortality worldwide. Abdominal aortic calcification (AAC), defined as abnormal deposition of calcium phosphate complexes in the abdominal aorta, is a common manifestation of vascular calcification (VC).1 Previous studies have demonstrated that AAC is a reliable marker for atherosclerotic CVD and can predict cardiovascular events.2–5
Sleep is an important component of cardiovascular health. In 2022, the American Heart Association (AHA) proposed the concept of “Life’s Essential 8” by adding sleep as one of the eight components that build optimal CV health.6 Sleep disorders are associated with numerous CVDs including coronary artery disease, heart failure, and arrhythmias.7–10
Previous studies investigated the relationship between sleep and coronary artery calcification.11,12 In addition, poor sleep quality is associated with aortic calcification in middle-aged women.13 Recently, Wang et al reported that long sleep duration is associated with AAC in male adults with chronic kidney disease (CKD).14 However, it remains unclear whether this relationship also applies to a broader population.
This study aimed to investigate the association between combined sleep factors and AAC in the US population using the 2013–2014 National Health and Nutrition Examination Survey (NHANES).
Methods
All data are publicly available and can be accessed from NHANES (https://www.cdc.gov/nchs/nhanes/index.htm). The National Center for Health Statistics Research Ethics Review Board approved all NHANES protocols, and this study was also approved by the Ethics Committee of the First Hospital of Jiaxing, Jiaxing, China.
Study Population
In this study, we analyzed data from the NHANES, focusing on the 2013–2014 cycle. In total, 10175 participants were enrolled, after excluding those with missing AAC data (n=7035), missing sleep data (n=15), and missing relevant covariate data (n=324), a total of 2801 participants were included (Figure 1).
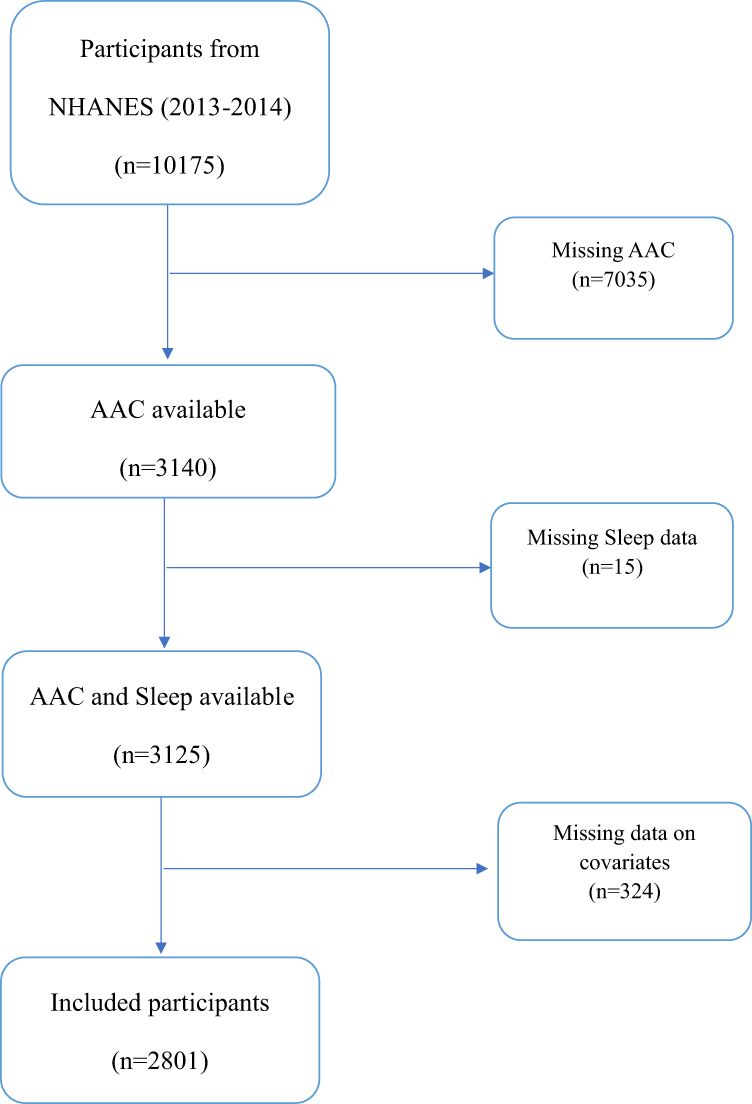 |
Figure 1 Flow chart of the participants’ enrollment. Abbreviations: NHANES, National Health and Nutrition Examination Survey; AAC, abdominal aortic calcification. |
Assessment of Sleep Pattern
Sleep patterns were assessed, as previous study.15 Briefly, the sleep duration was divided into three groups: short (< 7 h per night), normal (7–9 h per night), and long (>9 h per night). The answers to Have you ever told a doctor or other health professionals that you have trouble sleeping? and “Have you/Has SP ever been told by a doctor or other health professional that you have a sleep disorder?” was used to assess trouble sleeping and other sleep disorders. A score of 1 or 0 was assigned to each sleep factor according to a low or high risk, respectively. Low-risk sleep was defined as sleeping 7–9 hours per night without trouble sleeping or sleep disorders. Finally, the following three sleep patterns were obtained: poor sleep (0 ≤ sleep score ≤ 1), intermediate sleep (sleep score = 2), and healthy sleep (sleep score = 3).
Evaluation of AAC and Severe AAC
AAC was scanned using dual-energy X-ray absorptiometry (DXA) and semi-quantified using the Kauppila score system.16 Briefly, the anterior and posterior aortic walls were divided into four segments, and each segment was assigned a score (0–6) according to the degree of calcium deposition. AAC was diagnosed when the total AAC score was >0 and severe AAC was defined as a total AAC score >6.
Assessment of Covariates
Other covariates including age, sex, race, marital status, education level, ratio of family income to poverty (RIP), lifestyle risk factors (smoking, alcohol, and physical activity), general health condition (BMI, hypertension, and diabetes), and biochemical parameters (total cholesterol, total triglycerides, total 25-hydroxyvitamin D, serum alkaline phosphatase, eGFR, serum uric acid, serum phosphorus, and serum calcium) were obtained through interviews and physical examinations. In brief, demographic characteristics and lifestyle risk factors were collected using household interview and mobile examination center (MEC) questionnaires. Physical examination information, biochemical parameters were derived from medical examinations and laboratory assessments in the MEC. The selection of all covariates was based on previous studies.17–19 Race was categorized into five groups: Mexican American, Non-Hispanic White, Non-Hispanic Black, Other Hispanic, and Other others. Educational level was divided into less than high school, high school and higher than high school. Marital status included marriage or living with a partner or a single. PIR was classified into three groups: <1.30, 1.31, 3.50, and ≥3.50.18 Smokers were defined as those who had smoked more than 100 cigarettes in their lifetime. Drinkers were defined as those who drank at least 12 alcoholic drinks per year. BMI was categorized as under/normal weight (<25.0 kg/m2), overweight (25.0–30.0 kg/m2), and obesity (≥30.0 kg/m2).20 Physical activity was classified into two groups, active and inactive, according to the Physical Activity Guidelines recommendation of ≥75 min/week of vigorous or ≥150 min/week of moderate physical activity.21 The eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation.22 Hypertension was defined as a blood pressure measurement of ≥ 140/90 mmHg, self-reported physician-diagnosed hypertension, or the use of antihypertensive medications.23 Diabetes was defined as a fasting glucose level of ≥7.0 mmol/L, or a plasma glucose level of ≥11.1 mmol/L 2 h after an oral glucose tolerance test, self-reported physician-diagnosed diabetes, or taking oral hypoglycemic agents or insulin.17
Statistical Analysis
In accordance with the NHANES analytic guidelines, all statistical analyses were conducted using appropriate sampling weights. We adjusted for the complex, multistage, stratified, cluster-sampling design of the sample by applying the survey weight from the MEC (wtmec2yr). Continuous variables are presented as mean ± standard deviation or median (quartiles: Q1, Q3) depending on whether the data was normal distribution, and weighted linear regression or Mann–Whitney U or Kruskal–Wallis H ware used to examine the differences between the two groups. Categorical variables were expressed as weighted percentages (95% CI) and compared using the chi-square test. Multivariate regression models were used to assess the association between sleep pattern and AAC. Model 1 shows the unadjusted results. Model 2 was adjusted for age, sex, race, marital status, and educational level. Model 3 was further adjusted for PIR, BMI, smoking and drinking status, diabetes, hypertension, physical activity status, eGFR, serum uric acid, serum phosphorus, total 25-hydroxyvitamin D, and total serum calcium levels.
All statistical analyses were performed using STATA (version 16.0; StataCorp, College Station, TX, USA) and SPSS 25.0 (IBM SPSS, Turkey). Two-tailed P value less than 0.05 was considered statistically significant.
Results
Baseline Characteristics
The baseline characteristics of the participants are summarized in Table 1 and Table 2. Significant differences were found between participants with and without AAC in terms of age, race, marital status, PIR, smoking status, physical activity, sleep pattern, hypertension, diabetes, eGFR, total 25-hydroxyvitamin D level, serum uric acid level, and serum calcium level (all p <0.05). Participants with AAC were older and more likely to be black, single, smokers, and less physically active; had less PIR; lower eGFR; and had a high prevalence of hypertension, diabetes, and higher levels of total 25-hydroxyvitamin D, serum uric acid, and serum calcium. Participants with poor sleep patterns were older, more likely to be female, single, smokers, and engaged in less physical activity. In addition, these participants had a lower PIR, lower eGFR, higher prevalence of hypertension and diabetes, and higher BMI, serum uric acid, and serum phosphorus levels.
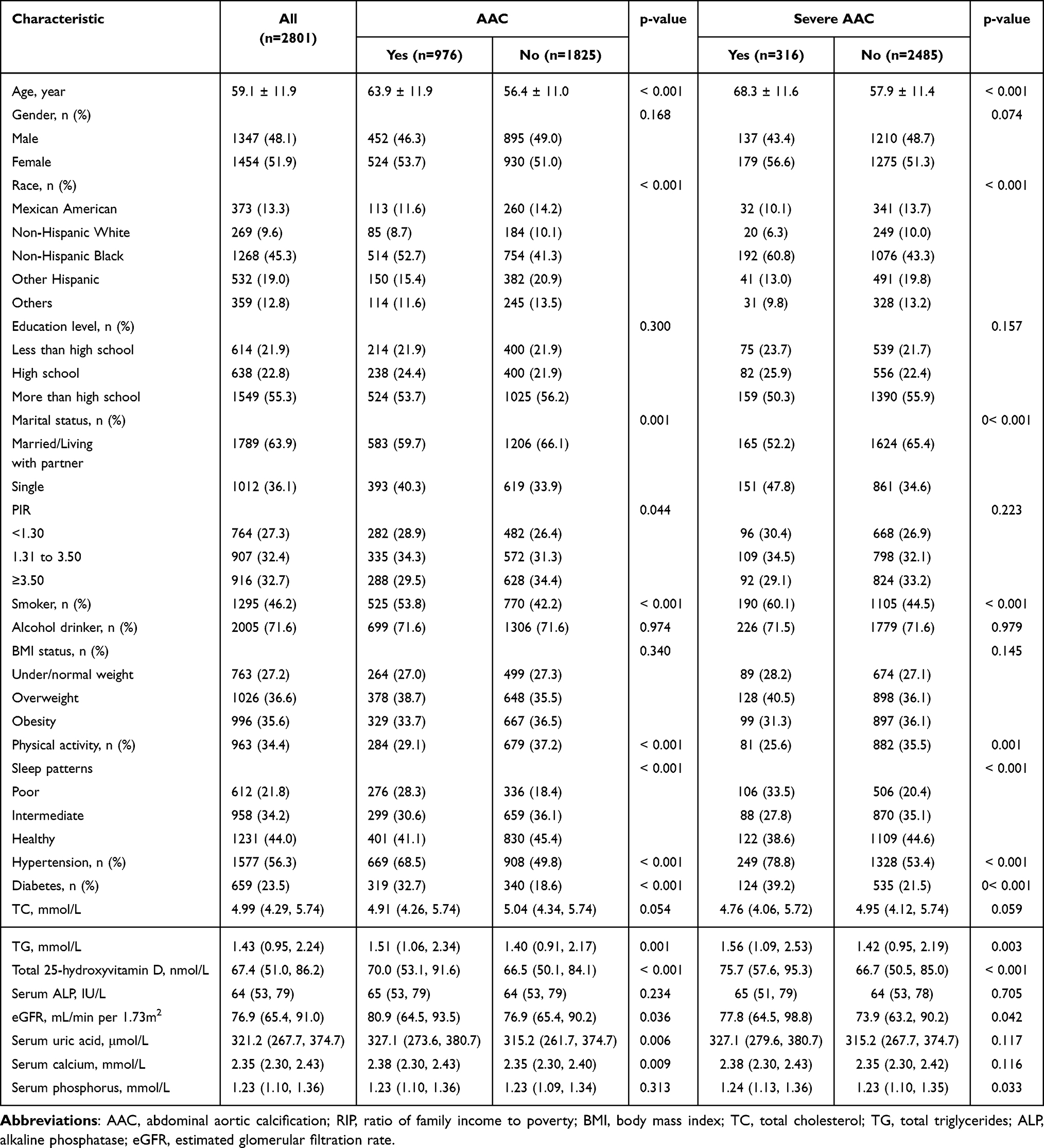 |
Table 1 Characteristics of the Study Population |
 |
Table 2 General Characteristics of Participants Stratified by Sleep Pattern |
Sleep Pattern and AAC
Multiple logistic regression in Table 3 showed that compared with the healthy sleep pattern group, the odds ratios (ORs) for AAC and severe AAC were 1.664 (95% CI, 1.286–2.152) and 2.179 (95% CI, 1.539–3.087), respectively, in the poor sleep pattern group before adjusted for any covariates (Model 1). After adjusting for age, sex, race, education level, and marital status, the ORs for AAC and severe AAC in the poor sleep pattern group were 1.891 (95% CI, 1.423–2.512) and 2.747 (95% CI, 1.882–4.010), respectively, compared to those in the healthy sleep pattern group (Model 3). After adjusting for all covariates, the ORs for AAC and severe AAC in the poor sleep pattern group were 1.657 (95% CI, 1.235–2.222) and 2.374 (95% CI, 1.616–3.488), respectively (Model 3).
 |
Table 3 Associations Between Sleep Pattern and AAC or Severe AAC |
Discussion
In this cross-sectional study, we investigated the relationship between sleep patterns and AAC and found that poor sleep patterns may increase the prevalence of AAC. We also found that several factors, such as age, smoking, physical activity, hypertension, diabetes, eGFR, and serum uric acid, were simultaneously associated with AAC and poor sleep patterns, which further supported the conclusion that poor sleep patterns are associated with higher AAC risk. Since AAC a reliable marker for atherosclerotic CVD and cardiovascular events, improve the quality of sleep might reduce the risk of CVD and cardiovascular events.
Although previous studies have explored the association between sleep and AAC risk, the number of enrolled patients was relatively limited. Our study further expanded the research population and validated previous findings. In addition, our study integrated sleep duration, self-reported trouble sleeping, and sleep disorders into a single sleep measurement, which differs from previous studies. In the future, sleep assessment should be integrated into cardiovascular risk evaluations. Sleep interventions, such as cognitive behavioral therapy, may reduce the risk of AAC.
Vascular calcification is a complex process similar to bone formation. Several mechanisms may have contributed to the association between poor sleep patterns and AAC. Poor sleep patterns may promote the release of inflammatory cytokines such as interleukin-1β (IL-1β) and interleukin-6 (IL-6),24,25 which play crucial roles in the transformation of vascular smooth muscle cells (VSMC) into osteoblast-like cells, followed by calcification.26,27 In addition, poor sleep patterns may also facilitate oxidative stress,28,29 which stimulates the osteoblastic transition of VSMC.30 Bone mineral density (BMD) has been reported to be associated with AAC.31,32 BMD has also been found to be related to sleep quality,33 it is reasonable to speculate that sleep quality might be associated with AAC. Endothelial dysfunction is an important pathophysiological basis for vascular calcification, and sleep disorders may cause endothelial dysfunction and promote AAC.34,35 Maybe we can perform some basic researches by constructing models of sleep disorder and AAC to further explore the relationship between sleep and AAC and the underline mechanisms.
Our study may provide important guidance for the prevention of AAC; however, several limitations should be considered. First, this was a cross-sectional study, and we could not determine a causal relationship between sleep patterns and AAC. Future longitudinal studies are needed to explore the temporal relationships and causality. Second, sleep-related data were collected from self-reports, which might have led to estimation errors. Objective sleep measures such as actigraphy or polysomnography may further validate these findings. Third, we excluded many missing data, which may have influenced our results. Finally, AAC measurement was performed only in the US population aged ≥ 40 years; whether the association existed in other age groups or populations from other countries remains unclear and warrants additional research.
Conclusion
Our study indicated that poor sleep patterns are associated with a higher risk of AAC. Therefore, sleep may be relevant for primary prevention of AAC.
Data Sharing Statement
The data of the current study are available in the NHANES repository, https:// www.cdc.gov/nchs/nhanes/.
Ethics Approval and Consent to Participate
This study analyzed de-identified information downloaded from the National Health and NHANES public database. This study was approved by the National Center for Health Statistics Research Ethics Review Board. Informed consent was obtained from each participant before the survey.
Acknowledgments
The authors gratefully acknowledge all staff and participants of the NHANES for their participation and contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Pioneer Innovation Team of the Jiaxing Institute of Atherosclerotic Diseases (Grant No. XFCX--DMYH), Jiaxing Science and Technology Program (Grant No.2024AD30032), and Jiaxing Key Laboratory of Virus-mediated Infectious Diseases (Grant No. 2021‑bdzdsys).
Disclosure
The authors declare no competing interests in this work.
References
1. Golledge J. Abdominal aortic calcification: clinical significance, mechanisms and therapies. Curr Pharm Des. 2014;20:5834–5838. doi:10.2174/1381612820666140212195309
2. Bastos Goncalves F, Voûte MT, Hoeks SE, et al. Calcification of the abdominal aorta as an independent predictor of cardiovascular events: a meta-analysis. Heart. 2012;98:988–994. doi:10.1136/heartjnl-2011-301464
3. Bolland MJ, Wang TK, van Pelt NC, et al. Abdominal aortic calcification on vertebral morphometry images predicts incident myocardial infarction. J Bone Miner Res. 2010;25:505–512. doi:10.1359/jbmr.091005
4. Golestani R, et al. Abdominal aortic calcification detected by dual X-ray absorptiometry: a strong predictor for cardiovascular events. Ann Med. 2010;42:539–545. doi:10.3109/07853890.2010.515604
5. Bartstra JW, Mali W, Spiering W, de Jong PA. Abdominal aortic calcification: from ancient friend to modern foe. Eur J Prev Cardiol. 2021;28:1386–1391. doi:10.1177/2047487320919895
6. Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health: a presidential advisory from the American Heart Association. Circulation. 2022;146:e18–e43. doi:10.1161/CIR.0000000000001078
7. Jaspan VN, Greenberg GS, Parihar S, et al. The role of sleep in cardiovascular disease. Curr Atheroscler Rep. 2024;26:249–262. doi:10.1007/s11883-024-01207-5
8. Kadier K, et al. Association of sleep-related disorders with cardiovascular disease among adults in the United States: a cross-sectional study based on national health and nutrition examination survey 2005-2008. Front Cardiovasc Med. 2022;9:954238. doi:10.3389/fcvm.2022.954238
9. Fan T, Su D. Interaction effects between sleep disorders and depression on heart failure. BMC Cardiovasc Disord. 2023;23:132. doi:10.1186/s12872-023-03147-5
10. Li X, Zhou T, Ma H, et al. Healthy sleep patterns and risk of incident arrhythmias. J Am Coll Cardiol. 2021;78:1197–1207. doi:10.1016/j.jacc.2021.07.023
11. King CR, et al. Short sleep duration and incident coronary artery calcification. JAMA. 2008;300:2859–2866. doi:10.1001/jama.2008.867
12. Kowall B, Lehmann N, Mahabadi -A-A, et al. Sleep characteristics and progression of coronary artery calcification: results from the Heinz Nixdorf Recall cohort study. Atherosclerosis. 2018;271:45–52. doi:10.1016/j.atherosclerosis.2018.02.013
13. Matthews KA, Everson-Rose SA, Kravitz HM, et al. Do reports of sleep disturbance relate to coronary and aortic calcification in healthy middle-aged women?: study of women’s health across the nation. Sleep Med. 2013;14:282–287. doi:10.1016/j.sleep.2012.11.016
14. Wang Y, et al. Long sleep duration is associated with abdominal aortic calcification among male adults with chronic kidney disease: NHANES 2013-2014. Sci Rep. 2024;14:22076. doi:10.1038/s41598-024-72879-x
15. Li C, Shang S. Relationship between sleep and hypertension: findings from the NHANES (2007-2014). Int J Environ Res Public Health. 2021;18. doi:10.3390/ijerph18157867.
16. Kauppila LI, Polak JF, Cupples LA, et al. New indices to classify location, severity and progression of calcific lesions in the abdominal aorta: a 25-year follow-up study. Atherosclerosis. 1997;132:245–250. doi:10.1016/s0021-9150(97)00106-8
17. Cai C, et al. Association between hemoglobin A1c and abdominal aortic calcification: results from the national health and nutrition examination survey 2013-2014. BMC Cardiovasc Disord. 2024;24:26. doi:10.1186/s12872-023-03700-2
18. Cai Z, et al. Associations between life’s essential 8 and abdominal aortic calcification among middle-aged and elderly populations. J Am Heart Assoc. 2023;12:e031146. doi:10.1161/JAHA.123.031146
19. Li W, Wang Z, Li M, et al. Association between a body shape index and abdominal aortic calcification in general population: a cross-sectional study. Front Cardiovasc Med. 2022;9:1091390. doi:10.3389/fcvm.2022.1091390
20. Xie ZQ, Li H-X, Tan W-L, et al. Association of Serum Vitamin C With NAFLD and MAFLD Among Adults in the United States. Front Nutr. 2021;8:795391. doi:10.3389/fnut.2021.795391
21. Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320:2020–2028. doi:10.1001/jama.2018.14854
22. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi:10.7326/0003-4819-150-9-200905050-00006
23. Heffernan KS, Barreira TV. Association between pulse pressure and aortic calcification: findings from the national health and nutrition examination survey 2013-2014. J Clin Hypertens. 2020;22:879–885. doi:10.1111/jch.13853
24. Zhang Y, Zhao W, Liu K, et al. The causal associations of altered inflammatory proteins with sleep duration, insomnia and daytime sleepiness. Sleep. 2023;46. doi:10.1093/sleep/zsad207
25. Morales-Munoz I, Marwaha S, Upthegrove R, Cropley V. Role of inflammation in short sleep duration across childhood and psychosis in young adulthood. JAMA Psychiatry. 2024;81:825–833. doi:10.1001/jamapsychiatry.2024.0796
26. Kurozumi A, Nakano K, Yamagata K, et al. IL-6 and sIL-6R induces STAT3-dependent differentiation of human VSMCs into osteoblast-like cells through JMJD2B-mediated histone demethylation of RUNX2. Bone. 2019;124:53–61. doi:10.1016/j.bone.2019.04.006
27. Han L, Zhang Y, Zhang M, et al. Interleukin-1beta-induced senescence promotes osteoblastic transition of vascular smooth muscle cells. Kidney Blood Press Res. 2020;45:314–330. doi:10.1159/000504298
28. Lei X, Xu Z, Chen W. Association of oxidative balance score with sleep quality: NHANES 2007-2014. J Affect Disord. 2023;339:435–442. doi:10.1016/j.jad.2023.07.040
29. BinHeyat MB, Akhtar F, Sultana A, et al. Role of oxidative stress and inflammation in insomnia sleep disorder and cardiovascular diseases: herbal antioxidants and anti-inflammatory coupled with insomnia detection using machine learning. Curr Pharm Des. 2022;28:3618–3636. doi:10.2174/1381612829666221201161636
30. Huang M, et al. Oxidative stress contributes to vascular calcification in patients with chronic kidney disease. J Mol Cell Cardiol. 2020;138:256–268. doi:10.1016/j.yjmcc.2019.12.006
31. Naves M, Rodriguez-Garcia M, Diaz-Lopez JB, Gomez-Alonso C, Cannata-Andia JB. Progression of vascular calcifications is associated with greater bone loss and increased bone fractures. Osteoporos Int. 2008;19:1161–1166. doi:10.1007/s00198-007-0539-1
32. Paccou J, Mentaverri R, Renard C, et al. The relationships between serum sclerostin, bone mineral density, and vascular calcification in rheumatoid arthritis. J Clin Endocrinol Metab. 2014;99:4740–4748. doi:10.1210/jc.2014-2327
33. Xiong M, Liu X, You L, Chen X. Relationship between sleep quality and bone mineral density in urban residents. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2020;49:431–438. doi:10.3785/j.issn.1008-9292.2020.08.01
34. Calvin AD, Covassin N, Kremers WK, et al. Experimental sleep restriction causes endothelial dysfunction in healthy humans. J Am Heart Assoc. 2014;3:e001143. doi:10.1161/JAHA.114.001143
35. Farabi SS, et al. Endothelial dysfunction is related to glycemic variability and quality and duration of sleep in adults with type 1 diabetes. J Cardiovasc Nurs. 2018;33:E21–E25. doi:10.1097/JCN.0000000000000485
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.