Back to Journals » International Journal of Nanomedicine » Volume 14
Poly(lactic-co-glycolic acid) nanoparticle-mediated interleukin-12 delivery for the treatment of diabetic retinopathy
Authors Zeng L ![]() , Ma W, Shi L, Chen X, Wu R, Zhang Y, Chen H, Chen H
, Ma W, Shi L, Chen X, Wu R, Zhang Y, Chen H, Chen H
Received 7 May 2019
Accepted for publication 16 July 2019
Published 8 August 2019 Volume 2019:14 Pages 6357—6369
DOI https://doi.org/10.2147/IJN.S214727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mian Wang
Lina Zeng,1,* Wenbei Ma,1,* Lingyu Shi,1 Xiaohong Chen,1 Rong Wu,1 Yingying Zhang,2 Huaiwen Chen,2 Hui Chen1
1Department of Ophthalmology, Zhujiang Hospital, Southern Medical University, Guangzhou 510282, People’s Republic of China; 2Sunlipo Biotech Research Center for Nanomedicine, Shanghai 201507, People’s Republic of China
*These authors contributed equally to this work
Background: Diabetic retinopathy (DR) is a complication of diabetes that affects the eyes and vision. It is a leading cause of visual impairment and blindness in working-age people. Vascular endothelial growth factor-A (VEGF-A) is a primary initiator and potential mediator of DR. Matrix metalloproteinase-9 (MMP-9) plays a progressive role in the onset and severity of DR. Interleukin-12 (IL-12) is a cytokine of the chemokine family that could reduce the levels of MMP-9 and VEGF-A and suppress tumor angiogenesis. We hypothesize that IL-12 may also have superior therapeutic efficacy against DR. However, protein drugs are prone to degradation by various proteases after drug injection. Therefore, they have short half-lives and low blood concentrations. The objective of this study was to develop IL-12-loaded nanoparticles for long-term and sustained DR treatment.
Methods: IL-12-loaded poly(lactic-co-glycolic acid) (PLGA) nanoparticles (IL-12-PNP) were developed by double emulsion. The characteristics, anti-DR activity, and mechanisms of IL-12-PNP were examined in vitro and in vivo.
Results: The nanoparticles had suitable particle size (∼132.8 nm), drug encapsulation efficiency (∼34.7%), and sustained drug release profile. Compared with IL-12 and blank nanoparticles, IL-12-PNP showed better inhibitory efficacy against VEGF-A and MMP-9 expression in rat endothelial cells and DR mouse retina. Intraocular IL-12-PNP administration significantly reduced retinal damage in DR mice as they presented with increased thickness and decreased neovascularization after treatment.
Conclusion: These data indicate that IL-12-PNP is an effective drug delivery platform for DR therapy. It restores the thickness and reduces neovascularization of the retinas of DR mice.
Keywords: interleukin-12, nanoparticles, angiogenesis, controlled release, diabetic retinopathy
Introduction
Diabetic retinopathy (DR) is a complication of diabetes affecting the eyes and vision. It is caused by damage to the blood vessels in the light-sensitive tissue of the retina.1 About one-third of all patients with diabetes mellitus present with DR of varying degrees of severity. One-third of all DR cases are at very high risk of vision loss.1 DR is a leading cause of visual impairment and blindness in working-age people.1
Angiogenic factors such as vascular endothelial growth factor-A (VEGF-A) may be closely associated with DR pathogenesis.2 VEGF-A is a potent cytokine that increases vascular permeability and stimulates neovascularization in physiological and pathological processes.2 The involvement of VEGF-A in DR pathogenesis has been frequently investigated. Recent studies showed that VEGF-A is a primary initiator of proliferative DR and a potential mediator of nonproliferative DR.3 The Food and Drug Administration (FDA) approved Lucentis® (ranibizumab (anti-VEGF-A antibody) injection; Genentech, Inc., South San Francisco, CA, USA) for DR.4 Matrix metalloproteinases (MMPs) are enzymes requiring metal cations to digest extracellular matrix proteins.5,6 MMP-9 plays a progressive role in DR onset and severity.7 MMP-9 overexpression promotes retinal cell apoptosis which precedes the development of clinically significant DR histopathology.8
Interleukin-12 (IL-12) is a cytokine of the chemokine family secreted by activated inflammatory cells. It has a wide range of biological activities. Recent studies have shown that IL-12 has strong anti-angiogenic and antitumor efficacy.9–11 IL-12 inhibited pathological neovascularization in a rat model of oxygen-induced retinopathy.12 IL-12 treatment downregulated MMP-9 and VEGF-A which, in turn, suppressed tumor angiogenesis.13–15 IL-12 had good therapeutic effects in clinical phase I and phase II trials on melanoma and other tumors.16–18 As IL-12 is potentially anti-angiogenic and has entered several clinical trials, we hypothesize that it may have strong therapeutic efficacy against DR. To the best of our knowledge, the application of IL-12 for the treatment of DR has not been previously reported.
The administration routes for drugs used in the treatment of DR include vitreous and subconjunctival injection.19 However, protein drugs are susceptible to degradation by various proteases after injection. Consequently, they have short half-lives and low blood concentrations.20,21 Certain carriers may significantly increase the half-lives and blood concentration of protein drugs and prolong their action.20–22 Poly(lactic-co-glycolic acid) (PLGA) nanoparticles are highly biocompatibility and safe and have been widely used in sustained drug release systems. Optimization of the ratio of lactic to glycolic acid can extend the drug release time of PLGA nanoparticles to several weeks.23 We hypothesized that IL-12-loaded PLGA nanoparticles could provide long-term and sustained DR treatment.
In the present study, we prepared IL-12-loaded PLGA nanoparticles (IL-12-PNP) to treat DR. IL-12-PNP is expected to prolong the release time and reduce the side effects and number of required doses of IL-12. Here, the characteristics, anti-DR activity, and mechanisms of IL-12-PNP were examined both in vitro and in vivo.
Materials and methods
Polymers, proteins, kits, and reagents
Rat interleukin-12 (IL-12), poly(D,L-lactide-coglycolide) (lactide:glycolide =50:50; MW =30,000–60,000), poly(vinyl alcohol) (PVA; MW =30–70 kDa), streptozotocin, and type II collagenase were purchased from Sigma-Aldrich Corp. (St. Louis, MO, USA). The IL-12 was diluted to 10 μg mL−1 in phosphate-buffered saline (PBS)/0.1% (w/v) murine serum albumin and stored at −70°C prior to use. A micro bovine calf albumin (BCA) protein assay kit, fetal bovine serum (FBS), Dulbecco’s modified Eagle’s medium (DMEM), and SuperSignal West Dura Extended Duration Substrate were obtained from Thermo Fisher Scientific (Waltham, MA, USA). Endothelial cell medium (ECM) was purchased from ScienCell Research Laboratories (Carlsbad, CA, USA). Rat vascular endothelial growth factor-A (VEGF-A) and matrix metallopeptidase-9 (MMP-9) enzyme-linked immunosorbent assay (ELISA) kits, primary antibodies (rabbit anti-rat VEGF-A, MMP-9, vWf, and CD31) and secondary antibodies (horseradish peroxidase (HRP)-linked goat anti-rabbit IgG and Alexa Fluor® 488 goat anti-rabbit IgG) were purchased from Abcam (Cambridge, UK). All other chemicals were of analytical grade and were acquired from Shanghai Sinopharm (Shanghai, China).
Preparation and characterization of IL-12 loaded nanoparticles
IL-12 loaded nanoparticles were prepared by double emulsion as previously described, with slight modification.24 In brief, the initial W1/O (water/oil) emulsion was prepared by dispersing the inner phase (0.2 mL IL-12 solution containing 10% trehalose ((w/v))) into the disperse phase with polymer (3 mL ethyl acetate solution dissolved in 100 mg PLGA polymer) by sonication in an ice bath at 100 W for 60 s. The W1/O emulsion was injected dropwise into 5 mL of 1% (w/v) PVA solution and homogenized at 20,000 g for 5 min to form the W1/O/W2 emulsion. The latter was injected into 50 mL of 0.3% (w/v) PVA solution which was then mechanically stirred for 6 h to evaporate the organic solvent. The residue was washed with PBS and freeze-dried and the nanoparticles were obtained. Drug-free nanoparticles were prepared by adding water instead of IL-12 solution. Hereafter, IL-12-loaded polymeric nanoparticles are referred to as IL-12-PNP and drug-free polymeric nanoparticles are called PNP.
The nanoparticles were dispersed in deionized water and their size and zeta potential were measured with a Zetasizer Nano S (Malvern Instruments, Malvern, UK). Nanoparticle morphology was examined under a transmission electron microscope (TEM; JEOL JEM2100F, JEOL Ltd., Tokyo, Japan). The nanoparticles were stained with 2% (w/v) phosphotungstic acid (PTA).
Drug encapsulation efficacy and nanoparticle loading were evaluated as previously described.24 In brief, 20 mg of nanoparticles were completely dispersed in 10 mL of 2.5% (w/v) SDS/0.04 M NaOH solution. The dispersion was agitated in an orbital shaker at a constant 100 rpm and 37°C to hydrolyze the nanoparticles. The IL-12 concentration was measured with a micro BCA assay kit according to the manufacturer’s instruction. The IL-12 encapsulation efficiency was calculated from the ratio of loaded- to initial IL-12 and the ratio of loaded IL-12 to the total quantity of nanoparticles.
The release of IL-12 from IL-12-PNP was evaluated as described below. In brief, 5 mg of IL-12-PNP was suspended in either PBS or PBS with 10% (w/v) rat serum. The mixtures were placed in centrifuge tubes and gently agitated at 37°C and 100 rpm on an orbital shaker. At designated time points, 0.1 mL of the mixture was removed and centrifuged at 100,000× g for 30 min. The IL-12 concentration in the supernatant was measured by enzyme-linked immunosorbent assay (ELISA). The cumulative rate of release of IL-12 from the nanoparticles was calculated as follows:
(1)
where Mr is the mass of released IL-12 and Mt is the total amount of IL-12.
Animal study
Male Sprague-Dawley (SD) rats (~200 g) were purchased from the Laboratory Animal Center of Southern Medical University (Guangzhou, China). The rats were provided with standard laboratory food, had free access to water, and were kept in an air-conditioned room with a 12-h light/12-h dark cycle. The study was conducted in strict compliance with the Guide for the Care and Use of Laboratory Animals of Southern Medical University (Guangzhou, China). The protocol was approved by the Committee on the Ethics of Animal Experiments of Southern Medical University (Guangzhou, China).
Culture and identification of rat retinal capillary endothelial cells
Rat retinal capillary endothelial cells were isolated and cultured as previously described.25 In brief, retinas were isolated from ten rat eyes, minced into small pieces, washed with PBS, and digested in 5 mL of 0.2% (w/v) type II collagenase at 37°C with agitation for 1 h. The retinal fragment suspension was filtered through a 70-µm cell strainer and centrifuged at 175× g for 10 min. Pellets containing the microvessel fragments were suspended in endothelial cell medium (ECM; ScienCell Research Laboratories, Carlsbad, CA, USA). The suspension was transferred to culture plates pre-coated with 1% (w/v) gelatin and incubated at 37°C in a humidified incubator under a a 5% CO2 atmosphere. The medium was replaced every 2–3 d. Cell passage was conducted by detaching the cells with 0.1% (w/v) trypsin and plating them at a 1:2 split ratio. The cells used in the present study were passaged three to six times.
The expression of vWf and CD31 in the endothelial cells was confirmed by immunofluorescence assay. In brief, the cells were fixed in 4% (w/v) paraformaldehyde (PFA) at 25°C for 20 min, washed with PBS, and blocked with normal goat serum for 1 h. They were then treated with primary antibodies (anti-rat vWf and anti-rat CD31) at 4°C overnight, washed with PBS, and treated with FTIC-labeled anti-rabbit secondary antibodies. The nuclei were stained with 4’,6-diamidino-2-phenylindole (DAPI). The cells were visualized under a fluorescence microscope (Olympus IX71; Olympus, Tokyo, Japan).
Cytokine analysis of rat endothelial cells after treatment
Rat retinal capillary endothelial cells were grown to 50–60% confluence in 12-well culture plates for 15 h before treatment. The cells were then treated with either IL-12 or IL-12-PNP at an equivalent concentration of 5 ng mL−1 IL-12 for 24 h. Saline-treated cells were the negative controls. Fresh medium was added to the cells and they were incubated at 37°C. After various time intervals, the cells were extracted for Western blot analysis and the cytokines in the supernatants were measured by ELISA.
Establishment of a rat diabetic retinopathy model
The diabetic rat model was established by streptozotocin administration as previously described.26 Streptozotocin induces experimental diabetes in rodents as it destroys pancreatic beta islet cells. Within 2 d after a single dose of streptozotocin, the rats presented with hyperglycemia. The control rats received citrate buffer. The diabetic state of the rats was confirmed by daily glucometry. Rats with blood glucose levels >250 mg dL−l were considered diabetic after 24 h. Intraretinal hemorrhage and ischemia were detected in the diabetic rats after 6 mo and were regarded as the pre-proliferative stage of diabetic retinopathy.
Intravitreal injections
After the establishment of the rat diabetic retinopathy model, intravitreal injections were administered as previously described.19 The rats were anesthetized by intramuscular injection of 14 mg kg−1 xylazine and 85 mg kg−1 ketamine. The cornea was penetrated with a 30-gauge needle to which a syringe was attached to deliver IL-12 or IL-12-PNP into the vitreal cavity at an equivalent dose of 100 ng IL-12 per rat. This procedure was performed under an operating microscope. After injection, one drop of triple antibiotic ointment (Equate®; Wal-Mart, Bentonville, AR, USA) was applied to the corneal surface. In vivo assays were conducted at various time intervals. The retina was excised from the rats and homogenized in 1 mL of T-PER tissue lysis buffer (Thermo Fisher Scientific, Waltham, MA, USA). The cytokine levels in the homogenate was measured by ELISA. The retina was also excised for Western blot analysis. Tissues were fixed with 4% PFA (paraformaldehyde), embedded in paraffin, sectioned, immunostained for VEGF-A and MMP-9 or stained with hematoxylin and eosin (H&E), and examined under a microscope.
Western blot
Protein extraction from cells or retinas was conducted with RIPA (radioimmunoprecipitation assay) buffer in PBS pH 7.4 comprising 1% (w/v) Triton X-100, 5 mM EDTA, 5 mg mL−l n-ethylmaleimide, and protease inhibitor cocktail. The protein was separated by sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) and transferred to PVDF (polyvinylidene fluoride) membrane which was then blocked with 5% nonfat milk in TBST (Tris-buffered saline and polysorbate- (Tween-) 20). Primary anti-rat VEGF-A and MMP-9 and secondary HRP-linked goat anti-rat IgG antibodies were added to the PVDF membrane which was then incubated overnight at 4°C. Beta-actin antibody was used as an internal control. The protein bands were visualized with SuperSignal West Dura Extended Duration Substrate (Thermo Fisher Scientific, Waltham, MA, USA) and a ChemiDoc™ MP imaging system (Bio-Rad Laboratories, Hercules, CA, USA).
Measurement of VEGF-A and MMP-9 by ELISA
The concentrations of VEGF-A and MMP-9 were determined using VEGF-A and MMP-9 ELISA kits. In brief, all reagents, samples, and standards were prepared per kit manufacturer instructions and added to each well followed by biotinylated labeled detector antibody. After incubation at room temperature, the solutions were aspirated, the wells were rinsed, and streptavidin-HRP mix was added to them. After incubation at 25°C, the solutions were aspirated and the wells were rinsed. TMB (3,3’,5,5’-tetramethylbenzidine) solution was added dropwise to each well until color developed and another solution was added to stop the reaction. Absorbances were measured at 450 nm (primary wavelength) and at 630 nm (reference wavelength).
Immunohistochemical assays
The immunohistochemical assay was conducted according to a standard protocol. In brief, paraffin-embedded tissue sections were dewaxed and antigens were retrieved with antigen repair solution (pH 9.0) containing ethylenediaminetetraacetic acid (EDTA). Endogenous peroxidase was blocked by immersing the sections in 3% (w/v) hydrogen peroxide solution. The tissues sections were blocked with 3% (w/v) bovine serum albumin (BSA) at room temperature for 30 min. The primary antibodies (rabbit anti-rat VEGF-A or rabbit anti-rat MMP-9) were added to the tissue sections which were incubated overnight at 4°C. The secondary antibody (HRP-labeled goat anti-rabbit) was added to the tissue sections which were incubated for 1 h at room temperature. The 3,3’-diaminobenzidine (DAB) solution was added and the nuclei in the tissue sections were counterstained. The tissue sections were also counterstained with hematoxylin and eosin (H&E). Finally, the tissue sections were dehydrated, sealed with neutral gum, and observed under a microscope. The images were photographed at 40× magnification under a light microscope (Axiovert; Carl Zeiss, Inc., Chester, VA, USA) fitted with a digital color camera.
Retinal histology
Rat eyes were excised, enucleated, immobilized with 4% (w/v) paraformaldehyde, embedded with paraffin, sliced into 5-μm sections, and stained with H&E. Microphotographs were taken at 40× under an Axiovert (Carl Zeiss, Inc., Chester, VA, USA) fitted with a digital color camera. At a distance of 0.5 mm ventrally and dorsally from the optic disk, total retinal thickness was measured at 1.0–1.5 mm (central) and 3.0–3.5 mm (peripheral) from the optic disk. To obtain representative data, nine sections per eye were captured and their thicknesses were averaged.
Quantitative assessment of retinal neovascularization
Rat eyes were excised, enucleated, immobilized with 4% (w/v) paraformaldehyde, embedded with paraffin, sliced into 5-μm sections, and stained with H&E to assess retinal vasculature via light microscopy (Axiovert; Carl Zeiss, Inc., Chester, VA, USA). Vascular lumens were counted on the vitreal side of the inner limiting membrane in nine sections per eye and averaged. The average number of intravitreal vessels per section was determined for each group.
Statistics
SPSS v. 13.0 (IBM Corp., Armonk, NY, USA) was used to analyze the data generated in this study. Student’s non-paired t-tests compared the normally distributed differences between pairs of groups. One-way ANOVA and Newman-Keuls post-hoc tests were run to compare differences among ≥3 groups. P<0.05 was considered statistically significant.
Results
Development and characterization of IL-12-PNP
We encapsulated IL-12 in the PLGA nanoparticles by double emulsion (Figure 1) as IL-12 is a hydrophilic protein. In this technique, the larger PLGA droplets engulf the smaller dispersed IL-12 to encapsulate them in nanoparticles. In the single emulsion method, the drug would accumulate in the external aqueous phase and be rapidly released.24,27
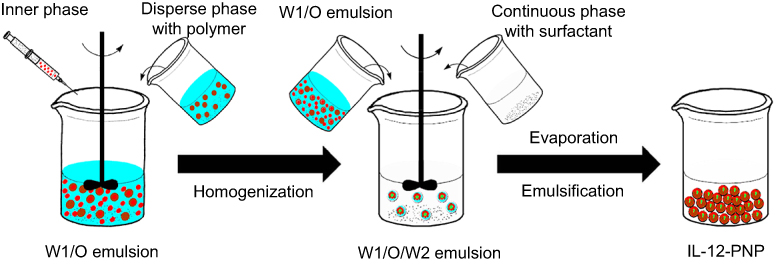 |
Figure 1 Preparation of IL-12 loaded nanoparticles (IL-12-PNP). IL-12-PNP was prepared by the double emulsion method. In brief, the initial W1/O (water/oil) emulsion was prepared by dispersing the inner phase (IL-12 solution) via sonication into the disperse phase with ethyl acetate solution dissolved in PLGA polymer. The W1/O emulsion was injected into PVA solution to form the W1/O/W2 emulsion which was then mechanically stirred to evaporate the organic solvent, washed, and freeze-dried to yield the final nanoparticles. |
Characteristics of the nanoparticles are shown in Figure 2. Nanoparticle morphology was examined by TEM (Figure 2A). Negative staining with PTA revealed that the nanoparticles had a smooth surface morphology, round shape, and diffuse distribution. As shown in Figure 2B, IL-12-PNP was 132.8 nm in diameter and had a zeta potential of −31 mv. The small polydispersity index (PDI) of the nanoparticles (0.15) indicated that they had a narrow size distribution. The blank PNP nanoparticles had sizes, zeta potentials, and PDI similar to those for IL-12-PNP. The encapsulation efficacy (EE) of IL-12 was 34.7% and drug loading was 1.9%. The drug release profile is a critical parameter reflecting the process by which the drug loaded in the delivery system is released in the body. Figure 2C shows that IL-12-PNP had an Il-12 burst release within the first 24 h. About 50% of the IL-12 was released from the nanoparticles in PBS or PBS with 10% (w/v) rat serum. The release of IL-12 reached ~90% over the next 216 h. Thus, IL-12-PNP steadily and stably releases IL-12 over a long period. IL-12-PNP released IL-12 more rapidly in PBS with 10% (w/v) rat serum than in PBS alone. Therefore, serum may destabilize the nanoparticle structure and facilitate the release of IL-12.
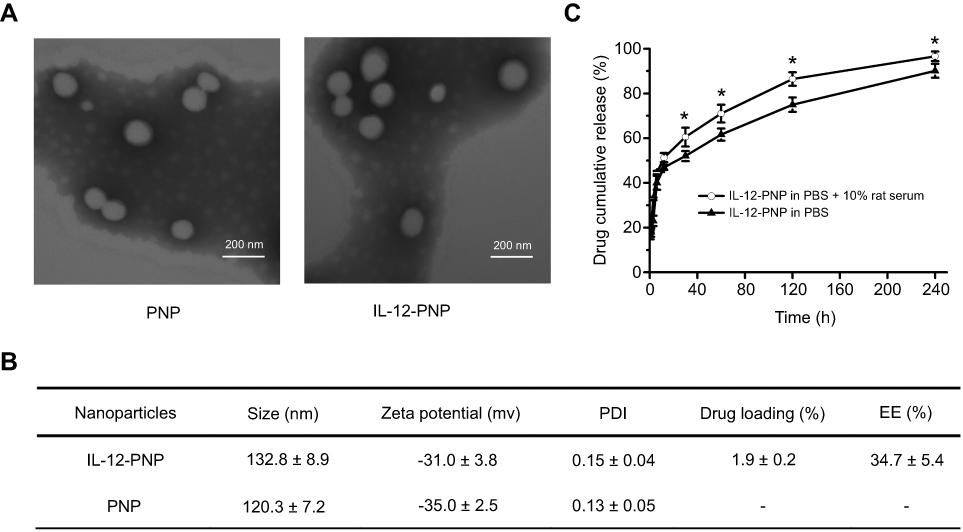 |
Figure 2 Nanoparticle characterization. (A) Morphology of the nanoparticles was observed under a transmission electron microscope. Bar =200 nm. (B) Nanoparticle size, zeta potential, polydispersity index (PDI), drug loading, and encapsulation efficiency (EE). Data are mean ± SD (n=3). (C) Drug release profile of IL-12-PNP in PBS or PBS with 10% (w/v) rat serum. Groups were compared with non-paired Student’s t-tests. *P<0.05. Data are mean ± SD (n=3). |
Analysis of cytokines in rat endothelial cells
Rat endothelial cells present with a cobblestone morphology under an inverted microscope (Figure S1). Expression of the endothelial markers CD31 and vWF was measured by immunofluorescence assay. As shown in Figure S1, CD31 and vWF were moderately expressed in rat endothelial cells.
The rat endothelial cells were treated with IL-12 or IL-12-PNP and their cytokine (MMP-9 and VEGF-A) levels were measured by ELISA and Western blot (Figure 3). On day 1 after the IL-12 treatment, MMP-9 significantly decreased from 650 pg mL−1 to 250 pg mL−1 whereas the blank nanoparticles (PNP) had no effect on MMP-9 concentration (Figure 3A). Similar results were obtained for MMP-9 in response to IL-12-PNP treatment. On days 3 and 7, the MMP level of the IL-12-PNP group was significantly lower than that of the IL-12 group (P<0.05). Similar results were obtained for VEGF-A in response to the IL-12, PNP, and IL-12-PNP treatments (Figure 3B). On day 7, expression of MMP-9 and VEGF-A in rat endothelial cells was evaluated by Western blot. As shown in Figure 3C, PNP had no effect on the expression of MMP-9 or VEGF-A. After treatment with IL-12, MMP-9 and VEGF-A levels decreased but IL-12-PNP treatment further reduced the levels of these cytokines. Thus, IL-12-PNP effectively downregulates the angiogenic factors (VEGF and MMP-9) in rat endothelial cells in a sustained manner.
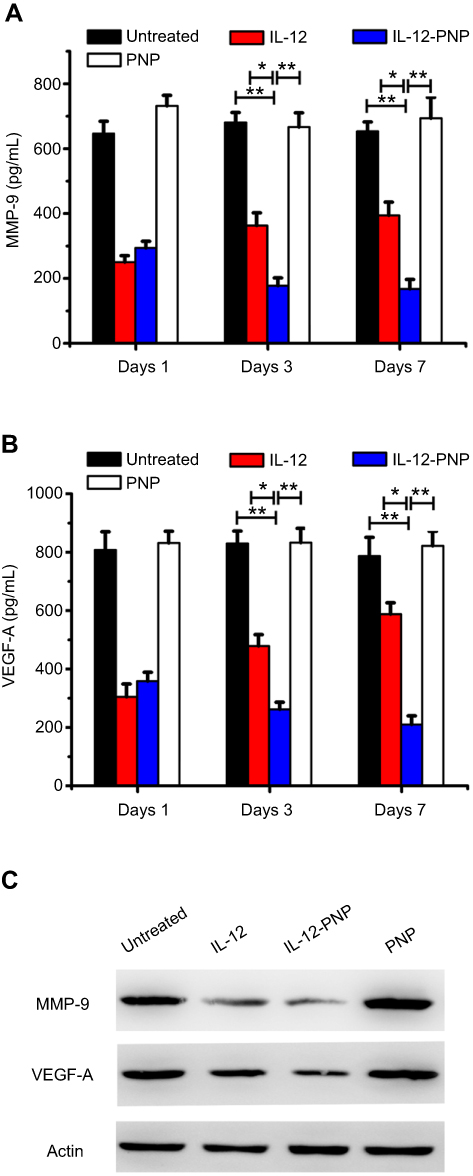 |
Figure 3 Measurement of cytokines VEGF-A and MMP-9 in rat endothelial cells after in vitro treatment. Cells were treated with IL-12 or IL-12-PNP at an equivalent concentration of 5 ng mL−1 IL-12 for 24 h. Saline-treated cells were negative controls. Fresh medium was added to the cells and they were incubated at 37°C. After various time intervals, the cytokines in the supernatant were analyzed by ELISA (A and B). One-way ANOVA and Newman-Keuls post-hoc test were used to determine differences among ≥3 groups. *P<0.05; **P<0.05. Data are mean ± SD (n=3). On day 7, cellular protein was extracted for Western blot analysis (C). Representative Western blot from three independent experiments. |
Analysis of cytokines in rat retina after intravitreal injections
After the intravitreal injections, the cytokines were analyzed in rat retinas by ELISA and Western blot (Figure 4). The expression levels of MMP-9 and VEGF-A in the diabetic rat model treated with saline were significantly higher than those in the healthy rat (control). Therefore, MMP-9 and VEGF-A may contribute to DR pathogenesis. As shown in Figure 4A, IL-12 treatment significantly decreased MMP-9 on day 1 but the level of MMP-9 gradually increased by days 3 and 7. For this reason, the therapeutic efficacy of IL-12 diminished over time. In contrast, IL-12-PNP consistently and stably downregulated MMP-9. On days 3 and 7, the MMP level of the IL-12-PNP group was significantly lower than that of the IL-12 group (P<0.05). Similar results were obtained for VEGF-A (Figure 4B). By day 7, the results obtained from Western blot analysis were consistent with those acquired by ELISA (Figure 4C). After IL-12 treatment, MMP-9 and VEGF-A were downregulated but the IL-12-PNP treatment lowered the levels of these cytokines even more so. Thus, IL-12-PNP effectively downregulates the angiogenic factors (VEGF and MMP-9) in a diabetic rat retina model in a sustained manner.
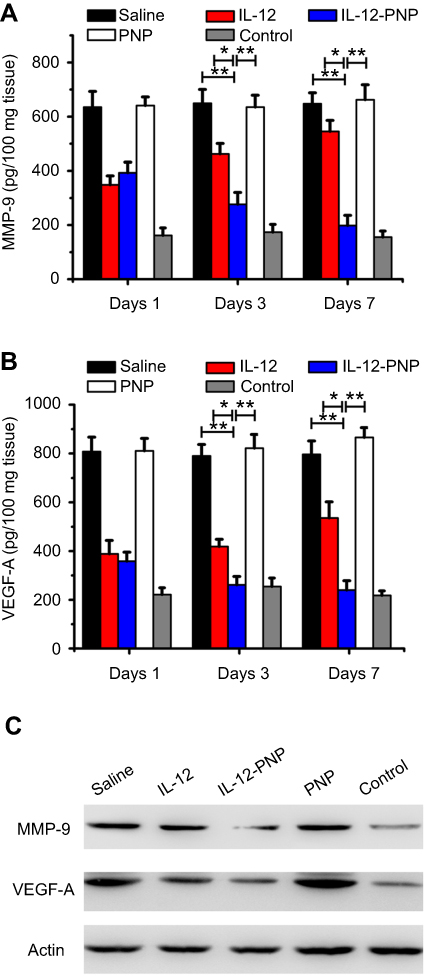 |
Figure 4 Measurement of cytokines in rat retina after intravitreal IL-12 or IL-12-PNP injections. After various time periods, cytokines were analyzed by ELISA (A and B). One-way ANOVA and Newman-Keuls post-hoc test were used to determine differences among ≥3 groups. *P<0.05; **P<0.05 . Data are mean ± SD (n=3). On day 7, retinal tissue protein was extracted for Western blot analysis (C). Representative Western blot from three independent experiments. |
Immunohistochemical analysis of retinal cytokines
Seven days after the intravitreal injections, MMP-9 and VEGF-A were measured in rat retina by immunohistochemistry. As shown in Figure 5, the expression level of MMP-9 in the saline-treated diabetic rat model was significantly higher than that in the healthy rat (control). IL-12 treatment downregulated MMP-9 but IL-12-PNP lowered its level even more so. PNP had no effect on MMP-9 expression. Similar results were obtained for VEGF-A (Figure 6). IL-12 treatment downregulated VEGF-A but IL-12-PNP lowered its level even more so. Therefore, IL-12-PNP effectively downregulates VEGF and MMP-9 in the retina of a diabetic rat model.
 |
Figure 5 Analysis of VEGF-A expression in rat retina 7 d after intravitreal IL-12 or IL-12-PNP injections. Immunohistochemical assays were performed on tissue sections stained with rabbit anti-rat VEGF-A antibody and hematoxylin-eosin (H&E). Bar =100 μm. |
 |
Figure 6 Analysis of MMP-9 expression in rat retina 7 d after intravitreal IL-12 or IL-12-PNP injections. Immunohistochemical assays were performed on tissue sections stained with rabbit anti-rat MMP-9 antibody and hematoxylin-eosin (H&E). Bar =100 μm. |
Histology
Rat retinal histology was examined by H&E staining (Figure 7A). In the normal control group, the retinal layers were clear and their cell morphologies were equal and organized. In the saline-treated diabetic group, however, the ganglion cell layer (GCL) was markedly thinner than that of the healthy control and was accompanied by obvious neovascularization and apoptosis. Seven days after intravitreal IL-12 injection, the GCL layer was thickened and its neovascularization had regressed. Intravitreal IL-12-PNP injection had even stronger effects (GCL thickening and reduction of neovascularization) than intravitreal IL-12 after seven days. However, no substantial difference was detected between the PNP and diabetic groups. Therefore, PNP had no therapeutic efficacy against DR in diabetic rats. Retinal thickness was precisely measured to evaluate the therapeutic efficacy of IL-12 and IL-12-PNP (Figure 7B). Retinal thickness in the saline-treated diabetic group (98.2±2.9 μm) was significantly less than that of the healthy controls (127.2±3.2 μm; P<0.05). Intravitreal IL-12-PNP administration was highly effective at protecting the retina. The mean retinal thickness for this treatment group was 124.2±4.2 μm which resembles that of the healthy controls. Retinal thickness in the IL-12-PNP group was higher than that in the IL-12 group (103.2±4.5 μm; P<0.05). Thus, IL-12-PNP was more efficacious for DR treatment than IL-12. To quantify intravitreal neovascularization, the vascular lumens were counted on the vitreal side of the inner limiting membrane (Figure 8). The number of vascular lumens in the saline-treated diabetic rats was greater than that in the healthy controls (P<0.05). The IL-12 treatment decreased the number of vascular lumens (P<0.05) whereas the IL-12-PNP treatment reduced it even more so (P<0.01). PNP had no effect on the number of vascular lumens. Thus, PNP does not influence retinal neovascularization in diabetic rats. Overall, IL-12-PNP exerted superior therapeutic efficacy against DR as indicated by the restored thickness and reduced neovascularization of the retina in diabetic rats.
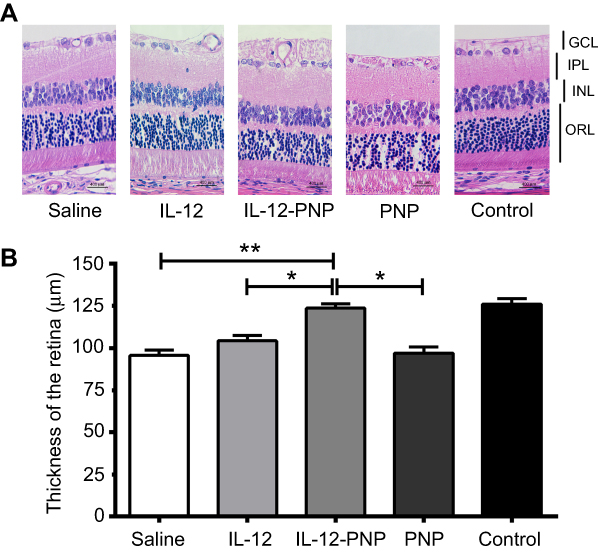 |
Figure 7 Retinal histology on day 7 after intravitreal IL-12 or IL-12-PNP injections. Each group consisted of six mice. (A) Representative photomicrographs of rat retina stained with H&E. Retinal layers are indicated on the left part of the figure as follows: GCL, ganglion cell layer; IPL, inner plexiform layer; INL, inner nuclear layer; ORL, outer retinal layer. Bar =400 μm. (B) Thicknesses of the total retina. One-way ANOVA and Newman-Keuls post-hoc test were used to determine differences among ≥3 groups. *P<0.05; **P<0.05. Data are mean ± SD (n=12). |
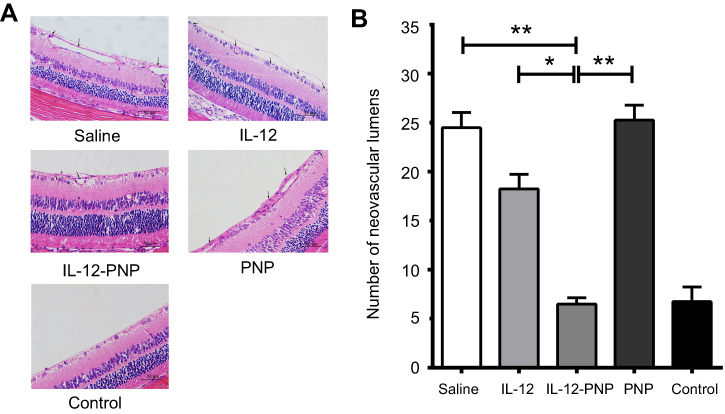 |
Figure 8 Quantitative analysis of retinal neovascularization by counting vascular lumens on day 7 after intravitreal IL-12 or IL-12-PNP injections. Each group consisted of six mice. (A) H&E-stained sections. Vascular lumens of new vessels growing into the vitreous humor are indicated by black arrows. Bar =50 μm. (B) Data in each column are mean ± SD (n=12). One-way ANOVA and Newman-Keuls post-hoc test were used to determine differences among ≥3 groups. *P<0.05; **P<0.05. |
Discussion
DR is a major cause of visual impairment and blindness in working-age people. The annual incidence of DR ranges from 2.2–12.7%.28 Anti-VEGF therapies have entered clinical DR trials but demonstrated limited therapeutic efficacy.28,29 As IL-12 is potently anti-angiogenic, we integrated it into PNP nanoparticles to create a sustained and topical controlled-release system. Our results confirmed that IL-12-PNP provided sustained release of IL-12, downregulated the angiogenic factors VEGF-A and MMP-9, and reduced DR angiogenesis and retinal damage in diabetic rats.
The safety of drug delivery systems is crucial for their clinical application.30 Poor degradability and biocompatibility of drug delivery systems severely limit their potential clinical use.30 In the present study, IL-12 was encapsulated in nanoparticles composed of PLGA which is biocompatible and approved by the FDA. IL-12 has demonstrated good patient tolerance in clinical trials. However, the safety of IL-12-PNP must be confirmed in future investigations.
The identification of VEGF-A as a key regulator of DR pathogenesis has revolutionized the treatment of this condition. Intravitreal injection of anti-VEGF antibody (bevacizumab; Avastin®; Genentech, Inc., South San Francisco, CA, USA) for DR treatment has entered clinical trials.31,32 MMP-9 is associated with DR severity and plays a crucial role its pathogenesis as reflected by serum MMP-9 levels.6,7 IL-12 may downregulate MMP-9 and VEGF and suppress tumor angiogenesis.13–15 In the present study, the selection of IL-12 as the anti-DR drug in our nanoparticle formulation was of vital importance for satisfactory IL-12-PNP activity. IL-12 is a potent cytokine with a wide range of biological activities. It has strong anti-angiogenic efficacy in various disease models such as tumors and retinopathy.9–12 Moreover, the anti-angiogenic mechanisms of IL-12 have been elucidated and include VEGF and MMP-9 downregulation.12,33,34 The relative safety of IL-12 in clinical trials, as indicated by good patient tolerance, suggests that IL-12 is promising in the treatment of DR.
A practical approach towards the reduction of side effects and enhancement of the therapeutic efficacy of drugs is to alter their formulations and administration routes.30 As IL-12 has multiple biological activities, systemic in vivo IL-12 application of IL-12 could be toxic. In contrast, topical IL-12 administration is comparatively less harmful.16–18 In clinical trials, then, intratumoral injections of IL-12 plasmid DNA, liposome-encapsulated IL-12, IL-12-expressing Semliki virus, and fibroblasts expressing IL-12 were administered.35–37 All of these presented with good patient tolerance. As nanotechnology may facilitate ocular drug delivery,38,39 we constructed IL-12-PNP for the topical application and sustained release of IL-12. In addition, PLGA protects proteins against degradation and stabilizes their structure.40 We demonstrated that IL-12-PNP furnished sustained release of IL-12. In vitro, the latter showed anti-angiogenic efficacy comparable to that of IL-12-PNP at day 1 according to the diminished levels of VEGF-A and MMP-9. Nevertheless, the anti-angiogenic effect of the IL-12-PNP treatment was significantly stronger than that of the IL-12 treatment at days 3 and 7. In vivo, the therapeutic efficacy of IL-12-PNP was also greater than that of IL-12 as the levels of MMP-9 and VEGF-A were significantly lower in response to the IL-12-PNP treatment than the IL-12 treatment at days 3 and 7. Saline-treated diabetic rats presented with a significant reduction in retinal thickness and increase in retinal angiogenesis whereas those treated with IL-12-PNP treatment had relatively less retinal damage and angiogenesis. Thus, IL-12-PNP has strong efficacy against DR.
In addition to the IL-12/VEGF/MMP-9 pathway, other mechanisms are involved in inflammation associated with DR pathogenesis. Numerous systemic and local inflammatory cytokines participate and collaborate in DR. These include vascular adhesion molecules (VCAM-1, ICAM-1, E-selectin, and sVAP), proinflammatory cytokines (TNF-α, IL-1α, 1β, 6, 8, and HMGB1) and proinflammatory/angiogenic chemokines (CP-1, MIF, SDF-1, and fractalkine).41 The cellular surface receptor also plays a critical role in DR. The early phases of DR are characterized by the loss of retinal pericytes concurrent with the inflammatory process. An important link between the P2X7 receptor (P2X7R) and inflammation has been demonstrated. P2X7R is a potential pharmacological target in DR.42 Thus, we must investigate the effects of IL-12 on the other pathways involved in DR pathogenesis.
The present study elucidated the mechanism of the anti-angiogenic activity of IL-12-PNP. After it is injected intravitreally, the polymer matrix of IL-12-PNP degrades and releases IL-12 in a sustained manner. When IL-12 is released, it downregulates the angiogenic factors VEGF and MMP-9 and reduces angiogenesis and retinal damage in DR. In contrast, injected IL-12 is rapidly eliminated in circulation. Therefore, this drug administration approach offers poor therapeutic efficacy against DR.
Conclusion
DR is a leading cause of visual impairment and blindness in working-age people. Here, we prepared IL-12-PNP and tested it as a sustained and topical controlled IL-12 release system. Our results confirmed that IL-12-PNP provided the sustained release of IL-12 and had superior therapeutic efficacy against DR relative to IL-12 alone. Thus, IL-12-PNP may be an effective candidate for the clinical treatment of DR.
Acknowledgment
This work was supported by the National Natural Science Foundation of China (Project No. 81802714).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis (Lond). 2015;2:17. doi:10.1186/s40662-015-0026-2
2. Kusuhara S, Fukushima Y, Ogura S, Inoue N, Uemura A. Pathophysiology of diabetic retinopathy: the old and the new. Diabetes Metab J. 2018;42(5):364–376. doi:10.4093/dmj.2018.0182
3. Mahdy RA, Nada WM, Hadhoud KM, El-Tarhony SA. The role of vascular endothelial growth factor in the progression of diabetic vascular complications. Eye (Lond). 2010;24(10):1576–1584. doi:10.1038/eye.2010.7
4. Yang CS, Hung KC, Huang YM, Hsu WM. Intravitreal bevacizumab (Avastin) and panretinal photocoagulation in the treatment of high-risk proliferative diabetic retinopathy. J Ocul Pharmacol Ther. 2013;29(6):550–555. doi:10.1089/jop.2012.0202
5. Kim Y-S, Joh TH. Matrix metalloproteinases, new insights into the understanding of neurodegenerative disorders. Biomol Ther. 2012;20(2):133–143. doi:10.4062/biomolther.2012.20.2.133
6. Stamenkovic I. Extracellular matrix remodelling: the role of matrix metalloproteinases. J Pathol. 2003;200(4):448–464. doi:10.1002/path.1400
7. Kowluru RA. Role of matrix metalloproteinase-9 in the development of diabetic retinopathy and its regulation by H-Ras. Invest Ophthalmol Vis Sci. 2010;51(8):4320–4326. doi:10.1167/iovs.09-4851
8. Suarez S, McCollum GW, Jayagopal A, Penn JS. High glucose-induced retinal pericyte apoptosis depends on association of GAPDH and Siah1. J Biol Chem. 2015;290(47):28311–28320. doi:10.1074/jbc.M115.682385
9. Airoldi I, Di Carlo E, Cocco C, et al. Endogenous IL-12 triggers an antiangiogenic program in melanoma cells. Proc Natl Acad Sci USA. 2007;104(10):3996–34001. doi:10.1073/pnas.0609028104
10. Gafner V, Trachsel E, Neri D. An engineered antibody-interleukin-12 fusion protein with enhanced tumor vascular targeting properties. Int J Cancer. 2006;119(9):2205–2212. doi:10.1002/ijc.22101
11. Nisari M, Ulger H, Unur E, Karaca O, Ertekin T. Effect of interleukin 12 (IL-12) on embryonic development and yolk sac vascularisation. Bratisl Lek Listy. 2014;115(9):532–537.
12. Zhou Y, Yoshida S, Kubo Y, et al. Interleukin-12 inhibits pathological neovascularization in rat model of oxygen-induced retinopathy. Sci Rep. 2016;6:28140. doi:10.1038/srep28140
13. Roupakia E, Markopoulos GS, Kolettas E. IL-12-mediated transcriptional regulation of matrix metalloproteinases. Biosci Rep. 2018;38(3):
14. Vecchio MD, Emilio B, Canova S, et al. Interleukin-12: biological properties and clinical application. Clin Cancer Res. 2007;13(16):4677–4685. doi:10.1158/1078-0432.CCR-07-0776
15. Strasly M, Cavallo F, Geuna M, et al. IL-12 inhibition of endothelial cell functions and angiogenesis depends on lymphocyte-endothelial cell cross-talk. J Immunol. 2001;166(6):3890–3899. doi:10.4049/jimmunol.166.6.3890
16. Gollob JA, Mier JW, Veenstra K, et al. Phase I trial of twice-weekly intravenous interleukin 12 in patients with metastatic renal cell cancer or malignant melanoma: ability to maintain IFN-gamma induction is associated with clinical response. Clin Cancer Res. 2000;6:1678–1692.
17. Alatrash G, Hutson TE, Molto L, et al. Clinical and immunologic effects of subcutaneously administered interleukin-12 and interferon alfa-2b: phase I trial of patients with metastatic renal cell carcinoma or malignant melanoma. J Clin Oncol. 2004;22(14):2891–2900. doi:10.1200/JCO.2004.08.040
18. Younes A, Pro B, Robertson MJ, et al. Phase II clinical trial of interleukin-12 in patients with relapsed and refractory non-Hodgkin’s lymphoma and Hodgkin’s disease. Clin Cancer Res. 2004;10(16):5432–5438. doi:10.1158/1078-0432.CCR-04-1002
19. Mitra RN, Nichols CA, Guo J, et al. Nanoparticle-mediated miR200-b delivery for the treatment of diabetic retinopathy. J Control Release. 2016;236:31–37. doi:10.1016/j.jconrel.2016.06.020
20. Gao J, Kou G, Wang H, et al. PE38KDEL-loaded anti-HER2 nanoparticles inhibit breast tumor progression with reduced toxicity and immunogenicity. Breast Cancer Res Treat. 2009;115(1):29–41. doi:10.1007/s10549-008-0043-0
21. Gao J, Zhong W, He J, et al. Tumor-targeted PE38KDEL delivery via PEGylated anti-HER2 immunoliposomes. In J Pharm. 2009;374(1–2):145–152.
22. Gao J, Kou G, Chen H, et al. Treatment of hepatocellular carcinoma in rats with PE38KDEL type I mutant-loaded poly(lactic-co-glycolic acid) nanoparticles conjugated with humanized SM5-1 F(ab’) fragments. Mol Cancer Ther. 2008;7:3399–3407. doi:10.1158/1535-7163.MCT-07-2370
23. Gao J, Xia Y, Chen H, et al. Polymer-lipid hybrid nanoparticles conjugated anti-EGFR antibody for targeted drug delivery to hepatocellular carcinoma. Nanomedicine (Lond). 2014;9(2):279–293. doi:10.2217/nnm.13.20
24. Chen H, Gao J, Lu Y, et al. Preparation and characterization of PE38KDEL-loaded anti-HER2 nanoparticles for targeted cancer therapy. J Control Release. 2008;128:209–216. doi:10.1016/j.jconrel.2008.03.010
25. Fan Y, Qiao Y, Huang J, Tang M. Protective effects of panax notoginseng saponins against high glucose-InducedOxidative Injury in Rat Retinal Capillary Endothelial Cells. Evid Based Complement Alternat Med.2016 ;2016:5326382. doi:10.1155/2016/5326382
26. Amadio M, Bucolo C, Leggio GM, Drago F, Govoni S, Pascale A. The PKCbeta/HuR/VEGF pathway in diabetic retinopathy. Biochem Pharmacol. 2010 Oct 15;80(8):1230-7. doi:10.1016/j.bcp.2010.06.033
27. Chen D, Pan X, Xie F, et al. Codelivery of doxorubicin and elacridar to target both liver cancer cells and stem cells by polylactide-co-glycolide/d-alpha-tocopherol polyethylene glycol 1000 succinate nanoparticles. In J Nanomedicine. 2018;13:6855–6870.
28. Sang DN, D’Amore PA. Is blockade of vascular endothelial growth factor beneficial for all types of diabetic retinopathy? Diabetologia. 2008;51(9):1570–1573. doi:10.1007/s00125-008-1078-9
29. Gonzalez VH, Campbell J, Holekamp NM, et al. Early and long-term responses to anti-vascular endothelial growth factor therapy in diabetic macular edema: analysis of protocol I data. Am J Ophthalmol. 2016;172:72–79. doi:10.1016/j.ajo.2016.09.012
30. Gao J, Li W, Guo Y, Feng SS. Nanomedicine strategies for sustained, controlled and targeted treatment of cancer stem cells. Nanomedicine (Lond). 2016;11(24):3261–3282. doi:10.2217/nnm-2016-0233
31. Bahrami B, Hong T, Gilles MC, Chang A. Anti-VEGF therapy for diabetic eye diseases. Asia Pac J Ophthalmol (Phila). 2017;6(6):535–545.
32. Uemura A. Pharmacologic management of diabetic retinopathy. J Biochem. 2018;163(1):3–9. doi:10.1093/jb/mvy010
33. Wong RJ, Chan MK, Yu Z, et al. Angiogenesis inhibition by an oncolytic herpes virus expressing interleukin 12. Clin Cancer Res. 2004;10(13):4509–4516. doi:10.1158/1078-0432.CCR-04-1002
34. Sgadari C, Angiolillo AL, Tosato G. Inhibition of angiogenesis by interleukin-12 is mediated by the interferon-inducible protein 10. Blood. 1996;87(9):3877–3882.
35. Mahvi DM, Henry MB, Albertini MR, et al. Intratumoral injection of IL-12 plasmid DNA–results of a phase I/IB clinical trial. Cancer Gene Ther. 2007;14(8):717–723. doi:10.1038/sj.cgt.7701064
36. Ren H, Boulikas T, Lundstrom K, et al. Immunogene therapy of recurrent glioblastoma multiforme with a liposomally encapsulated replication-incompetent Semliki forest virus vector carrying the human interleukin-12 gene–a phase I/II clinical protocol. J Neurooncol. 2003;64(1–2):147–154. doi:10.1007/BF02700029
37. Kang WK, Park C, Yoon HL, et al. Interleukin 12 gene therapy of cancer by peritumoral injection of transduced autologous fibroblasts: outcome of a phase I study. Hum Gene Ther. 2001;12(6):671–684. doi:10.1089/104303401753153974
38. Bucolo C, Drago F, Salomone S. Ocular drug delivery: a clue from nanotechnology. Front Pharmacol. 2012;3:188. doi:10.3389/fphar.2012.00188
39. Musumeci T, Bucolo C, Carbone C, Pignatello R, Drago F, Puglisi G. Polymeric nanoparticles augment the ocular hypotensive effect of melatonin in rabbits. Int J Pharm. 2013;440(2):135–140. doi:10.1016/j.ijpharm.2012.10.014
40. Malik A, Gupta M, Mani R, Bhatnagar R. Single-dose Ag85B-ESAT6-loaded poly(lactic-co-glycolic acid) nanoparticles confer protective immunity against tuberculosis. Int J Nanomedicine. 2019;14:3129–3143. doi:10.2147/IJN.S198376
41. Semeraro F, Cancarini A, dell’Omo R, Rezzola S, Romano MR, Costagliola C. Diabetic retinopathy: vascular and inflammatory disease. J Diabetes Res. 2015;2015:582060. doi:10.1155/2015/815839
42. Platania CBM, Giurdanella G, Di Paola L, et al. P2X7 receptor antagonism: implications in diabetic retinopathy. Biochem Pharmacol. 2017;138:130–139. doi:10.1016/j.bcp.2017.05.001
Supplementary material
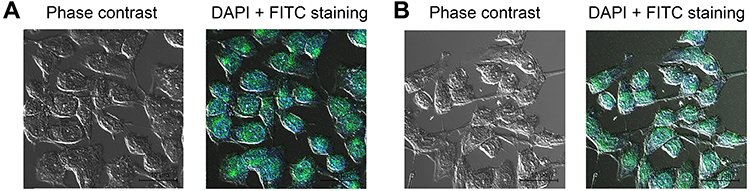 |
Figure S1 The expression of vWf and CD31 on endothelial cells was confirmed by the immunofluorescence assay. The cells were treated with the first antibodies (anti-rat vWf and anti-rat CD31 antibodies), and treated with FTIC-labeled anti-rabbit secondary antibodies. 4’,6-diamidino-2-phenylindole (DAPI) was used to stain the nuclei. (A) vWf staining. (B) CD31 staining. Bars represent 10 μm. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.