Back to Journals » Psychology Research and Behavior Management » Volume 12
Polycystic Ovary Syndrome in adolescents: a qualitative study
Authors Saei Ghare Naz M, Ramezani Tehrani F, Ozgoli G
Received 5 March 2019
Accepted for publication 1 July 2019
Published 22 August 2019 Volume 2019:12 Pages 715—723
DOI https://doi.org/10.2147/PRBM.S207727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Marzieh Saei Ghare Naz,1 Fahimeh Ramezani Tehrani,2 Giti Ozgoli3
1Student Research Committee, Department of Midwifery and Reproductive Health, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Reproductive Endocrinology Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 3Department of Midwifery and Reproductive Health, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Correspondence: Giti Ozgoli
Department of Midwifery and Reproductive Health, School Of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Opposite to Rajaee Heart Hospital, Cross of Vali-Asr and Neiaiesh Highway, Vali-Asr Avenue, 19968-35119 Tehran, Iran
Tel/Fax +98 218 820 2512
Email [email protected]
Background: Adolescents with Polycystic Ovary Syndrome (PCOS) use different coping strategies to confront the challenges of this disorder. Various studies extracted coping strategies amongst adult women with PCOS, but regarding the mental difference between adults and adolescents, specific study was conducted to gain a deep understanding of how adolescents cope to the many health issues they experience.
Methods: Fifteen adolescents aged 13–19 years with PCOS participated in comprehensive individual interviews with goal-oriented, semi-structured questions. Sampling was purposive and continued until data saturation was reached. Data were analyzed using the thematic analysis technique. The validity of the data was verified through measures including credibility, transferability, dependability, confirmability and authenticity.
Results: The analysis of the data helped extract the main theme of the research as “dealing with PCOS”. The main theme consisted of three themes and 12 sub-theme: (1) Escaping the problem (sub-themes: Adopting a forgetting mindset, and concealment and minimization of the disorder); (2) Depressive mood (sub-themes: Poor self-perception and low self-esteem, isolation, sleep disturbances, passive aggressive behavior, emotional turmoil, feelings of humiliation, and adolescents’ perceptions); and (3) Coping with the disease (sub-themes: Recovery of health, positive thinking, hope for recovery).
Conclusion: In this study, the adolescents with PCOS showed a coping response to their disorder in the form of problem-solving, developing a depressive mood or adjusting to the disorder. Recognizing the mental health needs of these adolescents and improving their quality of life require the identification of ways through which they deal with PCOS.
Keywords: polycystic ovary syndrome, adolescents, qualitative research
Introduction
Polycystic Ovary Syndrome (PCOS) is a multifactorial disorder caused by interactions between genetic, environmental and intrauterine factors.1 Various studies have reported the prevalence of this syndrome in adolescence as 9% to 15%.2–4 Based on the available evidence, metabolic, inflammatory, oxidative, emotional and psychological stress is an important part of PCOS.5 While the incidence of any disease or disorder can lead to anxiety and worry,6 studies have shown that women with PCOS experience emotional distress, depression and anxiety more frequently than others, and when confronted with the disorder, some become more anxious and stressful.7–10 PCOS therefore affects the daily life of many people.11 It disturbs the joys of adolescence, because the stigma associated with hyperandrogenism is more intensely felt in this age group and is likely to damage the psychosocial development of adolescent girls.12
Patients with this disorder have to go through different stages of coping wherein they will likely have to respond to internal stress (physiological and psychological stressors) and external stress (environmental and social factors related to the syndrome) using coping responses.13 The acceptance of any disorder is a complicated process that depends on factors such as the manifestation of the disorder, the availability and quality of treatment, individual demands (eg, mental demands, emotional demands, stress, coping strategies, etc.), support of the family members and other relatives and socioeconomic status.14 Adolescence is a time of physical, cognitive and emotional changes as well as a period of great change in various aspects of life.15 Adolescents usually deal with their problems through a variety of methods, including problem-solving methods that focus on changing the status quo, problem-solving, approaching others (seeking spiritual and social support from friends), using strategies to ignore their problems and running away from them, and self-blaming and non-coping behaviors.16 Managing chronic conditions such as chronic pain, diabetes and cancer in adolescents leads to a variety of coping responses and some are associated with successful adaptation.17
The aim of qualitative research is to understand the experiences and circumstances of individuals and explain concepts from their perspective, and experiences often vary from one person to the other.18 The review of literature suggests the diversity of the coping strategies used by adult women with PCOS,19,20 while studies on adolescents with this syndrome are rather limited. Given the crucial role of coping strategies in adolescents with this chronic disease, the present study was conducted to gain a comprehensive understanding of the strategies used by adolescents with PCOS to cope with the challenges of this disorder.
Methods
Fifteen adolescents with PCOS able to share their rich experiences of coping with the disorder participated in this qualitative study. All the interviews were in Persian. The entire research team members and participants were fluent in Persian. The research team was composed of a qualitative methodologist as the principal researcher, a gynecologist and a PhD student of reproductive health. Purposive sampling continued until data saturation was achieved. The inclusion criteria for the study consisted of being an adolescent with PCOS as diagnosed by a gynecologist (based on the National Institute of Child Health and Human Development (NICHD) or the National Institutes of Health (NIH) criteria), having hyperandrogenism, oligo-ovulation/anovulation, age between 13 and 19 years, and willingness of the patient and their parents for participation in the study and sharing experiences. In this study parent or legal guardian provided written informed consent for any participant under the age of 18 years.
Before beginning data collection, the research project was approved by the ethics committee of Shahid Beheshti University of Medical Sciences in Tehran, Iran. The ethical principles observed for the research included obtaining informed consent, preserving the confidentiality of the data and giving the participants the right to leave the study whenever they desired.
Individual in-depth interviews were held with semi-structured questions (“What are your experiences with this disorder at this stage of life?” and “How has this disorder affected your mental state?”). The minimum and maximum duration of the interviews was 30 and 55 mins. The interviews were held in a relaxed and private environment in the health centers of Shahid Beheshti University of Medical Sciences in Tehran, Iran. All the interviews were recorded with prior permission from the participants. Thematic analysis was used in this study. Thematic analysis is a flexible and foundational method for qualitative analysis.21 In the beginning, to immerse in the data, the research team transcribed the recorded audio interviews and the members read transcripts thoroughly. In order to generate the initial codes, the research team members extracted the semantic units. Then, the codes were collated into potential themes. The themes were reviewed for generating a thematic map. Finally, the themes were defined and given names and the final report was prepared.
Trustworthiness
Credibility, transferability, dependability, confirmability and authenticity measures were used to verify the data. The methods used in this study to verify the accuracy of the data included the selection of contributors with a variety of experiences, persistent observation, member checking, use of a coding framework, prolonged engagement with data, team consensus on themes, thick descriptions of context, purposive maximum variation sampling (selection of adolescents with different characteristic such as age, family economic status, education, etc.) and discussing some of the findings with a number of the participants.
Results
Thematic analysis categorized coping strategy into one main-theme as “Dealing with PCOS” and 3 themes and 12 sub-themes. Themes and sub-themes are as follow:
Escaping the problem (sub-themes: Adopting a forgetting mindset, and concealment and minimization of the disorder).
Depressive mood (sub-themes: Poor self-perception and low self-esteem, isolation, sleep disturbances, passive aggressive behavior, emotional turmoil, feelings of humiliation, adolescents’ perceptions)
Coping with the disease (sub-themes: Recovery of health, positive thinking, hope for recovery), as shown in Figure 1.
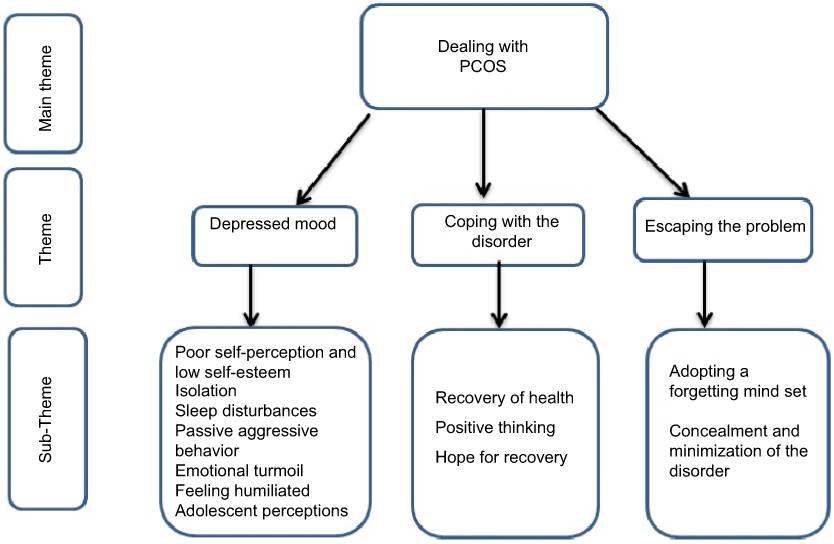 |
Figure 1 Theme and sub-themes. |
The characteristics of selected participants are mentioned in Table 1.
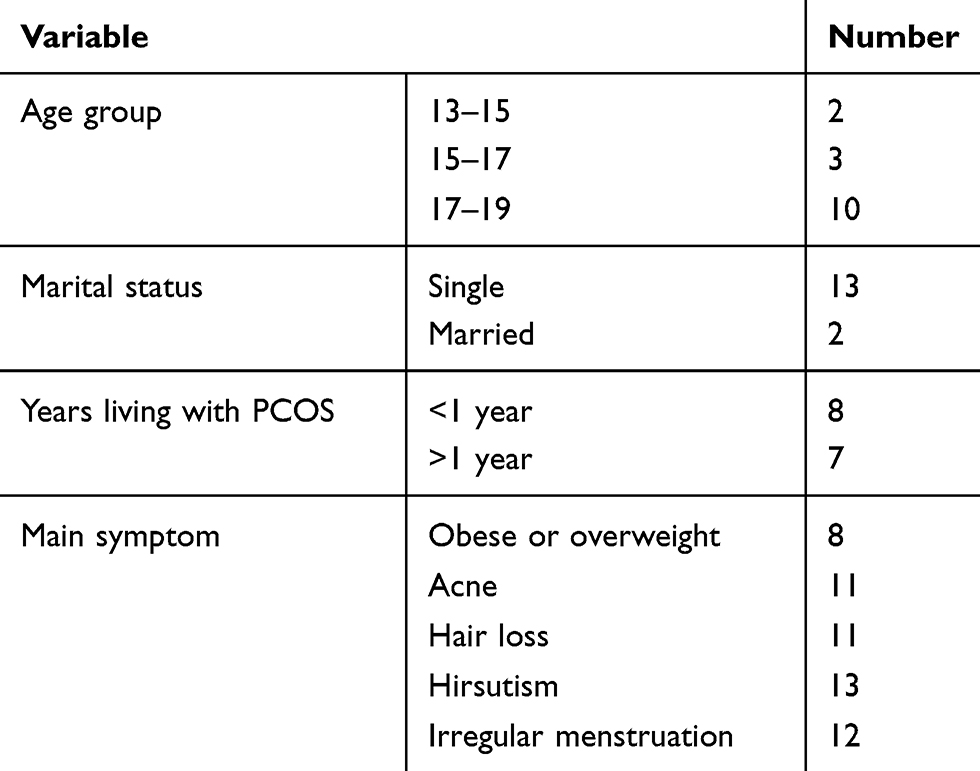 |
Table 1 Characteristics of study samples (n=15) |
Escaping the problem
The “escaping the problem” theme was formed in this study by combining two sub-themes, namely “forgetting” and “concealment and minimization of the disorder”. The adolescents tried to escape their challenges by not disclosing their disorder to others so as to reduce the burden of psychological issues, and they used the method of forgetting to rid themselves of intrusive thoughts. The experiences of some of the participants in the study showed that they used the method of “forgetting” to escape their problems and tried to understand which thoughts resulted in their stress and then chose different ways to distract themselves from these thoughts. In the words of the participants:
“Sometimes, when I think of the disorder, I push the thoughts away. I’ve become inattentive” (Participant 1, 19 years old).
Because I was immersed in my university entrance exam, my mind was preoccupied. This issue (PCOS) has not been important to me at all. I’m always busy studying. I do not have the time to think about it. (Participant 8, 18 years old).
I’ve become indifferent now. It’s no more important to me how it has gotten on my nerves. I don’t think about it anymore because I can’t do anything about it. I went to the doctor, I took medicines, but it didn’t get better. (Participant 6, 19 years old).
The experiences of some of the participants also showed that they somehow tried to escape the problem by “concealing and minimizing the syndrome”. In the words of the participants:
“I’m not upset because they say it is very common and could happen to anyone, and it’s not a rare disorder. Anyone I see, I tell them I have PCOS and I’m taking medicines. It’s normal” (Participant 1, 19 years old).
“I try not to take my pills in front of people because they ask why I’m taking pills. I don’t tell anyone about my disorder” (Participant 9, 18 years old).
Depressive mood
The “depressive mood” theme was developed with seven sub-themes, including “poor self-perception and self-esteem”, “isolation”, “sleep disturbances”, “passive aggressive behavior”, “emotional turmoil”, “feeling humiliated” and “adolescents’ perceptions”. Some of the adolescents experienced “laziness” and “sadness” after their diagnosis with PCOS and also concerns about failing to recover, constant worries about the disorder and psychological distress, which eventually ended in their “losing the joys of adolescence” and they began to lose focus. These experiences led to unpleasant feelings, and struggles with the disorder for many years caused “emotional disturbances” for some of the adolescents. According to participants’ experiences, some of them tried to cope with their problems through “aggressiveness” and “making excuses.” Often, they became isolated because of “limiting their relationships with their friends and close relatives” and “preferring to be alone than to be with others”. The experiences of the participants also showed that, because of “internal feelings of distress when in gatherings where people were inquisitive” and “being in turmoil due to feeling different from peers”, some of them felt humiliated and had a low self-esteem and sometimes also experienced symptoms of physical change caused by their psychological changes. The experiences of most participants showed that the visibility of their symptoms to their peers and others made them feel vulnerable, and as a result, they preferred not to be in touch with anyone in order to avoid showing their vulnerability. In the words of the participants:
“When I’m in front of the mirror, I feel bad, cause I have a lot of hair and acne” (Participant 15, 19 years old).
“I do not have much confidence when with others, cause I think they are better than me. It’s the same for my family, my friends … ” (Participant 3, 16 years old).
Loneliness and “isolation” were one of the common strategies of the adolescents in this study to cope with their disorder. In the words of the participants:
I don’t have much patience for myself; I don’t have patience for others; I prefer to be left alone at home. What I mean is that I prefer everyone to go out visiting and enjoying themselves but leaving me home alone. (Participant 13, 19 years old).
“I try not to be in touch with my friends … I’ve only told my best friend about my polycystic ovary syndrome” (Participant 15, 19 years old).
Stressful conditions were associated with “sleep disturbances” in some of the participants. In the words of the participants:
“I’m always sleepy. I feel so sleepy. I’m constantly falling asleep. It’s awful. It has been two or three years that I’ve become like this. I mean, since the morning, when I wake up, I feel sleepy” (Participant 6, 19 years old).
“I think so much about it that I can’t sleep. I go out [of my bedroom] to drink water. I can’t sleep at all until 5 or 7 am” (Participant 12, 13 years old).
Some of the adolescents who participated in the study expressed their agitation and negative feelings about the onset of their syndrome and were unknowingly showing passive aggressive behavior. In the words of the participants:
“I’m always fighting with everyone. I’ve become stubborn. When I get worried about something, I go to my room and shut the door. I start to cry and then lock the door” (Participant 3, 16 years old).
“I’m so distressed that I keep fighting with my family. I say, ‘It’s all your fault, you’ve caused this problem for me!” (Participant 12, 13 years old).
Concerns about the syndrome and its presentations and reasons caused tension in most of the participants and they were faced with “emotional disturbances”. In the words of these participants:
“I’m worried about seeking further treatment because they told me that no special treatment exists yet” (Participant 2, 15 years old).
“I really don’t have the patience, unlike in the past. For example, I had so many interests to pursue that I really enjoyed going out, but not anymore” (Participant 10, 19 years old).
“I don’t think so much about it. It makes me very upset. My entire life has become consumed with this problem. I’ve lost my appetite. I’m so upset” (Participant 12, 13 years old).
“My inner feelings are such that, like, when you want to do something for yourself, say, make an effort for the sake of your life, continuing it causes problems because of this disorder” (Participant 2, 15 years old).
“Right now, I feel that, the way my friends hang out and are happy in each other’s company, I’m not like that” (Participant 6, 19 years old).
“Most of the time, my mind was preoccupied and I couldn’t concentrate on a particular problem” (Participant 2, 15 years old).
“My particular concern is that if this continues, what’s going to happen … Will this illness be with me all my life and will I have to always cope with it and take medications?” (Participant 4, 19 years old).
“I think so much about it. When I look at myself in the mirror, I say, ‘What kind of life is this?” (Participant 2, 15 years old).
“My nerves are so weakened … ” (Participant 12, 13 years old).
I didn’t use to go and visit others … not that I said I didn’t like to go and see people. For example, when I sat down, someone would ask me if I was on a diet and I would get angry and want to answer back, but I had to keep the boundries of respect, so I wouldn’t say anything. And then, I wouldn’t go to visit people at all because of this. (Participant 13, 19 years old).
Some of the adolecents who participated in the study preceived themselves as below optimal because of the symptoms of their syndrome and imagined that they were not worthy and felt “humiliated”. In the words of the participants:
Compared to my friends, I see myself very different. For example, they wear fashionable items that I have always liked to own, but I could never be like that, because of the excessive hair that I have to hide, my obesity and hair loss. (Participant 2, 15 years old).
The manifestation of mental stress as a result of the syndrome and mental turmoil in some of the participants led to “adolescents’ perceptions”. In the words of the participants:
“I’m usually tired. My activities have diminished, unlike the vitality I had before” (Participant 14, 17 years old).
“I don’t like to move too much. I like to just always sit somewhere” (Participant 10, 19 years old).
Coping with the disorder
“Coping with the disorder” consisted of three sub-themes, namely “the recovery of health”, “positive thinking” and “hope for recovery”. Most of the adolecents who participated in this study tried to reduce the mental stress of having PCOS through academic accomplishments and took measures to promote their physical health.Although the adolescents felt responsible for their own health, they neglected it nonetheless, because they prioritized their studies and future career prospects.
Some of the adolescents attempted to create a positive image of their disorder and created a positive vibe for seeking treatment by adopting a “hope for recovery” approach. Some of them coped with the syndrome through a “positive internal dialogue”. Some of the participants in this study were taking “health recovery” measures to cope with their syndrome. In the words of the participants:
“Right now, studying is my priority, and when I’ve completed my studies, I want to go to the doctor again” (Participant 1, 19 years old).
“I am far too busy with the university entrance examination and my studies to have any time for this disease at all” (Participant 8, 18 year-old).
“I used to regard my disorder as trivial. I didn’t think it was necessary for me to take my pills. Later, I began taking it very seriously” (Participant 9, 18 years old).
Some of the participants were able to rid themselves of disturbing thoughts through “positive thinking” and coped with their disorder. In the words of these participants:
“I came to accept myself, ‘Okay, you have this condition, you have this pimple!’ I accepted it as it was and then wouldn’t think about it” (Participant 4, 19 years old).
“It’s a mild illness –not a very dangerous disorder” (Participant 4, 19 years old).
Some of the participants took steps to cope with the disorder through a “hope for recovery”. In the words of this group of the participants:
“My medications are one too many, but I take them with the hope of getting better. Just like this. I take my medications to get better soon” (Participant 6, 19 years old).
“When I take my medicines, since they regulate my period, I feel good” (Participant 8, 18 years old).
Discussion
The findings of this study include concepts such as escaping the problem, depressed mood and coping with the disorder. In conjunction with each other, these concepts led to the formulation of dealing with PCOS.
As the sociocultural context of any society can affect individuals’ strategies for coping with critical situations, the sociocultural and religious contexts of the Iranian society can also affect the type of strategies adolescents adopt to cope with PCOS. Like in many Middle Eastern countries, cultural and educational issues also have a major role in adolescents’ mental health in Iran.22
Evidence suggests that dealing with a chronic disease, such as adolescent diabetes, requires a coping strategy that can help improve the health outcomes and quality of life of the patient.23
Other chronic diseases such as adolescent cancer or serious infections that may cause future infertility have also become a serious concern for both adolescent patients and their parents as per their responses.24,25 The diagnosis of any fertility disorder in adolescents can disrupt the normal psychosocial development of the individual.26 In general, the manifestation of symptoms such as obesity, acne, hirsutism and the disruption of the menstrual cycle lead to stress in these patients and they cope with this stress in different ways.
In the experiences of the participants, some of the adolescents with PCOS were trying to escape their problems by forgetting and often with the concealment and minimization of their disorder. The results of a study on women with PCOS showed that those who suffered more psychological problems used maladaptive coping strategies, such as avoidance strategies, and used less problem-focused coping strategies.27 Avoidance coping is known as an effective short-term strategy, but in the long term, it prevents psychological adjustment and increases depression.28,29
The results of other studies on social coping strategies have shown that adolescents use different coping techniques, such as avoidance coping, problem-solving and seeking social support.30
It seems that most participants in the present study were turning to these strategies to escape being labeled as “sick” and to be able to cope with the disorder in some way by denying its existence to themselves and others. It is a proven fact, however, that avoidance coping could cause a downward spiral in the long-term.
The experiences of the participants of this study showed that adaptation to illness could emerge as a depressive mood in some adolescents. The diagnosis of PCOS has psychological ramifications.31 Depression and moodiness in adolescents and the appearance of a depressive mood have been argued to be associated with symptoms such as disturbed sleep, lethargy, restlessness, changes in appetite and weight, decreased motivation and concentration, decreased self-esteem and isolation.32 In one qualitative study, the experiences of 12 people with PCOS aged 17 to 51 years revealed great mental anxiety in coping with this disorder.19 The onset of PCOS is associated with the instability of emotions, confusion and moodiness and leads to feelings of irritability, fear and despair in social relationships and a general sense of unhappiness.33,34
The establishment of social relationships is vital during adolescence.35 Adolescents with this disorder choose isolation to counteract the reactions of those around them. The acceptance of adolescents with PCOS by the community and those close to them helps improve their behavior, while increased criticism, especially in this vulnerable age group, reduces self-esteem and increases anxiety and depression and ultimately leads to abandoned social relationships.36 In contrast, a negative body image destroys the individual’s social competence and causes the abandoning of intimate relationships.37,38 Changes in one’s physical appearance, concerns over changes in one’s mental body image and the development of anxiety about the ramifications of the disorder seem to play a role in the manifestation of a depressive mood as a kind of coping response to the disease.
The experiences of the participants in this study also showed that those who responded with positive thoughts and had hope for their future well-being and recovery chose an adaptive coping response to the disorder. The various factors affecting the acceptance of the disorder also contribute to the PCOS patient’s coping with the disorder.39 The results of a study on women with PCOS showed that coping strategies were more excitement-oriented.40 Another qualitative study on women with PCOS also showed that coping strategies include deliberation (religious beliefs, paradoxical thoughts), practical steps (positive steps such as seeking information and treatment as well as negative steps such as detachment and concealment) and seeking support (family support and peer support) in these patients.41 Evidence suggests that the types of coping strategies chosen by women with PCOS affect their quality of life.20 Some studies have even suggested that hope is a very powerful force that can play a key role in coping with adolescent illnesses.42 Hope is occasionally a solution to tension that increases the individual’s ability to adapt.43 Some of the participants of this study were able to cope with their mental turmoil through their hope to recover. Meanwhile, some attempted to take steps towards coping with their disorder through positive thoughts. Positive thoughts comprise a branch of cognitive therapy that can be defined as the usage of hopefulness, happiness and positive mental abilities.44
A study by Benson et al (2010) conducted on 449 women with PCOS showed that some participants had a passive coping strategy in dealing with this syndrome (retreating and accepting one’s fate regarding the disorder), which is an unharmonious strategy that leads to the emergence of anxiety and depression and in turn decreases the quality of life. In contrast, some participants who adopted active coping strategies (problem-solving and information-seeking) had lower levels of depression.45 The participating adolescents of this study had a positive attitude and took health-recovery measures to cope with the disorder.
Active coping involves problem-solving and social support-seeking while passive coping involves social isolation.17 The results of one study on children and adolescents with a chronic illness showed that coping with such a disease may lead to effective coping with daily stressors of life.46
Some of the participants used problem-solving through positive thoughts and measures to deal with the stressful conditions of life. They used a rational strategy to accept their disorder and their tensions thus decreased. In general, chronic PCOS requires self-efficacy and lifestyle modifications.47 As for the psychological burden of PCOS, choosing a proper coping strategy plays a decisive role in the quality of life of adolescents with the disorder, as irrational strategies could cause harm and threaten different dimensions of life. The use of clinical counseling, mental health services, beauty counseling services and support services for patients and their families can contribute significantly to the improvement of the quality of life of adolescents with chronic PCOS.48
Implementing psychological counseling programs (by psychologists and other allied health professionals) and teaching adolescents adaptive coping strategies are recommended to prevent future mental health problems. Attention to mental health and related care measures is imperative for medical teams.
The study limitations include the non-generalizability of the results to all adolescents with this syndrome, although this limitation applies to all qualitative studies in nature. Furthermore, forgetting certain experiences or the unwillingness to actually express these experiences and feelings on the part of the adolescents could be considered another limitation of the study.
Conclusion
When confronted with the stressful symptoms of PCOS, the participants adolescents of this study showed coping responses such as escaping the problem, depressive mood or coping with the syndrome. Identifying the ways through which these adolescents cope with their syndrome is vital for recognizing the mental health needs of PCOS patients and improving their quality of life.
Acknowledgments
This article is a part of a PhD thesis of Shahid Beheshti University of Medical Sciences, Tehran, Iran. The researchers are grateful to the adolescents who participated in the study and their parents and vice-chancellor of research from the Shahid Beheshti University of Medical Sciences.
Disclosure
The authors have no conflicts of interest in this work.
References
1. de Melo AS, Dias SV, de Carvalho Cavalli R, et al. Pathogenesis of polycystic ovary syndrome: multifactorial assessment from the foetal stage to menopause. Reproduction. 2015;150(1):R11–R24. doi:10.1530/REP-14-0499
2. Bhuvanashree N, Gupta S, Anitha M, Venkatarao E. Polycystic ovarian syndrome: prevalence and its correlates among adolescent girls. Ann Trop Med Public Health. 2013;6(6):632. doi:10.4103/1755-6783.140233
3. Desai N, Tiwari R, Patel S. Prevalence of polycystic ovary syndrome and its associated risk factors among adolescent and young girls in Ahmedabad region. Indian J Pharm Pract. 2018;11(3):119. doi:10.5530/ijopp.11.3.27
4. Nidhi R, Padmalatha V, Nagarathna R, Amritanshu R. Prevalence of polycystic ovarian syndrome in Indian adolescents. J Pediatr Adolesc Gynecol. 2011;24(4):223–227. doi:10.1016/j.jpag.2011.03.002
5. Papalou O, Diamanti-Kandarakis E. The role of stress in PCOS. Expert Rev Endocrinol Metab. 2017;12(1):87–95. doi:10.1080/17446651.2017.1266250
6. Brady C, Mousa SS, Mousa SA. Polycystic ovary syndrome and its impact on women’s quality of life: more than just an endocrine disorder. Drug Healthc Patient Saf. 2009;1:9.
7. Barry JA, Hardiman PJ, Saxby BK, Kuczmierczyk A. Testosterone and mood dysfunction in women with polycystic ovarian syndrome compared to subfertile controls. J Psychosomatic Obstetrics Gynecol. 2011;32(2):104–111. doi:10.3109/0167482X.2011.568129
8. Balikci A, Erdem M, KESKIN U, et al. Depression, anxiety, and anger in patients with polycystic ovary syndrome. Nöro Psikiyatri Arsivi. 2014;51(4):328. doi:10.5152/npa.2014.6898
9. Veltman-Verhulst SM, Boivin J, Eijkemans MJ, Fauser BJ. Emotional distress is a common risk in women with polycystic ovary syndrome: a systematic review and meta-analysis of 28 studies. Hum Reprod Update. 2012;18(6):638–651. doi:10.1093/humupd/dms029
10. Barry JA, Kuczmierczyk AR, Hardiman PJ. Anxiety and depression in polycystic ovary syndrome: a systematic review and meta-analysis. Human Reprod. 2011;26(9):2442–2451. doi:10.1093/humrep/der197
11. Love JG, McKenzie JS, Nikokavoura EA, Broom J, Rolland C, Johnston KL. The experiences of women with polycystic ovary syndrome on a very low-calorie diet. Int J Women’s Health. 2016;8:299. doi:10.2147/IJWH.S100385
12. Homburg R, Lambalk CB. Polycystic ovary syndrome in adolescence—a therapeutic conundrum. Human Reprod. 2004;19(5):1039–1042. doi:10.1093/humrep/deh207
13. Azizi M, Elyasi F. Psychosomatic aspects of polycystic ovarian syndrome: a review. Iran J Psychiatry Behav Sci. 2017;11:2. doi:10.5812/ijpbs
14. Obiegło M, Uchmanowicz I, Wleklik M, Jankowska-Polańska B, Kuśmierz M. The effect of acceptance of illness on the quality of life in patients with chronic heart failure. Eur J Cardiovasc Nurs. 2016;15(4):241–247. doi:10.1177/1474515114564929
15. Markova S, Nikitskaya E. Coping strategies of adolescents with deviant behaviour. Int J Adolesc Youth. 2017;22(1):36–46. doi:10.1080/02673843.2013.868363
16. Caycho TP. Relationship with parents and coping strategies in adolescents of lima. J Educ Psychol Propósitos Y Representaciones. 2016;4(1):37–59.
17. Compas BE, Jaser SS, Dunn MJ, Rodriguez EM. Coping with chronic illness in childhood and adolescence. Annu Rev Clin Psychol. 2012;8:455–480. doi:10.1146/annurev-clinpsy-032511-143108
18. Ormston R, Spencer L, Barnard M, Snape D. The foundations of qualitative research. Qual Res Pract. 2014;2:52–55.
19. Hadjiconstantinou M, Mani H, Patel N, et al. Understanding and supporting women with polycystic ovary syndrome: a qualitative study in an ethnically diverse UK sample. Endocr Connections. 2017;6(5):323–330. doi:10.1530/EC-17-0053
20. Kolahi L, Asemi N, Mirzaei M, Adibi N, Beiraghdar M, Mehr AM. The relationship between quality of life and coping strategies in polycystic ovary syndrome patients. Adv Biomed Res. 2015;4.
21. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
22. Sharifi V, Shahrivar Z, Alaghband-Rad J. Child and adolescent mental health care in Iran: current status and future directions. Arch Iran Med. 2016;19(11):797.
23. Jaser SS, Faulkner MS, Whittemore R, et al. Coping, self-management, and adaptation in adolescents with type 1 diabetes. Ann Behav Med. 2012;43(3):311–319. doi:10.1007/s12160-012-9343-z
24. Quinn GP, Knapp C, Murphy D, Sawczyn K, Sender L. Congruence of reproductive concerns among adolescents with cancer and parents: pilot testing an adapted instrument. Pediatrics. 2012;129(4):e930–e936. doi:10.1542/peds.2011-2568
25. Ellis SJ, Wakefield CE, McLoone JK, Robertson EG, Cohn RJ. Fertility concerns among child and adolescent cancer survivors and their parents: a qualitative analysis. J Psychosoc Oncol. 2016;34(5):347–362. doi:10.1080/07347332.2016.1196806
26. Covington SN, Martinez PE, Popat V, Nandagopal R, Ryan M, Nelson LM. The psychology of antecedents to adult reproductive disorders in adolescent girls. Ann N Y Acad Sci. 2008;1135(1):155–162. doi:10.1196/annals.1429.016
27. Carron R, Kooienga S, Boyle DK, Alvero R. Coping in women with polycystic ovary syndrome: implications for practitioners. J Nurse Pract. 2017;13(10):700–707. doi:10.1016/j.nurpra.2017.08.004
28. Holahan CJ, Moos RH, Holahan CK, Brennan PL, Schutte KK. Stress generation, avoidance coping, and depressive symptoms: a 10-year model. J Consult Clin Psychol. 2005;73(4):658. doi:10.1037/0022-006X.73.4.658
29. Nahlén Bose C, Elfström ML, Björling G, Persson H, Saboonchi F. Patterns and the mediating role of avoidant coping style and illness perception on anxiety and depression in patients with chronic heart failure. Scand J Caring Sci. 2016;30(4):704–713. doi:10.1111/scs.12297
30. Kingsbury M, Liu J, Coplan RJ, Chen X, Li D. Assessment and implications of coping styles in response to a social stressor among early adolescents in China. J Early Adolesc. 2016;36(2):222–250. doi:10.1177/0272431614561262
31. Sulaiman MA, Al-Farsi YM, Al-Khaduri MM, Waly MI, Saleh J, Al-Adawi S. Psychological burden among women with polycystic ovarian syndrome in Oman: a case–control study. Int J Women’s Health. 2017;9:897. doi:10.2147/IJWH.S145383
32. Roberts J. Low mood and depression in adolescence: clinical update. Br J Gen Pract. 2013;63(610):273–274. doi:10.3399/bjgp13X667367
33. Ann Manlove H, Guillermo C, Gray PB. Do women with polycystic ovary syndrome (PCOS) report differences in sex-typed behavior as children and adolescents?: results of a pilot study. Ann Hum Biol. 2008;35(6):584–595. doi:10.1080/03014460802337067
34. Scaruffi E, Gambineri A, Cattaneo S, Turra J, Vettor R, Mioni R. Personality and psychiatric disorders in women affected by polycystic ovary syndrome. Front Endocrinol (Lausanne). 2014;5:185. doi:10.3389/fendo.2014.00185
35. Choudhury S, Blakemore SJ, Charman T. Social cognitive development during adolescence. Soc Cogn Affect Neurosci. 2006;1(3):165–174. doi:10.1093/scan/nsl024
36. Zachurzok A, Pasztak-Opilka A, Forys-Dworniczak E, Drosdzol-Cop A, Gawlik A, Malecka-Tendera E. Are psychosocial consequences of obesity and hyperandrogenism present in adolescent girls with polycystic ovary syndrome? Int J Endocrinol. 2018;2018.
37. Trent ME, Rich M, Austin SB, Gordon CM. Quality of life in adolescent girls with polycystic ovary syndrome. Arch Pediatr Adolesc Med. 2002;156(6):556–560. doi:10.1001/archpedi.156.6.556
38. Dokras A, Clifton S, Futterweit W, Wild R. Increased risk for abnormal depression scores in women with polycystic ovary syndrome: a systematic review and meta-analysis. Obstetrics Gynecol. 2011;117(1):145–152.
39. Rzońca E, Iwanowicz-Palus G, Bień A, Wdowiak A, Szymański R, Chołubek G. Generalized self-efficacy, dispositional optimism, and illness acceptance in women with polycystic ovary syndrome. Int J Environ Res Public Health. 2018;15(11):2484. doi:10.3390/ijerph15061188
40. Özenl Y, Haydardedeoğlu B, Mıcozkadioğlu İ, Şımşek E, Kiliçdağ EB, Bağiş T. Anxiety, depression and ways of coping skills by women with polycystic ovary syndrome: a controlled study. J Turk Ger Gynecological Assoc. 2009;10:4.
41. Bazarganipour F, Hosseini N, Taghavi SA. Coping strategies in patients with polycystic ovarian syndrome; A qualitative research. J Knowl Health. 2014;9(3):28–39.
42. Griggs S, Walker RK. The role of hope for adolescents with a chronic illness: an integrative review. J Pediatr Nurs. 2016;31(4):404–421. doi:10.1016/j.pedn.2016.02.011
43. Rustøen T. Hope and quality of life, two central issues for cancer patients: a theoretical analysis. Cancer Nurs. 1995;18(5):355–361.
44. Ebad N, Sodani M, Faghihi A, Hosseinpoor M. The Study of Effectiveness of Positive Thinking Training with Emphasis on the Signs of Quran on Increasing Hope to Divorced Women’s Life of Ahvaz City. Iran; 2009.
45. Benson S, Hahn S, Tan S, Janssen OE, Schedlowski M, Elsenbruch S. Maladaptive coping with illness in women with polycystic ovary syndrome. J Obstetric Gynecologic Neonatal Nurs. 2010;39(1):37–45. doi:10.1111/j.1552-6909.2009.01086.x
46. Hampel P, Rudolph H, Stachow R, Laß-Lentzsch A, Petermann F. Coping among children and adolescents with chronic illness. Anxiety Stress Coping. 2005;18(2):145–155. doi:10.1080/10615800500134639
47. Kozica SL, Gibson-Helm ME, Teede HJ, Moran LJ. Assessing self-efficacy and self-help methods in women with and without polycystic ovary syndrome. Behav Med. 2013;39(3):90–96. doi:10.1080/08964289.2012.720312
48. Lanzo E, Monge M, Trent M. Diagnosis and management of polycystic ovary syndrome in adolescent girls. Pediatr Ann. 2015;44(9):e223–e230. doi:10.3928/00904481-20150910-10
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.