Back to Journals » Clinical Ophthalmology » Volume 20
Polarization-Sensitive OCT Assessment of Retinal Emboli in Branch Retinal Artery Occlusion: A Pilot Study
Authors Terao R ![]() , Saeki Y, Yashiro K, Ota M, Aoki S, Kitamoto K, Azuma K
, Saeki Y, Yashiro K, Ota M, Aoki S, Kitamoto K, Azuma K
Received 21 March 2026
Accepted for publication 25 June 2026
Published 9 July 2026 Volume 2026:20 610278
DOI https://doi.org/10.2147/OPTH.S610278
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Ryo Terao, Yuki Saeki, Kazuki Yashiro, Mami Ota, Shuichiro Aoki, Kohdai Kitamoto, Keiko Azuma
Department of Ophthalmology, Graduate School of Medicine, the University of Tokyo, Tokyo, Japan
Correspondence: Ryo Terao, Department of Ophthalmology, Graduate School of Medicine, the University of Tokyo, 7-3-1 Hongo, Bunkyo, Tokyo, 113-8655, Japan, Tel +81 3 3815 5411, Fax +81 3 3817 0798, Email [email protected]
Purpose: To evaluate intraluminal emboli in branch retinal artery occlusion (BRAO) using polarization-sensitive optical coherence tomography (PS-OCT).
Patients and Methods: Eight eyes of 8 patients with BRAO were included. Fundus photography, swept-source (SS)-OCT, and PS-OCT were performed. Detection rates and entropic profiles of retinal emboli were examined.
Results: In this retrospective study of 8 BRAO eyes, fundus photography found thromboemboli in five eyes (62.5%). While SS-OCT detected thromboembolus in two eyes (25.0%), PS-OCT identified in all (100%) eyes, demonstrating a higher detection rate than SS-OCT. Polarimetric entropy (PE) value of thromboemboli was significantly higher than that of background retina (p = 0.0078), whereas SS-OCT did not show significant difference in reflectivity. Image contrast was significantly higher in PS-OCT than SS-OCT (p = 0.0078).
Conclusion: PS-OCT enables noninvasive visualization of intraluminal embolic material and may provide additional pathophysiological insight beyond conventional OCT. However, these findings are based on a small retrospective cohort and require validation in larger prospective studies.
Keywords: retinal artery occlusion, polarization-sensitive optical coherence tomography, thromboembolism, polarimetric entropy, retinal ischemia
Introduction
Retinal artery occlusions (RAOs) including central retinal arterial occlusion (CRAO) and branch retinal arterial occlusion (BRAO) are emergent retinal disorders that cause immediate infarction and irreversible visual loss.1–3 RAOs are typically caused by embolic or thrombotic obstruction of retinal arteries, leading to acute, severe vision or visual field loss. Retinal emboli originate from various sources, including carotid atherosclerotic plaques and cardiac lesions. Previous studies have reported cholesterol emboli as the most common subtype, accounting for approximately 74% of visible retinal emboli.4,5 However, the reported distribution of embolus composition varies among studies, and platelet-fibrin emboli have been reported as the predominant subtype in some cohorts of retinal artery occlusion.6 These discrepancies may reflect differences in study populations, disease stage, and embolus detection methods. Sustained arterial occlusion results in persistent and irreversible visual impairment.7,8 BRAO represents embolic occlusion of a branching artery. Beyond their ocular consequences, retinal artery occlusions are recognized as manifestations of systemic vascular disease and are considered analogous to ischemic stroke. Patients with RAO have an elevated risk of subsequent cerebrovascular and cardiovascular events, underscoring the importance of identifying the underlying embolic source and vascular pathology.9,10 Therefore, imaging techniques capable of directly visualizing retinal emboli may provide clinically relevant information not only for understanding local disease mechanisms but also for guiding systemic vascular assessment and risk stratification. Ophthalmological examinations including visual acuity, fundus examinations, optical coherence tomography (OCT), and fluorescence angiography (FA) are essential for accurate diagnosis of RAO. Although fundus photography and fluorescein angiography (FA) can identify perfusion defects, direct visualization of the embolic material is often difficult because of its small size and the limited axial resolution of conventional imaging. Conventional OCT provides detailed cross-sectional imaging of retinal microstructure and can depict secondary ischemic changes, such as inner retinal hyperreflectivity, thickening, and subsequent thinning. However, while the detailed characterization of retinal emboli on cross-sectional images is necessary for the mechanistic understanding, direct visualization of the embolic material and its optical characteristics of emboli with conventional OCT is not consistently achievable.
Polarization-sensitive optical coherence tomography (PS-OCT) is a functional extension of OCT that measures the polarization state of backscattered light. PS-OCT provides tissue-specific contrast by polarization properties, allowing detailed analysis of each retinal layer.11 In the eye, PS-OCT can detect melanin-rich materials, lipids, hard exudates, as well as activated inflammatory cells.12–16 We have previously demonstrated that PS-OCT enables clear visualization of retinal pigment epithelium (RPE), choroid, hyperreflective foci within the retina.17–19 These findings support the feasibility of using PS-OCT to assess chorioretinal pathology. However, the application of PS-OCT to retinal vascular occlusive diseases has not yet been reported.
Given that previous studies demonstrated that polarimetric measurements can detect thrombosis in vessels as high-entropy lesions,20,21 we hypothesized that PS-OCT could detect retinal emboli as high-entropy lesions in eyes with RAO. In fact, we have previously reported a case in which retinal emboli were successfully visualized using PS-OCT.22 Building on this initial observation, the present study aimed to explore the reproducibility of this finding and to characterize the detection and imaging features of retinal emboli using PS-OCT.
Materials and Methods
Study Design and Participants
This retrospective study was approved by the Institutional Review Board of the University of Tokyo (CU22-R003) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was waived by the Institutional Review Board due to the retrospective nature of the study and the use of anonymized clinical data.
Patients diagnosed with BRAO at the University of Tokyo Hospital between April 2025 and March 2026 were included. Ophthalmologic examinations were performed in all patients, including best-corrected visual acuity (BCVA; logMAR converted from Snellen), color fundus photography, FA (Heidelberg Retina Angiograph 2; Heidelberg Engineering, Heidelberg, Germany), swept-source (SS)-OCT, and PS-OCT imaging.
The diagnosis of BRAO was based on previously established criteria; (1) a history of sudden onset of visual deterioration in the affected eye, (2) evidence of sectorial retinal ischemia (retinal opacification, whitening, or thinning) corresponding to the distribution of an affected branch retinal artery.17 The presence of a visible thromboemboli was not required, as occlusion by microemboli can also cause BRAO. Patients with a history of retinal vascular disorders (eg retinal vein occlusion, diabetic retinopathy, or prior RAO) were excluded. Eyes with CRAO were also excluded because some CRAO eyes result from non-thromboembolic conditions, such as ocular ischemic syndrome or giant cell arteritis.
PS-OCT and Imaging Analysis
PS-OCT (ROCTIA®; TOMEY, Nagoya, Japan) was used to obtain images, as previously reported.23 The mechanical and technical principle of PS-OCT system has been described in our previous studies.24 In brief, polarimetric entropy (PE) represents spatial randomness of the polarization property, quantified statistically from the measured Jones matrix.25 PE values, reflecting the randomness of backscattered polarization (0 = uniform, 1 = random), were calculated from PS-OCT data to visualize intraluminal heterogeneity.
A 40° (approximately 12 mm) × 40° area centered on the macula was scanned in each eye using a raster-scan pattern consisting of 1024 A-lines (horizontal) × 256 B-scans (vertical). The Kernel size for entropy calculation was 11×7 pixels, and size of each pixel measured 11.7×4.4 μm in the lateral and axial directions, respectively. SS-OCT images were also simultaneously acquired using the identical device.
Since the retinal arteries are located within the retinal nerve fiber layer (RNFL), en face images were reconstructed by automatic segmentation of RNFL. PE values of each pixel in en face image were calculated from the mean entropy across the corresponding RNFL B-scan. Two-dimensional en face entropy maps were then reconstructed from the three-dimensional dataset.
The presence of intraretinal emboli in each imaging modality was independently assessed by two masked graders (R.T. and K.A), who were aware of the diagnosis of BRAO but masked to the findings of the other imaging modalities. Lesions were considered positive when both graders agreed on their presence. Inter-grader agreement for embolus detection was assessed using Cohen’s kappa coefficient. For entropy quantification of retinal emboli, the region of interest (ROI) was manually cropped to delineate the embolic lesion. The mean entropy and reflectivity of the entire RNFL were calculated as the internal background reference.
Statistical Analysis
Because of the exploratory retrospective nature of this pilot study, no formal sample size or statistical power calculation was performed. All eligible BRAO eyes examined during the study period were included. All statistical analyses were performed using JMP Pro software (version 18; JMP Statistical Discovery LLC, Cary, NC, USA). McNemar’s exact test was used to compare the detection rates of retinal emboli between SS-OCT and PS-OCT. Continuous data are presented as mean ± standard deviation (SD). In comparing parameters in identical eyes (eg. PS-OCT vs SS-OCT, lesion vs background), Wilcoxon signed-rank test was performed to compare two groups. Given the exploratory nature of this pilot study, adjustments for multiple comparisons were not performed. A p-value < 0.05 was considered statistically significant.
Results
Participants
Eight eyes from eight patients with BRAO were included in this study. The mean age was 62.6 ± 12.9 years (range, 37–75 years). Two patients were female, and six were male. Ophthalmologic examinations were performed 15.1 ± 17.1 days after the symptom onset. The mean BCVA was 0.0317 ± 0.125 logMAR. Among them, five eyes (62.5%) exhibited visible thromboemboli. Five eyes (62.5%) had occlusion site in intrapapillary area, and the others presented in peripapillary area. Table 1 shows epidemiologic and baseline characteristics.
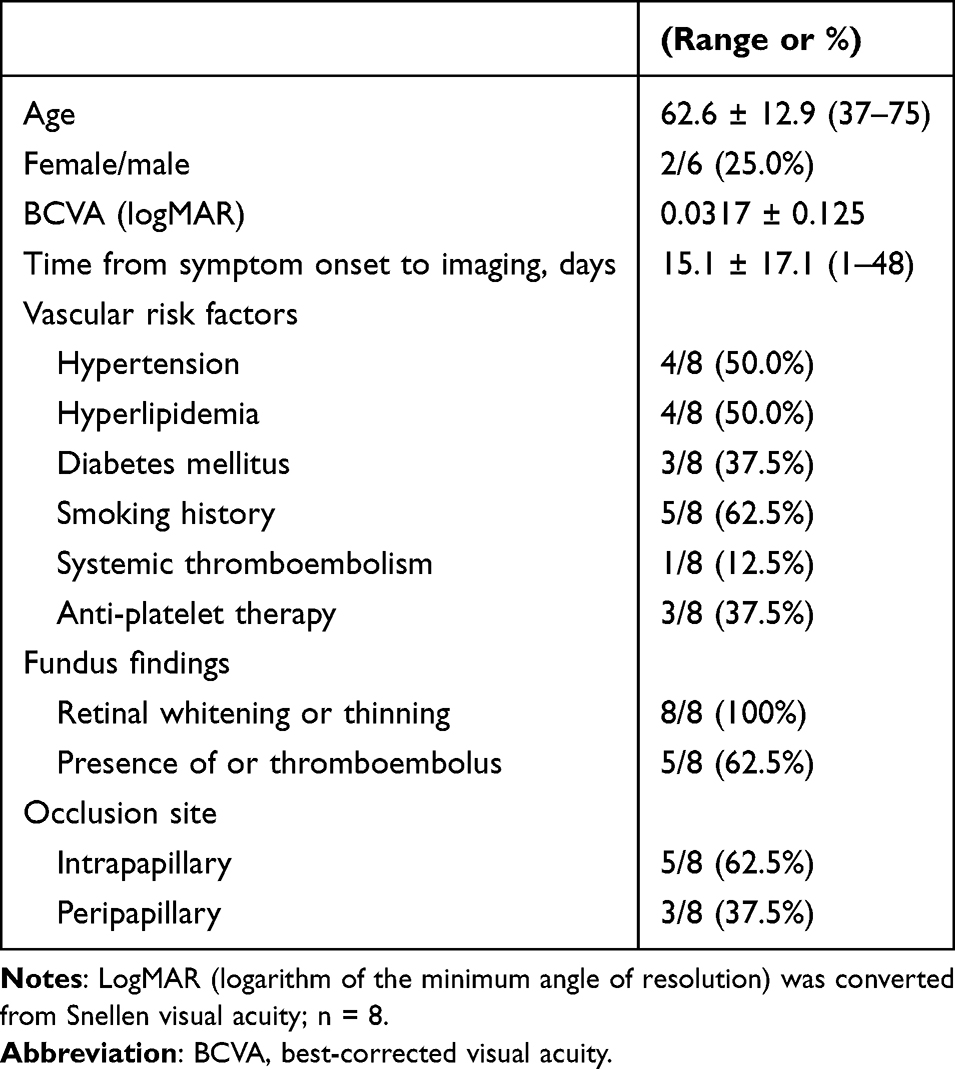 |
Table 1 Epidemiologic and Baseline Characteristics of Patients with Branch Retinal Artery Occlusion |
PS-OCT Identifies Emboli in BRAO
SS-OCT found a high reflectivity lesion corresponding to retinal emboli in two cases (25.0%) (Figure 1A–D). In PS-OCT images, a focal region of high entropy was observed corresponding to the emboli (Figure 1E and F). PS-OCT identified intraluminal thromboembolic lesions in all eyes (100%), including those without visible plaques on fundus photography (Figure 2A–F). For SS-OCT, inter-grader agreement was substantial (Cohen’s κ = 0.71). For PS-OCT, Cohen’s κ could not be calculated because both graders identified embolic lesions in all eyes, resulting in no variability in classification. En face entropy maps reconstructed from RNFL also demonstrated that retinal emboli appeared as the highly entropic foci within the neurosensory retina, whereas SS-OCT showed no increased reflectivity in the lesions (Figure 2G and H), indicating the high sensitivity of PS-OCT. Moreover, area of thickened retina by artery occlusion did not exhibit increased entropy, indicating that ischemic changes did not affect the increased entropy. The detection rate of retinal emboli by PS-OCT was higher than that of SS-OCT (Table 2).
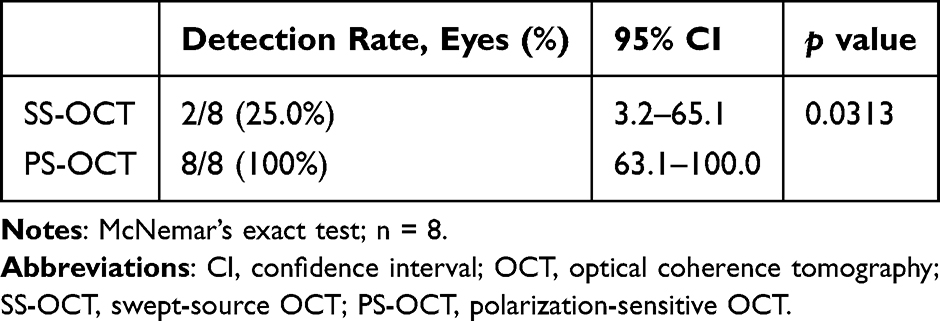 |
Table 2 Detection Rate of Retinal Emboli by OCT Modality |
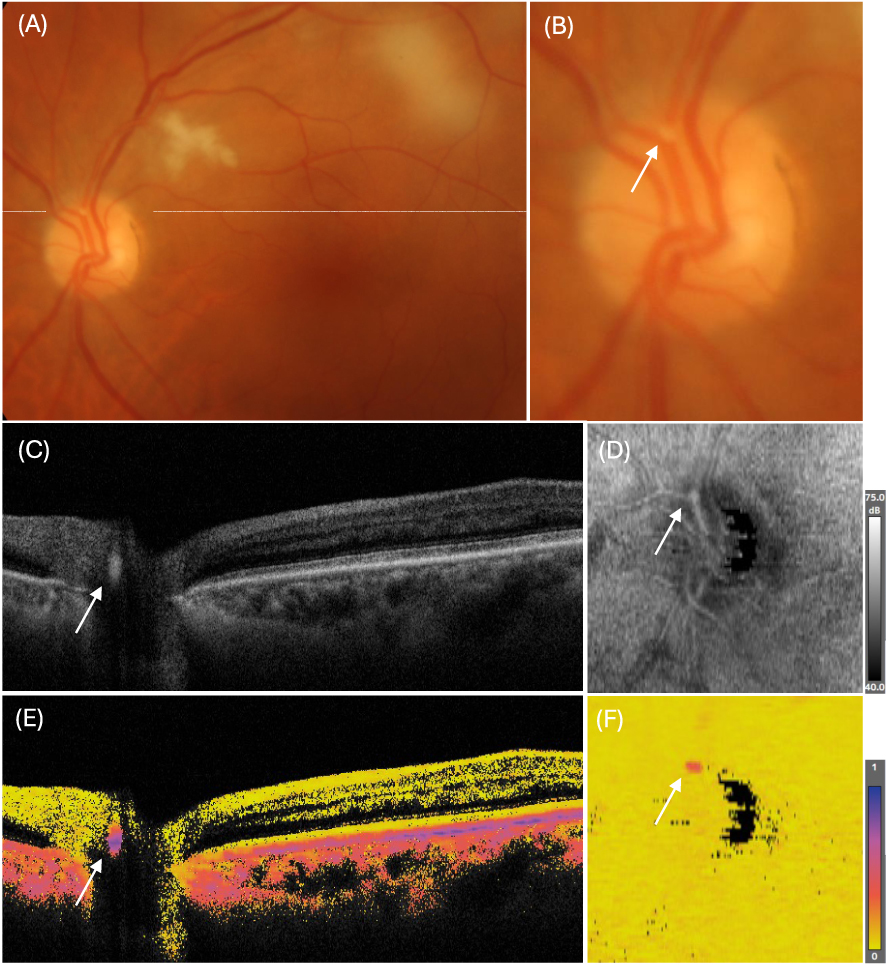 |
Figure 1 Representative images of eye with retinal emboli visible in fundus photography and conventional optical coherence tomography (OCT). (A) Fundus photography of affected eye exhibited a thromboembolic lesion in retinal artery (arrow). (B) The magnified image of optic nerve. (C) A swept-source OCT B-scan image corresponding to the occlusion site indicated by a dash line in (A). A high-reflective lesion corresponding to the emboli was observed (arrow). (D) En face image reconstructed from reflectivity of retinal nerve fiber layer (RNFL). (E) A polarization-sensitive OCT (PS-OCT) B-scan image revealed a high-entropy lesion corresponding to the emboli (arrow). (F) En face image of PS-OCT reconstructed from reflectivity of RNFL layer. The arrow corresponds to the high-entropy foci in PS-OCT. Entropy maps were displayed using an identical color scale ranging from 0 (yellow, low entropy) to 1 (purple, high entropy) across all PS-OCT images. |
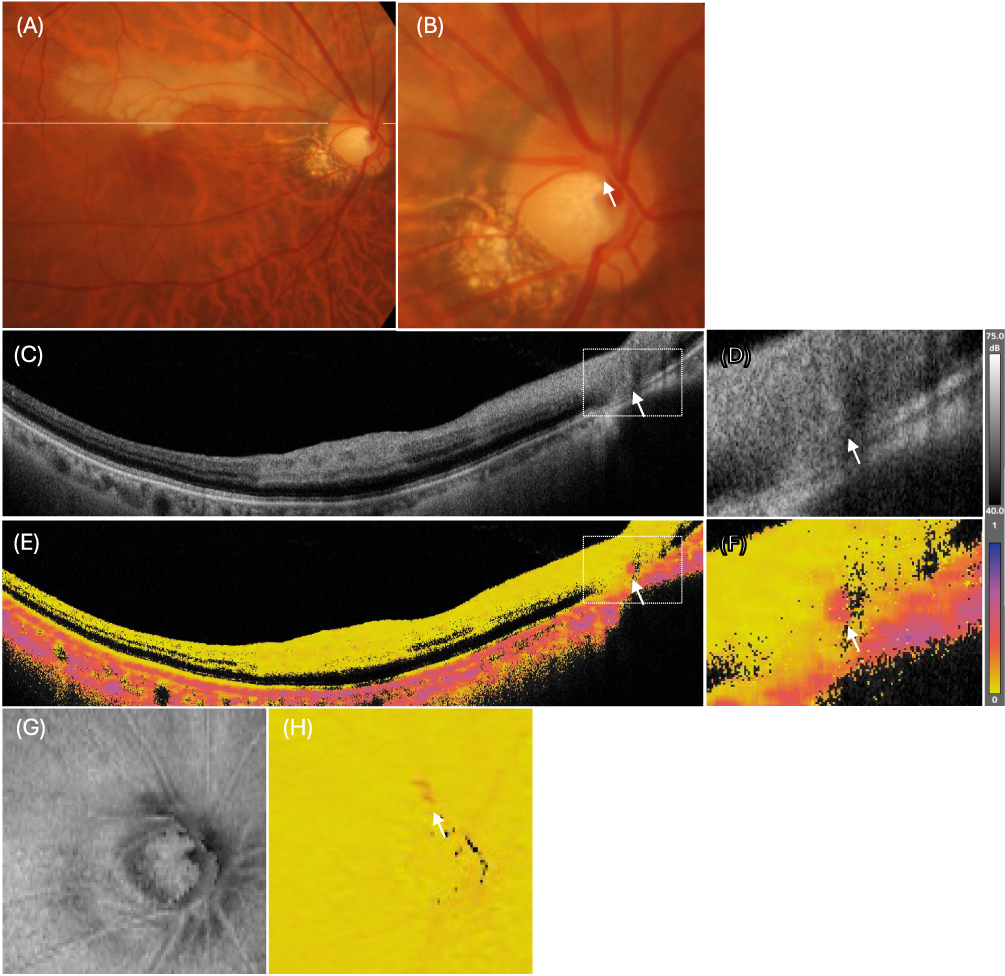 |
Figure 2 Representative images of eye without visible emboli. (A) Fundus photography of affected eye exhibited sectorial retinal whitening corresponding to the distribution of an affected branch retinal artery. (B) The magnified image of optic nerve. While the embolic lesion was suspected within a branch retinal artery at the peripapillary region based on the affected ischemic retinal area (arrow), no visible retinal emboli were observed. (C) A B-scan image of swept-source optical coherence tomography (SS-OCT) corresponding to the occlusion site indicated by a dash line in (A). No visible retinal emboli were observed (arrow). (E) A B-scan image of polarization-sensitive optical coherence tomography (PS-OCT) revealed a high-entropy lesion corresponding to the distribution of an affected branch retinal artery (arrow). (D and F) Magnified images of the region indicated by the white dashed rectangle in (C and E). (G) En face image of SS-OCT reconstructed from reflectivity of retinal nerve fiber layer (RNFL). (H) En face image of PS-OCT reconstructed from entropy of RNFL layer. Note a high-entropy lesion corresponding to the affected branch retinal artery (arrow). Entropy maps were displayed using an identical color scale ranging from 0 (yellow, low entropy) to 1 (purple, high entropy) across all PS-OCT images. |
Entropic Profiles of Retinal Emboli
To evaluate image contrast between modalities, the reflectivity and entropy of retinal emboli were compared with internal background values. As the result, the entropy of embolic ROIs extracted from B-scan images was substantially higher than that of background (0.356 ± 0.215 vs 0.0436 ± 0.00374, p = 0.0078), whereas reflectivity did not differ significantly (53.41 ± 1.87 vs 50.92 ± 1.89; Table 3, Figure 3A and B). In en face images, the mean entropy of areas corresponding to retinal emboli was also significantly increased (0.186 ± 0.12 vs 0.0436 ± 0.00374, p = 0.0078; Figure 3D and E).
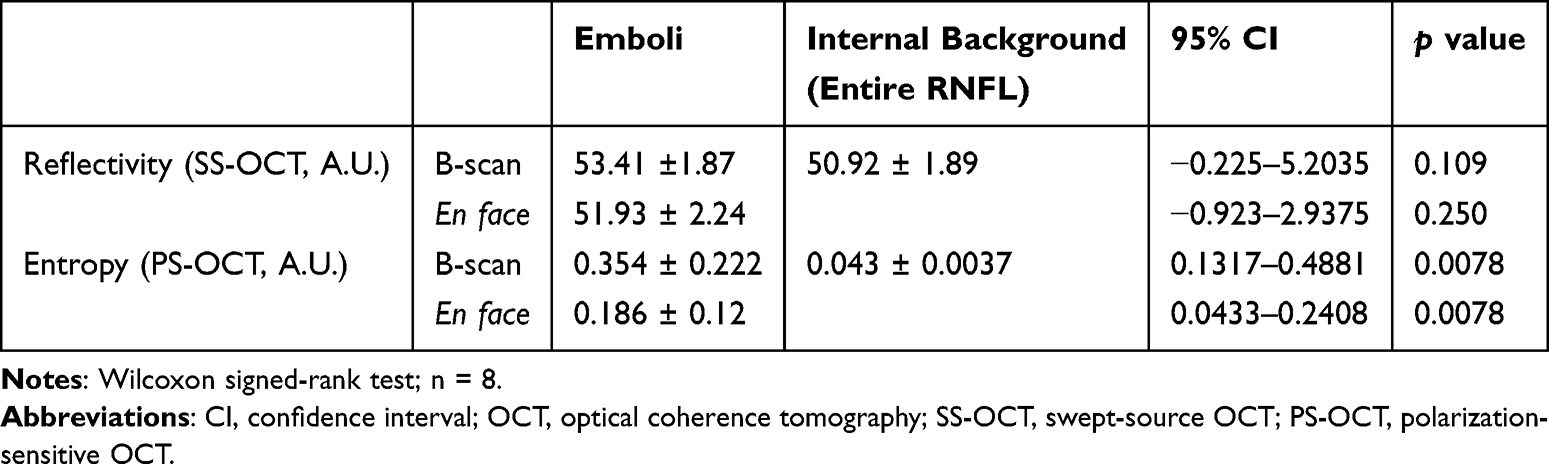 |
Table 3 Reflectivity and Entropy of Retinal Emboli Evaluated by OCT |
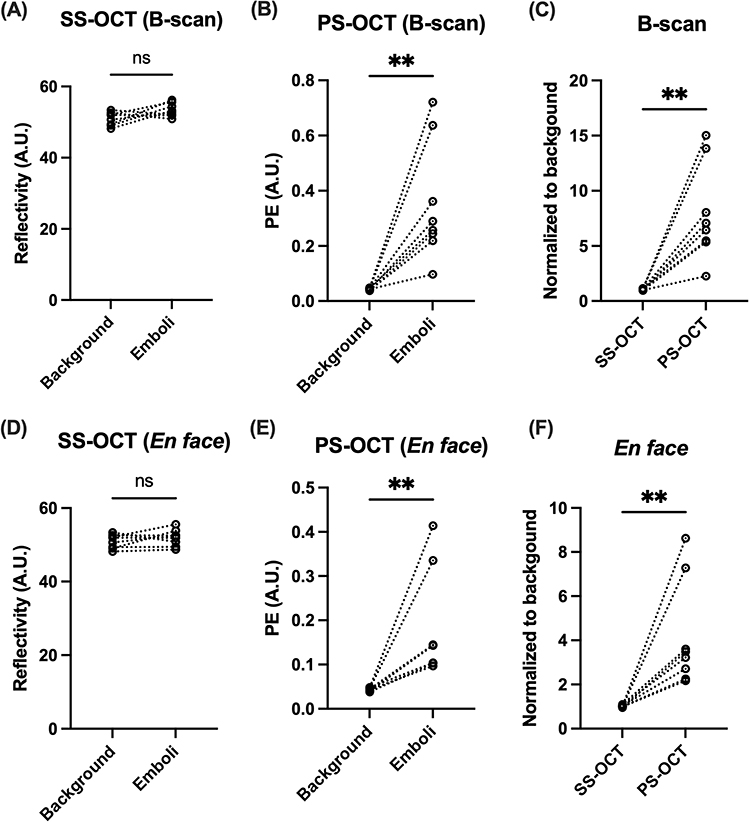 |
Figure 3 Quantification of retinal emboli using SS-OCT and PS-OCT. The signal intensity of retinal emboli and background calculated using reflectivity by SS-OCT (A) and entropy by PS-OCT (B) from B-scan images. (C) Contrast ratio calculated from B-scan images of SS-OCT and PS-OCT. The signal intensity of retinal emboli and background calculated by reflectivity by SS-OCT (D) and entropy by PS-OCT (E) from en face images. (F) Contrast ratio calculated from en face images of SS-OCT and PS-OCT. Connecting lines indicate identical eyes. Contrast was calculated as the ratio of the ROI parameter to the internal background (n = 8; Wilcoxon signed-rank test). ** p < 0.01. Abbreviations: OCT, optical coherence tomography; SS-OCT, swept-source OCT; PS-OCT, polarization-sensitive OCT; PE, polarimetric entropy; A.U., Arbitrary unit; ns, not significant. |
Moreover, we also calculated contrast ratios of embolic lesions (signal intensity relative to background). While the contrast ratio of B-scan and en face on SS-OCT was approximately “1” (1.06 ± 0.060 for B-scan, 1.02 ±0.045 for en face; Figure 3C and F), that of PS-OCT substantially increased (7.94 ± 4.36 for B-scan, 4.17 ± 2.42 for en face; Figure 3C and F). There were significant differences between SS-OCT and PS-OCT, both on B-scan and en face images (p = 0.0078, respectively; Table 4).
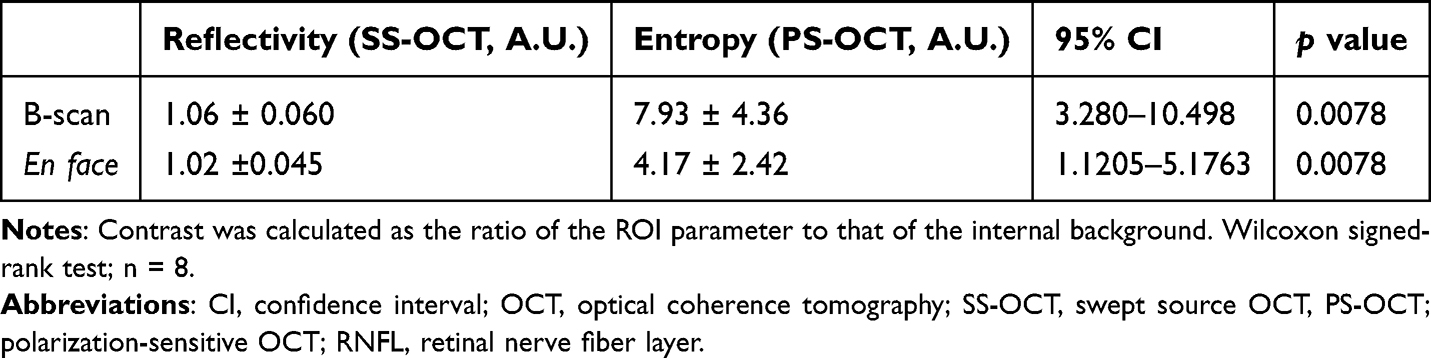 |
Table 4 Contrast of Retinal Emboli Evaluated by OCTs |
Discussion
We demonstrated that PS-OCT successfully visualized retinal emboli in eyes with BRAO as focal regions of increased polarimetric entropy within the occluded arteries. While our previous report demonstrated the feasibility of visualizing a retinal embolus using PS-OCT in a single eye,22 the present study extends this observation by demonstrating reproducible detection across multiple cases and by quantitatively characterizing embolic lesions using entropy-based analysis. These findings suggest that PS-OCT can directly identify the pathological source of retinal artery occlusion in vivo, providing additional information regarding the structural heterogeneity of embolic lesions beyond that obtainable with conventional OCT.
This study should be interpreted as an exploratory investigation because of the limited sample size, reflecting the rarity of cases. Although PS-OCT detected embolic lesions in all included eyes, the small sample size limits statistical power and the precision of the estimated detection rates. Therefore, these findings should be considered preliminary and hypothesis-generating rather than definitive evidence of superior diagnostic performance, and the results of the exact statistical analysis should be interpreted cautiously. Furthermore, no formal sample size calculation was performed because of the retrospective exploratory design. These results provide a rationale for future prospective studies with larger cohorts to validate the diagnostic performance and clinical utility of PS-OCT in retinal vascular occlusive diseases.
Although polarization-sensitive OCT is not yet routinely used in daily clinical practice, its ability to provide polarization-based tissue contrast offers unique insights into disease pathophysiology that cannot be obtained with conventional reflectivity-based OCT. This pathophysiology-oriented imaging approach complements standard structural assessment and may serve as a valuable research tool to bridge clinical findings with underlying vascular pathology. As PS-OCT technology becomes more accessible, such insights may ultimately inform future diagnostic and therapeutic strategies. Nevertheless, several practical barriers including equipment availability currently limit the widespread clinical adoption of PS-OCT. The cost-effectiveness and incremental clinical value of PS-OCT relative to existing imaging modalities also remain to be established. Consequently, PS-OCT is presently best regarded as a research-oriented imaging technology, although continued technological development and broader commercialization may facilitate future clinical implementation.
The visual prognosis of BRAO varies depending on whether the fovea is involved. Among eyes with BRAO, approximately 40–50% have a visual acuity of 20/40 or better at presentation, which improves to about 80% during follow-up.26,27 Central scotoma and peripheral nasal defect have been reported in 20% and 53% of BRAO, respectively.7 Since inner retina is supplied by the retinal artery, RAO causes inner retinal thickening in acute phase, followed by thinning in the late phase.28 The identification of retinal emboli is clinically important for both patients and clinicians, as it provides an opportunity to select appropriate therapeutic options, including surgical interventions.29,30 However, retinal emboli are visible on fundus examination in only about 34% of BRAO eyes.6 High-resolution structural OCT is highly sensitive for detecting secondary ischemic changes, including inner retinal hyperreflectivity, edema, and subsequent retinal thinning.28 It is generally difficult to identify retinal emboli by conventional OCT, except in selected cases such as calcific emboli.31 OCT angiography enables noninvasive assessment of retinal perfusion and capillary nonperfusion.32 However, neither modality consistently visualizes the embolic material responsible for arterial occlusion. In contrast, PS-OCT identified retinal emboli in all cases in this study, whereas SS-OCT detected them in only two cases (25.0%). PS-OCT may uniquely facilitate direct visualization of embolic material through polarization-based tissue contrast. Therefore, these imaging modalities should be considered complementary rather than competing approaches, providing information on ischemic tissue injury, vascular perfusion, and embolic pathology, respectively.
A previous report demonstrated that intravascular catheter-based polarization measurements enable visualization of thrombotic and atherosclerotic lesions as highly entropic structures.21 Although these differ substantially from transocular retinal PS-OCT in imaging geometry and optical conditions, both approaches quantify polarization randomness and may therefore provide information regarding tissue heterogeneity beyond conventional reflectivity-based imaging. Moreover, since all layers of the normal neurosensory retina exhibit low entropy, the presence of a high-entropy lesion can be identified with high contrast under pathological conditions,18 enabling precise evaluation of embolus size and temporal changes. In fact, although histopathological confirmation was not available, the high-entropy lesions corresponded anatomically to retinal arterial emboli identified on fundus photography and were not observed within the surrounding ischemic retina, supporting the interpretation that these signals represent embolic material.
The intraluminal high-entropy signal on PS-OCT may indicate a complex mixture of fibrin, blood cells, and lipid- or cholesterol-rich material within the thrombus, which gives rise to strong multiple scattering and polarization scrambling. In fact, PS-OCT provides complementary information on tissue composition and organization based on polarization characteristics. Pathologically, thromboembolic events typically caused by cholesterol emboli derived from atherosclerotic plaques or platelet–fibrin thrombi formed within small arteries or arterioles.33 In cases of this study, emboli could not be clearly identified by conventional OCT, whereas PS-OCT successfully visualized them as high-entropy regions, providing enhanced contrast and additional information regarding structural heterogeneity. The increased polarimetric entropy of retinal emboli likely reflects heterogeneous optical properties caused by a mixture of lipids, fibrin, blood cells, and cholesterol crystals that scramble the polarization state of backscattered light. The relatively large variability observed in PS-OCT contrast ratios suggests heterogeneity among embolic lesions. Although differences in embolus composition may contribute to this variability, the present study did not evaluate embolus composition directly, and other factors such as lesion size, location, and imaging conditions may also influence the measured contrast ratios.
There are several limitations in this study. First, the sample size was small; larger studies are needed to determine the true detection rate of PS-OCT compared with other modalities. Second, retinal emboli were evaluated only at baseline. Therefore, the temporal stability, prognostic significance, and clinical utility of the observed PS-OCT findings could not be assessed. Longitudinal studies are warranted to evaluate changes in embolic lesions over time and their relationship with clinical outcomes. Third, although image grading was performed independently and the graders were masked to the findings of the other imaging modalities, they were aware of the diagnosis of BRAO. Therefore, the possibility of observer bias cannot be completely excluded. In addition, ROI delineation was performed by manual segmentation, and formal ROI-based reproducibility analyses were not performed. Future studies incorporating independent ROI segmentation and quantitative reproducibility assessments would further strengthen the reliability of entropy-based measurements. Fourth, we could not distinguish the specific composition of emboli (cholesterol, platelet–fibrin, or calcific). Further studies are warranted to characterize polarimetric entropy profiles according to embolus subtype and to establish compositional correlations. Fifth, this study lacks healthy control eyes or eyes with other retinal vascular diseases. Although normal and ischemic retinal tissue demonstrated uniformly low entropy values and served as internal controls in the present study, the specificity of focal high-entropy signals for retinal emboli cannot be fully established. Future studies incorporating appropriate control groups will be required to determine the specificity of PS-OCT findings.
Conclusion
Although further investigations in larger cohorts are warranted to evaluate the detectability and clinical utility of PS-OCT for retinal vascular occlusions and to correlate entropy-based parameters with clinical outcomes, PS-OCT may offer advantages over conventional imaging modalities for visualizing embolic material in RAO. The observed increase in polarimetric entropy suggests that PS-OCT may provide additional information regarding structural heterogeneity of embolic lesions beyond conventional reflectivity-based imaging. However, the present study was not designed to evaluate diagnostic accuracy, clinical utility, or embolus subtype differentiation. Given the limited sample size and absence of an independent reference standard, the findings should be considered preliminary and hypothesis-generating. Larger multicenter prospective studies are warranted to further evaluate the potential value of PS-OCT-derived findings in retinal vascular occlusive disease.
Acknowledgments
The authors acknowledge Satoshi Sugiyama, Masahiro Yamanari, Kota Totani, Daisuke Santou, Nobuyori Aoki, Michiaki Okamoto, Asako Ogawa-Murano, and Kayoko Komatsu for technical assistance. Ryo Terao declares lecturer’s fees from Chugai, Bayer, and Santen, and research grant from Japan Medical Association, ARVO Foundation for Eye Research, and Kowa Life Science Foundation, Takeda Science Foundation, Manpei Suzuki Diabetes Foundation, Japan National Society For The Prevent Of Blindness, ONO Research Foundation outside this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Scott IU, Campochiaro PA, Newman NJ, Biousse V. Retinal vascular occlusions. Lancet. 2020;396(10266):1927–10. doi:10.1016/S0140-6736(20)31559-2
2. Dattilo M, Newman NJ, Biousse V. Acute retinal arterial ischemia. Ann Eye Sci. 2018;3. doi:10.21037/aes.2018.05.04.
3. Terao R, Fujino R, Ahmed T. Risk factors and treatment strategy for retinal vascular occlusive diseases. J Clin Med. 2022;11(21). doi:10.3390/jcm11216340
4. Arruga J, Sanders MD. Ophthalmologic findings in 70 patients with evidence of retinal embolism. Ophthalmology. 1982;89(12):1336–1347. doi:10.1016/s0161-6420(82)34626-6
5. Hayreh SS. Prevalent misconceptions about acute retinal vascular occlusive disorders. Prog Retin Eye Res. 2005;24(4):493–519. doi:10.1016/j.preteyeres.2004.12.001
6. Cho KH, Ahn SJ, Cho JH, et al. The characteristics of retinal emboli and its association with vascular reperfusion in retinal artery occlusion. Invest Ophthalmol Vis Sci. 2016;57(11):4589–4598. doi:10.1167/iovs.16-19887
7. Hayreh SS. Ocular vascular occlusive disorders: natural history of visual outcome. Prog Retin Eye Res. 2014;41:1–25. doi:10.1016/j.preteyeres.2014.04.001
8. Schmidt DP, Schulte-Monting J, Schumacher M. Prognosis of central retinal artery occlusion: local intraarterial fibrinolysis versus conservative treatment. AJNR Am J Neuroradiol. 2002;23(8):1301–1307.
9. Mac Grory B, Schrag M, Biousse V, et al. Management of central retinal artery occlusion: a scientific statement from the American heart association. Stroke. 2021;52(6):e282–e294. doi:10.1161/STR.0000000000000366
10. Dumitrascu OM, Koronyo-Hamaoui M. Retinal vessel changes in cerebrovascular disease. Curr Opin Neurol. 2020;33(1):87–92. doi:10.1097/WCO.0000000000000779
11. Pircher M, Hitzenberger CK, Schmidt-Erfurth U. Polarization sensitive optical coherence tomography in the human eye. Prog Retin Eye Res. 2011;30(6):431–451. doi:10.1016/j.preteyeres.2011.06.003
12. Gotzinger E, Pircher M, Hitzenberger CK. High speed spectral domain polarization sensitive optical coherence tomography of the human retina. Opt Express. 2005;13(25):10217–10229. doi:10.1364/opex.13.010217
13. Grafe MGO, van de Kreeke JA, Willemse J, et al. Subretinal fibrosis detection using polarization sensitive optical coherence tomography. Transl Vis Sci Technol. 2020;9(4):13. doi:10.1167/tvst.9.4.13
14. Lammer J, Bolz M, Baumann B, et al. Detection and analysis of hard exudates by polarization-sensitive optical coherence tomography in patients with diabetic maculopathy. Invest Ophthalmol Vis Sci. 2014;55(3):1564–1571. doi:10.1167/iovs.13-13539
15. Terao R, Saeki Y, Yashiro K, et al. Evaluation of leak sites in central serous chorioretinopathy and the effects of PDT on RPE by polarization-sensitive OCT. Transl Vis Sci Technol. 2025;14(10):14. doi:10.1167/tvst.14.10.14
16. Terao R, Yashiro K, Kuriyama T, et al. Polarimetric entropy mapping of retinal pigment epithelium in full-thickness macular hole by polarization-sensitive OCT. BMC Ophthalmol. 2026. doi:10.1186/s12886-026-05008-z
17. Azuma K, Santo D, Sugiyama S, et al. Polarization-sensitive optical coherence tomography features of the repair tissue following retinal pigment epithelium tear and functional correlation with visual outcomes. Retin Cases Brief Rep. 2025. doi:10.1097/ICB.0000000000001752
18. Terao R, Aoki S, Kitamoto K, et al. Quantification of hyperreflective foci in age-related macular degeneration by polarization sensitive optical coherence tomography. Ophthalmol Sci. 2025. doi:10.1016/j.xops.2025.100792
19. Terao R, Kitamoto K, Aoki S, et al. Short-term changes in retinal pigment epithelium after anti-vascular endothelial growth factor therapy for neovascular age-related macular degeneration evaluated by polarization-sensitive optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2025. doi:10.1007/s00417-025-06995-3
20. Jones GL, Albadawi H, Hariri LP, Bouma BE, Oklu R, Villiger M. Aging of deep venous thrombosis in-vivo using polarization sensitive optical coherence tomography. Biomed Opt Express. 2024;15(6):3627–3638. doi:10.1364/BOE.522238
21. Villiger M, Otsuka K, Karanasos A, et al. Coronary plaque microstructure and composition modify optical polarization: a new endogenous contrast mechanism for optical frequency domain imaging. JACC Cardiovasc Imaging. 2018;11(11):1666–1676. doi:10.1016/j.jcmg.2017.09.023
22. Terao R, Aoki S, Azuma K. Retinal arterial emboli visualized by polarization-sensitive OCT. Ophthalmology. 2026. doi:10.1016/j.ophtha.2025.12.002
23. Fujita A, Amari T, Ueda K, et al. Three-dimensional distribution of fundus depolarization and associating factors measured using polarization-sensitive optical coherence tomography. Transl Vis Sci Technol. 2021;10(2):30. doi:10.1167/tvst.10.2.30
24. Obata R, Yoshinaga A, Yamamoto M, et al. Imaging of a retinal pigment epithelium aperture using polarization-sensitive optical coherence tomography. Jpn J Ophthalmol. 2021;65(1):30–41. doi:10.1007/s10384-020-00787-4
25. Yamanari M, Tsuda S, Kokubun T, et al. Estimation of Jones matrix, birefringence and entropy using Cloude-Pottier decomposition in polarization-sensitive optical coherence tomography. Biomed Opt Express. 2016;7(9):3551–3573. doi:10.1364/BOE.7.003551
26. Yuzurihara D, Iijima H. Visual outcome in central retinal and branch retinal artery occlusion. Jpn J Ophthalmol. 2004;48(5):490–492. doi:10.1007/s10384-004-0102-y
27. Mason JO 3rd, Shah AA, Vail RS, Nixon PA, Ready EL, Kimble JA. Branch retinal artery occlusion: visual prognosis. Am J Ophthalmol. 2008;146(3):455–457. doi:10.1016/j.ajo.2008.05.009
28. Hakim N, Hakim J. Intra-arterial thrombolysis for central retinal artery occlusion. Clin Ophthalmol. 2019;13:2489–2509. doi:10.2147/OPTH.S232560
29. Bi DG, Ma BW, Wang WL, Zhang W, Li ZQ. Modified YAG laser treatment of retinal artery occlusion. Lasers Med Sci. 2025;40(1):410. doi:10.1007/s10103-025-04666-7
30. Kadonosono K, Hayashi A, de Juan E Jr. Endovascular surgery in the field of ophthalmology. Jpn J Ophthalmol. 2021;65(1):1–5. doi:10.1007/s10384-020-00776-7
31. Shah VA, Wallace B, Sabates NR. Spectral domain optical coherence tomography findings of acute branch retinal artery occlusion from calcific embolus. Ind J Ophthalmol. 2010;58(6):523–524. doi:10.4103/0301-4738.71703
32. Bonini Filho MA, Adhi M, de CarloTE, et al. Optical coherence tomography angiography in retinal artery occlusion. Retina. 2015;35(11):2339–2346. doi:10.1097/IAE.0000000000000850
33. Flaxel CJ, Adelman RA, Bailey ST, et al. Retinal and ophthalmic artery occlusions preferred practice pattern (R). Ophthalmology. 2020;127(2):P259–P287. doi:10.1016/j.ophtha.2019.09.028
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.