Back to Journals » International Medical Case Reports Journal » Volume 19
POEMS Syndrome with Peripheral Neuropathy as the First Presentation: A Case Report
Received 21 January 2026
Accepted for publication 16 April 2026
Published 27 April 2026 Volume 2026:19 594691
DOI https://doi.org/10.2147/IMCRJ.S594691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Yujie Di,1,* Chongmei Liu2,*
1Department of Internal Medicine, Yueyang Hospital Affiliated to Hunan Normal University, Yueyang, Hunan, 414000, People’s Republic of China; 2Department of Pathology, Yueyang Hospital Affiliated to Hunan Normal University, Yueyang, Hunan, 414000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chongmei Liu, Department of Pathology, Yueyang Hospital Affiliated to Hunan Normal University, No. 263 Bayue Road, Yueyang, Hunan, 414000, People’s Republic of China, Email [email protected]
Introduction: POEMS syndrome is a rare multisystem plasma cell disorder, often misdiagnosed when peripheral neuropathy is the initial manifestation. This report illustrates the effectiveness of autologous hematopoietic stem cell transplantation (ASCT) combined with lenalidomide that reversed neurological deficits, supported by objective electrophysiological evidence rarely documented.
Case Presentation: A 54-year-old Chinese woman presents with progressive bilateral lower extremity weakness, numbness, and edema. Initially misdiagnosed as suspected spinal metastases, POEMS syndrome was later confirmed by elevated serum IgG-λ M protein (2.57 g/L) and VEGF (556.74 pg/mL). Treatment follows a three-phase regimen: induction with lenalidomide (25 mg/day, days 1– 21) plus dexamethasone (20 mg/day pulsed); ASCT with cyclophosphamide mobilization, melphalan conditioning (300 mg), and CD34⁺ cell infusion (5.18× 106/kg); and maintenance with lenalidomide consolidation (25 mg/day, days 1– 14 monthly).
Results: Significant symptom resolution occurred post-treatment. Serum M-protein and VEGF normalized. Complete remission (CR) was sustained over 24 months. Repeat electromyography demonstrated sensory nerve amplitude increased 2– 4 fold (eg, left sural nerve: 2.2 → 9.0 μV) and motor conduction velocity improved > 50% in lower limbs (eg, left tibial nerve: 15.8 → 36.7 m/s).
Conclusion: This case demonstrates that ASCT-lenalidomide combination achieves dual neurological and hematological remission in POEMS syndrome. Early VEGF testing and multidisciplinary collaboration are critical to prevent diagnostic delays. Quantitative EMG improvement provides objective evidence for treatment efficacy assessment.
Keywords: POEMS syndrome, peripheral neuropathy, electromyography, autologous hematopoietic stem cell transplantation, lenalidomide
Introduction
POEMS syndrome is a monoclonal plasma cell proliferative disorder and a paraneoplastic syndrome associated with abnormal plasma cell proliferation. Due to its rarity, multisystem involvement, and high clinical heterogeneity, early diagnosis poses significant challenges, and it is frequently misdiagnosed because of its neuropathy-predominant onset. Although peripheral neuropathy as a first presentation is a recognized feature, detailed longitudinal electromyography (EMG) data documenting objective neurological recovery after treatment are rarely reported. This article reports a case of POEMS syndrome presenting with peripheral neuropathy as the initial manifestation, demonstrating how early VEGF testing and ASCT-based therapy reverse neurological deficits. We herein describe the diagnostic process to explore its clinical characteristics and management approach, followed by an analysis of prognosis, long-term management, and future directions.
Case Presentation
A 54-year-old female patient presented to an external hospital in January 2022 with intermittent claudication. PET-CT suggested possible lumbar metastasis, but lumbar biopsy revealed no malignant evidence. Symptoms subsequently worsened, manifesting as bilateral lower limb weakness, numbness, and edema, exacerbated by activity, accompanied by night sweats. Lower limb edema was worse in the evening. EMG performed externally revealed: bilateral lower limb peripheral neuropathy, primarily demyelinating changes with concomitant axonal involvement, affecting both proximal and distal segments, with involvement of the deep sensory pathway from the lower limbs to the cerebral cortex. Further investigations, including bone marrow aspiration and biopsy, detected a minor population of plasma cells by flow cytometry. Immunofixation electrophoresis was positive for IgG λ-type M-protein. A plasma cell dyscrasia-related disorder was suspected. The patient was subsequently referred to our hospital for further evaluation.
Key Investigation Results (Table 1): Upon referral, a detailed clinical examination revealed additional findings consistent with POEMS syndrome. The patient had diffuse skin hyperpigmentation, most pronounced on the lower extremities and trunk. Endocrine evaluation demonstrated abnormalities in multiple axes: impaired glucose tolerance (fasting glucose 6.3 mmol/L, 2-hour postprandial glucose 11.2 mmol/L) and primary hypothyroidism (TSH 8.5 mIU/L, free T4 0.7 ng/dL). Abdominal ultrasound revealed mild hepatomegaly (span 16 cm) and moderate splenomegaly (span 14 cm). There was no evidence of lymphadenopathy.
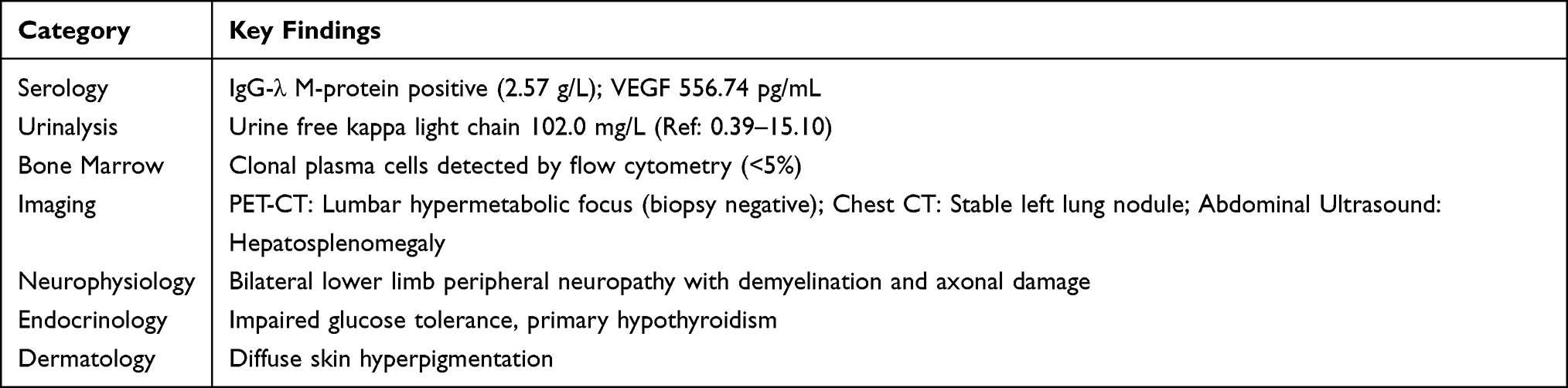 |
Table 1 Key Diagnostic Findings at Presentation |
Based on the presence of polyneuropathy (mandatory), monoclonal plasma cell proliferation (mandatory), elevated VEGF (major), endocrinopathy (minor), organomegaly (minor), skin changes (minor), and extravascular volume overload (edema, minor), the patient fulfilled the diagnostic criteria for POEMS syndrome.
After obtaining informed consent, systemic treatment was initiated as follows:
Induction Therapy (April 4, 2022): Lenalidomide 25 mg/day (days 1–21) + Dexamethasone 20 mg/day (days 1, 2, 8, 9, 15, 16, 21, 22), supported by gastroprotective and hepatoprotective agents. Partial symptomatic relief was achieved.
Mobilization/Collection & ASCT (May 31 - July 8, 2022): Mobilization with Cyclophosphamide (3100 mg total, 50mg/kg/day on days 1–2). Peripheral blood stem cell collection yielded CD34+ cells: 5.18 × 106/kg. The patient was admitted to a laminar flow room. Conditioning with Melphalan (300 mg) was followed by autologous stem cell infusion. The procedure was uneventful.
Maintenance Therapy (Starting October 2022): Lenalidomide (25 mg/day, days 1–14) combined with Dexamethasone (20.25 mg/day on days 1, 8, 15) to consolidate efficacy.
Follow-up: Assessments in October 2022, April 2023, and April 2024 consistently showed CR with sustained symptomatic improvement. VEGF and M-protein became undetectable The skin hyperpigmentation gradually faded, and the hepatosplenomegaly resolved on follow-up imaging. The patient’s endocrine function partially improved, with normalization of blood glucose levels and a reduced requirement for thyroid hormone replacement.
Discussion
POEMS syndrome is a complex and rare hematological disorder. The acronym, proposed by Bardwick et al,1 originates from five key clinical features: Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal protein (M-protein), and Skin changes. It is characterized by peripheral nerve demyelination and monoclonal plasma cell proliferation, with an estimated prevalence of approximately 0.3 per 100,000 individuals.2 A definitive diagnosis requires meeting two mandatory criteria (polyneuropathy and monoclonal plasma cell disorder), at least one major criterion (including elevated VEGF), and at least one minor criterion (organomegaly, endocrinopathy, skin changes, etc).3
Overproduction of vascular endothelial growth factor (VEGF) is a central feature of POEMS syndrome, contributing to peripheral nerve damage through disruption of the blood-nerve barrier.4,5 In our patient, the initially elevated VEGF level (556.74 pg/mL) normalized after treatment, correlating with significant clinical and electrophysiological improvement.
The detailed quantitative EMG findings in this case (Table 2 and Figures 1–4) provide objective evidence of neurological recovery following ASCT and lenalidomide therapy. Improvements were observed not only in distal lower limb nerves but also in proximal segments, suggesting a global reversal of neuropathic processes. This degree of electrophysiological documentation is uncommon in case reports and underscores the potential for nerve regeneration even in severe neuropathy.
 |
Table 2 Comparison of Pre-Treatment (2022) and Post-Treatment (2024) Electromyography (EMG) Findings |
 |
Figure 1 Left superficial peroneal sensory nerve (Mid/Low lateral leg - Ankle; 20 μV/division, 2 ms/division). |
 |
Figure 2 Right superficial peroneal sensory nerve (Mid/Low lateral leg - Ankle; 20 μV/division, 2 ms/division). |
 |
Figure 3 Left sural sensory nerve (Mid/Low posterior leg - Lateral malleolus; 20 μV/division, 2 ms/division). |
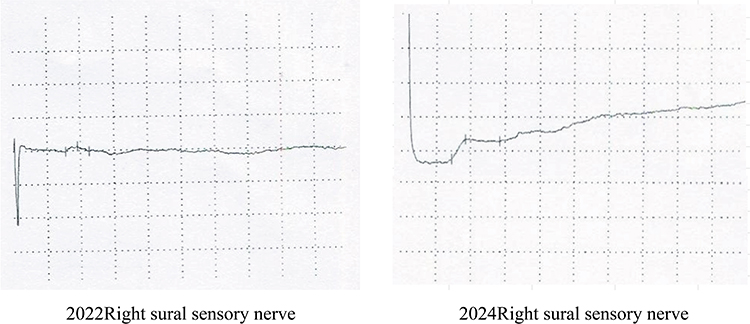 |
Figure 4 Right sural sensory nerve (Mid/Low posterior leg - Lateral malleolus; 20 μV/division, 2 ms/division). |
While the combination of ASCT and lenalidomide is not novel as a concept, this case highlights the importance of a sequential, well-documented approach. ASCT serves as a potent debulking therapy, while lenalidomide maintenance may help suppress residual clones and prevent relapse.6,7 Recent reviews have further supported the efficacy of this treatment paradigm in POEMS syndrome.8,9 However, lenalidomide, while considered less neurotoxic than thalidomide, still carries a potential risk of peripheral neuropathy, necessitating close neurological monitoring.10 In this patient, no worsening of neuropathy was observed, and instead, continued improvement was noted during maintenance, suggesting a favorable risk-benefit profile. Long-term follow-up studies indicate that sustained remission is achievable with such approaches, though late relapse remains a consideration.11
This report has several limitations. As a single case study, the findings are not generalizable to all POEMS patients. The follow-up period of 24 months, while showing sustained remission, is insufficient to assess long-term outcomes such as late relapse or secondary malignancies. Additionally, the relative contributions of ASCT versus lenalidomide maintenance to the observed neurological recovery cannot be definitively separated. Standardized neuropathy scales and minimal residual disease assessment were not employed, which would have provided additional granularity. As a single case, the findings require validation in larger cohorts.
Differential diagnosis is crucial for POEMS syndrome. Its peripheral neuropathy must be distinguished from chronic inflammatory demyelinating polyneuropathy (CIDP), which typically lacks M-protein and multisystem involvement. Sclerotic bone lesions need differentiation from multiple myeloma, which primarily causes lytic bone destruction and is often associated with hypercalcemia and renal insufficiency.12 This patient was initially suspected of having metastatic bone disease, highlighting the diagnostic challenge and the value of a multidisciplinary approach in recognizing the constellation of symptoms.
Conclusion
This case illustrates a favorable outcome in a POEMS syndrome patient presenting with peripheral neuropathy, treated effectively with ASCT and lenalidomide induction/maintenance. The detailed EMG data provide valuable objective evidence of neurological recovery. However, clinicians should recognize that such outcomes may not be representative of all patients. The case underscores the need for a high index of suspicion for POEMS in patients with unexplained peripheral neuropathy, especially when accompanied by seemingly unrelated systemic findings. In particular, in patients with unexplained demyelinating polyneuropathy and systemic features, serum VEGF screening should be considered as a valuable diagnostic tool. Early VEGF testing and multidisciplinary collaboration are critical to prevent diagnostic delays. Future research should focus on optimizing patient selection for ASCT and defining the role of maintenance therapy, with careful consideration of individual patient risk factors.
Abbreviations
APB, Abductor Pollicis Brevis; ADM, Abductor Digiti Minimi; EDB, Extensor Digitorum Brevis; AH, Abductor Hallucis; EDC, Extensor Digitorum Communis; Lat., Latency; Amp., Amplitude; Dist., Distance; CV, Conduction Velocity; S, Sensory; M, Motor; Post., Posterior; Lat., Lateral/Lateralis; Med., Medialis; Ref., Reference.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethical Approval Statement
Approval was obtained from the Ethics Committee of Yueyang Hospital Affiliated to Hunan Normal University for the publication of this case report. Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Bardwick PA, Zvaifler NJ, Gill GN, et al. Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature. Medicine. 1980;59(4):311–7. doi:10.1097/00005792-198007000-00006
2. Tan S, Shang M, Masaki Y, et al. Case report: atypical POEMS syndrome without polyneuropathy, complicated by borderline TAFRO syndrome. Front Med Lausanne. 2024;11:1445971. doi:10.3389/fmed.2024.1445971
3. Dispenzieri A. POEMS syndrome: 2021 update on diagnosis, risk-stratification, and management. Am J Hematol. 2021;96(7):872–888. doi:10.1002/ajh.26240
4. Dispenzieri A. POEMS syndrome: 2019 update on diagnosis, risk-stratification, and management. Am J Hematol. 2019;94(7):812–827. doi:10.1002/ajh.25495
5. Zhang ZG, Zhang L, Jiang Q, et al. VEGF enhances angiogenesis and promotes blood-brain barrier leakage in the ischemic brain. J Clin Invest. 2000;106(7):829–838. doi:10.1172/JCI9369
6. Khouri J, Nakashima M, Wong S. Update on the diagnosis and treatment of POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes) syndrome: a review. JAMA Oncol. 2021;7(9):1383–1391. doi:10.1001/jamaoncol.2021.0586
7. Kim YR. Update on the POEMS syndrome. Blood Res. 2022;57(S1):S27–31. doi:10.5045/br.2022.2022001
8. Dispenzieri A. POEMS syndrome: update on diagnosis, risk-stratification, and management. Am J Hematol. 2020;95(7):803–814.
9. Li J, Huang XF, Cai QQ, et al. A prospective phase II study of low dose lenalidomide plus dexamethasone in patients with newly diagnosed polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes (POEMS) syndrome. Am J Hematol. 2018;93(6):803–809. doi:10.1002/ajh.25100
10. Kuwabara S, Misawa S, Kanai K, et al. Neurologic improvement after peripheral blood stem cell transplantation in POEMS syndrome. Neurology. 2008;71(21):1691–1695. doi:10.1212/01.wnl.0000323811.42080.a4
11. Kourelis TV, Baudi FK, Kumar SK, et al. Long-term outcomes of patients with POEMS syndrome. Blood. 2013;122(21):4026.
12. Mauermann ML. The peripheral neuropathies of POEMS syndrome and castleman disease. Hematol Oncol Clin North Am. 2018;32(1):153–163. doi:10.1016/j.hoc.2017.09.012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.