Back to Journals » Vascular Health and Risk Management » Volume 21
Platelet-to-Hemoglobin Ratio in Predicting Major Adverse Cardiovascular Events After Coronary Artery Bypass Grafting
Authors Chen S ![]() , Zhang K, Liu X, Yang Z, Guan X, Zhou X, Xiao J, Li X, Jin J, Ma X
, Zhang K, Liu X, Yang Z, Guan X, Zhou X, Xiao J, Li X, Jin J, Ma X ![]() , Li Q
, Li Q
Received 21 August 2025
Accepted for publication 29 November 2025
Published 10 December 2025 Volume 2025:21 Pages 1047—1058
DOI https://doi.org/10.2147/VHRM.S562298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Harry Struijker-Boudier
Shanghao Chen,1– 3,* Kefan Zhang,1,2,* Xuantao Liu,1,2,* Zhihao Yang,1,2,* Xiang Guan,1,2 Xin Zhou,1,2 Junwen Xiao,1,2 Xiaofang Li,1,2 Jing Jin,1,2 Xiaochun Ma,4 Qingguo Li1,2
1Department of Cardiovascular Surgery, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2Artificial Heart Research Institute, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3Department of Cardiovascular Surgery, Shandong Provincial Hospital of Shandong University, Jinan, Shandong, People’s Republic of China; 4Department of Cardiovascular Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingguo Li, Department of Cardiovascular Surgery, The Second Affiliated Hospital of Nanjing Medical University, No. 290 Heyan Road, Nanjing, Jiangsu, 210003, People’s Republic of China, Tel +0086 025 22681, Email [email protected] Xiaochun Ma, Department of Cardiovascular Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, No. 324 Jingwu Road, Jinan, Shandong, 250021, People’s Republic of China, Tel +86 531 6877 6353, Email [email protected]
Purpose: Coronary artery bypass grafting (CABG) is widely recognized as the gold standard treatment for patients with complex coronary artery disease (CAD). The identification of reliable hematologic predictors for major adverse cardiovascular events (MACE) after CABG remains limited. In recent years, the platelet-to-hemoglobin ratio (PHR) has emerged as a promising prognostic marker in various cardiovascular conditions and malignancies. This study investigated the prognostic value of the PHR for predicting in-hospital and short-term adverse outcomes after CABG.
Patients and Methods: This retrospective cohort study included 1672 Chinese patients who underwent isolated CABG surgery between 2015 and 2021. PHR was calculated as platelet count (× 109/L) divided by hemoglobin (g/L). The primary endpoint was 3-point MACE (3P-MACE), including cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke during hospitalization. A predictive nomogram was developed and validated using bootstrap resampling.
Results: In our study, individuals with elevated PHR levels were more likely to experience 3P-MACE and stroke. After propensity matching, the incidence of 3P-MACE was 5.7% in the high PHR group (PHR≥ 1.890) and 1.5% in the low PHR group (P = 0.010). Multivariate analysis identified preoperative PHR (odds ratio: 1.800 [95% CI 1.073– 3.021], P=0.026) as an independent predictor for 3P-MACE post-CABG. A predictive nomogram for 3P-MACE following CABG was successfully developed. The predictive performance of PHR was comparable to NLR and PLR, with an area under the ROC curve (AUC) of 0.595 (95% CI 0.486– 0.691). Combining PHR with nomogram parameters improved AUC to 0.762 (95% CI 0.687– 0.837).
Conclusion: Elevated PHR (≥ 1.890) was independently associated with postoperative 3P-MACE, reflecting the integrated effects of thrombosis and anemia risk. Although PHR demonstrated modest discrimination as a single variable, its integration into a multivariable nomogram improved predictive accuracy. These findings are hypothesis-generating and future multicenter, prospective validation studies are warranted.
Keywords: platelet-to-hemoglobin ratio, predicting, major adverse cardiovascular events, coronary artery bypass, nomograms
Introduction
Coronary artery disease (CAD) remains a leading global cause of mortality, despite significant advancements in coronary interventions and pharmacotherapy.1–5 Coronary artery bypass grafting (CABG) is widely regarded as the gold standard for managing complex CAD due to its established reliability and efficacy over many years.6–8 This underscores the necessity for practical and straightforward prognostic indicators to evaluate post-CABG patient outcomes, enabling the implementation of effective and timely intervention strategies.
Numerous studies have highlighted the prognostic significance of various peripheral blood cells and associated ratios in predicting inflammation and adverse cardiovascular outcomes.9–13 Recent studies have highlighted platelet-to-lymphocyte ratio (PLR) and neutrophil-to-lymphocyte ratio (NLR) as predictors of cardiovascular outcomes, yet their prognostic performance remains inconsistent.14,15 Furthermore, the platelet-to-hemoglobin ratio (PHR) has emerged as a notable prognostic marker in multiple cardiovascular diseases and certain cancers.16,17 Previous research has indicated that elevated PHRs may offer better predictive value for adverse events in patients undergoing percutaneous coronary intervention (PCI) compared to platelet and hemoglobin levels alone.18 However, the PHR—a composite measure integrating thrombosis potential and oxygen-carrying capacity—has not been systematically evaluated in CABG patients.18–20 Given that both thrombocytosis and anemia are linked to perioperative ischemic events and poor tissue oxygenation,21,22 PHR may serve as a biologically plausible and readily available biomarker.
We therefore aimed to ascertain whether PHR serves as an independent predictive indicator for 3-point major adverse cardiovascular events (3P-MACE) post-CABG, and to develop a nomogram specifically tailored for 3P-MACE prediction.
Materials and Methods
Study Design
The investigation was approved by the Shandong Provincial Hospital Biomedical Research Ethics Committee (SWYX: No 2022-498; 4 November 2022), all methods were performed in accordance with the relevant guidelines and regulations, patient consent was waived for analysis and publication of patient data in anonymized fashion. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki (2013 revision). This retrospective study included consecutive adults undergoing isolated CABG at Shandong Provincial Hospital between January 2015 and December 2021. Inclusions comprised patients (1) undergoing CABG procedures and (2) age ≥18 years. Exclusions comprised patients undergoing concomitant cardiovascular procedures such as valve replacement, valve repair, and aneurysm removal. Patients with incomplete preoperative platelet and hemoglobin data exceeding 5% were also excluded. Ultimately, 1672 patients were included for analysis.
Data Collection and Variables
Preoperative laboratory data, including platelet count, hemoglobin, neutrophil, and lymphocyte levels, were obtained from the first blood test within 24 hours before surgery. PHR was defined as platelet count (×109/L) divided by hemoglobin (g/L). Platelet and hemoglobin levels were measured using a standardized hematology analyzer (Mindray BC-6800, China). Preoperative imaging examinations such as echocardiographic (ECG), ultrasound, and computed tomography (CT) were completed within 3 days after admission.
CABG and Support Techniques
Surgical approaches for CABG, including off-pump CABG (OPCABG) and minimally invasive direct coronary artery bypass grafting (MIDCABG), were determined based on the patient’s cardiac symptoms and CAD severity. Median sternotomy was the standard approach, with MIDCABG preferred for isolated proximal disease of specific arteries. Following CABG, all patients received dual antiplatelet therapy (DAPT) comprising aspirin and clopidogrel.
End Points
The primary endpoint was 3P-MACE, a composite of cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke during hospitalization. Secondary endpoints included in-hospital cardiovascular mortality, postoperative events, lengths of stay, intubation time, ICU stays, readmission, and reoperation.
Clinical Definition
The patient’s medical history is outlined in the Document S1.
Quantification and Statistical Analysis
Presentation
Statistical analyses were carried out with SPSS statistical software, version 25.0, Stata statistical software, version 16.0, and R statistical software, version 4.5.1. Continuous variables were presented as means ± SD or medians and interquartile ranges (IQR), while categorical data were expressed as frequencies or percentages. To test for significant differences between groups, the t-test or Mann–Whitney U-test and χ2 test or Fisher’s exact test were used. For all two-tailed tests, a P value below 0.05 was regarded as statistically significant.
Nomogram
Nomograms are increasingly in use for predictive analysis due to their simplicity, intuitiveness and advanced capabilities.23 Univariable and multivariable logistic regression analyses identified independent predictors of 3P-MACE. ROC analysis identified the optimal PHR cutoff (1.890) using the Youden index. Internal validation was conducted using 1000 bootstrap resamples to estimate model stability and optimism-corrected AUC. The multivariable logistic regression models incorporated variables with P value <0.05, along with potential predictive factors identified in the univariable models. The selection of variables for inclusion in the models was guided by Forward: LR with probabilities of 0.05 and 0.10 for inclusion and exclusion, respectively. Candidate nomogram models were carefully crafted based on these significant risk factors to ensure robust predictive power. The predictive performance of the nomogram, as well as other models in predicting 3P-MACE, was quantified using the area under the curve (AUC). Furthermore, a well-calibrated curve was fitted to evaluate the nomogram’s predictive accuracy. To address the potential limitations of receiver operating characteristic (ROC) curves in simultaneously optimizing sensitivity and specificity, decision curve analysis (DCA) was employed to assess the clinical utility of the nomograms.
Propensity Matching
To evaluate the association between PHR and 3P-MACE, we employed propensity score matching to categorize patients based on whether their PHR exceeded 1.89. Initially, a parsimonious model was developed using multivariate logistic regression, as outlined in the previous section. Subsequently, clinically relevant variables that were not significantly associated with postoperative 3P-MACE were added to the fitted model to create a propensity-matched model. The effectiveness of the propensity matching model was assessed using kernel density plots and propensity matching test plots.
Results
Patient Characteristics
Altogether, 1799 patients were enrolled from January 1, 2015 to December 31, 2021. Exclusions were made for 29 patients who underwent concomitant cardiovascular surgeries, such as valve replacement, valve repair, and aneurysm removal. Additionally, 68 patients with missing data exceeding 5% and 30 patients lacking preoperative platelet and hemoglobin indices were excluded (refer to Figure 1). Ultimately, 1672 patients who underwent CABG were included in the study, with the following patient characteristics observed. The mean age of study participants was 63.02 (± 7.95) years, with 72.8% being male. A majority of patients were smokers (52.5%) and had hypertension (almost 70%). The study found that patients had several comorbidities, including diabetes (38.4%), hyperlipidemia (38.6%), myocardial infarction (42.3%), cerebrovascular accident (24.3%), peripheral vascular disease (7.1%), and chronic obstructive pulmonary disease (4.0%). Prior to the surgery, the median serum creatinine (SCr) level was 68.60 (19.65) μmol/L and the mean estimated glomerular filtration rate (eGFR) was 94.01 (± 16.08) mL/min/1.73m2. The median left ventricular ejection fraction (LVEF) before the surgery was 60.0% (5.00%). Of the 1672 patients, 746 (44.5%) had left main trunk diseases. Severe carotid artery stenosis was present in 116 (6.9%) patients, while 323 (19.3%) had moderate to severe stenosis. The surgical details revealed that 97.9% of the cases underwent off-pump coronary artery bypass grafting (OPCABG), while only 1.0% underwent minimally invasive direct coronary artery bypass (MIDCAB). Following the operation, 40 (2.4%) patients experienced 3P-MACE, 30 (1.8%) had an ischemic stroke, and 6 (0.4%) required a secondary surgery for bleeding. The mean hospital stay was 18.71 (± 5.93) days, the median intubation time was 11.17 (3.92) hours, and the median ICU stay was 2.07 (1.08) days (refer to Supplementary Table S1).
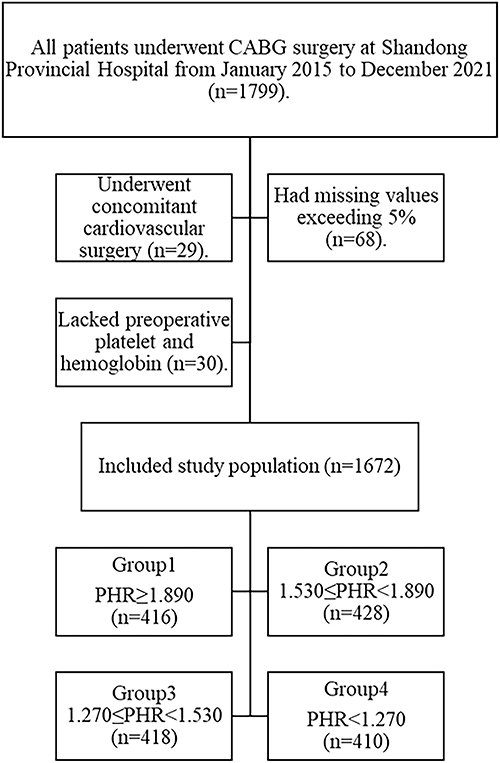 |
Figure 1 Flow diagram depicting the exclusion and enrollment of study participants. Abbreviations: CABG, coronary artery bypass grafting; PHR, platelet-to-hemoglobin ratio. Note: The flow diagram illustrates the process of participant exclusion and enrollment in the study. |
Elevated PHR Increased Incidences of 3P-MACE
The preoperative PHR had a median value of 1.53 (1.27–1.89). The cut-off level of PHR was determined through analysis of the receiver operating characteristics (ROC) curve between patients with and without 3P-MACE using the Youden index, which was found to be 1.89 (refer to Figure 2). Subsequently, to address potential sources of bias, subjects were categorized into four PHR groups: Group 1 (PHR≥1.890, n=416), Group 2 (1.530≤PHR<1.890, n=428), Group 3 (1.270≤PHR<1.530, n=418), and Group 4 (PHR<1.270, n=410). Baseline characteristics revealed that individuals with higher PHR levels had a higher prevalence of hypertension but a lower prevalence of smoking history. Moreover, those with elevated PHR levels showed a higher percentage of female participants, increased incidences of 3P-MACE and stroke, elevated levels of C-reactive protein (CRP) and B-type natriuretic peptide (BNP), and lower levels of height, weight, and serum creatinine (SCr) (refer to Supplementary Table S2).
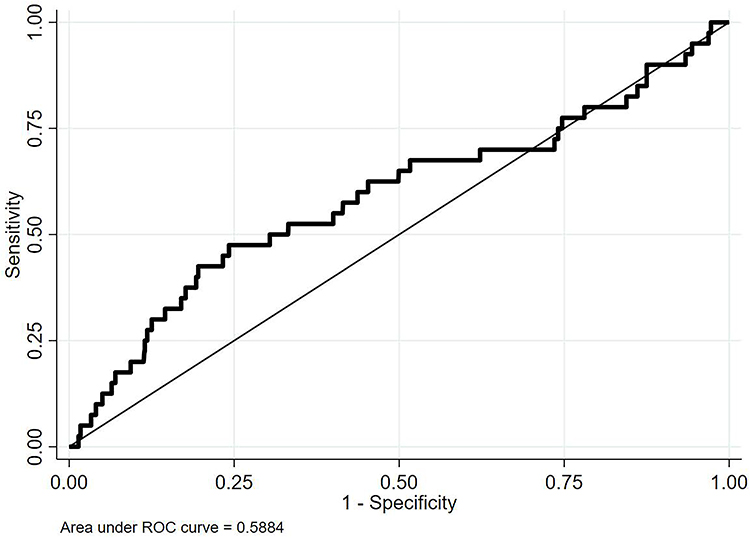 |
Figure 2 ROC curve analysis of PHR for predicting post-CABG 3P-MACE. Abbreviations: ROC, receiver operating characteristic; PHR, platelet-to-hemoglobin ratio; AUC, area under the curve; 3P-MACE, 3-point major cardiovascular adverse events; CABG, coronary artery bypass grafting. Notes: Figure 2 shows the ROC curve analysis for the AUC, sensitivity and specificity of PHR in predicting 3P-MACE following CABG. |
Risk Factors of 3P-MACE After CABG
Univariate Analysis of 3P-MACE Risk Factors After CABG
In univariate logistic regression analysis, the occurrence of 3P-MACE was found to be statistically linked to eight factors. These factors included pulse pressure, history of cerebrovascular accidents, preoperative hemoglobin levels, PHR, C-reactive protein (CRP) levels, presence of severe carotid artery stenosis, presence of moderate to severe carotid artery stenosis, and postoperative monocyte levels (refer to Supplementary Table S1). There was no statistically significant difference in NLR and PLR (P > 0.05) with less discriminative (AUC = 0.541 and 0.538, respectively), whereas PHR achieved an AUC = 0.595. The ROC analysis demonstrated that PHR alone yielded an AUC of 0.595 (95% CI 0.486–0.691) for predicting 3P-MACE, indicating a statistically significant but modest discriminative ability. This suggests that while PHR may serve as a useful indicator for risk stratification, its clinical predictive power as a standalone biomarker remains limited.
Multivariate Analysis of Risk Factors for 3P-MACE After CABG
A multivariate analysis was conducted to identify the risk factors for 3P-MACE after CABG. This analysis included all candidate variables from the univariate analysis and 16 potential predictive variables, such as age, weight, systolic blood pressure (SBP), pulse pressure, diabetes mellitus, history of cerebrovascular accidents (CVA), chronic kidney disease, preoperative hemoglobin levels, platelet-to-hemoglobin ratio (PHR), C-reactive protein (CRP), B-type natriuretic peptide (BNP), prothrombin time (PT), prothrombin time-international normalized ratio (PT-INR), presence of left main trunk disease, severe carotid artery stenosis, and postoperative monocyte levels. The study identified several independent risk factors for 3P-MACE after CABG, including age (OR 1.056, 95% CI 1.007–1.106, P = 0.024), weight (OR 1.043, 95% CI 1.013–1.075, P = 0.005), diabetes mellitus (OR 1.935, 95% CI 1.001–3.741, P = 0.050), history of CVA (OR 2.083, 95% CI 1.068–4.063, P = 0.031), PHR (OR 1.800, 95% CI 1.073–3.021, P = 0.026), and severe carotid artery stenosis (OR 3.364, 95% CI 1.497–7.558, P = 0.003) (refer to Table 1).
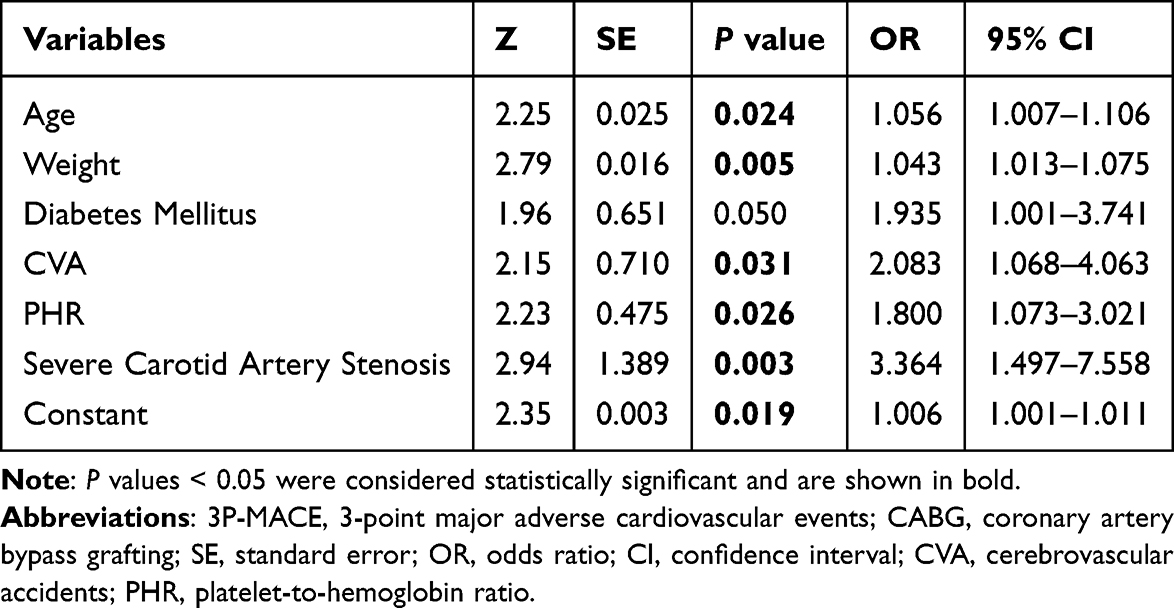 |
Table 1 Multivariate Analysis of Risk Factors for 3P-MACE After CABG |
Nomogram Model for 3P-MACE After CABG
Through ROC analysis, the individual and combined performance of the six factors from the multivariate analysis were assessed, leading to the creation of an optimal nomogram model (refer to Figure 3). The separate area under the curve (AUC) values for age, weight, diabetes mellitus, history of CVA, PHR, severe carotid stenosis, and the predictive model were 0.583, 0.586, 0.586, 0.604, 0.595, 0.586, and 0.762, respectively. The nomogram demonstrated good discrimination (AUC 0.762, 95% CI 0.687–0.837) and internal calibration using bootstrap analysis (1000 resamples) yielded stable discrimination estimates: AUC = 0.738 (95% CI: 0.656–0.812) and area under the precision-recall curve (AUPRC) = 0.623 (95% CI: 0.548–0.708). Additionally, as depicted in Figure 4, a score proportional to the value of each selected biomarker on the nomogram was assigned. The scores for each variable were summed to calculate the total score, and a vertical line was drawn on the total score to determine the corresponding probability of 3P-MACE. To validate the generalizability of the nomogram for predicting 3P-MACE incidence, a comprehensive screening was conducted. The calibration curves, as shown in Supplementary Figure S1, demonstrated good fit (Hosmer-Lemeshow P value = 0.744) and exhibited a high level of accuracy in predicting 3P-MACE incidence. Furthermore, Supplementary Figure S2 displayed the decision curve analysis (DCA) curves, indicating that the nomogram model performed well across various predictors and ensured maximal clinical utility. The DCA curves confirmed the viability of the nomogram model for making useful and beneficial decisions regarding 3P-MACE.
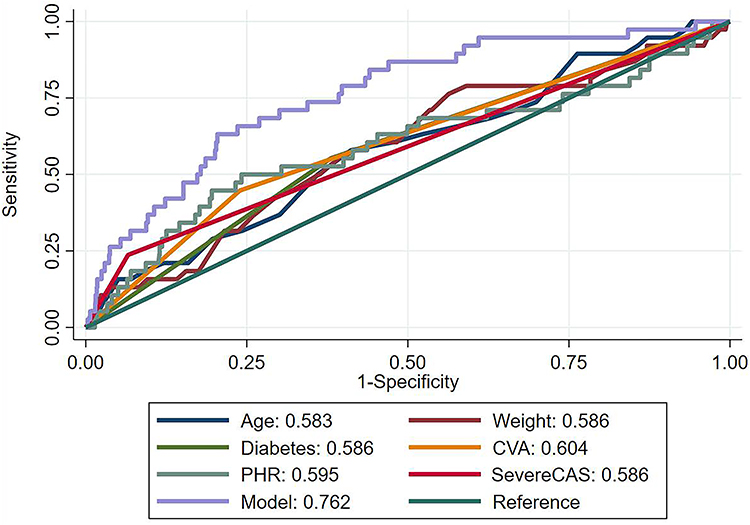 |
Figure 3 ROC curves for the nomogram model incorporating age, weight, diabetes mellitus, CVA, PHR, and severe CAS. Abbreviations: ROC, receiver operating characteristic; CVA, cerebrovascular accidents; PHR, platelet-to-hemoglobin ratio; CAS, carotid artery stenosis. Notes: Figure 3 displays the ROC curves of the nomogram model comprising age, weight, diabetes mellitus, CVA, PHR, and severe CAS. |
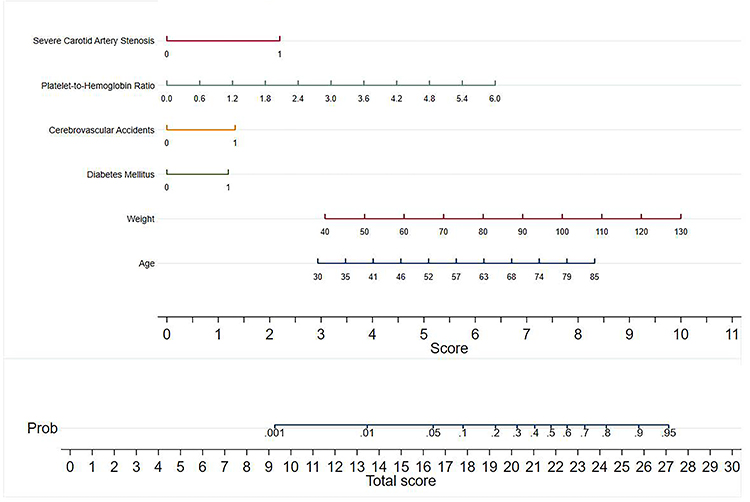 |
Figure 4 Nomogram for predicting 3P-MACE. Abbreviation: 3P-MACE, 3-point major cardiovascular adverse events. Notes: The total score is calculated by summing the scores for each variable, and the corresponding probability of MACE is determined by intersecting a vertical line with the total score. |
Propensity Matching
To assess the association between PHR and 3P-MACE, we utilized propensity score matching to classify patients based on whether their PHR exceeded 1.89. A total of 11 factors were included in the propensity-matched model, including age ≥ 65 years, male gender, height, weight, hypertension, diabetes mellitus, hyperlipidemia, chronic renal failure, smoking history, left main trunk disease and stenting of carotid arteries. The effectiveness of the propensity matching model was evaluated using kernel density plots (Supplementary Figure S3 presents the density before matching, while Supplementary Figure S4 illustrates the density after matching) and propensity matching test plots (Supplementary Figure S5). These analyses indicated a strong match between the two groups post-matching. The clinical and demographic characteristics of the patients after propensity-matched analysis are detailed in Supplementary Table S3. In the univariate logistic regression analysis, there was a statistically significant difference in cardiovascular mortality (P = 0.061). After matching, 3P-MACE occurred in 15 of 264 patients in the PHR ≥ 1.89 group (5.7% [95% CI, 2.87–8.49%]) compared to 4 of 264 patients in the PHR < 1.89 group (1.5% [95% CI, 0.03–3.00%]) (P = 0.01).
Discussion
This retrospective cohort study demonstrates that a higher PHR, particularly PHR≥1.890, was independently correlated with an increased hazard of 3P-MACE (a composite of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke) in patients with CAD following CABG. Additionally, PHR was found to modestly improve risk stratification when added to conventional factors, though absolute AUC gains were limited in CAD patients. These findings suggest that PHR could serve as a practical and straightforward indicator for identifying high-risk CAD patients (those with a PHR≥1.890) following CABG. To the best of our knowledge, this is the first study to demonstrate a significant association between preoperative PHR and 3P-MACE after CABG.
CABG has traditionally been considered the gold standard treatment for CAD patients.19 Studies have indicated that CABG results in lower rates of non-procedural myocardial infarction and less need for revascularization compared to Percutaneous Coronary Intervention (PCI).24 However, CABG is associated with increased risks of reoperations, blood transfusions, longer hospital stays, and a higher hazard of stroke compared to PCI.25,26 Furthermore, CABG remains associated with 3P-MACE, including cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke, which have substantial implications both commercially and medically for patients and healthcare systems.27,28 Therefore, there may be a need for straightforward metrics that physicians can use to evaluate outcomes in CAD patients following CABG.
Among hematologic indices, the neutrophil-to-lymphocyte ratio (NLR)29 and platelet-to-lymphocyte ratio (PLR)30 have been identified as valuable markers for predicting poor prognosis in patients with CAD. However, the prognostic utility of PHR has not been previously validated in CABG patients.
The PHR is a singular index derived from the precise levels of platelets and hemoglobin in peripheral blood. It has garnered attention for its prognostic value in various cardiovascular diseases and malignant cancers.16,19 Mechanistically, PHR may reflect a combined effect of thrombocytosis (enhanced platelet aggregation and inflammation) and anemia (tissue hypoxia and oxidative stress), both of which can exacerbate ischemic injury and endothelial dysfunction post-CABG.21,22 Previous observations have indicated that elevated PHRs were more predictive of adverse events than platelet and hemoglobin levels alone in patients undergoing Percutaneous Coronary Intervention (PCI).18 Our findings align with previous studies linking hemoglobin and platelet parameters to postoperative complications.21,31,32 Importantly, PHR integrates these two readily available measures into a single, interpretable marker of hemostatic and oxygen-transport imbalance. Furthermore, perioperative bleeding and transfusion—both major modifiers of platelet and hemoglobin levels—may partially explain the association between PHR and MACE, suggesting a potential mechanistic pathway.22,32
Given the pivotal role of platelets in CAD pathogenesis, antiplatelet agents are crucial for both immediate and long-term prevention of recurrent myocardial infarction (MI), stroke, cardiovascular death, and MACE.33,34 Persistent inflammation is a characteristic feature of CAD. In a state of heightened inflammation, various mediators are released, leading to megakaryocyte proliferation and increased platelet counts in circulation.35 This phenomenon suggests that platelet activation may be heightened in CAD patients, contributing to a prothrombotic state and potential thrombosis-related complications.36 Activated platelets have a significant association with the initiation and progression of atherosclerosis, as well as with atherosclerotic plaque instability and thrombus formation during vascular endothelial degeneration and plaque rupture.37
Hemoglobin levels have been linked to the severity of atherosclerosis.38 Decreased hemoglobin levels indicate a reduced capacity to transport oxygen, potentially worsening myocardial ischemic injury. This subsequent tissue hypoxia can trigger the sympathetic nervous system and renin-angiotensin-aldosterone systems, leading to an increase in cardiac output. These physiological changes may contribute to adverse left ventricle remodeling, fostering a detrimental cycle of heart failure progression and myocardial infarction.
All patients diagnosed with CAD undergo a comprehensive blood count upon admission, with subsequent tests during their hospitalization. Moreover, the platelet-to-hemoglobin ratio (PHR), a straightforward and easily calculable biomarker, has proven to be a consistent predictor of CAD outcomes without imposing any additional costs on patients or healthcare systems. Therefore, the hemoglobin-to-platelet ratio could emerge as a novel prognostic indicator for outcomes following CABG.
Our findings also resonate with recent research highlighting the broader prognostic significance of laboratory inflammatory markers in vascular disease. For example, C-reactive protein (CRP) and white blood cell (WBC) counts have been shown to influence outcomes after vascular interventions, underscoring the systemic inflammatory contribution to postoperative events.39 Taken together, these observations reinforce the concept that both inflammatory and hematologic markers can serve as integrative indicators of vascular and endothelial stress, complementing traditional clinical predictors.
A predictive nomogram was developed to anticipate 3P-MACE following CABG, incorporating variables such as age, weight, diabetes mellitus, history of CVA, PHR, and severe carotid artery stenosis. The nomogram was rigorously evaluated and proven effective in forecasting patient outcomes. Its simplicity and intuitive design facilitate easy interpretation by clinical staff.40 In a comprehensive multivariate logistic regression analysis, it was identified that age, weight, diabetes mellitus, CVA, PHR, and severe carotid artery stenosis were independently associated with the occurrence of 3P-MACE. The nomogram model exhibited satisfactory accuracy with an area under the curve (AUC) of 0.762 when these six variables were integrated. Previous studies have highlighted the escalating prevalence of cardiovascular disease with advancing age.41 In Nazir Savji’s study, age over 65 years was established as an independent predictor of major adverse cardiovascular or cerebrovascular events in diabetic patients with CAD.42 Susanna C Larsson’s research has linked higher BMI with an increased risk of various cardiovascular conditions, including aortic valve stenosis and coronary artery disease.43 Previous studies have shown that atherosclerotic cardiovascular disease was associated with insulin resistance, hyperinsulinemia, and elevated blood glucose levels.44 Furthermore, patients with a history of cerebrovascular accidents and coronary artery disease often exhibit a severe atherosclerotic profile. Yu et al found that CAS had a clear predictive value for the occurrence and severity of coronary artery disease.45 The correlation could be interpreted that atherosclerosis impacts both carotid and coronary systems.46 Our study corroborated the significant correlations of age, weight, diabetes mellitus, CVA, PHR, and severe carotid artery stenosis with 3P-MACE incidence following CABG, aligning with existing literature. By amalgamating these six predictive factors into a nomogram model, we aimed to enhance prediction accuracy and address the limitations of individual predictors. Results confirmed that the nomogram outperformed single predictors in 3P-MACE prediction (AUC=0.762). Furthermore, Decision curve analysis (DCA) has been widely utilized in various studies to evaluate the efficacy of specific clinical strategies. In our investigation, DCA was employed to assess the clinical utility of the nomogram, revealing its superior predictive value for 3P-MACE incidence compared to alternative indicators.
Complex CAD accompanied by MACE was linked to substantial morbidity and an unfavorable prognosis. Introducing strategies such as leveraging the nomogram for secondary prevention and optimizing the management of baseline parameters could prove advantageous in enhancing the outlook for this patient cohort. Specifically, for individuals with elevated PHR, notably those with PHR≥1.890, it would be imperative and advantageous to regulate the inflammatory response progression, administer anticoagulants or antiplatelet medications, and consider incorporating erythropoietin analogs or iron supplements to ameliorate anemia and prognosis.
The research is limited in several ways. Firstly, it was designed retrospectively and lacked randomization. Furthermore, the data analyzed were sourced from a single clinic, with a restricted selection of patients. The sample size was small, with fewer than forty patients experiencing 3P-MACE in this study. Consequently, the findings may not be broadly applicable to other Asian communities. Larger, multicenter prospective investigations are needed to validate these findings and to explore the potential of PHR as a modifiable prognostic biomarker. Secondly, the exclusion of patients who underwent emergency surgery due to the absence of pertinent laboratory data and ultrasound further restricted the scope of the study. Thirdly, since the PHR was a ratio, this article did not further stratify the study in cases where there were extreme values for platelets or hemoglobin. Fourthly, this study did not adjust for several important perioperative confounders—such as blood transfusion, cardiopulmonary bypass (CPB) duration, or postoperative anemia—which could potentially influence both platelet and hemoglobin levels and thereby affect the PHR and its association with outcomes. Future prospective studies should incorporate these variables to strengthen the causal interpretation of PHR as an independent prognostic factor.
Conclusion
Elevated PHR ≥1.890 was associated with an increased risk of postoperative 3P-MACE following CABG, demonstrating independent predictive value for 3P-MACE. Although PHR alone demonstrated modest discrimination, its incorporation into a multivariable nomogram improved predictive performance. These findings should be interpreted as preliminary and hypothesis-generating. External validation in prospective, multicenter cohorts is needed before clinical implementation.
Abbreviations
CABG, Coronary artery bypass grafting; DCA, Decision curve analysis; 3P-MACE, 3-point major adverse cardiovascular events; PHR, Platelet-to-hemoglobin ratio; CAS, carotid artery stenosis; CVA, cerebrovascular accidents.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Dr. [QL], upon reasonable request.
Ethics Approval and Informed Consent
The investigation was approved by the Shandong Provincial Hospital Biomedical Research Ethics Committee (SWYX: No 2022-498; 4 November 2022); patient consent was waived for analysis and publication of patient data in anonymized fashion.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the grants from the National Science Foundation of China (82170503 by QL), and Jiangsu Provincial Key Research and Development Program (BE2021749 by QL).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Kandaswamy E, Zuo L. Recent advances in treatment of coronary artery disease: role of science and technology. Int J Mol Sci. 2018;19(2):424. doi:10.3390/ijms19020424
2. Blaha MJ, Whelton SP, Al Rifai M, et al. Comparing risk scores in the prediction of coronary and cardiovascular deaths: coronary artery calcium consortium. JACC Cardiovasc Imaging. 2021;14(2):411–421. doi:10.1016/j.jcmg.2019.12.010
3. Hara H, Takahashi K, van Klaveren D, et al. Sex differences in all-cause mortality in the decade following complex coronary revascularization. J Am Coll Cardiol. 2020;76(8):889–899. doi:10.1016/j.jacc.2020.06.066
4. van der Aalst CM, Denissen S, Vonder M, et al. Screening for cardiovascular disease risk using traditional risk factor assessment or coronary artery calcium scoring: the ROBINSCA trial. Eur Heart J Cardiovasc Imaging. 2020;21(11):1216–1224. doi:10.1093/ehjci/jeaa168
5. Wong ND, Cordola Hsu AR, Rozanski A, et al. Sex differences in coronary artery calcium and mortality from coronary heart disease, cardiovascular disease, and all causes in adults with diabetes: the coronary calcium consortium. Diabetes Care. 2020;43(10):2597–2606. doi:10.2337/dc20-0166
6. Chen X, Zhang X, Yan Y, Wang G. The better option of revascularization in complex coronary artery disease patients complicate with chronic kidney disease: a review and meta-analysis. Curr Probl Cardiol. 2021;46(9):100886. doi:10.1016/j.cpcardiol.2021.100886
7. Rankin JS, Lerner DJ, Braid-Forbes MJ, McCrea MM, Badhwar V. Surgical ablation of atrial fibrillation concomitant to coronary-artery bypass grafting provides cost-effective mortality reduction. J Thorac Cardiovasc Surg. 2020;160(3):675–686e613. doi:10.1016/j.jtcvs.2019.07.131
8. Szwed K, Pawliszak W, Szwed M, Tomaszewska M, Anisimowicz L, Borkowska A. Reducing delirium and cognitive dysfunction after off-pump coronary bypass: a randomized trial. J Thorac Cardiovasc Surg. 2021;161(4):1275–1282e1274. doi:10.1016/j.jtcvs.2019.09.081
9. Gnanenthiran SR, Ng ACC, Cumming RG, et al. Hemoglobin, frailty, and long-term cardiovascular events in community-dwelling older men aged ≥ 70 years. Can J Cardiol. 2022;38(6):745–753.
10. Mohammed AA, Liu L, Mareai RM, et al. Combination of white blood cell count to mean platelet volume ratio and neutrophil-to-platelet ratio predicts long-term adverse events in patients with MINOCA. Mediators Inflamm. 2022;2022:5642406. doi:10.1155/2022/5642406
11. Laurikka A, Vuolteenaho K, Toikkanen V, et al. Inflammatory glycoprotein YKL-40 is elevated after coronary artery bypass surgery and correlates with leukocyte chemotaxis and myocardial injury, a pilot study. Cells. 2022;11(21):3378. doi:10.3390/cells11213378
12. Urbanowicz T, Michalak M, Olasinska-Wisniewska A, et al. Neutrophil counts, neutrophil-to-lymphocyte ratio, and Systemic Inflammatory Response Index (SIRI) predict mortality after off-pump coronary artery bypass surgery. Cells. 2022;11(7):1124. doi:10.3390/cells11071124
13. Wollborn J, Zhang Z, Gaa J, et al. Angiopoietin-2 is associated with capillary leak and predicts complications after cardiac surgery. Ann Intensive Care. 2023;13(1):70. doi:10.1186/s13613-023-01165-2
14. Cho KI, Ann SH, Singh GB, Her AY, Shin ES. Combined usefulness of the platelet-to-lymphocyte ratio and the neutrophil-to-lymphocyte ratio in predicting the long-term adverse events in patients who have undergone percutaneous coronary intervention with a drug-eluting stent. PLoS One. 2015;10(7):e0133934. doi:10.1371/journal.pone.0133934
15. Lim HA, Kang JK, Kim HW, Song H, Lim JY. The neutrophil-to-lymphocyte ratio as a predictor of postoperative outcomes in patients undergoing coronary artery bypass grafting. J Chest Surg. 2023;56(2):99–107. doi:10.5090/jcs.22.082
16. Guo H, Wang T, Li C, et al. Development and validation of a nomogram for predicting the risk of immediate postoperative deep vein thrombosis after open wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2023;31(11):4724–4734. doi:10.1007/s00167-023-07488-8
17. Huang J, Xu P, Chen Y. A retrospective study from a single center to identify hematological factors that distinguish between patients with colorectal carcinoma and colorectal adenoma. Med Sci Monit. 2022;28:e936745. doi:10.12659/MSM.936745
18. Zheng YY, Wu TT, Chen Y, et al. Platelet-to-hemoglobin ratio as a novel predictor of long-term adverse outcomes in patients after percutaneous coronary intervention: a retrospective cohort study. Eur J Prev Cardiol. 2020;27(19):2216–2219. doi:10.1177/2047487319870346
19. Bao K, Huang H, Huang G, et al. Platelet-to-hemoglobin ratio as a valuable predictor of long-term all-cause mortality in coronary artery disease patients with congestive heart failure. BMC Cardiovasc Disord. 2021;21(1):618. doi:10.1186/s12872-021-02423-6
20. Isik F, Soner S. Platelet-to-hemoglobin ratio is an important predictor of in-hospital mortality in patients with ST-segment elevation myocardial infarction. Cureus. 2022;14(7):e26833. doi:10.7759/cureus.26833
21. Ranucci M, Di Dedda U, Castelvecchio S, et al. Impact of preoperative anemia on outcome in adult cardiac surgery: a propensity-matched analysis. Ann Thorac Surg. 2012;94(4):1134–1141. doi:10.1016/j.athoracsur.2012.04.042
22. Weil IA, Kumar P, Seicean S, Neuhauser D, Seicean A. Platelet count abnormalities and peri-operative outcomes in adults undergoing elective, non-cardiac surgery. PLoS One. 2019;14(2):e0212191. doi:10.1371/journal.pone.0212191
23. Huang L, Balavarca Y, van der Geest L, et al. Development and validation of a prognostic model to predict the prognosis of patients who underwent chemotherapy and resection of pancreatic adenocarcinoma: a large international population-based cohort study. BMC Med. 2019;17(1):66. doi:10.1186/s12916-019-1304-y
24. Holm NR, Makikallio T, Lindsay MM, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020;395(10219):191–199. doi:10.1016/S0140-6736(19)32972-1
25. Head SJ, Milojevic M, Daemen J, et al. Stroke rates following surgical versus percutaneous coronary revascularization. J Am Coll Cardiol. 2018;72(4):386–398. doi:10.1016/j.jacc.2018.04.071
26. Makikallio T, Holm NR, Lindsay M, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): a prospective, randomised, open-label, non-inferiority trial. Lancet. 2016;388(10061):2743–2752. doi:10.1016/S0140-6736(16)32052-9
27. Gaudino M, Andreotti F, Kimura T. Current concepts in coronary artery revascularisation. Lancet. 2023;401(10388):1611–1628. doi:10.1016/S0140-6736(23)00459-2
28. Mohamed MO, Hirji S, Mohamed W, et al. Incidence and predictors of postoperative ischemic stroke after coronary artery bypass grafting. Int J Clin Pract. 2021;75(5):e14067. doi:10.1111/ijcp.14067
29. Bagyura Z, Kiss L, Lux A, et al. Neutrophil-to-lymphocyte ratio is an independent risk factor for coronary artery disease in central obesity. Int J Mol Sci. 2023;24(8):7397. doi:10.3390/ijms24087397
30. Tangjitgamol S, Udayachalerm W, Wanishsawad C, Kaewwanna W, Ativanichayapong N. Association of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio and coronary artery disease among the physicians. J Inflamm Res. 2024;17:59–66. doi:10.2147/JIR.S447750
31. Kulier A, Levin J, Moser R, et al. Impact of preoperative anemia on outcome in patients undergoing coronary artery bypass graft surgery. Circulation. 2007;116(5):471–479. doi:10.1161/CIRCULATIONAHA.106.653501
32. Woldendorp K, Manuel L, Srivastava A, Doane M, Bassin L, Marshman D. Perioperative transfusion and long-term mortality after cardiac surgery: a meta-analysis. Gen Thorac Cardiovasc Surg. 2023;71(6):323–330. doi:10.1007/s11748-023-01923-w
33. Lettino M, Leonardi S, De Maria E, Halvorsen S. Antiplatelet and antithrombotic treatment for secondary prevention in ischaemic heart disease. Eur J Prev Cardiol. 2017;24(3_suppl):61–70. doi:10.1177/2047487317707854
34. Tramarin R, Pistuddi V, Maresca L, et al. Patterns and determinants of functional and absolute iron deficiency in patients undergoing cardiac rehabilitation following heart surgery. Eur J Prev Cardiol. 2017;24(8):799–807. doi:10.1177/2047487317689975
35. Kurtul A, Murat SN, Yarlioglues M, et al. Association of platelet-to-lymphocyte ratio with severity and complexity of coronary artery disease in patients with acute coronary syndromes. Am J Cardiol. 2014;114(7):972–978. doi:10.1016/j.amjcard.2014.07.005
36. Ozcan Cetin EH, Cetin MS, Aras D, et al. Platelet to lymphocyte ratio as a prognostic marker of in-hospital and long-term major adverse cardiovascular events in ST-segment elevation myocardial infarction. Angiology. 2016;67(4):336–345. doi:10.1177/0003319715591751
37. Jennings LK. Mechanisms of platelet activation: need for new strategies to protect against platelet-mediated atherothrombosis. Thromb Haemost. 2009;102(2):248–257. doi:10.1160/TH09-03-0192
38. Dijk JM, Wangge G, Graaf Y, et al. Hemoglobin and atherosclerosis in patients with manifest arterial disease. The SMART-study. Atherosclerosis. 2006;188(2):444–449. doi:10.1016/j.atherosclerosis.2005.11.010
39. Oddi FM, Vacca F, Ciattaglia R, Fresilli M, Fazzini S, Ippoliti A. Polyester stent graft devices and higher risk of post-implantation syndrome after EVAR: single-center analysis of 367 patients. Ann Vasc Surg. 2021;75:455–460. doi:10.1016/j.avsg.2021.03.020
40. Chen L, Cai BB, Zhou CJ, et al. A sample model established by S-index predicting overall survival after curative resection of primary hepatocellular carcinoma. Cancer Manag Res. 2019;11:693–703. doi:10.2147/CMAR.S193593
41. Savji N, Rockman CB, Skolnick AH, et al. Association between advanced age and vascular disease in different arterial territories: a population database of over 3.6 million subjects. J Am Coll Cardiol. 2013;61(16):1736–1743. doi:10.1016/j.jacc.2013.01.054
42. Karagiannidis E, Moysidis DV, Papazoglou AS, et al. Prognostic significance of metabolomic biomarkers in patients with diabetes mellitus and coronary artery disease. Cardiovasc Diabetol. 2022;21(1):70. doi:10.1186/s12933-022-01494-9
43. Larsson SC, Back M, Rees JMB, Mason AM, Burgess S. Body mass index and body composition in relation to 14 cardiovascular conditions in UK Biobank: a Mendelian randomization study. Eur Heart J. 2020;41(2):221–226. doi:10.1093/eurheartj/ehz388
44. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. doi:10.1016/S0140-6736(04)17018-9
45. Yu JB, Wang XL, An ZJ, et al. Predicting coronary artery disease by carotid color Doppler ultrasonography. Eur Rev Med Pharmacol Sci. 2023;27(24):11713–11721. doi:10.26355/eurrev_202312_34768
46. Bytyci I, Shenouda R, Wester P, Henein MY. Carotid atherosclerosis in predicting coronary artery disease: a systematic review and meta-analysis. Arterioscler Thromb Vasc Biol. 2021;41(4):e224–e237. doi:10.1161/ATVBAHA.120.315747
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.