Back to Journals » Journal of Blood Medicine » Volume 14
Platelet Selectin Levels in Patients with Cerebral Venous Sinus Thrombosis: Preliminary Findings
Authors Zenobia E, Lailiyya N, Dian S ![]() , Juli C, Nugraha Hermawan A, Amalia L
, Juli C, Nugraha Hermawan A, Amalia L ![]()
Received 18 February 2023
Accepted for publication 26 May 2023
Published 31 May 2023 Volume 2023:14 Pages 359—365
DOI https://doi.org/10.2147/JBM.S405975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Eswi Zenobia, Nushrotul Lailiyya, Sofiati Dian, Cep Juli, Asep Nugraha Hermawan, Lisda Amalia
Neurology Department, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Lisda Amalia, Neurology Department, Faculty of Medicine, Universitas Padjadjaran, Jl. Eykman 38 Bandung, Bandung, 40161, Indonesia, Email [email protected]
Background: Cerebral Venous Sinus Thrombosis (CVST) is a cerebrovascular disease with an estimated annual incidence of 3– 4 cases per 1 million population with an 8% mortality rate caused by hypercoagulable conditions and hyper aggregation and also Platelet Selectin (P-Selectin) as one of coagulation biomarker for both of them. This study aimed to describe the levels of P-selectin in CVST patients at RSHS Bandung.
Objective: This study aimed to describe the levels of P-selectin in CVST patients at RSHS Bandung.
Methods: This is a descriptive observational study on patients ≥ 18 years old diagnosed with CVST at the Neurology outpatient polyclinic of RSUP Dr. Hasan Sadikin Bandung for March-May 2022. All samples that meet the inclusion criteria will be included as research subjects.
Results: There were 55 research subjects with a median age of 48 (range 22– 69 years), the majority were women (80%), the most complaints were headaches (92.7%), the majority onset was chronic (96.4%) with a length of treatment ≥ 12 months (61.8%). P-selectin levels were found to increase in the group of subjects with subacute onset (mean 5.20 ± 2.977), infectious etiology (mean 5.26 ± 3.561), duration of treatment < 3 Months (mean 3.79 ± 3.065), history of hyper aggregation (mean 3.89± 2.805), hypercoagulation (mean 3.50± 2.719), increased D-dimer (mean 3.93± 2.710), normal fibrinogen (mean 3.38± 2.693), and in the group with multiple affected sinuses (mean 6.08± 2.681).
Conclusion: P-selectin could be a diagnostic marker for hyper aggregation and hypercoagulable state in patients with CVST, but it still needs further research to prove it.
Keywords: Cerebral Venous Sinus Thrombosis, P-selectin, platelet hyperaggregation, hypercoagulation
Introduction
Cerebral Venous Sinus Thrombosis (CVST) is a cerebrovascular disease in the form of thrombus occlusion in the venous and cerebral sinuses.1 The incidence rate per year is estimated at2,3 cases per 1 million population with a mortality rate of 8%.1,2,4 Patients with CVST are more numerous, especially in young adults than the elderly, with a median age of 45.1–4
The cause of 22–25% of thrombosis in CVST is hyper platelet aggregation caused by dysfunction and disruption of the endothelial structure due to inflammation which triggers platelet activation, which begins with platelet adhesion and continues with the process of secreting platelet granules and forming platelet aggregation.4–6 P-selectin levels can asses impaired function of platelet adhesion and secretion.7–9
P-selectin is a transmembrane glycoprotein identified using a monoclonal antibody specific for platelets that activates thrombin.7,10,11 P-selectin is a molecule that plays a role in platelet adhesion.12,13 Activated platelets will undergo granule fusion with the endothelial plasma membrane, causing exposure of P- selectin to the surface of activated platelets. P-selectin causes adhesion and granule secretion, which in turn causes platelet aggregation.12,13 Disruption of platelet function can be predicted by examining P- selectin, which is the result of endothelial and platelet activation and can describe the initial process of thrombosis.7,10,11,13 P-selectin is said to have a higher specificity, namely 87%, when compared with D- dimer and fibrinogen because it specifically describes the hypercoagulable process that causes thrombus formation in veins.14 P-selectin may be used as a diagnostic tool with D-dimer and fibrinogen examination to diagnose CVST so that patients can be handled more quickly and precisely.
Methods
Sample Size
Sampling was carried out using consecutive sampling from all patients who were ≥ 18 years old and diagnosed with Cerebral Venous Sinus Thrombosis by a neurologist in the cerebrovascular subdivision based on radiological findings (Digital Substraction Angiography or Magnetic Resonance Venography) and laboratory findings (D-dimer level and coagulation profile) at the Outpatient Neurology Polyclinic at RSUP Dr. Hasan Sadikin Bandung in March-May 2022. There is a lack of examination materials or an insufficient number of samples, patients with hypertension, dyslipidemia, smoking, pre-eclampsia, sepsis, Alzheimer’s disease, consuming GP IIb-IIIa agonist, clopidogrel, aspirin, heparin, protamine sulfate, aprotinin, heparinase, insulin, cocaine, and nitric oxide as exclusion criteria. Subjects who met the inclusion criteria expressed their willingness to participate in this study by signing informed consent after obtaining an explanation. The ethics committee of Dr. Hasan Sadikin Hospital Bandung received the research ethics approval under the ethical clearance number LB.02.01/X.6.5/119/2022 and complies with the Declaration of Helsinki. Writing informed consent was obtained from the study participants.
Data Collection
Research subjects were selected at the Neurology Outpatient Polyclinic of RSUP Dr. Hasan Sadikin Bandung obtained from patients who are routinely re-controlled at the polyclinic (a chronic case). Research materials were examined at the Clinical Pathology Laboratory of RSUP Dr. Hasan Sadikin Bandung.
P-Selectin Measurement
Blood samples were taken in the morning after the patient had fasted for at least 8 hours. The serum was separated by allowing blood to clot for 30 minutes and then centrifuging 3500 RPM for 20 min. It was stored at −20°C if not directly processed. The Enzyme-linked immune-sorbent assay was done according to the manufacturer’s protocol.
Statistical Analysis
This descriptive analysis is used to determine the characteristics of the research subjects who are the research samples. Data analysis to describe the proportion of each variable that will be presented descriptively can be broken down into a descriptive study. Data on a numerical scale, such as the patient’s age, are presented with the mean, standard deviation, median, and range. Then for sample characteristic data in the form of categorical data, such as the sex of the patient, coding is given and presented as a frequency and percentage distribution. The data obtained are recorded in a special form and then processed through the SPSS program version 24.0 for Windows.
Results
A total of 55 research subjects met the inclusion criteria and signed informed consent during the study (Supplementary Material). The mean age was 45.04±12.100 years, and most research subjects were women. The participant’s demographic distribution is described in Table 1.
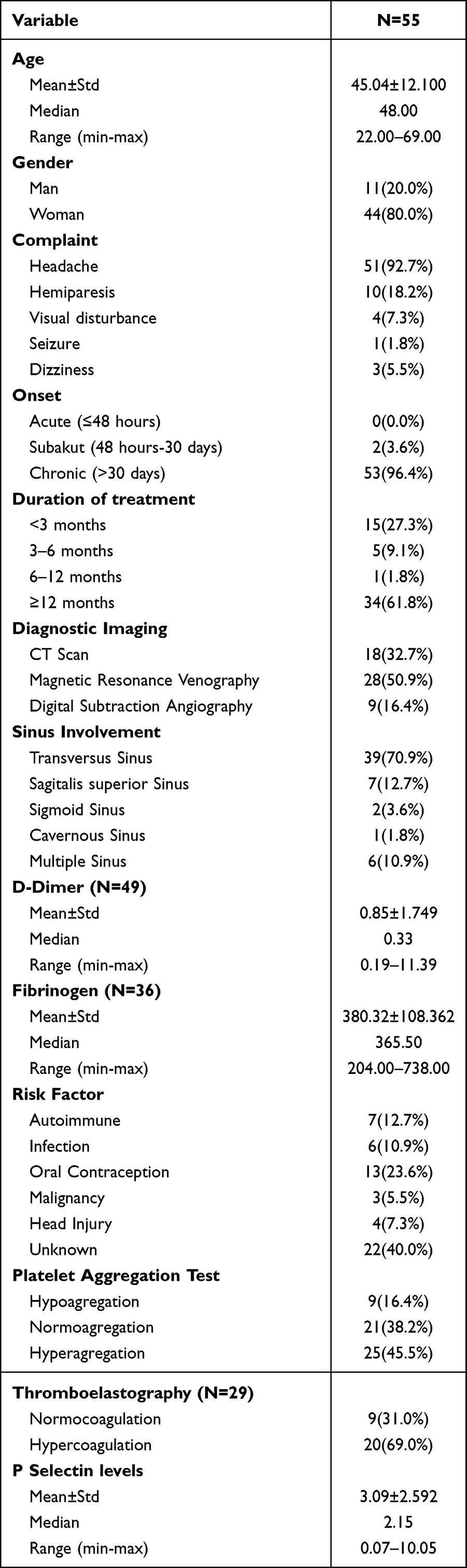 |
Table 1 Demographic Characteristics of Participants |
P-Selectin was highest in the subacute onset group (2 days–30 days) with an average of 5.20 ± 2.977. The highest group for the infectious risk factor, with an average of 5.26 ± 3.561. Study subjects with treatment duration <3 Months had the highest average P-selectin value of 3.79 ± 3.065. P-Selectin with high D-dimer had an average of 3.93 ± 2.710, and normal fibrinogen had the highest standard of 3.38 ± 2.693. Subjects with a history of hyper aggregation had an average P-selectin level of 3.89 ± 2.805.
Whereas research subjects with a history of hypercoagulation had an average of 3.50 ± 2.719. Multiple affected sinuses had the highest average P-selectin of 6.08±2.681 (Table 2).
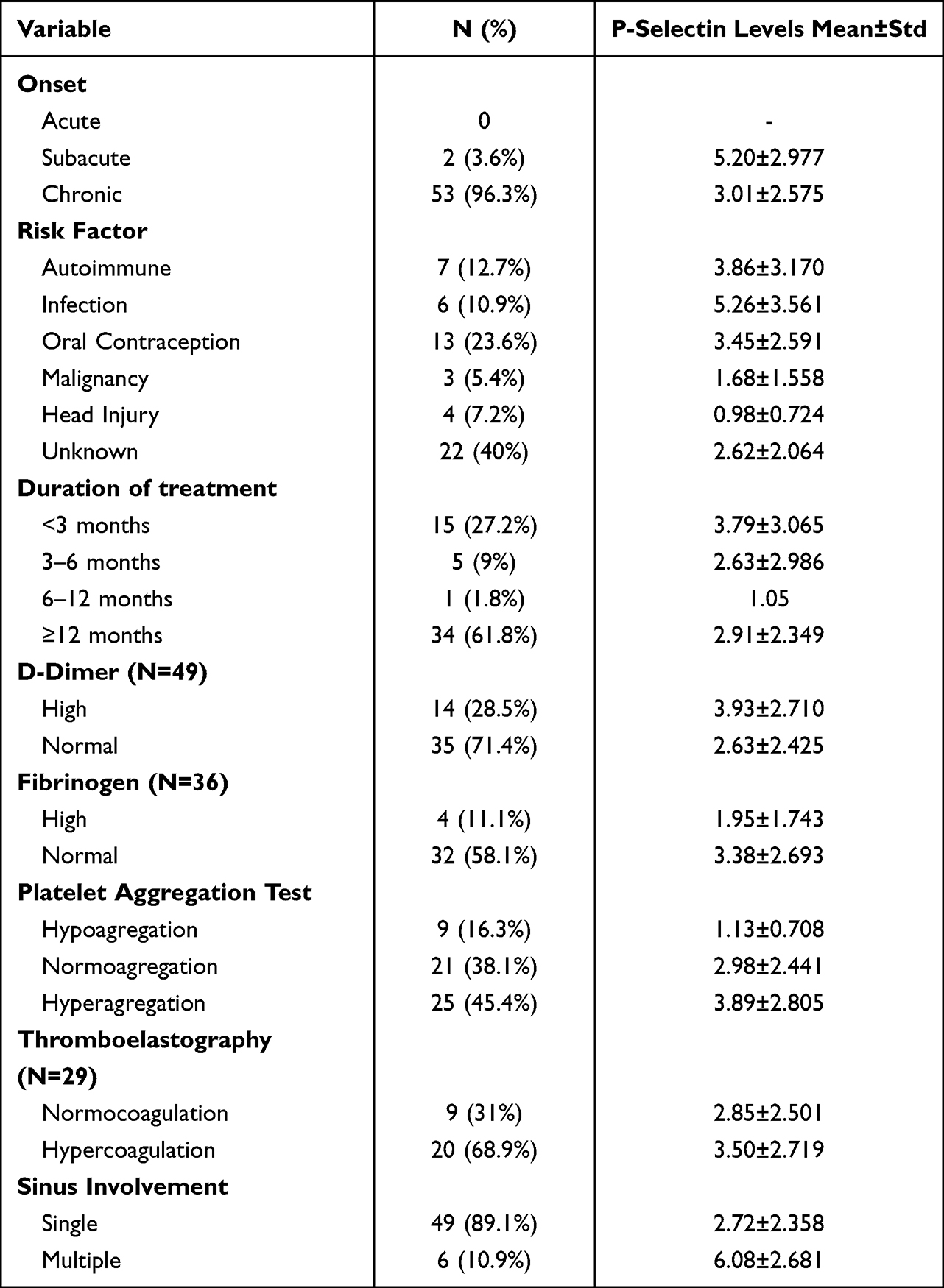 |
Table 2 Platelet Selectin Level Based on Characteristics of Research Subjects |
Discussion
The median age of the study subjects was 48 years, with a range of 22–69 years, predominantly women. High estrogen levels in women of reproductive age who use hormonal contraceptives are known to induce a prothrombotic state through various mechanisms that affect the hemostatic pathway.15 The first mechanism, estrogen, modulates platelet activation and aggregation and increases von Willebrand Factor (vWF) levels which have an important role in hemostasis.15 Venous thrombosis risk increases with oral contraceptives (OCs) use. Combined OCs containing estrogen and progesterone have higher risk. When the patient has a history of previous CVST, the recurrence risk is increased by OC use. In the subgroup analysis, a previous history of CVST was high in the “pregnancy group”. Very little is known about the relapse rate during pregnancy and puerperium in women with a history of CVST. The results of some study suggest that physicians must keep in mind the possible recurrence of CVST in pregnancy.16 In reproductive age, women, accompanied by other risk factors, especially genetic ones, will increase the likelihood of CVST.15,16
The most frequent complaint was headache (92.7%). It is hypothesized that several mechanisms underlie the occurrence of headaches in CVST, namely intracranial hypertension, distention of veins and sinuses, and venous infarction.17–19 Clinical manifestations that appear in CVST patients can be according to the location of the affected sinus.20 The most location of the affected sinuses in this study is in the transverse sinuses, as much as 70.9%, which will give symptoms of increased intracranial pressure, headache, hemianopia, contralateral hemiparesis, and aphasia if there is a cortical disturbance.20
This study showed high P-selectin (>3.5 ng/mL) in 18 subjects. The majority of issues had normal P- selectin levels (0.95–3.5 ng/mL) in 25 subjects, and 12 subjects had low results (<0.95 ng/mL). In this study, 18 research subjects had increased P-selectin levels, seven subjects had unknown risk factors, five issues had risk factors for oral contraceptive use, and three had an infection and autoimmune risk factors. Of the 55 research subjects, there were 22 subjects with unknown risk factors due to the limitations of laboratory tests, such as examination of levels of Protein S, Protein C, and antiphospholipid, which are genetic risk factors related to hypercoagulation in CVST. The most risk factor was research subjects who consumed oral contraceptives, but the highest levels of P-selectin were found in the group with the infectious risk factor. The oral contraceptive user group has a 3 to 5 times higher risk of thrombotic events than the non-oral contraceptive group.21–23 The chance of thrombosis in oral contraceptive users depends on estrogen dose, progestin type, age, family history, and thrombophilic
conditions.22 The results of meta-analyses showed that gender-specific risk factors were only not effective in children and the elderly female groups and that the use of OCs increased venous thrombosis development in reproductive age females and thrombotic events most often occur in the first 12 months (especially the first three months) of oral contraceptive use, which is associated with exposure to new risk factors, especially the presence of other risk factors.16,21,22
History of D-dimer examination showed 14 study subjects (28.5%) with high D-dimer levels and 35 study subjects (71.5%) with normal D-dimer levels. High P-selectin levels were also found in groups with high D-dimer values. An increase in D-dimer levels and P-selectin indicate activation of coagulation and fibrinolysis, which is also associated with increased thrombotic and recurrent thrombotic events.24 D-dimer and P-selectin levels are grown in the acute phase and decreased significantly after one month of Deep Vein Thrombosis (DVT).24 The combination of P-selectin, D-dimer, and total microparticle examinations had a sensitivity of 78% and a specificity of 81% for diagnosing DVT.25 P-selectin has greater specificity compared to D-dimer and fibrinogen, namely 87% for predicting venous thrombosis events because it can specifically describe the hypercoagulable process that causes thrombus formation in veins.14 P-selectin levels can represent platelet activation in the early stages of thrombosis and as a direct inducer of procoagulant conditions associated with vascular and thrombotic events.7,10,11,13 No study has directly compared the D-dimer and P- selectin levels in CVST patients.
In this study, D-dimer and fibrinogen examinations were not carried out simultaneously with P-selectin tests but were carried out when the study subjects first came to the outpatient neurology polyclinic, when they were still in the acute and subacute phases. There were 14 study subjects with high D-dimer yields and four research subjects with high fibrinogen yields. The P-selectin examination was conducted when most study subjects (96.4%) were already in the chronic phase and had received anticoagulant or antiplatelet therapy. There were 18 study subjects with high P-selectin levels, with two issues in the subacute phase and 16 in the chronic phase. P-selectin levels can still increase in chronic phase CVST patients who have received anticoagulant or antiplatelet drugs. The P-selectin examination may help screen and diagnose more patients with hypercoagulable disorders or hyper platelet aggregation, in this case, CVST, when examined in the acute or subacute phase, so it can help patients to get appropriate and fast therapy. P-selectin may also be a tool for evaluating therapy in patients currently receiving anticoagulant therapy and have reached the treatment target (INR 2–3) but have not experienced clinical improvement because P-selectin appears early in the thrombotic phase so that it will describe hypercoagulable conditions in CVST patients.
Limitations of Study
The following limitation should have been considered further in this study. First, the research subjects were patients diagnosed with CVST. They had received therapy, so this study did not show P-selectin levels in the acute phase, and the onset of P-selectin carried out was not homogenous. Second, many research subjects’ risk factors still need to be discovered due to limited examinations. This study cannot describe all etiologies in CVST, especially genetic etiologies related to coagulation.
Conclusion
P-selectin levels were found to be increased in CVST patients with subacute and chronic onset, with the duration of treatment <3 Months, etiology of hormonal contraceptive use and multiple sinuses being affected. We need further study of P-selectin in acute onset CVST patients who have not received anticoagulant therapy and link it to genetic factors related to coagulation disorders. P-selectin could be a diagnostic marker for hyper aggregation and hypercoagulable state in patients with CVST, but it still needs further research to prove it.
Funding
No funding research.
Disclosure
There is no competing interest.
References
1. Stam J. Thrombosis of the cerebral veins and sinuses; 2005. Available from: www.nejm.org.
2. Ferro JM, Aguiar de Sousa D. Cerebral venous thrombosis: an update. Curr Neurol Neurosci Rep. 2019;19(10):1–9. doi:10.1007/s11910-019-0988-x
3. Bousser MG, Ferro JM. Cerebral venous thrombosis: an update. Lancet Neurol. 2007;6(2):162–170. doi:10.1016/S1474-4422(07)70029-7
4. Ferro JM, Canhão P, Aguiar de Sousa D. Cerebral venous thrombosis. Press Med. 2016;45(12):e429–e450. doi:10.1016/j.lpm.2016.10.007
5. Amalia L. The role of platelet-selectin as a marker of thrombocyte aggregation on cerebral sinus venous thrombosis. J Blood Med. 2022;13:267–274. doi:10.2147/JBM.S356028
6. Jellinger KA. Handbook of cerebral venous thrombosis. Eur J Neurol. 2009;16(2):e38–e38. doi:10.1111/j.1468-1331.2008.02469.x
7. Kozuka K, Kohriyama T, Ikeda J, Nakamura S, Nomura E, Kajikawa H. Endothelial markers and adhesion molecules in acute ischemic stroke-Sequential change and differences in stroke subtype. Atherosclerosis. 2002;161(1):161–168. doi:10.1016/S0021-9150(01)00635-9
8. Wagner DD. New links between inflammation and thrombosis. Arterioscler Thromb Vasc Biol. 2005;25(7):1321–1324. doi:10.1161/01.ATV.0000166521.90532.44
9. Ramacciotti E, Blackburn S, Hawley AE, et al. Evaluation of soluble P-selectin as a marker for diagnosing deep venous thrombosis. Clin Appl Thromb. 2011;17(4):425–431. doi:10.1177/1076029611405032
10. André P. P-selectin in haemostasis. Br J Haematol. 2004;126(3):298–306. doi:10.1111/j.1365-2141.2004.05032.x
11. Antonopoulos CN, Sfyroeras GS, Kakisis JD, Moulakakis KG, Liapis CD. The role of soluble P selectin in the diagnosis of venous thromboembolism. Thromb Res. 2014;133(1):17–24. doi:10.1016/j.thromres.2013.08.014
12. Ferroni P, Martini F, Riondino S, et al. Soluble P-selectin as a marker of in vivo platelet activation. Clin Chim Acta. 2009;399(1–2):88–91. doi:10.1016/j.cca.2008.09.018
13. Vandendries ER, Furie BC, Furie B. Role of P-selectin and PSGL-I in coagulation and thrombosis. Thromb Haemost. 2004;92(3):459–466. doi:10.1160/TH04-05-0306
14. Fei Y, Zong GQ, Chen J, Liu RM. Evaluation of the value of d -dimer, P-selectin, and platelet count for prediction of portal vein thrombosis after devascularization. Clin Appl Thromb. 2016;22(5):471–475. doi:10.1177/1076029615569273
15. Abou-Ismail MY, Sridhar DC, Nayak L. Estrogen and thrombosis: A bench to bedside review. Thromb Res. 2020;192:40–51. doi:10.1016/j.thromres.2020.05.008.
16. Uluduz D, Sahin S, Duman T, et al. Cerebral venous sinus thrombosis in women: subgroup analysis of the VENOST study. Stroke Res Treat. 2020:2020. doi:10.1155/2020/8610903
17. Botta R, Donirpathi S, Yadav R, Kulkarni G, Kumar M, Nagaraja D. Headache patterns in cerebral venous sinus thrombosis. J Neurosci Rural Pract. 2017;8(5):72–77. doi:10.4103/jnrp.jnrp_339_16
18. Agostoni E. Headache in cerebral venous thrombosis. Neurol Sci. 2004;25(3):s206–s210. doi:10.1007/s10072-004-0287-3
19. Cumurciuc R, Crassard I, Sarov M, Valade D, Bousser MG. Headache as the only neurological sign of cerebral venous thrombosis: a series of 17 cases. J Neurol Neurosurg Psychiatry. 2005;76(8):1084–1087. doi:10.1136/jnnp.2004.056275
20. Saposnik G, Barinagarrementeria F, Brown RD, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(4):1158–1192. doi:10.1161/STR.0b013e31820a8364
21. Saadatnia M, Tajmirriahi M. Hormonal contraceptives as a risk factor for cerebral venous and sinus thrombosis. Acta Neurol Scand. 2007;115(5):295–300. doi:10.1111/j.1600-0404.2007.00824.x
22. Trenor CC, Chung RJ, Michelson AD, et al. Hormonal contraception and thrombotic risk: a multidisciplinary approach. Pediatrics. 2011;127(2):347–357. doi:10.1542/peds.2010-2221
23. Sandset PM. Mechanisms of hormonal therapy related thrombosis. Thromb Res. 2013;131(1):S4–S7. doi:10.1016/S0049-3848(13)70009-4
24. Gremmel T, Ay C, Seidinger D, Pabinger I, Panzer S, Koppensteiner R. Soluble p-selectin, D- dimer, and high-sensitivity C-reactive Protein after acute deep vein thrombosis of the lower limb. J Vasc Surg. 2011;54(6):48S–55S. doi:10.1016/j.jvs.2011.05.097
25. Rectenwald JE, Myers DD, Hawley AE, et al. D-dimer, P-selectin, and microparticles: novel markers to predict deep venous thrombosis: a pilot study. Thromb Haemost. 2005;94(6):1312–1317. doi:10.1160/TH05-06-0426
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.