Back to Journals » Journal of Asthma and Allergy » Volume 18
Plasma MRGPRX2 Correlates with Severity of Artemisia-Induced Allergic Rhinitis, Particularly in IgE-Negative Patients: A Cross-Sectional Study
Authors Wang C, Wang N, Gong L, Du H, Luo S, Ji X, Yuan Y, Ding Y, Guan X, Liu R, Zhang T ![]()
Received 20 August 2025
Accepted for publication 4 December 2025
Published 13 December 2025 Volume 2025:18 Pages 1761—1772
DOI https://doi.org/10.2147/JAA.S561910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Chao Wang,1,* Na Wang,2,* Ling Gong,1 Hongfen Du,1 Shiqiong Luo,1 Xiaolan Ji,1 Yujuan Yuan,1 Yuanyuan Ding,1 Xukai Guan,3 Rui Liu,1 Tao Zhang1
1School of Pharmacy, Health Science Center, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2North China University of Science and Technology Affiliated Hospital, Tangshan, People’s Republic of China; 3Allergic Rhinitis Analysis and Testing Center, Central Laboratory, Science and Teach Department, Yulin Hospital, The First Affiliated Hospital of Xi’an Jiaotong University, Yulin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rui Liu, School of Pharmacy, Health Science Center, Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected] Tao Zhang, School of Pharmacy, Health Science Center, Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected]
Purpose: Mas-related G-protein-coupled receptor member X2 (MRGPRX2) is a key receptor in mast cell activation and plays a critical role in mediating pseudo-allergic reactions. However, its role in allergic rhinitis (AR) remains poorly understood. Therefore, we investigated the correlation between plasma MRGPRX2 and symptoms in AR patients.
Patients and Methods: A total of 116 patients with typical AR symptoms and positive skin prick test results and 100 healthy controls were recruited. Plasma MRGPRX2, total and specific IgE, and histamine were measured. AR patients who tested negative for both total IgE and sIgE were defined as IgE-negative. Symptom severity was evaluated using a questionnaire combining the Total Nasal Symptom Score (TNSS) and the Visual Analog Scale (VAS). TNSS assessed nasal (sneezing, rhinorrhea, congestion, itching), each scored from 0 (none) to 3 (severe). The VAS ranged from 0 cm (no symptoms) to 10 cm (most severe).
Results: Plasma MRGPRX2 levels were significantly elevated in patients with AR compared with healthy controls (P< 0.001) and demonstrated good discriminative performance (AUC=0.92, P< 0.001). Moreover, patients with moderate to severe AR had significantly higher plasma MRGPRX2 levels than those with mild AR (P< 0.001). A significant positive correlation was also observed between plasma MRGPRX2 levels and VAS scores (ρ=0.37, P< 0.001). This correlation was stronger in the IgE-negative AR group (ρ=0.61, P< 0.001) compared with the IgE-positive group (ρ=0.25, P=0.027) (Z=2.25, P=0.024). Notably, plasma MRGPRX2 levels were positively correlated with TNSS only in IgE-negative AR patients (ρ=0.38, P=0.016), whereas no significant correlation was observed in the IgE-positive group (ρ=0.17, P=0.238).
Conclusion: Plasma MRGPRX2 levels are elevated in patients with AR and are positively correlated with disease symptoms, particularly in IgE-negative cases. MRGPRX2 may serve as a novel biomarker to improve the classification and management of AR, especially in patients exhibiting allergic symptoms despite clinically insignificant IgE levels.
Keywords: allergic rhinitis, MRGPRX2, pseudo-allergic reaction, IgE
Introduction
Allergic rhinitis (AR) is a common chronic inflammatory disorder of the nasal mucosa mediated by allergen-specific immunoglobulin E (IgE).1–4 However, a subset of patients exhibit classical AR symptoms despite having negative levels of circulating IgE.5,6 The absence of measurable IgE poses a diagnostic challenge, as these IgE-negative cases mimic the clinical manifestations of conventional, IgE-mediated AR.
Both IgE-positive and IgE-negative AR are characterized by nasal congestion, rhinorrhea, and sneezing, making it difficult to distinguish them clinically in the absence of clear allergic sensitization.7 The immunopathogenesis of IgE-mediated AR has been well defined as a type I hypersensitivity reaction. This involves the production of IgE antibodies in response to environmental allergens, leading to the activation of Mast cells (MCs) and the release of pro-inflammatory mediators.3,8,9 However, the underlying mechanisms of IgE-negative AR remain poorly understood. This knowledge gap hampers the identification of reliable diagnostic biomarkers and limits the development of targeted therapeutic strategies.
MCs are central effector cells in allergic inflammation and can be activated through both IgE-dependent and IgE-independent pathways.10–12 In particular, pseudo-allergic reactions can induce MC degranulation without the involvement of IgE, leading to the release of histamine and various inflammatory mediators.13,14 Among the receptors implicated in these reactions, the MAS-related G protein–coupled receptor X2 (MRGPRX2) has emerged as a key mediator of non-IgE-mediated hypersensitivity.15,16 MRGPRX2 is highly expressed on the surface of MCs and can be triggered by a wide range of ligands, including neuropeptides, cationic drugs, and components of Artemisia.17–21 Underscoring its pivotal role in drug-induced and pseudo-allergic inflammation.
Upon activation by cationic ligands, MRGPRX2 engages Gq- and Gi-coupled signaling pathways, leading to phospholipase Cγ (PLCγ) activation and subsequent Ca2+ influx through stromal interaction molecule 1 (STIM1) and calcium release-activated calcium modulator (Orai) channels.12 This triggers MC degranulation and the release of mediators such as histamine, tryptase, and cytokines. Tryptase activates protease-activated receptor 2 (PAR2) on sensory nerve endings,22 promoting the release of neuropeptides, including calcitonin gene-related peptide (CGRP) and SP. These neuropeptides induce arteriolar dilation and plasma extravasation, amplifying local inflammation.23,24 Moreover, SP reinforces MC activation via MRGPRX2, forming a positive neuro-immune feedback loop. Parallel activation of phosphoinositide 3-kinase/protein kinase B (PI3K/Akt) and extracellular signal-regulated kinase (ERK) pathways supports cytokine production and sustains the inflammatory response.25 Collectively, MRGPRX2 functions as a key mediator linking MC activation to sensory nerve signaling, contributing to pseudo-allergic and neurogenic inflammatory symptoms such as pruritus and rhinorrhea.13,18,26 Figure 1 illustrates the proposed mechanism of MRGPRX2-mediated allergic inflammation.
 |
Figure 1 Schematic illustration of the MRGPRX2-mediated mast cell activation pathway. |
Recent studies have identified extracellular vesicles (EVs) derived from MCs in human plasma, which contain MRGPRX2. These vesicles are produced through degranulation and membrane budding of MCs.27 Clinically, elevated circulating MRGPRX2 levels have been observed in patients with chronic spontaneous urticaria and asthma, highlighting its potential as both a diagnostic biomarker and therapeutic target.28–30 Although preliminary findings have suggested an association between plasma MRGPRX2 and AR,31 the available evidence remains limited and inconclusive.
In the present study, we investigated plasma MRGPRX2 levels in patients with AR compared with healthy controls and explored their relationship with symptom severity in both IgE-positive and IgE-negative AR. This work aims to elucidate the role of MRGPRX2 in AR pathogenesis and to assess its potential as a biomarker.
Materials and Methods
Participant Criteria
Samples were collected from Yulin City, located in northern Shaanxi Province, China, where Artemisia ordosica is densely distributed and blooms from July to September each year. This region is characterized by an arid to semi-arid climate and steppe vegetation, providing favorable conditions for Artemisia pollen dispersal. Epidemiological data and local clinical observations have shown that Artemisia pollen is one of the major aeroallergens in northern China and a frequent trigger of AR.
Patients with AR were recruited from the Department of Allergy and Clinical Immunology. Diagnosis was made by allergists based on a comprehensive clinical assessment, including characteristic nasal symptoms and ocular symptoms. All patients met the diagnostic criteria outlined in current guidelines.7,32 Due to limited clinical acceptance of nasal provocation testing and its strong concordance with skin prick testing, the latter was used to confirm Artemisia sensitization.33
A total of 199 patients met the inclusion criteria and were screened. Those with negative Artemisia SPT results or incomplete questionnaires (n = 86) were excluded. Finally, 116 patients were included in the analysis, comprising 76 IgE-positive AR patients and 40 IgE-negative AR patients. The overall study design and participant selection process are illustrated in Figure 2.
 |
Figure 2 Study design and participant selection process. Flowchart illustrating the participant recruitment process for AR patients. |
Only individuals aged 18 years or older were included.
Age- and sex-matched healthy controls were selected from the general population undergoing routine physical examinations. These individuals had no history or clinical evidence of allergic AR, asthma, atopic dermatitis, or any other allergic conditions.
Exclusion criteria for both groups included pregnancy, lactation, immunodeficiency, recent upper respiratory infections, history of nasal or sinus surgery, structural nasal abnormalities, chronic systemic diseases. Patients who had taken medications known to influence allergic symptoms within the two weeks prior to enrollment were excluded, including oral and/or topical antihistamines, intranasal corticosteroids, and oral corticosteroids (alone or combined with intranasal agents).32
All participants were fully informed about the study protocol, and written informed consent was obtained prior to inclusion. This study was approved by the Ethics Committee of The First Affiliated Hospital of Xi’an Jiaotong University (Yulin Hospital) (2023034) and conducted in accordance with the Declaration of Helsinki.
The Skin Prick Test
The Artemisia skin prick test was performed at the First Affiliated Hospital of Xi’an Jiaotong University (Yulin Hospital) and interpreted by the same physician for all participants. Skin Prick Solution for Artemisia Pollen Allergens (33333 DU/mL, 2 mL; Wolwo Pharma, Zhejiang, China) was used for testing. The test was conducted on the volar surface of the forearm, and the size of the resulting wheal was measured 15 minutes after allergen application. The largest diameter of the wheal was recorded for analysis. A wheal diameter greater than 3 mm was considered positive.
Symptom Assessment and Scoring Using a Questionnaire
The questionnaire evaluated symptom severity for the Total nasal symptom score (TNSS) (sneezing, rhinorrhea, congestion, and itching) and eyes (itching and tearing). Each symptom is rated on a scale from 0 (no symptoms) to 3 (most severe symptoms).
Visual Analog Scale (VAS) consists of a 10-cm horizontal line, where 0 cm indicates no symptoms and 10 cm represents the most severe symptoms. Patients can mark any point along the line to reflect their perception of symptom severity. The VAS measures the overall level of discomfort caused by AR symptoms.34,35
A VAS score greater than 5 cm was considered indicative of moderate to severe AR, while a score of 5 cm or less was categorized as mild AR.36,37
Plasma Extraction and Storage
Whole blood from each participant was added to an anticoagulant blood collection vessel and centrifuged at 4000 ×g for 5 min. The supernatants were collected for testing, and the plasma was stored at −80 °C.
Detection of MRGPRX2 in Plasma
Plasma MRGPRX2 levels were quantified using an in-house enzyme linked immunosorbent assay (ELISA) based on two specific antibodies.29,38 The assay was validated for specificity and sensitivity, with a detection limit of 1.85 ng/mL, an intra-assay coefficient of variation of 3.36%, and an inter-assay coefficient of variation of 4.63%. The spike-recovery rate ranged from 85.70% to 112.04%, confirming acceptable accuracy and reproducibility.
For the ELISA procedure, a 96-well microplate was coated with 100 μL of capture antibody (4 μg/mL) and incubated overnight at 4 °C. After washing, 200 μL of blocking buffer was added and incubated at 37 °C for 2 h. Subsequently, 100 μL of plasma sample was added to each well, followed by incubation with horseradish peroxidase-conjugated detection antibody (2 μg/mL) and five washing steps. Then, 100 μL of 3,3’,5,5’-Tetramethylbenzidine substrate was added and incubated at 37 °C for 15 min, after which the reaction was terminated with 50 μL of stop buffer. The optical density was measured at 450 nm using a microplate reader. Recombinant MRGPRX2 (Cusabio, Wuhan, China) was used as the calibration standard.
Detection of IgE in Plasma
Plasma total IgE and sIgE levels were quantified using electrochemiluminescence assays. The specific IgE (sIgE) included common allergens (house dust mite, cockroach, dog dander, mold, Artemisia, peanut, crab, and shrimp).39 All measurements were performed at KingMed Diagnostics (Xi’an, China). The assay kits were provided by Roche Diagnostics GmbH (Mannheim, Germany) and used according to the manufacturer’s instructions. In the general population, the reference range for tIgE is 0.00–100.00 IU/mL, while that for sIgE is 0.00–0.35 IU/mL.40,41 AR patients who test negative for both total IgE and sIgE are considered to be IgE-negative.
Detection of Histamine in Plasma
For sample preparation, 50 μL of plasma was mixed with 100 μL of a 10 ng/mL deuterated histamine internal standard solution, vortexed thoroughly, and filtered through a 0.22 μm membrane filter. The filtrate was transferred to an autosampler vial, and 10 μL of the supernatant was injected into the Liquid Chromatograph Mass Spectrometer system for analysis. Calibration curves were established using histamine standards spiked into blank plasma, and quantification was based on the ratio of histamine to deuterated histamine peak areas.
The liquid chromatography–mass spectrometry system consisted of a LabSolutions workstation equipped with a 75×2.0 mm Ultra Performance Liquid Chromatography column (Shimadzu Corporation, Kyoto, Japan). The mobile phase comprised acetonitrile and water containing 0.5% acetic acid (40:60, v/v), delivered at a flow rate of 0.4 mL/min under isocratic elution. The electrospray ionization source was operated in positive mode with the following parameters: nebulizer gas (N2, ≥99.999%) at 3.0 L/min, drying gas (N2, ≥99.999%) at 15.0 L/min, desolvation line temperature at 250 °C, heat block temperature at 400 °C, interface voltage at 4.5 kV, and detector voltage at 1.72 kV. Argon (≥99.999%) was used as the collision-induced dissociation gas at a pressure of 230 kPa. Quantification was performed in multiple reaction monitoring mode.42
Statistical Analysis
IBM SPSS software version 24 was used to analyze data. One-Sample Kolmogorov–Smirnov test was performed to check the normality assumption for the distribution of continuous variables. Categorical data were expressed as number and percentages, while quantitative data were expressed as median and Interquartile range due to non-normal distribution. The Mann–Whitney U-test was used to compare differences between two independent groups, Spearman’s rank correlation coefficient (ρ) was applied to analyze relationships between variables. Differences in correlation coefficients between groups were further tested using Fisher’s r-to-z transformation, to estimate the uncertainty of correlation differences, non-parametric bootstrap resampling (1000 iterations) was performed to calculate the 95% CI. The Receiver operating characteristic (ROC) curve was constructed to evaluate the discriminative ability of MRGPRX2. All statistical assessments were two-tailed and P<0.05 was considered significant.
Results
Clinical Characteristics of the Subjects
The study comprised 116 AR patients with Artemisia allergy. The median age was 38.00 years (range 31.00–45.00), with 49 patients (42.24%) being male. Among the participants, 24 patients (20.69%) had a family history of atopy, 59 patients (50.86%) had a history of chronic urticaria, 45 patients (38.79%) had allergic asthma, and 38 patients (32.76%) had atopic dermatitis. Regarding the severity of AR, as assessed by the VAS, 73 patients (62.93%) were classified as having moderate to severe AR. In this study, 65 patients (56.03%) showed total IgE positivity. Among these, 76 patients (65.52%) tested positive for Artemisia sIgE, making it the most common allergen detected, followed by peanut sIgE in 39 patients (33.62%). Other common allergens included dog dander sIgE (23 patients, 19.83%), and house dust mite sIgE (15 patients, 12.93%). Fewer patients tested positive for cockroach sIgE (12 patients, 10.34%), mold sIgE (8 patients, 6.89%), shrimp sIgE (4 patients, 3.45%), and crab sIgE (3 patients, 2.59%). Furthermore, 40 patients (34.48%) were negative for both total IgE and common sIgE, indicating no apparent allergic sensitization to the allergens tested (Table 1).
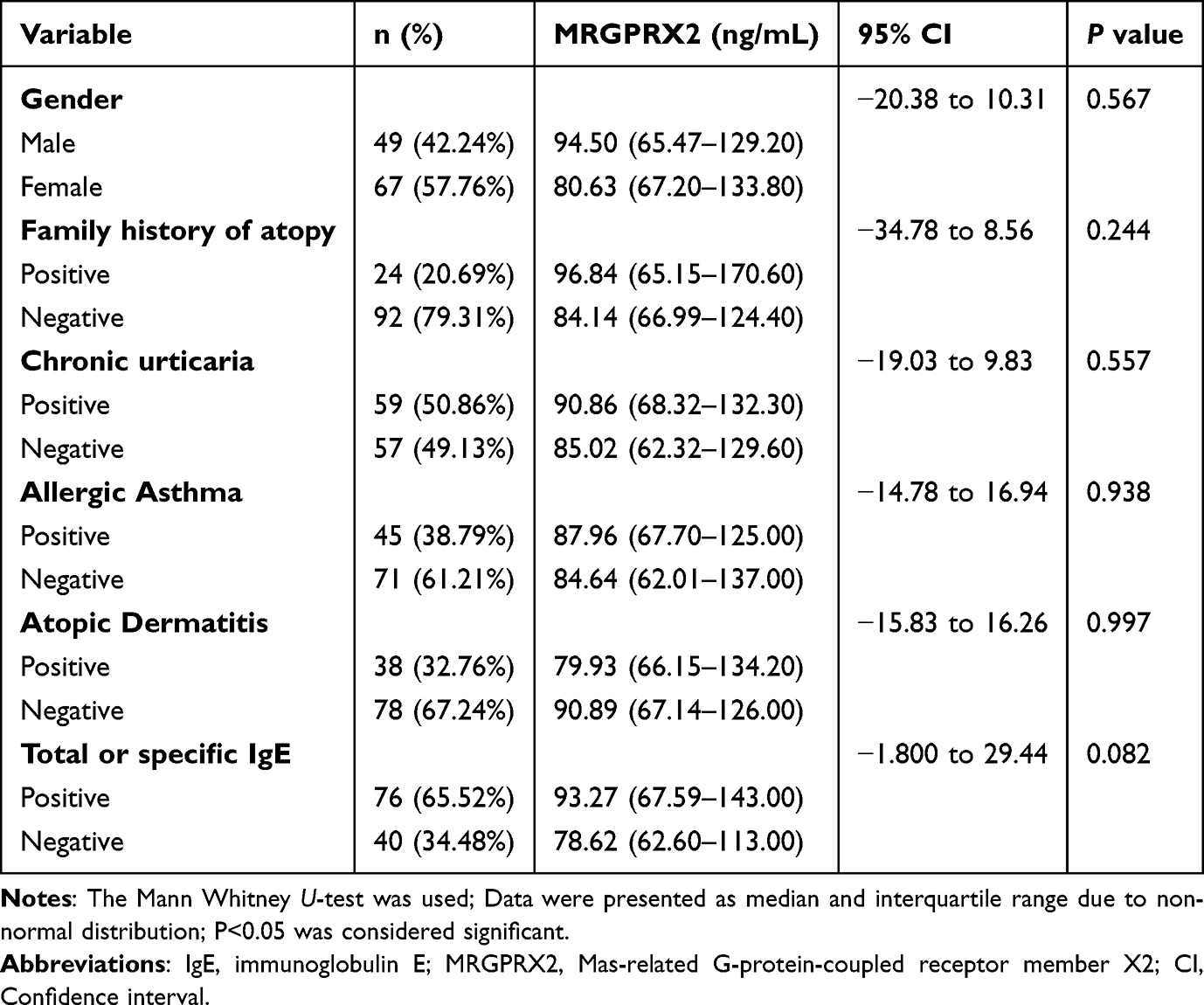 |
Table 1 Demographic Characteristics and Plasma MRGPRX2 in AR Patients |
Stratification Analysis of MRGPRX2 in Patients with AR
No significant difference in plasma MRGPRX2 was observed between male and female patients (P>0.05). Additionally, the presence of concomitant allergic conditions—including chronic urticaria, allergic asthma, and atopic dermatitis—had no significant impact on plasma MRGPRX2 (P>0.05 for all). A family history of atopy was not associated with significant differences in MRGPRX2 (P>0.05). Furthermore, no difference in plasma MRGPRX2 was found between patients with total IgE or common sIgE-positive AR and those with IgE-negative AR (P>0.05; Table 1).
AR patients had significantly higher plasma MRGPRX2 compared with healthy controls (95% CI, 43.00–60.45 ng/mL; P<0.001; Figure 3A). ROC curve analysis demonstrated excellent discriminative ability of plasma MRGPRX2 in distinguishing AR patients from controls (Area under the curve, AUC=0.92, P<0.001; Figure 3B). No significant correlation was observed between age and plasma MRGPRX2 in AR patients (P>0.05; Figure 3C).
 |
Figure 3 Correlation between plasma MRGPRX2 and AR. (A) Plasma MRGPRX2 expression in AR patients (n=116) compared to healthy controls (n=100) (95% CI: 43.00 to 60.45 ng/mL). (B) ROC curve analysis for plasma MRGPRX2 in distinguishing AR patients (n=116) from healthy controls (n=100). (C) Correlation between plasma MRGPRX2 and age in AR patients (n=116) and healthy controls (n=100). (D) Plasma MRGPRX2 expression in moderate-to-severe (n=73) versus mild (n=43) AR patients (95% CI: 17.35 to 45.69 ng/mL). (E) ROC curve analysis for plasma MRGPRX2 in classifying moderate-to-severe (n=73) versus mild AR patients (n=43). (F) Correlation between plasma MRGPRX2 and VAS scores in AR patients (n=116). ***P<0.001. |
The VAS was used to assess overall AR-related discomfort, with scores ≤5 classified as mild and >5 as moderate to severe. Plasma MRGPRX2 was significantly higher in patients with moderate to severe symptoms compared with those with mild symptoms (95% CI, 17.35–45.69 ng/mL; P<0.001; Figure 3D). ROC analysis further indicated that plasma MRGPRX2 could moderately differentiate between these two symptom groups (AUC=0.74, P<0.001; Figure 3E). Moreover, plasma MRGPRX2 levels were positively correlated with VAS in AR patients (ρ=0.37, P<0.001; Figure 3F).
Correlation Between MRGPRX2 and Clinical Characteristics
Significant correlations were observed with total IgE levels (ρ=0.23, P=0.014), TNSS (ρ=0.20, P=0.032), rhinorrhea score (ρ=0.19, P=0.036), nasal congestion score (ρ=0.30, P<0.001), and nasal itching score (ρ=0.19, P=0.032). No significant correlations were found between plasma MRGPRX2 and age, disease duration, histamine levels, sneezing score, ocular itching score, or tearing score (P>0.05 for all) (Table 2).
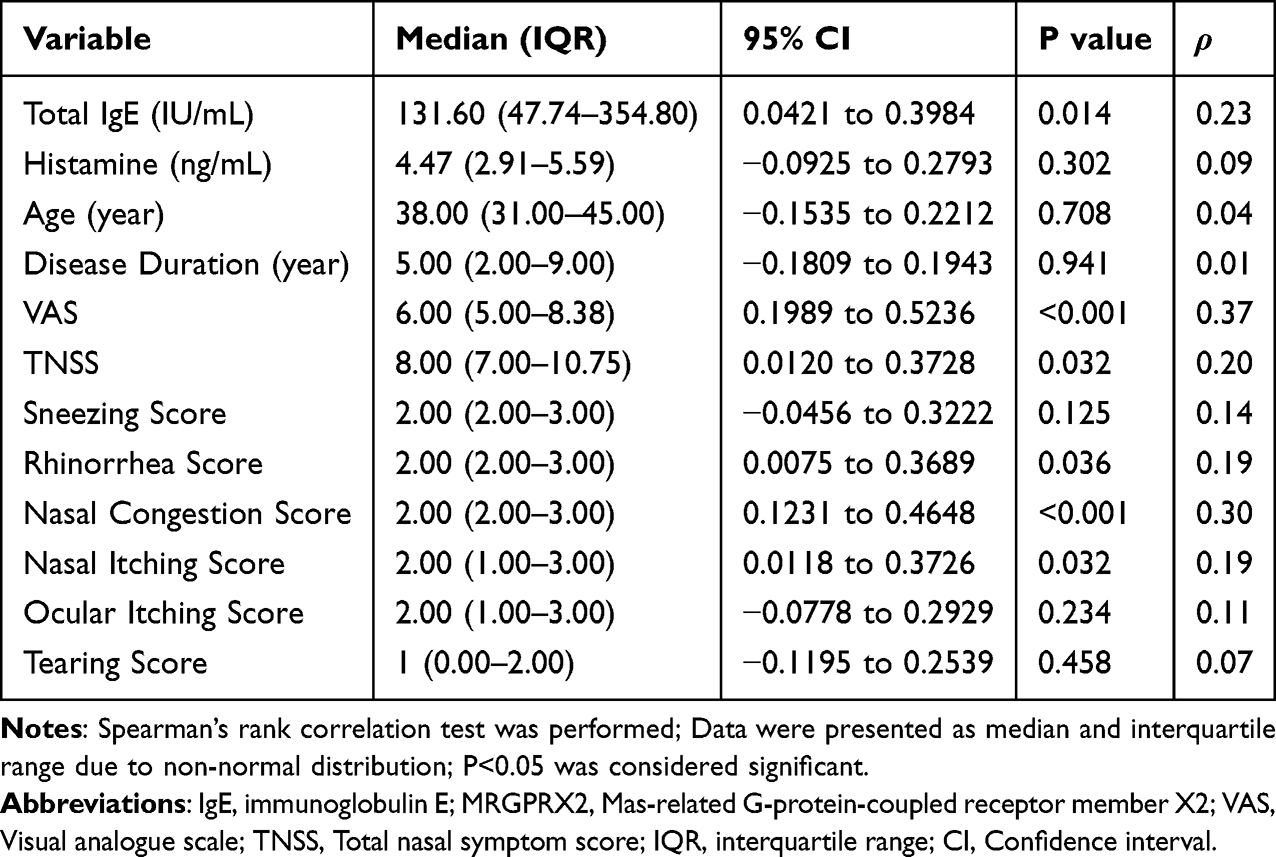 |
Table 2 Correlation of Plasma MRGPRX2 in AR Patients (n=116) |
Plasma MRGPRX2 was positively correlated with total IgE levels. However, no significant correlations were observed between plasma MRGPRX2 and sIgE, including house dust mite, cockroach, dog dander, mold, Artemisia, peanut, crab, and shrimp (P>0.05 for all) (Table 3).
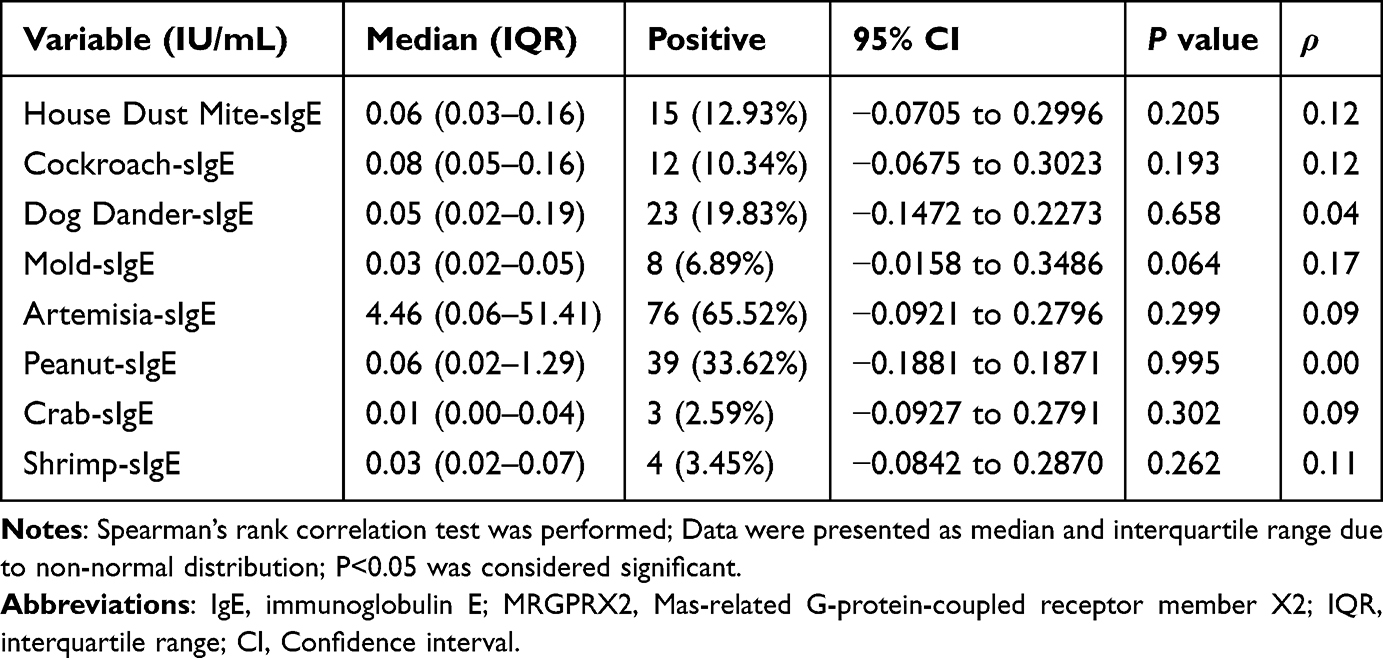 |
Table 3 Correlations Between Plasma MRGPRX2 and sIgE in AR Patients (n=116) |
Comparison of MRGPRX2 Between IgE-Positive and IgE-Negative AR
A total of 40 patients were negative for both total IgE and common sIgE in plasma. Plasma MRGPRX2 demonstrated strong discriminative ability between AR patients and healthy controls in both IgE-negative (AUC=0.89, P<0.001; Figure 4A) and IgE-positive AR (AUC=0.93, P<0.001; Figure 4B) subgroups. Additionally, plasma MRGPRX2 moderately differentiated between mild and moderate-to-severe symptom groups in both IgE-negative (AUC=0.84, P<0.001; Figure 4C) and IgE-positive AR (AUC=0.68, P=0.008; Figure 4D).
 |
Figure 4 Correlation between plasma MRGPRX2 and AR in IgE-negative (n=40) and IgE-positive (n=76) subgroups. (A) ROC curve for plasma MRGPRX2 in distinguishing AR patients from healthy controls (n=100) in the IgE-negative subgroup (n=40). (B) ROC curve for plasma MRGPRX2 in distinguishing AR patients from healthy controls (n=100) in the IgE-positive subgroup (n=76). (C) ROC curve for plasma MRGPRX2 in classifying moderate-to-severe (n=24) versus mild (n=16) AR patients in the IgE-negative subgroup (n=40). (D) ROC curve for plasma MRGPRX2 in classifying moderate-to-severe (n=49) versus mild (n=27) AR patients in the IgE-positive subgroup (n=76). (E) The correlation between plasma MRGPRX2 levels and VAS scores in the IgE-negative AR subgroup (n=40). (F) The correlation between plasma MRGPRX2 levels and VAS scores in the IgE-positive AR subgroup (n=76). |
A significant positive correlation was observed between plasma MRGPRX2 and TNSS in the IgE-negative AR group (ρ=0.38, P=0.016), whereas no such correlation was found in the IgE-positive AR group (P>0.05). Furthermore, plasma MRGPRX2 were positively correlated with VAS scores in both the IgE-negative (ρ=0.61, P<0.001; Figure 4E) and IgE-positive AR groups (ρ=0.25, P=0.027; Figure 4F), with a stronger correlation observed in the IgE-negative group (Z=2.25, P=0.024; Table 4).
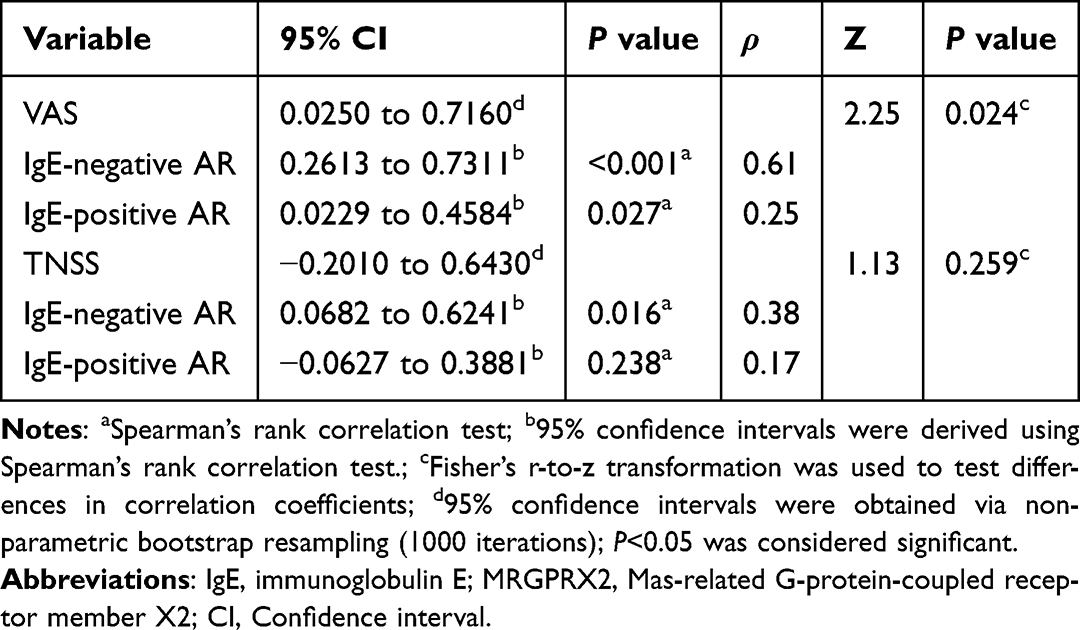 |
Table 4 Correlation of Plasma MRGPRX2 in Patients with IgE-Positive (n=76) and IgE-Negative AR (n=40) |
Discussion
In this study, which focused on patients with AR sensitized to Artemisia, a prevalent aeroallergen in northern China, we demonstrated that plasma MRGPRX2 levels were significantly elevated in patients with AR and strongly correlated with symptom severity, particularly in IgE-negative cases. These findings indicate that plasma MRGPRX2 may serve as a promising diagnostic biomarker, especially when conventional IgE-based tests yield inconclusive results.
Previous studies have shown elevated plasma MRGPRX2 levels in patients with chronic spontaneous urticaria and asthma, where plasma MRGPRX2 has been proposed as a marker reflecting disease severity.28–30 However, its role in AR has not been fully explored.31 Our findings extend these observations to AR, showing that plasma MRGPRX2 levels not only correlate with clinical symptoms but also that IgE-negative AR patients exhibit a stronger association with symptom severity. This suggests that plasma MRGPRX2 may aid in diagnosis of AR, complementing, but not replacing, traditional IgE-based diagnostics.
MRGPRX2 is a critical receptor mediating pseudo-allergic reactions, leading to MC degranulation and the release of various pro-inflammatory mediators.43,44 Plasma MRGPRX2 originates from EVs released by activated MCs.27 The observed correlation between plasma MRGPRX2 levels and both VAS and TNSS scores, specifically in nasal symptoms, supports its role as a biomarker for nasal mucosal inflammation. Notably, the lack of correlation with ocular symptoms further emphasizes its specificity for nasal symptoms, highlighting its clinical relevance as a potential biomarker for AR severity.
We also found a positive correlation between plasma MRGPRX2 and total IgE levels, but not with allergen-sIgE. This observation suggests that MRGPRX2 may act synergistically with IgE-mediated mechanisms rather than being entirely independent. IgE-triggered MC activation could enhance the release of endogenous peptides that, in turn, activate MRGPRX2, creating a potential amplification loop of allergic inflammation.45,46 However, the stronger correlation between plasma MRGPRX2 and symptom severity in IgE-negative AR suggests that pseudo-allergic mechanisms may play a predominant role in this subgroup.
Our results suggest that plasma MRGPRX2 levels reflect ongoing inflammatory activity, correlating with AR symptoms. Additionally, ROC curve analysis demonstrated the diagnostic potential of plasma MRGPRX2 in distinguishing AR patients from healthy controls. Its association with disease severity further supports the utility of plasma MRGPRX2 as a non-invasive biomarker for AR, offering a patient-friendly alternative to nasal provocation and skin prick tests, which are often poorly accepted due to discomfort.
Since all participants were sensitized to Artemisia, one possible explanation is that specific components of Artemisia may activate MCs via MRGPRX2 in the absence of IgE, providing a potential mechanism for IgE-negative AR. Interestingly, plasma MRGPRX2 levels did not correlate significantly with sneezing frequency. This may be due to the complex physiological mechanisms underlying sneezing, which involves multiple factors, including neural reflexes and local inflammatory mediators, rather than being solely regulated by MRGPRX2-related pathways.47 Furthermore, we observed no significant correlation between plasma MRGPRX2 and histamine levels, this may be due to the rapid release and metabolism of histamine. It is quickly degraded by diamine oxidase and histamine-N-methyltransferase.48
This study has several limitations. First, the relatively small sample size may affect the statistical power and generalizability of our findings. Larger, multicenter studies are needed to validate the diagnostic value of plasma MRGPRX2. Second, our study focused exclusively on Artemisia-induced AR, which limits the generalizability of the findings to other allergen-induced AR cases. Third, we assessed only plasma MRGPRX2 levels and did not evaluate its membrane-bound form on MCs or in nasal tissue. Future studies should explore the relationship between plasma and membrane-bound MRGPRX2, as well as the role of MRGPRX2 in mediating pseudo-allergic reactions in AR, including the underlying molecular mechanisms.
Conclusion
Our study reveals that plasma MRGPRX2 is elevated in AR patients and correlates with symptoms. Notably, plasma MRGPRX2 showed stronger correlations with clinical symptoms in the IgE-negative AR subgroup. These findings suggest that plasma MRGPRX2 may serve as a novel biomarker for both the diagnosis and assessment of disease severity to improve the classification and management of AR, especially when patients exhibit allergic symptoms despite clinically insignificant IgE levels. Pseudo-allergic mechanisms may contribute to AR pathogenesis independent of classical IgE pathways.
Abbreviations
AR, Allergic rhinitis; IgE, Immunoglobulin E; MCs, Mast cells; MRGPRX2, Mas-related G-protein-coupled receptor member X2; PLCγ, Phospholipase Cγ; STIM1, Stromal interaction molecule 1; Orai, Calcium release-activated calcium modulator; PAR2, Protease-activated receptor 2; CGRP, Calcitonin gene-related peptide; PI3K, Phosphoinositide 3-kinase; Akt, Protein kinase B; ERK, Extracellular signal-regulated kinase; TNSS, Total nasal symptom score; VAS, Visual Analog Scale; ELISA, enzyme linked immunosorbent assay; sIgE, Specific IgE; AUC, Area under the curve; CI, Confidence interval; ROC, Receiver operating characteristic.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author, Tao Zhang, upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of The First Affiliated Hospital of Xi’an Jiaotong University (Yulin Hospital) (2023034). All procedures involving human participants were performed in accordance with the principles of the Declaration of Helsinki. All the patients or guardians signed an informed consent form to participate in the study. Trial Registration: ChiCTR2400082024.
Funding
This work was supported by the National Natural Science Foundation of China (81872837), Hebei Provincial Government Funded Outstanding Clinical Medicine Talent Program (Jicai Yu Fu [2022] No. 180) and the Yulin City Science and Technology Major Special Project (YF-ZDZX-01-ZKT02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang Y, Lan F, Zhang L. Advances and highlights in allergic rhinitis. Allergy. 2021;76(11):3383–3389. doi:10.1111/all.15044
2. Leth‐Møller KB, Skaaby T, Linneberg A. Allergic rhinitis and allergic sensitisation are still increasing among Danish adults. Allergy. 2019;75(3):660–668. doi:10.1111/all.14046
3. Bousquet J, Anto JM, Bachert C, et al. Allergic rhinitis. Nat Rev Dis Primers. 2020;6(1):95. doi:10.1038/s41572-020-00227-0
4. Huang K, Yang T, Xu J, et al. Prevalence, risk factors, and management of asthma in China: a national cross-sectional study. Lancet. 2019;394(10196):407–418. doi:10.1016/S0140-6736(19)31147-X
5. Oh J, Ahn JC, Choi Y, et al. Factors influencing discrepancy between skin prick test and serum‐specific immunoglobulin E test results. Int Forum Allergy Rhinol. 2025;15(7):755–758. doi:10.1002/alr.23588
6. Liva G, Karatzanis A, Prokopakis E. Review of rhinitis: classification, types, pathophysiology. J Clin Med. 2021;10(14):3183. doi:10.3390/jcm10143183
7. Dykewicz MS, Wallace DV, Amrol DJ, et al. Rhinitis 2020: a practice parameter update. J Allergy Clin Immunol. 2020;146(4):721–767. doi:10.1016/j.jaci.2020.07.007
8. Savouré M, Bousquet J, Jaakkola JJK, Jaakkola MS, Jacquemin B, Nadif R. Worldwide prevalence of rhinitis in adults: a review of definitions and temporal evolution. Clin Transl Allergy. 2022;12(3). doi:10.1002/clt2.12130
9. Han X, Krempski JW, Nadeau K. Advances and novel developments in mechanisms of allergic inflammation. Allergy. 2020;75(12):3100–3111. doi:10.1111/all.14632
10. Shi Y, Tang R, Luo F, et al. The diagnosis and management of allergic reactions caused by Chinese Materia Medica. Clin Rev Allergy Immunol. 2021;62(1):103–122. doi:10.1007/s12016-020-08812-7
11. Worm M, Pazur K, Morakabati P, Redhu D. IgE and non-IgE-mediated pathways in anaphylaxis. Semin Immunopathol. 2025;47(1). doi:10.1007/s00281-025-01056-7
12. Castells M, Madden M, Oskeritzian CA. Mast cells and mas-related G protein-coupled receptor X2: itching for novel pathophysiological insights to clinical relevance. Curr Allergy Asthma Rep. 2024;25(1). doi:10.1007/s11882-024-01183-5
13. Fujisawa D, Kashiwakura J-I, Kita H, et al. Expression of Mas-related gene X2 on mast cells is upregulated in the skin of patients with severe chronic urticaria. J Allergy Clin Immunol. 2014;134(3):622–633.e9. doi:10.1016/j.jaci.2014.05.004
14. Hou Y, Wang C, Lu J, et al. Design and synthesis of first environment-sensitive coumarin fluorescent agonists for MrgX2. Int J Biol Macromol. 2022;203:481–491. doi:10.1016/j.ijbiomac.2022.01.037
15. Kumar M, Choi YG, Wong T, Li PH, Chow BKC. Beyond the classic players: mas‐related G protein‐coupled receptor member X2 role in pruritus and skin diseases. J Eur Acad Dermatol Venereol. 2024;39(3):476–486. doi:10.1111/jdv.20249
16. Aitella E, Romano C, Ginaldi L, Cozzolino D. Mast cells at the crossroads of hypersensitivity reactions and neurogenic inflammation. Int J Mol Sci. 2025;26(3):927. doi:10.3390/ijms26030927
17. Al Hamwi G, Riedel YK, Clemens S, Namasivayam V, Thimm D, Müller CE. MAS-related G protein-coupled receptors X (MRGPRX): orphan GPCRs with potential as targets for future drugs. Pharmacol Ther. 2022;238. doi:10.1016/j.pharmthera.2022.108259
18. Subramanian H, Gupta K, Ali H. Roles of Mas-related G protein–coupled receptor X2 on mast cell–mediated host defense, pseudoallergic drug reactions, and chronic inflammatory diseases. J Allergy Clin Immunol. 2016;138(3):700–710. doi:10.1016/j.jaci.2016.04.051
19. Lansu K, Karpiak J, Liu J, et al. In silico design of novel probes for the atypical opioid receptor MRGPRX2. Nat Chem Biol. 2017;13(5):529–536. doi:10.1038/nchembio.2334
20. Wolf K, Kühn H, Boehm F, et al. A group of cationic amphiphilic drugs activates MRGPRX2 and induces scratching behavior in mice. J Allergy Clin Immunol. 2021;148(2):506–522.e8. doi:10.1016/j.jaci.2020.12.655
21. Mo X, Wang C, Shan Y, et al. Screening and discovery of volatile allergenic components from artemisia ordosica in Yulin region of Northern China. J Hazard Mater. 2025;494:138759. doi:10.1016/j.jhazmat.2025.138759
22. Wang Z, Babina M. MRGPRX2 signals its importance in cutaneous mast cell biology: does MRGPRX2 connect mast cells and atopic dermatitis? Exp Dermatol. 2020;29(11):1104–1111. doi:10.1111/exd.14182
23. Lee MG, Dong X, Liu Q, et al. Agonists of the MAS-related gene (Mrgs) orphan receptors as novel mediators of mast cell-sensory nerve interactions. J Immunol. 2008;180(4):2251–2255. doi:10.4049/jimmunol.180.4.2251
24. Roosterman D, Goerge T, Schneider SW, Bunnett NW, Steinhoff M. Neuronal control of skin function: the skin as a neuroimmunoendocrine organ. Physiol Rev. 2006;86(4):1309–1379. doi:10.1152/physrev.00026.2005
25. Wang Y, Hu S, Dang B, et al. Silibinin attenuated pseudo‐allergic reactions and mast cell degranulation via PLCγ and PI3K/Akt signaling pathway. Phytother Res. 2023;37(8):3572–3582. doi:10.1002/ptr.7835
26. McNeil BD, Pundir P, Meeker S, et al. Identification of a mast-cell-specific receptor crucial for pseudo-allergic drug reactions. Nature. 2015;519(7542):237–241. doi:10.1038/nature14022
27. Kim D-K, Cho Y-E, Komarow HD, et al. Mastocytosis-derived extracellular vesicles exhibit a mast cell signature, transfer KIT to stellate cells, and promote their activation. Proc Natl Acad Sci U S A. 2018;115(45). doi:10.1073/pnas.1809938115
28. An J, Lee JH, Won HK, et al. Clinical significance of serum MRGPRX2 as a new biomarker in allergic asthma. Allergy. 2019;75(4):959–962. doi:10.1111/all.14084
29. Ding Y, Zhang T, Liu R, Che D, Wang N, He L. A novel ELISA method to determine human MrgX2 in chronic urticaria. Clin Transl Allergy. 2020;10(1):61. doi:10.1186/s13601-020-00361-8
30. Cao TBT, Cha H-Y, Yang E-M, Ye Y-M. Elevated MRGPRX2 levels related to disease severity in patients with chronic spontaneous urticaria. Allergy Asthma Immunol Res. 2021;13(3):498–506. doi:10.4168/aair.2021.13.3.498
31. Zhou Y, Xu M, Gong W, et al. Circulating MMP-12 as potential biomarker in evaluating disease severity and efficacy of sublingual immunotherapy in allergic rhinitis. Mediators Inflamm. 2022;2022:1–10. doi:10.1155/2022/3378035
32. Bousquet J, Schünemann HJ, Togias A, et al. Next-generation allergic rhinitis and its impact on asthma (ARIA) guidelines for allergic rhinitis based on grading of recommendations assessment, development and evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol. 2020;145(1):70–80.e3. doi:10.1016/j.jaci.2019.06.049
33. Lee Y, Kim GT, Kang SJ, Park MJ. Do skin prick tests predict nasal provocation test outcomes in allergic rhinitis patients? Int Forum Allergy Rhinol. 2025:e23622. doi:10.1002/alr.23622
34. Zemelka‐Wiacek M, Kosowska A, Winiarska E, Sobanska E, Jutel M. Validated allergen exposure chamber is plausible tool for the assessment of house dust mite‐triggered allergic rhinitis. Allergy. 2022;78(1):168–177. doi:10.1111/all.15485
35. Li AR, Zhang K, Reddy PD, et al. Systematic review of measures of disease severity in rhinitis. Int Forum Allergy Rhinol. 2021;11(9):1367–1377. doi:10.1002/alr.22794
36. Bousquet PJ, Combescure C, Neukirch F, et al. Original article: visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy. 2007;62(4):367–372. doi:10.1111/j.1398-9995.2006.01276.x
37. Zhu XJ, Lu MP, Chen RX, et al. Serum periostin as a potential biomarker in the evaluation of allergic rhinitis: a pilot study. J Asthma Allergy. 2025;18:1–12. doi:10.2147/JAA.S496020
38. Ding Y, Li X, Gao Q, et al. A paper-based ELISA for rapid sensitive determination of anaphylaxis-related MRGPRX2 in human peripheral blood. Anal Biochem. 2021;633:114392. doi:10.1016/j.ab.2021.114392
39. Rondón C, Campo P, Galindo L, et al. Prevalence and clinical relevance of local allergic rhinitis. Allergy. 2012;67(10):1282–1288. doi:10.1111/all.12002
40. Zetterstöm O, Johansson SGO. IgE concentrations measured by PRIST® in serum of healthy adults and in patients with respiratory allergy. Allergy. 2007;36(8):537–547. doi:10.1111/j.1398-9995.1981.tb01871.x
41. Gould HJ, Sutton BJ, Beavil AJ, et al. The biology of IgE and the basis of allergic disease. Annu Rev Immunol. 2003;21(1):579–628. doi:10.1146/annurev.immunol.21.120601.141103
42. Han S, Lv Y, Kong L, et al. Use of the relative release index for histamine in LAD2 cells to evaluate the potential anaphylactoid effects of drugs. Sci Rep. 2017;7(1):13714. doi:10.1038/s41598-017-14224-z
43. Porebski G, Kwiecien K, Pawica M, Kwitniewski M. Mas-related G protein-coupled receptor-X2 (MRGPRX2) in drug hypersensitivity reactions. Front Immunol. 2018;9:3027. doi:10.3389/fimmu.2018.03027
44. He SH, Zhang HY, Zeng XN, Chen D, Yang PC. Mast cells and basophils are essential for allergies: mechanisms of allergic inflammation and a proposed procedure for diagnosis. Acta Pharmacol Sin. 2013;34(10):1270–1283. doi:10.1038/aps.2013.88
45. Bawazir M, Sutradhar S, Roy S, Ali H. MRGPRX2 facilitates IgE-mediated systemic anaphylaxis in a newly established knock-in mouse model. J Allergy Clin Immunol. 2025;155(3):974–987.e1. doi:10.1016/j.jaci.2024.11.021
46. Breiteneder H, Peng YQ, Agache I, et al. Biomarkers for diagnosis and prediction of therapy responses in allergic diseases and asthma. Allergy. 2020;75(12):3039–3068. doi:10.1111/all.14582
47. Li F, Jiang H, Shen X, et al. Sneezing reflex is mediated by a peptidergic pathway from nose to brainstem. Cell. 2021;184(14):3762–3773.e10. doi:10.1016/j.cell.2021.05.017
48. Maintz L, Novak N. Histamine and histamine intolerance. The American Journal of Clinical Nutrition. 2007;85(5):1185–1196. doi:10.1093/ajcn/85.5.1185
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.