Back to Journals » International Medical Case Reports Journal » Volume 16
Placenta Percreta Managed by Ultrasound-Guided Vertical Transfundal Uterine Incision with Hysterectomy: Case Report
Authors Legesse AY ![]() , Teka H
, Teka H ![]() , Kiros S
, Kiros S
Received 29 December 2022
Accepted for publication 24 March 2023
Published 28 March 2023 Volume 2023:16 Pages 221—225
DOI https://doi.org/10.2147/IMCRJ.S403052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ronald Prineas
Awol Yemane Legesse,1 Hale Teka,1 Sara Kiros2
1Department of Obstetrics and Gynecology, Mekelle University, Mekelle, Tigray, Ethiopia; 2Department of Pathology, Mekelle University, Mekelle, Tigray, Ethiopia
Correspondence: Awol Yemane Legesse, Obstetrician and Gynecologist, Department of Obstetrics and Gynecology, Mekelle University, P.O. Box: 1871, Mekelle, Tigray, Ethiopia, Email [email protected]
Abstract: Placenta accreta spectrum is an obstetrics complication in which the placenta has abnormally adhered to the decidua and uterine wall. Placenta percreta is the rarest and sternest variant of accreta syndrome. In this study, we present a case of placenta percreta where we have done ultrasound-guided trans fundal vertical uterine incision to deliver a healthy fetus and subsequent cesarean hysterectomy. Antepartum diagnosis, involvement of a multidisciplinary team, appropriate counseling of women and their families, ultrasound guidance for placental margin demarcation, and vertical transfundal uterine incision can be considered for patients with placenta percreta.
Keywords: placenta percreta, vertical trans fundal incision, hysterectomy
Introduction
Placenta accreta spectrum is an obstetrics complication in which the placenta has abnormally adhered to the decidua and uterine wall.1 Cesarean delivery is associated with an increased risk of placenta accreta spectrum in subsequent pregnancies. This risk rises as the number of prior caesarean sections increases.2–6 According to the degree of placental invasion to the myometrium, there are three variants of the spectrum: accreta, increta, and percreta. Placenta percreta is the rarest and sternest variant of accreta syndrome. The placenta penetrates through the myometrium and is often associated with massive obstetric hemorrhage and urinary tract injury.7,8 Studies suggest that antenatal diagnosis of placenta accreta spectrum is crucial in decreasing the occurrence of complications. Doppler ultrasound and MRI are reported to be effective in the diagnosis of placenta accreta spectrum.8,9 Moreover, the involvement of a multidisciplinary team and a pre-planned procedure leads to an optimal outcome.10 In this study we aimed to present a case of placenta percreta where we have performed ultrasound-guided transfundal vertical uterine incision to deliver a healthy fetus and subsequent cesarean hysterectomy.
Case Presentation
This is a 28-year-old gravida 5, para 4 lady with four previous cesarean sections. The gestational age of the pregnancy from early ultrasound at 7 weeks was 28 weeks at her first presentation to Ayder Comprehensive Specialized Hospital, Mekelle, Tigray, Ethiopia. She visited our hospital for antenatal care. The physical examination was unremarkable. Ultrasound examination revealed a placenta along the anterior uterine wall covering the internal cervical os completely, multiple lacunas, and loss of the bladder serosal interface. Fetal growth was appropriate for gestational age. She was admitted to the maternity ward for inpatient follow-up and dexamethasone. She was followed with an antepartum hemorrhage chart and a biophysical profile.
Ultrasonography revealed multiple lacunae, loss of serosal-bladder interface, and placenta previa. Based on these, we suspected placenta accreta spectra (Figure 1).
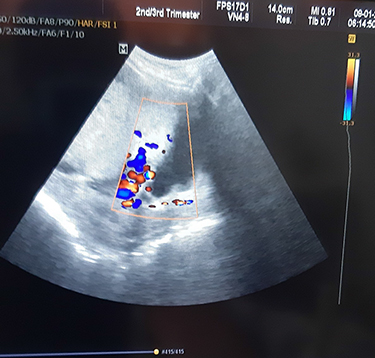 |
Figure 1 Ultrasonography revealed multiple lacunae, loss of serosal-bladder interface, placenta previa. Based on these, we suspected a placenta accreta spectrum. |
Patient and her family members were counseled on the condition and the possibility of blood transfusion and hysterectomy. A multidisciplinary team was involved including an anesthesiologist, pediatrician, and urologist. Four units of cross-matched blood were prepared. Pregnancy termination was planned at a gestational age of 35 weeks. Diagnostic cystoscopy was done on the day of surgery at the operation table and the findings were unremarkable.
The abdomen was entered via a midline infra umbilical incision. The intraoperative findings were a vascular lower segment with visible placental tissue past the anterior uterine wall. Only the serosa of the bladder was involved. An ultrasound was utilized to localize the upper margin of the placenta. Subsequently, a trans-fundal incision above the margin of the placenta was made to effect the delivery of 2600-g alive female neonate with a good APGAR score. Then the cord was tied and the uterine incision was closed, while the placenta undisrupted in situ. An attempt to detach the placenta was not made. The bladder wall was stripped from the uterine wall with a sharp dissection. Subsequently, using the standard technique, a total abdominal hysterectomy was done. The estimated blood loss was 600 mL. No intraoperative accident was reported. The patient left the operation theater table with stable vital signs. Conventional cesarean hysterectomy could have caused massive hemorrhage and bladder injury.
Vertical transfundal incision made without disrupting the placenta (Figure 2).
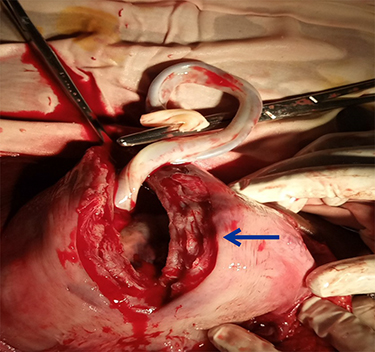 |
Figure 2 Vertical trans fundal incision made without disrupting the placenta. Incision (arrow) following the delivery of the fetus. |
This hysterectomy specimen illustrates a bulging placenta through the lower segment (Figure 3).
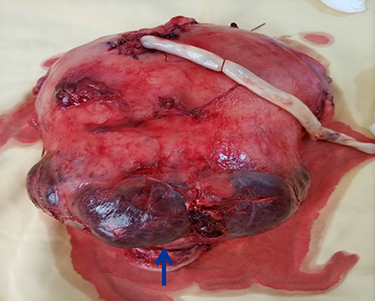 |
Figure 3 Hysterectomy specimen illustrating bulging placenta through the serosa of the lower segment (arrow). |
She was discharged after 4 days of hospital stay with stable maternal and neonatal conditions. Presented 1 week after the surgery for follow-up in a stable condition. Histopathology results revealed placenta percreta.
Histopathology of the uterus shows hemorrhage and fibrin on low-power field. The deep ink on the left side shows the margin serosal surface (Figure 4).
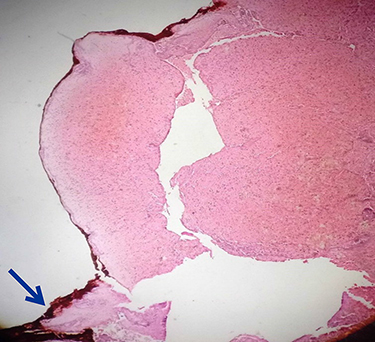 |
Figure 4 Histopathology of the uterus showing hemorrhage and fibrin on low power field. The ink (arrow) shows the margin of the serosal surface. |
High-power field, where the serosal margin has been infiltrated by variable-sized chorionic villi lined by cytotrophoblasts and syncytiotrophoblasts with intervillous fibrin as well as hemorrhage (Figure 5).
 |
Figure 5 High power field, where the serosal margin (Arrow) has been infiltrated by variable size chorionic villi lined by cytotrophoblasts and syncytiotrophoblasts (Asterix) with intervillous fibrin as well as hemorrhage. |
Discussion
The incidence of placenta accreta spectrum has increased from 0.8/1000 deliveries to 3/1000 deliveries during the past three decades. This is primarily because of the rise of cesarean section rates.2–6,11 Among all the placenta accreta spectrums, placenta percreta has an incidence of only 0.008%.11,12
Diagnosis of a placenta accreta spectrum antenatally is challenging. Early diagnosis using imaging, followed by planning of peripartum management by a multidisciplinary team, may successfully reduce morbidity and mortality.8
It is a standard practice to discuss with women and their partners on the management options and complications.8 This was adhered in our case.
Although nowadays, conservative interventions such as compression using uterine sutures, intrauterine packing, uterotonic agents, segmental resection, and selective embolization of vessels are recommended, hysterectomy remains the commonest surgical procedure for placenta accreta spectrum.13 Increased numbers of previous cesarean sections and complete placental invasion were reported to be associated with poor success of conservative management and unfavorable clinical outcome.14,15 Because our case had placenta percreta and was her fifth delivery, conservative techniques were not attempted.8,14–17
Uterine trans-fundal incision for the management of placenta accreta can reduce accidental incision into the placental tissue and then avoid fetal and maternal hemorrhage. Most of the techniques reported in the literature suggest, compared to vertical fundal incision, a transverse uterine fundal incision is associated with a less iatrogenic incision into the placenta.18–20 In our patient, the placenta covered the anterior uterine segment. Intraoperative ultrasound was utilized to localize the upper margin of the placenta. Thus, a vertical trans-fundal incision adequate for the delivery of the fetus was made successfully. We opted for vertical incision over the commonly reported transverse incisions because we were able to avoid disruption of the placenta and extension into the lateral major blood vessels.20 The technique employed in our case gave us adequate time to dissect the bladder of the uterus. If we had used a blind vertical uterine incision without localization, massive hemorrhage due to placental disruption may have been encountered. Thus, leading to bladder injury due to the urge to prioritize hemostasis control.
In summary, we have successfully managed a case of placenta percreta with serosal bladder invasion with tolerable blood loss using ultrasound-guided vertical trans-fundal incision and total hysterectomy. Antepartum diagnosis, involvement of a multidisciplinary team, appropriate counseling of women and their families, ultrasound guidance for placental margin demarcation, vertical transfundal uterine incision to deliver the fetus, and subsequent hysterectomy can be considered as reasonable strategies for patients with placenta percreta.
Care check list is attached as Supplementary Material.
Data Sharing Statement
All data used are included within the manuscript.
Consent for Publication
A written informed consent to publication (case details and accompanying image) was obtained. Institutional review board of College of Health Sciences, Mekelle University waived the ethical clearance for the study.
Acknowledgments
The authors are grateful to the woman presented for her willingness to be published.
Funding
No funding was acquired for this paper.
Disclosure
All authors declare no conflict of interest.
References
1. Clausen C, Lonn L, Langho-Roos J. Management of placenta percreta: a review of published cases. Acta Obstet Gynecol Scand. 2014;93:138–143. doi:10.1111/aogs.12295
2. Marshall NE, Fu R, Guise JM. Impact multiple cesarean deliveries on maternal morbidity: a systematic review. Am J Obstet Gynecol. 2011;205:262.e1–8. doi:10.1016/j.ajog.2011.06.035
3. Eshkoli T, Weintraub AY, Sergienko R, Sheiner E. Placenta accreta: risk factors, perinatal outcomes, and consequences for subsequent births. Am J Obstet Gynecol. 2013;208:219.e1–7. doi:10.1016/j.ajog.2012.12.037
4. Kamara M, Henderson JJ, Doherty DA, Dickinson JE, Pennell CE. The risk of placenta accreta following primary elective caesarean delivery: a case-control study. BJOG. 2013;120:879–886. doi:10.1111/1471-0528.12148
5. Creanga AA, Bateman BT, Butwick AJ, et al. Morbidity associated with cesarean delivery in the United States: is placenta accreta an increasingly important contributor? Am J Obstet Gynecol. 2015;213:384.e1–11. doi:10.1016/j.ajog.2015.05.002
6. Thurn L, Lindqvist PG, Jakobsson M, et al. Abnormally invasive placenta-prevalence, risk factors and antenatal suspicion: results from a large population-based pregnancy cohort study in the Nordic countries. BJOG. 2016;123:1348–1355. doi:10.1111/1471-0528.13547
7. Silver RM. Abnormal placentation: placenta previa, vasa previa and placenta accreta. Obstet Gynecol. 2015;126:654–668. doi:10.1097/AOG.0000000000001005
8. Jauniaux ERM, Alfirevic Z, Bhide AG, et al. Sentilhes L on behalf of the royal college of obstetricians and gynaecologists. Placenta praevia and placenta accreta: diagnosis and management. Green-top guideline No. 27a. BJOG. 2018;126(1):e1–48. doi:10.1111/1471-0528.15306
9. Sun X, Ren R, Xiaoqian Y, Peng F, Gao X. Application of color Doppler ultrasound combined with magnetic resonance imaging in placenta accreta. Scanning. 2022;2022:1–7. doi:10.1155/2022/1050029
10. Warshak CR, Ramos GA, Eskander R, et al. Effect of predelivery diagnosis in 99 consecutive cases of placenta accreta. Obstet Gynecol. 2010;115:65–69. doi:10.1097/AOG.0b013e3181c4f12a
11. Fitzpatrick KE, Sellers S, Spark P, Kurinczuk JJ, Brocklehurst P, Knight M. Incidence and risk factors for placenta accreta/increta/ percreta in the UK: a national case-control study. PLoS One. 2012;7:e52893. doi:10.1371/journal.pone.0052893
12. Abbas F, Talati J, Wasti S, Akram S, Qureshi R, Qureshi R. Placenta percreta with bladder invasion as a cause of life threatening hemorrhage. J Urol. 2000;164:1270–1274. doi:10.1016/S0022-5347(05)67153-4
13. Cırpan T, Akdemir A, Okmen F, Hortu I, Ekici H, Imamoglu M. Effectiveness of segmental resection technique in the treatment of placenta accreta spectrum. J Matern Fetal Neonatal Med. 2021;34(19):3227–3233. doi:10.1080/14767058.2019.1702019
14. Shazly SA, Hortu I, Shih J-C, et al. Prediction of clinical outcomes in women with placenta accreta spectrum using machine learning models: an international multicenter study. J Matern Fetal Neonatal Med. 2022;35(25):6644–6653. doi:10.1080/14767058.2021.1918670
15. Shazly SA, Hortu I, Shih J-C, et al. Prediction of Success of Uterus-Preserving Management in Women with Placenta Accreta Spectrum (CON-PAS Score): a Multicenter International Study. Int J Gynaecol Obstet. 2021;154(2):304–311. doi:10.1002/ijgo.13518
16. Flood KM, Said S, Geary M, Malone FD. Changing trends in peripartum hysterectomy over the last 4 decades. Am J Obstet Gynecol. 2009;200(6):632.e1–632.e6. doi:10.1016/j.ajog.2009.02.001
17. Cho JH, Jun HS, Lee CN. Hemostatic suturing technique for uterine bleeding during cesarean delivery. Obstet Gynecol. 2000;96(1):129–131. doi:10.1016/s0029-7844(00)00852-8
18. Shukunami K, Hattori K, Kotsuji F, Kotsuji F. Transverse fundal uterine incision in a patient with placenta increta. J Matern Fetal Neonatal Med. 2004;16:355–356. doi:10.1080/jmf.16.6.355.356
19. Kotsuji F, Nishijima K, Kurokawa T, et al. Transverse uterine fundal incision for placenta praevia with accreta, involving the entire anterior uterine wall: a case series. BJOG. 2013;120:1144–1149. doi:10.1111/1471-0528.12252
20. Matsuzaki S, Yoshino K, Kumasawa K, et al. Placenta percreta managed by transverse uterine fundal incision with retrograde cesarean hysterectomy: a novel surgical approach. Clin Case Rep. 2014;2(6):260–264. doi:10.1002/ccr3.108
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.