Back to Journals » International Journal of Nanomedicine » Volume 20
Photothermal and Combinatory Therapy as an Emerging Therapeutic Paradigm of Breast Cancer Treatment
Authors Li M, Hasan I, Zhang L, Peng T, Guo B ![]() , Wang Z
, Wang Z
Received 5 July 2025
Accepted for publication 5 November 2025
Published 20 November 2025 Volume 2025:20 Pages 13955—13988
DOI https://doi.org/10.2147/IJN.S551712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yan Shen
Mifang Li,1,* Ikram Hasan,2,* Lingyan Zhang,1 Tingting Peng,3 Bing Guo,4 Zun Wang5
1Lab of Molecular Imaging and Medical Intelligence, Department of Radiology, Longgang Central Hospital of Shenzhen, Shenzhen, 518116, People’s Republic of China; 2School of Biomedical Engineering Medical School, Shenzhen University, Shenzhen, Guangdong, 518060, People’s Republic of China; 3State Key Laboratory of Bioactive Molecules and Druggability Assessment, Guangdong Basic Research Center of Excellence for Natural Bioactive Molecules and Discovery of Innovative Drugs/College of Pharmacy, Jinan University, Guangzhou, 511436, People’s Republic of China; 4School of Science, Shenzhen Key Laboratory of Advanced Functional Carbon Materials Research and Comprehensive Application, Harbin Institute of Technology, Shenzhen, 518055, People’s Republic of China; 5Department of Breast and Thyroid Surgery, Shenzhen Baoan Women’s and Children’s Hospital, Jinan University, Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bing Guo, Email [email protected] Zun Wang, Email [email protected]
Abstract: Breast cancer has a high mortality rate and is one of the most common malignancies among women. Conventional therapies such as radiotherapy, chemotherapy, and surgery are not sufficiently effective and have notable drawbacks, including toxicity and damage to healthy cells, resulting in an unsatisfactory prognosis. Photothermal therapy (PTT) and combinatory therapies have emerged as a promising therapeutic paradigm for breast cancer treatment to achieve precise, minimally invasive tumor ablation with real-time imaging guidance, synergistic therapeutic effects, reduced systemic toxicity, enhanced immune activation, and improved outcomes against recurrence, metastasis, and drug resistance. These approaches utilize near-infrared light to visualize tumor margins and locally generate hyperthermia to destroy cancerous tissue. The development of novel nanomaterials has significantly enhanced the efficacy of breast cancer treatments. This review explores the mechanisms, current advancements, and clinical potential of PTT and combinatory therapy in breast cancer treatment, with an emphasis on developments to a three-level progression: material innovation, targeted delivery, and multimodal synergy. Special focus is given to the rapidly advancing image-guided PTT in combination with other treatment modalities for precise and effective treatment of breast cancer. Furthermore, the review addresses the challenges and future directions in translating these technologies from preclinical models to clinical settings, including the optimization of imaging resolution and thermal efficiency, while minimizing potential side effects. We hope this perspective offers valuable insights into PTT and combinatory therapies for breast cancer and contributes to advancing their clinical translation, ultimately enhancing women’s health.
Keywords: breast cancer, conventional therapies, photothermal therapy, combinatory therapy, image-guided photothermal therapy
Introduction
Breast cancer (BC) is a significant health concern, being one of the most common cancers among women and a leading cause of death. Various factors, including genetics, lifestyle choices, population characteristics, and environmental conditions, can influence its occurrence and outcomes. Essentially, breast cancer arises from the uncontrolled growth of cells in the breast, driven by both genetic and epigenetic factors.1,2 Breast cancer’s genetics are complex, with several genes that can raise the risk of acquiring the disease. Notably, mutations in critical genes like BRCA1 and BRCA2 are especially important. People with a family connection to breast cancer are frequently encouraged to undergo screening for these mutations to detect the disease early and improve outcomes.
Conventional therapies, including surgery, chemotherapy, and radiotherapy, while effective, often have significant limitations, such as systemic toxicity, treatment resistance, and damage to surrounding healthy tissues. In recent years, advancements in nanotechnology and optical imaging have propelled the development of innovative, minimally invasive treatment modalities, with PTT and combinatory therapy emerging as promising approaches. Millions of new breast cancer cases are identified each year, making it one of the most common and complex malignancies worldwide.3–6 Despite significant progress in early detection and traditional treatment modalities such as hormone therapy, radiation therapy, chemotherapy, and surgery, the survival rate for advanced breast cancer remains comparatively low. This has prompted scientists and medical professionals to explore novel, targeted therapeutic strategies aimed at improving treatment outcomes and reducing adverse effects. One promising non-invasive method is PTT, which utilizes the principles of light-mediated heat to selectively destroy cancer cells.7–9
PTT operates by converting absorbed NIR light into heat, achieving hyperthermic conditions (typically 42–45°C) in targeted tissues that induce cancer cell apoptosis. To achieve this effect, photothermal agents such as gold-based nanoparticles, carbon nanotubes, or certain organic dyes efficiently absorb NIR light and convert it into localized heat (Figure 1). When combined with NIR fluorescence imaging (NIRFI), NIRFI-guided PTT enables precise localization of cancer cells and selective thermal ablation, significantly reducing damage to surrounding healthy tissues.10,11 Because PTT uses light-activated nanoparticles to specifically target and destroy tumor cells, it stands out as a viable, non-invasive therapeutic option in the rapidly advancing field of breast cancer treatment. Although PTT offers numerous advantages, such as high precision and minimal harm to nearby healthy tissues, it also presents challenges, including uneven tumor response and limited tissue penetration. To overcome these limitations and enhance therapeutic outcomes, combinatory therapies are gaining traction. These approaches integrate PTT with traditional treatments like radiation and chemotherapy, as well as emerging modalities such as gene therapy and immunotherapy (Scheme 1). Combining PTT with other treatments can produce significant synergistic effects, including improved drug delivery, immune system activation, and enhanced tumor cell destruction. This multifaceted strategy not only addresses the limitations of PTT alone but also tackles broader challenges in BC therapy, such as drug resistance, tumor heterogeneity, and treatment recurrence.12–14
 |
Scheme 1 Here is the schematic diagram illustrating the photothermal and combinatory therapy of breast cancers. |
Additionally, the combination of PTT and nanotechnology creates the possibility of creating multipurpose nanoparticles that may carry heat, therapeutic medications, and even genetic material straight to cancer cells at the same time. This advancement supports the creation of highly personalized treatment plans tailored to individual patients. As the field progresses, future efforts will likely focus on enhancing light penetration, optimizing nanoparticle design, and refining synergistic treatment combinations to maximize both safety and therapeutic efficacy. Ongoing preclinical studies and clinical trials will be essential for determining the optimal parameters for these combination therapies and for thoroughly evaluating their safety profiles in human patients.15,16
However, photothermal agents can be organic, inorganic, or hybrid in nature. Organic photothermal agents, such as conjugated polymers like polydopamine, polypyrrole, polyaniline, and PEDOT, are valued for their biocompatibility and biodegradability. However, they may exhibit lower stability compared to inorganic materials. Compounds such as porphyrins and phthalocyanines show strong NIR absorption along with excellent photothermal conversion efficiency. Indocyanine green (ICG), an FDA-approved dye, also offers NIR absorption but suffers from photobleaching and instability.17,18 Inorganic nanoparticles, including gold nanostructures, copper-based nanoparticles, iron oxide nanoparticles, black phosphorus (BP), MXenes, and materials based on silicon and molybdenum, are known for their strong light absorption, excellent stability, and high photothermal conversion efficiency. Many of these materials are also suitable for dual-modality applications, such as combining PTT with MRI, and they feature tunable plasmon resonance in the NIR range.19–22 On the other hand, hybrid materials, which combine organic and inorganic components, offer improved biocompatibility, stability, and multifunctionality. Examples include metal-organic frameworks (MOFs), graphene-based nanocomposites, polymer-coated nanoparticles, liposome/nanoparticle hybrids, and DNA- and peptide-based hybrid nanostructures.20,23 These hybrid systems offer enhanced optical properties, drug-loading capabilities, targeting efficiency, and controlled drug release.
Currently, several comprehensive reviews have explored the application of PTT in the treatment of BC. Sun, Jingjun et al (2022) published a review focusing on the development of PTT based on nanotechnology for treating breast cancer and its metastases. The review highlights the advantages of PTT, including its low invasiveness and high spatiotemporal selectivity, and emphasizes the enhanced therapeutic outcomes achieved when PTT is combined with chemotherapy and/or photodynamic therapy.3 Xiong, Yao et al (2023) provided a detailed overview of various nanoparticles used in PTT for breast cancer. This review discusses the effectiveness, mechanisms of action, and probable clinical applications of different nanoparticle-based PTT approaches.2 Duan, Shufan et al (2023) also contributed to the field with a review focused on the application of nanoparticles in PTT. It explores their photothermal properties, tumor-killing capabilities, and their development for use in nanomaterial-based PTT for cancer treatment.8
Breast cancer was selected for this review due to its status as the most commonly diagnosed cancer and a leading cause of cancer-related deaths in women. Despite progress in cancer treatment, significant challenges remain, including tumor heterogeneity, drug resistance, systemic toxicity, and high recurrence rates. This underscores the need for alternative therapies. PTT, especially when combined with methods like gas therapy, starvation therapy, chemotherapy, immunotherapy, and chemodynamic therapy, provides unique benefits due to its minimally invasive nature and ability to induce systemic antitumor immunity. The extensive research in nanomedicine related to breast cancer supports the exploration of nanoparticle-based PTT strategies as promising therapeutic options. In this review, we offer a timely update of the burgeoning photothermal and combinatory therapy in breast cancer treatment (Scheme 1). This review examines the underlying mechanisms, current technological developments, and the clinical potential of both PTT and combinatory therapies, with a focus on nanoparticle engineering, targeting strategies, and multimodal treatment approaches. We also address the key challenges and future directions for translating these therapies from preclinical studies to clinical practice, emphasizing the need for optimized imaging, precise thermal control, and enhanced biocompatibility. In particular, we explore the promise of image-guided PTT in combination with other treatment modalities as an accurate and effective approach for managing breast cancer metastasis. Ultimately, PTT and combinatory therapy represent a significant advancement in the development of targeted, minimally invasive cancer treatments, with the potential to progress patient outcomes and diminish treatment-related side effects. A well-structured, up-to-date review like this one can help consolidate current knowledge, identify unresolved challenges, and guide future research efforts toward the clinical translation of PTT in routine breast cancer care.
Patho-Physiology of Breast Cancer (BC)
BC is a complex disease with various pathophysiological mechanisms. Understanding its pathophysiology is crucial for developing targeted therapies and improving preventative strategies. Genetic mutations, hormonal influences, cell cycle alterations, the tumor microenvironment, and metastasis all contribute to its development. Genetic alterations in genes such as BRCA1 and BRCA2 surge the risk of BC, while hormonal factors like estrogen and progesterone can promote tumor growth. Hormone replacement therapy in postmenopausal women has been shown to elevate the risk. Other risk factors include age, gender, family history, and lifestyle features such as alcohol drinking, obesity, and deficiency of physical activity.2,4,9,10
Breast cancers universally arise from the terminal duct lobular units (TDLUs), the functional structures located within the collecting duct system of the breast. Classification of these tumors has evolved through systems grounded in both histological and molecular features, which are essential for guiding therapeutic decisions. The two primary histological forms of breast cancer are ductal carcinoma, currently termed “no special type” (NST), and lobular carcinoma. Their non-invasive forms include ductal carcinoma in situ (DCIS) and lobular carcinoma in situ (LCIS), the latter also known as lobular neoplasia.4,9–11,24 The molecular classification of breast cancer was pioneered by Perou and Sørlie, who identified intrinsic subtypes through analysis of a 50-gene signature (PAM50). In routine clinical practice, these subtypes are often approximated using histopathology and immunohistochemical analysis of key biomarkers, including the proliferation marker Ki67, estrogen receptor (ER), progesterone receptor (PR), and HER2. Tumors expressing ER and/or PR are termed hormone receptor-positive, while those lacking ER, PR, and HER2 are classified as triple-negative. Additional factors influencing classification include tumor grade, proliferation index, and molecular alterations such as ESR1 mutations, which may arise due to aromatase inhibitor therapy. In cases with low tumor cell content, expression of normal breast tissue components may also impact diagnostic interpretation.4
Traditional breast cancer therapies, including surgery, chemotherapy, radiotherapy, endocrine treatment, and HER2-targeted drugs, show limited effectiveness in advanced or metastatic stages (particularly Stage IV and recurrent disease), where curative outcomes are rarely achieved. Their efficacy is further reduced in aggressive subtypes such as TNBC, which lacks hormone and HER2 targets, HER2-positive tumors that acquire resistance to targeted agents, and endocrine-resistant ER-positive cancers that fail to respond to hormonal manipulation over time. Moreover, conventional approaches are least effective against metastases in critical organs: brain metastases are poorly treated due to the restrictive blood-brain barrier, bone metastases are typically managed only palliatively with limited eradication, and liver or lung metastases often present with high tumor burden and poor therapeutic response.2,4,9,13
Strategies for Breast Cancer Treatment
Breast cancer treatment is tailored to each individual, taking into account factors such as the specific type and stage of the cancer, hormone receptor status, the patient’s overall health, and personal treatment preferences. Surgical options typically include lumpectomy, mastectomy, and sentinel lymph node biopsy. Following surgery, radiation therapy is often used to target and destroy any residual cancer cells. In addition, systemic treatments like chemotherapy, hormone therapy, targeted therapy, and immunotherapy are utilized to address cancer throughout the body. Participation in clinical trials may also offer access to emerging therapies and innovative treatment combinations.1,13,25
In addition to these treatments, supportive care shows a vital role in dealing with symptoms and side effects, including palliative care, nutritional support, and psychological counseling. Lifestyle amendments, such as nutritional changes and workouts, can also be combined into a comprehensive treatment strategy. However, PTT and combination therapy strategies are gaining attention as advanced approaches for breast cancer treatment. These strategies combine modalities like photodynamic therapy, radiotherapy, immunotherapy, and chemotherapy (Figure 2). 1 By enhancing treatment efficacy, selectively targeting cancer cells, and diminishing injury to healthy tissues, these approaches provide higher precision and more effective tumor eradication. Furthermore, combining PTT with these therapies leads to reduced side effects and better patient outcomes.
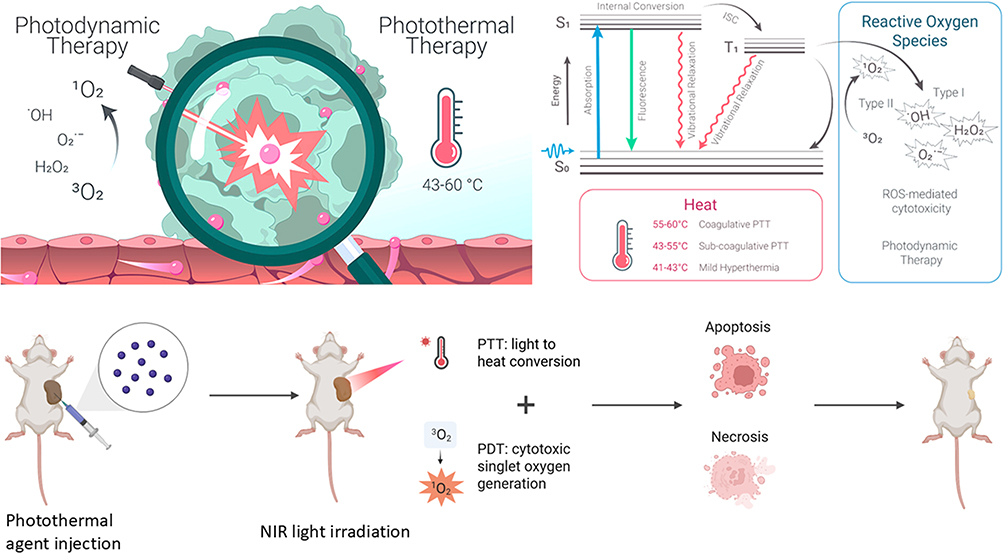 |
Figure 1 An illustration of the various nano-conjugated PTT techniques applied in the present situation. The main therapeutic combinations with PTT include photodynamic therapy, radiotherapy, immunotherapy, and chemotherapy. These integrated approaches work synergistically to enhance tumor destruction and achieve effective ablation.1 [Reproduced from ref.1 Copyright Elsevier 2024. |
Although PTT shows great promise in enhancing the efficacy of combination treatments for breast cancer, the key molecular mechanisms driving this synergy remain insufficiently clarified. In particular, the role of heat shock proteins (HSPs) in modulating stress responses and potential tumor resistance is not fully understood, raising questions about how thermal stress influences long-term therapeutic outcomes. Similarly, while PTT-induced immunogenic cell death has been suggested to promote antitumor immunity, the extent and consistency of this effect across different breast cancer subtypes are not well established. Another underexplored area is vascular normalization, where mild hyperthermia may improve tumor perfusion and drug delivery, yet the optimal parameters and durability of this effect are poorly defined. Without a deeper mechanistic understanding, it is difficult to accurately assess or optimize the therapeutic rationale for integrating PTT with chemotherapy, immunotherapy, radiotherapy, or other modalities. Therefore, future studies must focus on systematically elucidating these molecular pathways to validate the scientific foundation of PTT-based combination therapies and to enable their more effective translation into clinical practice.15,26,27
Mechanism of PTT in Breast Cancer
PTT is a slightly invasive treatment that uses light energy to selectively destroy cancer cells, particularly in breast cancer.28–31 The core mechanism of PTT involves the use of light-absorbing materials, such as nanoparticles, which can absorb light and change it into heat. These agents, including gold nanoparticles (AuNPs), graphene oxide (GO), carbon nanotubes (CNTs), copper sulfide (CuS) nanoparticles, and organic dyes, are selectively deposited in the tumor area. When exposed to an external light source, typically in the NIR area of the electromagnetic spectrum (700–900 nm), these photothermal agents convert photon energy into thermal energy. This results in a localized increase in tumor tissue temperature, often reaching between 42–45°C (Figure 1). This localized heating induces several effects on cancer cells, including protein denaturation, cell membrane disruption, apoptosis, necrosis, tumor ablation, and cell death. Additionally, PTT impacts the tumor microenvironment, potentially enhancing oxygenation and creating opportunities for synergy with other therapies.10–12,32
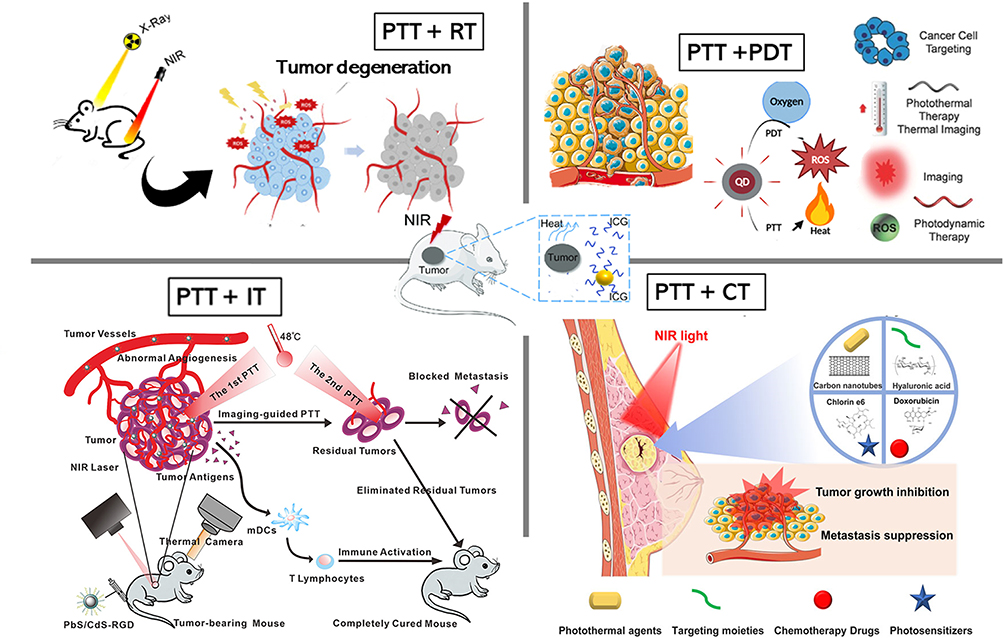 |
Figure 2 This figure shows how PDT and PTT are based on photophysical and photochemical processes. S0 stands for ground state, S1 for excited singlet state, T1 for excited triplet state, and ISC for intersystem crossover.12 Reproduced from ref.12 Copyright ACS nano 2023. |
PTA-Based Nanomaterials
Photothermal agent (PTA)-based nanomaterials have become a central focus in breast cancer therapy due to their ability to generate localized heat under NIR irradiation, offering minimally invasive yet highly effective tumour ablation. Gold nanostructures, including gold nanorods, nanostars, and nanoshells, are among the most studied PTAs for breast cancer because of their strong surface plasmon resonance and tunable NIR absorption.33,34 For example, PEGylated gold nanorods have been applied in 4T1 breast tumour-bearing mice, showing excellent tumour accumulation, efficient heating, and significant tumour regression with minimal side effects. Gold nanostars have also been used for photoacoustic imaging-guided therapy, enabling real-time monitoring of treatment response. These studies demonstrate how metallic PTAs combine therapeutic and diagnostic functions, making them highly valuable for precision oncology.35,36 However, organic NIR dyes such as ICG and IR-780 are also widely employed but often suffer from poor photostability and rapid clearance. To address this, nanocarrier-based delivery systems have been developed. For instance, ICG-loaded liposomes and polymeric micelles have demonstrated enhanced stability and tumour targeting, enabling effective fluorescence imaging and photothermal ablation of breast cancer cells. Similarly, IR-780 incorporated into liposomal or polymeric nanocarriers has shown promising results in triple-negative breast cancer models, where it not only improved PTT efficacy but also served as a dual-function probe for fluorescence and photoacoustic imaging. These examples highlight the role of nanoplatforms in overcoming the limitations of free dyes and enhancing their theranostic potential.37,38
On the other hand, inorganic semiconductor-based nanomaterials, such as copper sulfide (CuS) and bismuth sulfide (Bi2S3), represent another important class of PTAs. CuS nanoparticles, with strong NIR absorption and high photothermal conversion efficiency, have been combined with doxorubicin for synergistic PTT and chemotherapy, achieving marked tumour growth suppression in triple-negative breast cancer models. Bi2S3 nanoparticles, due to their high X-ray attenuation coefficient, have been employed for combined PTT and radiotherapy, offering an effective strategy to overcome the limitations of monotherapy. In addition, carbon-based nanomaterials like graphene oxide and carbon nanotubes have been tested for breast cancer treatment, showing strong NIR absorption and efficient heat generation, though their long-term biodegradability remains a challenge for clinical translation. More recently, multifunctional and biodegradable PTA nanoplatforms have been developed to enhance therapeutic outcomes.39,40 However, black phosphorus (BP) nanosheets, known for their high photothermal efficiency and biodegradability, have been used in 4T1 tumour-bearing mice for PTT combined with immunotherapy, stimulating systemic immune responses against metastasis. Polydopamine nanoparticles, which are biocompatible and easy to functionalize, have been applied as carriers for chemotherapeutic drugs, enabling combined photothermal chemotherapy. On the other hand, MOF-based nanoplatforms have also gained attention; for instance, IR-780-loaded MOFs co-delivering paclitaxel achieved tumour-targeted drug release triggered by NIR irradiation, leading to enhanced tumour regression while reducing systemic toxicity. These diverse examples underline the versatility and adaptability of PTA-based nanomaterials in breast cancer therapy, while also pointing to the need for further optimization in biosafety, biodegradability, and clinical scalability.35,41,42
However, PTAs are essential in PTT for tumor ablation, converting absorbed light into localized heat. Major PTA categories include inorganic nanomaterials and organic agents, with organic IR dyes gaining traction due to their biocompatibility and ease of modification. First-generation NIR-I dyes, like ICG, face limitations such as low penetration depth and rapid photobleaching, prompting the development of next-generation long-wavelength NIR-II dyes (1000–1700 nm) that offer deeper tissue penetration and improved imaging. Key NIR-II dye classes for breast cancer applications include modified cyanine derivatives, donor-acceptor structured small molecules, BODIPY and porphyrin-based dyes, and conjugated polymers. Despite advancements, challenges such as limited water solubility and rapid bodily clearance hinder clinical use. Solutions like nanocarrier encapsulation and stimuli-responsive systems are being explored to enhance effectiveness and safety in treatments. For example, ICG, the only FDA-approved dye, faces limitations like rapid degradation in PTT. Nanocarrier formulations such as ICG-loaded liposomes improve stability and efficacy, evidenced by successful tumor ablation in mice. IR-780 iodide is another promising dye, though its hydrophobicity restricts direct usage; its incorporation into nanoparticles has shown improved targeting and PTT performance. Other dyes like IR-820 and IR-1048 have also been investigated for their photothermal capabilities, with IR-1048 demonstrating effective tumor suppression at lower laser powers. Long-wavelength NIR dyes are often combined into multifunctional platforms, enhancing therapy efficacy through combined PTT and chemotherapy or photodynamic therapy. Overall, these findings highlight the potential of NIR dyes as effective therapeutic agents and versatile components in advanced breast cancer treatment strategies.35,36,43,44
Photothermal Therapy (PTT)
The core principle of PTT is that light, particularly in the NIR spectrum, excites photothermal agents, often nanoparticles, which change light energy into localized heat. This heat can effectively abolish cancer cells while sparing surrounding healthy tissue by causing irreversible cellular damage. PTT is considered a desirable alternative or complement to traditional cancer treatments due to its non-invasive nature and its ability to precisely target tumors.13,14,45,46 For example, one study examined the use of various nanoparticles in PTT for non-invasive breast cancer treatment. The article highlights the roles and mechanisms of these nanoparticles and emphasizes their potential when integrated with existing clinical therapies. The authors suggest that future research should focus on developing integrative platforms that combine multiple therapeutic approaches and optimizing nanoparticle synthesis to enhance treatment efficacy.2
Additionally, combining chemotherapeutic agents with PTT offers a promising synergistic effect. One study explored this combination by using spherical gold nanoparticles (AuNPs), approximately 14 nm in diameter, functionalized with polyethylene glycol (PEG) to improve stability as well as biocompatibility. These AuNPs exhibit a surface plasmon resonance peak around 520 nm, making them highly efficient at converting visible light into heat. In vitro experiments were conducted with MCF-7 breast cancer cells, which were incubated with the PEGylated AuNPs and then exposed to a 532 nm green laser. The irradiation led to a localized temperature increase, resulting in significant cancer cell death due to hyperthermia. When combined with the chemotherapeutic agent doxorubicin (DOX), the treatment demonstrated a synergistic effect, further reducing cell viability compared to either therapy alone. These findings suggest that using visible light to activate AuNPs can effectively enhance the efficacy of chemotherapy in breast cancer treatment, offering a promising avenue for developing minimally invasive therapies that selectively target cancer cells while diminishing injury to nearby healthy tissues.15
PTT using small organic molecules is a promising method for breast cancer treatment. One study introduced a novel strategy by designing small molecular organic nanoparticles that specifically target mitochondria within cancer cells. These nanoparticles enable mild PTT, using controlled heating to induce cancer cell death. By focusing the thermal effect on mitochondria, the treatment effectively triggers apoptosis and modulates autophagy, leading to enhanced elimination of cancer cells and reduced migration potential. This sub-cellular targeting strategy shows promise for controlling these cellular processes and holds potential for future metastatic cancer therapy.16 For example, one study developed a novel small molecule, TA1, designed for effective PTT against malignant breast cancer. TA1 incorporates a donor–acceptor structure as well as molecular rotors, resulting in high absorptivity, excellent photothermal conversion efficiency (84.8%), and remarkable photothermal stability. To optimize its application, TA1 was processed into uniform nanoparticles, approximately 44 nm in diameter, using microfluidic techniques. These nanoparticles exhibited strong inhibition of primary breast tumor growth and metastasis when exposed to NIR laser irradiation, as demonstrated in both in vitro and in vivo experiments. The findings underscore the potential of small organic molecule-based nanoparticles as promising agents in cancer nanomedicine, providing an effective molecular engineering strategy for developing efficient organic photothermal agents.17
In another study, a novel PTT-induced feedback carbon nanosystem was developed to enhance breast cancer treatment by remodeling the extracellular matrix (ECM). This study explores how this nanosystem improves the tumor microenvironment, making cancer cells more susceptible to therapy. The nanosystem consists of carbon-based nanoparticles that, when activated by NIR light, generate localized heat, disrupting the ECM and facilitating deeper drug penetration. The nanosystem enhances photothermal conversion efficiency, ensuring effective tumor ablation. Furthermore, ECM remodeling reduces tumor stiffness, improving drug diffusion and cellular uptake. The feedback mechanism helps sustain therapeutic efficacy, preventing tumor regrowth. In vivo and in vitro experiments demonstrate significant tumor inhibition and reduced metastasis (Figure 3). Overall, this study underscores the potential of PTT-induced ECM remodeling as a promising strategy to improve breast cancer therapy by enhancing drug delivery and tumor destruction.47
 |
Figure 3 ECM remodeling and associated consequences of increased PTT mediated by LCTi/L. (a) ECM remodeling and associated effects mediated by laser-irradiated LCTi are shown schematically. (b) In tumor tissues with various treatments, IF staining for (i) α-SMA, (ii) collagen I (green) and HA (red), (iii) TGF-β, and (iv) HIF-1α. In tumor tissues with various treatments, FC immunoassay of (c) CD80+CD86+ DCs and (d) CTLs. In tumor-draining lymph nodes after different treatments, FC immunoassay of (e) CD80+CD86+ DCs and (f) CTLs. In tumor tissues after various treatments, the contents of (g) IFN-γ and (h) TNF-α Data shown are mean ± SD (n = 3). *p < 0.05, **p < 0.01, ***p < 0.001.47 Reproduced from ref.47 Copyright ACS 2025. |
Combination Photothermal Therapy
Combination photothermal therapy provides a multifaceted strategy to breast cancer treatment. Combining the precise imaging capabilities of NIRFI with the therapeutic effects of PTT may enhance treatment results, reduce adverse effects, and provide a more customized strategy for cancer treatment. This approach offers real-time visualization of drug delivery, enabling accurate targeting, monitoring treatment response, and guiding personalized adjustments throughout the therapy. Moreover, NIRFI allows for tracking multiple therapeutic agents simultaneously, enabling clinicians to ensure precise targeting and optimize each component of the combination therapy.16,40 It also guides the delivery of therapies to ensure they specifically reach the tumor, diminishing contact with healthy tissues. This precision targeting is especially valuable when using potent agents, such as chemotherapeutics, immune modulators, or photothermal agents, which can cause significant side effects if administered systemically.
Recent research has explored the combination of PTT with other treatment modalities to enhance efficacy against breast cancer. For instance, one study investigated the synergistic effects of PTT combined with Lycium barbarum polysaccharide (LBP) and doxorubicin (DOX) for breast cancer treatment. The researchers developed a drug delivery system incorporating polypyrrole nanoparticles (PPY NPs) as photothermal agents. In vitro experiments demonstrated that the combination of DOX, LBP, and PPY NPs under NIR laser irradiation significantly inhibited the proliferation of 4T1 breast cancer cells. In vivo studies further showed that this combined therapy efficiently prevented tumor growth and reduced systemic toxicity, signifying a promising strategy for breast cancer treatment.40 However, various types of photothermal agents have been applied in PTT and combinatory therapy for breast cancer, as summarized in Table 1.
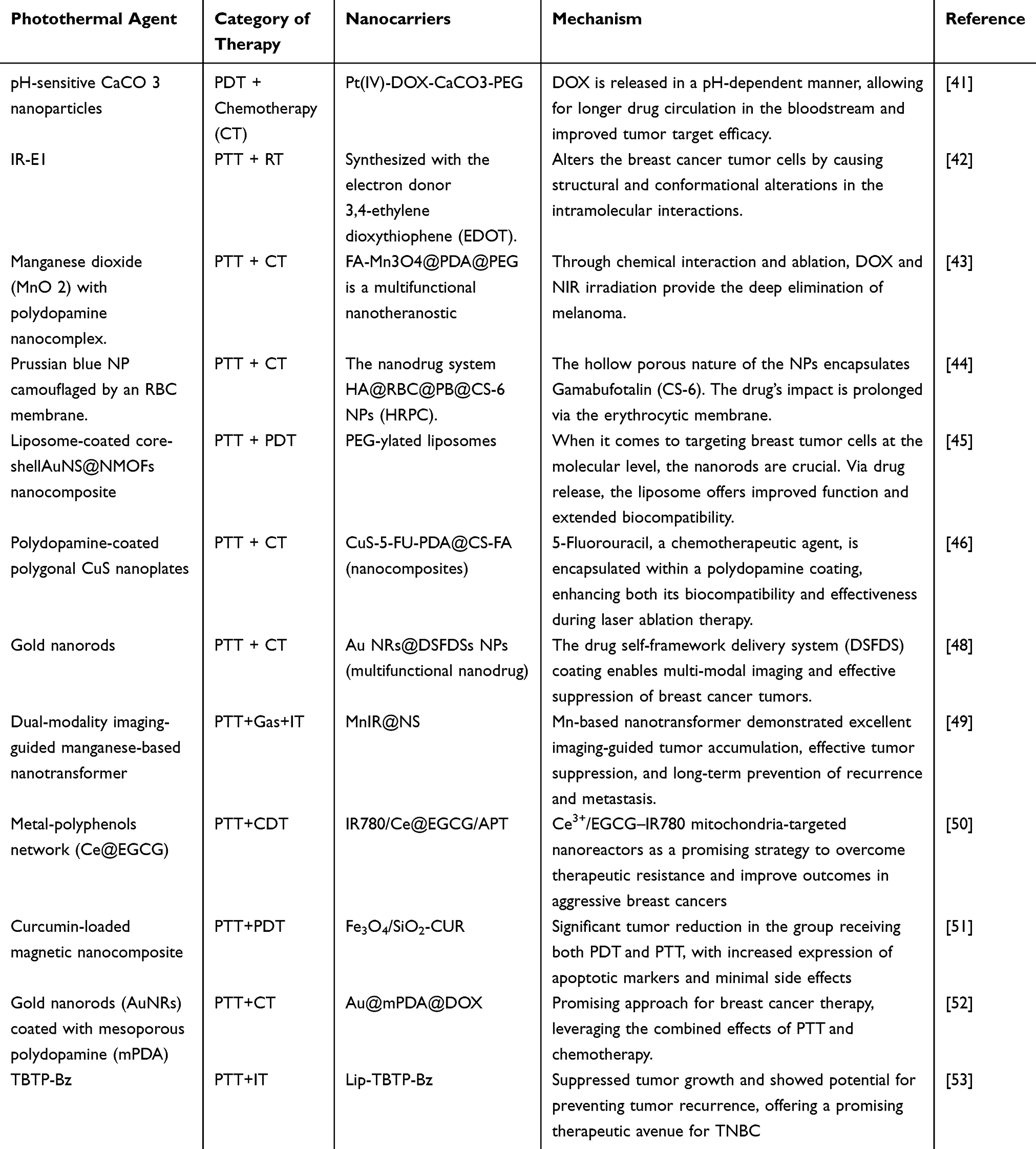 |
Table 1 Various Types of Photothermal Agents Used in PTT and Combinatory Therapy in Breast Cancer |
Chemo-Photothermal Therapy
Chemo-photothermal therapy, a promising approach, combines the therapeutic effects of CT and PTT therapy to create a synergistic treatment approach for breast cancer. The mechanism of chemo-photothermal therapy involves the use of nanoparticles as photothermal agents. These nanoparticles absorb light from an NIR laser and convert the energy into heat. This localized heat can lead to the damage of cancer cells through hyperthermia, which induces membrane disruption, protein denaturation, and apoptosis or necrosis.26 The combination of PTT and chemotherapy can also generate an immune response that helps clear remaining cancer cells, aiding in tumor eradication and preventing metastasis.
Advantages of chemo-photothermal therapy for breast cancer include enhanced efficacy, reduced side effects, tumor-specific targeting, minimized drug resistance, non-invasiveness, and synergistic immunomodulation.27 For example, one study investigated the combined use of PTT and CT to treat breast cancer cells. Researchers utilized spherical gold nanoparticles (AuNPs) approximately 14 nm in diameter, functionalized with polyethylene glycol (PEG) to enhance their stability and biocompatibility. These AuNPs exhibit a surface plasmon resonance peak around 520 nm, enabling efficient conversion of visible light into heat. In vitro experiments were performed using MCF-7 breast cancer cells. The cells were incubated with the PEGylated AuNPs and subsequently exposed to a 532 nm green laser. This irradiation led to a localized temperature increase, causing significant cancer cell death due to hyperthermia. When combined with the chemotherapeutic agent DOX, the treatment demonstrated a synergistic effect, further reducing cell viability compared to either therapy alone. The findings suggest that activating AuNPs with visible light can effectively enhance the efficacy of chemotherapy in breast cancer treatment. This method suggests a promising path for developing minimally invasive therapies that selectively target cancer cells while diminishing injury to surrounding healthy tissues.15
However, the combination of chemo-magnetic field-PTT therapy is a capable method in breast cancer treatment. For instance, research has focused on porous magnetite nanospheres (PMNSs) as carriers for combined chemo-magnetic field-PTT therapy.28 In one study, PMNSs were loaded with doxorubicin and coated with lactoferrin to target breast cancer cells. The combination of chemotherapy, magnetic field therapy, and PTT using these nanospheres resulted in enhanced tumor cell death and reduced side effects compared to traditional treatments. On the other hand, RBC-mimetic nanoparticles combined with NIR irradiation effectively inhibited primary tumor growth in mouse models of metastatic breast cancer, achieving a 98% reduction in lung metastases. The study demonstrated that this multi-modal approach could effectively target and abolish breast cancer cells while diminishing injury to surrounding healthy tissues.
Researchers developed red blood cell (RBC)-mimetic nanoparticles (NPs) designed for targeted as well as controlled drug delivery in breast cancer treatment. These nanoparticles consist of a core loaded with the chemotherapeutic drug DOX and a photothermal agent, wrapped in a membrane derived from RBCs. This design aims to combine chemotherapy and PTT for enhanced therapeutic efficacy. This study demonstrates the promise of bioinspired, NIR-responsive nanoparticles in providing a controlled and targeted approach to breast cancer therapy, effectively integrating chemotherapy and photothermal treatment modalities. These studies collectively suggest that integrating chemotherapy with photothermal therapy, particularly through the use of nanotechnology, holds promise for more effective breast cancer treatments. By combining these modalities, it is possible to achieve synergistic effects that enhance cancer cell destruction while potentially reducing the adverse effects associated with conventional therapies.29
Photothermal-Photodynamic Therapy
The combination of photothermal and photodynamic therapies (PTT and PDT) offers a synergistic treatment approach, enhancing the effectiveness of both therapies. PTT induces heat, which increases tumor vasculature permeability, thereby enhancing the effectiveness of PDT. PDT causes direct oxidative injury to tumor cells, while PTT generates oxidative stress and reactive oxygen species (ROS). Combining PTT and PDT helps overcome limitations such as tumor hypoxia and allows for more flexible targeting of both oxygenated and hypoxic tumor regions.32,38,51,54 This combination provides a synergistic effect, reducing side effects and minimizing damage to surrounding normal tissues. Due to its minimal adverse effects and favorable outcomes, this combination is frequently selected in therapeutic settings. The photosensitizing agent (PS), essential for PDT, plays a critical role in generating ROS. When a nano-scale electric field interaction is utilized to create ROS, it increases cytotoxicity and shortens the half-life of tumor cells, thereby enhancing the anti-cancer efficacy of PDT. There are three main types of PS agents. One example is the hematoporphyrin derivative (HPD), which is particularly effective in targeting tumors in cases involving esophageal, lung, and breast cancers.32,51 However, dual-function nanocomposites offer a synergistic treatment approach. For example, researchers have developed a dual-function nanocomposite (NC) to progress the effectiveness of breast cancer treatment. This NC combines PDT and PTT by integrating curcumin, a natural photosensitizer, with magnetic nanoparticles. The NC consists of Fe3O4 magnetic nanoparticles coated with silica, onto which curcumin molecules are immobilized. A study involving six groups of Balb/c mice with induced breast tumors found a significant reduction in tumor volume. The NC + PDT + PTT group exhibited induced apoptosis in tumor cells, making it a promising alternative to traditional chemotherapy. Moreover, the study concluded that combining PDT and PTT using the curcumin-loaded magnetic nanocomposite is a promising strategy for treating triple-negative breast cancers. This dual approach leverages the advantages of both therapies, potentially leading to more effective and safer cancer treatments.51
In another study, gold nanocages (AuNCs) co-assembled with Spinacia oleracea (spinach) leaf extract were developed as a multifunctional nanoplatform for combined photothermal and photodynamic therapy against 4T1 breast cancer cells. The Spinacia oleracea extract provided chlorophyll molecules that acted as natural photosensitizers, capable of generating reactive oxygen species under NIR irradiation. The AuNCs served as efficient photothermal converters, rapidly increasing local temperature upon NIR exposure. The co-assembly process produced uniform spherical SPAuNCs with an average diameter of about 70 ± 10 nm, ensuring excellent dispersion and stability in aqueous media. The synergistic effect of photothermal heating from AuNCs and ROS generation from chlorophyll enabled enhanced tumor cell ablation compared with either therapy alone. Green synthesis using plant extract reduced the need for toxic reducing agents, improving biocompatibility. Characterization techniques such as UV–Vis spectroscopy, TEM, and DLS confirmed the successful integration of AuNCs with chlorophyll. Overall, SPAuNCs demonstrated a promising, eco-friendly nanoplatform for efficient dual-mode phototherapy in breast cancer treatment.54 Collectively, these studies indicate that integrating PTT and PDT, especially when combined with other treatments like immunotherapy, holds significant potential for improving breast cancer therapy. Ongoing research is focused on optimizing these combinations to maximize therapeutic effectiveness while diminishing side effects.
Photothermal-Immunotherapy
Photothermal immunotherapy (PTI) is a capable method for breast cancer treatment, combining PTT with immunotherapy. This synergistic strategy enhances the therapeutic efficacy of PTT while exciting the body’s immune system to identify and attack residual cancer cells, potentially improving long-term outcomes and preventing recurrence.55–57 A key advantage of PTI lies in its ability to simultaneously ablate tumor cells and activate immune responses targeting both primary tumors and metastatic lesions. The mechanism of PTI in breast cancer involves selective tumor ablation via light-activated heat, which induces tumor cell death. This process can cause vascular disruption, ischemic damage, and the release of tumor-associated antigens and damage-associated molecular patterns, thereby triggering an immune response. Thermal ablation also promotes the release of immune-stimulating molecules such as cytokines, chemokines, and exosomes, which help recruit immune cells to the tumor site. Additionally, dendritic cells can be triggered following PTT, playing a crucial role in antigen presentation to T cells and the stimulation of cytotoxic T lymphocytes. For example, one study developed a versatile hydrogel composed of polydopamine (PDA) nanoparticles, DOX, and CpG oligodeoxynucleotides. This hydrogel was designed for intratumoral injection followed by NIR light irradiation. The treatment demonstrated a synergistic effect against 4T1 breast cancer cells and activated cytokine secretion from immune cells. In vivo experiments showed that this combined chemo-photothermal immunotherapy eradicated primary tumors and significantly inhibited metastasis. The high anticancer efficacy was attributed to the induced host immune response, suggesting that this combinational strategy holds great promise for effective breast cancer treatment.57
The use of nanoparticles in PTT has shown significant potential in enhancing immunotherapy for breast cancer treatment. PTT can produce immunogenic cell death, inducing to the release of tumor-associated antigens that stimulate an immune response. When combined with immunotherapeutic agents, this approach can produce a more robust and systemic anti-tumor effect, addressing both primary and metastatic tumors.2 For instance, researchers have developed a novel nanoprobe designed for both imaging and therapeutic applications in cancer treatment. This nanoprobe emits in the near-infrared IIb (NIR-IIb) window, offering advantages in biological imaging due to declined light scattering and deeper tissue penetration. In vivo studies demonstrated that nanoprobe-mediated photothermal therapy effectively ablated tumors in mouse models. The treatment not only destroyed tumor cells but also triggered an anti-tumor immune response, as demonstrated by increased infiltration of immune cells into the tumor microenvironment. This study focuses on the possibility of NIR-IIb-emitting nanoprobes as multifunctional agents for cancer theranostics. In another study, an innovative approach was developed to treat triple-negative breast cancer by combining photothermal therapy with immunotherapy. Researchers designed a phototheranostic agent, TBTP-Bz, featuring aggregation-induced emission properties and a pyridinium rotor structure. This agent was co-encapsulated with the STING agonist MSA-2 into thermally responsive exosome-liposome hybrid nanoparticles for targeted tumor delivery. Upon near-infrared light exposure, TBTP-Bz induced immunogenic cancer cell death and facilitated the specific release of MSA-2, thereby enhancing STING pathway stimulation and promoting a robust antitumor immune response. This strategy effectively suppressed tumor growth and showed potential for preventing tumor recurrence, offering a promising therapeutic avenue for TNBC. By combining high-resolution imaging with effective photothermal therapy and immune system activation, these nanoprobes present a hopeful method for improving cancer treatment consequences (Figure 4).53
 |
Figure 4 (a) Regulating molecular mobility in the aggregate state allows for the rational strategy of the AIE NIR-II emissive photothermal agent. (b) Coadministration of the STING agonist MSA-2 with the AIE phototheranostic agent TBTP-Bz via exosome–liposome hybrid AMFL. (c) Drug distribution for synergistic photothermal immunotherapy of breast cancer is facilitated by tumor-targeting AMFL that is thermoresponsive through activation of the STING pathway.53 Reproduced from ref.53 Copyright ACS 2025. |
A recent study investigated the use of microfluidic technology to develop biocompatible conjugated polymer nanoparticles (CP NPs) for PTT in cancer treatment. By precisely regulating the antisolvent conditions within the microfluidic system, researchers produced CP NPs with a consistent size of approximately 52 nm. To improve cancer cell targeting, the nanoparticles were functionalized with cyclic arginine-glycine-aspartic acid (c-RGD) peptides. When exposed to an 808 nm near-infrared laser, these c-RGD-modified CP NPs demonstrated strong photothermal conversion capabilities, leading to efficient cancer cell ablation. In vitro assays revealed that the CP NPs stimulated a proinflammatory response in macrophages. Moreover, in vivo studies using tumor-bearing mice showed that a single session of CP NP-mediated PTT significantly enhanced antitumor immune activity and suppressed tumor progression. This research highlights the advantages of microfluidic synthesis for creating uniform, functionalized nanoparticles and underscores the therapeutic potential of CP NPs in eliciting immune-driven cancer suppression.58 In addition, researchers have addressed the challenge of tumor hypoxia, an obstacle that often limits therapeutic efficacy, by designing oxygen-releasing nanoparticles capable of responding to the specific conditions of the tumor microenvironment. These nanoparticles were engineered to deliver oxygen to hypoxic tumor regions, improving drug delivery efficiency. The oxygen-rich environment also enhances the effectiveness of immunotherapeutic agents, improving tumor cell recognition and destruction. This nano-vehicle promotes a stronger immune attack against tumors, improving therapeutic outcomes in preclinical models. The study suggests that this approach could be translated into clinical settings to boost cancer immunotherapy, offering a novel strategy to overcome tumor resistance. This research presents a promising strategy for enhancing immunotherapy by addressing tumor hypoxia, potentially leading to more effective cancer treatments.59
Photothermal-Radiotherapy
A new and promising treatment approach called photothermal-radiotherapy (PTR) combines radiation therapy with PTT to improve cancer treatment outcomes. Photothermal radiotherapy for breast cancer represents an exciting frontier in cancer treatment, providing the potential for enhanced tumor destruction, enhanced precision, and reduced side effects.60–63 By combining the localized heat of PTT with the DNA-damaging effects of radiation, this approach aims to produce a synergistic effect that can overcome some of the limitations of traditional therapies. Photothermal therapy utilizes light-absorbing nanoparticles, usually in the NIR spectrum, to generate localized heat when exposed to light. This heat induces necrosis or apoptosis, damaging cancer cells. Radiation therapy, by contrast, causes cell death through ionizing radiation that damages the DNA of cancer cells. By leveraging their complementary mechanisms, PTT and RT work together to address the drawbacks of each therapy when used alone. PTT can increase cell membrane permeability and improve tumor vasculature, thereby enhancing the susceptibility of tumor cells to radiation-induced damage.
For example, one study investigated the usage of alginate-coated gold nanoparticles for combined PTT and RT in breast cancer treatment. The alginate coating enhanced the biocompatibility and stability of the AuNPs, facilitating their accumulation in tumor tissues. Upon exposure to NIR light, these nanoparticles generated localized heat, effectively inducing tumor cell death through PTT. Additionally, the high atomic number of gold increased the local radiation dose during RT, further contributing to tumor eradication. In vivo research demonstrated that the combination of PTT and RT using alginate-coated AuNPs led to substantial tumor regression related to either therapy alone.63 Another study explored the application of zirconium carbide (ZrC) nanoparticles in the treatment of TNBC. ZrC nanoparticles exhibit excellent photothermal conversion efficiency and radiotherapeutic properties. In vitro and in vivo research showed that combining ZrC-mediated PTT with RT significantly prevented tumor development and generated tumor cell apoptosis. Additionally, the treatment modulated the tumor microenvironment, promoting an anti-tumor immune response. These results propose that ZrC nanoparticles could assist as applicable agents for combined PTT and RT in TNBC therapy. In summary, integrating PTT with radiotherapy presents a capable avenue for enhancing breast cancer treatment efficacy. The use of multifunctional nanoparticles facilitates this combined approach, offering potential for improved patient outcomes.64
Photothermal-Chinese Medicine Therapy
Photothermal-Chinese Medicine Therapy for breast cancer is a therapeutic approach that combines traditional Chinese medicine (TCM) with modern PTT to treat breast cancer. PTT involves using light to generate heat in specific tissues, causing thermal damage to cancer cells and leading to their destruction. Common herbs used in breast cancer treatment include Ginseng, Astragalus, Curcumin, Huang Qi, and Scutellaria baicalensis. Nanoparticles are employed to enhance the efficiency of PTT by coating them with Chinese medicinal compounds. These nanoparticles improve drug delivery to the tumor site and increase the precision of photothermal treatment. The mechanism of action for this combined approach involves targeted therapy using nanoparticle-enhanced photothermal therapy. For example, one study investigated an innovative process to enhance the effectiveness of doxorubicin (DOX) in breast cancer therapy. Researchers developed a drug delivery system combining Lycium barbarum polysaccharides (LBP) with polypyrrole nanoparticles (PPY NPs), known for their photothermal properties. This system was administered locally to target tumor sites. In vitro cytotoxicity tests revealed that the combination of DOX, LBP, and PPY NPs under NIR laser irradiation significantly prevented the proliferation of 4T1 cells, achieving an inhibition rate eight times higher than that of DOX alone at the equal concentration (64% vs 8%). In vivo antitumor research demonstrated a tumor prevention rate of 87.86% in the group treated with LBP, DOX, PPY NPs, and NIR irradiation.40
Furthermore, histological analyses and biochemical assays indicated that this combined treatment reduced systemic toxicity and minimized liver damage compared to other treatment groups. The findings suggest that integrating LBP and PPY NPs with PTT therapy can notably enhance the antitumor effectiveness of DOX while mitigating its adverse side effects. This strategy holds promise for developing more effective and safer breast cancer treatments. TCM has been extensively used as a complementary approach in breast cancer care. Studies have shown that TCM can improve survival rates in patients with advanced breast cancer. For instance, an observational study indicated that incorporating adjunctive TCM into treatment may be associated with a reduced mortality risk in patients with advanced-stage breast cancer. Integrating photothermal therapy with traditional Chinese medicine offers a promising avenue for breast cancer treatment. This combined approach aims to harness the strengths of both therapies, possibly leading to enhanced therapeutic consequences and decreased side effects.65 Further investigation is warranted to augment treatment protocols and fully understand the underlying mechanisms of this synergistic strategy.
Triple Therapies for Breast Cancer
Triple Therapies with PTT for Breast Cancer is a novel approach that combines PTT with chemotherapy and immunotherapy to improve treatment efficacy. PTT uses light to generate localized heat, which destroys cancer cells and enhances drug delivery. It is particularly effective when combined with chemotherapy, which applies cytotoxic drugs to kill quickly spreading cancer cells.66–68 The heat generated by PTT can enhance blood flow to the tumor, improving the delivery of chemotherapy drugs directly to the tumor cells. Immunotherapy activates the body’s immune defenses, enabling them to identify and target cancer cells more effectively. PTT can potentially improve the efficacy of immunotherapies by altering the tumor microenvironment to favor immune cell infiltration. Additionally, PTT can help overcome chemotherapy resistance by increasing the effectiveness of chemotherapeutic agents.67,68 However, challenges such as toxicity management and optimal treatment timing remain. Nanoparticle-based drug delivery increases the tumor’s ability to absorb light, enhancing PTT efficiency by improving light absorption and targeted delivery.
Combining PTT with radiation therapy increases tumor sensitivity to radiation, improving the overall effectiveness of treatment. However, nanoparticle toxicity must be carefully managed, and radiation resistance may still develop. PTT and acupuncture are two complementary treatments that can improve cancer patients’ complete health and treatment outcomes. Acupuncture, a TCM system, includes inserting needles into precise points on the body to balance Qi, relieve pain, reduce inflammation, and support healing. It can help reduce the side effects of PTT and additional cancer treatments, such as radiation and chemotherapy. Herbal medicine, another component of TCM, may enhance PTT by sensitizing tumors to heat or improving the immune response. These integrative approaches offer a holistic treatment strategy, addressing not only the tumor but also the patient’s overall well-being. For example, one study explored a novel strategy for enhancing breast cancer treatment by combining PTT, sonodynamic therapy (SDT), and immune checkpoint blockade. Researchers engineered cancer cell membrane-mimicking nanoparticles (CHINPs) encapsulating superparamagnetic iron oxide (SPIO) and hematoporphyrin monomethyl ether (HMME). These CHINPs exhibited strong tumor-targeting efficiency and could be sequentially activated by ultrasound and NIR light, with guidance from MRI, PA, and PT imaging. This dual-mode activation resulted in complete localized tumor ablation and triggered a robust systemic anti-tumor immune response. When combined with immune checkpoint blockade therapy, this approach effectively suppressed tumor metastasis (Figure 5).69
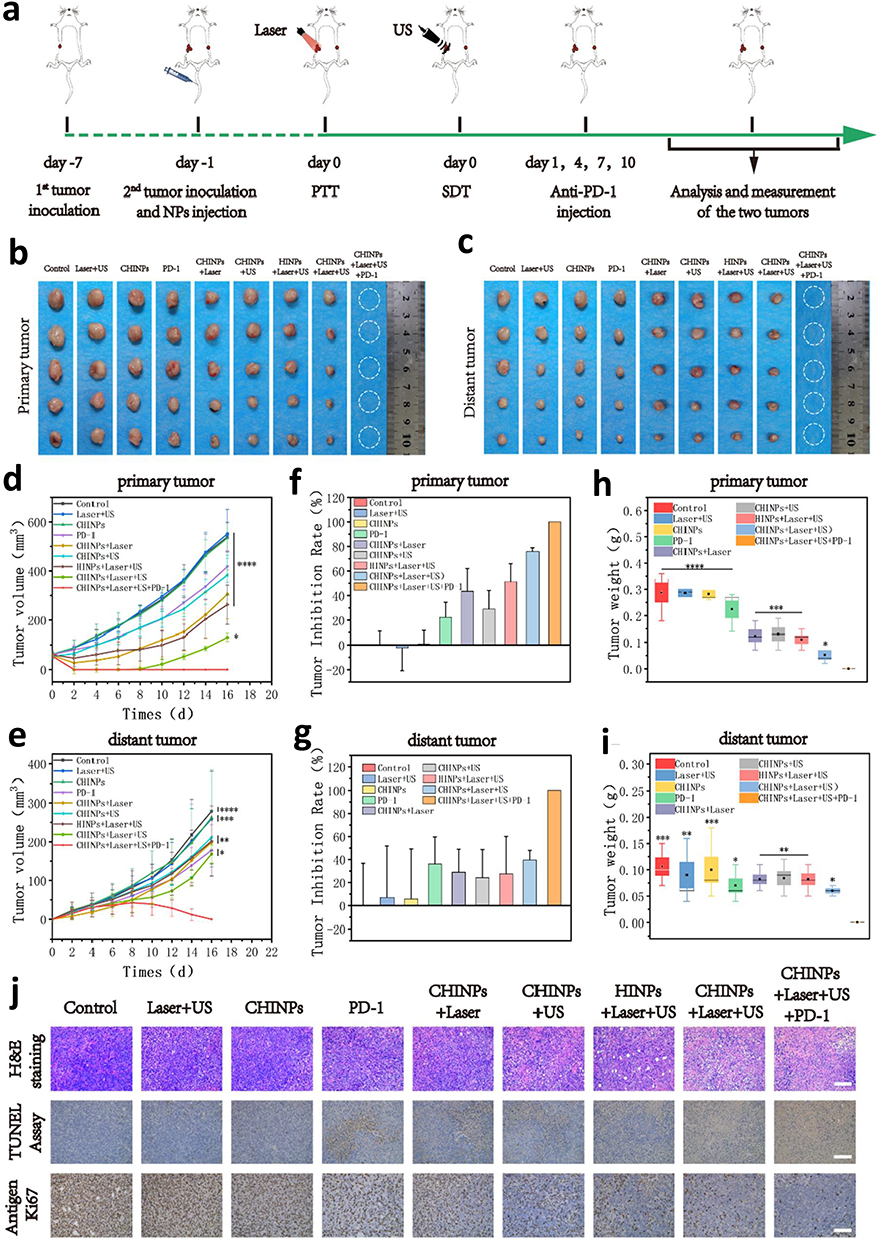 |
Figure 5 PTT/SDT composed with anti-PD-1 immunotherapy has anticancer properties in vivo. (a) A schematic representation of the in vivo experimental setup. The tumor located on the right abdomen was designated as the primary tumor, while the tumor on the left flank served as a model for distant metastasis. Representative images of excised primary (b) and distant (c) tumors from 4T1 tumor-bearing mice subjected to different treatment regimens. Tumor growth curves of the primary (d) and distant (e) tumors in various treatment groups. Tumor inhibition rates for the primary (f) and distant (g) tumors after therapy. Average tumor weights for the primary (h) and distant (i) tumors post-treatment. (j) Histological analysis of tumor tissues from each group, including H&E staining, TUNEL assay, and Ki-67 immunohistochemistry, to assess tissue damage, apoptosis, and proliferation, respectively. Data shown are mean ± SD (n = 3). Statistical differences determined by one-way ANOVA; *p < 0.05, **p < 0.01, ***p < 0.001, **** p< 0.0001.69 Reproduced from ref.69 Copyright BMC 2022. |
In another study, researchers constructed a core–shell nanocomposite by integrating gold nanostars (AuNS) with nanoscale metal–organic frameworks (NMOFs) composed of zirconium ions (Zr4+) and tetrakis(4-carboxyphenyl)porphyrin (TCPP). This composite was further encapsulated with gambogic acid (GA), a heat-shock protein 90 (HSP90) inhibitor, and coated with PEGylated liposomes to augment stability and biocompatibility. Upon cellular uptake, the nanocomposite was designed to degrade in the acidic tumor microenvironment, releasing its components for synergistic therapeutic effects. The AuNS facilitated mild PTT by converting NIR light into heat to induce cancer cell death. Simultaneously, TCPP within the NMOFs mediated PDT by generating reactive oxygen species under light irradiation. GA inhibited HSP90, reducing the thermal conflict of cancer cells and enhancing PTT efficacy.70 In vitro and in vivo experiments proved that this nanoplatform effectively induced cancer cell apoptosis and inhibited tumor growth under NIR laser irradiation. The integration of PTT, PDT, and chemotherapy within a single nanoplatform provides a promising method for breast cancer treatment.70
Another study investigated the application of AuNPs to augment the efficacy of DOX chemotherapy through PTT. The combination of DOX with AuNPs under laser irradiation led to a synergistic reduction in breast cancer cell viability, underscoring the potential of combining PTT with chemotherapy.15 Additionally, researchers explored a dual therapy approach using PTT and PDT by employing curcumin as a photosensitizer and magnetic nanoparticles as carriers. This combination significantly inhibited tumor growth in vivo, suggesting that integrating PTT and PDT could be a potent method for BC treatment.51 Another study presented a biomimetic tumor cell membrane-encapsulated nanoparticle system designed to enhance immunotherapy for TNBC by combining NIR-II PTT and chemotherapy. These nanoparticles, coated with tumor cell membranes, allowed for immune evasion and efficient targeting of cancer cells. The system integrated NIR-II PTT, which generated localized heat for tumor ablation, with chemotherapy, providing enhanced cancer cell destruction. The tumor cell membrane coating also activated the immune system, promoting anti-tumor immune outcomes. This biomimetic coating improved nanoparticle retention and tumor penetration while reducing off-target effects. Experimental results demonstrated significant tumor suppression, reduced metastasis, and increased immune activation, ultimately improving overall therapeutic outcomes. This study highlights a promising nanotechnology-based strategy for TNBC treatment, demonstrating how a combination of PTT, chemotherapy, and immune modulation can enhance cancer therapy.71
PTT- Gas Therapy
PTT is a non-invasive breast cancer treatment that uses NIR irradiation to induce localized hyperthermia and ablative effects on tumors. However, its clinical use faces challenges such as thermotolerance from heat shock proteins, limited light penetration, and hypoxic microenvironments that reduce effectiveness. Gas therapy, involving bioactive gases like nitric oxide (NO) and carbon monoxide (CO), complements PTT by inducing apoptosis, improving oxygen levels, and enhancing vascular permeability. The combination of PTT and gas therapy enhances tumor suppression through synergistic effects, as seen in preclinical studies with nanoplatforms that release therapeutic gases upon PTT activation.49,72 Although promising, issues like gas delivery control, light penetration, and biosafety hinder clinical application. Overall, this combined approach holds significant potential to enhance breast cancer treatment outcomes.
However, in one study, researchers designed a dual-modality imaging-guided manganese-based nanotransformer (Mn-NM) to integrate gas therapy, PTT, and immunotherapy for the treatment of TNBC. The nanoplatform was constructed by embedding manganese dioxide (MnO2) nanosheets with a nitric oxide (NO) donor, followed by surface modification with biocompatible polymers to enhance stability and tumor accumulation. Under the tumor microenvironment’s acidic and H2O2-rich conditions, MnO2 decomposed to release Mn2+ ions for MRI and simultaneously triggered catalytic decomposition of endogenous H2O2 to generate oxygen, thereby alleviating tumor hypoxia. In addition, NIR irradiation activated the photothermal conversion capability of the Mn-based nanosystem, which not only produced localized hyperthermia for tumor ablation but also accelerated the release of therapeutic NO gas, inducing oxidative/nitrosative stress and synergistic cytotoxicity. Importantly, this combination of gas-PTT promoted immunogenic cell death, enhancing tumor antigen release and dendritic cell maturation, which, when paired with checkpoint blockade therapy, significantly boosted systemic antitumor immune responses. Moreover, in 4T1 TNBC mouse models, the Mn-based nanotransformer exhibited excellent imaging-guided tumor accumulation, effective tumor suppression, and long-term prevention of recurrence and metastasis, highlighting its promise as a multifunctional theranostic platform for aggressive breast cancers.49
In another study, a self-assembled hydrogen sulfide (H2S) generating photosensitizer nanoplatform was developed that integrates gas therapy with PTT for effective cancer treatment. The system was based on a rationally designed sulfur-containing small-molecule photosensitizer, which, through amphiphilic modification, could self-assemble into stable nanoparticles without additional carriers. Under NIR laser irradiation, the photosensitizer exhibited strong photothermal conversion efficiency, producing localized hyperthermia for tumor ablation. Simultaneously, the sulfur-rich segments within the nanostructure were activated to continuously release H2S gas, a therapeutic gas known to induce mitochondrial dysfunction, oxidative stress, and apoptosis in tumor cells. Furthermore, this dual action enabled a gas-assisted synergistic PTT effect, where H2S potentiated the photothermal damage and improved overall therapeutic efficacy. In murine tumor models, these self-assembled nanoparticles showed excellent tumor accumulation, efficient NIR-triggered heating, controlled H2S release, and significant tumor growth inhibition with negligible systemic toxicity. However, the results demonstrate that carrier-free, self-assembling H2S-generating photosensitizer nanoparticles are a powerful and biocompatible strategy for advancing multifunctional nanomedicine in cancer therapy.72
PTT-Chemodynamic Therapy
PTT has significant potential in breast cancer treatment by inducing localized tumor ablation with NIR irradiation. Its effectiveness is often hindered by incomplete tumor eradication, thermotolerance, and heterogeneity of the tumor microenvironment. Chemodynamic therapy (CDT) enhances this approach by utilizing Fenton reactions to generate cytotoxic hydroxyl radicals from hydrogen peroxide, inducing tumor cell death through oxidative stress. Combining PTT and CDT allows for a synergistic effect, where PTT boosts reaction kinetics, improves tumor perfusion, and promotes reactive oxygen species (ROS) generation, while CDT addresses thermotolerance and reduces tumor recurrence risk. Recent studies have introduced multifunctional nanoplatforms like Fe3O4 nanoparticles and CuS nanostructures that act as both photothermal agents and ROS catalysts, yielding promising therapeutic outcomes and minimizing systemic toxicity.50,73 Additionally, PTT can stimulate antitumor immunity, while CDT mitigates tumor hypoxia. Despite these advances, challenges such as optimizing catalytic efficiency and achieving precise tumor targeting persist. Overall, PTT-CDT combination therapy shows promise in nanomedicine for breast cancer, enhancing treatment efficacy compared to traditional monotherapies.
However, one study reported the design of a mitochondria-targeted nanoreactor to augment the sensitivity of photothermal ferroptosis combination therapy for TNBC. The nanoplatform was constructed using a Ce3+/EGCG (epigallocatechin gallate) coordination complex that was further co-loaded with the near-infrared dye IR780 as the photothermal agent. In addition, surface functionalization with a mitochondria-targeting moiety (eg, triphenylphosphonium, TPP) enabled preferential accumulation of the nanoreactor within mitochondria, the subcellular site highly vulnerable to oxidative damage. Upon NIR irradiation, IR780 generated localized hyperthermia to trigger ferroptotic pathways, while the Ce3+/EGCG complex catalyzed the depletion of intracellular glutathione (GSH) and enhanced lipid peroxidation (LPO), both of which are key drivers of ferroptosis. Moreover, this dual mechanism produced a synergistic effect: mitochondrial oxidative stress was amplified, ferroptosis sensitivity was increased, and photothermal ablation efficacy was markedly improved. In 4T1 TNBC cell and animal models, the mitochondria-targeted nanoreactor exhibited strong tumor accumulation, efficient subcellular localization, enhanced ferroptotic cell death, and significant tumor growth suppression with minimal systemic toxicity. This work highlights Ce3+/EGCG–IR780 mitochondria-targeted nanoreactors as a promising strategy to overcome therapeutic resistance and improve outcomes in aggressive breast cancers.50
In another study, the authors designed an NIR-II excitation phototheranostic nanoplatform capable of integrating PTT, chemotherapy, and CDT for the treatment of breast cancer bone metastases. However, the system was built from a hollow mesoporous carbon-based nanocarrier that exhibited strong absorption in the NIR-II window (1000–1350 nm), ensuring deep tissue penetration and efficient photothermal conversion. In addition, to achieve multimodal therapy, the nanocarrier was loaded with the chemotherapeutic drug DOX and decorated with iron-based catalytic components to trigger Fenton-like reactions, converting tumor-overexpressed H2O2 into highly toxic hydroxyl radicals (•OH) for CDT. Under NIR-II laser irradiation, the platform not only generated localized hyperthermia for tumor ablation but also accelerated drug release and improved catalytic activity, thereby enhancing the synergistic effect of chemotherapy and CDT. Furthermore, the nanoplatform allowed photoacoustic and thermal imaging, enabling real-time monitoring of drug distribution and therapeutic outcomes. In mouse models of breast cancer bone metastases, this multifunctional system demonstrated excellent tumor accumulation, potent tumor growth inhibition, and significant suppression of osteolytic lesions, with minimal off-target toxicity. Collectively, the NIR-II carbon-based nanoplatform co-loaded with DOX and Fe catalysts offers a promising strategy for imaging-guided, multimodal therapy of metastatic breast cancer in bone.73
PTT-Starvation Therapy
PTT is a minimally invasive treatment for breast cancer that uses NIR irradiation to induce localized hyperthermia and destroy tumor tissues. However, its effectiveness is often limited by thermotolerance from heat shock proteins and NIR light’s shallow penetration. Complementary starvation therapy, achieved through glucose depletion or interference with tumor metabolism, can enhance the treatment. The integration of PTT and starvation therapy yields a synergistic effect, where PTT increases intratumoral temperature and blood flow, while starvation makes cancer cells more susceptible to hyperthermia. Recent innovations include multifunctional nanoplatforms, such as GOx-loaded gold nanostructures and polymeric nanoparticles, which simultaneously elevate local temperatures and deplete glucose, leading to increased oxidative stress and apoptosis.74,75 While these combined therapies show promise, challenges such as enzyme stability, off-target effects, and tumor-specific delivery persist, making this dual-modality approach a potential avenue for more effective breast cancer treatments. However, one study reported the development of glucose oxidase (GOx)-loaded colloidally stable tungsten disulfide (WS2) nanobowls as a multifunctional nanoplatform for synergistic starvation therapy and PTT. In addition, the nanobowls were fabricated from ultrathin WS2 nanosheets via a templated synthesis strategy, giving them a unique bowl-like morphology with a high surface area and abundant sites for enzyme loading. GOx was immobilized on the surface to catalyze glucose oxidation, consuming glucose and generating gluconic acid and H2O2, thereby inducing nutrient deprivation and oxidative stress within tumor cells. Meanwhile, the intrinsic NIR absorption of WS2 endowed the nanobowls with excellent photothermal conversion efficiency, enabling effective tumor ablation upon near-infrared (808 nm) irradiation. Importantly, the colloidal stabilization strategy significantly improved the dispersion and physiological stability of WS2 nanobowls, overcoming aggregation issues typically associated with 2D transition-metal dichalcogenides. This study highlights WS2–GOx hybrid nanobowls as a versatile therapeutic design for combining metabolic intervention with nanophotothermal therapy.74
In another study, the researchers engineered an antineoplastic enzyme–based nanocarrier that not only served as a drug delivery platform but also exhibited activatable catalytic activity for combined cancer therapy. In addition, the system was constructed by coating the enzyme glucose oxidase (GOx) with a pH-sensitive polymer shell, which kept the catalytic activity “OFF” during systemic circulation to avoid premature glucose depletion and systemic toxicity. Once in the acidic tumor microenvironment, the polymer shell disassembles, reactivating GOx’s catalytic function to oxidize glucose into gluconic acid and H2O2, thereby initiating starvation therapy and oxidative stress. At the same time, the nanocarrier co-loaded the chemotherapeutic drug DOX, enabling a synergistic effect of chemotherapy with enzyme-mediated starvation therapy. Moreover, the H2O2 generated by GOx activity could participate in Fenton-like reactions when combined with iron-based components, amplifying CDT. This multifunctional enzyme–drug platform thus integrated chemotherapy, starvation therapy, and CDT in a tumor-activated manner. In 4T1 breast cancer models, the system demonstrated efficient tumor accumulation, significant glucose depletion, enhanced DOX release, and potent tumor growth suppression with minimal systemic toxicity. Overall, the GOx–polymer–DOX nanocarrier represents a smart strategy to overcome tumor metabolic adaptability and improve therapeutic efficacy through activatable, synergistic multimodal therapy.75
Imaging-Guided PTT and Combinatory Therapy
Image-Guided PTT and Combinatory Therapy for Breast Cancer is a personalized treatment approach that applies real-time imaging techniques to guide the delivery of PTT. This strategy enhances precision, effectiveness, and safety by allowing clinicians to monitor and direct the therapy as it progresses. Key components include image guidance, utilizing techniques such as CT, ultrasound, MRI, and FL imaging to visualize the tumor and surrounding tissues, and PTT, which uses light to heat and destroy cancer cells.76 Image-guided PTT is a powerful tool that can be combined with various other therapies to improve breast cancer treatment outcomes. Common combinations include chemotherapy, immunotherapy, radiation therapy, nanoparticle delivery, and stem cell therapy. Chemotherapy targets and kills quickly dividing cancer cells using cytotoxic drugs, whereas immunotherapy enhances the body’s immune system to detect and eliminate cancer cells. The heat generated by PTT can enhance the sensitivity of cancer cells to chemotherapy, thereby augmenting drug delivery and uptake.
For instance, one study explored a novel therapeutic approach that integrates PTT with chemotherapy to augment the efficacy of breast cancer treatment. Researchers developed a core, shell nanoplatform, denoted as Au@mPDA@DOX, consisting of gold nanorods (AuNRs) coated with mesoporous polydopamine (mPDA) and loaded with the chemotherapeutic agent doxorubicin (DOX). This design harnesses the photothermal properties of AuNRs and the drug-loading capability of mPDA to achieve a synergistic therapeutic effect. The Au@mPDA@DOX nanoplatform exhibits superior photothermal conversion efficiency and features a dual-responsive drug release system triggered by both acidic pH and NIR laser irradiation. This enables precise and controlled drug delivery specifically within the tumor microenvironment. In vitro experiments revealed increased cellular uptake and enhanced tumor penetration under NIR exposure. The synergistic application of PTT and chemotherapy significantly amplified cancer cell apoptosis compared to either modality alone. In vivo studies using 4T1 breast tumor-bearing mice demonstrated efficient tumor site accumulation of Au@mPDA@DOX via the enhanced permeability and retention (EPR) effect. Following NIR laser treatment, the group showed marked tumor growth suppression and extended survival, with minimal toxicity to vital organs. These results highlight Au@mPDA@DOX as a promising approach for breast cancer therapy, leveraging the combined effects of PTT and chemotherapy. This synergistic approach not only enhances anti-tumor efficacy but also minimizes systemic toxicity, offering a potential pathway for more effective cancer therapeutics (Figure 6). 52
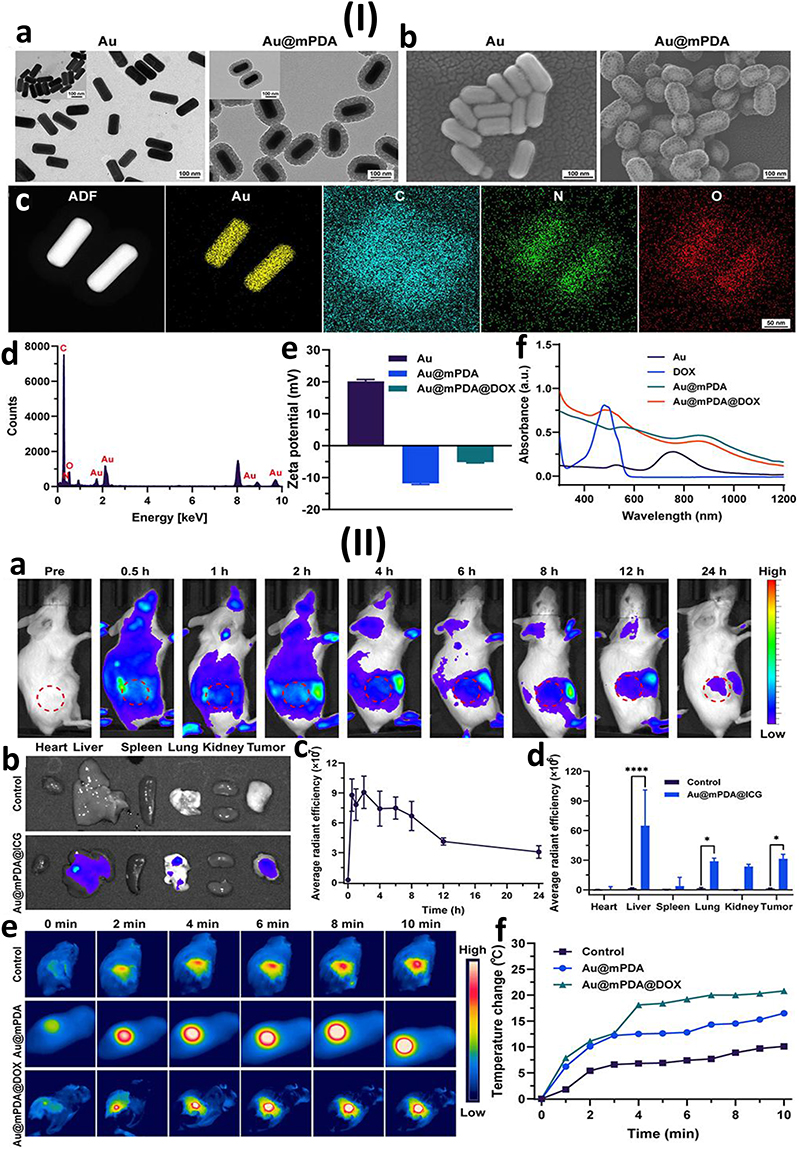 |
Figure 6 (I) Au@mPDA@DOX nanoparticles characterization. Representative images show the morphology of Au and Au@mPDA nanoparticles captured via (a) transmission electron microscopy (TEM) and (b) scanning electron microscopy (SEM). (c) Elemental mapping of Au@mPDA@DOX confirms its composition, while (d) energy-dispersive X-ray spectroscopy (EDS) further validates the elemental distribution. (e) Zeta potential measurements compare surface charges of Au, Au@mPDA, and Au@mPDA@DOX. (f) UV-Vis absorption spectra highlight the optical properties of Au, DOX, Au@mPDA, and Au@mPDA@DOX. (II) Fluorescence and photothermal imaging were conducted both in vivo and ex vivo. (a) In vivo fluorescence images display Au@mPDA@ICG biodistribution in 4T1 tumor-bearing mice at various time points post-injection (0, 0.5, 1, 2, 4, 6, 8, 12, and 24 hours), with tumor areas indicated by red circles. (b) Ex vivo fluorescence images of major organs and tumors at 24 hours post-injection. (c) Quantitative analysis of average radiant efficiency over time supports prolonged tumor retention. Ex vivo fluorescence images at 24 hours post-injection show signal intensity in major organs and tumors, quantified in (d). (e) NIR thermal imaging shows tumor regions treated with saline, Au@mPDA, or Au@mPDA@DOX under 808 nm laser irradiation, with (f) corresponding temperature changes demonstrating the photothermal response. The data are presented as mean ± SD (n = 3). *P < 0.05, ****P < 0.0001.52 Reproduced from ref.52 Copyright International journal of nanomedicine 2024. |
However, one study explored the use of membrane-wrapped nanoparticles (MWNPs) to enhance tumor-specific delivery and reduce immune recognition. These MWNPs improved systemic circulation and tumor accumulation, thereby facilitating more effective PTT. Additionally, they enabled dual tumor imaging and PTT, allowing for enhanced tumor detection and ensuring sufficient nanoparticle accumulation before laser irradiation.65 In another instance, a study investigated the application of gold nanoparticles (AuNPs) to augment the efficacy of doxorubicin (DOX) chemotherapy through PTT. The combination of DOX with AuNPs under laser irradiation leads to a synergistic decrease in breast cancer cell viability, highlighting the potential of integrating PTT with chemotherapy to improve therapeutic outcomes.15
Fluorescence Imaging-Guided PTT
Fluorescence Imaging-Guided PTT Therapy is a non-invasive strategy that combines the precise imaging capabilities of fluorescence imaging with the tumor-targeting potential of PTT. This approach seeks to enhance the precision, efficacy, and safety of breast cancer therapy by enabling real-time monitoring and ensuring that PTT is accurately targeted to the tumor site. Fluorescence imaging relies on the use of fluorescent probes or molecules that emit light at a different wavelength after being excited by a specific light source.77,78 These probes can be specifically designed to bind to tumor cells or tumor-specific markers, enabling real-time visualization of tumor location, size, and capability to treat. By visualizing the accumulation of these agents in real time, clinicians can optimize PTT delivery and ensure that it is applied accurately to the tumor area. Advantages of fluorescence imaging-guided PTT for breast cancer include high precision and accuracy, minimal side effects, non-invasive tracking of photothermal agents, enhanced tumor detection, improved efficacy of PTT, and the potential for personalized treatment. However, challenges and limitations include tissue depth, fluorophore development, thermal damage to healthy tissues, limited clinical experience, cost and complexity, and theranostic approaches.77,78
For example, one study developed an innovative optical probe, ICG-ER, designed to enhance the detection and treatment of breast cancer. This probe integrates Indocyanine Green (ICG), a NIR imaging agent, with Evans Blue (EB) and the RGD peptide to improve tumor targeting and retention. ICG-ER demonstrated high uptake by 4T1 breast cancer cells, as confirmed through flow cytometry and confocal laser scanning microscopy, indicating improved specificity towards tumor cells compared to ICG alone. Additionally, in vivo photoacoustic imaging revealed that ICG-ER accumulated at tumor sites, reaching peak concentration at approximately 42 hours post-injection. This prolonged retention is advantageous for both imaging and therapeutic applications. Following laser irradiation, the tumor site temperature in mice treated with ICG-ER rose to approximately 56 °C. This thermal elevation led to significant tumor tissue necrosis and prevented tumor recurrence during the observation period. Moreover, the ICG-ER probe shows promise as a dual-functional agent for optical imaging and PTT therapy in breast cancer. Its enhanced tumor targeting and retention capabilities, combined with effective photothermal properties, suggest the possibility for clinical use in breast cancer diagnosis and treatment.79
In another study, researchers designed a croconaine-based nanoplatform for NIR-II fluorescence imaging-guided PTT. This system allowed for precise tumor imaging and effective removal of breast cancer cells upon laser irradiation, highlighting the benefits of NIR-II fluorescence guidance in enhancing PTT accuracy. Croconaine dyes exhibit strong NIR-II fluorescence and efficient photothermal conversion, allowing for precise tumor imaging and effective PTT with minimal off-target effects. The study demonstrates that PTT not only eradicates primary tumors but also triggers an immune response that leads to immune memory, preventing tumor recurrence. This effect is mediated by the activation of dendritic cells and cytotoxic T lymphocytes, which enhance systemic antitumor immunity. These findings suggest that croconaine-based NIR-II imaging-guided PTT could serve as a hopeful strategy for both cancer treatment and long-term immune protection against tumor relapse (Figure 7).80
 |
Figure 7 (I) (a) The CR-TPE-T’s chemical structure and optimum molecular geometry. (b) Frontier molecular orbitals of CR-TPE-T were calculated using density functional theory (DFT) at the B3LYP/6-31G level. (c) The fluorescence and absorption spectra of croconaine dye nanoparticles (CR NPs) were recorded in aqueous solution with excitation at 808 nm.(d) A schematic representation of a transmission electron microscope (TEM) is provided for visualization. (II) (a) In vivo imaging and (b) quantitative analysis were performed on Colon26 tumor-bearing mice following administration of CR/DIR nanoparticles at various time points. (c) Ex vivo fluorescence images of major organs and tumors. (d) Ex vivo biodistribution analysis and quantitative measurements of dissected tumors and major organs were conducted to assess nanoparticle accumulation. (e) NIR-II fluorescence imaging and (f) corresponding quantitative analysis were carried out in 4T1 tumor-bearing mice over time to track CR NP distribution. (g) Ex vivo NIR-II fluorescence imaging and (h) quantification of major organs were performed 36 hours post-injection to evaluate systemic distribution.80 Reproduced from ref.80 Copyright BMC 2024. |
MRI Imaging-Guided PTT
MRI-guided PTT is an advanced therapeutic strategy that merges the detailed imaging capabilities of magnetic resonance imaging with the targeted treatment advantages of photothermal therapy. This combination enables accurate real-time visualization, precise tumor targeting, and dynamic adjustment of treatment parameters, ultimately improving therapeutic outcomes while reducing potential side effects. MRI-guided PTT is a promising technique that enables personalized cancer treatment, particularly for tumors that are challenging to locate or are inaccessible by traditional methods. MRI imaging is a non-invasive imaging technique that offers high-resolution images of internal tissues, offering excellent soft-tissue contrast and the ability to visualize deep tumors, including those in the breast. It can also provide information about the tumor’s size, location, shape, and functional changes, which is crucial for planning precise PTT treatment. MRI-guided PTT offers several advantages, including high spatial and temporal resolution, real-time monitoring, non-invasiveness, precise tumor localization, thermal monitoring, personalized treatment plans, and the ability to combine with other treatments.81,82 However, challenges and limitations include tumor depth penetration, photothermal agent development, treatment complexity, cost, accessibility, and the potential for tissue damage from heat.
For example, researchers developed a core-shell nanostructure combining gold nanorods with iron oxide nanoparticles. This design leverages the photothermal characteristic of gold nanorods and the MRI imaging capabilities of iron oxide. The study demonstrated that this nanoplatform effectively facilitated MRI-guided PTT, leading to significant tumor reduction in TNBC models. Assessed using a CCK-8 assay, the GNs@Fe-MOF nanocomposite exhibited good biocompatibility. Under laser irradiation, the nanocomposite effectively killed TNBC cells, demonstrating its potential for PTT. The nanocomposite provided a clear contrast in T2-weighted MRI images, both in vitro and in vivo, facilitating tumor visualization. When administered to mice with TNBC tumors, followed by laser irradiation, the GNs@Fe-MOF nanocomposite significantly inhibited tumor growth. Additionally, H&E staining revealed substantial damage to tumor tissues post-treatment, confirming the effectiveness of the photothermal therapy. This research introduces a multifunctional nanoplatform that combines the photothermal capabilities of gold nanorods with the imaging advantages of iron-based metal-organic frameworks. The GNs@Fe-MOF nanocomposite demonstrates promising potential for MRI-guided PTT therapy in treating TNBC.83
In another instance, one study introduced a novel nanocarrier by conjugating humic acid with gadolinium ions, resulting in a biocompatible platform with excellent dispersity. This nanocarrier exhibited high photothermal conversion efficiency and served as a T1-weighted MRI contrast agent. When loaded with doxorubicin, it enabled MRI-guided chemo-photothermal therapy, effectively preventing tumor growth with negligible side effects in breast cancer models.84 Additionally, researchers designed magnetically targeted phase-shifted nanoparticles that integrate chemotherapy and PTT, guided by MRI, ultrasound, and fluorescence imaging. This multifunctional approach allowed for precise tumor localization and effective treatment, demonstrating significant tumor suppression in breast cancer models.85
Raman Imaging-Guided PTT
Raman Imaging-Guided PTT is a novel treatment for breast cancer that combines Raman imaging with non-invasive photothermal therapy. PTT employs specialized agents, such as gold nanoparticles or carbon nanotubes, that absorb NIR light and convert it into localized heat. This heat elevates the temperature within tumor tissues, leading to thermal ablation and subsequent cancer cell death. These photothermal agents are typically designed to accumulate preferentially in tumor sites through the enhanced permeability and retention (EPR) effect, ensuring targeted treatment with minimal impact on surrounding healthy tissues. Raman imaging, an extension of Raman spectroscopy, provides detailed and precise visualization of molecular markers and agents.86–88 For example, one study introduced a novel imaging technique utilizing surface-enhanced resonance Raman scattering (SERRS) nanostars to accurately delineate tumor margins and detect microscopic cancerous lesions. These nanostars are composed of a star-shaped gold core, a Raman reporter molecule resonant in the NIR spectrum, and a silica coating applied through a primer-free silication method. This design enhances their stability and biocompatibility. The SERRS nanostars demonstrated a detection limit as low as 1.5 femtomolar, indicating their high sensitivity in identifying cancerous tissues. In genetically engineered mouse models of cancers, including pancreatic, breast, prostate, and sarcoma, as well as in a human sarcoma xenograft model, SERRS nanostars demonstrated precise imaging of both large tumors and microscopic disease without requiring targeting ligands. Their exceptional sensitivity enabled the detection of premalignant lesions in pancreatic and prostate tissues, underscoring their potential for early cancer diagnosis. The study highlights that the nanostars’ high sensitivity, versatility across cancer types, and biocompatible design position them as a valuable tool for accurate cancer imaging and image-guided surgery.89
However, another study explored the advances of multifunctional nanoprobes for enhanced cancer detection and therapy. Researchers synthesized nanostars with a silver core and gold shell (Ag@Au) conjugated with the Raman reporter dye DTTC, aiming to improve surface-enhanced Raman scattering (SERS) imaging and enable NIR-triggered PTT for breast cancer. The two-step coupling of DTTC to the Ag@Au nanostars significantly improved the SERS signal, providing sharp and distinct Raman peaks. Moreover, in vitro as well as in vivo SERS evaluation demonstrated clear detection of these signals in MCF-7 breast cancer cells and tumor-bearing nude mice, indicating the potential for precise tumor imaging. The Ag@Au-DTTC nanostars demonstrated excellent PCE, reaching up to 79.01% under 808 nm NIR laser irradiation. In a 14-day treatment study involving MCF-7 tumor-bearing mice, those treated with the nanostars and exposed to NIR laser showed a marked reduction in tumor volume, with near-complete tumor regression. These findings highlight the strong therapeutic potential of combining SERS imaging with photothermal therapy. Overall, the study supports Ag@Au-DTTC nanostars as promising multifunctional agents for enhanced imaging and effective NIR-triggered photothermal treatment of breast cancer.90
Photoacoustic Imaging-Guided PTT
Photoacoustic imaging-guided PTT is a hopeful strategy for breast cancer treatment that combines non-invasive imaging with targeted thermal ablation. PAI is a hybrid technique that uses pulsed laser energy to generate high-resolution images, providing deep tissue penetration, high contrast imaging, and real-time observation of therapeutic interventions. PTT uses near-infrared light to heat nanoparticles in tumors, leading to localized hyperthermia and cancer cell destruction.91,92 PAI shows a crucial role in guiding and optimizing PTT by providing high-contrast imaging, real-time monitoring, thermal feedback, and treatment evaluation. Recent advances include nanoparticle development, smart PTT systems, and integrating PTT with immunotherapy, chemotherapy, or photodynamic therapy.
For example, one study explored the employment of anti-EGFR conjugated gold nanorods (GNs) for PAI-guided NIR-PTT in treating TNBC. TNBC often overexpresses EGFR, making it a suitable target for this approach. Moreover, the anti-EGFR-GNs demonstrated enhanced tumor accumulation and enabled PAI to monitor the distribution of the nanorods within the tumor. Upon NIR laser irradiation, the targeted GNs effectively induced tumor cell apoptosis and inhibited tumor growth, showcasing the potential of PAI-guided PTT in TNBC treatment.10 Another study presents the development of HA-FeOOH/PPy nanorods, a multifunctional nanoplatform for photoacoustic imaging (PAI)-guided PTT. The nanorods, composed of iron oxyhydroxide (FeOOH) and polypyrrole (PPy), are coated with hyaluronic acid (HA) to enable active tumor targeting via CD44 receptor recognition. They reveal strong NIR absorption, allowing for high-contrast PAI for real-time tumor imaging and efficient PTT for cancer treatment upon laser irradiation. The study demonstrates their high PCE, significant tumor ablation in vitro and in vivo, and good biocompatibility with minimal side effects, creation them a capable candidate for cancer theranostics.93
For instance, one research study explores the strategy and usage of fluorescence/photoacoustic (FL/PA) imaging-guided nanomaterials for breast cancer PTT. The study focuses on multifunctional nanoplatforms that integrate fluorescence imaging for precise tumor localization and PAI for deep-tissue visualization, enabling real-time treatment monitoring. These nanomaterials, often incorporating near-infrared responsive agents like gold nanostructures, conjugated polymers, or carbon-based materials, efficiently convert NIR light into heat, inducing targeted cancer cell destruction while reducing damage to healthy tissues.94 The article highlights their enhanced PCE, excellent biocompatibility, and tumor-targeting capabilities, demonstrating their potential for improving breast cancer diagnosis and treatment through precise, image-guided PTT.
Multimodal Imaging-Guided PTT
Multimodal Imaging-Guided PTT is a precision-driven approach for breast cancer treatment that combines multiple imaging techniques to augment tumor visualization, treatment accuracy, and safety. Common modalities include PAI, MRI, CT, FI, NIR Imaging, and Ultrasound Imaging (USI). PTT uses near-infrared light to activate photothermal agents, leading to localized tumor heating and destruction.94,95 Key components of PTT include gold nanoparticles, carbon-based nanomaterials, and semiconducting polymers. Recent research focuses on multifunctional nanoparticles that enhance tumor imaging precision, improve PTT efficiency, and ensure biocompatibility. Overall, multimodal imaging-guided PTT is a promising, precision-driven approach for breast cancer treatment, enhancing tumor visualization, treatment accuracy, and minimizing damage to healthy tissues. A notable study introduces a one-pot seed-mediated growth method for synthesizing gold nanoshells on UiO-66-NH2 nanoscale metal–organic frameworks (NMOFs), achieving strong absorption in the NIR-II. By precisely tuning the ratio of formaldehyde to formic acid and regulating the reaction temperature, the researchers guided the formation of gold nanoshells along a controlled diffusion-driven growth pathway, resulting in uniform and well-defined nanostructures. The resulting gold nanoshells (AuNSs) exhibit a broad absorption peak beyond 1300 nm and an impressive PCE of 74.0%. These properties make them highly effective for multimodal imaging techniques, including PA and CT, as well as PTT for breast cancer. Upon NIR laser irradiation, the AuNSs effectively ablated breast cancer tumors in vivo, showcasing their potential as a multifunctional theranostic agent. Both in vitro and in vivo studies proved significant tumor suppression, underscoring the potential of these gold nanoshells as a multifunctional platform for cancer detection and treatment (Figure 8).95
 |
Figure 8 (I) Characterization of UiO-66-NH2-Based Nanocomposites. (a) PXRD patterns of synthesized UiO-66-NH2, Au, and UGs compared with the simulated UiO-66-NH2 structure, confirming crystallinity and successful synthesis. (b) Hydrodynamic size distributions of UiO-66-NH2, UGs, and UGs@PEG, indicating size changes upon nanoparticle modification and PEGylation. (c) Zeta potential measurements for UiO-66-NH2, UGs, and UGs@PEG, demonstrating surface charge alterations at each synthesis stage. (d) TEM image of UGs@PEG, showing the nanoparticle morphology and uniform coating. (e) Elemental mapping of UGs@PEG, confirming the presence and distribution of constituent elements. (II) In Vivo and In Vitro Imaging and Photothermal Evaluation. (a) In vivo photoacoustic imaging (PAI) of tumor-bearing mice and internal organs at various time points (0, 3, 6, 9, 12, 24, and 36 h) post-intravenous injection of UGs@PEG, under 1064 nm laser excitation. (b) Quantitative analysis of PAI signal intensity over time, indicating tumor accumulation. (c) In vitro CT images of UGs@PEG at different concentrations (0, 1.5, 3, 6, 12, and 24 mg/mL), demonstrating dose-dependent contrast enhancement. (d) In vivo CT imaging 24 hours post-injection, confirming accumulation in tumor regions. (e) Comparison of CT values before and after intravenous (i.v.) and intratumoral (i.t.) injection of UGs@PEG in tumor-bearing mice. (f) Representative photothermal images of mice treated with PBS and UGs@PEG under 1064 nm laser irradiation for 10 minutes, showing localized temperature increase in treated tumors. (g) Heating curves of tumor regions following treatment, comparing temperature elevation in mice administered UGs@PEG versus PBS.96 Reproduced from ref.96 Copyright BMC 2023. |
Another research group explores the use of rare-earth nanoparticles (RENPs) as a multifunctional platform for multimodal imaging and PTT. RENPs possess unique optical and magnetic properties, enabling their application in FI, PAI, CT, and MRI for comprehensive tumor diagnosis and treatment monitoring. These nanoparticles exhibit strong near-infrared absorption, facilitating efficient photothermal conversion for targeted tumor ablation upon laser irradiation. The study demonstrates their high biocompatibility, deep tissue imaging capabilities, and effective tumor suppression in vitro and in vivo, highlighting RENPs as a promising nanoplatform for specific and non-invasive cancer theranostics.97 In another study, a polypyrrole (PPy)-based nanoplatform is presented for multimodal imaging-guided therapy, integrating PAI, FI, and PTT for enhanced cancer diagnosis and treatment. PPy, known for its excellent near-infrared absorption and photothermal conversion efficiency, enables real-time tumor visualization and targeted ablation under laser irradiation. The study demonstrates that these nanoplatforms can be further altered with tumor-targeting ligands or biocompatible coatings to enhance specificity and biostability. In vitro and in vivo experiments confirm high photothermal efficacy, effective tumor suppression, and minimal toxicity, positioning PPy-based nanomaterials as a promising candidate for precise and non-invasive cancer theranostics.96
Limitations and Future Prospects
PTT has shown promise in treating breast cancer, but several challenges remain. These include limited tissue penetration, tumor heterogeneity, toxicity of nanomaterials, heat-induced damage to healthy tissues, and challenges in systemic delivery (Scheme 2). The use of conventional NIR light is particularly challenging due to its restricted penetration depth. Tumor heterogeneity also poses challenges in the uniform distribution of photothermal agents within the tumor. Nanomaterials used in PTT, such as gold nanoparticles, carbon nanotubes, or copper-based compounds, are not without risks, and their biocompatibility, biodegradability, and clearance mechanisms need further optimization. Excessive heating can cause unintended damage to healthy tissues surrounding the tumor, and precise control over temperature distribution is essential to avoid skin burns, inflammation, or damage to critical organs. Systemic delivery of PTT is often obstructed by biological barriers like the blood-brain barrier or poor tumor vasculature, which can lead to insufficient accumulation of therapeutic agents at the target site. Combining PTT with other treatments presents both opportunities and challenges, as tumors may respond differently to these combinations.98,99
 |
Scheme 2 The schematic diagram illustrates limitations and challenges of breast cancer photothermal and combinatory therapy. |
One major challenge in the clinical use of PTAs is their photostability and dispersibility. IR dyes like ICG are commonly used PTAs but face issues such as poor photostability and rapid photobleaching, adversely affecting therapeutic outcomes. Enhancements through chemical modifications or hybridization with scaffolds are essential for future research. MOFs and zeolitic imidazolate frameworks (ZIFs) present potential as PTA carriers, yet their effective application is hindered by challenges in dispersibility and maintaining structural integrity, which impacts biodistribution and photothermal efficiency. Future investigations should emphasize surface engineering and rational design of composites to improve stability and performance, facilitating the transition from preclinical studies to effective cancer therapies.100,101
Despite significant advances, clinical treatment of breast cancer still faces multiple challenges that limit therapeutic efficacy. Conventional therapies such as surgery, chemotherapy, radiotherapy, and targeted agents often encounter issues of drug resistance, tumor heterogeneity, and limited penetration into metastatic sites, particularly in the brain, bone, and liver. For PTT, although preclinical studies show precise tumor ablation and minimal invasiveness, translation to the clinic is hindered by inadequate understanding of heat-induced molecular responses, such as heat shock protein activation, immunogenic cell death, and vascular normalization, as well as the difficulty in delivering photothermal agents efficiently to deep or dispersed tumors. Combination therapies, while promising for overcoming resistance and enhancing efficacy, introduce additional complexities, including potential systemic toxicity, unpredictable synergistic effects, and challenges in optimizing timing, dosing, and sequence of multiple modalities. Furthermore, the lack of standardized protocols and reliable imaging guidance for real-time monitoring of PTT limits its reproducibility and clinical adoption. Addressing these issues requires mechanistic studies, improved nanomaterial design, precise delivery strategies, and rigorous clinical trials to ensure safety, efficacy, and practical feasibility in diverse patient populations.102–104
Limited Tissue Penetration of NIR Light
Most photothermal agents rely on NIR light, which can only penetrate a few centimeters into tissue. This limits the effectiveness of treatment for deep-seated breast tumors and often necessitates invasive methods such as fiber optics to achieve deeper penetration. High-intensity irradiation may result in unintended damage to adjacent healthy tissues. Heat dissipation in surrounding areas can lead to inflammation and side effects. Specifically, NIR-I light (700–900 nm) penetrates only a few millimeters to centimeters into biological tissues due to absorption and scattering by water, hemoglobin, and lipids, making it difficult to treat deep-seated tumors effectively.57,105–108 The NIR-II window offers improved penetration and reduced scattering, but still faces challenges in reaching deeper tumors without invasive procedures or specialized light delivery systems. PTT using NIR light generates localized heat, which can unintentionally damage surrounding healthy tissue if not precisely targeted. If nanoparticles used in NIR therapy accumulate in non-tumor tissues, exposure to NIR light can cause unwanted hyperthermia and toxicity. Prolonged or high-intensity NIR exposure can also lead to burns or inflammation in the overlying skin and adjacent tissues.109,110
NIR-II Light-Excited PTT
NIR-II light-excited PTT has garnered attention due to its deeper tissue penetration, lower autofluorescence, and diminished scattering compared to NIR-I. However, several limitations hinder its broad clinical adoption for breast cancer therapy. These include the limited availability of clinically approved NIR-II photothermal agents, complex synthesis processes, potential toxicity, challenges in deep tissue heating, suboptimal tumor accumulation of NIR-II agents, heat-induced damage to surrounding normal tissues, difficulties in thermoregulation, limited availability of NIR-II imaging systems, and hurdles in clinical translation and regulatory approval. Potential solutions involve addressing limited penetration depth and uneven nanoparticle distribution through smart nanocarriers with controlled release and tumor microenvironment responsiveness. Approaches such as surface modification with PEG, biomimetic coatings, or cell membrane cloaking aim to extend circulation time and enhance targeting. Additionally, AI-guided real-time temperature monitoring may enable more precise thermal control. Large-scale clinical trials and the development of biocompatible NIR-II agents are crucial for successful clinical translation. Future directions include multiplexed therapies, advanced delivery systems, and integrated real-time monitoring technologies.102,111
Low-Temperature PTT
Low-temperature photothermal therapy (LPTT) is a mild hyperthermia-based treatment designed to induce apoptosis rather than necrosis, thereby minimizing damage to healthy tissues. However, it faces multiple limitations, including incomplete tumor ablation, heterogeneous tumor responses, therapy resistance mediated by heat shock proteins (HSPs), limited tissue penetration, suboptimal tumor accumulation of photothermal agents, and reduced immune activation compared to high-temperature PTT. It also demonstrates limited efficacy against breast cancer stem cells (BCSCs). Real-time temperature monitoring remains a challenge, though AI-guided feedback systems offer a promising solution. Clinical translation is further hindered by regulatory challenges, high costs of nanoparticles and laser systems, and a lack of large-scale trials. Future strategies include combining LPTT with immunotherapy, chemotherapy, and HSP inhibitors; incorporating AI-guided heating systems; and designing advanced nanocarriers for deeper penetration and prolonged circulation.112,113
Immunosuppressive Tumor Microenvironment (TME)
TME can suppress immune responses, reducing the efficacy of PTT and immune-based combination therapies. PTT-induced hyperthermia alone is often insufficient to reverse the immunosuppressive nature of certain breast tumors. Many subtypes, particularly hormone receptor-positive (HR+) cancers, exhibit low levels of tumor-infiltrating lymphocytes (TILs) and low mutational burdens, making them less responsive to immunotherapies such as checkpoint inhibitors. The TME also reduces the effectiveness of CAR-T cell therapy, immune checkpoint blockade, and cancer vaccines by impairing immune cell function. Furthermore, tumor cells may adapt by upregulating alternative immune checkpoint pathways (eg, TIM-3, LAG-3) or altering antigen presentation mechanisms.114,115
Targeting
PTT targeting strategies aim to improve nanoparticle accumulation in tumors, reduce off-target effects, and enhance therapeutic efficacy. However, several biological and technical challenges persist, including limited tumor accumulation due to biological barriers, insufficient specificity of targeting mechanisms, antibody-based targeting complications, rapid nanoparticle clearance, off-target accumulation and associated heating, tumor heterogeneity, and clinical translation barriers. Potential solutions involve tumor-penetrating peptides, enzyme-responsive nanocarriers, dual- or multi-targeting approaches, real-time biomarker monitoring via liquid biopsies, and multimodal therapies. Future directions emphasize the development of biodegradable and biocompatible PTT agents and the need for large-scale clinical trials.116,117
Tumor Heterogeneity and Resistance
Breast cancers, especially TNBC, are characterized by high genetic and phenotypic heterogeneity, leading to resistance to PTT monotherapy. Sub-lethal heat exposure may allow some cancer cells to survive and develop resistance. Contributing factors include genetic and epigenetic variability, clonal evolution, cancer stem cells (CSCs), phenotypic plasticity, and microenvironment-induced resistance. These mechanisms limit the effectiveness of chemotherapy, targeted therapy, immunotherapy, and hormone therapy. Strategies to address these challenges include combination therapies, targeting CSCs, overcoming epithelial-mesenchymal transition (EMT), and employing precision medicine and personalized approaches. Modulating the TME also holds promise for improving outcomes and reducing recurrence and metastasis.45,118
Limited Clinical Translation and Delivery Challenges
Although many PTT-based nanomaterials have shown promising preclinical results, few have received FDA approval due to worries over lasting safety and biodegradability. Large-scale, standardized clinical trials are desired to introduce efficacy and safety. Additionally, effective delivery of photothermal agents remains a significant hurdle, as the augmented EPR effect is often inconsistent in human tumors. Off-target accumulation can lead to systemic toxicity.119,120
To overcome these restrictions and fully appreciate the potential of PTT and combination therapies, continuous research and development are essential. Future advancements should focus on developing nanomaterials with deeper tissue penetration, tumor-specific accumulation, and minimal toxicity. Multifunctional nanoparticles capable of integrating PTT with drug delivery, imaging, and immune modulation may revolutionize breast cancer treatment. Innovations in light delivery systems, such as optical fibers, endoscopes, and LEDs, will enhance light penetration and uniform heat distribution in tumors. Researchers are also exploring multiplexed laser systems and thermally responsive light sources to improve heat control and minimize damage to healthy tissues. Clinical translation will require integration with standard therapies and collaboration among oncologists, nanotechnologists, and regulatory bodies to facilitate adoption into mainstream clinical practice.121–123
Conclusion
PTT is a promising non-invasive method for breast cancer treatment, targeting and ablating tumor cells using light-activated nanoparticles. However, challenges such as limited tissue penetration and heterogeneity in tumor responses persist. Combinatory therapies, which integrate PTT with conventional treatments like chemotherapy, radiation, immunotherapy, and gene therapy, are gaining attention. This approach can enhance tumor destruction, improve drug delivery, and activate the immune system. It can also address drug resistance, tumor heterogeneity, and treatment relapse. The integration of nanotechnology with PTT opens avenues for developing multifunctional nanoparticles that deliver heat, drugs, and genetic material to cancer cells, enabling highly personalized treatment strategies. As the field progresses, focus will shift toward optimizing nanoparticle design, improving light penetration, and fine-tuning synergistic combinations of therapies. Clinical trials and preclinical studies will be essential in determining optimal parameters and safety profiles. Image guidance and a systematic comparison of nanoengineering strategies are essential to optimize PTT-based platforms for precise, effective, and clinically translatable breast cancer therapy. In summary, photothermal and combinatory therapies offer the potential for more potent, tailored, and less harmful treatment alternatives, making them an intriguing new frontier in the fight against breast cancer. These strategies hold promise for improving patient outcomes and offering hope for more individualized and efficient breast cancer treatments shortly, even though further research is obligatory to realize their therapeutic potential fully. To fully realize their therapeutic potential, rigorous experimental studies are still required to clarify molecular mechanisms, optimize dosing parameters, and evaluate long-term safety in relevant preclinical models. Moreover, carefully designed clinical trials are essential to validate efficacy and translate these strategies into individualized breast cancer treatments.
Acknowledgments
Mifang Li and Ikram Hasan contributed equally to this work. The authors are grateful to the Science and Technology Plan Project of Shenzhen (No. JCYJ20220530160017037, JCYJ20240813114628038), and Guangdong Basic and Applied Basic Research Foundation (2024A1515220001), Talent Development Program of Longgang Central Hospital of Shenzhen, and Shenzhen Key Laboratory of Advanced Functional Carbon Materials Research and Comprehensive Application (ZDSYS20220527171407017). This work was supported by the Science and Technology Project in Guangzhou (grant number 202102070001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sagnik N, Mitra O, Tripathi G. et al. Nanomaterials-assisted photothermal therapy for breast cancer: state-of-the-art advances and future perspectives. Photodiagn Photodyn Ther. 2024;45:103959. doi:10.1016/j.pdpdt.2023.103959
2. Yao X, Rao Y, Hu J, et al. Nanoparticle-based photothermal therapy for breast cancer noninvasive treatment. Advanced Materials. 2025;37:e2305140. doi:10.1002/adma.202305140
3. Jingjun S, Zhao H, Xu W, Jiang GQ, et al. Recent advances in photothermal therapy-based multifunctional nanoplatforms for breast cancer. Frontiers in Chemistry. 2022;10:1024. doi:10.3389/fchem.2022.1024177
4. Ruoxi H, Binghe X, et al. Breast cancer: an up-to-date review and future perspectives. Cancer Commun. 2022;42(10):913–936. doi:10.1002/cac2.12358
5. Nadia H, Gnant M, et al. Breast cancer. Lancet. 2017;389(10074):1134–1150. doi:10.1016/S0140-6736(16)31891-8
6. Yuxing S, Chen Z, Hao P, et al. Boosting photothermal-assisted photocatalytic water/seawater splitting into hydrogen based on greenhouse-induced photothermal effect. Journal of Colloid and Interface Science. 2024;653:1339–1347. doi:10.1016/j.jcis.2023.09.170
7. Junlong G, Sun C, Liu J, et al. Biocompatible conjugated polymer nanoparticles for efficient photothermal tumor therapy. Small. 2015;11(13):1603–1610. doi:10.1002/smll.201402092
8. Shufan D, Hu Y, Zhao Y, et al. Nanomaterials for photothermal cancer therapy. RSC Adv. 2023;13(21):3–14460. doi:10.1039/d3ra02620e
9. Giaquinto Angela N, Sung H, Newman LA, et al. Breast cancer statistics 2024. CA: a Cancer Journal for Clinicians. 2024;74(6):477–495. doi:10.3322/caac.21863
10. Meihua Z, Kim HS, Jin T, et al. Near-infrared photothermal therapy using anti-EGFR-gold nanorod conjugates for triple-negative breast cancer. Oncotarget. 2017;8(49):6–86575. doi:10.18632/oncotarget.21243
11. Zou L, Wang H, He B, et al. Current Approaches of Photothermal Therapy in Treating Cancer Metastasis with Nanotherapeutics. Theranostics. 2016;6(6):762–772. doi:10.7150/thno.14988
12. Marta O, Weersink RA, Wilson BC, et al. Photodynamic and photothermal therapies: synergy opportunities for nanomedicine. ACS nano. 2023;17(9):7979–8003. doi:10.1021/acsnano.3c00891
13. Tatsuki O, Kato S, Hatakeyama Y, et al. Photothermal therapy of tumors in lymph nodes using gold nanorods and near-infrared laser light. J Control Release. 2013;172(3):879–884. doi:10.1016/j.jconrel.2013.10.014
14. Daisuke M, Adewale O, Horie S, et al. Treatment of tumor in lymph nodes using near-infrared laser light-activated thermosensitive liposome-encapsulated doxorubicin and gold nanorods. Journal of Biophotonics. 2017;10(12):1676–1682. doi:10.1002/jbio.201600241
15. Mendes R, Pedrosa P, Lima JC, Fernandes AR, Baptista PV. Photothermal enhancement of chemotherapy in breast cancer by visible irradiation of Gold Nanoparticles. Scientific Reports. 2017;7(1):2. doi:10.1038/s41598-017-11491-8
16. Qinglian H, He C, Lu Z, et al. Engineering of small molecular organic nanoparticles for mitochondria-targeted mild photothermal therapy of malignant breast cancers. Biomater. Sci. 2022;10(20):6023. doi:10.1039/d2bm01239a
17. Sung JH, Verwilst P, Sharma A, et al. Organic molecule-based photothermal agents: an expanding photothermal therapy universe. Chem. Soc. Rev. 2018;47(7):2280–2297. doi:10.1039/c7cs00522a
18. Shuang L, Pan X, Liu H, et al. Two-dimensional nanomaterials for photothermal therapy. angewandte chemie. Angewandte Chemie. 2020;59(15):5890–5900. doi:10.1002/anie.201911477
19. Natanael F, Rodrigues CF, Moreira AF, et al. Overview of the application of inorganic nanomaterials in cancer photothermal therapy. Biomater. Sci. 2020;8(11):2990–3020. doi:10.1039/d0bm00222d
20. Xiaoliang Q, Xiang Y, Cai E, et al. Inorganic–organic hybrid nanomaterials for photothermal antibacterial therapy. Coordination Chemistry Reviews. 2023;496:215426. doi:10.1016/j.ccr.2023.215426
21. Zhang L, Forgham H, Huang X, et al. All-in-one inorganic nanoagents for near-infrared-II photothermal-based cancer theranostics. Mater Today Adv. 2022;14:100226. ISSN 2590-0498.doi:10.1016/j.mtadv.2022.100226
22. Yan Z, Xu C, Yang X, et al. Photoactivatable protherapeutic nanomedicine for cancer. Advanced Materials. 2020;32(34):e2002661. doi:10.1002/adma.202002661
23. Jingchao L, Kanyi P, et al. Development of organic semiconducting materials for deep-tissue optical imaging, phototherapy, and photoactivation. Chem. Soc. Rev. 2019;48(1):38–71. doi:10.1039/c8cs00001h
24. Zhang M, Kim HS, Jin T, Woo J, Piao YJ, Moon WK. Near infrared photothermal therapy using anti-EGFR-gold nanorod conjugates for triple negative breast cancer. Oncotarget. 2017;8(49):86566–86575. doi:10.18632/oncotarget.21243
25. Shakil MS, Hasan MA, Sarker SR. Iron oxide nanoparticles for breast cancer theranostics. Curr Drug Metab. 2019;20(6):446–456. doi:10.2174/1389200220666181122105043
26. Li B, Zhou Q, Wang H, et al. Mitochondria-targeted magnetic gold nanoheterostructure for multi-modal imaging guided photothermal and photodynamic therapy of triple-negative breast cancer. Chem Eng J. 2021;403:126364. doi:10.1016/j.cej.2020.126364
27. Zhao W-B, Chen -D-D, Liu -K-K, et al. Near-infrared I/II emission and absorption carbon dots via constructing localized excited/charge transfer state for multiphoton imaging and photothermal therapy. Chem Eng J. 2023;452:139231. doi:10.1016/j.cej.2022.139231
28. Majid S, Hasan A, Nanakali NM, et al. Combined chemo-magnetic field-photothermal breast cancer therapy based on porous magnetite nanospheres. Scientific Reports. 2020;10(1). doi:10.1038/s41598-020-62429-6
29. Jinghan S, Sun H, Meng Q, et al. Bioinspired nanoparticles with nir‐controlled drug release for synergetic chemophotothermal therapy of metastatic breast cancer. Advanced Functional Materials. 2016;26. doi:10.1002/adfm.201603381.
30. Yue W, Chang L, Gao H, Yu C, Gao Y, Peng Q. Nanomaterials-based advanced systems for photothermal/photodynamic therapy of oral cancer. Eur. J. Med. Chem. 2024;272:116508. doi:10.1016/j.ejmech.2024.116508
31. Niloufar C, Avizheh S, Karimifard SA. Recent advances in efficacy of using doxorubicin gold nanoparticles for chemo-, radio-, photothermal, and photodynamic therapy. Curr Drug Delivery. 2022;19(7):745–762. doi:10.2174/1567201818666210707110742
32. Neha T, Arya RKK, Bisht D, et al. Mechanism and potentialities of photothermal and photodynamic therapy of transition metal dichalcogenides (TMDCs) against cancer. Luminescence: the Journal of Biological and Chemical Luminescence. 2024;39(5):e4770. doi:10.1002/bio.4770
33. Yang S, Palanikumar L, Jeong S, et al. Synergistic effect of photothermal therapy and chemotherapy using camptothecin-conjugated gold nanorods, Part. Part. Syst. Charact. 2018;35:1700307. doi:10.1002/ppsc.201700307
34. Peng X, Liang F, et al. Nanomaterial-Based Tumor Photothermal Immunotherapy. Int J Nanomed. doi:10.2147/IJN.S249252
35. Hang L, Li H, Li M, et al. Lactoferrin docking NIR-II cyanine dye as a potentiated phototheranostic for synchronous multimodal bioimaging and tumor photo-immunotherapy. Theranostics. 2024;14(17):6671–6691. doi:10.7150/thno.102663
36. Ghosh A, Rajdev B, Parihar N, et al. Bio-nanoconjugates of lithocholic acid/IR 780 for ROS-mediated apoptosis and optoacoustic imaging applications in breast cancer. Colloids Surf. B. 2023;221:113023. doi:10.1016/j.colsurfb.2022.113023
37. Wang X, Liu X, Guo Y, et al. The remarkable anti-breast cancer efficacy and anti-metastasis by multifunctional nanoparticles co-loading squamocin, R848 and IR 780. Int J Nanomed. 2024;19:4679–4699. doi:10.2147/IJN.S448860
38. Zhou Y, Kou J, Zhang Y, et al. Magnetic-guided nanocarriers for ionizing/non-ionizing radiation synergistic treatment against triple-negative breast cancer. Biomedical Engineering Online. 2024;23(1). doi:10.1186/s12938-024-01263-7
39. Guo B, Huang Z, Shi Q, et al. Organic small molecule-based photothermal agents with molecular rotors for malignant breast cancer therapy. Advanced Functional Materials. 2019;30(5). doi:10.1002/adfm.201907093
40. Lina S, Zuo C, Liu X, et al. Combined photothermal therapy and lycium barbarum polysaccharide for topical administration to improve the efficacy of doxorubicin in the treatment of breast cancer. Pharmaceutics. 2022;14(12). doi:10.3390/pharmaceutics14122677
41. Xu Y, Wang C, Shen F, et al. Lipid-coated CaCO 3 nanoparticles as a versatile ph-responsive drug delivery platform to enable combined chemotherapy of breast cancer. ACS Appl Bio Mater. 2022;5:1194–1201. doi:10.1021/acsabm.1c01234
42. Wang J, Wu X, Shen P, et al. Applications of inorganic nanomaterials in photothermal therapy based on combinational cancer treatment. Int J Nanomed. 2020;15:1903–1914. doi:10.2147/IJN.S239751
43. Ding X, Liu J, Li J, et al. Polydopamine coated manganese oxide nanoparticles with ultrahigh relaxivity as nanotheranostic agents for magnetic resonance imaging guided synergetic chemo-/photothermal therapy. Chem Sci. 2016;7:6695–6700. doi:10.1039/C6SC01320A
44. Tang N, Shi L, Yu Z, et al. Gamabufotalin, a major derivative of bufadienolide, inhibits VEGF- induced angiogenesis by suppressing VEGFR-2 signaling pathway. Oncotarget. 2016;7:3533. doi:10.18632/oncotarget.6514
45. Li Y, Zhang R, Xu Z, Wang Z. Advances in nanoliposomes for the diagnosis and treatment of liver cancer. Int J Nanomed. 2022;17:909–925. doi:10.2147/IJN.S349426
46. Pal K, Mahato P, Singh S, Roy P. NIR-responsive 5-Fluorouracil delivery using polydopamine-coated polygonal CuS nanoplates for synergistic chemo-photothermal therapy on breast cancer. J. Drug Deliv. Sci. Technol. 2023;80:104092. doi:10.1016/j.jddst.2022.104092
47. Min Z, Zhang H, Dai M, et al. A PTT-induced feed-back carbon nanosystem for enhanced breast cancer therapy by extracellular matrix remodeling. Nano Letters. 2025;25(8):3180–3190. doi:10.1021/acs.nanolett.4c05625
48. Hou Y-K, Zhang Z-J, Li R-T, et al. Remodeling the tumor microenvironment with core–shell nanosensitizer featuring dual-modal imaging and multimodal therapy for breast cancer. ACS Appl. Mater. Interfaces. 2023;15:2602–2616. doi:10.1021/acsami.2c17691
49. Guan X, Zeng N, Zhao Y, et al. dual-modality imaging-guided manganese-based nanotransformer for enhanced gas-photothermal therapy combined immunotherapeutic strategy against triple-negative breast cancer. Small. 2024;20(22):e2307961. doi:10.1002/smll.202307961
50. Mu M, Chen B, Li H, et al. Augmented the sensitivity of photothermal-ferroptosis therapy in triple-negative breast cancer through mitochondria-targeted nanoreactor. Journal of Controlled Release. 2024;375:733–744. doi:10.1016/j.jconrel.2024.09.042
51. Ali A, Rezaei F, Attari F, Ashkevarian S. Treatment of breast cancer in vivo by dual photodynamic and photothermal approaches with the aid of curcumin photosensitizer and magnetic nanoparticles. Scientific Reports. 2020;10(1):6. doi:10.1038/s41598-020-78241-1
52. Junzi C, Xiang Y, Bao R, et al. Combined photothermal chemotherapy for effective treatment against breast cancer in mice model. Int J Nanomed. 9973. doi:10.2147/IJN.S473052
53. Shipeng N, Shangguan P, Zhu X, et al. Pyridinium rotor strategy toward a robust photothermal agent for sting activation and multimodal image-guided immunotherapy for triple-negative breast cancer. J Am Chem Soc. 2025;147(9):7433–7444. doi:10.1021/jacs.4c15534
54. Dehariya D, Tarafdar A, Pebam M, Sankaranarayanan SA, Khatun S, Rengan AK. Gold nanocages co-assembled with Spinacia oleracea extract combined photothermal/photodynamic therapy in 4T1 breast cancer cell line. Biomed. Mater. 2025;20(2):025014. doi:10.1088/1748-605X/ada83e
55. Jiaqiang X, Wu M, Chen J, et al. Cancer-erythrocyte hybrid membrane-camouflaged magnetic nanoparticles with enhanced photothermal-immunotherapy for ovarian cancer. ACS nano. 2021;15(12):19756–19770. doi:10.1021/acsnano.1c07180
56. Jiawen H, Song R, Xiao F, Wang M, Wen L, Cu3P/1-MT nanocomposites potentiated photothermal-immunotherapy. Int J Nanomed. 3021:
57. Zhuang B, Chen T, Huang Y, Xiao Z, Jin Y, Chemo-photothermal immunotherapy for eradication of orthotopic tumors and inhibition of metastasis by intratumoral injection of polydopamine versatile hydrogels. Acta Pharmaceutica Sinica B. 2022;12(3):1447–1459. doi:10.1016/j.apsb.2021.09.001
58. Zhe W, Guo B, Middha E, et al. Microfluidics-prepared uniform conjugated polymer nanoparticles for photo-triggered immune microenvironment modulation and cancer therapy. ACS Applied Materials & Interfaces. 2019;11(12):11167–11176. doi:10.1021/acsami.8b22579
59. Sidi Z, Wang X, Chen X, et al. An on-demand oxygen nano-vehicle sensitizing protein and nucleic acid drug augment immunotherapy. Advanced Materials. 2025;37(9):e2409378. doi:10.1002/adma.202409378
60. Mengyuan Y, et al. Ultrasmall zirconium carbide nanodots for synergistic photothermal-radiotherapy of glioma. Nanoscale. 2022;14(40):5–14949. doi:10.1039/d2nr04239h
61. Pranjali Y, et al. Biodegradable protein-stabilized inorganic nanoassemblies for photothermal radiotherapy of hepatoma cells. ACS Omega. 2022;7(10):8937. doi:10.1021/acsomega.1c07324
62. Min W, Huang Y, Huang X, Wang F, Wei X, Copolymerized carbon nitride nanoparticles for near-infrared II photoacoustic-guided synergistic photothermal/radiotherapy. Frontiers in Chemistry. 2023;11:559. doi:10.3389/fchem.2023.1124559
63. Mohammadreza G, Rashidzadeh H, Mohammadi A, et al. Photothermal and radiotherapy with alginate-coated gold nanoparticles for breast cancer treatment. Scientific Reports. 2024;14(1):9. doi:10.1038/s41598-024-60396-w
64. Shan J, Liu Z, Tian Y, et al. A comprehensive evaluation of zrc nanoparticles in combined photothermal and radiation therapy for treatment of triple-negative breast cancer. Frontiers in Oncology. 8013:52. doi:10.3389/fonc.2021.801352
65. Yuan-Wen L, Chen T-L, Shih Y-RV, et al. Adjunctive traditional Chinese medicine therapy improves survival in patients with advanced breast cancer: a population-based study. Cancer. 2014;120(9):1338–1344. doi:10.1002/cncr.28579
66. Leon-Ferre RA, Goetz MP, et al. Advances in systemic therapies for triple-negative breast cancer. BMJ. 2023;381:e071674. doi:10.1136/bmj-2022-071674
67. Yun L, Zhang H, Merkher Y, et al. Recent advances in therapeutic strategies for triple-negative breast cancer. Journal of Hematology & Oncology. 15(1):121. doi:10.1186/s13045-022-01341-0
68. Fan Y, Xiao Y, Ding JH, et al. Ferroptosis heterogeneity in triple-negative breast cancer reveals an innovative immunotherapy combination strategy. Cell Metabolism. 2023;35(1):84–100.e8. doi:10.1016/j.cmet.2022.09.021
69. Xiaohong L, He T, Tang R, et al. Biomimetic nanoprobe-augmented triple therapy with photothermal, sonodynamic, and checkpoint blockade inhibits tumor growth and metastasis. J Nanobiotechnol. 2022;20(1):80. doi:10.1186/s12951-022-01287-y
70. Rong-Tian L, Zhu Y-D, Li W-Y, et al. Synergistic photothermal-photodynamic-chemotherapy toward breast cancer based on a liposome-coated core-shell AuNS@NMOFs nanocomposite encapsulated with gambogic acid. J Nanobiotechnol. 2022;20(1):212. doi:10.1186/s12951-022-01427-4
71. Xiong W, Cheng Z, Chen H, et al. Biomimetic tumor cell membrane-encapsulated nanoparticles combine nir-ii photothermal therapy and chemotherapy for enhanced immunotherapy in triple-negative breast cancer. Adv. Funct. Mater. 2024;34:2410841. doi:10.1002/adfm.202410841
72. Kong H, Tang Y, Hao X, et al. Self-assembly of h2s-generating photosensitizer for gas-assisted synergistic photothermal therapy. Small. 2025;21(13):e2411242. doi:10.1002/smll.202411242
73. Sun P, Qu F, Zhang C, et al. NIR-II excitation phototheranostic platform for synergistic photothermal therapy/chemotherapy/chemodynamic therapy of breast cancer bone metastases. Advanced Science. 2022;9(33):e2204718. doi:10.1002/advs.202204718
74. Chen Z, Zheng X, Zhao J, Tang J, Hu L, Wang S. Glucose oxidase-loaded colloidal stable WS2 nanobowls for combined starvation/photothermal therapy of colorectal tumors. International Journal of Pharmaceutics. 2023;636:122848. doi:10.1016/j.ijpharm.2023.122848
75. Zhang Y, Jiang S, Lin J, Huang P. Antineoplastic enzyme as drug carrier with activatable catalytic activity for efficient combined therapy. Angewandte Chemie. 2022;61(41):e202208583. doi:10.1002/anie.202208583
76. Chunyue W, Wang X, Tian Y, et al. CsxWO3@nbs as a multi-image guided photothermal/photodynamic combination therapy platform for the treatment of hepatocellular carcinoma. Int J Nanomed. 2024;19:5–13389. doi:10.2147/IJN.S484694
77. Wenqi W, Zhang X, Ni X, et al. Semiconducting polymer nanoparticles for NIR-II fluorescence imaging-guided photothermal/thermodynamic combination therapy. Biomater. Sci. 2022;10(3):846–853. doi:10.1039/d1bm01646f
78. Hangqi L, Gao S, et al. Recent advances in fluorescence imaging-guided photothermal therapy and photodynamic therapy for cancer: from near-infrared I to near-infrared-II. J Control Release. 2023;362:425–445. doi:10.1016/j.jconrel.2023.08.056
79. Weng Y, Wang ZJ, Guo TY, et al. ICG-ER: a new probe for photoimaging and photothermal therapy for breast cancer. American Journal of Translational Research. 1991;14(3).
80. Yafang D, Wang H, Zhang X, et al. Croconaine-based NIR-II fluorescence imaging-guided tumor photothermal therapy induces long-term antitumor immune memory. J Nanobiotechnol. 2024;22(1):481. doi:10.1186/s12951-024-02695-y
81. Yupeng S, Zhou M, Zhang Y, et al. MRI-guided dual-responsive anti-tumor nanostructures for synergistic chemo-photothermal therapy and chemodynamic therapy. Acta biomaterialia. 2023;158:571–582. doi:10.1016/j.actbio.2022.12.053
82. Liang D, Chen W Zhong J, et al. Dopamine multivalent-modified polyaspartic acid for MRI-guided near-infrared photothermal therapy. Regenerative Biomaterials. 2023;10:rbad022. doi:10.1093/rb/rbad022
83. He J, Zhang H. Abstract PS14-28: core−shell structured gold nanorods@iron-based metal-organic framework for magnetic resonance imaging guided photothermal therapy in triple-negative breast cancer. Cancer Research. 2021;81(4_Supplement):S14–28. doi:10.1158/1538-7445.sabcs20-ps14-28
84. Chuan KJ, Li Y, Ma W, et al. A novel vector for magnetic resonance imaging-guided chemo-photothermal therapy for cancer. Frontiers in Oncology. 2022. doi:10.3389/fonc.2022.972082
85. Long W, Chen S, Zhu Y, et al. Triple-modal imaging-guided chemo-photothermal synergistic therapy for breast cancer with magnetically targeted phase-shifted nanoparticles. ACS Applied Materials & Interfaces. 2018;10(49):42102–42114. doi:10.1021/acsami.8b16323
86. Sihang Z, et al. Au@cus nanoshells for surface-enhanced raman scattering image-guided tumor photothermal therapy with accelerated hepatobiliary excretion. Pharmaceutics. 2024;16(8):1089. doi:10.3390/pharmaceutics16081089
87. Jinping W, Sun J, Wang Y, et al. Gold nanoframeworks with mesopores for raman-photoacoustic imaging and photo-chemo tumor therapy in the second near-infrared biowindow. Advanced Functional Materials. 2020;30(9):1908825. doi:10.1002/adfm.201908825
88. Suchetan P, Ray A, Andreou C, et al. DNA-enabled rational design of fluorescence-Raman bimodal nanoprobes for cancer imaging and therapy. Nat Commun. 2019;10(1):1926. doi:10.1038/s41467-019-09173-2
89. Stefan H, Huang R, Wall MA, et al. Surface-enhanced resonance Raman scattering nanostars for high-precision cancer imaging. Science Translational Medicine. 2015;7(271):271ra7. doi:10.1126/scitranslmed.3010633
90. Leyong Z, Pan Y, Wang S, et al. Raman reporter-coupled ag core @au shell nanostars for in vivo improved surface enhanced raman scattering imaging and near-infrared-triggered photothermal therapy in breast cancers. ACS Applied Materials & Interfaces. 2015;7(30):16781–16791. doi:10.1021/acsami.5b04548
91. Yijing L, Bhattarai P, Dai Z, et al. Photothermal therapy and photoacoustic imaging via nanotheranostics in fighting cancer. Chem. Soc. Rev. 2019;48(7):2053–2108. doi:10.1039/c8cs00618k
92. Lyu Y, Li J, Pu K. Second near-infrared absorbing agents for photoacoustic imaging and photothermal therapy. Small Methods. 2019;3:1900553. doi:10.1002/smtd.201900553
93. Vy PTT, Bui NQ, Cho SW, et al. Photoacoustic imaging-guided photothermal therapy with tumor-targeting ha-feooh@ppy nanorods. Scientific Reports. 2018;8(1):8809. doi:10.1038/s41598-018-27204-8
94. Minh DVH, Nguyen VT, Mondal S, et al. Fluorescence/photoacoustic imaging-guided nanomaterials for highly efficient cancer theragnostic agents. Scientific Reports. 2021;11(1):1594. doi:10.1038/s41598-021-95660-w
95. Ming C, Chen X-T, Zhang L-Y, et al. Kinetically and thermodynamically controlled one-pot growth of gold nanoshells with NIR-II absorption for multimodal imaging-guided photothermal therapy. J Nanobiotechnol. 2023;21(1):138. doi:10.1186/s12951-023-01907-1
96. Xueru S, Chen Q, Yin X, et al. Polypyrrole-based double rare earth hybrid nanoparticles for multimodal imaging and photothermal therapy. J Mat Chem B. 2020;8(3):426–437. doi:10.1039/c9tb02254f
97. Tingting G, Gao S, Li Y, Zhang R, Dong H, et al. The down-shifting luminescence of rare-earth nanoparticles for multimodal imaging and photothermal therapy of breast cancer. Biology. 2024;13(3). doi:10.3390/biology13030156
98. Misung P, et al. Breast cancer metastasis: mechanisms and therapeutic implications. Int J Mol Sci. 2022;23(12):6806. doi:10.3390/ijms23126806
99. Ibragimova Marina K, Syganov MM, Kravtsova EA, Tsydenova IA, Litviakov NV. Organ-specificity of breast cancer metastasis. Int J Mol Sci. 2023;24(21):1562. doi:10.3390/ijms242115625
100. Priyadarshini A, Senapati D, Das N, et al. Development of UiO-66 and ZIF-8 MOF nanocarriers for anticancer drug delivery in breast cancer cells. Chem Asian J. 2025;20:e00672. doi:10.1002/asia.202500672
101. Iranpour S, Bahrami AR, Dayyani M, Saljooghi AS, Matin MM. A potent multifunctional ZIF-8 nanoplatform developed for colorectal cancer therapy by triple-delivery of chemo/radio/targeted therapy agents. Journal of Materials Chemistry. 2024;12:1096–1114. doi:10.1039/d3tb02571c
102. Xueqi O, Tan Y, Xie J, et al. Methylation of GPRC5A promotes liver metastasis and docetaxel resistance through activating the mTOR signaling pathway in triple-negative breast cancer. Drug resistance updates: reviews and commentaries in antimicrobial and anticancer chemotherapy. Drug Resistance Updates. 2024;73:101063. doi:10.1016/j.drup.2024.101063
103. Jie L, Wang J, Li H, et al. Supramolecular materials based on AIE luminogens (AIEgens): construction and applications. Chem. Soc. Rev. 2020;49(4):1144–1172. doi:10.1039/c9cs00495e
104. Jie L, et al. A facile strategy of boosting photothermal conversion efficiency through state transformation for cancer therapy. Adv materials. 2021;33(51):e2105999. doi:10.1002/adma.202105999
105. Qian C, et al. Photothermal therapy with immune-adjuvant nanoparticles together with checkpoint blockade for effective cancer immunotherapy. Nat Commun. 2016;7:1319. doi:10.1038/ncomms13193
106. Chen B, Huang R, Zeng W, et al. Nanocodelivery of an NIR photothermal agent and an acid-responsive TLR7 agonist prodrug to enhance cancer photothermal immunotherapy and the abscopal effect. Biomaterials. 2024;305:122434. doi:10.1016/j.biomaterials.2023.122434
107. Aquib M, Juthi AZ, Farooq MA, et al. Advances in local and systemic drug delivery systems for post-surgical cancer treatment. J Mat Chem B. 2020;8(37):8507–8518. doi:10.1039/d0tb00987c
108. Yang X, Gao L, Wei Y, et al. Photothermal hydrogel platform for prevention of post-surgical tumor recurrence and improving breast reconstruction. J Nanobiotechnol. 2021;19(1):307. doi:10.1186/s12951-021-01041-w
109. Kim MY, et al. Breast cancer metastasis. advances in experimental medicine and biology. Adv Exp Med Bio. 2021;1187:183–204. doi:10.1007/978-981-32-9620-6_9
110. S MC, Miao Z, Superville D, et al. The temporal progression of lung immune remodeling during breast cancer metastasis. Cancer Cell. 2024;42(6):1018–1031.e6. doi:10.1016/j.ccell.2024.05.004
111. Lin M, Kang Y, Zhang XF. et al. Nanotechnology for the theranostic opportunity of breast cancer lung metastasis: recent advancements and future challenges. Front. Bioeng. Biotechnol. 2024;12:1410. doi:10.3389/fbioe.2024.1410017
112. Açelya Y, Eroglu Z, Gurcan C, et al. Synergized photothermal therapy and magnetic field-induced hyperthermia via bismuthene for lung cancer combinatorial treatment. Materials Today. Bio. 2023;23:1008. doi:10.1016/j.mtbio.2023.100825
113. Mujie Y, Han Z, Li Y, et al. A pH-responsive nanoplatform with dual-modality imaging for enhanced cancer phototherapy and diagnosis of lung metastasis. J Nanobiotechnol. 2024;22(1):180. doi:10.1186/s12951-024-02431-6
114. Zheng L, Cheng L, Xu X, et al. Cuproptosis-based layer-by-layer silk fibroin nanoplatform-loaded PD-L1 siRNA combining photothermal and chemodynamic therapy against metastatic breast cancer. Materials Today. Bio. 2024;29:1012. doi:10.1016/j.mtbio.2024.101298
115. Yutian Z, Ye F, Kong Y, et al. The single-cell landscape of intratumoral heterogeneity and the immunosuppressive microenvironment in liver and brain metastases of breast cancer. Advanced Science. 2023;10(5):e2203699. doi:10.1002/advs.202203699
116. A R-AA, Selby LV, Lustberg MB, et al. Surgical management of breast cancer liver metastasis. Hematology/Oncology Clinics of North America. 2025;39(1):25–35. doi:10.1016/j.hoc.2024.08.012
117. Yanbing C, Wei D, Yang L, et al. nanoplatform self-assembly from small molecules of porphyrin derivatives for nir-ii fluorescence imaging guided photothermal-immunotherapy. Advanced Healthcare Materials. 2022;11(11):e2102526. doi:10.1002/adhm.202102526
118. Lixuan T, Yang X, He L, et al. Preclinical advances in nanoliposome-mediated photothermal therapy in liver cancer. Lipids in Health and Disease. 2025;24(1):31. doi:10.1186/s12944-024-02429-x
119. Siqiong W, Chen Y, Wang K, et al. Multifunctional mesoporous polydopamine nanoplatforms for synergistic photothermal-chemotherapy and enhanced immunotherapy in breast cancer treatment. colloids and surfaces. B, Biointerfaces. 2025;248:114483. doi:10.1016/j.colsurfb.2024.114483
120. Na L, Jiang X, Zhang W, et al. Synergetic photodynamic-photothermal-chemotherapy dual targeting nanoplatform effective against breast cancer in-mice model. Int J Nanomed. 2023;18:6365. doi:10.2147/IJN.S428022
121. Jintong G, Liu Y, Liang X, Chen Z, Liu B, Yuan Z. 4T1 Cell Membrane-Coated Pdots with NIR-II Absorption and Fluorescence Properties for Targeted Phototheranostics of Breast Tumors. ACS Applied Materials & Interfaces. 2024;16(48):66425–66435. doi:10.1021/acsami.4c12845
122. Fan T, Hu H, Xu Y, et al. Hollow copper sulfide nanoparticles carrying ISRIB for the sensitized photothermal therapy of breast cancer and brain metastases through inhibiting stress granule formation and reprogramming tumor-associated macrophages. Acta Pharmaceutica Sinica B. 2023;13(8):3471–3488. doi:10.1016/j.apsb.2022.11.003
123. Xingyue H, Lu Y, Guo M, Du S, Han N. Recent strategies for nano-based PTT combined with immunotherapy: from a biomaterial point of view. Theranostics. 11(15):7569. doi:10.7150/thno.56482
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.