Back to Journals » Clinical Ophthalmology » Volume 15
Photobiomodulation Therapy for Age-Related Macular Degeneration and Diabetic Retinopathy: A Review
Authors Muste JC, Russell MW, Singh RP
Received 15 June 2021
Accepted for publication 24 August 2021
Published 2 September 2021 Volume 2021:15 Pages 3709—3720
DOI https://doi.org/10.2147/OPTH.S272327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Justin C Muste, Matthew W Russell, Rishi P Singh
Center for Ophthalmic Bioinformatics, Cole Eye Institute, Cleveland Clinic, Cleveland, Ohio, USA
Correspondence: Rishi P Singh
Center for Ophthalmic Bioinformatics, Cole Eye Institute, Cleveland Clinic, 9500 Euclid Ave, i-32, Cleveland, OH, 44195, USA
Email [email protected]
Purpose: Photobiomodulation therapy (PBT) has emerged as a possible treatment for age-related macular degeneration (AMD) and diabetic retinopathy (DR). This review seeks to summarize the application of PBT in AMD and DR.
Methods: The National Clinical Trial (NCT) database and PubMed were queried using a literature search strategy and reviewed by the authors.
Results: Fourteen studies examining the application of PBT for AMD and nine studies examining the application of PBT for diabetic macular edema (DME) were extracted from 60 candidate publications.
Discussion: Despite notable methodological differences between studies, PBT has been reported to treat certain DR and AMD patients. DR patients with center involving DME and VA ≥ 20/25 have demonstrated response to treatment. AMD patients at Age-Related Eye Disease Study Stages 2– 4 with VA ≥ 20/200 have also shown response to treatment. Results of major clinical trials are pending.
Conclusion: PBT remains an emergent therapy with possible applications in DR and AMD. Further, high powered studies monitored by a neutral party with standard devices, treatment delivery and treatment timing are needed.
Keywords: photobiomodulation therapy, age-related macular degeneration, diabetic macular edema, diabetic retinopathy
Introduction
Patients with diabetic retinopathy (DR) and age-related macular degeneration (AMD) are at increased risk of vision loss. With an ageing population increasingly afflicted by diabetes, the prevalence of both conditions is expected to increase. An estimated 288 million people will have AMD by 2040 and 191 million people will have DR by 2030.1,2 Up to one third of DR patients develop diabetic macular edema (DME), a manifestation of DR that produces loss of central vision.3
Treatment for DME began with focal photocoagulation and evolved to anti-Vascular Endothelial Growth Factor (anti-VEGF) injections. The advent of the anti-VEGF era led to landmark trials demonstrating efficacy of these injections in eyes with DME, however, entry criteria was visual acuity (VA) ≤ 20/40.4 This left the management of patients with DME and VA ≥ 20/25 Snellen (or ≥ 79 letters) unknown. The DRCR Retina Network Protocol V aimed to compare VA and retinal thickness after three different treatments: initiation of monthly aflibercept, focal laser therapy with deferred aflibercept, or initial observation with deferred aflibercept. At 2 years, patients in each treatment group had similar VA outcomes. Although 66.0% did not require further treatment, 12.0% of this group continued to lose ≥ 5 letters of vision.5 These results reveal an absence of preventative treatment for this subset of DME patients. While focal laser, micropulse diode laser, intravitreal steroid injections, and anti-VEGF injections are effective treatments, they are invasive and costly. The DRCR Retina Network Protocol I, which followed 346 participants initially treated with focal laser and ranibizumab for DME, disclosed the five-year cumulative probability of worsening was 18% for eyes with non-proliferative diabetic retinopathy and 31% for eyes with proliferative diabetic retinopathy.6
The anti-VEGF era also revolutionized treatment for a subset of patients with advanced exudative age-related macular degeneration (exudative AMD). However, no such treatments exist to control the progression of non-exudative AMD. Although the AREDS/AREDS2 vitamin formulation shows promise in individuals with intermediate AMD, its efficacy for all patients is being called into question: some authors now suggest patients should be selected for AREDS therapy based on genetic testing.7,8
Photobiomodulation (PBT) is an emerging therapy that shows potential as a treatment for patients with DME and non-exudative AMD. PBT consists of serial, brief illuminations with Near Infrared Spectrum light (600–1000 nm) from a laser or, more commonly, a light emitting diode (LED). This review article explores potential mechanisms of action and current clinical activity around PBT treatment in these applications.
Methods
This narrative review was performed with the primary objective of this study to summarize available literature on photobiomodulation therapy employed for any stage of AMD as well as DR including DME. Preclinical studies, case reports, case series, observational studies, and randomized controlled trials were considered for inclusion.
The National Clinical Trial (NCT) database was searched for “Photobiomodulation” and “Age Related Macular Degeneration” as well as “Photobiomodulation” and “Diabetic Retinopathy OR Diabetic Macular Edema.” PubMed was queried with the following search query: (((Age-Related Macular Degeneration) OR (exudative AMD) OR (neovascular AMD) OR (nonexudative AMD) OR (dry AMD) OR (diabetic macular edema) OR (diabetic retinopathy)) AND ((photobiomodulation) OR (PBT) OR (PBM) Or. (photobiomodulation therapy))). Additional articles were identified from a manual search of reference lists within included articles.
Studies were considered and classified dichotomously. Inclusion criteria were: English language, description of PBT for any stage of AMD or any stage of DR including DME. The full text of each article was reviewed by JCM and MWR. The subjects, eyes, device used, wavelength, dose, delivery parameters, and results were extracted. If applicable, NCT number was provided. For trials pending results, the date and outcome measures were reported.
Results
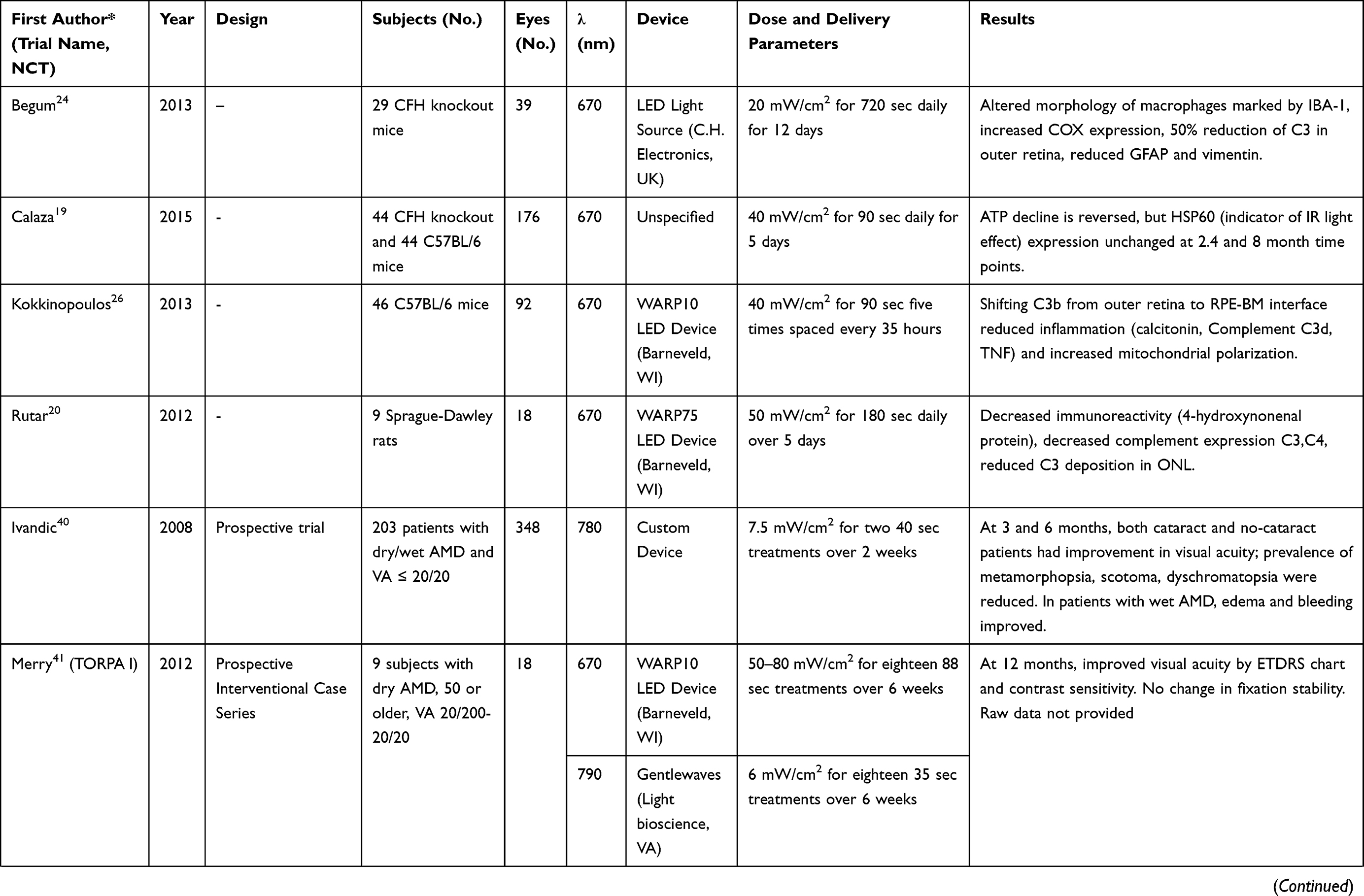
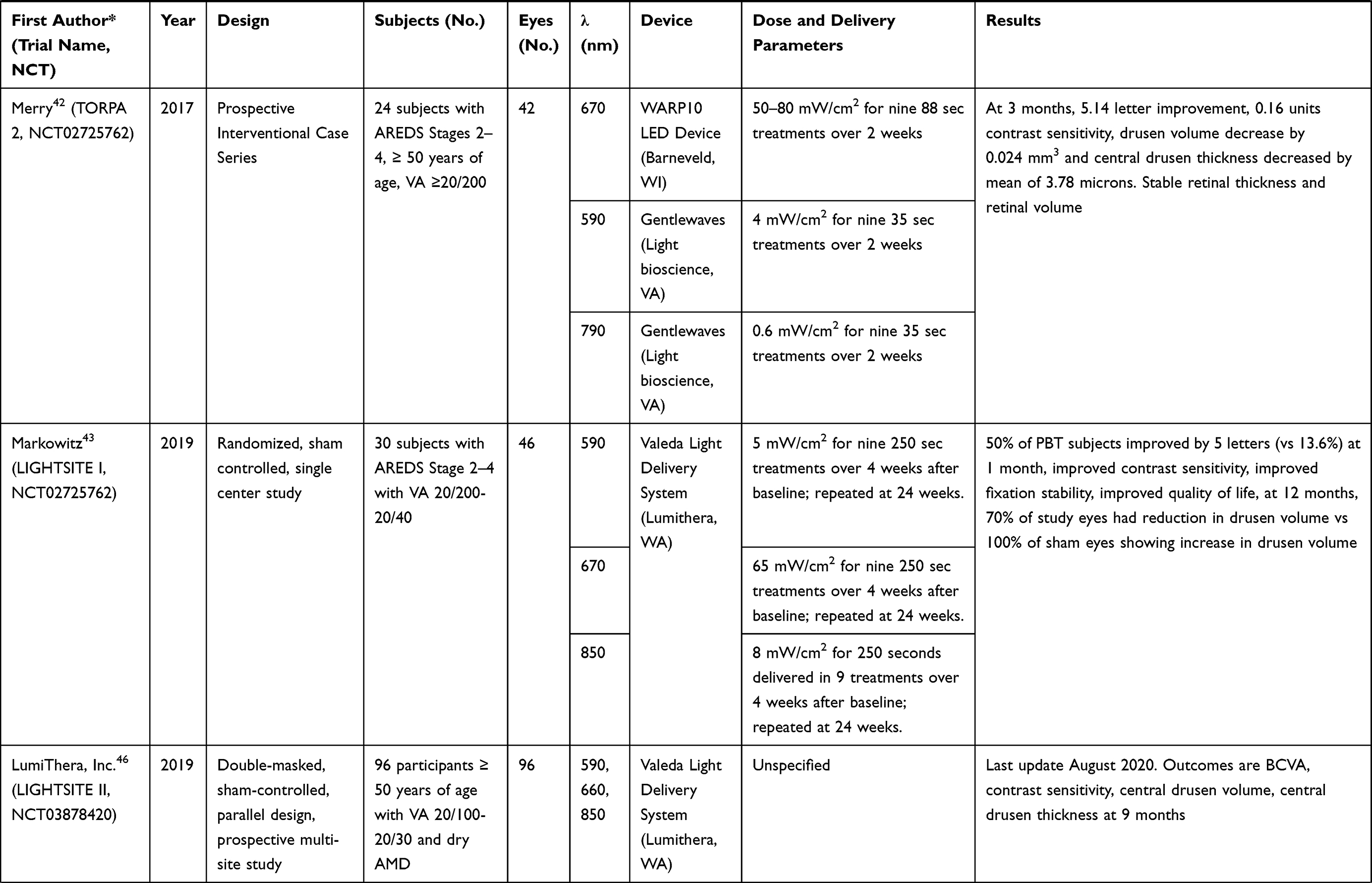
After screening 60 candidate publications, a total of 23 studies were included. 37 Studies were eliminated as they did not report on PBT as an intervention (n=30), combined therapies (n=5), non-English language (n=2). Fourteen studies examining the application of PBT for AMD can be found in Table 1. Nine studies examining the application of PBT for DME can be found in Table 2.
 |
 |
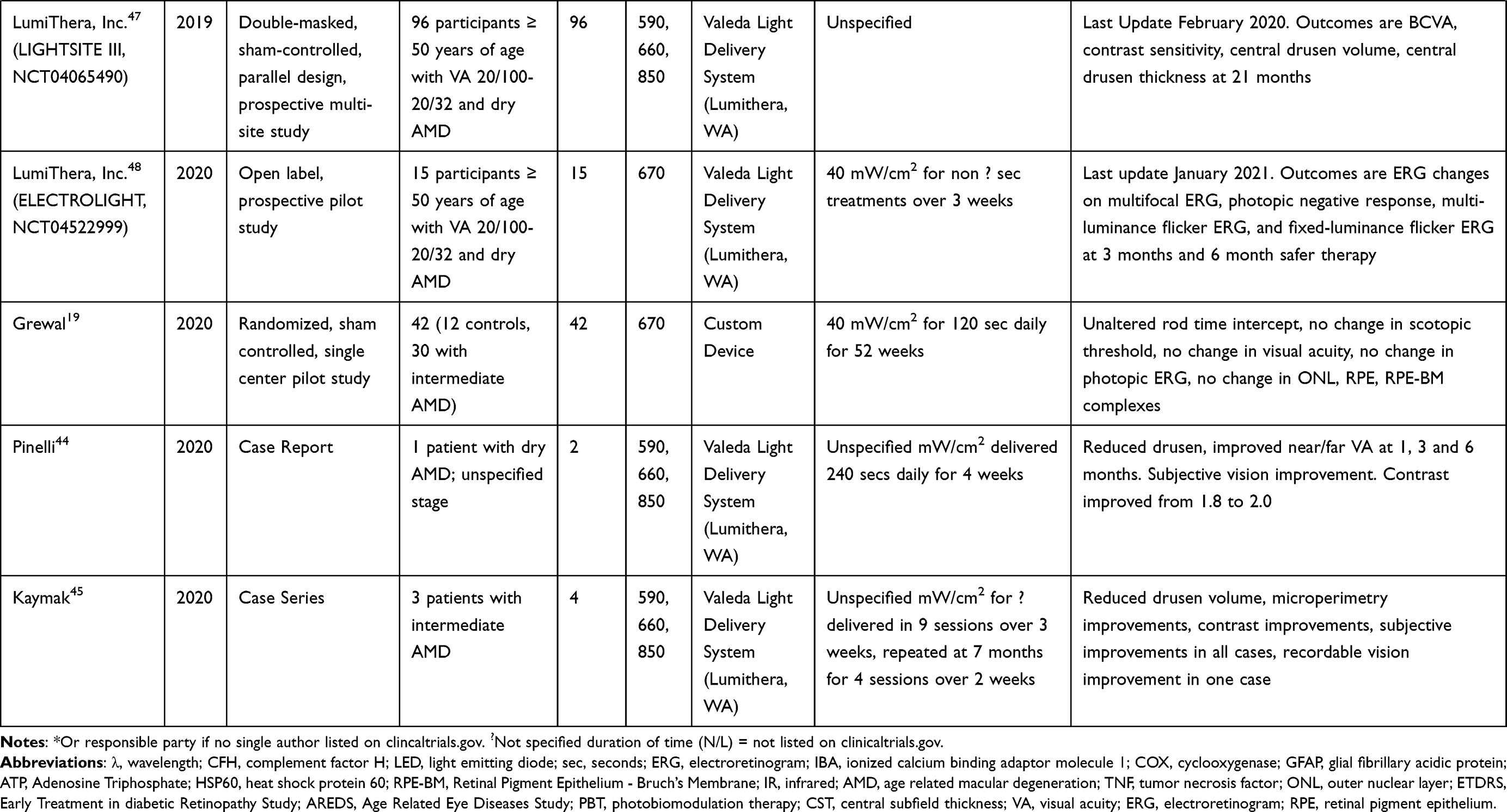 |
Table 1 Summary of Available Articles Describing the Application of Photobiomodulation for Age-Related Macular Degeneration. Subjects, Eyes, Wavelength Treated, Device Used, Dose and Delivery Parameters as Well as Results of the Studies are Presented |
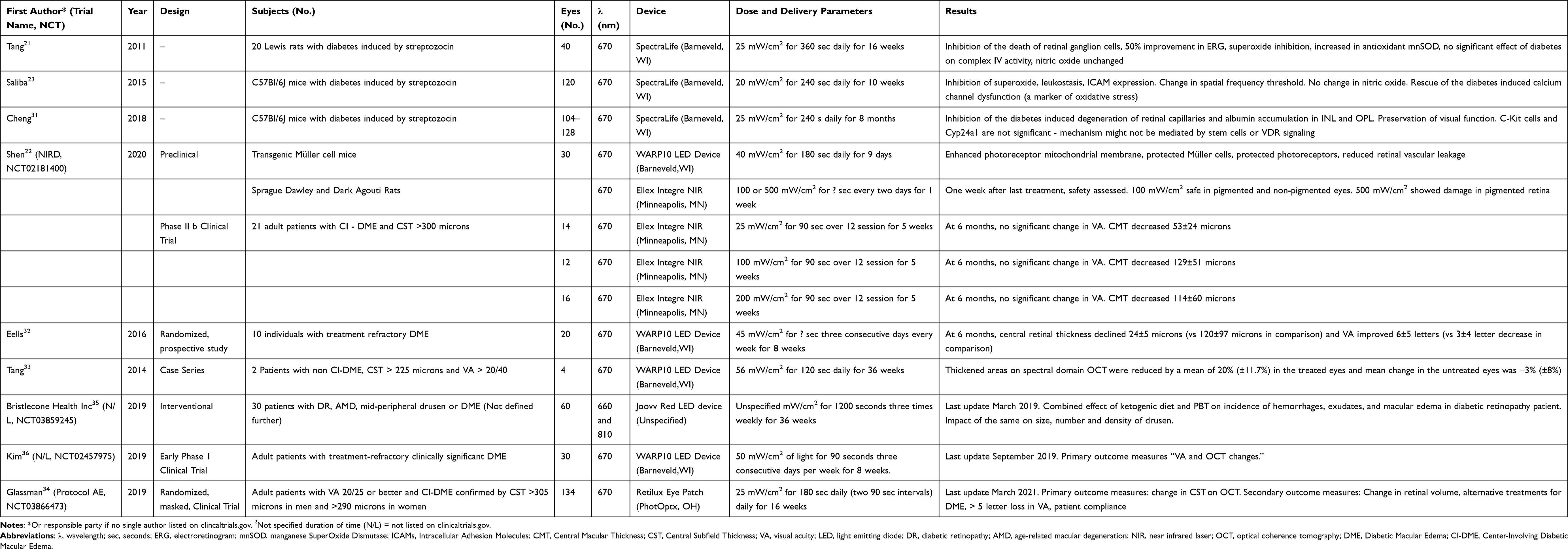 |
Table 2 Summary of Available Articles Describing the Application of Photobiomodulation for Diabetic Retinopathy. Subjects, Eyes, Wavelength Treated, Device Used, Dose and Delivery Parameters as Well as Results of the Studies are Presented |
Discussion
Mechanism of Action
Proposed mechanisms of action for PBT include enhanced photoreceptor mitochondrial function, counteracting inflammation, and enhanced supporting cell function.
In PBT, near-infrared spectral light (660–1000 nm) induces a photochemical reaction on the cellular level, starting with complex IV in the electron transport chain.9–14 Complex IV colocalizes to retinal layers rich in mitochondria such as the nerve fiber layer, around retinal ganglion cell nuclei, the inner/outer plexiform layers, the photoreceptor inner segment and basal surface of retinal pigment epithelium (RPE) cells.15 Complex IV is directly activated by NIR light, increasing respiratory chain function and mitochondrial activity.9,16 Photic stimulation uncouples nitric oxide, which would otherwise inhibit complex IV, thereby indirectly increasing mitochondrial activity.12,14,17 The freed nitric oxide also triggers downstream cascades to increase anti-antioxidant production, anti-apoptotic pathways, and cellular metabolism.18 Within photoreceptors, these changes amount to globally improved photoreceptor performance as measured by ATP production and electroretinogram (ERG).11,12,14,19,20 Although enhanced photoreceptor function shown in ERG is reported in diabetic mouse models, the same models suggest the complex IV direct and indirect pathways may not mediate the effect.21–23 Confounders, such as severity of hyperglycemia, might explain this result. It is possible that the PBT’s mechanism of action is specific to disease state, triggering pathways in a patient DME which may not be shared with those triggered in a patient with AMD. Further basic science studies might clarify if disease specific pathways are present.
The anti-inflammatory effect of PBT might be mediated across multiple pathways. Murine models for AMD and DME agree that PBT reduces C3 and C2 complement expression within the outer retina.20,23–25 Other studies upheld and expanded this observation, showing C3 presence shifted from the photoreceptors to RPE/Bruch’s membrane.20,26 This could be seen as the retina is not only expressing less early inflammatory triggers, but also clearing them. Studies have also demonstrated inhibition of superoxide as well as increased expression of the antioxidant mitochondrial antioxidant manganese superoxide dismutase (mnSOD).23,25 Others have shown decreased signals of cellular inflammation such as Glial Fibrillary Acidic Protein (GFAP), Vimentin, Cyclooxygenase (COX), calcitonin, Tumor Necrosis Factor (TNF), 4 hydroxyneal, and Intracellular Adhesion Molecules (ICAMs).20,23,24,26 These studies suggest a net anti-inflammatory effect of PBT which may be mediated by complement downregulation.
Supporting cells in the retina also react to PBT in both diabetic and AMD murine models. Müller cells show a decrease in Vimentin and GFAP, which are cell-specific markers for stress and inflammation, and possibly a prolonged lifetime.22,24,27 Tang et al demonstrated rescue of retinal ganglion cells, while Fuma et al demonstrated PBT increased phagocytic activity of RPE cell lines.25,28 Supporting cells are crucial for a healthy retina and evidence of their rescue appears positive.
Finally, PBT therapy can alter retinal gene expression. Natoli et al analyzed the change in expression of 175 neuroprotective retinal genes and ncRNAs after five days of exposure to PBT therapy. 126 of these entities increased expression as a result.29 This effect is potentiated when combined with dietary saffron intake as suggested confirmed in other studies.29,30 The effect of isolated PBT was further confirmed by Heinig et al who utilize gene expression analysis to identify upregulation of α-crystallins; a result the authors interpreted as indicating rescued mitochondrial function.13
Murine models suggest several mechanisms of action across multiple cell types, pathways, and modalities. However, these models are limited for several reasons: the disease states discussed are induced, murine and human physiology differ, and targeting light efficiently into the murine eye is an imperfect science. Due to the difficulty in targeting rodent eyes specifically, there is the possibility that PBT’s effect is may be mediated by the skin and propagated systemically through an unspecified pathway.21 Although these results must be considered with the limitations discussed above, they form the basis for clinical trials.
Diabetic Macular Edema: Clinical Applications
In addition to the aforementioned mechanisms, separate experimenters demonstrated a significant reduction in retinal microvascular leakage observed in the inner plexiform layer, inner nuclear layer and outer plexiform layer.22,31 These would suggest a unique application for PBT in diabetic retinopathy.
Two clinical studies for treatment of DME followed murine studies. Eells et al conducted a randomized prospective study in 10 patients to compare anti-VEGF alone (n=4) or anti-VEGF plus PBT (n=6). 670 nm-light treatment was administered at a transpupillary dose of 4.5 J/cm2 three consecutive days per week for 8 weeks.32 At the end of 24 weeks, the authors reported a reduction in central retinal thickness (CRT) of −24±5 microns and improvement of 6±5 letters in the PBT group as compared to a +120 ± 97 microns gain and −3 ± 4 letter VA decrease in the standard treated group (P values not reported). Tang et al reported four consecutive cases with bilateral non-center involving DME. One eye was selected for PBT, while the fellow eye was an untreated control.33 670 nm light treatment was administered at a dose of 9.0 J/cm2 for 2 to 9 months. After treatment, thickened areas on spectral domain OCT were reduced by a mean of 20.0% (±11.7%) in the treated group as compared to −3.0% (± 8.0%) in the control group.33
These results offer a new application for PBT in center involving DME (CI-DME) in the absence of a truly preventative treatment for this subset of DME patients. Shen et al delivered 670 nm light at varying energy levels (25, 100, 200 mW/cm2) to 42 eyes for 5 weeks. A maximal reduction of −129±51 μm in central macular thickness (CMT) for patients dosed 100 mW/cm2 was observed.22 Although CMT reductions were noted across all dosages, no significant VA gains were noted.
These results prompted a randomized, multi-center, sham-controlled clinical trial, Protocol AE, through the Diabetic Retinopathy Clinical Research Network on patients with CI-DME and good VA.34 Other ongoing trials investigate combinations of ketogenic diet and PBT to attenuate DME as well as treatment refractory DME, however details on these trials are limited.35,36 Trials such as Shen et al and Protocol AE show a focus on patients with VA ≥ 20/25 and Central Subfield Thickness (CST) ≥ 300 μm as inclusion criteria, which limits generalizability of available results and conclusions.22,34
At the time of this writing, evidence would suggest CI-DME patients with VA ≥ 20/25 could benefit from PBT. However, the role of PBT in DR treatment remains to be well defined in future trials standardizing devices, treatment patterns, and inclusion criteria must determine this pending the results of current work.
Age-Related Macular Degeneration: Clinical Applications
The mechanisms suggested for PBT function - an increase in mitochondrial function, reduced oxidative damage and decline in complement expression - directly foils the declining mitochondrial function, declining photoreceptor and supporting cell performance, and complement activation that characterize AMD.37–40
Ivandic treated 348 eyes with VA ≤ 20/20 at various stages of AMD with 670 nm light aimed through the conjunctiva and sclera at the macula. Patients with concomitant vision impairing disease or prior treatment affecting vision and VA >20/20 were excluded. VA by the Snellen chart improved (P<0.00001) as did color vision.40 This preliminary work did not provide details on VA measures, CST changes or fundus photography. In the following TORPA 1 trial, ETDRS acuity, contrast sensitivity and fixation stability were tested in 18 AMD eyes after 18 PBT treatments.41 Eyes that were AREDS stages 2–4 from patients 50 or older with VA ranging 20/200 - 20/20 were included. Eyes with previous or active exudative AMD, other retinal diseases, previous retinal surgery, significant media opacity or contraindications to dilation drops were excluded. At 12 months, VA improved from 0.25 logMar units (20/36) to 0.13 logMar units (20/27). Contrast sensitivity improved while fixation stability remained unchanged.
TORPA 2 expanded the TORPA 1 study to 42 eyes. Inclusion and exclusion criteria were identical with the exception that VA >20/200 was considered. At 3 months, +5.14 letters were recovered compared to baseline.42 Similarly, LIGHTSITE I evaluated PBT efficacy in 46 eyes AREDS stages 2–4 with VA 20/40-20/200.43 Major exclusion criteria were shared with the TORPA studies. 670 nm light was delivered in 9 treatment installments at baseline and again at 6 months. VA was noted to increase by up to 4 letters, then decline to baseline 6 months after each treatment, suggesting some level of consistent therapy would be required. VA variation included overlap between groups, and a significant change was noted only when analysis generated a high responder group (≥ 5 letters gained at one month).
In both TORPA 2 and LIGHTSITE I, OCT monitoring showed significant reduction in drusen volume and thickness in the setting of an unchanged CRT and central retinal volume. These observations were made relative to a control group, accounting for changes which may result from the natural course of AMD. Both studies reported improvement in contrast sensitivity and fixation stability. These functional and objective metrics are substantiated in individual case series.44,45 In both trials and case series, these improvements are noted to be last up to 6 months after PBT.
The ongoing LIGHTSITE II and LIGHTSITE III were launched in response to these findings.46,47 Eligible subjects for these studies are ≥ 50 years of age, with VA of 20/32-20/100, with eyes containing drusen ≥ 63 μm confirmed by a reading center. The ELECTROLIGHT study, which is also ongoing, seeks to assess the effect of PBT by recording electroretinograms from non-exudative AMD patients.48 Notable inclusion criteria are documented as non-exudative AMD, VA of 20/32-20/100, and ≥ 50 years of age. Salient exclusion criteria across these studies include GA, media opacity, ocular surgery, other visually significant disease. Results of the above studies are pending at the time of this writing.
As in studies for DME, the methodology of human trials for AMD show variation in treatment delivery, measurement, and outcomes. Additionally, the absence of control arms and sponsorship by device manufacturers raises further concern for bias. For this reason, Grewal et al exposed 42 eyes (12 controls, 30 intermediate AMD) to a simple easily reproducible Light Emitting Diode based light source for 120 seconds daily for 12 months.49 At the end of the study period, no significant anatomic or functional changes were reported.
Though the results are contradictory to other studies, a true comparison is difficult. Paradoxically, Grewal’s methodology – using a different device, control group, and much higher cumulative dose and exposure period – differs significantly from prior work. Nonetheless, future, well-appointed trials standardizing devices, treatment patterns, and inclusion criteria are needed to determine the true effect of PBT in AMD. Moreover, these trials have focused largely on AREDS stages 2–4. Although patients with advanced stages (geographic atrophy or exudative AMD) have been included as a subset, future work may investigate the potential for PBT to serve as an adjunctive treatment in exudative AMD and clarify the potential role it may play in a dedicated GA subset without center involvement.40,42,43,50
Available studies suggest PBT is best suited to AREDS stages 2–4 AMD, where it might alter complement deposition, attenuate oxidative damage, and enhance mitochondrial function. As with DME, the patient subset is narrow, shared in study design limitations, and high-level evidence remains wanting.
Conclusion
As a non-invasive therapy with no adverse effects reported from human subjects as of this writing, PBT may fill a role in treating niches of DR and AMD patients, specifically CI-DME with VA ≥ 20/25 or AREDS stages 2–4 with VA ≥ 20/200. The promising reports surrounding PBT might justify prospective, randomized controlled trials. If possible, a consensus of optimal timing, energy, wavelength(s) to be tested in these trials ought to be employed. Additionally, to prevent bias the trials ought to be initiated and monitored by a neutral party without vested interest.
Funding
The authors report no funding sources or conflicts of interest related to this research.
Disclosure
RPS reports personal fees from Genentech/Roche, personal fees from Alcon/Novartis, grants from Apellis and Graybug, personal fees from Zeiss, personal fees from Bausch + Lomb, personal fees from Regeneron Pharmaceuticals, Inc. the authors report no other conflicts of interest in this work. This work has not been presented at any meetings.
References
1. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Heal. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
2. Zheng Y, He M, Congdon N. The worldwide epidemic of diabetic retinopathy. Indian J Ophthalmol. 2012;60(5):428–431. doi:10.4103/0301-4738.100542
3. Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis (London, England). 2015;2(1):17. doi:10.1186/s40662-015-0026-2
4. Khanna S, Komati R, Eichenbaum DA, Hariprasad I, Ciulla TA, Hariprasad SM. Current and upcoming anti-VEGF therapies and dosing strategies for the treatment of neovascular AMD: a comparative review. BMJ Open Ophthalmol. 2019;4(1):e000398. doi:10.1136/bmjophth-2019-000398
5. Baker CW, Glassman AR, Beaulieu WT, et al. Effect of initial management with aflibercept vs laser photocoagulation vs observation on vision loss among patients with diabetic macular edema involving the center of the macula and good visual acuity: a randomized clinical trial. JAMA. 2019;321(19):1880–1894. doi:10.1001/jama.2019.5790
6. Bressler SB, Odia I, Glassman AR, et al. Changes in diabetic retinopathy severity when treating diabetic macular edema with ranibizumab: DRCR.net protocol I 5-year report. Retina. 2018;38(10):1896–1904. doi:10.1097/IAE.0000000000002302
7. Rojas-Fernandez CH, Tyber K. Benefits, potential harms, and optimal use of nutritional supplementation for preventing progression of age-related macular degeneration. Ann Pharmacother. 2017;51(3):264–270. doi:10.1177/1060028016680643
8. Mukhtar S, Ambati BK. The value of nutritional supplements in treating age-related macular degeneration: a review of the literature. Int Ophthalmol. 2019;39(12):2975–2983. doi:10.1007/s10792-019-01140-6
9. Eells JT, Henry MM, Summerfelt P, et al. Therapeutic photobiomodulation for methanol-induced retinal toxicity. Proc Natl Acad Sci U S A. 2003;100(6):3439–3444. doi:10.1073/pnas.0534746100
10. Eells JT, Gopalakrishnan S, Valter K. Near-infrared photobiomodulation in retinal injury and disease. Adv Exp Med Biol. 2016;854:437–441. doi:10.1007/978-3-319-17121-0_58
11. Ao J, Wood JP, Chidlow G, Gillies MC, Casson RJ. Retinal pigment epithelium in the pathogenesis of age-related macular degeneration and photobiomodulation as a potential therapy? Clin Experiment Ophthalmol. 2018;46(6):670–686. doi:10.1111/ceo.13121
12. Geneva II. Photobiomodulation for the treatment of retinal diseases: a review. Int J Ophthalmol. 2016;9(1):145–152. doi:10.18240/ijo.2016.01.24
13. Heinig N, Schumann U, Calzia D, et al. Photobiomodulation mediates neuroprotection against blue light induced retinal photoreceptor degeneration. Int J Mol Sci. 2020;21(7):7. doi:10.3390/ijms21072370
14. Muste JC, Kalur A, Iyer A, Valentim CCS, Singh RP. Photobiomodulation therapy in age-related macular degeneration. Curr Opin Ophthalmol. 2021;32(3):225–232. doi:10.1097/ICU.0000000000000742
15. Tao J-X, Zhou W-C, Zhu X-G. Mitochondria as potential targets and initiators of the blue light hazard to the retina. Oxid Med Cell Longev. 2019;2019:6435364. doi:10.1155/2019/6435364
16. Wong-Riley MTT, Liang HL, Eells JT, et al. Photobiomodulation directly benefits primary neurons functionally inactivated by toxins: role of cytochrome c oxidase. J Biol Chem. 2005;280(6):4761–4771. doi:10.1074/jbc.M409650200
17. Karu TI, Pyatibrat LV, Kolyakov SF, Afanasyeva NI. Absorption measurements of a cell monolayer relevant to phototherapy: reduction of cytochrome c oxidase under near IR radiation. J Photochem Photobiol B. 2005;81(2):98–106. doi:10.1016/j.jphotobiol.2005.07.002
18. de Freitas LF, Hamblin MR. Proposed mechanisms of photobiomodulation or low-level light therapy. IEEE J Sel Top Quant Elect. 2016;22:3. doi:10.1109/JSTQE.2016.2561201
19. Calaza KC, Kam JH, Hogg C, Jeffery G. Mitochondrial decline precedes phenotype development in the complement factor H mouse model of retinal degeneration but can be corrected by near infrared light. Neurobiol Aging. 2015;36(10):2869–2876. doi:10.1016/j.neurobiolaging.2015.06.010
20. Rutar M, Natoli R, Albarracin R, Valter K, Provis J. 670-nm light treatment reduces complement propagation following retinal degeneration. J Neuroinflammation. 2012;9:257. doi:10.1186/1742-2094-9-257
21. Tang J, Kern TS. Inflammation in diabetic retinopathy. Prog Retin Eye Res. 2011;30(5):343–358. doi:10.1016/j.preteyeres.2011.05.002
22. Shen W, Teo KYC, Wood JPM, et al. Preclinical and clinical studies of photobiomodulation therapy for macular oedema. Diabetologia. 2020;63(9):1900–1915. doi:10.1007/s00125-020-05189-2
23. Saliba A, Du Y, Liu H, et al. Photobiomodulation mitigates diabetes-induced retinopathy by direct and indirect mechanisms: evidence from intervention studies in pigmented mice. PLoS One. 2015;10(10):e0139003. doi:10.1371/journal.pone.0139003
24. Begum R, Powner MB, Hudson N, Hogg C, Jeffery G. Treatment with 670 nm light up regulates cytochrome C oxidase expression and reduces inflammation in an age-related macular degeneration model. PLoS One. 2013;8(2):e57828. doi:10.1371/journal.pone.0057828
25. Tang J, Du Y, Lee CA, Talahalli R, Eells JT, Kern TS. Low-intensity far-red light inhibits early lesions that contribute to diabetic retinopathy: in vivo and in vitro. Invest Ophthalmol Vis Sci. 2013;54(5):3681–3690. doi:10.1167/iovs.12-11018
26. Kokkinopoulos I. 670 nm LED ameliorates inflammation in the CFH(-/-) mouse neural retina. J Photochem Photobiol B. 2013;122:24–31. doi:10.1016/j.jphotobiol.2013.03.003
27. Albarracin R, Valter K. 670 nm red light preconditioning supports Müller cell function: evidence from the white light-induced damage model in the rat retina. Photochem Photobiol. 2012;88(6):1418–1427. doi:10.1111/j.1751-1097.2012.01130.x
28. Fuma S, Murase H, Kuse Y, Tsuruma K, Shimazawa M, Hara H. Photobiomodulation with 670 nm light increased phagocytosis in human retinal pigment epithelial cells. Mol Vis. 2015;21:883–892.
29. Natoli R, Zhu Y, Valter K, Bisti S, Eells J, Stone J. Gene and noncoding RNA regulation underlying photoreceptor protection: microarray study of dietary antioxidant saffron and photobiomodulation in rat retina. Mol Vis. 2010;16:1801–1822.
30. Di Marco F, Romeo S, Nandasena C, et al. The time course of action of two neuroprotectants, dietary saffron and photobiomodulation, assessed in the rat retina. Am J Neurodegener Dis. 2013;2(3):208–220.
31. Cheng Y, Du Y, Liu H, Tang J, Veenstra A, Kern TS. Photobiomodulation inhibits long-term structural and functional lesions of diabetic retinopathy. Diabetes. 2018;67(2):291–298. doi:10.2337/db17-0803
32. Eells J, Gopalakrishnan S, Connor T, et al. 670 nm photobiomodulation as a therapy for diabetic macular edema: a pilot study. Poster presented at: 2017 ARVO Annual Meeting; May 7-11, 2017; Baltimore, MD.,
33. Tang J, Herda AA, Kern TS. Photobiomodulation in the treatment of patients with non-center-involving diabetic macular oedema. Br J Ophthalmol. 2014;98(8):1013–1015. doi:10.1136/bjophthalmol-2013-304477
34. Kim J. A Pilot study evaluating photobiomodulation therapy for diabetic Macular Edema (AE) ClinicalTrials.gov Identifier: NCT03866473. Other Study ID Numbers: DRCR.netProtocol AE; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT03866473.
35. Bristlecone Health, Inc. Photobiomodulation & ketogenic diet for treatment of mid-periphery retinal disorders for Alzheimer’s disease prevention. ClinicalTrials.gov Identifier: NCT03859245; 2019. Available from: https://clinicaltrials.gov/ct2/show/NCT03859245.
36. Kim J. Photobiomodulation for the Treatment of Diabetic Macular Edema (PTDME). ClinicalTrials.gov Identifier: NCT02457975; 2019. Available from: https://clinicaltrials.gov/ct2/show/NCT02457975.
37. Eells JT. Mitochondrial dysfunction in the aging retina. Biology (Basel). 2019;8:2. doi:10.3390/biology8020031
38. Ennis S, Gibson J, Cree AJ, Collins A, Lotery AJ. Support for the involvement of complement factor I in age-related macular degeneration. Eur J Hum Genet. 2010;18(1):15–16. doi:10.1038/ejhg.2009.113
39. Keenan TDL, Clemons TE, Domalpally A, et al. Retinal specialist versus artificial intelligence detection of retinal fluid from OCT: age-related eye disease study 2: 10-year follow-on study. Ophthalmology. 2021;128(1):100–109. doi:10.1016/j.ophtha.2020.06.038
40. Ivandic BT, Ivandic T. Low-level laser therapy improves vision in patients with age-related macular degeneration. Photomed Laser Surg. 2008;26(3):241–245. doi:10.1089/pho.2007.2132
41. Merry G, Dotson R, Devenyi R, Markowitz SRS. Photobiomodulation as a new treatment for dry age related macular degeneration RESULTS from the Toronto and Oak Ridge Photobimodulation study in AMD (TORPA). Invest Ophthalmol Vis Sci. 2012;53:2049.
42. Merry GF, Munk MR, Dotson RS, Walker MG, Devenyi RG. Photobiomodulation reduces drusen volume and improves visual acuity and contrast sensitivity in dry age-related macular degeneration. Acta Ophthalmol. 2017;95(4):e270–e277. doi:10.1111/aos.13354
43. Markowitz SN, Devenyi RG, Munk MR, et al. A double-masked, randomized, sham-controlled, single-center study with photobiomodulation for the treatment of dry age-related macular degeneration. Retina. 2019;40:1471. doi:10.1097/IAE.0000000000002632
44. Pinelli R. Photobiomodulation Shows the Power of Light: study results demonstrate effectiveness in treating dry-age related macular degeneration. Ophthalmol Times. 2020;45(13).
45. Kaymak H, Schwahn H Photobiomodulation as a treatment in dry AMD. Retina Today: May/June Special Edition; 2020. Available from: https://retinatoday.com/articles/2020-may-june/photobiomodulation-as-a-treatment-in-dry-amd.
46. LumiThera, Inc., Study of photobiomodulation to treat non-exudative age-related macular degeneration (LIGHTSITE II). ClinicalTrials.gov Identifier: NCT03878420; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT03878420.
47. LumiThera, Inc. Study of photobiomodulation to treat non-exudative age-related macular degeneration (LIGHTSITE III). ClinicalTrials.gov Identifier: NCT04065490; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT04065490.
48. LumiThera, Inc.Study of photobiomodulation effect on electroretinogram outcomes in dry age-related macular degeneration (ELECTROLIGHT). ClinicalTrials.gov Identifier: NCT04522999; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT04522999.
49. Grewal MK, Sivapathasuntharam C, Chandra S, et al. A pilot study evaluating the effects of 670 nm photobiomodulation in healthy ageing and age-related macular degeneration. J Clin Med. 2020;9(4):1001. doi:10.3390/jcm9041001
50. Samanta A, Aziz AA, Jhingan M, et al. Emerging therapies in nonexudative age-related macular degeneration in 2020. Asia Pac J Ophthalmol. 2021. doi:10.1097/APO.0000000000000355
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.