Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Phenotypic and Dermoscopic Features in First-Degree Relatives of Melanoma Patients: A Controlled Cross-Sectional Study
Authors Ünlü CI ![]() , Sarıcaoğlu H, Aydoğan K, Bülbül Başkan E
, Sarıcaoğlu H, Aydoğan K, Bülbül Başkan E ![]() , Yazici S, Öztürk F, Şeker Ü
, Yazici S, Öztürk F, Şeker Ü
Received 17 April 2026
Accepted for publication 24 June 2026
Published 9 July 2026 Volume 2026:19 615578
DOI https://doi.org/10.2147/CCID.S615578
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Cansu Irmak Ünlü,1 Hayriye Sarıcaoğlu,2 Kenan Aydoğan,2 Emel Bülbül Başkan,2 Serkan Yazici,2 Ferdi Öztürk,2 Ümmühan Şeker2
1Department of Dermatology, Ümraniye Training and Research Hospital, University of Health Sciences, Istanbul, Türkiye; 2Department of Dermatology, Uludağ University Faculty of Medicine, Bursa, Türkiye
Correspondence: Cansu Irmak Ünlü, Email [email protected]
Background: Melanoma is a multifactorial malignancy influenced by genetic susceptibility, phenotypic traits, and exposure to ultraviolet radiation. First-degree relatives of melanoma patients represent a recognized high-risk group, yet data integrating detailed dermoscopic assessment with clinical risk profiling remain limited. This study aimed to compare phenotypic characteristics, nevus patterns, and sun-exposure–related factors between first-degree relatives of melanoma patients and matched controls, and to evaluate whether observed associations reflect an independent familial risk pattern.
Methods: In this controlled cross-sectional study, 100 first-degree relatives of 68 melanoma patients and 102 geographically matched controls without a personal or family history of melanoma underwent full-body dermatologic and dermoscopic examination. Nevi were classified by number, type, and anatomical distribution. Demographic, phenotypic, and behavioral variables were recorded. To address potential within-family correlation, a sensitivity analysis was conducted by randomly selecting one relative per family. Multivariable logistic regression adjusted for age and sex.
Results: First-degree relatives demonstrated a significantly higher prevalence of individuals with > 50 nevi and atypical nevi compared with controls. They also reported an earlier age at first sunburn and showed distinct phenotypic characteristics, including lighter hair color. In sensitivity analyses including one relative per family, these associations remained significant. After adjustment for age and sex, familial status remained independently associated with a high nevus count and the presence of atypical nevi.
Conclusion: First-degree relatives of melanoma patients exhibit dermoscopic and phenotypic features consistent with an increased melanoma risk, independent of demographic differences. These findings support targeted dermoscopic surveillance and preventive education in this high-risk population to facilitate earlier detection and improved clinical outcomes.
Keywords: melanoma, familial risk, atypical nevi, dermoscopy
Introduction
Melanoma is a highly aggressive malignancy that arises from melanocytes and represents the deadliest form of skin cancer. Its incidence has increased globally in recent decades, primarily due to cumulative ultraviolet (UV) exposure, genetic predisposition, and phenotypic risk factors.1–3 The etiology of melanoma is multifactorial, involving both inherited susceptibility and environmental influences. Established risk factors include genetic mutations, phenotypic traits resulting from gene–environment interactions (such as atypical nevi, solar lentigines, and acquired nevi), and behavioral factors such as intense intermittent sun exposure. First-degree relatives of melanoma patients are considered a high-risk population because they share genetic susceptibility, phenotypic characteristics, and environmental exposures. Epidemiological studies have demonstrated that first-degree relatives of melanoma patients have an approximately two- to eight-fold increased risk of developing melanoma compared with the general population, depending on the number of affected family members and the age at diagnosis of the index case. Familial melanoma accounts for approximately 5–10% of all melanoma cases and is most commonly associated with pathogenic variants in the CDKN2A gene. However, other susceptibility genes, including CDK4, MITF, and TERT, as well as several low-penetrance variants involved in pigmentation and nevus development, have also been implicated. These genetic factors contribute to melanoma susceptibility through effects on cell-cycle regulation, telomere maintenance, and melanocyte proliferation. Nevertheless, even in the absence of an identified pathogenic mutation, first-degree relatives of melanoma patients remain at increased risk for melanoma, suggesting that additional genetic, phenotypic, and environmental factors contribute to disease susceptibility.1–4
Although first-degree relatives of melanoma patients are recognized as a high-risk population, data integrating detailed dermoscopic findings with phenotypic risk factors in these individuals remain limited. Furthermore, the distribution of atypical and congenital nevi among first-degree relatives has not been fully characterized in many populations. A better understanding of these clinical and dermoscopic features may contribute to improved risk stratification and surveillance strategies in this high-risk group.
In this controlled, cross-sectional study, we evaluated 100 first-degree relatives of melanoma patients and 102 geographically matched controls. In addition to comprehensive full-body dermatologic and dermoscopic examinations, participants had demographic and sun exposure data collected. Both groups, with comparable gender ratios (56 females and 44 men in Group 1; 60 females and 42 males in Group 2), comprised persons usually in their fifth decade of life. Therefore, we aimed to compare the phenotypic and dermoscopic characteristics of first-degree relatives of melanoma patients with those of geographically matched controls.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted from March 8, 2023, to September 16, 2024. The study comprised two groups: Group 1 consisted of 100 first-degree relatives (parents, siblings, or offspring) of 68 individuals diagnosed with malignant melanoma. Group 2 consisted of 102 patients attending the dermatological clinic for unrelated reasons without a family history of melanoma. Participants with a personal history of melanoma were excluded from both groups. First-degree relatives were grouped by shared surnames, which served as proxies for family units. One relative per family was randomly selected for sensitivity analysis. All participants were at least eighteen years old.
Ethics Statement
Ethical approval for this study was obtained from the Clinical Research Ethics Committee of Bursa Uludağ University Faculty of Medicine (approval number: 2023–5/13; date: March 7, 2023). The study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to inclusion in the study.
Data Collection
We conducted a comprehensive body examination of all participants utilizing a handheld dermatoscope and a computer-based imaging system (FotoFinder® Medicam 500; Fotofinder Systems, 2007). Nevi were classified by total number (<10, 10–50, or >50), type (congenital, atypical), and anatomical location (head and neck, upper and lower extremities, anterior and posterior trunk, gluteal, palmoplantar). Further demographic and clinical information included age, sex, body mass index (BMI), Fitzpatrick skin type, hair color, eye color, history of sunburn, phototherapy treatment history, use of sunscreen, alcohol and tobacco use, educational level, and household income. Three classifications for income were low, below the gross minimum salary, medium, up to twice the minimum gross salary, and high, beyond twice the gross minimum salary.
Statistical Analysis
The sample size was computed using G*Power software, requiring at least 93 participants per group and targeting 80% power at a 5% significance level and an effect size of 0.20. Data normality was judged using the Shapiro–Wilk test. Continuous variables were stated as mean ± standard deviation or median (range); categorical variables as frequency and percentage. As appropriate, independent-samples t-tests or Mann–Whitney U-tests were used for between-group comparisons. Categorical data were analyzed using chi-square, Fisher’s exact, or Fisher-Freeman-Halton tests. Bonferroni correction was used for several comparisons wherever relevant. IBM SPSS Statistics for Windows, Version 29.0.2.0 (IBM Corp., Armonk, NY, USA) was used in statistical analysis. Considered statistically significant was a two-tailed p-value of less than 0.05.
To assess the robustness of the primary findings and to address potential within-family correlation, a sensitivity analysis was conducted. In this analysis, first-degree relatives were grouped by shared surnames, which were used as a proxy for family units, and one relative per family was randomly selected. All statistical analyses were repeated using this reduced dataset, assuming independent observations. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were assessed for normality and compared using the Mann–Whitney U-test. Multivariable logistic regression analysis was performed to adjust for potential confounders, including age and sex. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were calculated. A two-sided p-value of <0.05 was considered statistically significant.
Results
Participant Demographics
Group 1 (n = 100) included 56 females and 44 males, with a mean age of 42.2 ± 12.6 years (range: 19–73). Among them, 69% had a parent, 17% had a sibling, and 14% had a child diagnosed with melanoma. Group 2 (n = 102) included 60 females and 42 males, with a mean age of 49.6 ± 17.7 years (range: 18–86).
No statistically significant differences were observed between the groups in terms of sex distribution, BMI, eye color, Fitzpatrick skin type, smoking status, education level, working environment (indoor/outdoor), or sunscreen use (all p> 0.05) (Table 1).
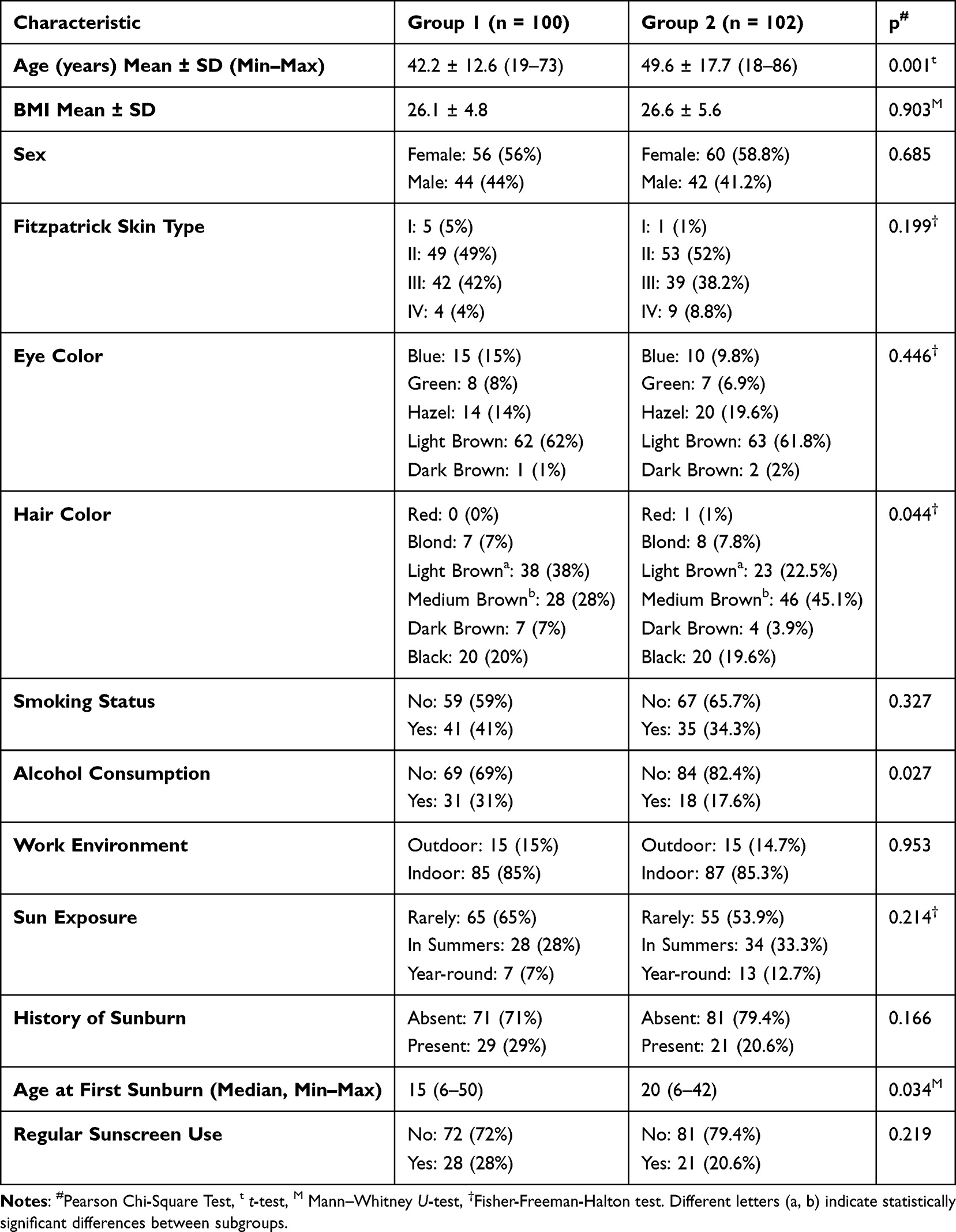 |
Table 1 Demographic, Phenotypic, and Sun Exposure History of Study Participants |
Sunburn History and Phenotypic Characteristics
Group 1 participants experienced their first sunburn significantly earlier than those in Group 2 (median: 15 vs 20 years, p = 0.034). Light brown hair color (p <0.001), alcohol consumption (p = 0.027), and middle-income status (p <0.001) were more prevalent in Group 1.
In contrast, Group 2 more frequently exhibited brown hair and a lower income status (p = 0.044 and p = 0.001, respectively).
Nevus Characteristics
Group 1 showed a significantly higher proportion of individuals with more than 50 nevi compared to Group 2 (22% vs 4.9%, p <0.001).
Atypical nevi were also more common in Group 1 (29%) than in Group 2 (10.8%) (p = 0.001). The overall number of atypical nevi was markedly higher in Group 1 (p <0.001) (Table 2 and Figure 1). There were no significant gender differences in atypical nevus distributions among the participants (p = 1.000).
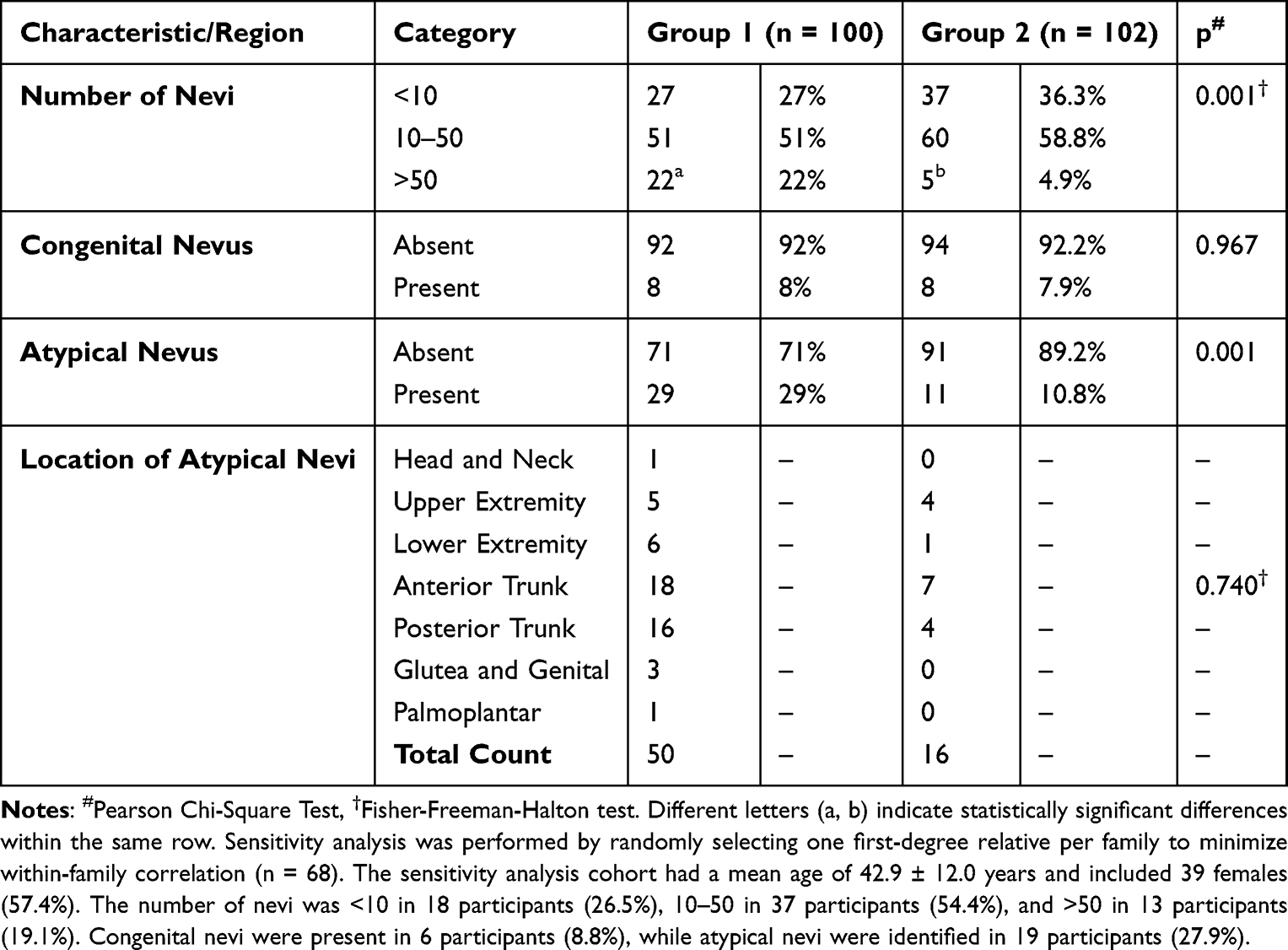 |
Table 2 In Both Groups, the Distribution of Total, Congenital, and Atypical Nevi and the Anatomical Location of Atypical Nevi |
 |
Figure 1 Clinical and dermoscopic images of a male participant in Group 1. Clinical photograph showing numerous melanocytic nevi distributed over the anterior trunk (a) and posterior trunk (b). Clinical image of a congenital melanocytic nevus (c). Dermoscopic image of an atypical melanocytic nevus demonstrating asymmetry and variegated pigmentation (d). Dermoscopic image of an atypical melanocytic nevus showing architectural disorder and heterogeneous pigmentation (e). Dermoscopic image of an atypical melanocytic nevus demonstrating asymmetry, eccentric hyperpigmentation, and color variegation (f). Dermoscopic image of an atypical melanocytic nevus showing an irregular pigment network and asymmetrical distribution of pigmentation (g). |
Nevus Distribution
The anatomical distribution of atypical nevi did not show any statistically significant variations between the groups (p = 0.740). The most common anatomical sites in both groups were the anterior and posterior trunk.
Eight participants from each group had congenital nevi (p = 0.967).
Additional Observations
The groups showed no appreciable variations regarding the presence of ephelides, solar lentigines, or actinic keratosis. However, a history of phototherapy was more often mentioned in Group 2 (p = 0.007). This may reflect differences in comorbidity profiles, such as the higher prevalence of chronic dermatologic conditions in Group 2.
Sensitivity Analysis Results
In the sensitivity analysis, including one randomly selected first-degree relative per index melanoma patient (n = 68) and the full control group (n = 102), the main findings remained consistent with the primary analysis.
First-degree relatives continued to demonstrate a significantly higher prevalence of individuals with more than 50 nevi compared with controls (19.1% vs 4.9%, p = 0.003). The presence of atypical nevi also remained significantly more frequent among relatives than controls (27.9% vs 10.8%, p = 0.004).
After adjustment for age and sex using logistic regression analysis, being a first-degree relative of a melanoma patient remained independently associated with both a high nevus count (>50 nevi; adjusted odds ratio [aOR] 4.11, 95% confidence interval [CI] 1.37–12.34, p = 0.012) and the presence of atypical nevi (aOR 3.09, 95% CI 1.34–7.14, p = 0.008).
Discussion
Our findings indicate that first-degree relatives of melanoma patients have a significantly higher total nevus count and prevalence of atypical nevi, along with distinct phenotypic and demographic characteristics such as light brown hair, an earlier age at first sunburn, and middle-income status. These results are consistent with prior large-scale studies, including the Australian Melanoma Family Study, which evaluated 629 cases diagnosed with primary cutaneous melanoma before the age of 40, 240 age-matched population-based controls, and 295 friend or partner controls, comprising a total of 1164 participants. That study demonstrated significant associations between melanoma risk and phenotypic features such as hair color, skin response to sun exposure, nevus burden—particularly on the back—and family history. Notably, sibling controls with 16 or more nevi on the back were shown to have an increased melanoma risk compared with other controls.5
Importantly, the robustness of our findings was further supported by sensitivity analyses addressing potential within-family correlation. When analyses were repeated after randomly selecting one first-degree relative per index melanoma patient, the main associations—specifically the higher prevalence of both a high nevus count (>50 nevi) and atypical nevi among relatives—remained statistically significant. Furthermore, these associations persisted after adjustment for age and sex, suggesting that the observed differences were not merely attributable to demographic imbalances between groups but rather reflect an independent familial risk pattern.
Although genetic testing was not performed in this study, the high frequency of phenotypic traits associated with melanoma risk—particularly Fitzpatrick skin types I–II, fair or light-colored hair, and susceptibility to early sunburn—supports the presence of an underlying hereditary component.6–9 Atypical nevi are well established as melanoma risk markers, particularly when present in increased numbers, and they also carry a potential risk of malignant transformation. In line with existing literature, atypical nevi in our cohort were predominantly located on the trunk in both groups.10,11
Environmental and behavioral factors also appear to contribute meaningfully to melanoma risk. While overall sun exposure patterns and sunscreen use did not differ significantly between groups, the younger age at first sunburn observed among melanoma relatives underscores the long-term impact of early ultraviolet exposure.12–16 Although the overall rate of regular sunscreen use did not differ between groups, it remained relatively low—approximately one-third of participants, particularly among melanoma relatives, consistent with previously reported data.17 Alcohol consumption was more frequent in the relative group. Although the association between alcohol intake and melanoma risk remains inconclusive, emerging evidence suggests that alcohol may increase skin cancer susceptibility through mechanisms such as photosensitization or immune modulation.18,19
No significant differences were observed between groups regarding congenital nevi, photoaging markers (including solar lentigines and ephelides), or occupational ultraviolet exposure, findings that may indicate a stronger contribution of genetic susceptibility than environmental exposure in this population. An unexpected observation was the higher prevalence of a phototherapy history in the control group, potentially reflecting selection bias or a greater burden of chronic inflammatory dermatoses, such as psoriasis. Additionally, incidental findings—including eclipse nevi, halo nevi, and, in rare cases, basal cell carcinoma and squamous cell carcinoma in situ—were identified. Although not statistically significant, these observations may warrant closer clinical surveillance in genetically susceptible individuals. The presence of blue nevi and café-au-lait macules may also suggest underlying genetic variants or syndromic associations, although this was beyond the scope of the present study.20–25
Several limitations should be acknowledged. The cross-sectional design precludes causal inference, and the predominance of offspring among melanoma relatives means that melanoma risk may not yet have fully manifested in some participants. Furthermore, the single-center nature of the study may limit generalizability. Detailed clinicopathological characteristics of melanoma in affected relatives, including anatomical location, Breslow thickness, stage, metastatic status, and melanoma subtype, were not available for analysis and therefore could not be evaluated. These factors may influence familial awareness, surveillance practices, and perceived melanoma risk. Future multicenter, longitudinal studies incorporating both genetic profiling and detailed clinicopathological information from index melanoma cases are needed to better stratify melanoma risk and to inform targeted surveillance and early intervention strategies.
Given the increased prevalence of atypical nevi and high nevus counts observed in first-degree relatives of melanoma patients, targeted surveillance strategies may be beneficial in this population. In addition to routine dermoscopic examinations, advanced non-invasive imaging techniques such as reflectance confocal microscopy (RCM) and, in selected cases, dynamic optical coherence tomography (D-OCT) may further improve the evaluation of suspected melanocytic lesions in selected high-risk individuals.26,27 Future studies are needed to determine the clinical utility and cost-effectiveness of these approaches in familial melanoma surveillance programs.
Conclusions
In conclusion, first-degree relatives of melanoma patients exhibit a higher frequency of both atypical and total nevi, along with phenotypic features associated with an increased risk of melanoma. These associations remained robust after sensitivity analyses accounting for potential within-family correlation and adjustment for age and sex, underscoring an independent familial risk pattern.
These findings support the implementation of targeted dermoscopic surveillance and structured educational interventions in this high-risk population. Early identification and routine monitoring tailored to familial risk may facilitate earlier diagnosis, enable timely intervention, and ultimately improve melanoma-related outcomes.
Acknowledgments
This study was presented as a poster at the EADV Congress 2025 (https://eadv.org/wp-content/uploads/scientific-abstracts/EADV-congress-2025/Cutaneous-oncology.pdf) and as an oral presentation at the Turkish National Dermatology Congress 2024 (https://turkdermatoloji.org.tr/public/media/pdf/32%20TDD%20Bildiri%20Kitab%C4%B1.pdf).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare no conflict of interest.
References
1. Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur J Cancer. 2005;41:45–9. doi:10.1016/j.ejca.2004.10.016
2. Nikolaou V, Stratigos AJ. Emerging trends in the epidemiology of melanoma. Br J Dermatol. 2014;170:11–19. doi:10.1111/bjd.12492
3. Tucker MA, Goldstein AM. Melanoma etiology: where are we? Oncogene. 2003;22:3042–3052. doi:10.1038/sj.onc.1206444
4. Bishop DT, Demenais F, Goldstein AM, et al. Geographical variation in the penetrance of CDKN2A mutations for melanoma. J Natl Cancer Inst. 2002;94:894–903. doi:10.1093/jnci/94.12.894
5. Cust AE, Schmid H, Maskiell JA, et al. Population-based study of prognostic factors and survival in cutaneous melanoma. J Clin Oncol. 2009;27:5944–5950. doi:10.1200/JCO.2008.19.6147
6. Zalaudek I, Argenziano G, Di Stefani A, et al. Dermoscopy of facial nonpigmented actinic keratosis. Br J Dermatol. 2006;155:951–956. doi:10.1111/j.1365-2133.2006.07426.x
7. Han J, Colditz GA, Hunter DJ. Risk factors for skin cancers: a prospective study among US women. Int J Epidemiol. 2006;35:1511–1518.
8. Abbasi NR, Shaw HM, Rigel DS, et al. Early diagnosis of cutaneous melanoma: revisiting the ABCD criteria. JAMA. 2004;292:2771–2776. doi:10.1001/jama.292.22.2771
9. Terushkin V, Wang SQ, Halpern AC. Update on evidence for the harmful effects and risk factors associated with ultraviolet radiation exposure. Br J Dermatol. 2010;163:929–936.
10. Fears TR, Guerry D, Pfeiffer RM, et al. Identifying individuals at high risk of melanoma: a practical predictor of absolute risk. J Clin Oncol. 2006;24:3590–3596. doi:10.1200/JCO.2005.04.1277
11. Olsen CM, Carroll HJ, Whiteman DC. Estimating the attributable fraction for melanoma: a meta-analysis of pigmentary characteristics and freckling. Int J Cancer. 2010;127:2430–2445. doi:10.1002/ijc.25243
12. Duffy DL, Lee KJ, Jagirdar K, et al. High naevus count and MC1R red hair alleles contribute synergistically to increased melanoma risk. Br J Dermatol. 2020;183:1116–1122. doi:10.1111/bjd.19340
13. Cust AE, Jenkins MA, Goumas C, et al. Early-life sun exposure and risk of melanoma before age 40 years. JAMA Dermatol. 2011;147:995–1002.
14. Armstrong BK, Cust AE. Sun exposure and skin cancer, and the puzzle of cutaneous melanoma. Cancer Epidemiol Biomarkers Prev. 2017;26:881–885.
15. Lee TK, Rivers JK, Gallagher RP, Coldman AJ, McLean DI. Sunlight exposure and other risk factors for multiple primary melanomas. Arch Dermatol. 1997;133:278–282.
16. Demierre MF, Balin SJ, Geller AC, Koh HK. Behavioral and psychosocial determinants of sunburn among college undergraduates. Arch Dermatol. 1999;135:857–862. doi:10.1001/archderm.135.7.857
17. Azzarello LM, Dessureault S, Jacobsen PB. Sun-protective behavior among individuals with a family history of melanoma. Cancer Epidemiol Biomarkers Prev. 2006;15:142–145. doi:10.1158/1055-9965.EPI-05-0478
18. Dennis LK, Lynch CF, Sandler DP, Alavanja MC. Alcohol consumption and the risk of melanoma in the Agricultural Health Study. Cancer Causes Control. 2008;19:583–590.
19. Rivera A, Nan H, Li T, Qureshi AA, Cho E. Alcohol intake and risk of melanoma and non-melanoma skin cancer in the Nurses’ Health Study. Eur J Clin Nutr. 2013;67:1259–1263.
20. Kessides MC, Püttgen KB, Cohen BA. No biopsy needed for eclipse and cockade nevi found on the scalps of children. Arch Dermatol. 2009;145:1334–1336.
21. Seneschal J, Passeron T, Torrelo A, Ortonne JP. Vitiligo and other disorders of hypopigmentation. In: Bolognia JL, Schaffer JV, Cerroni L, editors. Dermatology.
22. Băicoianu-Nițescu LC, Gheorghe AM, Carsote M, Dumitrascu MC, Sandru F. Approach of multiple endocrine neoplasia type 1 syndrome-related skin tumors. Diagnostics. 2022;12:2768. doi:10.3390/diagnostics12112768
23. Peltonen S, Kallionpää RA, Peltonen J. Neurofibromatosis type 1 gene: beyond café au lait spots and dermal neurofibromas. Exp Dermatol. 2017;26:645–648. doi:10.1111/exd.13212
24. Boon LM, Ballieux F, Vikkula M. Vascular malformations. In: Kang S, Amagai M, Bruckner AL, editors. Fitzpatrick’s Dermatology.
25. Hand JL, Christiano AM. Basic principles of genetics. In: Bolognia JL, Schaffer JV, Cerroni L, editors. Dermatology.
26. Pellacani G, Cesinaro AM, Seidenari S. Reflectance-mode confocal microscopy of pigmented skin lesions--improvement in melanoma diagnostic specificity. J Am Acad Dermatol. 2005;53(6):979–985. doi:10.1016/j.jaad.2005.08.022
27. Wan B, Ganier C, Du-Harpur X, et al. Applications and future directions for optical coherence tomography in dermatology. Br J Dermatol. 2021;184(6):1014–1022. doi:10.1111/bjd.19553
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost–Benefit Analysis of in vivo Reflectance Confocal Microscopy for Melanoma Diagnosis in a Real-World Clinical Setting
Bruno GM, Di Matteo S, Longo C, Stanganelli I, Farnetani F, Borsari S, Mazzoni L, Ciardo S, Raucci M, Magi S, Bassoli S, Spadafora M, Mandel VD, Casari A, Chester J, Kaleci S, Colombo GL, Pellacani G
Risk Management and Healthcare Policy 2025, 18:163-172
Published Date: 15 January 2025