Back to Journals » Therapeutics and Clinical Risk Management » Volume 13
Pharmacovigilance and adverse drug reaction reporting: a perspective of community pharmacists and pharmacy technicians in Sana’a, Yemen
Authors Al-Worafi YM ![]() , Kassab YW, Alseragi WM
, Kassab YW, Alseragi WM ![]() , Almutairi MS, Ahmed A, Ming LC, Alkhoshaiban AS, Hadi MA
, Almutairi MS, Ahmed A, Ming LC, Alkhoshaiban AS, Hadi MA ![]()
Received 28 April 2017
Accepted for publication 12 July 2017
Published 7 September 2017 Volume 2017:13 Pages 1175—1181
DOI https://doi.org/10.2147/TCRM.S140674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Yaser Mohammed Al-Worafi,1,2 Yaman Walid Kassab,3 Wafa Mohammed Alseragi,4 Masaad Saeed Almutairi,5 Ali Ahmed,6 Long Chiau Ming,7 Ali Saleh Alkhoshaiban,8,9 Muhammad Abdul Hadi10
1Faculty of Pharmacy, University of Science and Technology, Sana’a, Yemen; 2Clinical Pharmacy Department, College of Pharmacy, Ajman University, Ajman, United Arab Emirates; 3Hospital and Clinical Pharmacy Department, Faculty of Pharmacy, Cyberjaya University College of Medical Sciences, Selangor, Malaysia; 4Faculty of Arts, Ibb University, Ibb, Yemen; 5College of Pharmacy, Qassim University, Qassim, Saudi Arabia; 6Unit for Medication Outcomes Research and Education (UMORE), Pharmacy, School of Medicine, University of Tasmania, Hobart, Tasmania, Australia; 7School of Pharmacy, KPJ Healthcare University College, Nilai, Negeri Sembilan, Malaysia; 8College of Medicine, Qassim University, Qassim, Saudi Arabia; 9Faculty of Pharmacy, Universiti Teknologi MARA, Puncak Alam, Selangor, Malaysia; 10Leicester School of Pharmacy, De Montfort University, Leicester, UK
Objective: The aim of this study was to compare the knowledge, attitude and barriers of pharmacy technicians and pharmacists toward pharmacovigilance, adverse drug reactions (ADRs) and ADR reporting in community pharmacies in Yemen.
Methods: This cross-sectional survey was conducted among community pharmacists and pharmacy technicians in the capital of Yemen, Sana’a. A total of 289 community pharmacies were randomly selected. The validated and pilot-tested questionnaire consisted of six sections: demographic data, knowledge about pharmacovigilance, experience with ADR reporting, attitudes toward ADR reporting, and the facilitators to improve ADR reporting.
Results: A total of 428 pharmacy technicians and pharmacists were contacted and 179 went on to complete a questionnaire (response rate: 41.8%). Of the 179 respondents, 21 (11.7%) were pharmacists and 158 (88.3%) were pharmacy technicians, of which, 176 (98.3%) were male and 3 (1.7%) were female. The mean age of the respondents was 25.87±2.63 years. There was a significant difference between the pharmacists and pharmacy technicians in terms of knowledge scores (P<0.05). The mean knowledge scores for pharmacists was 3.33±2.852 compared to 0.15±0.666 for pharmacy technicians. With regard to attitudes toward ADR reporting, all pharmacists (100%) showed a positive attitude, while only 43% of pharmacy technicians showed a positive attitude.
Conclusion: Pharmacists have a significantly better knowledge than pharmacy technicians with regard to pharmacovigilance. More than half of pharmacy technicians showed a negative attitude toward ADR reporting. Therefore, educational interventions and training is very important for community pharmacists and pharmacy technicians in Yemen to increase their awareness and participation in ADR reporting.
Keywords: pharmacovigilance, adverse drug reactions, knowledge, attitude, community pharmacy, Yemen
Background
The World Health Organization (WHO) defines pharmacovigilance as “the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other possible drug-related problems”.1 Pharmacovigilance is essential for the safe, rational, as well as cost-effective utilization of medicines worldwide; it plays an important role in improving the clinical outcomes and also decreasing mortality and morbidity rates.2 The success of pharmacovigilance centres depend on the rate of effective and spontaneous reporting of suspected adverse drug reactions (ADRs), as is considered the core component of pharmacovigilance activities.3–5 ADRs is defined by WHO as “any noxious, unintended, and undesired effect of drug that occurs as a result of treatment with drug at normal doses used in man for diagnosis, prophylaxis, and treatment”.6 ADRs are considered a major cause of patients’ morbidity, mortality, hospital admissions, as well as increasing length of hospitalization and cost of treatment.6 Literature demonstrates the importance of involving pharmacists in ADR reporting and considered pharmacists the most valuable sources of spontaneous reporting of ADRs.7–9
Community pharmacies in Yemen are considered as the most accessible and affordable health care facility to patients. This gives both licensed community pharmacists (BPharm holders) and pharmacy technicians working under the pharmacists supervision (diploma holders) the opportunity to detect and report ADRs more than any other health care professional.10,11 The Yemeni Pharmacovigilance Centre in Yemen was established in the capital, Sana’a, in early 2011 serving as a national centre to collect, compile and analyze data on ADRs; identification of risk factors and possible mechanisms underlying adverse reactions; as well as drug quality surveillance.12
Underreporting is considered one of the major challenges of the Yemeni Pharmacovigilance Centre. ADR knowledge among health care professionals is one of the major factors affecting ADRs reporting. Pharmacists, as well as other health care professionals, cannot participate effectively in ADR reporting without sufficient knowledge of ADRs and ADR reporting process. Literature review shows that health care professionals, including pharmacists, have a poor knowledge regarding pharmacovigilance.13,14 There is a lack of studies about knowledge and attitude of community pharmacy technicians toward pharmacovigilance and ADR reporting in Yemen. Therefore, the aim of this study was to assess the knowledge, attitude and barriers of community pharmacists, as well as pharmacy technicians, toward pharmacovigilance, and ADR reporting in Yemen.
Methods
A cross-sectional study was conducted over a period of 3 months among community pharmacists and pharmacy technicians in Sana’a, Yemen.
Sample size
According to the annual reports of the Ministry of Public Health and Population 2011, there were 1,160 community pharmacies in the capital, Sana’a.14,15 Based on this report, a random sample of 289 community pharmacies were selected, this was to have an estimate of precision at a 95% confidence interval (CI), with α=0.05.
Study tools
This cross-sectional survey was conducted using a self-administered questionnaire given face-to-face by the researchers. The questionnaire was developed and validated based on the information from literature.16–18
The questionnaire was pilot tested on a convenience sample of 6 pharmacists and 4 pharmacy technicians to test the validity of the questionnaire. The final questionnaire comprised of six sections. Section one included the demographic characteristics of respondents, qualifications and experience. Section two included ten open ended questions to evaluate the knowledge of the participants toward pharmacovigilance, ADRs and ADR reporting. Section three contained two questions exploring the experience of participants with ADRs and its reporting. Section four was looking at the attitude of participants toward pharmacovigilance and ADR reporting. Section five looked at determining the barriers of reporting ADRs. Section six aimed at exploring the factors that would encourage community pharmacy technicians in Yemen to report ADRs.
A score of 1 and 0 was given for each correct or incorrect answer, respectively, the total score for each participant was the summation of the scores in each section. In the knowledge section, scores could range from zero to ten and were trichotomized into three levels: good knowledge (score ≥7), moderate knowledge (score 5–6), and poor knowledge (score ≤4). Regarding attitudes, barriers, and factors that encourage ADRs reporting, a 4-point Likert scale was used (A: agree; SA: strongly agree; D: disagree; and SD: strongly disagree).
The attitude evaluation had a maximum score of 13. A score of 1 and 0 was given for each positive (strongly agree, agree) or negative answer (disagree, strongly disagree), respectively. Total scores were calculated for each participant. A total score >7 was considered as a positive attitude, a score ≤7 were considered as a negative attitude.
All community pharmacy technicians without an appropriate certification or diploma in pharmacy were excluded from this study.
Ethical approval
This study was approved by the Ethics Committee of University of Science and Technology, Yemen, and also by the managers of the enrolled community pharmacies. Furthermore, all respondents were fully informed and gave their written informed consent before participating in the study.
Statistical analysis
Demographic variables and experiences of participants included in the study were examined on a descriptive basis. Percentages and frequencies were used for the categorical variables, while mean and standard deviation were calculated for the continuous variables. To examine for differences between pharmacists and pharmacy technicians in terms of knowledge, attitude and barriers to ADRs reporting, a Student’s t-test was used to compare continuous variables, whereas a Pearson’s chi square test/Fisher’s exact test was used to compare categorical variables. All analyses were performed using SPSS statistical software version 18 (SPSS Inc., Chicago, IL, USA). P-values <0.05 was considered to indicate statistical significance.
Results
A total of 428 community pharmacists and pharmacy technicians were contacted, with 179 completing the questionnaire. Of the 179 respondents, 21 (11.7%) were pharmacists and 158 (88.3%) were pharmacy technicians, of which 176 (98.3%) were male and 3 (1.7%) were female. One-hundred-and-seventy-seven respondents (98.9%) had graduated in Yemen. The mean age of the respondents was 25.87±2.63 years. A majority of the respondents (108 [60.3%]) had ≤3 years work experience while 71 respondents (39.7%) had >3 years work experience.
Knowledge about pharmacovigilance, ADRs and ADR reporting in Yemen
Findings of this study showed significant differences between the pharmacists and pharmacy technicians in terms of understanding the concept and importance of pharmacovigilance, ADRs and its type, the difference between ADRs and side effects, who should report ADRs, the reporting procedures, establishment year, and the location of the Pharmacovigilance Centre in Yemen (P<0.05). The pharmacists answered the knowledge related questions better than pharmacy technicians. There was no significant difference between pharmacists and pharmacy technicians with regard to the question “What is the objectives of the Pharmacovigilance Centre in Yemen?” (P=0.117), with only one pharmacist answering this question correctly. There was a significant difference between the pharmacists and pharmacy technicians in terms of knowledge total scores (P<0.05). The mean knowledge scores for pharmacists was 3.33±2.852 compared to 0.15±0.666 for pharmacy technicians. There was a significant difference between the pharmacists and pharmacy technicians in terms of good knowledge (P<0.05). Five pharmacists (23.8%) had good knowledge, while two (1.3%) pharmacy technicians had moderate knowledge, and 98.7% had poor knowledge. Table 1 shows the comparison between pharmacists and pharmacy technicians in terms of knowledge related questions.
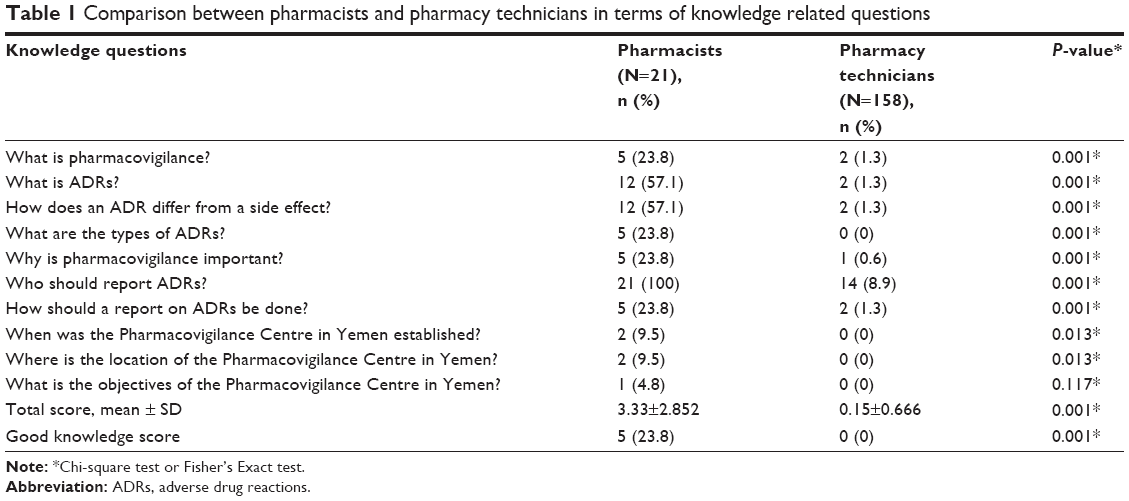 | Table 1 Comparison between pharmacists and pharmacy technicians in terms of knowledge related questions |
ADR reporting experience among community pharmacists and pharmacy technicians in Yemen
The findings of this study showed that no pharmacy technicians and only nine pharmacists (42.9%) had observed ADRs in their practice. The most common ADRs they detected were allergy and diarrhea. However, no ADRs were reported.
Attitude of community pharmacy technicians in Yemen toward pharmacovigilance and ADRs reporting
The findings of this study showed no significant difference between the pharmacists and pharmacy technicians in terms of attitude toward the question “I believe that pharmacovigilance is important” (P=0.11). The majority of pharmacists (61.9%) believed that pharmacovigilance is important, while only 43% pharmacy technicians believed that pharmacovigilance is important. There was a significant difference between pharmacists and pharmacy technicians in terms of believing that reporting ADRs is part of their professional duties (P<0.05). The majority of pharmacists (76.2%) felt that reporting ADRs was part of their professional duties compared to only 27.2% of pharmacy technicians. There was no significant difference between the pharmacists and pharmacy technicians in terms of attitude toward the question “I have to be sure the ADR is related to the drug before reporting” (P=0.14). There was a significant difference between the pharmacists and pharmacy technicians in terms of attitude toward reporting ADRs related to over the counter products (P<0.05). Only five pharmacists (23.8%) said that they would report an event, while only two pharmacy technicians (1.3%) said that they would report it. There were no significant differences between pharmacists and pharmacy technicians in terms of attitude toward reporting ADRs that caused hospitalization, life-threatening situations, a congenital anomaly, persistent disability or incapacity, or death (P=1.00).
The majority of pharmacists, as well as pharmacy technicians, said that they would report these ADRs. There was a significant difference (P<0.05) between pharmacists and pharmacy technicians in terms of attitude toward the following questions: “I report to get more insight into ADR questions that I come across in my practice”; “I report to show the patient that their concern is being taken seriously”; “I always report ADRs because it is part of pharmaceutical care” and “Consulting the physician is important before reporting an ADR”. Generally, pharmacists showed better attitudes toward the above four mentioned questions than pharmacy technicians. There was a significant difference between the pharmacists and pharmacy technicians in terms of attitude total scores (P<0.05). There was a significant difference between pharmacists attitude mean score (9.62±2.50) and pharmacy technicians attitude mean score (6.56±1.79) (P<0.05). All pharmacists had a positive attitude while only 68 (43%) of pharmacy technicians had a positive attitude toward pharmacovigilance and ADR reporting. Table 2 shows the comparison between pharmacists and pharmacy technicians in terms of attitude related questions.
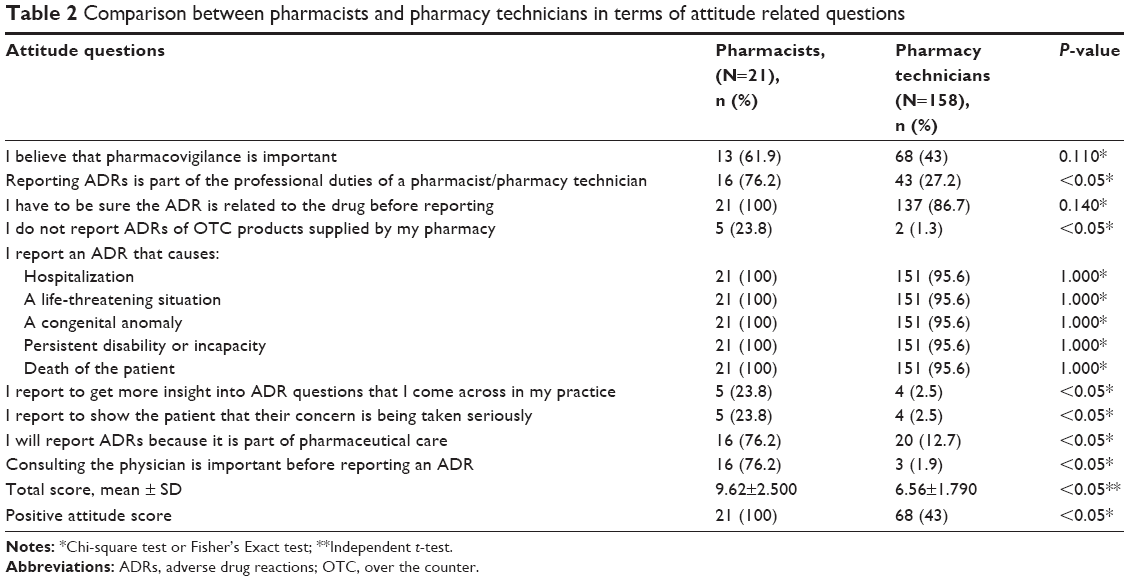 | Table 2 Comparison between pharmacists and pharmacy technicians in terms of attitude related questions |
Association between good knowledge and positive attitude
The findings of this study showed that there was a significant association (P<0.05) between good knowledge and a positive attitude toward reporting ADRs.
Barriers of ADR reporting
There was a significant difference between pharmacists and pharmacy technicians in terms of reported barriers in this study (Table 3). The most commonly given reasons for not reporting ADRs by community pharmacists were: “I don’t report because I find it difficult to admit that the patient has been harmed” (100%); “I don’t report because reporting may give the impression that I am ignorant concerning ADRs” (100%) and “All serious ADRs are detected before registration” (76.2%). The most commonly given reasons for not reporting ADRs by pharmacy technicians were reported: “All serious ADRs are detected before registration” (99.4%); “Reporting ADRs is time consuming” (98.9%); “I don’t report ADR because reporting forms are not available” (92.4%); “I don’t report because I have insufficient clinical knowledge” (80.4%) and “I don’t report ADRs because I don’t know the address where these reports should be sent” (92.4%). Table 3 shows the comparison between pharmacists and pharmacy technicians in terms of barriers related questions.
 | Table 3 Comparison between pharmacists and pharmacy technicians in terms of barriers to ADR reporting questions |
Factors encouraging ADR reporting
The findings of this study showed that the factors to encourage ADRs reporting were attending course or workshops, educational materials, more attention to ADR reporting in pharmacy curriculum, simplification of reporting procedure, and promoting reporting as a part of professional duty. Table 4 shows the comparison between pharmacists and pharmacy technicians in terms of factors encouraging ADRs reporting questions.
 | Table 4 Comparison between pharmacists and pharmacy technicians in terms of factors that encourage ADRs reporting |
Discussion
This study aimed to investigate the knowledge, attitude and barriers of both community pharmacists and pharmacy technicians toward pharmacovigilance, ADRs and ADR reporting in Yemen. This issue is very important to research in order to identify the required interventions so that the spontaneous ADR reporting can be improved, as both pharmacists and pharmacy technicians cannot participate effectively in ADR reporting without sufficient knowledge about pharmacovigilance and reporting process.
The concept of pharmacovigilance in Yemen is relatively new as until recently there was only a minimum exposure given during the training of pharmacy or medical students. The national Yemeni Pharmacovigilance Centre was only established in early 2011, which is considered late in comparison to other countries in the region. Few studies have investigated the knowledge, attitude and practice of community pharmacists toward ADRs and its reporting in Arabic countries, with none of these studies in Yemen.7,19,20
The results of this study show that the majority of community pharmacies in Yemen is run by pharmacy technicians (88.7%), which is consistent with previous reports.10,11 These reports state that pharmacy practice in Yemen faces major challenges to move toward providing better pharmaceutical care due to a number of reasons including that the number of pharmacists working in community pharmacies is insuffiecent.10,11 The results of these studies show that the majority of pharmacists and pharmacy technicians in Yemeni community pharmacies were male (98.3%), which is similar to a previous study,21 and could be due to the fact that 70% of pharmacy students in Yemen are males.
Knowledge about pharmacovigilance, ADRs and ADR reporting in Yemen
Only five pharmacists (23.8%) had a good knowledge toward pharmacovigilance, ADRs and ADR reporting, while no pharmacy technicians met the “good knowledge” criteria. This is a similar finding with studies from other Arabic countries in terms of poor knowledge among pharmacists.19,20,22–24 However, the current study differs from these other studies in design and sample size. This study also included mixed qualitative and quantitative analysis along with including pharmacy technicians due to the nature of the pharmacy practice in Yemeni community pharmacies being different from other Arabic countries.10
Experience of community pharmacy technicians in Yemen with ADRs and its reporting
The findings of this study showed that there were only nine pharmacists (42.9%) who observed ADRs in their practice. The most common ADRs they detected were allergy and diarrhea. However, they did not report these ADRs. This finding is different from studies undertaken in other Arabic countries19,20,22–24 in terms of reporting ADRs. This could be due to the Yemeni Pharmacovigilance Centre only being established in Sana’a early 2011 which has faced challenges in reporting and marketing its activities.12
Attitude of community pharmacy technicians in Yemen toward pharmacovigilance and ADRs reporting
There was a significant difference between pharmacists and pharmacy technicians in terms of positive attitude toward pharmacovigilance (P<0.05). All pharmacists had a positive attitude while only 68 (43%) pharmacy technicians had a positive attitude toward pharmacovigilance and ADR reporting. This was due to the difference in knowledge between pharmacists and pharmacy technicians. As expected, the finding of this study showed a significant association (P<0.05) between good knowledge and positive attitude toward reporting ADRs. This finding is in line with that of a study conducted in Saudi Arabia by Bawazir in terms of attitude of community pharmacists toward ADR reporting by pharmacists.22 A difference in attitude between pharmacy technicians in Yemen and community pharmacists reported by Bawazir in Saudi Arabia22 was observed, possibly due to the nature of pharmacy practice in community pharmacies being different.
Encouraging ADR reporting
Similar to other countries,22–24 this study provides strong evidence of ADR under-reporting in Yemen. More efforts should be taken by the Pharmacovigilance Centre in Yemen to improve the awareness of health care professionals on benefits and risk of medicines, and thus, practice rational prescription of drugs and implement ADR reporting. In addition, patients should also be equipped with better knowledge of the consequences of drug use, and thus, using drugs more appropriately. ADR reporting can be promoted in many ways, such as distributing manuals on ADR reporting to all medical practitioners and pharmacists. ADR reporting forms with prepaid postage could be given free to doctors and pharmacists or online reporting system could be implemented. Educational talks, bulletins and annual-reports on ADRs could be distributed to public and private sector doctors and pharmacists.
Limitations of the study
The current study has several limitations. This study was conducted in the capital, Sana’a, only, therefore the findings cannot be generalized to all Yemeni community pharmacists and pharmacy technicians. Another limitation is the small sample size of pharmacists included in this study. This is an intrinsic problem because of gross shortage of pharmacists in Yemen.
Conclusion
Pharmacists have significantly better knowledge than pharmacy technicians with regard to pharmacovigilance. More than half of pharmacy technicians also showed a negative attitude toward ADR reporting. Therefore, educational interventions and training is very important for community pharmacists and pharmacy technicians in Yemen to increase their awareness and participation in ADR reporting.
Acknowledgments
The current study is funded by Research Entity Initiative: 600-IRMI/DANA 5/3/REI (0004/2016), UiTM, Ministry of Higher Education. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors would like to express their gratitude to Ministry of Higher Education and Universiti Teknologi MARA (UiTM), Malaysia for financial support for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. The Importance of Pharmacovigilance – Safety Monitoring of Medicinal Products. WHO Collaborating Centre for International Drug Monitoring, Geneva, Switzerland. 2002. | ||
AbdulRazzaq HA, Aziz NA, Syed Sulaiman SA, Hassan Y, Kassab YW, Ismail O. Adverse drug reactions of statin based on patients’ self reports. J Pharm Res. 2012;5(2):864–868. | ||
World Health Organization. The Safety of Medicines in Public Health Programmes: Pharmacovigilance, an Essential Tool. Available from: http://www.who.int/medicines/areas/quality_safety/safety_efficacy/Pharmacovigilance_B.pdf. Accessed April 28, 2017. | ||
Rosli R, Dali AF, Aziz NA, Ming LC, Manan MM. Reported adverse drug reactions in infants: a nationwide analysis in Malaysia. Front Pharmacol. 2017;8:30. | ||
Rosli R, Ming LC, Abd Aziz N, Manan MM. A retrospective analysis of spontaneous adverse drug reactions reports relating to paediatric patients. PLoS One. 2016;11(6):e0155385. | ||
Amin MN, Khan TM, Dewan SM, Islam MS, Moghal MR, Ming LC. Cross-sectional study exploring barriers to adverse drug reactions reporting in community pharmacy settings in Dhaka, Bangladesh. BMJ Open. 2016;6(8):e010912. | ||
Hadi MA, Neoh CF, Zin RM, Elrggal ME, Cheema E. Pharmacovigilance: pharmacists’ perspective on spontaneous adverse drug reaction reporting. Integr Pharm Res Pra. 2017;6:91–98. | ||
Hadi MA, Helwani R, Long CM. Facilitators and barriers towards adverse drug reaction reporting: perspective of Malaysian hospital pharmacists. J Pharm Health Serv Res. 2013;4(3):155–158. | ||
Hadi MA, Ming LC. Impact of pharmacist recruitment on ADR reporting: Malaysian experience. South Med Rev. 2011;4(2):102–103. | ||
Al-Worafi YM. Pharmacy practice and its challenges in Yemen. Australas Med J. 2014;7(1):17–23. | ||
Al-Worafi YM. The challenges of pharmacy education in Yemen. Am J Pharm Educ. 2014;78(8):146. | ||
Al-Worafi YM. Comment on: “Pharmacovigilance in the Middle East”. Drug Saf. 2014;37(8):651–652. | ||
Lopez-Gonzalez E, Herdeiro MT, Figueiras A. Determinants of under-reporting of adverse drug reactions: a systematic review. Drug Saf. 2009;32(1):19–31. | ||
Vessal G, Mardani Z, Mollai M. Knowledge, attitudes, and perceptions of pharmacists to adverse drug reaction reporting in Iran. Pharm World Sci. 2009;31(2):183–187. | ||
Ministry of Public Health and Population. Ministry of Public Health and Population. Annual Statistical Health Report 2011. Available from: http://www.mophp-ye.org/arabic/docs/Report2011.pdf. Accessed April 28, 2017. Arabic. | ||
World Health Organization. Pharmacovigilance: Ensuring the Safe Use of Medicines – WHO Policy Perspectives on Medicines, No. 009, October 2004. Available from: http://apps.who.int/medicinedocs/en/d/Js6164e/. Accessed April 28, 2017. | ||
Green CF, Mottram DR, Rowe PH, Pirmohamed M. Attitudes and knowledge of hospital pharmacists to adverse drug reaction reporting. Br J Clin Pharmacol. 2001;51(1):81–86. | ||
Mes K, de Jong-van den Berg LT, Van Grootheest AC. Attitudes of community pharmacists in the Netherlands towards adverse drug reaction reporting. Int J Pharm Pract. 2002;10(4):267–272. | ||
Mahmoud MA, Alswaida Y, Alshammari T, et al. Community pharmacists’ knowledge, behaviors and experiences about adverse drug reaction reporting in Saudi Arabia. Saudi Pharm J. 2014;22(5):411–418. | ||
Khan TM. Community pharmacists’ knowledge and perceptions about adverse drug reactions and barriers towards their reporting in Eastern region, Alahsa, Saudi Arabia. Ther Adv Drug Saf. 2013;4(2):45–51. | ||
Al-Worafi YM. Pharmacy education in Yemen. Am J Pharm Educ. 2013;77(3):65. | ||
Bawazir SA. Attitude of community pharmacists in Saudi Arabia towards adverse drug reaction reporting. Saudi Pharm J. 2006;14(1):75–83. | ||
Suyagh M, Farah D, Abu Farha R. Pharmacist’s knowledge, practice and attitudes toward pharmacovigilance and adverse drug reactions reporting process. Saudi Pharm J. 2015;23(2):147–153. | ||
Jose J, Jimmy B, Al-Ghailani AS, Al Majali MA. A cross sectional pilot study on assessing the knowledge, attitude and behavior of community pharmacists to adverse drug reaction related aspects in the Sultanate of Oman. Saudi Pharm J. 2014;22(2):163–169. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.