Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 17
Pharmacotherapy for Obesity: Recent Updates
Authors Fredrick TW, Camilleri M ![]() , Acosta A
, Acosta A
Received 21 March 2025
Accepted for publication 7 September 2025
Published 19 September 2025 Volume 2025:17 Pages 305—327
DOI https://doi.org/10.2147/CPAA.S497904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Khaled Deeb
Thomas Ward Fredrick, Michael Camilleri, Andres Acosta
Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN, 55905, USA
Correspondence: Michael Camilleri, Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN, 55905, USA, Tel +1-507-266-2305, Email [email protected]
Abstract: In this narrative review we describe the recent updates regarding anti-obesity medications as of February 2025. We describe the physiologic mechanisms underpinning the development of hunger, satiation, and maintenance of satiety to address targets for anti-obesity medications. The efficacy, mechanism, and additional beneficial effects of anti-obesity medications are then further detailed. For this review, we focus on FDA-approved medications for obesity and on select medications currently under development and undergoing Phase 2 and 3 trials. We start by focusing on the non-incretin anti-obesity medications orlistat, phentermine, phentermine-topiramate, and naltrexone-bupropion. We also highlight setmelanotide for heritable obesity. The mechanism of action and comparative efficacy of the GLP-1 receptor agonists liraglutide and semaglutide are reviewed. Tirzepatide, the GLP-1 and GIP-receptor dual agonist is described, and weight loss is compared to alternative anti-obesity medications. Additional incretin targets in the pipeline include dual co-agonists to glucagon and GLP-1 receptors, triple agonists targeting glucagon, GLP-1 and GIP, novel GLP-1 agonists, oral formulations of GLP-1 agonists, and amylin agonists. Finally, we provide best practices for adjuncts to pharmacologic treatments of obesity, monitoring efficacy of obesity treatments, and adjusting medication regimens for providers.
Keywords: obesity, pharmacotherapy, glucagon-like peptide-1, obesity management
Introduction
Obesity remains a disease of epidemic proportions, with up to 43% of the United States population affected and rates worldwide doubling from 1990 to 2022.1,2 This rising prevalence of obesity brings significant costs to the healthcare system, estimated to be up to $172 billion in annual expenditures.3
Obesity is a disease of excess adiposity, but the diagnostic criteria remain an area of debate.4 Obesity has traditionally been classified based upon body mass index (BMI), as described in Table 1.5 BMI is a simple and reliable, population-based, metric for measuring body size, but comes with limitations for identifying individuals at increased risk of complications of obesity, particularly within different ethnic groups.6 Additional methods of measuring adiposity are detailed in Table 1. Most studies investigating obesity treatments rely on BMI, which will be the criterion used in this paper.
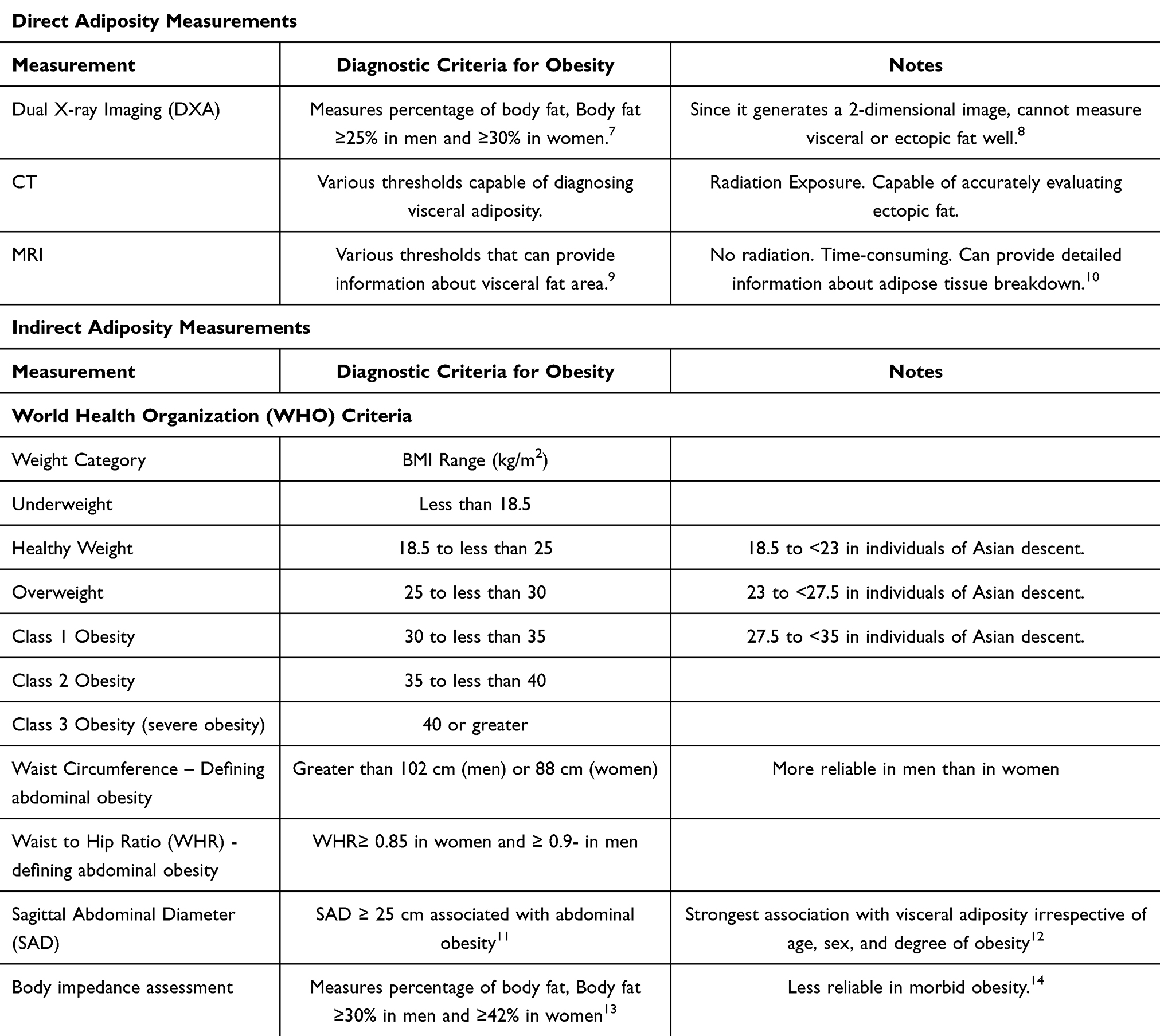 |
Table 1 Definitions of Obesity and Processes of Measuring Obesity |
Untreated obesity is associated with significant additional health consequences (Figure 1),7,15–29 and obesity is an independent risk factor for increased all-cause mortality.30 The 2013 joint American Heart Association (AHA), Obesity Society (TOS) and American College of Cardiology (ACC) guidelines for management of overweight and obesity state that “the greater the BMI, the higher the risk of fatal coronary heart disease” and “that the higher the BMI, the greater the risk of all-cause mortality”.31,32 Additionally, “overweight and obese adults with type 2 diabetes who intentionally lost 9 kg to 13 kg had a 25% decrease in mortality rate” and “there is a dose–response relationship between the amount of weight loss achieved by lifestyle intervention and the improvement in lipid profile”. Thus, treatments aimed at both correcting weight management and optimizing metabolic risk profiles can have the largest benefit in improving health outcomes.
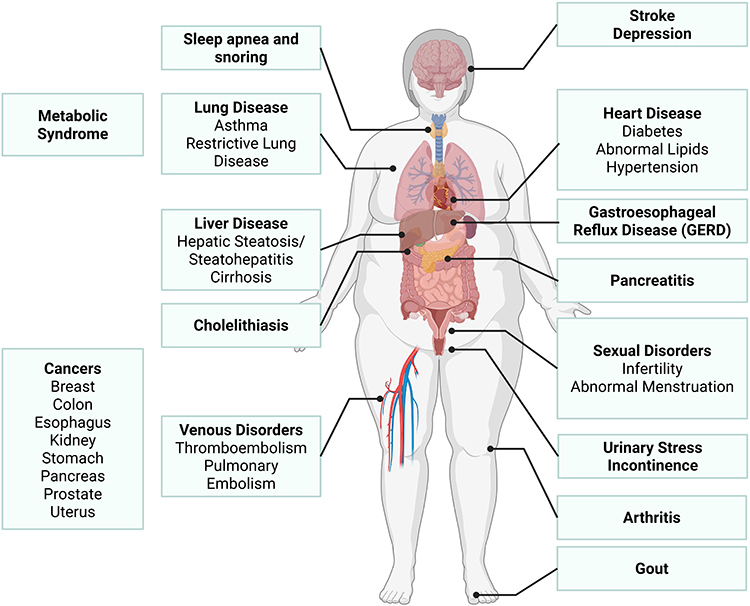 |
Figure 1 Complications of obesity. Created in BioRender. Fredrick, T. (2025) https://BioRender.com/or5mfyt. |
At a fundamental level, obesity arises from caloric imbalance where intake exceeds expenditure. Food intake regulation and signaling between the gut-adipose-brain axis are important targets for treatment of obesity.33 Historically, options for treatment of obesity focused on dietary modification and exercise.34 Many of the comorbidities associated with obesity can be effectively managed with a sustained 5–10% body weight loss, which is a reasonable first step for most patients.35 Bariatric surgical options, which result in more than 25% total body weight loss, are not widely adopted due to costs and side effect profile.36,37
Fortunately, there has been substantial expansion of pharmacological therapies for obesity in the last decade. In this article, we briefly review the pathophysiology and pertinent signals associated with food intake, the recently approved pharmacological treatments for obesity, and several novel treatments currently under investigation.
Methods
This narrative review was performed utilizing targeted literature search of PubMed, MEDLINE, and Google Scholar searches and recent high-impact reviews.38,39 We began our narrative review by reviewing the included references and searching the above registries with pertinent keywords including obesity, pharmacotherapy, phentermine, naltrexone, bupropion, topiramate, GLP-1, bariatric, anti-obesity, weight loss, and nutrition among others. Included studies were available up to February 1st, 2025. References from retrieved articles were also evaluated to extract relevant studies. Active obesity trials were identified through Clinicaltrials.gov.
Regulation of Appetite
The details regarding the physiology of appetite and caloric consumption have been well described.40,41 However, a brief review is essential to understanding the mechanism of action of novel pharmacologic treatments of obesity.
Food intake is mainly regulated by a homeostatic and a hedonic process. The homeostatic food intake regulation has three phases: hunger, satiation, and postprandial satiety. These three homeostatic phases drive food intake or appetite behavior of seek, consume, and rest. The hypothalamic arcuate nucleus (ARC) contains orexigenic neurons secreting neuropeptide Y (NPY) and agouti-related peptide (AgRP) which increase appetite38,42,43 (Figure 2A). Additional hypothalamic pathways contributing to hunger involve the lateral hypothalamus and the parabrachial nucleus via calcitonin gene-related peptide (CGRP) neurons.44,45
 |
Figure 2 Mechanisms of Hunger, Satiety, and Satiation. (A) In the fasting state, hunger arises starting with increased signaling arising from hypothalamic hormones Agouti-related peptide (AgRP), Neuropeptide Y (NPY), and Calcitonin-Gene Related Peptide (CGRP). These hormones contribute to the hunger sensation, which causes individuals to consume food. Upon food entry to the stomach (B), the stomach expands, which signals the nucleus tractus solitarius (NTS) in the brainstem. Nerve fibers then signal the stomach fundus to relax and accommodate more food. Changes in gastric hormones, including increased leptin and deacyl-ghrelin and decreased acyl-ghrelin promote changes in satiety (green arrow). As food enters the duodenum (C), enterocytes secrete additional hormones, enterokinase, CCK, GIP, and glucagon which both slow gastric emptying and promote satiety. As the bolus reached the ileum, PYY, GLP-1, and INSL5 hormones are secreted and further delay gastric emptying. The end result of these hormones is action at the level of the hypothalamus to increase POMC secretion and promote satiety. Upward green arrows reflect increases, and downward red arrow reflects decreases. Created in BioRender. Fredrick, T. (2025) https://BioRender.com/ gd6ph92. |
With food entry into the stomach, afferents in the vagus nerve signals to the nucleus tractus solitarius (NTS), and reflexively induces gastric accommodation.46 This relaxation (Figure 2B) results in distention of the stomach and vagal signals fire to induce the sensation of fullness and terminate the meal. This phenomenon is known as satiation, and individuals perceive this as a sensation of fullness and freedom from hunger.
As food is digested, incretin signals and other enzymes or hormones are released, leading to a fasting state called satiety. The signals start with changes in gastric distention, leading to decreased acyl-ghrelin, increased deacyl-ghrelin, and increased gastric leptin.47 As food enters the duodenum, other enzymes or hormones including enterokinase, cholecystokinin (CCK), glucose-dependent insulinotropic peptide (GIP, previously called gastric inhibitory polypeptide) and glucagon are all secreted and act systemically to promote postprandial satiety (Figure 2C).48 With food entry into the small intestine, intestinal L-cells release glucagon-like peptide 1 (GLP-1), which has wide ranging systemic effects promoting satiety.49–51 Once food reaches the terminal ileum, enterocytes release peptide YY (PYY), oxyntomodulin and insulin-like peptide 5 (INSL5), which constitute the “ileal brake” and further delay gastric emptying and enteric motility.52 The cumulative effect is a central sensation of postprandial satiety, (Figure 2C). As food leaves of the stomach, the anorexigenic signaling is reduced, and orexigenic signals from the hypothalamus start to promote hunger, driving the cycle again.
Adipose tissue secretes the hormone leptin, which promotes satiety. After years of excessive intake, adipose tissue stores increase throughout the body, with significant deposition in subcutaneous, liver, and mesenteric tissues. Obesity leads to changes in adipose tissue signaling through upregulation of pro-inflammatory cytokines and induces increased insulin resistance.53,54
Regulation of this neurohormonal signaling forms the basis for novel pharmacologic treatments for obesity and obesity-related conditions. When describing the beneficial and adverse effects of each anti-obesity medication, we will highlight the novel mechanisms behind their induction of weight loss.
Pharmacologic Treatments for Obesity
Details of FDA-approved anti-obesity medications are described in Tables 2 and 3, and medications in development are highlighted in Table 4. We will classify pharmacologic treatments based on their mechanisms of action and explicitly characterize those treatments which are approved by the US Food and Drug Administration (FDA) for treatment of obesity.
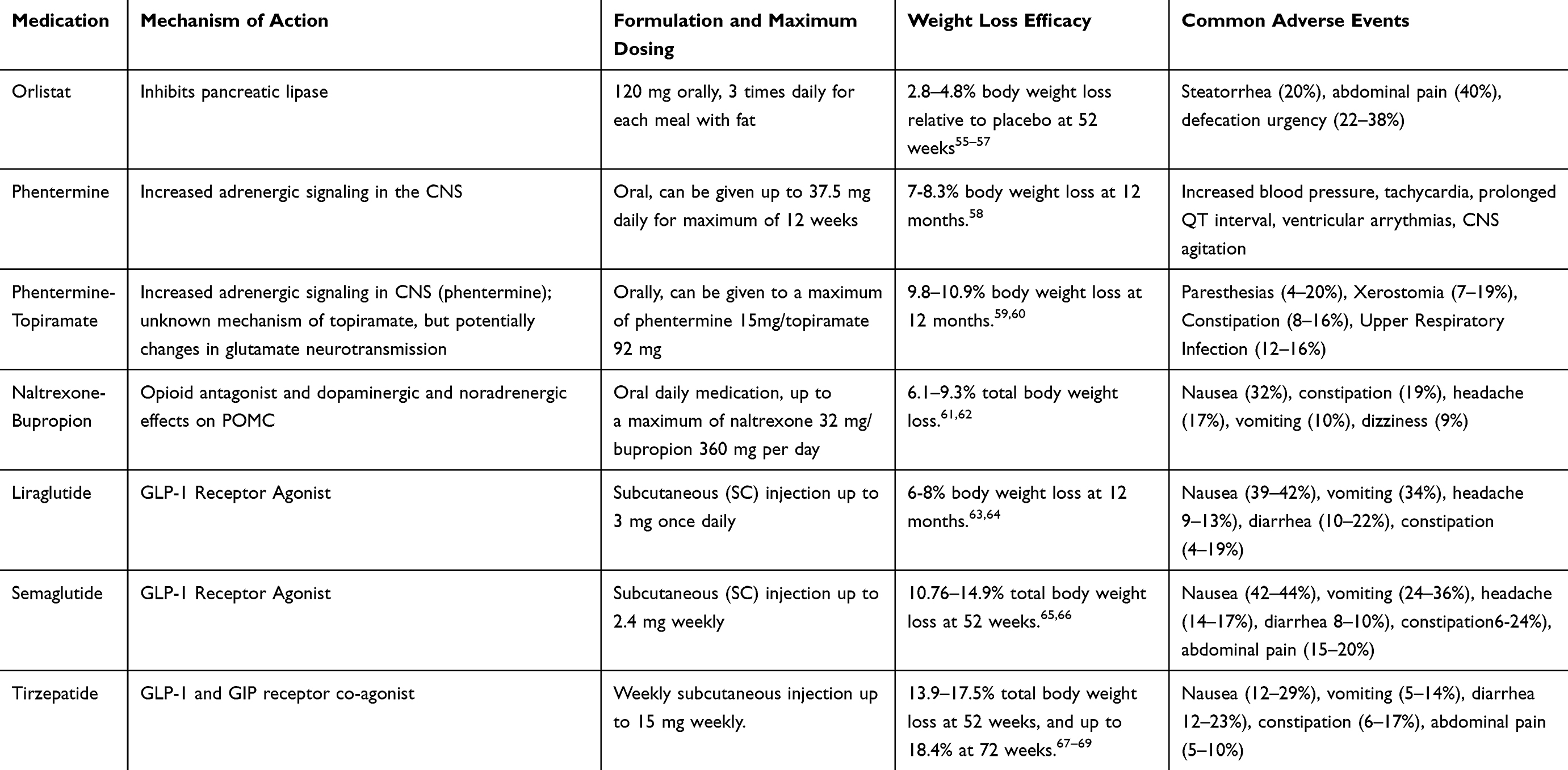 |
Table 2 Details on FDA Approved Medications for Weight Loss |
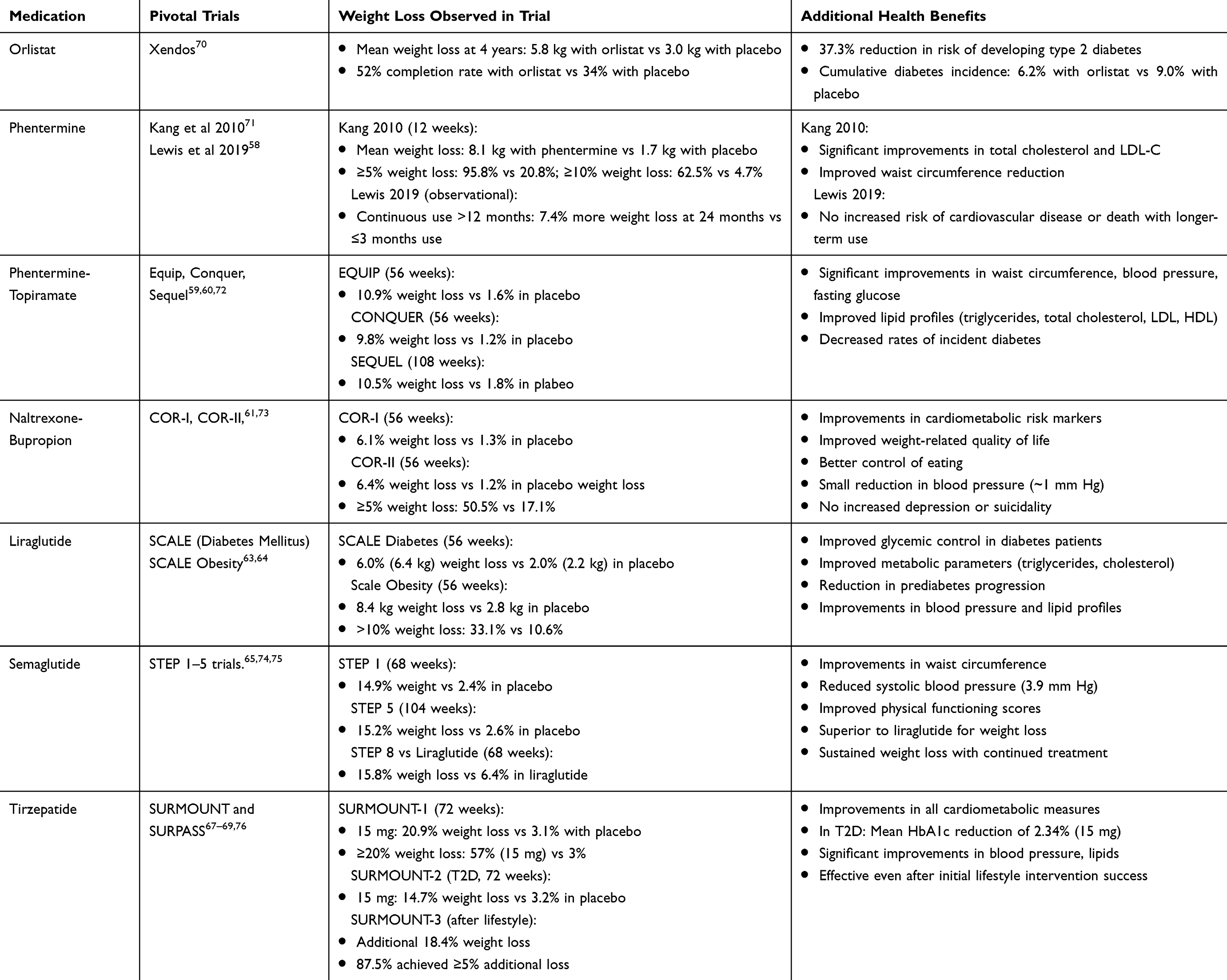 |
Table 3 Pivotal Trials Results |
 |
Table 4 Selected Anti-Obesity Medications Under Development |
Anti-Absorptive Treatments
Orlistat
Orlistat was approved by the FDA in 1999 for treatment of obesity in adults.86 Orlistat inhibits gastric and pancreatic lipase, preventing triglycerides from being hydrolyzed and decreasing the absorption of free fatty acids from the diet. Weight reduction (denoted henceforth with the minus [-] sign) ranges from −2.8 to −4.8% total body weight loss (TBWL).55,56,70,87 Additional benefits of orlistat include reduced total cholesterol, LDL, fasting glucose, and systolic and diastolic blood pressure (Table 5).88–90 Side effects arise from the reduced fat absorption, including flatulence, fecal urgency, fecal incontinence, and fat-soluble vitamin deficiencies, which result in high rates of treatment discontinuation, and low clinical use.87,91
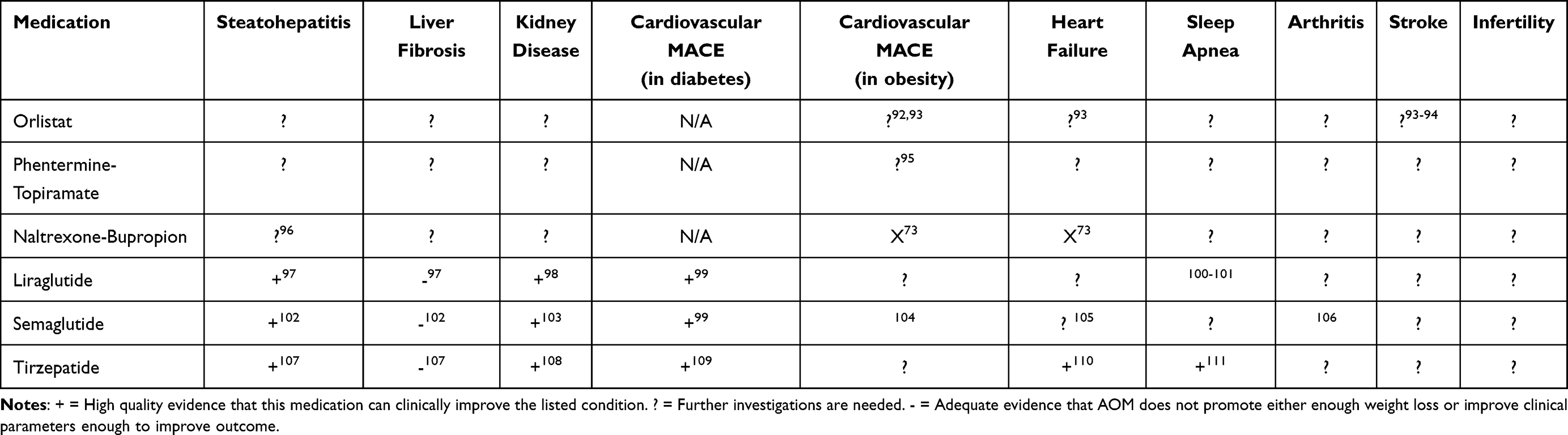 |
Table 5 Additional Benefits of FDA-Approved Anti-Obesity Treatments. Summary of Potential Additional Benefits From AOM Which Have Previously Been Investigated |
Centrally Acting Medications
Phentermine
Phentermine is a sympathomimetic medication with amphetamine-like stimulant effects initially FDA approved in 1959 for short-term weight loss.112 Through increasing extracellular dopamine, norepinephrine, and serotonin in the brain, it reduces appetite.113,114 Side effects arising from the sympathomimetic nature of phentermine include insomnia, palpitations, elevated blood pressure, and gastrointestinal distress.115 Phentermine is contraindicated in individuals with underlying cardiovascular disease given risk of arrythmias.116
Weight loss with phentermine varies from −6.7 to −8.1 kg after 12 weeks of treatment.71,117 While phentermine is only approved by FDA for 12 weeks use for weight loss, treatment can be continued longer via either continuous or intermittent use, with no increased cardiovascular risk.58
Phentermine-Topiramate (Phen-Top)
Topiramate is an anticonvulsant and anti-migraine treatment that induces weight loss of −6 to −8 kg,118 through unclear mechanisms, but likely by modulating GABA in the hypothalamus.119 Combination 15 mg/92 mg phentermine-topiramate resulted in −10.92% weight loss vs −1.55% in placebo at 56 weeks,59 and was confirmed in patients followed up to 108 weeks.60,72
Secondary benefits include a weight-loss mediated reduction in blood pressure, reduced triglycerides and LDL, improved fasting glucose, fasting insulin, and high-sensitivity C-reactive protein (HS-CRP).60 In a small randomized controlled trial (RCT), followed by a pragmatic trial, phentermine-topiramate was shown to work best in those with abnormal satiation, defined as need for high calorie intake to reach fullness.33,120
Naltrexone-Bupropion (NB)
Bupropion increases hypothalamic dopamine and norepinephrine signaling, reducing food intake,121–124 and naltrexone is approved for opioid abuse and helps reduce cravings for alcohol. The combination therapy naltrexone-bupropion (NB) has been shown to result in TBWL up to −6.1% compared to −1.3% in the placebo group at 56 weeks.61,73 When combined with intensive lifestyle changes, NB weight loss was −9.3% compared to −5.1% with placebo.62 The most common adverse events with NB include nausea, headache, constipation, dizziness, vomiting, and dry mouth. NB improves central obesity and LDL levels but without significant improvement in other cardiovascular parameters.61,62,73,125 NB is effective in binge eating disorder, which presents a patient population potentially best served by this medication.126
Setmelanotide
Setmelanotide is a daily subcutaneous injection which acts as a melanocortin-4 (MC4) receptor agonist, and was approved by the FDA in 2020 in patients with obesity arising from genetically confirmed Bardet-Biedl syndrome (BBS), POMC, PCSK1, or LEPR deficiency.127,128 Human studies of setmelanotide showed significant weight loss and improved hunger scores.129 A phase 2 study of 18 patients with hypothalamic obesity found that setmelanotide led to 80% experiencing ≥ 5% body weight loss at 16 weeks.130 Adverse events of setmelanotide include nausea, depression, suicidal ideation, and hyperpigmentation.127,129–131 Its use remains limited for these genetic alterations in MC4R signaling and given its specific actions is unlikely to be effective in the general population.
Incretin Agonists
GLP-1 Receptor Agonists
One class of anti-obesity medications experiencing a large rise in prescriptions are the GLP-1 receptor agonists (GLP-1RAs, Figure 3). GLP-1 RAs have been shown to impact functions associated with metabolism and energy balance by delaying gastric emptying, reducing hunger, increasing postprandial satiety, and reducing ad libitum food intake.132–134 In addition, GLP-1 activation in the CNS via the hypothalamus and medulla drives reduced appetite.135–137 GLP-1 directly acts on pancreatic B-cells to increase insulin secretion and on hepatic cells to decrease glucagon excretion and regulate blood glucose levels, leading to reductions in body fat.138–140
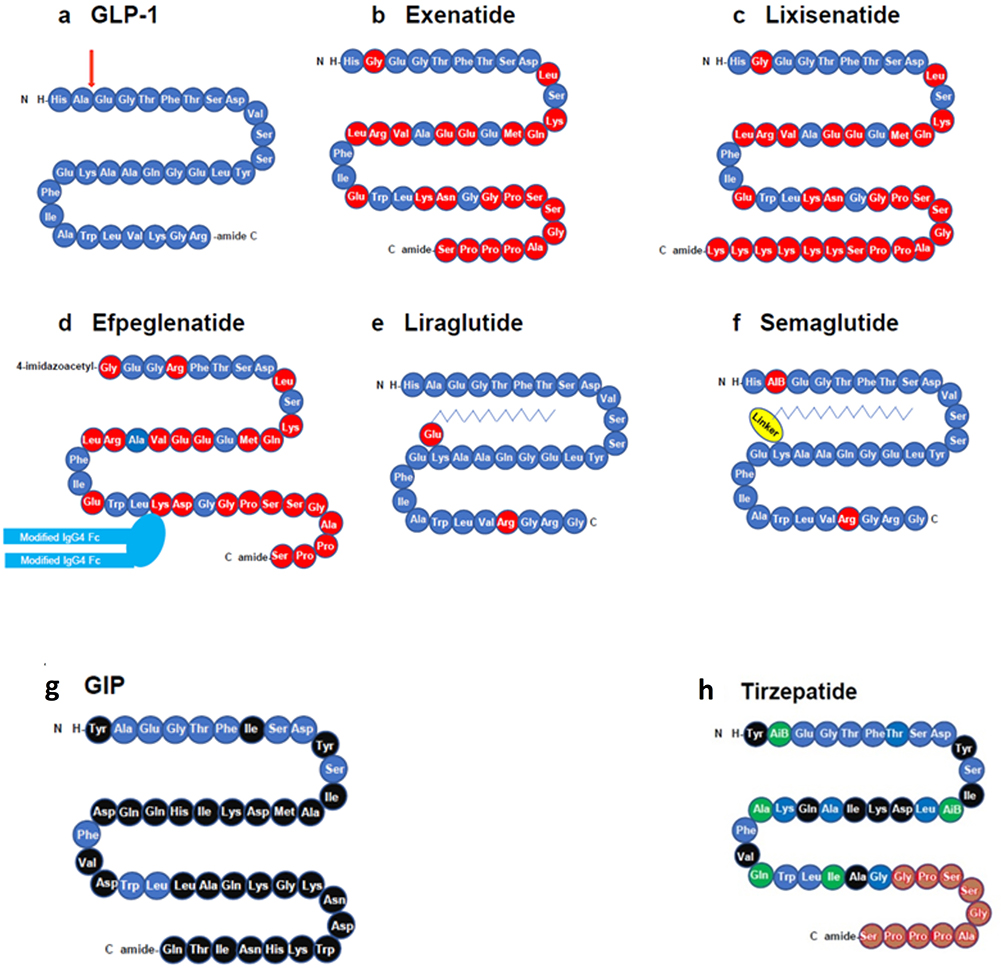 |
Figure 3 Composition of Different Incretin Agonists. Structures of formulations of GLP-1 receptor agonists (a) GLP-1, (b) exenatide, (c) lixisenatide, (d) efpeglenatide, (e) liraglutide, (f) semaglutide, (g) GIP and (h) tirzepatide. Amino acids are illustrated in circles; red circles show amino acids that are different from those in GLP-1; blue circles show amino acids that are identical to those in GLP-1; black circles show amino acids that are present in GIP and tirzepatide but not in GLP-1; brown circles show amino acids that are identical in tirzepatide and exenatide, and green circles show amino acids that are present in tirzepatide but not in GLP-1, GIP or exenatide. AiB, aminoisobutyric acid. The red arrow in (a) illustrates the site of DPP-4 inactivation. Adapted from Tschöp M, Nogueiras R, Ahrén B. Gut hormone-based pharmacology: novel formulations and future possibilities for metabolic disease therapy. Diabetologia. 2023/10/01 2023;66(10):1796–1808. Creative Commons.141 |
Liraglutide
Liraglutide was developed by modifying GLP-1 protein to include a free fatty acid side chain bound to the peptide, allowing for albumin binding and (longer) half- allowing for daily dosing.142 Five randomized controlled trials of liraglutide in individuals with obesity have shown weight loss of −4.4 kg to −6.1 kg relative to placebo.63,64,143–145
Semaglutide
Semaglutide is a GLP-1 RA with significantly longer half-life supporting weekly SQ administration. Like liraglutide, the GLP-1 sequence of semaglutide is bound to a free fatty acid side chain, mediating even stronger coupling to albumin.146,147
The STEP trials were the pivotal trials evaluating semaglutide for obesity.65 The STEP 1 randomized controlled trial investigated semaglutide 2.4 mg weekly and found a body weight loss of −14.9% vs −2.4% with placebo at 68 weeks.148 Similar effects were seen across STEP 2–5 and STEP 8 (which included both overweight and obese without diabetes), with sustained weight loss seen at 104 weeks in the STEP 5 trial.149,150
Additional benefits of semaglutide include reduced incidence of cardiovascular complications in individuals with type 2 diabetes and chronic kidney disease.151,152 The SELECT RCT showed improvement in a composite endpoint of death from cardiovascular causes, nonfatal MI, or nonfatal stroke in individuals receiving semaglutide relative to placebo (HR=0.80, 95% CI 0.72–0.90).152 Pooling results from additional trials including SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM confirmed improvement in composite outcomes in patients with heart failure (HF) with preserved ejection fraction, but no significant reduction in cardiovascular death alone in individuals receiving semaglutide.105 Notably, these studies included variable dosages of semaglutide, with few individuals on the maximum dosage used for obesity treatment. Recommendations from the American College of Cardiology have yet to support empiric GLP-1 RA use for HF.153,154
Secondary benefits of GLP-1 receptor agonists and other anti-obesity medications remain an active area of investigation and are summarized in Table 5. These include improvement in MASLD-related steatohepatitis and steatosis,155,156 knee pain in osteoarthritis,106 cardiovascular outcomes,99 and potentially substance use disorders.157
Common side effects of GLP-1 agonists include nausea, constipation, diarrhea, vomiting, abdominal discomfort, and reduced appetite.63,67,148,158 Side effects tend to be transient and resolve with time, but impact real-world adherence.159 Patients on GLP-1 receptor agonists do lose muscle mass, as is commonly seen with all forms of weight loss.160 Serious adverse events include gallbladder and biliary disease, which are believed to be dose-related and result from GLP-1 inhibiting gallbladder emptying through CCK suppression.120,140 Contraindications to use of GLP-1 receptor agonists include medullary thyroid carcinoma, family history of MEN type 2 syndrome, pancreatitis, and relative contraindications include diabetic retinopathy and uncontrolled diabetes.161,162
Given the recent approvals of these anti-obesity medications, providers and patients are undoubtedly concerned about what long-term safety data is available. Human studies have shown these medications are safe, and even protective when patients are followed for up to 5 years.163
GIP
GIP acts in synergy with GLP-1 to regulate postprandial insulin secretion.164 The effect of GIP agonism in obesity is most significant when combined with GLP-1 agonism. GIP-induced inhibition of centrally mediated emesis signals triggered by GLP-1 administration enhances weight loss seen with GLP-1 RA administration.165 Unlike GLP-1, GIP by itself does not retard gastric emptying.166
Tirzepatide
The GLP-1/GIP co-agonist, tirzepatide, has shown efficacy for both management of diabetes mellitus and weight loss.167 The SURMOUNT-1 trial found mean 72-week weight loss up to −20.9% at 15 mg weekly compared to −3.1% with placebo.67 Similar results were seen in the 5 SURPASS trials.76,168–171
Tirzepatide was approved by the FDA for weight loss in 2022.172,173 Significant benefits for obesity-associated diseases are also being reported (Table 5) including reduced heart failure events at 104 weeks of follow up (hazard ratio [HR] 0.62 compared to placebo),110 improved management of obstructive sleep apnea at 52 weeks,111 and improved management of metabolic-dysfunction associated steatohepatitis (MASH) with a decrease of ≥1 fibrosis stage with no worsening of MASH at 52 weeks.107 Side effects of tirzepatide are similar to those of the GLP-1 receptor agonists.169,172,173
Real-World Impacts
Although weight loss is significant in clinical trials of these medications, real-world evidence has shown significant variability in weight loss.174 Given high costs of these medications, discontinuation rates are as high as 50%, resulting in most real-world studies showing weight loss lower than clinical trials.174 Desire for these medications led to high levels of compounded formulations, potentially representing increased safety events reported in adverse events reported in Europe.175
AOMs Under Investigation
With advances in understanding of the incretin system, there has been substantial development of new agents for obesity. Currently there are over 100 agents being investigated in human trials.176 While each potential agent is beyond the scope of this review, we will focus on selected compounds anticipated for phase 3 trials, grouped by their mechanism of action and detailed in Table 4.
Peripheral Tissue Actors
Bimagrumab
Bimagrumab is a human monoclonal antibody that binds to the activin type II receptor (ActRII), which inhibits ligands which negatively regulate skeletal muscle growth.177 A single dose of bimagrumab increased lean mass by 2.7% and reduced fat mass by −7.9% at 10 weeks relative to placebo, and improved markers of insulin sensitivity.178 Bimagrumab also led to significant reductions in fat mass, waist circumference, improved lean mass, and reduced hemoglobin A1C. Side effects include respiratory tract infections (in elderly), rashes, and diarrhea, and muscle spasms.177
Additional GLP-1 RAs
Oral formulations of GLP-1 RAs with absorption enhancers have been developed, with semaglutide (Rybelsus) currently approved for management of diabetes mellitus.156 To investigate weight loss, the OASIS trials pursued higher doses of up to 50 mg daily, which led to up to −15.1% body weight loss vs −2.4% in placebo.179
Orforglipron is a non-peptide oral GLP-1 RA which has completed phase 2 trials and has shown weight reduction ranging from −8.6% to −12.6% along with improved hemoglobin A1C.78,180,181 Danuglipron represents another non-peptide oral GLP-1 RA shown to lead to −8% to −13% weight loss after 32 weeks of treatment.182
Novel subcutaneous GLP-1 RA competitors are also being investigated. Ecnoglutide (XW03), is in phase 3 trials after phase 2 trials showed up to −14.7% TBWL at 26 weeks (80). GZR18 is a novel GLP-1 injection with bi-weekly dosing in phase 2 trials that has demonstrated up to –17.29% TBWL at 30 weeks (CTR20231695).
Glucagon
Glucagon presents an important target for weight management and metabolism. Excess adiposity causes glucagon resistance, and leads to MASLD by reducing lipid metabolism in the liver.183 The glucagon receptor (GCGR) also plays a key role in thermogenesis, or the burning of calories.184 Thus, changes in the incretin signaling process can drive changes in body composition.
Several GLP-1 and glucagon receptor (GCGR) co-agonists are in development. Phase 3 trials of Mazdutide showed −14.0% TBWL vs 0.3% body weight gain in placebo group at 48 weeks.185 Survodutide has also demonstrated an average TBWL of −14.9% vs −2.8% on placebo after 46 weeks.186 Treatment was also associated with improvement in MASH with no worsening of fibrosis after 48 weeks treatment.187 Phase 3 trials are ongoing to assess survodutide for obesity and MASH.188
Triple Agonism
Given the additive effect of GCGR agonism to GLP-1 agonism, combining these with GIP agonism presented a novel therapeutic target. One “triple agonist” to GLP-1/GIP/GCGR, retatrutide, is a single peptide conjugated to a fatty diacid moiety that showed a mean TWBL in obesity of −24.2% vs −2.1% in placebo after 48 weeks,84 with significant reductions in liver fat after 24 weeks.189 Adverse events were frequent and most commonly GI related. Phase 3 trials for obesity, diabetes mellitus, and cardiovascular outcomes are currently ongoing.
Amylin
Pramlintide is a synthetic amylin analog approved for management of diabetes with only modest weight loss.190 Cagrilintide is a long-acting amylin analog administered once-weekly. Phase 2 trials of the combination of cagrilintide and semaglutide (CagriSema) have shown a synergistic effect on TWBL, showing −15.6% in combined treatment vs −5.1% in semaglutide only after 32 weeks.85
Comparisons of Different Anti-Obesity Medications
Few studies have evaluated the medications detailed above in head-to-head comparisons, which remains an area of investigation. The STEP-8 RCT found greater weight loss with semaglutide than with liraglutide at 68 weeks (Table 3).74
Comparisons of tirzepatide to semaglutide head-to-head remain limited to few studies.169,191,192 However, both the randomized clinical trial of Frias et al from 2021169 and the Bayesian meta-analysis of Ding et al from 2024191 did not evaluate the maximum dose of semaglutide, but rather the 1 mg weekly dosing. Results from the SURMOUNT-5 RCT are anticipated to be available this year and will reflect a direct comparison of tirzepatide 15 mg and semaglutide 2.4 mg weekly.193
One head-to-head trial compared orlistat to liraglutide at up to 1 year and found that patients on liraglutide lost −3.8 kg more than those on orlistat.144
Treatment Adjuncts to Pharmacological Agents in Obesity
A proposed framework for treating obesity is outlined in Figure 4. When starting individuals on anti-obesity treatment, we recommend first starting to ascertain the reasons for which individuals are obese. Readily reversible causes and causative medications should be evaluated and addressed.194 All patients benefit from dietary and lifestyle modification:66 reducing caloric intake to 1200–1500 or 1500–1800 calories per day for women and men respectively,195 with incorporation of moderate-intensity exercise of 150 minutes per week.196 Administration of anti-obesity medications alone, without incorporating lifestyle treatments limits effectiveness and fails to provide the lifelong changes needed to promote weight maintenance.197 Failing to address the role of dietary changes and exercise adoption when treating obesity would not be within the ethical guidelines of most societies. Medications are not without side effects, and providers must always weigh potential risks and benefits prior to prescription.198
 |
Figure 4 A proposed treatment scheme for anti-obesity medications. |
Our practice aims to personalize the treatment for obesity to each patient (Figure 4). Certain patients tend to get hungry quickly after meals, or have abnormal postprandial satiety and may benefit from medications that slow gastrointestinal transit such as the GLP-1 RAs.199 Those with diabetes also benefit greater from GLP-1 RAs and tirzepatide given the positive effects on insulin sensitivity. Patients who require more calories to feel full at any one meal may benefit from the effects on satiation signaling observed with phentermine-topiramate.200 Individuals with binge-eating traits or anxiety disorders may benefit from NB over other therapies.120
Bariatric surgery has been one of the longest-studied treatments for obesity, with up to 25–30% TBWL after Roux-en-Y gastric bypass and 18–20% TBWL after sleeve gastrectomy, and recent research shows that weight regain is associated with increased morbidity and mortality.31,201 Endoscopic procedures have presented a novel alternative for weight loss, showing up to 15% TBWL at 1 year.202 The positioning of pharmacologic therapies relative to bariatric and endoscopic procedures remains to be determined.
Assessment of Pharmacologic Response to Selected Strategies
It is important to evaluate treatment response shortly after starting pharmacologic treatment for obesity early to ensure effectiveness. Patients who are likely to demonstrate long-term response to GLP-1 RAs will likely lose a significant amount of weight within the first month.203–205
Patients who fail to lose weight on treatment initiation should be evaluated for side effects, cost, or other factors impairing medication adherence. If side effects are unbearable, or they truly do not respond well it is reasonable to pursue a medication with an alternative pharmacological action.206,207
One important aspect of GLP-1 RA use is weight regain that occurs with stopping the medication.75,208,209 Strategies to combat this weight loss include aggressive dietary management, cognitive behavioral therapy, and switching to different anti-obesity medications.210–212
When switching from one once-weekly GLP-1 RA to another, it is ideal to stop the current GLP-1 RA, then begin the new GLP-1 RA one week later. It is recommend to restart the new GLP-1 RA at a reduced dose and titrate to the maximum tolerated dose, since side effects are more likely if starting immediately at the higher dose.213 When switching between GLP-1 RAs, providers should meet with patients within 2–3 months to assess for side effects and monitor for treatment efficacy.
The duration of the use of pharmacological agents including incretin agonists for longer than 68 weeks is not based on clinical trial evidence and requires full discussion between the patient and provider. The risks of weight regain compared to continued incretin agonist use should be evaluated, and dietary and lifestyle modifications should play an instrumental role in preventing weight regain in those who discontinue incretin agonists. Weight loss can also alter pharmacokinetics of many medications, and medication doses may require adjustment in patients receiving these medications.214
Economic Analysis of Pharmacotherapy
Many of the newer agents discussed in this review are not without high cost. The cost of novel GLP-1 agonists can be between $10-20,000 annually. Economic analysis comparing different anti-obesity medications has found inconclusive evidence of cost-effectiveness of semaglutide and liraglutide, with some support suggesting phentermine and orlistat are cost-effective.215 When comparing anti-obesity medications to bariatric surgery, multiple analysis have shown that bariatric surgery is more cost-effective than pharmacologic therapies, particularly the GLP-1 RAs.216 Additionally, it remains to be determined if reimbursement modules should vary based upon severity of an individual patient’s obesity. As further treatments are developed, additional analyses into cost effectiveness are certainly warranted.
Conclusion
The realm of pharmacologic treatments for obesity continues to expand rapidly. With the development of additional incretin agonists, we can expect the range of options for obesity and related comorbidities to improve dramatically. Further investigations are needed to address long-term use of incretin agonists and to provide recommendations for prevention of weight regain.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Dr. Camilleri: Stock options for consulting with Dignify Therapeutics and Phenomix. Research grants from Biocodex, Brightseed Bio, NGM Biopharmaceuticals, Pfizer, and Vanda. Consulting with Alfasigma, Amylyx Pharmaceuticals, BioKier, Brightseed Bio, Coloplast, Intercept Pharmaceuticals, Invea Therapeutics, Kallyope (fee to Mayo Clinic), Medpace, Monteresearch S.r.L., Neurogastrx, Renexxion, SKYE Bioscience, Sumitomo Pharmaceuticals, Synlogic, and McDermott Will & Emery LLP. Dr. Acosta: Gila Therapeutics and Phenomix Sciences have licensed Dr. Acosta’s research technologies from University of Florida and Mayo Clinic. Consultant Fees in the last 5 years from Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, Regeneron, Boehringer Ingelheim, Novo Nordisk, Currax, Structure Pharmaceutical, Eli Lilly, Nestle, Phenomix Sciences, Busch Health, RareDiseases. Funding support from the National Institute of Health, Vivus Pharmaceuticals, Novo-Nordisk, Apollo Endosurgery, Satiogen Pharmaceuticals, Spatz Medical, Rhythm Pharmaceuticals, Regeneron, Boehringer Ingelheim, Novo Nordisk. Dr. Acosta also reports issued patents licensed from Mayo Clinic to Phenomix Sciences and from the University of Florida to Gila Therapeutics for “Obesity Phenotyping” and “Sublingual PYY and GLP1”, respectively. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Obesity and Overweight. 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
2. Obesity and severe obesity prevalence in adults: United States, August 2021–August 2023, https://dx.doi.org/10.15620/cdc/159281. 2024. Available from: https://stacks.cdc.gov/view/cdc/159281.
3. Ward ZJ, Bleich SN, Long MW, Gortmaker SL. Association of body mass index with health care expenditures in the United States by age and sex. PLoS One. 2021;16(3):e0247307. doi:10.1371/journal.pone.0247307
4. Rubino F, Cummings DE, Eckel RH, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13(3):221–262. doi:10.1016/S2213-8587(24)00316-4
5. World Health Organization. Obesity: preventing and managing the global epidemic. World Health Organ Tech Rep Ser. 2000;894(i–xii):1–253.
6. Tan TC. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
7. Cornier M-A, Després J-P, Davis N, et al. Assessing Adiposity. Circulation. 2011;124(18):1996–2019. doi:10.1161/CIR.0b013e318233bc6a
8. Chaves L, Gonçalves TJM, Bitencourt AGV, Rstom RA, Pereira TR, Velludo SF. Assessment of body composition by whole-body densitometry: what radiologists should know. Radiol Bras. 2022;55(5):305–311. doi:10.1590/0100-3984.2021.0155-en
9. Zhang QH, Xie LH, Zhang HN, et al. Magnetic resonance imaging assessment of abdominal ectopic fat deposition in correlation with cardiometabolic risk factors. Front Endocrinol. 2022;13:820023. doi:10.3389/fendo.2022.820023
10. Borga M, West J, Bell JD, et al. Advanced body composition assessment: from body mass index to body composition profiling. J Invest Med. 2018;66(5):1–9. doi:10.1136/jim-2018-000722
11. Rådholm K, Tengblad A, Dahlén E, et al. The impact of using sagittal abdominal diameter to predict major cardiovascular events in European patients with type 2 diabetes. Nutr Metab Cardiovasc Dis. 2017;27(5):418–422. doi:10.1016/j.numecd.2017.02.001
12. Kahn HS. Replacing the body mass index with the sagittal abdominal diameter (abdominal height). Obesity. 2023;31(11):2720–2722. doi:10.1002/oby.23889
13. Potter AW, Chin GC, Looney DP, Friedl KE. Defining overweight and obesity by percent body fat instead of body mass index. J Clin Endocrinol Metab. 2024;110(4):e1103–7. doi:10.1210/clinem/dgae341
14. Dehghan M, Merchant AT. Is bioelectrical impedance accurate for use in large epidemiological studies? Nutr J. 2008;7(1):26. doi:10.1186/1475-2891-7-26
15. Reaven GM. Insulin resistance: the link between obesity and cardiovascular disease. Endocrinol Metab Clinics North Am. 2008;37(3):581–601. doi:10.1016/j.ecl.2008.06.005
16. Karaouzene N, Merzouk H, Aribi M, et al. Effects of the association of aging and obesity on lipids, lipoproteins and oxidative stress biomarkers: a comparison of older with young men. Nutr Metab Cardiovasc Dis. 2011;21(10):792–799. doi:10.1016/j.numecd.2010.02.007
17. Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–1428. doi:10.1016/S0140-6736(05)66378-7
18. Després J-P, Lemieux I. Abdominal obesity and metabolic syndrome. Nature. 2006;444(7121):881–887. doi:10.1038/nature05488
19. Lorenzo C, Okoloise M, Williams K, Stern MP, Haffner SM. The metabolic syndrome as predictor of type 2 diabetes: the san antonio heart study. Diabetes Care. 2003;26(11):3153–3159. doi:10.2337/diacare.26.11.3153
20. Bhaskaran K, Douglas I, Forbes H, dos-Santos-Silva I, Leon DA, Smeeth L. Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5·24 million UK adults. Lancet. 2014;384(9945):755–765. doi:10.1016/S0140-6736(14)60892-8
21. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008;371(9612):569–578. doi:10.1016/S0140-6736(08)60269-X
22. Pillar G, Shehadeh N. Abdominal fat and sleep apnea: the chicken or the egg? Diabetes Care. 2008;31(Supplement_2):S303–S309. doi:10.2337/dc08-s272
23. Wolk R, Shamsuzzaman AS, Somers VK. Obesity, sleep apnea, and hypertension. Hypertension. 2003;42(6):1067–1074. doi:10.1161/01.HYP.0000101686.98973.A3
24. Anderson JJ, Felson DT. Factors associated with osteoarthritis of the knee in the first national Health and nutrition examination survey (HANES I). Evidence for an association with overweight, race, and physical demands of work. Am J Epidemiol. 1988;128(1):179–189. doi:10.1093/oxfordjournals.aje.a114939
25. Beuther DA, Sutherland ER. Overweight, obesity, and incident asthma: a meta-analysis of prospective epidemiologic studies. Am J Respir Crit Care Med. 2007;175(7):661–666. doi:10.1164/rccm.200611-1717OC
26. Hunskaar S. A systematic review of overweight and obesity as risk factors and targets for clinical intervention for urinary incontinence in women. Neurourol Urodynamics. 2008;27(8):749–757. doi:10.1002/nau.20635
27. Chiu S, Birch DW, Shi X, Sharma AM, Karmali S. Effect of sleeve gastrectomy on gastroesophageal reflux disease: a systematic review. Surg Obesity Related Dis. 2011;7(4):510–515. doi:10.1016/j.soard.2010.09.011
28. Luppino FS, de Wit LM, Bouvy PF, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. 2010;67(3):220–229. doi:10.1001/archgenpsychiatry.2010.2
29. Bugianesi E, Leone N, Vanni E, et al. Expanding the natural history of nonalcoholic steatohepatitis: from cryptogenic cirrhosis to hepatocellular carcinoma. Gastroenterology. 2002;123(1):134–140. doi:10.1053/gast.2002.34168
30. Khan SS, Ning H, Wilkins JT, et al. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity. JAMA Cardiol. 2018;3(4):280–287. doi:10.1001/jamacardio.2018.0022
31. Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation. 2014;129(25_suppl_2):S102–S138. doi:10.1161/01.cir.0000437739.71477.ee
32. Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and cardiovascular disease: a scientific statement from the American heart association. Circulation. 2021;143(21):e984–e1010. doi:10.1161/CIR.0000000000000973
33. Acosta A, Camilleri M, Shin A, et al. Quantitative gastrointestinal and psychological traits associated with obesity and response to weight-loss therapy. Gastroenterology. 2015;148(3):537–546.e4. doi:10.1053/j.gastro.2014.11.020
34. Freire R. Scientific evidence of diets for weight loss: different macronutrient composition, intermittent fasting, and popular diets. Nutrition. 2020;69:110549. doi:10.1016/j.nut.2019.07.001
35. Garvey WT, Mechanick JI, Brett EM, et al. American association of clinical endocrinologists and American college of endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22:1–203. doi:10.4158/EP161365.GL
36. Conaty EA, Denham W, Haggerty SP, Linn JG, Joehl RJ, Ujiki MB. Primary care physicians’ perceptions of bariatric surgery and major barriers to referral. Obes Surg. 2020;30(2):521–526. doi:10.1007/s11695-019-04204-9
37. Surgery ASfMaB. Estimate of bariatric surgery numbers, 2011-2022. Available from: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers/.
38. Elmaleh-Sachs A, Schwartz JL, Bramante CT, Nicklas JM, Gudzune KA, Jay M. Obesity management in adults: a review. JAMA. 2023;330(20):2000–2015. doi:10.1001/jama.2023.19897
39. Melson E, Ashraf U, Papamargaritis D, Davies MJ. What is the pipeline for future medications for obesity? Int J Obesity. 2025;49(3):433–451. doi:10.1038/s41366-024-01473-y
40. Lupianez-Merly C, Dilmaghani S, Vosoughi K, Camilleri M. Review article: pharmacologic management of obesity - updates on approved medications, indications and risks. Aliment Pharmacol Ther. 2024;59(4):475–491. doi:10.1111/apt.17856
41. Camilleri M. Incretin impact on gastric function in obesity: physiology, and pharmacological, surgical and endoscopic treatments. J Physiol. 2024. doi:10.1113/JP287535
42. Sternson SM, Eiselt AK. Three pillars for the neural control of appetite. Annu Rev Physiol. 2017;79(1):401–423. doi:10.1146/annurev-physiol-021115-104948
43. Schwartz MW, Woods SC, Porte D, Seeley RJ, Baskin DG. Central nervous system control of food intake. Nature. 2000;404(6778):661–671. doi:10.1038/35007534
44. Campos CA, Bowen AJ, Schwartz MW, Palmiter RD. Parabrachial CGRP neurons control meal termination. Cell Metab. 2016;23(5):811–820. doi:10.1016/j.cmet.2016.04.006
45. Petrovich GD, Setlow B, Holland PC, Gallagher M. Amygdalo-hypothalamic circuit allows learned cues to override satiety and promote eating. J Neurosci. 2002;22(19):8748–8753. doi:10.1523/jneurosci.22-19-08748.2002
46. Gillis RA, Dezfuli G, Bellusci L, Vicini S, Sahibzada N. Brainstem neuronal circuitries controlling gastric tonic and phasic contractions: a review. Cell Mol Neurobiol. 2022;42(2):333–360. doi:10.1007/s10571-021-01084-5
47. Mason BL, Wang Q, Zigman JM. The central nervous system sites mediating the orexigenic actions of ghrelin. Annu Rev Physiol. 2014;76(1):519–533. doi:10.1146/annurev-physiol-021113-170310
48. Suzuki K, Simpson KA, Minnion JS, Shillito JC, Bloom SR. The role of gut hormones and the hypothalamus in appetite regulation. Endocr J. 2010;57(5):359–372. doi:10.1507/endocrj.K10E-077
49. Coveleskie K, Kilpatrick LA, Gupta A, et al. The effect of the GLP-1 analogue Exenatide on functional connectivity within an NTS-based network in women with and without obesity. Obesity Sci Pract. 2017;3(4):434–445. doi:10.1002/osp4.124
50. Secher A, Jelsing J, Baquero AF, et al. The arcuate nucleus mediates GLP-1 receptor agonist liraglutide-dependent weight loss. J Clin Invest. 2014;124(10):4473–4488. doi:10.1172/jci75276
51. Shah M, Vella A. Effects of GLP-1 on appetite and weight. Rev Endocr Metab Disord. 2014;15(3):181–187. doi:10.1007/s11154-014-9289-5
52. Camilleri M. Peripheral mechanisms in appetite regulation. Gastroenterology. 2015;148(6):1219–1233. doi:10.1053/j.gastro.2014.09.016
53. Cypess AM. Reassessing Human Adipose Tissue. N Engl J Med. 2022;386(8):768–779. doi:10.1056/NEJMra2032804
54. Taylor EB. The complex role of adipokines in obesity, inflammation, and autoimmunity. Clin Sci. 2021;135(6):731–752. doi:10.1042/cs20200895
55. Berne C; Group tOSTdS. A randomized study of orlistat in combination with a weight management programme in obese patients with Type 2 diabetes treated with metformin. Diabetic Med. 2005;22(5):612–618. doi:10.1111/j.1464-5491.2004.01474.x
56. Foxcroft DR, Milne R. Orlistat for the treatment of obesity: rapid review and cost-effectiveness model. Obesity Rev. 2000;1(2):121–126. doi:10.1046/j.1467-789x.2000.00011.x
57. LeBlanc ES, OConnor E, Whitlock EP, et al. Effectiveness of primary care-relevant treatments for obesity in adults a systematic evidence review for the U.S. Preventive Services TAsk Force. Ann Intern Med. 2011;155:434–447. doi:10.7326/0003-4819-155-7-201110040-00006
58. Lewis KH, Fischer H, Ard J, et al. Safety and effectiveness of longer-term phentermine use: clinical outcomes from an electronic health record cohort. Obesity. 2019;27(4):591–602. doi:10.1002/oby.22430
59. Allison DB, Gadde KM, Garvey WT, et al. Controlled-release phentermine/topiramate in severely obese adults: a randomized controlled trial (EQUIP). Obesity. 2012;20(2):330–342. doi:10.1038/oby.2011.330
60. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9774):1341–1352. doi:10.1016/S0140-6736(11)60205-5
61. Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595–605. doi:10.1016/S0140-6736(10)60888-4
62. Wadden TA, Foreyt JP, Foster GD, et al. Weight loss with naltrexone SR/bupropion SR combination therapy as an adjunct to behavior modification: the COR-BMOD trial. Obesity. 2011;19(1):110–120. doi:10.1038/oby.2010.147
63. Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11–22. doi:10.1056/NEJMoa1411892
64. Davies MJ, Bergenstal R, Bode B, et al. Efficacy of liraglutide for weight loss among patients with type 2 diabetes: the scale diabetes randomized clinical trial. JAMA. 2015;314(7):687–699. doi:10.1001/jama.2015.9676
65. Kushner RF, Calanna S, Davies M, et al. Semaglutide 2.4 mg for the Treatment of Obesity: key Elements of the STEP Trials 1 to 5. Obesity. 2020;28(6):1050–1061. doi:10.1002/oby.22794
66. Grunvald E, Shah R, Hernaez R, et al. AGA clinical practice guideline on pharmacological interventions for adults with obesity. Gastroenterology. 2022;163(5):1198–1225. doi:10.1053/j.gastro.2022.08.045
67. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205–216. doi:10.1056/NEJMoa2206038
68. Wadden TA, Chao AM, Machineni S, et al. Tirzepatide after intensive lifestyle intervention in adults with overweight or obesity: the SURMOUNT-3 phase 3 trial. Nat Med. 2023;29(11):2909–2918. doi:10.1038/s41591-023-02597-w
69. Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2023;402(10402):613–626. doi:10.1016/S0140-6736(23)01200-X
70. Torgerson JS, Hauptman J, Boldrin MN, Sjöström L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155–161. doi:10.2337/diacare.27.1.155
71. Kang JG, Park CY, Kang JH, Park YW, Park SW. Randomized controlled trial to investigate the effects of a newly developed formulation of phentermine diffuse-controlled release for obesity. Diabetes Obes Metab. 2010;12(10):876–882. doi:10.1111/j.1463-1326.2010.01242.x
72. Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297–308. doi:10.3945/ajcn.111.024927
73. Apovian CM, Aronne L, Rubino D, et al. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity. 2013;21(5):935–943. doi:10.1002/oby.20309
74. Rubino DM, Greenway FL, Khalid U, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes: the STEP 8 randomized clinical trial. JAMA. 2022;327(2):138–150. doi:10.1001/jama.2021.23619
75. Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325(14):1414–1425. doi:10.1001/jama.2021.3224
76. Dahl D, Onishi Y, Norwood P, et al. Effect of subcutaneous tirzepatide vs placebo added to titrated insulin glargine on glycemic control in patients with type 2 diabetes: the SURPASS-5 randomized clinical trial. JAMA. 2022;327(6):534–545. doi:10.1001/jama.2022.0078
77. Heymsfield SB, Coleman LA, Miller R, et al. Effect of bimagrumab vs placebo on body fat mass among adults with type 2 diabetes and obesity: a phase 2 randomized clinical trial. JAMA Network Open. 2021;4(1):e2033457–e2033457. doi:10.1001/jamanetworkopen.2020.33457
78. Wharton S, Blevins T, Connery L, et al. Daily oral GLP-1 receptor agonist orforglipron for adults with obesity. N Engl J Med. 2023;389(10):877–888. doi:10.1056/NEJMoa2302392
79. Harris E. Oral semaglutide led to similar weight loss as injection, company says. JAMA. 2023;329(23):2011. doi:10.1001/jama.2023.9601
80. Zhu Z, Li Y, Zheng Q, et al. 79-LB: an open-label, active-controlled phase 2 evaluation of novel GLP-1 analog ecnoglutide in adults with obesity. Diabetes. 2023;72(Supplement_1). doi:10.2337/db23-79-LB
81. Ji L, Jiang H, Cheng Z, et al. A phase 2 randomised controlled trial of mazdutide in Chinese overweight adults or adults with obesity. Nat Commun. 2023;14(1):8289. doi:10.1038/s41467-023-44067-4
82. Aronne L, Harris MS, Roberts MS, et al. Pemvidutide, a GLP-1/glucagon dual receptor agonist, in subjects with overweight or obesity-A 48-week, placebo-controlled, phase 2 (MOMENTUM) trial. Diabetes. 2024;73(Supplement_1). doi:10.2337/db24-262-OR
83. Amgen announces robust weight loss with maritide in people living with obesity or overweight at 52 weeks in a Phase 2 study. 2024. Available from: https://www.amgen.com/newsroom/press-releases/2024/11/amgen-announces-robust-weight-loss-with-maritide-in-people-living-with-obesity-or-overweight-at-52-weeks-in-a-phase-2-study.
84. Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–hormone-receptor agonist retatrutide for obesity — a phase 2 trial. N Engl J Med. 2023;389(6):514–526. doi:10.1056/NEJMoa2301972
85. Frias JP, Deenadayalan S, Erichsen L, et al. Efficacy and safety of co-administered once-weekly cagrilintide 2.4 mg with once-weekly semaglutide 2.4 mg in type 2 diabetes: a multicentre, randomised, double-blind, active-controlled, phase 2 trial. Lancet. 2023;402(10403):720–730. doi:10.1016/S0140-6736(23)01163-7
86. Administration USFD. Orlistat (marketed as Alli and Xenical) Information. Available from: https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/orlistat-marketed-alli-and-xenical-information.
87. Davidson MH, Hauptman J, DiGirolamo M, et al. Weight control and risk factor reduction in obese subjects treated for 2 years with orlistata randomized controlled trial. JAMA. 1999;281(3):235–242. doi:10.1001/jama.281.3.235
88. Rössner S, Sjöström L, Noack R, Meinders AE, Noseda G; Study obotEOO. Weight loss, weight maintenance, and improved cardiovascular risk factors after 2 years treatment with orlistat for obesity. Obesity Res. 2000;8(1):49–61. doi:10.1038/oby.2000.8
89. Sahebkar A, Simental-Mendía LE, Kovanen PT, Pedone C, Simental-Mendía M, Cicero AFG. Effects of orlistat on blood pressure: a systematic review and meta-analysis of 27 randomized controlled clinical trials. J Am Soc Hypertens. 2018;12(2):80–96. doi:10.1016/j.jash.2017.12.002
90. Sahebkar A, Simental-Mendía LE, Reiner Ž, et al. Effect of orlistat on plasma lipids and body weight: a systematic review and meta-analysis of 33 randomized controlled trials. Pharmacol Res. 2017;122:53–65. doi:10.1016/j.phrs.2017.05.022
91. Broom I, Wilding J, Stott P, Myers N; Group UKMS. Randomised trial of the effect of orlistat on body weight and cardiovascular disease risk profile in obese patients: UK multimorbidity study. Int J Clin Pract. 2002;56(7):494–499. doi:10.1111/j.1742-1241.2002.tb11307.x
92. Swinburn BA, Carey D, Hills AP, et al. Effect of orlistat on cardiovascular disease risk in obese adults. Diabetes Obes Metab. 2005;7(3):254–262. doi:10.1111/j.1463-1326.2004.00467.x
93. Ardissino M, Vincent M, Hines O, et al. Long-term cardiovascular outcomes after orlistat therapy in patients with obesity: a nationwide, propensity-score matched cohort study. Eur Heart J Cardiovasc Pharmacother. 2021;8(2):179–186. doi:10.1093/ehjcvp/pvaa133
94. Pavli P, Triantafyllidou O, Kapantais E, Vlahos NF, Valsamakis G. Infertility improvement after medical weight loss in women and men: a review of the literature. Int J Mol Sci. 2024;25(3):1909. doi:10.3390/ijms25031909
95. Hsia DS, Gosselin NH, Williams J, et al. A randomized, double-blind, placebo-controlled, pharmacokinetic and pharmacodynamic study of a fixed-dose combination of phentermine/topiramate in adolescents with obesity. Diabetes Obes Metab. 2020;22(4):480–491. doi:10.1111/dom.13910
96. Winokur A, Halseth A, Dybala C, Lam H, Chen S, Chalasani NP. Naltrexone/Bupropion Extended-Release 32 mg/360 mg significantly improves liver enzymes in obese/overweight individuals with elevated liver enzymes. Wiley-Blackwell 111 River St, Hoboken 07030-5774, NJ USA. 2015;1268A.
97. Armstrong MJ, Gaunt P, Aithal GP, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet. 2016;387(10019):679–690. doi:10.1016/S0140-6736(15)00803-X
98. Mann JFE, Ørsted DD, Brown-Frandsen K, et al. Liraglutide and renal outcomes in type 2 diabetes. N Engl J Med. 2017;377(9):839–848. doi:10.1056/NEJMoa1616011
99. Sattar N, Lee MMY, Kristensen SL, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021;9(10):653–662. doi:10.1016/S2213-8587(21)00203-5
100. Blackman A, Foster GD, Zammit G, et al. Effect of liraglutide 3.0 mg in individuals with obesity and moderate or severe obstructive sleep apnea: the SCALE Sleep Apnea randomized clinical trial. Int J Obesity. 2016;40(8):1310–1319. doi:10.1038/ijo.2016.52
101. Gudbergsen H, Overgaard A, Henriksen M, et al. Liraglutide after diet-induced weight loss for pain and weight control in knee osteoarthritis: a randomized controlled trial. Am J Clin Nutrition. 2021;113(2):314–323. doi:10.1093/ajcn/nqaa328
102. Newsome PN, Buchholtz K, Cusi K, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J Med. 2021;384(12):1113–1124. doi:10.1056/NEJMoa2028395
103. Perkovic V, Tuttle KR, Rossing P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med. 2024;391(2):109–121. doi:10.1056/NEJMoa2403347
104. Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221–2232. doi:10.1056/NEJMoa2307563
105. Kosiborod MN, Deanfield J, Pratley R, et al. Semaglutide versus placebo in patients with heart failure and mildly reduced or preserved ejection fraction: a pooled analysis of the SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM randomised trials. Lancet. 2024;404(10456):949–961. doi:10.1016/s0140-6736(24)01643-x
106. Bliddal H, Bays H, Czernichow S, et al. Once-weekly semaglutide in persons with obesity and knee osteoarthritis. N Engl J Med. 2024;391(17):1573–1583. doi:10.1056/NEJMoa2403664
107. Loomba R, Hartman ML, Lawitz EJ, et al. Tirzepatide for metabolic dysfunction–associated steatohepatitis with liver fibrosis. N Engl J Med. 2024;391(4):299–310. doi:10.1056/NEJMoa2401943
108. Bosch C, Carriazo S, Soler MJ, Ortiz A, Fernandez-Fernandez B. Tirzepatide and prevention of chronic kidney disease. Clin Kidney J. 2022;16(5):797–808. doi:10.1093/ckj/sfac274
109. Chuang M-H, Chen J-Y, Wang H-Y, Jiang Z-H, Wu V-C. Clinical outcomes of tirzepatide or GLP-1 receptor agonists in individuals with type 2 diabetes. JAMA Network Open. 2024;7(8):e2427258–e2427258. doi:10.1001/jamanetworkopen.2024.27258
110. Packer M, Zile MR, Kramer CM, et al. Tirzepatide for heart failure with preserved ejection fraction and obesity. N Engl J Med. 2024;392(5):427–437. doi:10.1056/NEJMoa2410027
111. Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the treatment of obstructive sleep apnea and obesity. N Engl J Med. 2024;391(13):1193–1205. doi:10.1056/NEJMoa2404881
112. Ryan D, Bray G. Sibutramine, phentermine, and diethylpropion sympathomimetic drugs in the management of obesity. In: Handbook of Obesity - Volume 2: Clinical Applications.
113. Baumann MH, Ayestas MA, Dersch CM, Brockington A, Rice KC, Rothman RB. Effects of phentermine and fenfluramine on extracellular dopamine and serotonin in rat nucleus accumbens: therapeutic implications. Synapse. 2000;36(2):102–113. doi:10.1002/(sici)1098-2396(200005)36:2<102::Aid-syn3>3.0.Co;2-%23
114. Nelson DL, Gehlert DR. Central nervous system biogenic amine targets for control of appetite and energy expenditure. Endocrine. 2006;29(1):49–60. doi:10.1385/ENDO:29:1:49
115. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. JAMA. 2014;311(1):74–86. doi:10.1001/jama.2013.281361
116. Prasad M, El Sabbagh A, Rihal C, Lerman A. Phentermine and coronary vasospasm–induced myocardial infarction. Mayo Clin Proc. 2019;94(7):1374–1377. doi:10.1016/j.mayocp.2018.08.029
117. Kim KK, Cho HJ, Kang HC, Youn BB, Lee KR. Effects on weight reduction and safety of short-term phentermine administration in Korean obese people. Yonsei Med J. 2006;47(5):614–625. doi:10.3349/ymj.2006.47.5.614
118. Kramer CK, Leitão CB, Pinto LC, Canani LH, Azevedo MJ, Gross JL. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obesity Rev. 2011;12(5):e338–e347. doi:10.1111/j.1467-789X.2010.00846.x
119. White HS. Molecular pharmacology of topiramate: managing seizures and preventing migraine. Headache. 2005;45(s1):S48–S56. doi:10.1111/j.1526-4610.2005.4501006.x
120. Acosta A, Camilleri M, Abu Dayyeh B, et al. Selection of antiobesity medications based on phenotypes enhances weight loss: a pragmatic trial in an obesity clinic. Obesity. 2021;29(4):662–671. doi:10.1002/oby.23120
121. Sinnayah P, Wallingford N, Evans A, Cowley MA. Bupropion and naltrexone interact synergistically to decrease food intake in mice. Obesity. 2007;15(9):A179.
122. Greenway FL, Whitehouse MJ, Guttadauria M, et al. Rational design of a combination medication for the treatment of obesity. Obesity. 2009;17(1):30–39. doi:10.1038/oby.2008.461
123. Hasegawa H, Meeusen R, Sarre S, Diltoer M, Piacentini MF, Michotte Y. Acute dopamine/norepinephrine reuptake inhibition increases brain and core temperature in rats. J Appl Physiol. 2005;99(4):1397–1401. doi:10.1152/japplphysiol.00435.2005
124. Billes SK, Cowley MA. Inhibition of dopamine and norepinephrine reuptake produces additive effects on energy balance in lean and obese mice. Neuropsychopharmacology. 2007;32(4):822–834. doi:10.1038/sj.npp.1301155
125. Nissen SE, Wolski KE, Prcela L, et al. Effect of naltrexone-bupropion on major adverse cardiovascular events in overweight and obese patients with cardiovascular risk factors: a randomized clinical trial. JAMA. 2016;315(10):990–1004. doi:10.1001/jama.2016.1558
126. Moawad MH-E, Sadeq MA, Abbas A, et al. Efficacy of naltrexone/bupropion in treatment of binge eating: a systematic review and meta-analysis. Psychiatry Int. 2024;5(3):323–337. doi:10.3390/psychiatryint5030022
127. Administration USFD. IMCIVREE® (setmelanotide) injection, for subcutaneous use initial U.S. approval: 2020. 2024. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/213793s007lbl.pdf.
128. Blüher S, Ziotopoulou M, Bullen JW, et al. Responsiveness to peripherally administered melanocortins in lean and obese mice. Diabetes. 2004;53(1):82–90. doi:10.2337/diabetes.53.1.82
129. Clément K, van den Akker E, Argente J, et al. Efficacy and safety of setmelanotide, an MC4R agonist, in individuals with severe obesity due to LEPR or POMC deficiency: single-arm, open-label, multicentre, phase 3 trials. Lancet Diabetes Endocrinol. 2020;8(12):960–970. doi:10.1016/s2213-8587(20)30364-8
130. Roth CL, Scimia C, Shoemaker AH, et al. Setmelanotide for the treatment of acquired hypothalamic obesity: a phase 2, open-label, multicentre trial. Lancet Diabetes Endocrinol. 2024;12(6):380–389. doi:10.1016/s2213-8587(24)00087-1
131. Haqq AM, Chung WK, Dollfus H, et al. Efficacy and safety of setmelanotide, a melanocortin-4 receptor agonist, in patients with Bardet-Biedl syndrome and Alström syndrome: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial with an open-label period. Lancet Diabetes Endocrinol. 2022;10(12):859–868. doi:10.1016/s2213-8587(22)00277-7
132. Maselli DB, Camilleri M. Effects of GLP-1 and its analogs on gastric physiology in diabetes mellitus and obesity. Adv Exp Med Biol. 2021;1307:171–192. doi:10.1007/5584_2020_496
133. Jalleh RJ, Marathe CS, Rayner CK, et al. Physiology and pharmacology of effects of GLP-1-based therapies on gastric, biliary and intestinal motility. Endocrinology. 2024;166(1). doi:10.1210/endocr/bqae155
134. Verdich C, Flint A, Gutzwiller JP, et al. A meta-analysis of the effect of glucagon-like peptide-1 (7-36) amide on ad libitum energy intake in humans. J Clin Endocrinol Metab. 2001;86(9):4382–4389. doi:10.1210/jcem.86.9.7877
135. Larsen PJ, Tang-Christensen M, Holst JJ, Orskov C. Distribution of glucagon-like peptide-1 and other preproglucagon-derived peptides in the rat hypothalamus and brainstem. Neuroscience. 1997;77(1):257–270. doi:10.1016/s0306-4522(96)00434-4
136. Hayes MR, Bradley L, Grill HJ. Endogenous hindbrain glucagon-like peptide-1 receptor activation contributes to the control of food intake by mediating gastric satiation signaling. Endocrinology. 2009;150(6):2654–2659. doi:10.1210/en.2008-1479
137. Zhao S, Kanoski SE, Yan J, Grill HJ, Hayes MR. Hindbrain leptin and glucagon-like-peptide-1 receptor signaling interact to suppress food intake in an additive manner. Int J Obes Lond. 2012;36(12):1522–1528. doi:10.1038/ijo.2011.265
138. Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet. 2006;368(9548):1696–1705. doi:10.1016/S0140-6736(06)69705-5
139. Halawi H, Khemani D, Eckert D, et al. Effects of liraglutide on weight, satiation, and gastric functions in obesity: a randomised, placebo-controlled pilot trial. Lancet Gastroenterol Hepatol. 2017;2(12):890–899. doi:10.1016/s2468-1253(17)30285-6
140. Maselli D, Atieh J, Clark MM, et al. Effects of liraglutide on gastrointestinal functions and weight in obesity: a randomized clinical and pharmacogenomic trial. Obesity. 2022;30(8):1608–1620. doi:10.1002/oby.23481
141. Tschöp M, Nogueiras R, Ahrén B. Gut hormone-based pharmacology: novel formulations and future possibilities for metabolic disease therapy. Diabetologia. 2023;66(10):1796–1808. doi:10.1007/s00125-023-05929-0
142. Damholt B, Golor G, Wierich W, Pedersen P, Ekblom M, Zdravkovic M. An open-label, parallel group study investigating the effects of age and gender on the pharmacokinetics of the once-daily glucagon-like peptide-1 analogue liraglutide. J Clin Pharmacol. 2006;46(6):635–641. doi:10.1177/0091270006288215
143. Astrup A, Rössner S, Van Gaal L, et al. Effects of liraglutide in the treatment of obesity: a randomised, double-blind, placebo-controlled study. Lancet. 2009;374(9701):1606–1616. doi:10.1016/s0140-6736(09)61375-1
144. Astrup A, Carraro R, Finer N, et al. Safety, tolerability and sustained weight loss over 2 years with the once-daily human GLP-1 analog, liraglutide. Int J Obes Lond. 2012;36(6):843–854. doi:10.1038/ijo.2011.158
145. Wadden TA, Hollander P, Klein S, et al. Weight maintenance and additional weight loss with liraglutide after low-calorie-diet-induced weight loss: the SCALE Maintenance randomized study. Int J Obes. 2013;37(11):1443–1451. doi:10.1038/ijo.2013.120
146. Lau J, Bloch P, Schäffer L, et al. Discovery of the once-weekly glucagon-like peptide-1 (GLP-1) analogue semaglutide. J Med Chem. 2015;58(18):7370–7380. doi:10.1021/acs.jmedchem.5b00726
147. Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102. doi:10.1016/j.molmet.2020.101102
148. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183
149. Bergmann NC, Davies MJ, Lingvay I, Knop FK. Semaglutide for the treatment of overweight and obesity: a review. Diabetes Obes Metab. 2023;25(1):18–35. doi:10.1111/dom.14863
150. Garvey WT, Batterham RL, Bhatta M, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022;28(10):2083–2091. doi:10.1038/s41591-022-02026-4
151. Pratley RE, Tuttle KR, Rossing P, et al. Effects of semaglutide on heart failure outcomes in diabetes and chronic kidney disease in the flow trial. J Am Coll Cardiol. 2024;84(17):1615–1628. doi:10.1016/j.jacc.2024.08.004
152. Deanfield J, Verma S, Scirica BM, et al. Semaglutide and cardiovascular outcomes in patients with obesity and prevalent heart failure: a prespecified analysis of the SELECT trial. Lancet. 2024;404(10454):773–786. doi:10.1016/s0140-6736(24)01498-3
153. Kittipibul V, Mentz RJ. Effects of GLP-1 receptor agonists on heart failure outcomes. J Am College Cardiol. 2024;84(17):1629–1631. doi:10.1016/j.jacc.2024.08.016
154. Khan MS, Fonarow GC, McGuire DK, et al. Glucagon-like peptide 1 receptor agonists and heart failure. Circulation. 2020;142(12):1205–1218. doi:10.1161/CIRCULATIONAHA.120.045888
155. Davies M, Pieber TR, Hartoft-Nielsen M-L, Hansen OKH, Jabbour S, Rosenstock J. Effect of oral semaglutide compared with placebo and subcutaneous semaglutide on glycemic control in patients with type 2 diabetes: a randomized clinical trial. JAMA. 2017;318(15):1460–1470. doi:10.1001/jama.2017.14752
156. Aroda VR, Rosenstock J, Terauchi Y, et al. PIONEER 1: randomized clinical trial of the efficacy and safety of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes. Diabetes Care. 2019;42(9):1724–1732. doi:10.2337/dc19-0749
157. Bruns Vi N, Tressler EH, Vendruscolo LF, Leggio L, Farokhnia M. IUPHAR review – glucagon-like peptide-1 (GLP-1) and substance use disorders: an emerging pharmacotherapeutic target. Pharmacol Res. 2024;207:107312. doi:10.1016/j.phrs.2024.107312
158. Long B, Pelletier J, Koyfman A, Bridwell RE. GLP-1 agonists: a review for emergency clinicians. Am J Emergency Med. 2024;78:89–94. doi:10.1016/j.ajem.2024.01.010
159. Sikirica MV, Martin AA, Wood R, Leith A, Piercy J, Higgins V. Reasons for discontinuation of GLP1 receptor agonists: data from a real-world cross-sectional survey of physicians and their patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2017;10:403–412. doi:10.2147/dmso.S141235
160. Linge J, Birkenfeld AL, Neeland IJ. Muscle mass and glucagon-like peptide-1 receptor agonists: adaptive or maladaptive response to weight loss? Circulation. 2024;150(16):1288–1298. doi:10.1161/CIRCULATIONAHA.124.067676
161. Bezin J, Gouverneur A, Pénichon M, et al. GLP-1 receptor agonists and the risk of thyroid cancer. Diabetes Care. 2022;46(2):384–390. doi:10.2337/dc22-1148
162. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMoa1607141
163. Huang YN, Liao WL, Huang JY, et al. Long-term safety and efficacy of glucagon-like peptide-1 receptor agonists in individuals with obesity and without type 2 diabetes: a global retrospective cohort study. Diabetes Obes Metab. 2024;26(11):5222–5232. doi:10.1111/dom.15869
164. Hayes MR, Borner T, De Jonghe BC. The role of GIP in the regulation of GLP-1 satiety and nausea. Diabetes. 2021;70(9):1956–1961. doi:10.2337/dbi21-0004
165. Borner T, Geisler CE, Fortin SM, et al. GIP receptor agonism attenuates GLP-1 receptor agonist-induced nausea and emesis in preclinical models. Diabetes. 2021;70(11):2545–2553. doi:10.2337/db21-0459
166. Meier JJ, Goetze O, Anstipp J, et al. Gastric inhibitory polypeptide does not inhibit gastric emptying in humans. Am J Physiol Endocrinol Metab. 2004;286(4):E621–5. doi:10.1152/ajpendo.00499.2003
167. Frias JP, Nauck MA, Van J, et al. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: a randomised, placebo-controlled and active comparator-controlled phase 2 trial. Lancet. 2018;392(10160):2180–2193. doi:10.1016/S0140-6736(18)32260-8
168. Ludvik B, Giorgino F, Jódar E, et al. Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomised, open-label, parallel-group, phase 3 trial. Lancet. 2021;398(10300):583–598. doi:10.1016/S0140-6736(21)01443-4
169. Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503–515. doi:10.1056/NEJMoa2107519
170. Del Prato S, Kahn SE, Pavo I, et al. Tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS-4): a randomised, open-label, parallel-group, multicentre, phase 3 trial. Lancet. 2021;398(10313):1811–1824. doi:10.1016/S0140-6736(21)02188-7
171. Rosenstock J, Wysham C, Frías JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial. Lancet. 2021;398(10295):143–155. doi:10.1016/s0140-6736(21)01324-6
172. Administration USFD. MOUNJAROTM (tirzepatide) Injection, for subcutaneous use initial U.S. Approval: 2022. 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215866s000lbl.pdf.
173. Administration USFD. ZEPBOUND™ (tirzepatide) Injection, for subcutaneous use Initial U.S. Approval: 2022. 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217806s000lbl.pdf.
174. Thomsen RW, Mailhac A, Løhde JB, Pottegård A. Real-world evidence on the utilization, clinical and comparative effectiveness, and adverse effects of newer GLP-1RA-based weight-loss therapies. Diabetes Obes Metab. 2025;27 Suppl 2(Suppl 2):66–88. doi:10.1111/dom.16364
175. Raičević BB, Belančić A, Mirković N, Janković SM. Analysis of reporting trends of serious adverse events associated with anti-obesity drugs. Pharmacol Res Perspectives. 2025;13(2):e70080. doi:10.1002/prp2.70080
176. Dolgin E. Dozens of new obesity drugs are coming: these are the ones to watch. Nature. 2025;638(8050):308–310. doi:10.1038/d41586-025-00404-9
177. Rooks D, Petricoul O, Praestgaard J, Bartlett M, Laurent D, Roubenoff R. Safety and pharmacokinetics of bimagrumab in healthy older and obese adults with body composition changes in the older cohort. J Cachexia Sarcopenia Muscle. 2020;11(6):1525–1534. doi:10.1002/jcsm.12639
178. Garito T, Roubenoff R, Hompesch M, et al. Bimagrumab improves body composition and insulin sensitivity in insulin-resistant individuals. Diabetes Obes Metab. 2018;20(1):94–102. doi:10.1111/dom.13042
179. Knop FK, Aroda VR, Do Vale RD, et al. Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023;402(10403):705–719. doi:10.1016/s0140-6736(23)01185-6
180. Nauck MA, Horowitz M. Non-peptide, once-per-day oral orforglipron to compete with established peptide-based, injectable GLP-1 receptor agonists. Lancet. 2023;402(10400):429–431. doi:10.1016/S0140-6736(23)01201-1
181. Frias JP, Hsia S, Eyde S, et al. Efficacy and safety of oral orforglipron in patients with type 2 diabetes: a multicentre, randomised, dose-response, phase 2 study. Lancet. 2023;402(10400):472–483. doi:10.1016/S0140-6736(23)01302-8
182. Saxena AR, Frias JP, Brown LS, et al. Efficacy and safety of oral small molecule glucagon-like peptide 1 receptor agonist danuglipron for glycemic control among patients with type 2 diabetes: a randomized clinical trial. JAMA Network Open. 2023;6(5):e2314493–e2314493. doi:10.1001/jamanetworkopen.2023.14493
183. McGlone ER, Bloom SR, Tan TM. Glucagon resistance and metabolic-associated steatotic liver disease: a review of the evidence. J Endocrinol. 2024;261(3). doi:10.1530/joe-23-0365
184. Conceição-Furber E, Coskun T, Sloop KW, Samms RJ. Is glucagon receptor activation the thermogenic solution for treating obesity? Front Endocrinol. 2022;13:868037. doi:10.3389/fendo.2022.868037
185. Innovent presents the results of the first phase 3 study of mazdutide for weight management at the ADA’s 84th scientific sessions. 2024. Available from: https://www.prnewswire.com/news-releases/innovent-presents-the-results-of-the-first-phase-3-study-of-mazdutide-for-weight-management-at-the-adas-84th-scientific-sessions-302180995.html.
186. le Roux CW, Steen O, Lucas KJ, Startseva E, Unseld A, Hennige AM. Glucagon and GLP-1 receptor dual agonist survodutide for obesity: a randomised, double-blind, placebo-controlled, dose-finding phase 2 trial. Lancet Diabetes Endocrinol. 2024;12(3):162–173. doi:10.1016/S2213-8587(23)00356-X
187. Sanyal AJ, Bedossa P, Fraessdorf M, et al. A Phase 2 randomized trial of survodutide in MASH and fibrosis. N Engl J Med. 2024;391(4):311–319. doi:10.1056/NEJMoa2401755
188. Boehringer receives U.S. FDA breakthrough therapy designation and initiates two Phase III trials in MASH for survodutide. 2024. Available from: https://www.boehringer-ingelheim.com/human-health/metabolic-diseases/survodutide-us-fda-breakthrough-therapy-phase-3-trials-mash.
189. Sanyal AJ, Kaplan LM, Frias JP, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nature Med. 2024;30(7):2037–2048. doi:10.1038/s41591-024-03018-2
190. Ryan G, Briscoe TA, Jobe L. Review of pramlintide as adjunctive therapy in treatment of type 1 and type 2 diabetes. Drug Des Devel Ther. 2009;2:203–214. doi:10.2147/dddt.s3225
191. Ding Y, Shi Y, Guan R, et al. Evaluation and comparison of efficacy and safety of tirzepatide and semaglutide in patients with type 2 diabetes mellitus: a Bayesian network meta-analysis. Pharmacol Res. 2024;199:107031. doi:10.1016/j.phrs.2023.107031
192. Rodriguez PJ, Goodwin Cartwright BM, Gratzl S, et al. Semaglutide vs tirzepatide for weight loss in adults with overweight or obesity. JAMA Intern Med. 2024;184(9):1056–1064. doi:10.1001/jamainternmed.2024.2525
193. Lilly’s tirzepatide superior to Wegovy® (semaglutide) in head-to-head trial showing an average weight loss of 20.2% vs. 13.7%. 2024. Available from: https://www.lilly.com/en-CA/news/press-releases/2024.12.4-tirzepatide-surmount-5-h2h.
194. Allen G, Safranek SM. Secondary causes of obesity. Am Family Phys. 2011;83(8):972.
195. Acosta A, Streett S, Kroh MD, et al. White paper AGA: POWER — practice guide on obesity and weight management, education, and resources. Clin Gastroenterol Hepatol. 2017;15(5):631–649.e10. doi:10.1016/j.cgh.2016.10.023
196. Radić J, Belančić A, Đogaš H, et al. The power of movement: linking physical activity with nutritional health and blood sugar balance in a dalmatian type 2 diabetic population. Nutrients. 2025;17(1):187. doi:10.3390/nu17010187
197. Mozaffarian D, Agarwal M, Aggarwal M, et al. Nutritional priorities to support GLP-1 therapy for obesity: a joint advisory from the American college of lifestyle medicine, the American Society for Nutrition, the Obesity Medicine Association, and the Obesity Society. Obesity. 2025;n/a(n/a):100181. doi:10.1002/oby.24336
198. Rieder M, Belančić A. Past, present and future of drug safety: editorial. Br J Clin Pharmacol. 2024;90(8):1760–1762. doi:10.1111/bcp.16140
199. Gonzalez-Izundegui D, Campos A, Calderon G, et al. Association of gastric emptying with postprandial appetite and satiety sensations in obesity. Obesity. 2021;29(9):1497–1507. doi:10.1002/oby.23204
200. Cifuentes L, Ghusn W, Feris F, et al. Phenotype tailored lifestyle intervention on weight loss and cardiometabolic risk factors in adults with obesity: a single-centre, non-randomised, proof-of-concept study. EClinicalMedicine. 2023;58:101923. doi:10.1016/j.eclinm.2023.101923
201. Carlsson LMS, Arnetorp I, Andersson-Assarsson JC, et al. Health outcomes and their association with weight regain after substantial weight loss in Sweden: a prospective cohort study. Lancet Reg Health Eur. 2025;52:101261. doi:10.1016/j.lanepe.2025.101261
202. Štimac D, Klobučar Majanović S, Belančić A. Endoscopic Treatment of Obesity: from Past to Future. Dig Dis. 2020;38(2):150–162. doi:10.1159/000505394
203. Maccora C, Ciuoli C, Goracci A, et al. One month weight loss predicts the efficacy of liraglutide in obese patients: data from a single center. Endocr Pract. 2020;26(2):235–240. doi:10.4158/EP-2019-0169
204. Sannaa W, Dilmaghani S, BouSaba J, et al. Factors associated with successful weight loss after liraglutide treatment for obesity. Diabetes Obes Metab. 2023;25(2):377–386. doi:10.1111/dom.14880
205. Acosta A, Camilleri M, Burton D, et al. Exenatide in obesity with accelerated gastric emptying: a randomized, pharmacodynamics study. Physiol Rep. 2015;3(11):e12610. doi:10.14814/phy2.12610
206. Lautenbach A, Wernecke M, Huber TB, et al. The potential of semaglutide once-weekly in patients without type 2 diabetes with weight regain or insufficient weight loss after bariatric surgery—a retrospective analysis. Obesity Surg. 2022;32(10):3280–3288. doi:10.1007/s11695-022-06211-9
207. Mok J, Adeleke MO, Brown A, et al. Safety and efficacy of liraglutide, 3.0 mg, once daily vs placebo in patients with poor weight loss following metabolic surgery: the bari-OPTIMISE randomized clinical trial. JAMA Surg. 2023;158(10):1003–1011. doi:10.1001/jamasurg.2023.2930
208. Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553–1564. doi:10.1111/dom.14725
209. Jensterle M, Ferjan S, Janez A. The maintenance of long-term weight loss after semaglutide withdrawal in obese women with PCOS treated with metformin: a 2-year observational study. Front Endocrinol. 2024;15:1366940. doi:10.3389/fendo.2024.1366940
210. Werrij MQ, Jansen A, Mulkens S, Elgersma HJ, Ament AJ, Hospers HJ. Adding cognitive therapy to dietetic treatment is associated with less relapse in obesity. J Psychosom Res. 2009;67(4):315–324. doi:10.1016/j.jpsychores.2008.12.011
211. Paddu NU, Lawrence B, Wong S, Poon SJ, Srivastava G. Weight maintenance on cost-effective antiobesity medications after 1 year of GLP-1 receptor agonist therapy: a real-world study. Obesity. 2024;32(12):2255–2263. doi:10.1002/oby.24177
212. Jensen SBK, Janus C, Lundgren JR, et al. Exploratory analysis of eating- and physical activity-related outcomes from a randomized controlled trial for weight loss maintenance with exercise and liraglutide single or combination treatment. Nat Commun. 2022;13(1):4770. doi:10.1038/s41467-022-32307-y
213. Almandoz JP, Lingvay I, Morales J, Campos C. Switching between glucagon-like peptide-1 receptor agonists: rationale and practical guidance. Clin Diabetes. 2020;38(4):390–402. doi:10.2337/cd19-0100
214. Belančić A, Al-Sallami HS. Spotlight commentary: changes in pharmacokinetics following significant weight loss. Br J Clin Pharmacol. 2025;91(3):678–680. doi:10.1111/bcp.16401
215. Finkelstein EA, Chodavadia PA, Strombotne K. A systematic review of the economic value proposition for commercially available nonsurgical weight-loss interventions. Obesity. 2023;31(7):1725–1733. doi:10.1002/oby.23760
216. Lauren BN, Lim F, Krikhely A, et al. Estimated cost-effectiveness of medical therapy, sleeve gastrectomy, and gastric bypass in patients with severe obesity and type 2 diabetes. JAMA Network Open. 2022;5(2):e2148317. doi:10.1001/jamanetworkopen.2021.48317
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.