Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Pharmacists’ “Full Scope of Practice”: Knowledge, Attitudes and Practices of Rural and Remote Australian Pharmacists
Authors Hays C ![]() , Sparrow M, Taylor S
, Sparrow M, Taylor S ![]() , Lindsay D, Glass B
, Lindsay D, Glass B ![]()
Received 31 August 2020
Accepted for publication 22 October 2020
Published 1 December 2020 Volume 2020:13 Pages 1781—1789
DOI https://doi.org/10.2147/JMDH.S279243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Catherine Hays,1 Melanie Sparrow,2 Selina Taylor,1 Daniel Lindsay,3 Beverley Glass2
1Centre for Rural and Remote Health, James Cook University, Mount Isa, Queensland, Australia; 2Pharmacy, College of Medicine and Dentistry, James Cook University, Townsville, Queensland, Australia; 3College of Public Health, Medical and Veterinary Science, James Cook University, Townsville, Queensland, Australia
Correspondence: Catherine Hays
Centre for Rural and Remote Health, James Cook University, PO Box 2572, Mount Isa, Queensland 4825, Australia
Tel +61 7 4745 4500
Fax +61 7 4749 5130
Email [email protected]
Purpose: Poor health outcomes for patients living in rural and remote areas of Australia are often attributed to the lack of a range of accessible health professionals delivering health services. Community pharmacists are already an integral part of these communities and as such are often the most frequently consulted health professionals. The aim of this study was to explore rural pharmacist knowledge and experiences of expanded pharmacy and to identify the barriers and enablers to remote pharmacists providing expanded pharmacy services (EPS), which can be described as services outside of usual medication management tasks.
Methods: Rural and remote pharmacists (Modified Monash Model (MMM) categories 2– 7) participated in an online survey. Descriptive statistics and chi-squared tests were performed and data from open-ended questions were analyzed, categorized into themes and quantitized.
Results: Two-thirds (n=13, 68%) of rural pharmacists surveyed (n=19) had knowledge of EPS in rural pharmacies and the majority (n=17, 89%) agreed that these services would benefit rural communities. Mental health service referral was considered very/extremely important by the majority (n=16, 84%) of respondents; however, no pharmacists were currently providing mental health screening services while (n=15, 79%) were willing to provide these services. While staff shortages, costs, time and training were indicated to be the main barriers to the provision of EPS, enablers included accessibility of rural pharmacies and a perceived need.
Conclusion: This study indicated that pharmacists are already providing some EPS and see value in their implementation; however, what constitutes an expanded service was unclear to some participants. Mental health services were highlighted as most important demonstrating a recognized burden of mental illness in rural and remote locations. Findings from this pilot study will provide further understanding for future development of the pharmacist’s scope of practice and implementation of EPS.
Keywords: pharmacy, workforce, rural and remote, health outcomes, expanded scope
Introduction
In Australia, one-third of the country’s population is currently living in either regional, rural or remote locations, equating to approximately seven million people.1 Australians living in rural and remote regions of the country experience higher mortality rates and poorer health outcomes than their metropolitan counterparts.1 These poorer health outcomes can be attributed to the distances that people are required to travel to access health services, which is related to a lack of availability of health services in their local regions, mainly due to a maldistribution of the health workforce.1–3 Difficulty of delivering health services is compounded by the lack of a range of health professionals, including doctors.4 In addition, these communities are small and highly dispersed, causing low population densities and long distances between rural towns.4 This presents a challenge when planning health service delivery for rural and remote locations.
Rural community pharmacists, accessible to rural and remote population groups, are frequently consulted by patients,5 and provide services to those who might not otherwise have contact with other health professionals.6 Pharmacists are well recognized by patients and other health professionals for their role in medication management, which is associated with supply of medicines.5 Expanded pharmacy services (EPS) have been defined as pharmacists working to their “full” or “enhanced” scope of practice, involving the performing of activities usually provided by other health professionals.7,8 These services are described using various terminology in different parts of the world with terms such as “cognitive pharmaceutical services“, “minor ailment services“, and “professional pharmacy services“ being utilized.9–11 However, patients often only recognize the traditional supply function of the pharmacist, which involves dispensing prescription medicines, providing over the counter medicines, advice and counselling.12 Recently, the pharmacist’s role has expanded to a “full scope of practice” to include public health services such as risk reduction of cardiovascular disease, osteoporosis screening, oral health care and immunization.12 However, in addition to patients lacking awareness of available services, pharmacists have also expressed concern about a lack of time, space and remuneration for the delivery of these services.13,14
Pharmacists’ opinions are that expanded practice would benefit the profession and their individual practice. This is aligned with the opinions of their customers, who perceived there to be barriers to expanded practice.13,14 Pharmacists appear also to have not taken opportunities to work to their “full scope of practice” and some seem confused as to what constitutes expanded practice.15 To bring about change is complex, with nine themes relevant to practice change being identified in a study based in Ontario, Canada.15 These included regulation associated with the expanded scope of practice, which involves changes to legalization and procedural guidance to translate EPS into day-to-day activities.15 Pharmacists also required practice to ensure confidence in the new activity, positive reinforcement and personalized attention rather than group-based education to support implementation of EPS.15 Due to the often solitary nature of pharmacy practice, particularly in rural areas, peer referencing to shape attitudes and redirect practices in addition to physician acceptance was also considered essential for EPS implementation. Patient expectations and professional identity were reported as both barriers and enablers toward changing practice.15
Pharmacists’ attitudes and attributes have been described by Luetsch16 as barriers and facilitators to the uptake of expanded practice. Some pharmacists appear to be hesitant to provide EPS, due to lack of evidence that these services will be beneficial to the patients.16 Although pharmacists often expressed positive attitudes, implementation and provision of these services was often lacking.16 Furthermore, literature regarding EPS in a rural and remote Australian context, where there is restricted access to other health providers including GPs, allied health practitioners, and specialist services, is limited. For this reason, and the potential contribution EPS could make to health outcomes for rural populations, the purpose of this study was to explore the knowledge, attitudes and practices of pharmacists towards EPS in rural and remote Australia, and to identify the perceived barriers and enablers to the delivery of these services.
Methods
A cross-sectional pilot study was conducted, which included the design of a survey of EPS in rural and remote Australia to explore the knowledge, attitudes and practices of rural pharmacists towards EPS, and their perceived barriers and enablers to delivery of these services. The survey and EPS listed therein was informed by a review of the literature examining EPS provided in rural locations globally. The survey was piloted with four rural pharmacists who were excluded from the results, minor changes were incorporated in the final survey. The survey was divided into four sections with a total of 23 questions, including knowledge of expanded services, attitudes and practices towards these services, barriers and enablers and demographic information. The survey included five-point Likert scale and open- and closed-ended questions. Participants received no incentives for participating in the survey, which took approximately 20 min to complete. Data were collected during April and May, 2019.
The survey was delivered online via Survey Monkey and distributed via email through various rural pharmacy networks including the Pharmaceutical Society of Australia, Society of Hospital Pharmacists of Australia, Services for Australian Rural and Remote Allied Health, Rural Pharmacy Support Network, and the James Cook University School of Pharmacy Alumni. The participants were required to be practicing in Modified Monash Model17 (MMM) category 2–7 locations. The MMM classifies areas of Australia according to level of geographical remoteness and population size, where MM1 is “metropolitan“, while MM7 is “very remote.”17
Data Analysis
Descriptive statistical analysis was undertaken to interpret, categorize, and describe the quantitative data. Data from open-ended questions were analyzed with meaningful statements categorized into themes and quantitized. Chi-squared tests using IBM SPSS Statistics for Windows, version 25.0. released 2017 (IBM Corporation, Armonk, NY, USA) were conducted to find out if there was a relationship between importance of listed EPS, MMM category, and length of time employed in rural pharmacy.
Research Ethics
James Cook University Human Research Ethics Committee granted ethical approval H7752. Information regarding the study and its objectives was provided before respondents commenced the survey to ensure informed consent.
Results
Participant Profile
A total of 19 pharmacists completed the survey. Demographic data are presented in Table 1. Just over two-thirds of participants were female and 37% were aged 26–35 years. Respondents were evenly distributed over all nonmetropolitan MMM categories (MM2-7), and 58% had over 10 years of pharmacy experience.
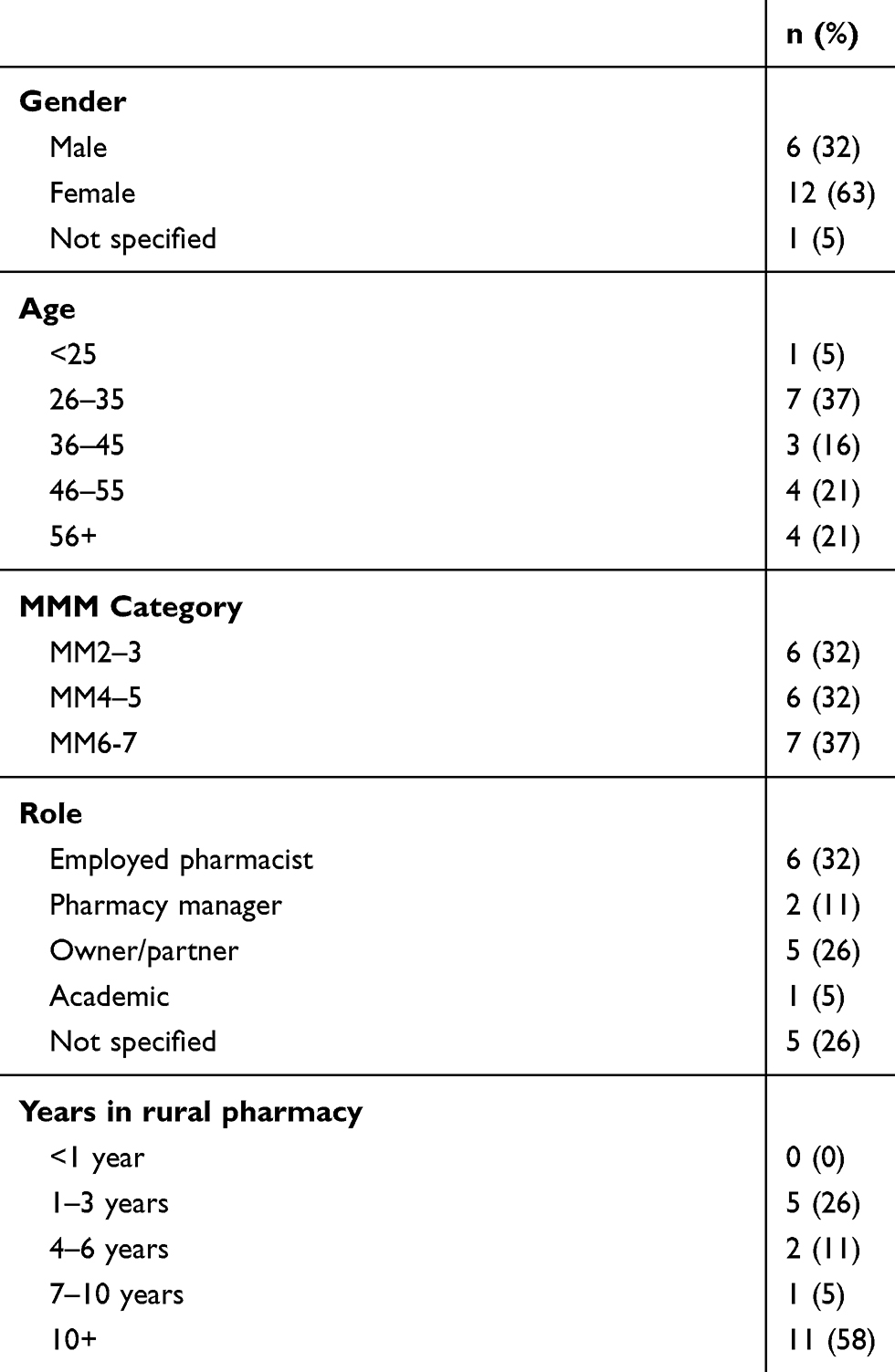 |
Table 1 Participant Demographic Data |
Knowledge of and Attitudes Towards EPS
The survey included questions designed to explore pharmacists’ knowledge of and attitudes towards EPS (see Table 2). While most participants (68%) agreed that EPS were currently being provided in rural pharmacies in Australia, only 58% agreed that they provide these services at their current place of employment. Respondents seem to view EPS positively, as the majority agreed that rural pharmacies are well placed to provide EPS (84%), and that these services would benefit those living in rural communities (89%). Almost two-thirds also agreed that EPS would be a motivating factor in attracting pharmacists to work in rural communities.
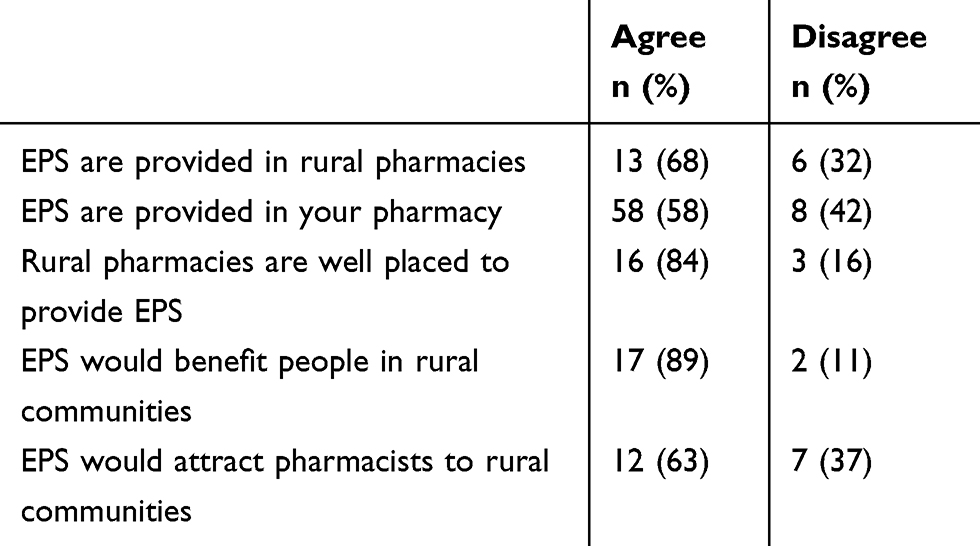 |
Table 2 Pharmacist Knowledge of and Attitudes Towards EPS |
Participants’ attitudes were also gauged by asking them to apply a rank of importance from one (not important) to five (extremely important) to 36 EPS. These EPS comprised of basic examination, assessment or screening; treatment; referral; and supply of relevant products and education for a range of acute and chronic conditions including speech and swallowing, mental health, respiratory health, osteoporosis, musculoskeletal conditions, oral health, ocular health, hearing, diabetic foot screening and podiatry, acute infections, and drug and alcohol services. Table 3 displays the 10 most and least important EPS as selected by the rural pharmacist participants. “Most important” EPS was determined by most frequent selection of very/extremely important, whilst “least important” was determined by most frequent selection of “not important”, and then by least frequent selection of “very/extremely important”.
 |
Table 3 Ten Most/Least Important EPS to Rural Pharmacy Practice as Selected by Rural Pharmacists |
Half of the most important EPS chosen were referral services and referral to available, appropriate mental health services was considered very/extremely important by 84% of respondents. The remaining most important EPS were for examination and treatment of acute conditions such as communicable diseases or mental health issues. EPS considered to be least important by respondents were assessment, examination, or screening services (70%). Speech and language assessments, heel scans, and hearing testing were most often selected to be “not important” to rural pharmacy practice, by the participants. Speech and swallowing, hearing, and substance-abuse related services all appeared more than once in the least important services table.
Participants were given the opportunity to list expanded services that they were already providing. The most common services included six pharmacists providing vaccinations, three providing home medicine reviews, three offering blood pressure monitoring, three preparing dose administration aids, and two offering sleep apnea services. Asthma management, COPD screening, CVD screening, blood sugar screening, weight management, and smoking cessation services were each listed once. Three participants’ inclusion of “dose administration aids” as an expanded service they provide at their pharmacy may indicate a possible misunderstanding among pharmacists of what defines an EPS.
Practices Involving EPS
Participants responded whether their pharmacy currently provides, or if they would be interested in providing each service (see Table 4). Of the ten most important services listed in Table 3, all were currently being provided in two (11%) participants’ place of work, with the exception of “conduct basic mental health assessments using screening tools.” The participant group consistently stated (100% of 10 most important EPS) that they would like to deliver these services as often or more often than current practice.
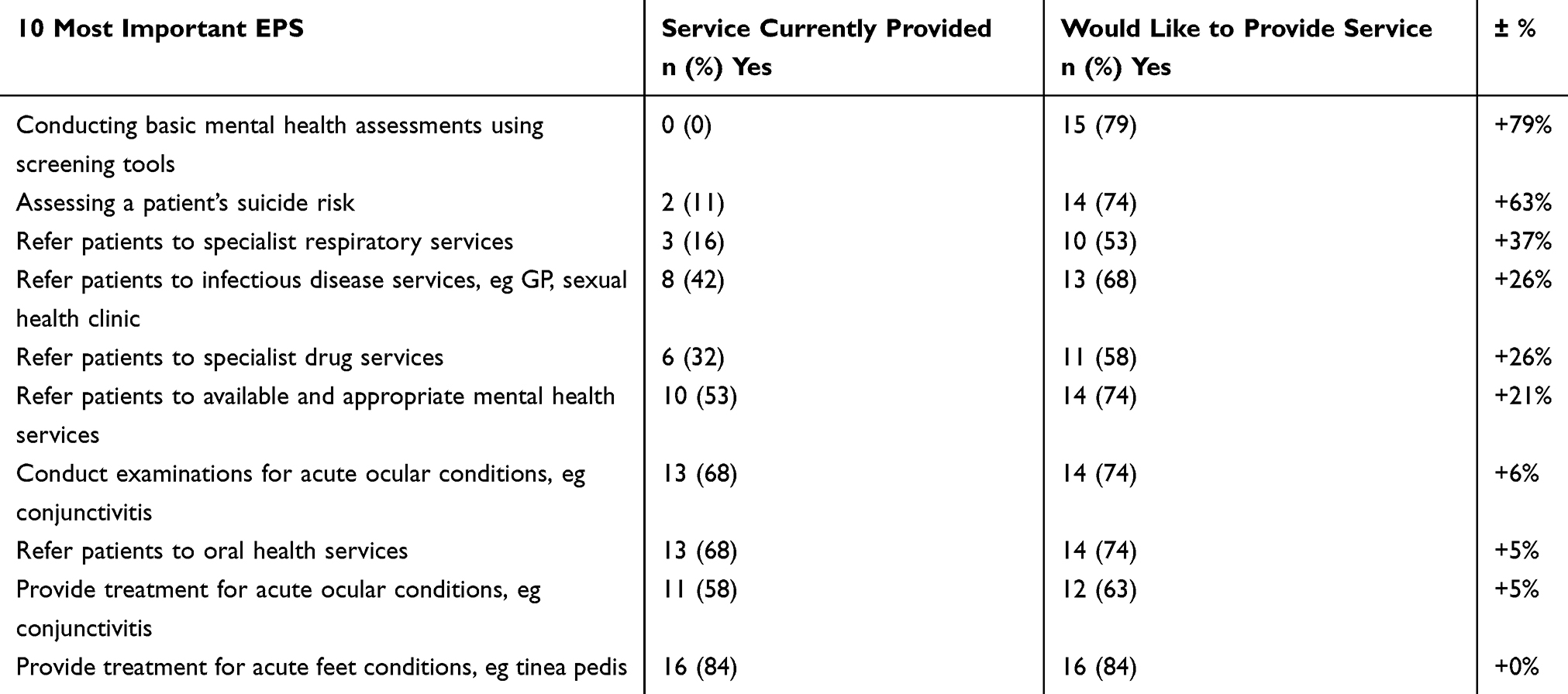 |
Table 4 EPS Currently Being Provided/Would Like to Provide in Rural Pharmacies (10 Most Important EPS) |
The importance attached to mental health service provision in rural and remote areas was clearly demonstrated. Although “conduct basic mental health assessments using screening tools” was not a current service at any of the participants’ workplaces, 79% responded that they would like to provide this service. Similarly, only two (11%) participants reported that they currently provide patient suicide risk assessments, however 74% would like to provide them. Referral to mental health services, the EPS that was considered “most important” in Table 3 was already being provided by approximately half of the pharmacists (n=10, 53%), while an additional four respondents stated that they would like to provide this service in their rural pharmacy. The “most important” examination and treatment of acute ocular and foot conditions services were already being provided by most respondents (all over 50%).
Barriers, Enablers and Expected Outcomes of Expanded Practice
Responses from open-ended question regarding the barriers, enablers, and expected outcomes of expanded pharmacy practice in rural and remote locations were analyzed and common or relevant statements and their frequency were identified and are presented in Table 5. Pharmacists perceived many more barriers than enablers to the provision of EPS. The most often stated barriers were regarding staff shortages, remuneration, training, and time. Enabling factors included a need for services, due to a lack of health providers in their area, and that rural pharmacies are well placed to provide EPS. They also believed that the introduction of EPS would be enabled by their existing rapport and frequent contact with patients. Expected outcomes of the introduction of EPS in their pharmacy were consistently positive, particularly regarding improved health outcomes for rural populations, benefits for health services, and improved community relationships.
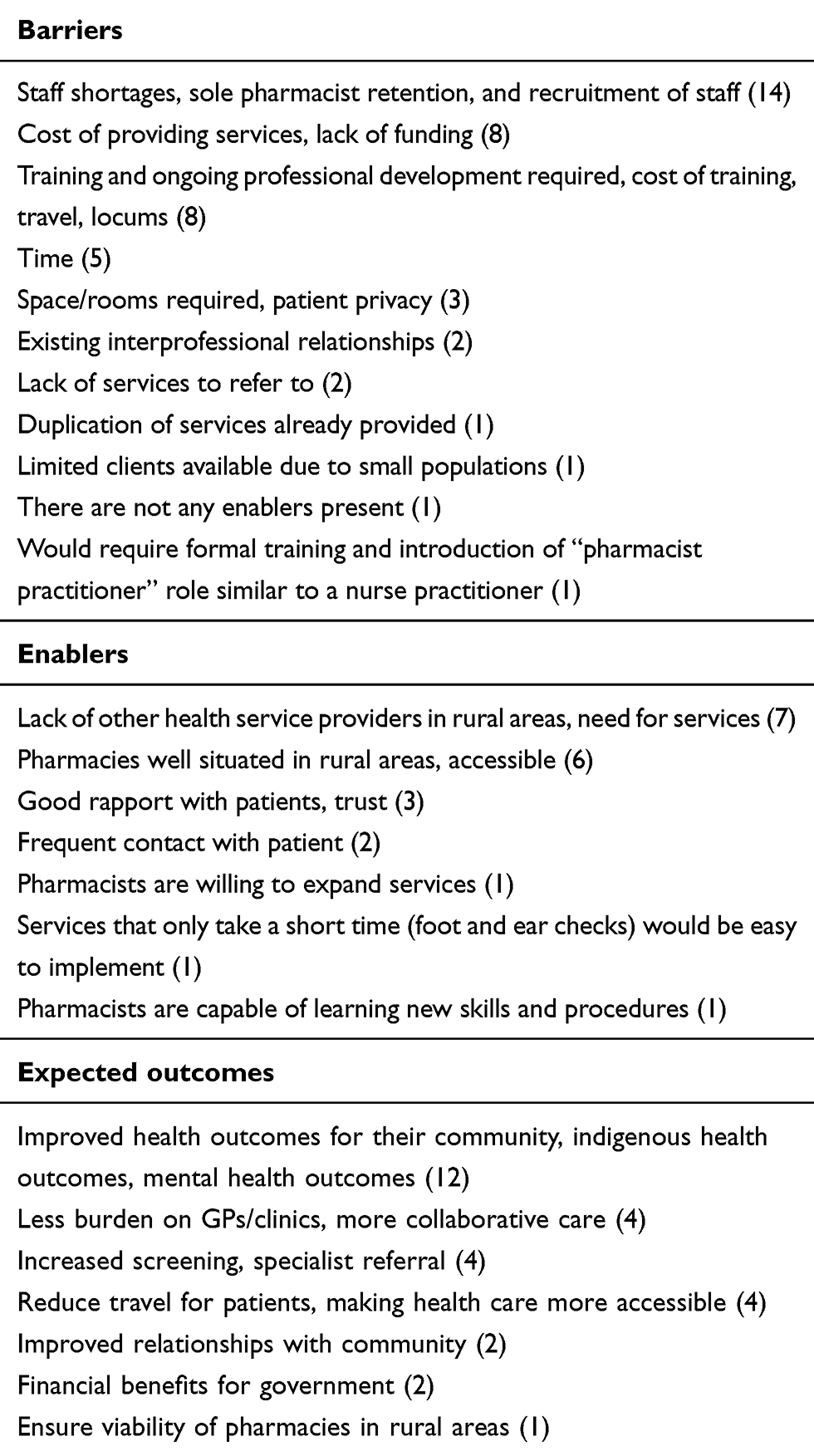 |
Table 5 Pharmacist Statements (and Their Frequency) Regarding Barriers, Enablers, and Expected Outcomes of Expanded Pharmacy Practice |
There was no statistically significant association between rurality or time spent working in rural areas and EPS (p>0.05). The lack of statistical significance between importance of EPS listed in this study, MMM category, and length of time employed in rural pharmacy may imply that all participants recognize that the EPS and associated health issues listed in the survey have some importance to their community. All health issues were generally considered to be “important” by respondents, regardless of these variables.
Discussion
While over two-thirds of pharmacists claimed knowledge that EPS were being delivered in community pharmacy, there appears to be some confusion as to which services constitute expanded practice, with blood pressure monitoring, provision of dose administration aids, blood sugar screening, weight management, and smoking cessation being listed as expanded services. Although expanded practice has been described as a distinct knowledge and skill base that is in addition to the recognized scope of the pharmacy profession,8 pharmacists might see any service other than the traditional supply of medicines as expanded practice.12 This demonstrates an urgent need for the pharmacy profession to develop clarity for pharmacists about what is defined as an expanded service. Attitudes to the provision of EPS are largely positive especially in relation to the accessibility of rural community pharmacists, as highlighted by Gregory et al15 and Luetsch16 however, the change in practice is complex and often reliant on acceptance by not only pharmacists and patients, but also other health professionals.
Respondents’ consistent high ranking of EPS related to mental health including referral to mental health services, conducting suicide risk assessments, and the use of basic mental health screening tools are expected considering the frequency and impact of poor mental health in rural and remote regions of Australia.18 There is evidence that an increased role of pharmacists in the treatment and management of mental health has had a positive influence on both patient and pharmacist.19,20 A Canadian study found that pharmacists perceived the provision of support to patients with mental health and addictions improved pharmacist–patient relationships through increased rapport and trust.19 Pharmacists also noticed a change in their own perceptions of stigma regarding mental illness, and benefited from increased collaboration with health professionals and community organizations.19 An Australian study found that mental health consumers and carers expected pharmacists to provide services beyond medication dispensing, including individualized counselling, explanation of medication side-effects or medication information, communication between pharmacists and doctor to avoid potential drug interactions, patient education and information about relevant community support services.20
Four of the “most important” EPS were services related to infectious diseases including minor ocular and sexually transmitted diseases. A consultation service for ear, nose, and throat and eye conditions was introduced in the UK, where pharmacists received training for patient examination and treatment of these conditions. Patients received appropriate diagnosis or treatment including prescription-only or over-the-counter medicine, advice, or referral to a GP.21 Most patients (85%) did not require treatment from another health professional after receiving treatment or advice from the pharmacist.21 Ninety-seven percent of patients who participated agreed that pharmacies were appropriate to provide the expanded service, and reasons for utilizing the pharmacist-provided consultation service included no need to make or wait for an appointment and convenience of pharmacy location or opening times.21
Five of the 10 “most important” EPS as perceived by respondents were referral services, which may imply that pharmacists recognize that they are well positioned to connect patients with appropriate health services via a formalized referral pathway. Pharmacist referrals to GPs and other health professionals have been documented in the literature and are generally described as appropriate and resulting in positive patient health outcomes.22 A UK-based study found that pharmacists referred patients to their GP within the first two weeks of taking antihypertensive medication, with most common reasons for referral being experience of side-effects, not using the medication as prescribed, or negative feelings towards the medication or condition. The pharmacist referred 4.5% of patients back to their GP, while the other 95.5% were supported by the pharmacist without the need for referral.23 Another study concerning the GP-pharmacist relationship found that while GP-pharmacist interactions can be limited and are often tense, some pharmacists felt they had doctor’s respect in regard to contact regarding patient conditions, medication, and referrals.24 Pharmacists perceived that their actions and decisions assisted with the GP’s heavy workloads, only referring serious conditions to the GP, while the pharmacist could manage and treat minor issues.24 A New Zealand-based pharmacy asthma management program, which aimed to resolve issues of medication/dose, administration, compliance, drug reactions and other related issues resulted in nearly half (49%) of patients being referred to a GP, respiratory specialist or asthma educator.25 However, while pharmacist referral to GP or other health providers is documented in the literature, sometimes no official referral procedure exists. For example, Hoang et al26 found that although rural Australian pharmacists provide oral health advice regularly, there is no referral pathway from pharmacy to oral health services, and pharmacists had limited or no communication with local dental services. This highlights a need for an explicit referral pathway and increased collaboration between pharmacists and other health services, which have the potential to benefit pharmacists, health providers and patients.24,26,27
Community pharmacies are often the first contact for patients for minor conditions, are widely available, have longer hours of operation compared to GP clinics, and do not require an appointment for consultation.22,28 Pharmacists are ideally placed to engage and educate patients, and are one of the most accessible and trusted health professionals.28 A review of literature regarding community pharmacist triage services found that when clinical guidelines or protocols were utilized, pharmacist accuracy of assessment ranged between 70% and 98%, and when no guideline was used, correct diagnosis became more likely as the number of questions increased.22 An evaluation of an Australian pharmacy-based COPD screening program, during which pharmacists received accredited training and equipment to provide lung function tests found that the service was feasible, and similar programs have potential and may improve identification of undiagnosed COPD cases.29
The literature confirms many of the barriers to providing the level of care required for EPS that arose from this study, including lack of time, poor support from other pharmacy staff or employers, lack of training for pharmacy staff, little or no remuneration for services, staff shortages, poor support from other health professionals, and low patient engagement or awareness of services.19,30,31 These issues could be addressed with the provision of training and education, staff support, and effective advertising and promotion of services.30 In order to allow pharmacists to provide effective and successful delivery of EPS, recommendations include the implementation of evidence-based guidelines or protocols to assist with assessment and diagnosis; thorough documentation and integration of care via collaboration with GPs and other health services, referrals and follow-up; the availability of a consult room to ensure patient privacy and confidentiality; patient consultation with pharmacists rather than other pharmacy support staff; and greater public awareness of pharmacy services are essential.22 Furthermore, governance and drive from the Australian professional pharmacy associations is essential for EPS to be successfully implemented.
Limitations
A limitation of the study is selection bias that might have occurred in that only rural pharmacists with knowledge of and an interest in EPS may have participated. Furthermore, the small sample size is a limitation, however the even distribution of participants across the MMM categories does provide perspectives from regional to very remote areas. The estimated number of registered pharmacists across regional to very remote (MM2-7) is approximately 5500, which constitutes less than 25% of total pharmacists in Australia.32 Although the number of responses are low, and generalizability is impaired, as a pilot study in an area of very limited evidence there is value in understanding rural pharmacists’ perceptions of expanded practice. The authors are planning further exploration using qualitative methods to provide a deeper understanding of this important topic.
Conclusion
The findings from this study have revealed that although pharmacists have knowledge of EPS there may be some confusion as to what constitutes an expanded service. This demonstrates a need for the pharmacy profession to provide clarity regarding the terms used, including “full scope of practice”, “enhanced practice” and “expanded practice”. Clear understanding of this is required for expanded services to be successfully implemented. This pilot study has also highlighted positive perceptions regarding a full scope of practice, however a change in pharmacy practice requires input from diverse pharmacy organizations and other health service providers to support pharmacists through this process. Findings suggest that rural Australian pharmacists value the concept of expanded services, and in some places already provide them. Particular interest in mental health services indicates the recognition of the burden of mental health in rural and remote practice and the motivation to improve current service delivery. Further exploration of rural pharmacists’ knowledge, attitudes, and practices of expanded services is important to provide evidence to support the design and development of future expanded practice models.
Acknowledgments
We acknowledge the rural and remote pharmacists who generously gave up their time to participate in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Australian Institute of Health and Welfare. Rural Remote Health. Canberra: Australian Institute of Health and Welfare; 2017.
2. Wakerman J, Humphreys JS. “Better health in the bush”: why we urgently need a national rural and remote health strategy. Medical J Aust. 2019;210(5):202–203.e201. doi:10.5694/mja2.50041
3. Gardiner FW, Richardson AM, Bishop L, et al. Health care for older people in rural and remote Australia: challenges for service provision. Med J Australia. 2019;211(8):363–364. doi:10.5694/mja2.50277
4. McGrail MR, Wingrove P, Petterson S, et al. Measuring the attractiveness of rural communities in accounting for differences of rural primary care workforce supply. Rural Remote Health. 2017;17(2):1. doi:10.22605/RRH3925
5. Wibowo Y, Berbatis C, Joyce A, Sunderland VB. Analysis of enhanced pharmacy services in rural community pharmacies in Western Australia. Rural Remote Health. 2010;10(3):1400.
6. Eades CE, Ferguson JS, O’Carroll RE. Public health in community pharmacy: A systematic review of pharmacist and consumer views. BMC Public Health. 2011;11(1):582. doi:10.1186/1471-2458-11-582
7. Paola S. Practising to Your ‘Full’ Scope. Aust J Pharm. 2018.
8. Jackson S, Martin G, Bergin J, et al. Understanding advanced and extended professional practice. Australian Pharmacist. 2015;34(4):76–79.
9. Aly M, García-Cárdenas V, Williams K, Benrimoj SI. A review of international pharmacy-based minor ailment services and proposed service design model. Res Social Adm Pharm. 2018;14(11):989–998. doi:10.1016/j.sapharm.2017.12.004
10. Perraudin C, Bugnon O, Pelletier-Fleury N. Expanding professional pharmacy services in European community setting: is it cost-effective? A systematic review for health policy considerations. Health Policy (New York). 2016;120(12):1350–1362. doi:10.1016/j.healthpol.2016.09.013
11. Campbell C, Braund R, Morris C. Beyond the four walls: an exploratory survey of location, employment and roles of pharmacists in primary health care. J Prim Health Care. 2017;9(4):297–310. doi:10.1071/HC17022
12. McMillan SS, Wheeler AJ, Sav A, et al. Community pharmacy in Australia: a health hub destination of the future. Res Social Adm Pharm. 2013;9(6):863–875. doi:10.1016/j.sapharm.2012.11.003
13. Um IS, Armour C, Krass I, Gill T, Chaar BB. Consumer perspectives about weight management services in a community pharmacy setting in NSW, Australia. Health Expectations. 2014;17(4):579–592. doi:10.1111/j.1369-7625.2012.00788.x
14. Sunderland B, Burrows S, Joyce A, McManus A, Maycock B. Rural pharmacy not delivering on its health promotion potential. Aust J Rural Health. 2006;14(3):116–119. doi:10.1111/j.1440-1584.2006.00774.x
15. Gregory PAM, Teixeira B, Austin Z. What does it take to change practice? Perspectives of pharmacists in Ontario. Can Pharm J. 2018;151(1):43–50. doi:10.1177/1715163517742677
16. Luetsch K. Attitudes and attributes of pharmacists in relation to practice change- A Scoping Review and discussion. Res Social Adm Pharm. 2017;13:440–455. doi:10.1016/j.sapharm.2016.06.010
17. Department of Health. Modified Monash Model; 2018. Available from: https://www.health.gov.au/health-workforce/health-workforce-classifications/modified-monash-model.
18. National Rural Health Alliance. Mental Health in Rural and Remote Australia. ACT, Australia: National Rural Health Alliance; 2017.
19. Murphy AL, Phelan H, Haslam S, Martin-Misener R, Kutcher SP, Gardner DM. Community pharmacists’ experiences in mental illness and addictions care: A qualitative study. Subst Abuse Treat Prev Policy. 2016;11(1):6. doi:10.1186/s13011-016-0050-9
20. Fejzic J, Knox K, Hattingh HL, Mey A, McConnell D, Wheeler AJ. Australian mental health consumers and carers expect more health management information from community pharmacy. Int J Pharm Pract. 2017;25(6):454–462. doi:10.1111/ijpp.12356
21. Hall G, Cork T, White S, Berry H, Smith L. Evaluation of a new patient consultation initiative in community pharmacy for ear, nose and throat and eye conditions. BMC Health Serv Res. 2019;19(1):285–288. doi:10.1186/s12913-019-4125-y
22. Curley LE, Moody J, Gobarani R, et al. Is there potential for the future provision of triage services in community pharmacy? Journal of Pharmaceutical Policy and Practice. 2016;9(1):29. doi:10.1186/s40545-016-0080-8
23. Albasri A, Prinjha S, McManus RJ, Sheppard JP. Hypertension referrals from community pharmacy to general practice: multivariate logistic regression analysis of 131 419 patients. Br J Gen Pract. 2018;68(673):e541–e550. doi:10.3399/bjgp18X697925
24. Bradley F, Ashcroft DM, Crossley N. Negotiating inter-professional interaction: playing the general practitioner-pharmacist game. Sociol Health Illn. 2018;40(3):426–444. doi:10.1111/1467-9566.12656
25. Emmerton L, Shaw J, Kheir N. Asthma management by New Zealand pharmacists: a pharmaceutical care demonstration project. J Clin Pharm Ther. 2003;28(5):395–402. doi:10.1046/j.0269-4727.2003.00507.x
26. Hoang H, Barnett T, Kirschbaum M, Dunbar S, Wong R. ‘The public rely on me a lot’: rural pharmacists’ perspectives on their roles in oral health care. Aust J Rural Health. 2019;27(1):57–63. doi:10.1111/ajr.12460
27. Hattingh HL, Sim TF, Parsons R, Czarniak P, Vickery A, Ayadurai S. Evaluation of the first pharmacist-administered vaccinations in Western Australia: a mixed-methods study. BMJ Open. 2016;6(9):e011948. doi:10.1136/bmjopen-2016-011948
28. Poudel A, Lau ETL, Deldot M, Campbell C, Waite NM, Nissen LM. Pharmacist role in vaccination: evidence and challenges. Vaccine. 2019;37(40):5939–5945. doi:10.1016/j.vaccine.2019.08.060
29. Fathima M, Saini B, Foster JM, Armour CL. Community pharmacy-based case finding for COPD in urban and rural settings is feasible and effective. Int J Chron Obstruct Pulmon Dis. 2017;12:2753–2761. doi:10.2147/COPD.S145073
30. Fathima M, Saini B, Foster JM, Armour CL. A mixed methods analysis of community pharmacists‘ perspectives on delivering COPD screening service to guide future implementation. Res Social Adm Pharm. 2019;15(6):662–672. doi:10.1016/j.sapharm.2018.08.007
31. Morrison J. Expanded pharmacy practice: where are we, and where do we need to go? Can Pharm J. 2013;146(6):365–367. doi:10.1177/1715163513508914
32. Department of Health. Pharmacists 2017 Factsheet. Health Workforce Data website; 2018. https://hwd.health.gov.au/webapi/customer/documents/factsheets/2017/Pharmacists.pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.