Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Perspectives On Perceived Stigma And Self-Stigma In Patients With Hidradenitis Suppurativa
Authors Koumaki D, Efthymiou O ![]() , Bozi E, Katoulis AC
, Bozi E, Katoulis AC
Received 1 April 2019
Accepted for publication 8 October 2019
Published 16 October 2019 Volume 2019:12 Pages 785—790
DOI https://doi.org/10.2147/CCID.S180036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Dimitra Koumaki, Ourania Efthymiou, Evangelia Bozi, Alexander C Katoulis
Hidradenitis Suppurativa Clinic, 2nd Department of Dermatology and Venereology, “Attikon” General University Hospital, National and Kapodistrian University of Athens, Medical School, Athens, Greece
Correspondence: Alexander C Katoulis
Hidradenitis Suppurativa Clinic, 2nd Department of Dermatology and Venereology, “Attikon” General University Hospital, National and Kapodistrian University of Athens, Medical School, Athens, Greece
Tel +30-210-5832495
Email [email protected]
Objective: To review current knowledge on how patients with hidradenitis suppurativa (HS) experience stigmatization, as well as on its associations with clinical and psychosocial characteristics of the disease. A better understanding of these may help dermatologists improve screening and management for the benefit of HS patients.
Methods: A MEDLINE search using the terms stigmatization, perceived stigma, self-stigma, and HS/acne inversa.
Results: Stigmatization is common among HS patients and has a strong psychosocial impact, which is often disproportional to the extent and severity of skin involvement. Stigmatization in HS has many faces and it is more prevalent and more severe than most other skin diseases. Stigmatization of HS patients is due not only to the distressing symptoms of pain, itch malodorous discharge, and disfiguring scars but also to the lack of knowledge about HS on part of the general public.
Conclusion: Stigma is a significant contributor to the impairment of quality of life and psychiatric co-morbidities commonly seen in patients with HS. Therefore, evaluation for stigma and formulation of strategies to prevent stigmatization and treat its consequences, in the context of a multidisciplinary approach, may ameliorate considerably the lives of HS patients.
Keywords: stigmatization, quality of life, psychosocial, comorbidities
Introduction
Stigmatization can be defined as an awareness of social disapproval, discrediting or devaluation, based on an attribute or a physical mark.1–3 Stigmatization distorts individual’s personal and social image, thus resulting in serious psycho-social consequences. Most psychological domains are negatively affected, but, most importantly, social relations are devastated. Stigmatization undermines the fundamental human need for acceptance by others and social participation.4
Hidradenitis suppurativa (HS) is a chronic, relapsing inflammatory dermatosis of the apocrine gland-bearing areas, clinically characterized by the formation of nodules, abscesses, sinus tracts, and scars, and associated with various comorbidities.5 Stigmatization is a well-appreciated characteristic of HS,6 significantly contributing to the impairment of patients’ quality of life (QoL) that is commonly seen in HS.7,8
HS patients often experience felt or perceived stigma, referring to the negative attitudes and responses that they perceive to be present in society and the sense of shame and fear of being discriminated against because of being “flawed” due to their illness.6 Stigmatized HS patients may internalize perceived prejudices, resulting in self-stigma, which is characterized by negative feeling of one’s self, decreased self-esteem and increased depression.6–11 Patients feeling shame and embarrassment for their disease, limit social interactions and exhibit occupational dysfunction.12 Actual experiences of stigmatization (i.e., enacted stigma) are also reported, for instance reactions of disgust or aversion, negative comments or avoidance of contact.6,7
As stigmatization contributes considerably to disability, depression and reduced quality of life among HS patients, it represents an important stressor itself that in turn may trigger HS exacerbation.7–12 Thus a vicious self-perpetuating cycle is established.
The purpose of this study is to review relevant published literature regarding perceived stigma or self-stigma in patients with HS.
Methods
In the present review, we included relevant articles which were identified either by searching PubMed, Medline, Web of Science, and Scopus databases, or by going through the reference list of already published reviews. We repeatedly used in different combinations the search terms: “stigma”, “self-stigma”, “perceived stigma”, “stigmatization”, “depression”, “hidradenitis suppurativa” and “acne inversa” without limitations regarding the year of publication. Only articles in English language have been taken into consideration. Selected publications were sorted in terms of relevance and importance and, finally, 41 articles were systematically reviewed.
Stigmatization In Hidradenitis Suppurativa Patients
As a chronic debilitating disease with high morbidity and strong negative impact on QoL that affects all aspects of personal and social life, HS has been associated with all types of stigmatization (Table 1).5,6,13
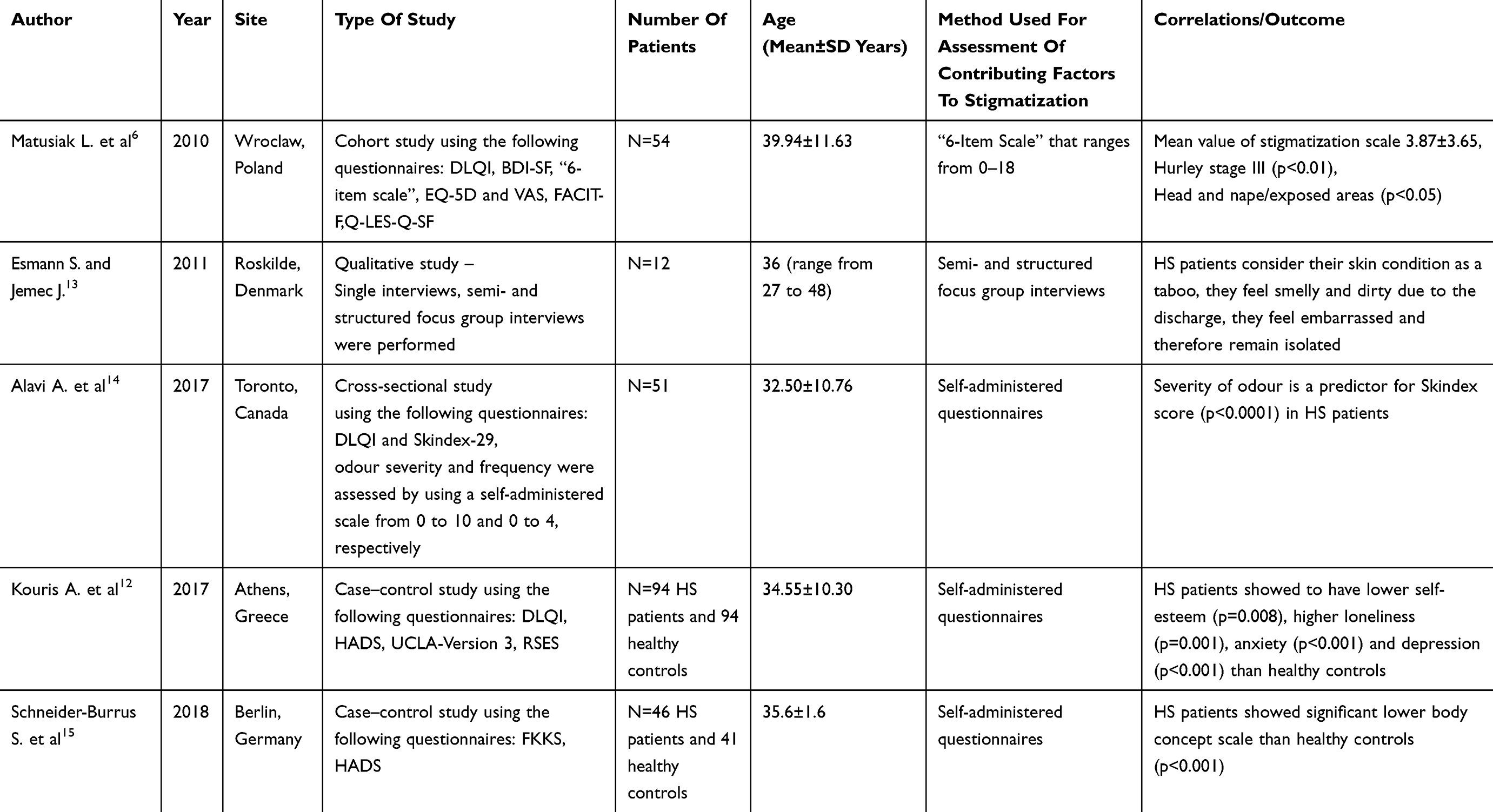 |
Table 1 Summary Of Studies On Hidradenitis Suppurativa (HS) And Contributing Factors To Stigmatization |
Matusiak et al analyzed the stigmatization experience in 54 patients with HS, using the ‘6-Item Stigmatization Scale’.6 Scores range from 0 to 18; the higher the score, the greater the level of stigmatization. In HS patients, the mean result was estimated to be 3.87±3.65 points. The stigmatization level was proportionately dependent on the clinical stage of the disease (p=0.006).6 The location of the lesions represented an important factor, with disease involvement in exposed skin areas, such as the head and the nape, also playing a crucial role in the level of stigmatization (p=0.031).6 In addition, a significant impact of HS on a wide spectrum of psychophysical aspects including fatigue, depression, and overall activity was observed, as well as an even greater impairment of related QoL than previously documented.6 According to the authors, the advancement of the disease was the most important factor negatively influencing patients’ well-being.6
In a qualitative study in 12 HS patients, participants reported feeling shame, unworthy, and not lovable because of their disease, especially when they had many large scars and active inflammatory lesions.13 Patients reasoned that their lesions look ugly, smell, appear quite frequently, and are painful or itchy. They expressed fear of revealing their scars and experiencing stigmatization, and reported sadness and worry when they were unable to do their work, or if the disease was unaffected by the treatment provided. The patients find the symptoms very embarrassing and repulsive, feel themselves to be impure, and feel shy about it. They tend to remain at home during periods of heavy malodorous discharge and try to hide disfiguring scars and affected areas by wearing appropriate clothing, such as long-sleeved blouses, trousers, or long shorts.13They also fear people’s negative reaction when they reveal the usually hidden parts of their body, e.g., in a sexual relationship or in a changing room, and modify their behavior, even by limiting their public appearances, in order to prevent an unpleasant situation from occurring.13
The fear of stigmatization and exclusion from the group is very common among patients with HS. Patients with lesions located at visible parts of the body experience a higher level of stigmatization compared with those with invisible lesions.13 Nevertheless, disease made invisible as covered by clothes may be revealed by smell. Therefore, most HS patients present a fear of stigmatization related to revealing the normally hidden affected areas and/or to an involuntary release of bad smell. As a result, they tend to adopt HS-specific precautions, such as use of perfume, bandages, and spare clothes.13 Furthermore, the fear of stigmatization promotes isolation.5,13 Patients feel ashamed of their symptoms and avoid talking about their disease, even with their family.13 Pain, itch, foul-smelling purulent discharge, and the fear of other people’s reactions to their symptoms can prevent patients from various social activities, including physical exercise and sports.5,13 In such activities, HS can make movements painful, and sweating may cause stinging and malodor.14
Malodourous discharge in patients with HS has a strong psychosocial impact and is often reported as a source of embarrassment, low self-esteem, social stigma, and barriers to interpersonal relationships.7,13 Alavi et al, in a cross-sectional study of 51 HS patients, assessed the relationship between the severity of malodourous discharge and QoL.14 They found that the severity of odour significantly predicts the total Skindex score, after controlling for disease severity as measured by the Hurley stage and Sartorius score (R2=0.39, F=8.11, p<0.0001). They also found correlations between odour severity and several questionnaire items in Skindex-29 and DLQI that pertain to social and sexual functioning, in addition to an item on the experience of social isolation.14 The same study showed that HS affects also other aspects of patients’ lives, including the emotional and social functioning, which are not related to disease severity. This may be due to the fact that odour and disfigurement may lead to embarrassment and a low self-image even in early stages of the disease. The fear of malodourous discharge, disfiguring scars, unpredictable flare, and lack of disease control results in low self-esteem, depression, and isolation, as a coping mechanism with the disease.14
Kouris et al studied 94 patients with HS for quality of life, depression, anxiety, loneliness, and self-esteem, using the Dermatology Life Quality Index (DLQI), the Hospital Anxiety and Depression Scale (HADS), the UCLA Loneliness Scale (UCLA-Version 3), and the Rosenberg Self-Esteem Scale (RSES), respectively.12 The patients with HS presented significantly higher anxiety (6.41±3.31 vs 5.00±1.59, p<0.001); depression (5.45±2.79 vs 4.16±1.54, p<0.001); loneliness and social isolation scores (42.86±8.63 vs 35.57±6.17, p<0.001); and lower self-esteem scores (18.91±1.79 vs 19.77±2.53, p=0.008) compared with a group of healthy controls.12 However, the impact of HS on patients’ self-esteem was not related to the disease severity. This may be due to the fact that the malodor and the scars resulting from even a single or few abscesses (Hurley stage I) can lead to reduced self-image and embarrassment.12
Negative perception of the body image refers to dissatisfaction with one person’s appearance and feelings of unattractiveness.15 Reduced body image is closely related to self-stigma. Schneider-Burrus et al,15 in case-control study of 46 HS patients and 41 healthy controls, investigated the impact on body image and its associations with disease severity, age at onset, disease duration, obesity, depression, using the Frankfurt Body Concept Scale (FKKS) and the Hospital Anxiety and Depression Scale (HADS). HS significantly reduced body image (mean FKKS score: 234.2 [5.4] in patients, and 276.9 [5.7] in controls; p<0.001), even when controlled for BMI, and this effect was associated with depression and anxiety. A correlation was also found for the extent of body image disruption and BMI (r =−0.589; p<0.001), HADS-depression score (r = −0.619; p<0.001), and HADS-anxiety score (r =−0.340; p= 0.03). No association was found for the body image score and the severity of HS, age at onset of disease, and duration of disease. The authors concluded that altered body image is another element of the psychosocial distress that HS patients experience, which might be linked to depression and anxiety and thus it could represent a target for therapeutic interventions.
Several studies have found that the prevalence of HS is higher in patients of African origin.16–18 It is well established that racial stigma could contribute to psychological impairment and lead to marginality.19 As a consequence, stigmatized and marginalized people have low self-esteem and reduced ability to resist to discrimination.19 As race could be also a risk factor for stigmatization,19 race, and ethnicity of HS patients should be taken into account in their evaluation for stigmatization, psycho-social sequelae, and impact on quality of life.
It is well established that obese people experience discrimination and stigmatization not only in their interpersonal relationships but also in the work and daily life.20,21 Obesity leads to low self-esteem and body image dissatisfaction.21 In HS, increased body mass index (BMI) has been correlated to more severe disease, Hurley stage III, and more recurrences of the disease.22,23 Therefore, high BMI might be considered as a contributing factor to HS stigmatization, isolation, body image dissatisfaction, and low self-esteem.
Perspectives
Stigmatization appears to be an important part of psychosocial morbidity in HS. Assessment of all types of stigma should be an integral part of patients’ evaluation. Further studies are needed to assess the extent and prevalence of stigmatization in HS and to develop effective screening and treatment strategies. Management should incorporate a patient-centered, optimized selection of empirically supported pharmacologic and behavioral treatments, in the context of a multidisciplinary approach that includes psychosocial assessment and intervention. Future research could study also the coping strategies utilized by patients with HS, the impact of teaching those coping strategies to patients with less positive styles, and the subsequent impact on QoL and HS severity.24
A variety of patients' associations have been established worldwide, including a European Federation of HS Patients' Organizations (EFPO), as it proves easier to talk with strangers coping with the same symptoms than with their family and friends. This provides an opportunity for patients to find out how others manage the disease and how they behave in daily life. Information campaigns addressed to the general public, explaining the true nature of HS, will not only improve the screening for the disease, but also will alter the negative attitudes of the social environment leading to stigmatization of HS patients.
Although much progress has been achieved already in understanding the mechanisms and impact of HS, as well as in treating HS, many more remain to be done at both medical and social level.
Abbreviations
SD, standard deviation; DLQI, Dermatology Life Quality Index questionnaire; BDI-SF, Beck Depression Inventory-Short Form questionnaire; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue Scale questionnaire; Q-LES-Q-SF, Quality of Life Enjoyment and Satisfaction Questionnaire short-form questionnaire; EQ-5D and VAS for health-related quality of life; HADS, Hospital Anxiety and Depression Scale; UCLA, loneliness scale version 3; RSES, Rosenberg Self-Esteem Scale; FKKS, Frankfurt Body Concept Scale.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Van Beugen S, van Middendorp H, Ferwerda M, et al. Predictors of perceived stigmatization in patients with psoriasis. Br J Dermatol. 2017;176:687–694. doi:10.1111/bjd.14875
2. Goffman E. Stigma: Notes on the Management of Spoiled Identity. New York: Simon and Schuster; 2009.
3. Jones EE, Farina A, Hastorf AH, Markus DT, Miller RA. Social Stigma. In: The Psychology of Marked Relationships. New York: W H Freeman & Co; 1984.
4. Baumeister RF, Leary MR. The need to belong: desire for interpersonal attachments as a fundamental human motivation. Psychol Bull. 1995;117:497–529.
5. Zouboulis CC, Desai N, Emtestam L, et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J Eur Acad Dermatol Venereol. 2015;29:619–644. doi:10.1111/jdv.12966
6. Matusiak L, Bieniek A, Szepietowski JC. Psychophysical aspects of hidradenitis suppurativa. Acta Derm Venereol. 2010;90:264–268.
7. Deckers IE, Kimball AB. The handicap of hidradenitis suppurativa. Dermatol Clin. 2016;34:17–22.
8. Alavi A, Anooshirvani N, Kim WB, Coutts P, Sibbald RG. Quality-of-life impairment in patients with hidradenitis suppurativa: a Canadian study. Am J Clin Dermatol. 2015;16:61–65.
9. Pavon Blanco A, Turner MA, Petrof G, Weinman J. To what extent do disease severity and illness perceptions explain depression, anxiety and quality of life in hidradenitis suppurativa? Br J Dermatol. 2019;180:338–345. doi:10.1111/bjd.17123
10. Von der Werth JM, Jemec GB. Morbidity in patients with hidradenitis suppurativa. Br J Dermatol. 2001;144:809–813. doi:10.1046/j.1365-2133.2001.04137.x
11. Onderdijk AJ, van der Zee HH, Esmann S, et al. Depression in patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2013;27:473–478. doi:10.1111/j.1468-3083.2012.04468.x
12. Kouris A, Platsidaki E, Christodoulou C, et al. Quality of life and psychosocial implications in patients with hidradenitis suppurativa. Dermatology. 2016;232:687–691. doi:10.1159/000453355
13. Esmann S, Jemec GB. Psychosocial impact of hidradenitis suppurativa: a qualitative study. Acta Derm Venereol. 2011;91:328–332. doi:10.2340/00015555-1082
14. Alavi A, Farzanfar D, Lee RK, Almutairi D. The contribution of malodour in quality of life of patients with hidradenitis suppurativa. J Cutan Med Surg. 2018;22:166–174. doi:10.1177/1203475417745826
15. Schneider-Burrus S, Jost A, Peters EMJ, Witte-Haendel E, Sterry W, Sabat R. Association of hidradenitis suppurativa with body image. JAMA Dermatol. 2018;154:447–451. doi:10.1001/jamadermatol.2017.6058
16. Vlassova N, Kuhn D, Okoye GA. Hidradenitis suppurativa disproportionately affects African Americans: a single-center retrospective analysis. Acta Derm Venereol. 2015;95:990–991. doi:10.2340/00015555-2176
17. Vaidya T, Vangipuram R, Alikhan A. Examining the race-specific prevalence of hidradenitis suppurativa at a large academic center; results from a retrospective chart review. Dermatol Online J. 2017;23:
18. Reeder VJ, Mahan MG, Hamzavi IH. Ethnicity and hidradenitis suppurativa. J Invest Dermatol. 2014;134:2842–2843. doi:10.1038/jid.2014.220
19. Ahmad WI, Bradby H. Locating ethnicity and health: exploring concepts and contexts. Sociol Health Illn. 2007;29:795–810. doi:10.1111/j.1467-9566.2007.01051.x
20. Puhl RM, Heuer CA. Obesity stigma: important considerations for public health. Am J Public Health. 2010;100:1019–1028. doi:10.2105/AJPH.2009.159491
21. Puhl RM, Heuer CA. The stigma of obesity: a review and update. Obesity (Silver Spring). 2009;17:941–964. doi:10.1038/oby.2008.636
22. Theut Riis P, Saunte DM, Benhadou F, et al. Low and high body mass index in hidradenitis suppurativa patients-different subtypes? J Eur Acad Dermatol Venereol. 2018;32:307–312.
23. Boer J. Does obesity cause a distinct phenotype of hidradenitis suppurativa? J Eur Acad Dermatol Venereol. 2018;32:e195–e196. doi:10.1111/jdv.14707
24. Kirby JS, Sisic M, Tan J. Exploring coping strategies for patients with hidradenitis suppurativa. JAMA Dermatol. 2016;152:1166–1167. doi:10.1001/jamadermatol.2016.1942
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.