Back to Journals » Psychology Research and Behavior Management » Volume 15
Perspectives on Dialectical Behavior Therapy and Mentalization-Based Therapy for Borderline Personality Disorder: Same, Different, Complementary?
Authors Stoffers-Winterling JM ![]() , Storebø OJ
, Storebø OJ ![]() , Simonsen E, Sedoc Jørgensen M, Pereira Ribeiro J, Kongerslev MT, Lieb K
, Simonsen E, Sedoc Jørgensen M, Pereira Ribeiro J, Kongerslev MT, Lieb K
Received 17 May 2022
Accepted for publication 11 September 2022
Published 28 October 2022 Volume 2022:15 Pages 3179—3189
DOI https://doi.org/10.2147/PRBM.S342257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Jutta M Stoffers-Winterling,1 Ole Jakob Storebø,2,3 Erik Simonsen,4,5 Mie Sedoc Jørgensen,2 Johanne Pereira Ribeiro,2,3 Mickey T Kongerslev,2,3,5 Klaus Lieb1
1Department of Psychiatry and Psychotherapy, University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany; 2Psychiatric Research Unit, Psychiatry Region Zealand, Slagelse, Denmark; 3Department of Psychology, University of Southern Denmark, Odense, Denmark; 4Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 5Mental Health Services East, Psychiatry Region Zealand, Roskilde, Denmark
Correspondence: Ole Jakob Storebø, Psychiatric Research Unit, Psychiatry Region Zealand, Fælledvej 6, Slagelse, 4200, Denmark, Tel +45 24965917, Email [email protected]
Abstract: Current evidence suggests that individuals with borderline personality disorder (BPD) are likely to benefit from specialized, or BPD-specific, treatments. Dialectical behavior therapy (DBT) and mentalization-based treatment (MBT) are currently the most intensively researched BPD treatments. Reviewing the current research, this paper highlights similarities and differences between the two treatments, and discusses possible ways they could complement each other. As the effectiveness of specialized treatments for BPD in general has been determined with some certainty, research now tends towards individualized approaches, identifying predictors of optimal treatment response. However, it is still to be settled who might profit from a combination of or sequential treatment with DBT and MBT.
Keywords: psychotherapy, treatment, dialectical behavior therapy, DBT, mentalization-based therapy, MBT, borderline personality disorder
Introduction
Current evidence-based treatment guidelines consistently recommend psychotherapy as the first-line treatment of borderline personality disorder (BPD).1 Pharmacotherapy has been studied less intensively in recent years,2,3 after enormous effort had been spent on application studies that resulted in disappointing results.4,5 The initial therapeutic nihilism, according to which people affected by BPD could neither benefit from nor maintain a steady attendance to psychotherapy over a longer period, emerged from very early observations of people with BPD being treated with classic psychoanalysis, but is no longer tenable.6 Since no main diagnostic BPD criterion shared by all people diagnosed with BPD exists, BPD is a highly heterogeneous disorder.7 Instead, any five or more out of nine optional criteria must be met, resulting in 256 different combinations of diagnostic criteria. This heterogeneity might have contributed to the difficulties in developing BPD-tailored treatment approaches that meet the needs and challenges of both patients and therapists who undergo an oftentimes intensive treatment together. Nevertheless, disorder-specific approaches are available today that have been found to be effective in ameliorating symptoms of BPD and associated psychopathology.8
What Constitutes a Disorder-Specific Treatment Approach for BPD?
For many years, several different psychotherapies have been used to treat BPD. Disorder-specific approaches can be delivered in individual or group format or as a combination of the two. Though disorder-specific, most of the available treatments have emerged from the major psychotherapeutic schools such as psychodynamically oriented psychotherapy, cognitive-behavioral or humanistic therapy.
BPD-specific treatments adapt the therapeutic approach to the specific individual and the situation as recommended in person-centered therapy. In particular, they recognize a high risk of dropout from therapy because of the BPD-associated disturbances in relational capacities, distorted perceptions, and interpretations of self and others, as well as previous traumatic relationship experiences and impulsive behavior tendencies.9 BPD-specific approaches, therefore, pay special attention to the ongoing maintenance of the therapeutic relationship. Therapists, in turn, often face challenging behaviors such as idealization and devaluation, desperate efforts to avoid actual or feared abandonment, especially at the end of therapy, and repeated crisis-like developments. Most disorder-specific procedures, therefore, highlight the importance of supervision or intervision for the therapists as an integral part of treatment. Due to the aforementioned challenges, the therapists should aim to establish a well-defined therapeutic relationship and setting which is reliable, appreciative, and sustainable. BPD treatments usually use treatment agreements and/or case formulations. Such tools are used to specify a reliable framework for both sides, within which constructive therapeutic cooperation is possible.10 In most BPD therapies, the therapists take an active stance, ie, they show their own involvement in the experience and reactions of the person affected. Depending on the theoretical basis of the approaches, the techniques have different names and are of varying importance.
In a very insightful review,9 Weinberg et al systematically identified the following treatment elements that are used by BPD-tailored approaches (cf. to Table 1):
 |
Table 1 Common Treatment Elements of BPD-Specific Therapy Approaches According to Weinberg et al. |
The recent Cochrane review on psychotherapy for BPD, which comprehensively and systematically analyzed randomized controlled trials (RCTs) according to methodologically rigorous criteria, supports the superiority of disorder-specific approaches over nonspecific control treatments: Small to moderate statistically significant effects were found for BPD-specific interventions in general as compared to non-specific treatments, such as treatment as usual regarding BPD severity, self-harm, suicide-related outcomes, and psychosocial functioning.3 Given the crucial importance of these outcomes, specifically regarding self-harm and suicide-related outcomes, these findings support the use of disorder-specific psychotherapies in BPD, despite the small to moderate effect sizes and low to moderate certainty of the evidence.3 The evidence was rated of low to moderate certainty for these effects, mainly because of the risk of bias, imprecision, and affiliation bias of investigators.3
Though there is some variation regarding the availability of individual treatments in different countries, the most common and most intensively studied treatments for BPD are dialectical-behavioral therapy (DBT),11 mentalization-based therapy (MBT),12 schema-focused therapy (SFT),13 transference-focused psychotherapy (TFP),14 cognitive analytic therapy (CAT),15 and system training for emotional predictability and problem-solving (STEPPS).16
In the following, we introduce the two specialist treatments DBT and MBT. Both treatments contain underlying theoretical concepts and explicit manualization of techniques. As such, they have substantially influenced the field and advanced our understanding of BPD. Both have stimulated further developments for patient groups with defined comorbidities and are probably the most prevalent treatments in clinical practice. We will note similarities and differences in both treatment formulation and formats, and review the existing effectiveness data. In addition, we will highlight results from RCTs that investigate the effectiveness of various specific components or significant further developments of the two approaches. Last, we will discuss the perspective of combining DBT and MBT, and try to determine who might profit from a combination or sequential treatment with DBT and MBT.
DBT and MBT: Two of a Kind?
Both methods traditionally make use of a treatment team, combine individual and group therapy, pursue explicit therapy goals that are based on a coherent theoretical base, and keep constant attention on therapy-interfering processes.
Further, both methods focus on current events and experiences in the here and now, use empathic validation, let the therapist take an active stance, dispense with the use of interpretations, and provide supportive inter- or intravision for the treatment team.17
The treatments, however, also differ in important ways. One major difference is the use of the therapeutic relationship. MBT explicitly focuses on the therapeutic relationship to research and train mentalizing within an ongoing interpersonal process. Instead, DBT rather uses the relationship to support skills coaching.17 MBT is usually conducted over 18-months, while standard DBT is conducted over 12-months. Moreover, MBT and DBT differ regarding their theoretical basis and the postulated “core” of BPD. MBT is primarily based on developmental psychopathology theory, with a focus on the self and affect regulation.12,18 Drawing from Bowlby’s attachment and the Theory of Mind theory, it is claimed that the sense of self and others is built on the infant’s experience of the caregiver’s expressions. If no secure attachments can be built, the mentalizing capacities are affected, and PD-related difficulties result as distinct internalized and externalized features. Mentalization, however, means the capacity to implicitly and explicitly make sense of subjective states and mental processes of oneself and others. Persons who have not developed healthy, secure attachment to their primary caregivers, are likely to develop an unstable sense of self, and problems in establishing sustainable, constructive social interactions characterized by epistemic trust, or considering diverse perspectives on how overt behavior or cognitive processes can be understood.17 MBT aims to support the patient’s understanding and recognition of own and others’ feelings and thoughts underlying overt behaviors, as well as to improve emotion regulation capacity and the ability to manage impulsiveness. The therapeutic relationship is used to study and train mentalizing of interpersonal processes.
DBT, on the other hand, as a cognitive-behavioral therapy-informed treatment, conceptualizes disturbed affect regulation as the core problem in BPD, ie, a high emotional reactivity combined with a diminished ability to recognize one’s feelings and to deal with them in a functional way. In its standard version, DBT includes the four components individual therapy, group skills training, telephone coaching in case of crisis and the therapist being part of a consultation team. DBT aims to change behavior and to enforce the ability to tolerate difficult or painful feelings through a focus on skills in mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness skills.19 Furthermore, DBT builds on a bio-social theory accounting for biological vulnerabilities along with environmental adversities as the core aetiologic factors that contribute to the development of BPD. According to this, temperamental factors (such as a heightened emotional sensitivity to external stimuli, intense reactions, and slow return to the emotional equilibrium) along with childhood adversities (such as emotional, physical, or sexual abuse, chronic invalidation, or neglect) promote a pronounced emotional dysregulation. Stress tolerance skills are used to help individuals manage and level down emotional distress, instead of feeling helpless and overwhelmed. Vulnerabilities and sensitivities are met with non-judging acceptance and validation by the therapist, who at the same time aims to find a way to support the individual to “get out of hell”.20 The focus on dialectical and wholeness is also important, favoring techniques that center around acting and personal involvement in change on the one hand, but also acceptance on the other.
MBT group sessions have the character of group therapy in a traditional psychodynamic sense. All group members are seated in a circle of chairs, and if somebody is missing, an empty chair is used to indicate this. While there is no teaching, the group members bring up incidents that have occurred since the last meeting, and all group members are invited to “mentalize” around that incident, eg, discuss hypotheses about mental states of the persons involved. The main difference between DBT and MBT regarding group sessions might be that DBT explicitly does not explore group processes beyond using them as an opportunity to practice skills, whereas MBT encourages them as an opportunity to enhance mentalizing capacities.
In contrast, DBT group sessions are not called “therapy” but “skills training” to account for the fact that the sessions are held in a group setting but in a seminar-like atmosphere. These sessions focus on the introduction of skills as specified in the manual, while actual skills acquisition is meant to happen between the group sessions when each individual practices these skills and reports their use and effects on a diary card.
In sum, both methods focus on the treatment of self-harm, impulsiveness and emotional dysregulation. DBT, however, intends to directly modify and prevent such behavior by skills use. MBT intends to enhance mentalizing capacities in order to make the inner and outer world understandable to the client, so that escalating behavior is prevented. These differences can best be understood by the fact that MBT is a psychodynamically rooted therapy (thus focusing more on the attachment relationships and psychodynamic processes), whereas DBT mainly is a behavior therapy (thus mainly focusing on changing problematic behaviors).
Evidence on DBT
The most comprehensive evidence is currently available on DBT. About one-third of all available RCTs on psychotherapeutic interventions for BPD focus on DBT or DBT adaptations for specific patient groups.3 Table 2 provides an overview of currently available RCTs comparing DBT and DBT adaptations with a non-specific control condition such as treatment as usual (TAU).
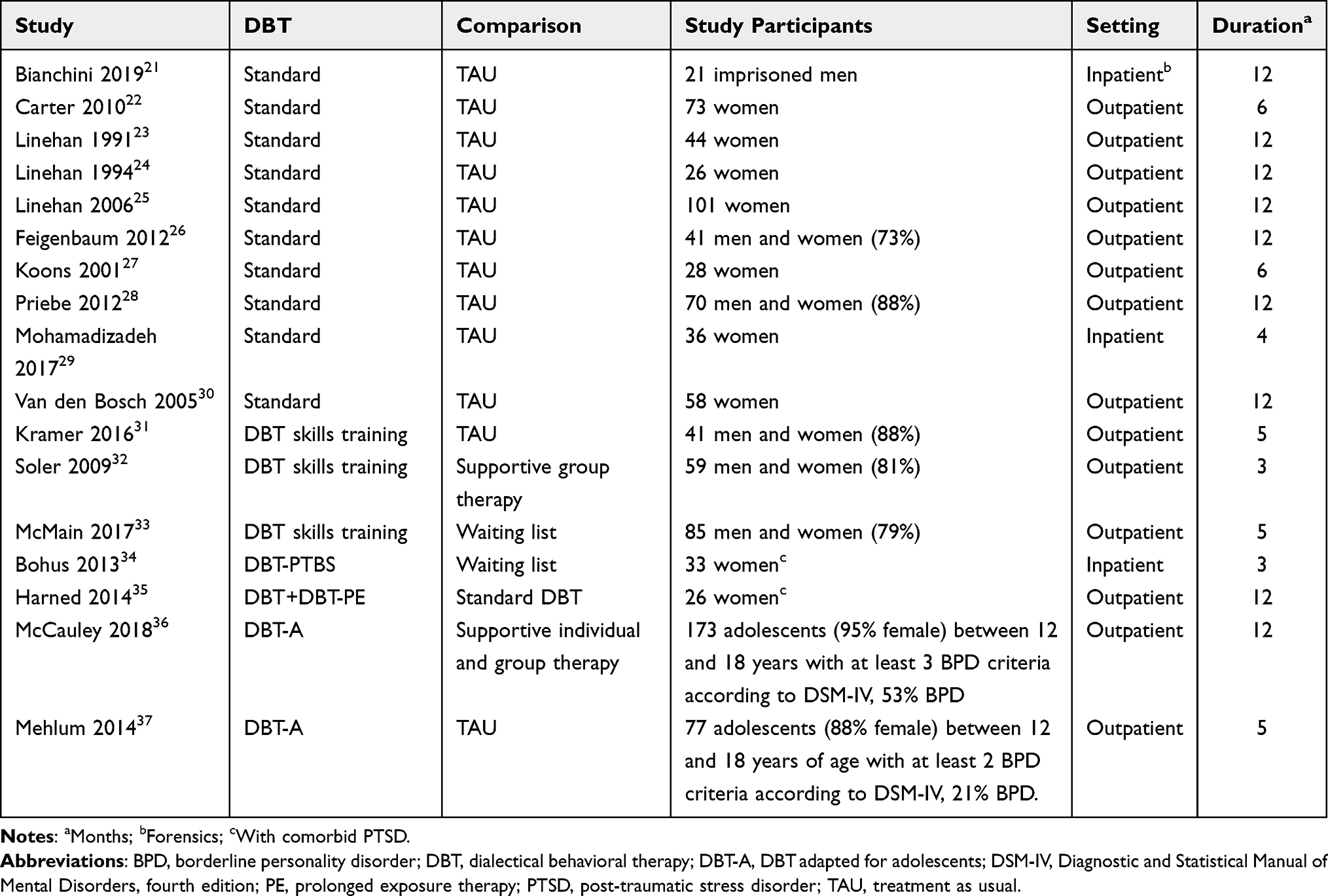 |
Table 2 Randomized-Controlled Trials Comparing DBT to Nonspecific Control Conditions in Samples with BPD |
In the Cochrane review of Psychotherapy for BPD, significant effects emerge for the comparison of standard DBT (including the four components individual therapy, group skills training, telephone coaching in case of crisis if needed, and the therapist being part of a consultation team) with nonspecific control groups such as TAU. Statistically significant effects are observed regarding BPD severity, psychosocial functioning, and individual BPD symptom expressions (self-injurious behavior, anger/rage, dissociations)3 (cf. Table 3).
 |
Table 3 Pooled Effect Estimates for Disorder-Specific Procedures in General and DBT, and MBT Specifically According to Outcomes |
DBT is usually delivered in an outpatient setting. In an RCT comparing a combination of inpatient and outpatient DBT with the usual 12-month outpatient DBT, no differences in efficacy were found.38 DBT skills training is typically delivered concurrently with individual DBT. The pooled effects from multiple studies of DBT skills training alone show that participants may benefit in terms of overall BPD severity, specific BPD symptom expressions (affective instability, impulsivity, anger/rage), and social functioning levels.31–33 These findings support the beneficial effects of skills training groups.31–33,39 In a dismantling trial, which compared the individual treatment modules of DBT individual therapy, DBT skills training, and standard combined treatment, Linehan et al also confirmed the positive effect of group training: The two groups that participated in skills training had larger and faster benefits concerning self-injurious behavior and depressive symptoms.40 However, more randomized comparisons of skills-groups alone to standard DBT are lacking, and long-term effects of group-only treatments in general are uncertain.39 Therefore, the findings support the use of skills groups, but do not allow for concluding that these could replace individual or combined treatment.
In addition to standard DBT, adaptations for individuals with BPD plus comorbid post-traumatic stress disorder (PTSD) are now available. Two studies demonstrate that even in the presence of BPD, PTSD can be treated safely and effectively, and that individuals affected by both diagnoses can benefit more from trauma-adapted DBT than from standard DBT or standard trauma treatment.34,35,41
An adapted version of DBT was found to have beneficial effects on BPD severity, suicidality, self-injury, and depression in adolescents with significant BPD symptoms in two RCTs.36,37 A DBT adaptation is now also available for relatives of affected individuals (of all ages; DBT Family Connections, DBT-FC).42 Initial studies indicate positive effects in terms of distress, grief, and family functioning.43,44 In a non-randomized comparison of DBT-FC, no differences in effectiveness were observed if DBT-FC was delivered face-to-face or in an online format.45
Evidence on MBT
Besides DBT, MBT is the psychotherapy for which the most RCTs are currently available (cf. Table 4). In the Cochrane review of psychotherapies for BPD, a difference in effects was seen in terms of a greater reduction of self-injurious, suicidal behavior, and interpersonal problems by MBT as compared to unspecific control treatments (cf. Table 3).3
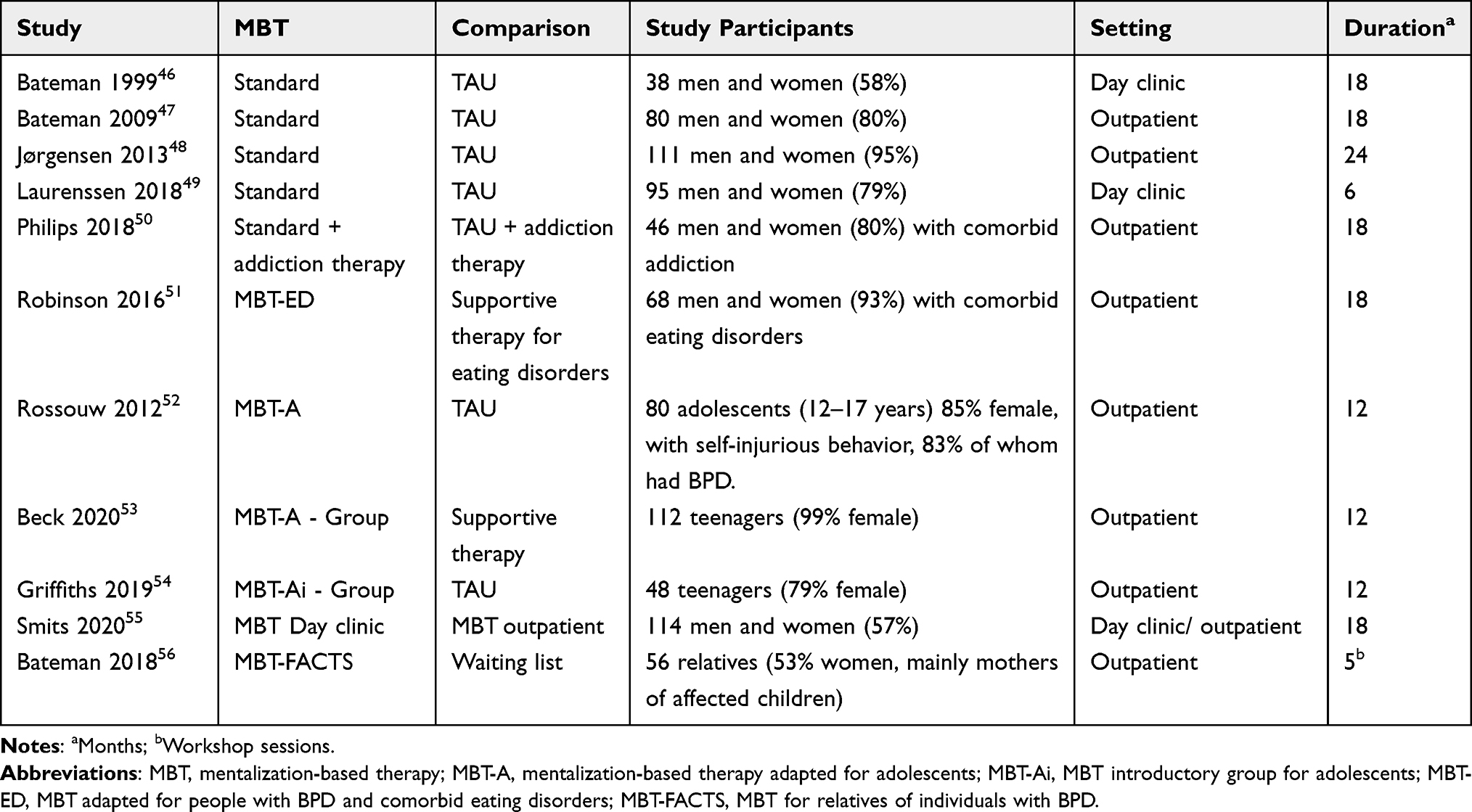 |
Table 4 Randomized-Controlled Trials Comparing MBT to Nonspecific Control Conditions in Samples with BPD |
One trial investigated the efficacy of an intensive two-year MBT intervention, which included both group and individual therapy.48 This intervention was compared with two years of less intensive (biweekly) supportive group therapy. There were no significant differences in outcome between the two treatments, but the authors found that both treatments showed large changes from baseline.48 Another trial investigated the difference between two versions of MBT: day-hospital MBT and intensive out-patient MBT.55 This trial found that there were no differences between groups on the primary outcome, but the day-hospital version of MBT showed a tendency for superiority on the secondary outcomes.55 In a three-year follow-up study, there were no differences between the day-hospital version of MBT or the more intensive out-patient MBT. Both groups, however, showed large improvements from baseline.57
A trial of MBT for individuals with BPD and comorbid addiction found no effects on addiction symptoms as compared to standard substance use disorder treatment.50 An adaptation for people with BPD and comorbid eating disorders was investigated in the MBT-ED trial, which similarly to the trial on comorbid addiction, found very limited effects on eating disorder symptomatology.51
Two RCTs, each examining the effects of MBT group treatment in adolescents with BPD or pronounced BPD features, found no evidence of MBT superiority as compared to treatment as usual.53,54 The evidence is summarized in a systematic review that showed limited evidence on the effect of MBT on adolescents when compared to control interventions.58 Another RCT compared individual MBT treatment in adolescents to TAU and concluded that it may be effective in reducing self-harm and depression.52
Encouraging effects were observed in an RCT of an MBT-based program for significant others, the MBT-FACTS trial, where the intervention was delivered by peers (relatives who were also affected).59 Participation resulted in less family conflict, improved well-being, and better family functioning levels compared to a waitlist control group.
Comparing Dialectical Behavior Therapy and Mentalization-Based Treatment
Research on psychotherapy for BPD and specifically DBT and MBT has made great progress over the past decade. More than one-third of all available RCTs have been published in the last five years. However, a direct randomized comparison of DBT and MBT has not yet been conducted. Even an indirect comparison of treatment effects is difficult, given that DBT and MBT research traditionally focus on different outcomes: While DBT traditionally targets impulsivity-related behaviors (including self-harm and suicidal behavior) as well as inappropriate anger, MBT research rather takes an interest in the effects on interpersonal outcomes and non-BPD-specific psychopathology such as depression or as expressed by composite scores like the Symptom Checklist-90-R (in −90-R) scale.3,60
In a subgroup analysis, Storebø et al found that the intervention effect did not vary between subgroups of MBT and DBT when compared to unspecific controls for BPD severity or psychosocial functioning.3 Taking into account the findings supporting the superiority of each of the two treatments to unspecific controls, this means both can be regarded effective regarding these two outcomes.
Recently, the results of a naturalistic, non-randomized controlled study carried out in the personality disorder services in the UK were published. No differences in intervention effects were observed between DBT and MBT after 12 months of treatment – for neither of the outcomes self-harm, BPD severity, emotional dysregulation, interpersonal relationships, or dissociation.61 There was, however, a steeper decline in self-harm and emotion dysregulation in the DBT group, which remained significant after adjustment for potentially confounding variables. There is some evidence indicating that DBT and MBT share some common helpful therapeutic processes. A mixed-methods re-analysis of the previously mentioned non-randomized comparison of DBT and MBT61 found that patients’ accounts of learning not to react impulsively, questioning one’s thoughts and assumptions, communicating more effectively, and exposing oneself to painful emotions were associated with less self-harm at the end of treatment across both therapies.62 Also, difficulties in the therapeutic relationship or with group members were associated with more severe BPD severity and emotion dysregulation at end of treatment for both MBT and DBT.61,62
Discussion
Though there are some differences in duration, frequency, and intensity between DBT and MBT, they share many similarities as well: They are both relatively complex interventions that usually combine individual and group treatment and are both delivered by a team of therapists in an outpatient setting. They aim to ameliorate impulsive behavior, including self-harm, and emotion dysregulation. To all intents and purposes, are DBT and MBT essentially just one and the same, achieving the same treatment goals, but using different techniques and wording?
Rather than using them interchangeably at random, it has been suggested to be attentive to the clinical characteristics of an individual; ie, which symptoms, and which severity. DBT is usually regarded the first-line treatment when it is necessary to address destructive behaviour.63 If frequent crises occur, reflective functions are impaired, and treatment will be interrupted repeatedly. However, once stress tolerance has increased by DBT treatment, and overt treatment-interfering behavioral problems have remitted, emotions come into the focus of treatment. Though mentalizing can already be found in many aspects of DBT (eg, “beginner’s mind”, non-judging validation, chain analysis), DBT might profit from the integration of techniques that are described in detail in the MBT manual, eg, to work towards a flexible mindset even in emotionally demanding situation.63 Both treatments seem complimentary here, as high emotional arousal disrupts adaptive mentalizing, whereas adaptive mentalization facilitates emotion regulation.63 Though both treatments pay constant attention to the therapeutic relationship, and DBT covers interpersonal effectiveness, MBT includes more detailed micro-tools to address and make use of relational disturbances as they occur.17 Once a stable level of minimum psychosocial functioning is achieved, it has been suggested to use General Psychiatric Management for long-term, low-frequency maintenance.20
In sum, DBT may either be followed or augmented by MBT, depending on the current clinical picture and severity of symptoms. At this point, it is mostly agreed upon from clinical expertise that a person with BPD and externalizing pathology and/or self-harm, self-destructive behaviors might better benefit from DBT, followed by MBT to gain more insight into relational difficulties and attachment patterns. However, a coherent case formulation including individual treatment goals and a transparent treatment structure are a prerequisite before borrowing interventions and techniques from MBT (or any other BPD-specific treatment).
Currently, there is very little research available on the systematic combination of DBT and MBT elements. To our knowledge, only a single, non-randomized study comparing the effects of DBT alone to DBT plus MBT in an inpatient sample exists.64 The only difference in effect between groups was found for the outcome of affective mentalizing, which was higher in the combined group. Since the enhancement of mentalizing capacities is an explicit treatment goal in MBT but not DBT, this finding is not surprising — on the contrary, one would not expect an increase in the outcome “skills-use” in persons who solely received MBT. More systematic research is needed that investigates the effects of the combination of DBT and MBT, or enhancement of standard DBT and standard MBT by adding elements of the alternate therapy, depending on the individual phenomenology and treatment goals. Importantly, the effects on direct, clinical outcomes like general functioning and overall BPD severity, that are of interest to people with BPD must be assessed, rather than the ability to use acquired techniques which are only vehicles to achieve beneficial effects.
Because resources are limited, not all individuals with a diagnosis of BPD need (and have the opportunity) to undergo specialized treatment by interventions such as DBT or MBT. As a first step, individuals with BPD might profit from General Psychiatry Management as suggested by Gunderson.65 More severe pathology might require specialized treatment such as DBT or MBT. In severe, persistent cases, sequential treatment with first DBT targeting acute, impulsive behavior, followed by MBT targeting persistent interpersonal difficulties might be indicated.66
In practice, resources are limited, and too many individuals are waiting for any kind of specialist treatment. Therefore, and given the expensive and time-consuming training that is needed to become a DBT or MBT therapist, it seems illusionary that therapists would be trained in both treatments, let alone other specialist treatments. Even in an ideal world with unlimited access to specialized therapies, it would be too costly and, again, time-consuming to let people undergo full courses of both treatments sequentially. However, it might be a first step to integrate a look beyond the own nose in DBT and MBT trainings, ie, let trainees learn some basic information about the alternate therapy, and how it might be used to augment treatment. However, a coherent case formulation and treatment plan is obligatory to reasonably integrate techniques of other treatments.
However, it is still unclear which characteristics predict an optimal response to a certain treatment. Building on the current findings that individuals with a diagnosis of BPD are likely to profit from specialized BPD treatments, future research should focus on the question of individualized treatments in order to increase moderate treatment gains. Specifically, more research is needed to understand who benefits optimally from which treatment. This is important to avoid frustrating treatment experiences for the individual, as it is likely to foster therapeutic pessimism and adverse outcomes, especially in affected youth. Also, available therapeutic resources must be allocated in a fair and economic way, taking into account the individual’s needs, in order to ameliorate both access to and effectiveness of mental health care as stepped care approaches suggest.67,68 This would help to reduce costs for individuals and health-care systems (both financial and time), and save treatment resources for individuals who might optimally profit.
Since the upcoming ICD-1169 will take a dimensional approach of diagnosing PDs in terms of dominating personality traits and abolish the existent categorical PDs (except from the newly introduced “borderline pattern”, 6D11.5 that reflects BPD as defined in the DSM-5), it will be even more important to individualize case formulations, treatments and techniques with respect to the individual clinical picture and treatment goals. Moreover, the newly introduced ICD-11 categories of mild, moderate and severe personality disorder (6D10.0 to 6D10.2) might be considered in terms of treatment intensity and duration. This would be in line with the suggested sequential proceeding, where impulsiveness-related behavior is focused first, then emotional dysregulation and interpersonal problems. We do believe that it is important to conduct research into the question what benefits each therapy brings, and benefits more from one or the other approach. In our Cochrane review on psychological therapies for people with borderline personality disorder3 we found evidence for both treatments for the “average patient”, but we do not know which patients benefits the most from which treatment. An individual patient data meta-analysis of the available evidence is currently underway to find out which treatments are likely to work in which individuals.70
Acknowledgments
No funding was received for the preparation of this paper.
Disclosure
Jutta M Stoffers-Winterling is a board-certified psychologist, who has received training on dialectical behaviour therapy (DBT) and schema-focused therapy (SFT).
Ole Jakob Storebø (OJS) is a certified specialist in child psychotherapy from the Danish Psychological Association. He is a board-certified therapist in group analysis. He was involved in a trial investigating group mentalization-based treatment (MBT) for adolescents with BPD (Beck 2020).
Johanne Pereira Ribeiro (JPR) has nothing to disclose.
Mickey Kongerslev is a certified specialist in psychotherapy from the Danish Psychological Association. He has received training in group analysis, cognitive behavioural therapy, and MBT. He received money, from private and public agencies, for teaching MBT for BPD, including supervising psychologists under training to becoming licenced “special psykolog” certified by the Danish National Health Authorities, and has published scientific articles together with the developers of this treatment. He also receives money for teaching and supervision in assessment and management of personality disorder.
Mie Sedoc Jørgensen (MSJ) is a trained DBT therapist and conducted a trial on group MBT for adolescents with BPD (Beck 2020). MSJ was not involved in the evaluation of this trial.
Klaus Lieb (KL) is a board-certified cognitive behavior therapist with a special interest in schema therapy. KL has been involved in trials investigating inpatient DBT (Bohus 2004); and inpatient SFT (Reiss 2014). He was not involved in the evaluation of these trials.
Erik Simonsen is a board-certified therapist in group analysis.
The authors report no other conflicts of interest in this work.
References
1. Simonsen S, Bateman A, Bohus M, et al. European guidelines for personality disorders: past, present and future. Borderline Personal Disord Emot Dysregulation. 2019;6(1):9. doi:10.1186/s40479-019-0106-3
2. Stoffers-Winterling J, Storebø OJ, Lieb K. Pharmacotherapy for borderline personality disorder: an update of published, unpublished and ongoing studies. Curr Psychiatry Rep. 2020;22(8):37. doi:10.1007/s11920-020-01164-1
3. Storebø OJ, Stoffers-Winterling JM, Völlm BA, et al. Psychological therapies for people with borderline personality disorder. Cochrane Database Syst Rev. 2020;5:CD012955. doi:10.1002/14651858.CD012955.pub2
4. Schulz SC, Zanarini MC, Bateman A, et al. Olanzapine for the treatment of borderline personality disorder: variable dose 12-week randomised double-blind placebo-controlled study. Br J Psychiatry. 2008;193(6):485–492. doi:10.1192/bjp.bp.107.037903
5. Zanarini MC, Schulz SC, Detke HC, et al. A dose comparison of olanzapine for the treatment of borderline personality disorder: a 12-week randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2011;72(10):4698. doi:10.4088/JCP.08m04138yel
6. Kernberg OF. Borderline Conditions and Pathological Narcissism. Rowman & Littlefield; 1985.
7. American Psychiatric Association D, Association AP. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Vol. 5. Washington, DC: American Psychiatric Association; 2013.
8. Rameckers SA, Verhoef REJ, Grasman RP, et al. Effectiveness of psychological treatments for borderline personality disorder and predictors of treatment outcomes: a multivariate multilevel meta-analysis of data from all design types. J Clin Med. 2021;10(23):5622. doi:10.3390/jcm10235622
9. Weinberg I, Ronningstam E, Goldblatt MJ, Schechter M, Maltsberger JT. Common factors in empirically supported treatments of borderline personality disorder. Curr Psychiatry Rep. 2011;13(1):60–68. doi:10.1007/s11920-010-0167-x
10. Karterud S, Kongerslev MT. Case formulations in mentalization-based treatment (MBT) for patients with borderline personality disorder. In: Case Formulation for Personality Disorders. Elsevier; 2019:41–60.
11. Dimeff LA, Rizvi SL, Koerner K. Dialectical Behavior Therapy in Clinical Practice: Applications Across Disorders and Settings. Guilford Press; 2021.
12. Bateman A, Fonagy P. Handbook of Mentalizing in Mental Health Practice. Psychiatric Pub Inc; 2019.
13. Young JE, Klosko JS, Weishaar ME. Schema Therapy: A Practitioner’s Guide. Guilford press; 2006.
14. Clarkin JF, Yeomans FE, Kernberg OF. Psychotherapy for Borderline Personality. John Wiley & Sons Inc; 1999.
15. Chanen AM, McCutcheon L, Kerr IB. HYPE: a cognitive analytic therapy-based prevention and early intervention programme for borderline personality disorder. In: Handbook of Borderline Personality Disorder in Children and Adolescents. Springer; 2014:361–383.
16. Black D, Blum N, St John D. STEPPS: a practical, evidence-based way to treat borderline personality disorder. Curr Psychiatr. 2009;8:31–37.
17. Daubney M, Bateman A. Mentalization-based therapy (MBT): an overview. Australas Psychiatry. 2015;23(2):132–135. doi:10.1177/1039856214566830
18. Bateman AW, Fonagy P. Mentalization-based treatment of BPD. J Pers Disord. 2004;18(1):36–51. doi:10.1521/pedi.18.1.36.32772
19. Linehan M. DBT? Skills Training Manual. Guilford Publications; 2014.
20. Choi-Kain LW, Albert EB, Gunderson JG. Evidence-based treatments for borderline personality disorder: implementation, integration, and stepped care. Harv Rev Psychiatry. 2016;24(5):342–356. doi:10.1097/HRP.0000000000000113
21. Bianchini V, Cofini V, Curto M, et al. Dialectical behaviour therapy (DBT) for forensic psychiatric patients: an Italian pilot study. Crim Behav Ment Health. 2019;29(2):122–130. doi:10.1002/cbm.2102
22. Carter GL, Willcox CH, Lewin TJ, Conrad AM, Bendit N. Hunter DBT project: randomized controlled trial of dialectical behaviour therapy in women with borderline personality disorder. Aust N Z J. 2010;44(2):162–173. doi:10.3109/00048670903393621
23. Linehan MM, Armstrong HE, Suarez A, Allmon D, Heard HL. Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48(12):1060–1064. doi:10.1001/archpsyc.1991.01810360024003
24. Linehan MM, Tutek DA, Heard HL, Armstrong HE. Interpersonal outcome of cognitive behavioral treatment for chronically suicidal borderline patients. Am J Psychiatry. 1994;151(12):1771–1775.
25. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63(7):757–766. doi:10.1001/archpsyc.63.7.757
26. Feigenbaum JD, Fonagy P, Pilling S, Jones A, Wildgoose A, Bebbington PE. A real‐world study of the effectiveness of DBT in the UK National Health Service. Br J Clin Psychol. 2012;51(2):121–141. doi:10.1111/j.2044-8260.2011.02017.x
27. Koons CR, Robins CJ, Tweed JL, et al. Efficacy of dialectical behavior therapy in women veterans with borderline personality disorder. Behav Ther. 2001;32(2):371–390. doi:10.1016/S0005-7894(01)80009-5
28. Priebe S, Bhatti N, Barnicot K, et al. Effectiveness and cost-effectiveness of dialectical behaviour therapy for self-harming patients with personality disorder: a pragmatic randomised controlled trial. Psychother Psychosom. 2012;81(6):356–365. doi:10.1159/000338897
29. Mohamadizadeh L, Makvandi B, Pasha R, Bakhtiarpour S, Hafezi F. Comparing of the effect of dialectical behavior therapy (DBT) and schema therapy (ST) on reducing mood activity and suicidal thoughts in patients with borderline personality disorder. Acta Med Mediterr. 2017;33(6):1025–1031.
30. Van den Bosch LM, Koeter MW, Stijnen T, Verheul R, van den Brink W. Sustained efficacy of dialectical behaviour therapy for borderline personality disorder. Behav Res Ther. 2005;43(9):1231–1241. doi:10.1016/j.brat.2004.09.008
31. Kramer U, Pascual-Leone A, Berthoud L, et al. Assertive anger mediates effects of dialectical behaviour-informed skills training for borderline personality disorder: a randomized controlled trial. Clin Psychol Psychother. 2016;23(3):189–202. doi:10.1002/cpp.1956
32. Soler J, Pascual JC, Tiana T, et al. Dialectical behaviour therapy skills training compared to standard group therapy in borderline personality disorder: a 3-month randomised controlled clinical trial. Behav Res Ther. 2009;47(5):353–358. doi:10.1016/j.brat.2009.01.013
33. McMain SF, Guimond T, Barnhart R, Habinski L, Streiner DL. A randomized trial of brief dialectical behaviour therapy skills training in suicidal patients suffering from borderline disorder. Acta Psychiatr Scand. 2017;135(2):138–148. doi:10.1111/acps.12664
34. Bohus M, Dyer AS, Priebe K, et al. Dialectical behaviour therapy for post-traumatic stress disorder after childhood sexual abuse in patients with and without borderline personality disorder: a randomised controlled trial. Psychother Psychosom. 2013;82(4):221–233. doi:10.1159/000348451
35. Harned MS, Korslund KE, Linehan MM. A pilot randomized controlled trial of dialectical behavior therapy with and without the dialectical behavior therapy prolonged exposure protocol for suicidal and self-injuring women with borderline personality disorder and PTSD. Behav Res Ther. 2014;55:7–17. doi:10.1016/j.brat.2014.01.008
36. McCauley E, Berk MS, Asarnow JR, et al. Efficacy of dialectical behavior therapy for adolescents at high risk for suicide: a randomized clinical trial. JAMA Psychiatry. 2018;75(8):777–785. doi:10.1001/jamapsychiatry.2018.1109
37. Mehlum L, Tørmoen AJ, Ramberg M, et al. Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: a randomized trial. J Am Acad Child Adolesc Psychiatry. 2014;53(10):1082–1091. doi:10.1016/j.jaac.2014.07.003
38. Sinnaeve R, van den Bosch LMC, Hakkaart-van Roijen L, Vansteelandt K. Effectiveness of step-down versus outpatient dialectical behaviour therapy for patients with severe levels of borderline personality disorder: a pragmatic randomized controlled trial. Borderline Personal Disord Emot Dysregulation. 2018;5:12. doi:10.1186/s40479-018-0089-5
39. Stoffers-Winterling JM, Storebø OJ, Kongerslev MT, et al. Psychotherapies for borderline personality disorder: a focused systematic review and meta-analysis. Br J Psychiatry. 2022;221:1–15.
40. Linehan MM, Korslund KE, Harned MS, et al. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: a randomized clinical trial and component analysis. JAMA Psychiatry. 2015;72(5):475–482. doi:10.1001/jamapsychiatry.2014.3039
41. Bohus M, Kleindienst N, Hahn C, et al. Dialectical Behavior Therapy for Posttraumatic Stress Disorder (DBT-PTSD) compared with Cognitive Processing Therapy (CPT) in complex presentations of PTSD in women survivors of childhood abuse: a randomized clinical trial. JAMA Psychiatry. 2020;77(12):1235–1245. doi:10.1001/jamapsychiatry.2020.2148
42. Fruzzetti A. The Family Guide to Borderline Personality Disorder.; Finding Peace in Your Family Using Dialectical Behavior Therapy. New Harbinger Publications; 2012.
43. Flynn D, Kells M, Joyce M, et al. Standard 12 month dialectical behaviour therapy for adults with borderline personality disorder in a public community mental health setting. Borderline Personal Disord Emot Dysregulation. 2017;4:19. doi:10.1186/s40479-017-0070-8
44. Liljedahl SI, Kleindienst N, Wångby-Lundh M, et al. Family connections in different settings and intensities for underserved and geographically isolated families: a non-randomised comparison study. Borderline Personal Disord Emot Dysregulation. 2019;6:14. doi:10.1186/s40479-019-0111-6
45. Guillén V, Fonseca-Baeza S, de Felipe IF, et al. Effectiveness of family connections intervention for family members of persons with personality disorders in two different formats: online vs face-to-face. In: Elsevier. 2022:100532.
46. Bateman A, Fonagy P. Effectiveness of partial hospitalization in the treatment of borderline personality disorder: a randomized controlled trial. Am J Psychiatry. 1999;156(10):1563–1569. doi:10.1176/ajp.156.10.1563
47. Bateman A, Fonagy P. Randomized controlled trial of outpatient mentalization-based treatment versus structured clinical management for borderline personality disorder. Am J Psychiatry. 2009;166(12):1355–1364. doi:10.1176/appi.ajp.2009.09040539
48. Jørgensen CR, Freund C, Bøye R, Jordet H, Andersen D, Kjølbye M. Outcome of mentalization-based and supportive psychotherapy in patients with borderline personality disorder: a randomized trial. Acta Psychiatr Scand. 2013;127(4):305–317. doi:10.1111/j.1600-0447.2012.01923.x
49. Laurenssen EM, Luyten P, Kikkert MJ, et al. Day hospital mentalization-based treatment v. specialist treatment as usual in patients with borderline personality disorder: randomized controlled trial. Psychol Med. 2018;48(15):2522–2529. doi:10.1017/S0033291718000132
50. Philips B, Wennberg P, Konradsson P, Franck J. Mentalization-based treatment for concurrent borderline personality disorder and substance use disorder: a randomized controlled feasibility study. Eur Addict Res. 2018;24(1):1–8. doi:10.1159/000485564
51. Robinson P, Hellier J, Barrett B, et al. The NOURISHED randomised controlled trial comparing mentalisation-based treatment for eating disorders (MBT-ED) with specialist supportive clinical management (SSCM-ED) for patients with eating disorders and symptoms of borderline personality disorder. Trials. 2016;17(1):549. doi:10.1186/s13063-016-1606-8
52. Rossouw TI, Fonagy P. Mentalization-based treatment for self-harm in adolescents: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. 2012;51(12):1304–1313.e1303. doi:10.1016/j.jaac.2012.09.018
53. Beck E, Bo S, Jørgensen MS, et al. Mentalization-based treatment in groups for adolescents with borderline personality disorder: a randomized controlled trial. J Child Psychol Psychiatry. 2020;61(5):594–604. doi:10.1111/jcpp.13152
54. Griffiths H, Duffy F, Duffy L, et al. Efficacy of mentalization-based group therapy for adolescents: the results of a pilot randomised controlled trial. BMC Psychiatry. 2019;19(1):167. doi:10.1186/s12888-019-2158-8
55. Smits ML, Feenstra DJ, Bales DL, et al. Day hospital versus intensive outpatient mentalization-based treatment: 3-year follow-up of patients treated for borderline personality disorder in a multicentre randomized clinical trial - ERRATUM. Psychol Med;2020. 1–4. doi:10.1017/S0033291720004018
56. Bateman A, Campbell C, Luyten P, Fonagy P. A mentalization-based approach to common factors in the treatment of borderline personality disorder. Curr Opin Psychol. 2018;21:44–49. doi:10.1016/j.copsyc.2017.09.005
57. Smits ML, Feenstra DJ, Bales DL, et al. Day hospital versus intensive outpatient mentalization-based treatment: 3-year follow-up of patients treated for borderline personality disorder in a multicentre randomized clinical trial. Psychol Med. 2022;52(3):485–495. doi:10.1017/S0033291720002123
58. Jørgensen MS, Storebø OJ, Stoffers-Winterling JM, Faltinsen E, Todorovac A, Simonsen E. Psychological therapies for adolescents with borderline personality disorder (BPD) or BPD features - a systematic review of randomized clinical trials with meta-analysis and trial sequential analysis. PLoS One. 2021;16(1):e0245331. doi:10.1371/journal.pone.0245331
59. Bateman A, Fonagy P. A randomized controlled trial of a mentalization-based intervention (MBT-FACTS) for families of people with borderline personality disorder. Personal Disord. 2019;10(1):70. doi:10.1037/per0000298
60. Derogatis LR, Savitz KL. The SCL-90-R, Brief Symptom Inventory, and Matching Clinical Rating Scales. Lawrence Erlbaum Associates Publishers; 1999.
61. Barnicot K, Crawford M. Dialectical behaviour therapy v. mentalisation-based therapy for borderline personality disorder. Psychol Med. 2019;49(12):2060–2068. doi:10.1017/S0033291718002878
62. Barnicot K, Redknap C, Coath F, Hommel J, Couldrey L, Crawford M. Patient experiences of therapy for borderline personality disorder: commonalities and differences between dialectical behaviour therapy and mentalization-based therapy and relation to outcomes. Psychol Psychother. 2022;95(1):212–233. doi:10.1111/papt.12362
63. Swenson CR, Choi-Kain LW. Mentalization and dialectical behavior therapy. Am J Psychother. 2015;69(2):199–217. doi:10.1176/appi.psychotherapy.2015.69.2.199
64. Edel M-A, Raaff V, Dimaggio G, Buchheim A, Brüne M. Exploring the effectiveness of combined mentalization-based group therapy and dialectical behaviour therapy for inpatients with borderline personality disorder - A pilot study. Br J Clin Psychol. 2017;56(1):1–15. doi:10.1111/bjc.12123
65. Gunderson J, Masland S, Choi-Kain L. Good psychiatric management: a review. Curr Opin Psychol. 2018;21:127–131. doi:10.1016/j.copsyc.2017.12.006
66. Bohus M, Stoffers-Winterling J, Sharp C, Krause-Utz A, Schmahl C, Lieb K. Borderline personality disorder. Lancet. 2021;398(10310):1528–1540. doi:10.1016/S0140-6736(21)00476-1
67. Hutsebaut J, Willemsen E, Bachrach N, Van R. Improving access to and effectiveness of mental health care for personality disorders: the guideline-informed treatment for personality disorders (GIT-PD) initiative in the Netherlands. Borderline Personal Disord Emot Dysregulation. 2020;7(1):1–7. doi:10.1186/s40479-020-00133-7
68. Paris J. Stepped care: an alternative to routine extended treatment for patients with borderline personality disorder. Psychiatr Serv. 2013;64(10):1035–1037. doi:10.1176/appi.ps.201200451
69. Mulder RT. ICD-11 personality disorders: utility and implications of the new model. Front Psychiatry. 2021;12:655548. doi:10.3389/fpsyt.2021.655548
70. Storebø OJ, Ribeiro JP, Kongerslev MT, et al. Individual participant data systematic reviews with meta-analyses of psychotherapies for borderline personality disorder: a protocol. BMJ Open. 2021;11:e047416. doi:10.1136/bmjopen-2020-047416
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.