Back to Journals » Local and Regional Anesthesia » Volume 15
Peripheral Nerve Blockade for Medial Patellofemoral Ligament Reconstruction in Pediatric Patients: The Addition of a Proximal Single-Injection Sciatic Nerve Block Provides Improved Analgesia
Authors Halpern L ![]() , Kogan CJ, Arnzen G
, Kogan CJ, Arnzen G
Received 8 February 2022
Accepted for publication 10 June 2022
Published 27 June 2022 Volume 2022:15 Pages 31—43
DOI https://doi.org/10.2147/LRA.S360738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Stefan Wirz
Lloyd Halpern,1 Clark J Kogan,2 Grady Arnzen3
1Department of Anesthesia, Shriners Children’s Hospital, Spokane, WA, USA; 2Department of Interdisciplinary Statistical Education and Research, Washington State University, Spokane, WA, USA; 3Creighton University School of Medicine, Omaha, NE, USA
Correspondence: Lloyd Halpern, Department of Anesthesia, Shriners Children’s Hospital, 911 W. 5th Ave, Spokane, WA, 99204, USA, Email [email protected]
Purpose: We tested the hypothesis that the addition of a single-injection proximal sciatic nerve block to an adductor canal block would significantly reduce pain scores and opioid requirements compared to a group of patients that received only an adductor canal or femoral nerve block for medial patellofemoral ligament reconstruction in pediatric patients. The primary end-point is the number of patients achieving a Patient Acceptable Symptom State (PASS) (pain score less than four) for the entire 24-hour postoperative period in patients with and without a proximal sciatic block.
Patients and Methods: This is a retrospective cohort study of 144 consecutive pediatric patients, ages 10 to 18 years, undergoing medial patellofemoral ligament reconstruction with peripheral nerve blockade for postoperative analgesia from 2016– 2020 at a pediatric orthopedics children’s hospital. Patients were divided into 2 cohorts with and without a proximal sciatic nerve block: group A/F: adductor canal or femoral CPNB and group AS: adductor canal CPNB and a proximal single-injection sciatic nerve block.
Results: There was strong evidence for an increase in the number of patients who reported a pain score less than four for the entire 24-hour postoperative period in the group that received the additional proximal sciatic block. (PASS: A/F 13/62 (21%) vs AS 43/82 (52%), p< 0.001) There was strong evidence for a reduction in mean and maximum pain scores and opioid requirements in the first 24-hours after surgery in the proximal sciatic group.
Conclusion: The addition of a proximal sciatic nerve block was associated with significantly reduced mean and maximum pain scores and opioid requirements after medial patellofemoral ligament reconstruction in pediatric patients and supports a randomized clinical trial to confirm these findings. Based on the results of this study we recommend the addition of a proximal sciatic nerve block, anterior or posterior, to an adductor canal block to provide improved analgesia and reduced opioid requirements in the 24-hours after MPFLR in pediatric patients.
Keywords: adductor canal block, femoral nerve block, medial patellofemoral ligament reconstruction, sciatic nerve block, opioids
Introduction
Medial patellofemoral ligament reconstruction (MPFLR) is a surgical procedure to treat recurrent patellar dislocation secondary to chronic patellar instability. Chronic patellar instability occurs most often in female adolescents with joint hyperlaxity with a reported incidence of 43 per 100,000 per year in the 10–17 year age group.1 The surgery is painful and requires three to six months of physical therapy and rehabilitation. It is important to control postoperative pain early to prevent loss of quadriceps strength and preserve joint range of motion.2 MPFLR is a relatively new procedure, first described in 2004, and we are unaware of another institution evaluating peripheral nerve blockade for MPFLR.3
Prior studies evaluating peripheral nerve blockade for procedures involving the knee have shown inconsistent results. A recent meta-analysis concluded that the adductor canal and femoral nerve blocks are equivalent to placebo for anterior cruciate ligament reconstruction.4,5 The single-injection adductor canal block offers short-term improvement in pain relief and analgesic requirements following total knee arthroplasty.6 Additional blocks have been added to the adductor canal and femoral nerve blocks to improve analgesia for procedures involving the knee. The addition of an injection between the popliteal artery and capsule of the knee (ipack block) to the adductor canal block decreases opioid requirements after total knee arthroplasty.7 The addition of a proximal sciatic nerve block to a femoral nerve block decreases opioid requirements and pain scores in adults having total knee arthroplasty and anterior cruciate ligament reconstruction.8–10 Because anterior cruciate ligament reconstruction and total knee arthroplasty primarily affect the posterolateral compartment of the knee and MPFLR focuses on the superomedial compartment of the knee,11 which block or combination of blocks is indicated for MPFLR is unclear.
In this study we compared pain scores and opioid usage in pediatric patients undergoing MPFLR with peripheral nerve blockade for postoperative pain control. The primary aim of the study is to test the hypothesis that the addition of a proximal single-injection sciatic nerve block to an adductor canal block will be associated with significantly reduced pain scores and opioid requirements compared to a group of patients that received only an adductor canal or femoral nerve block for MPFLR.
Materials and Methods
In this single-center, retrospective cohort study we reviewed 144 consecutive patients, ages 10 to 18 years, ASA 1–2, undergoing MPFLR at our institution from 2016 to 2020. Approval was obtained for all parts of the study by the Utilization Review Department of the Shriners Hospital for Children, a pediatric orthopedics hospital. In accordance with the principles stated in the Declaration of Helsinki, the ethics committee of the Utilization Review Department of the Shriners Hospital determined informed consent was not required to review patients’ medical records for this study because patient data confidentiality was ensured in accordance with national and international guidelines. In 2016 our practice was to provide an ultrasound-guided femoral continuous peripheral nerve block (CPNB) for postoperative pain control for all patients undergoing MPFLR. In 2017 we replaced the femoral nerve block with the adductor canal CPNB to provide improved quadriceps strength and the ability to ambulate with crutches postoperatively more efficiently. In a Quality Improvement project in September 2018 (unpublished) we reviewed our experience with the adductor canal and femoral nerve blocks and found no differences in opioid usage or pain scores in the two groups. However, only 20% of patients in the adductor canal and femoral groups were consistently reporting pain scores less than four in the first 24 hours after surgery despite access to opioids and a multimodal analgesic regimen. In October 2018, in an attempt to improve analgesia, we added a proximal single-injection sciatic nerve block, anterior or posterior, to the adductor canal CPNB for all patients undergoing MPFLR. In 2019 we published preliminary data comparing pain scores and opioid usage in 48 patients undergoing MPFLR with an adductor canal block or combined adductor canal and proximal posterior sciatic block.12 These 48 patients appear in this study to compare the results of all peripheral nerve blocks and to illustrate our progression in the use of peripheral nerve blockade for MPFLR.
Patients were grouped into two cohorts based on the presence of the proximal sciatic block: group A/F; adductor canal or femoral CPNB and group AS; combined adductor canal CPNB and proximal single-injection sciatic nerve block. The primary outcome is the number of patients achieving a patient acceptable symptom state (PASS) (pain scores less than four) for the entire 24-hour period. The proportion of patients reaching a patient acceptable pain state is an additional measure of postoperative pain control.13 We defined PASS as a pain score less than four because patients received opioids for a pain score of four or greater. Secondary outcomes were mean and maximum pain scores and opioid usage on the day of surgery and postoperative day one. Maximum and mean pain scores (visual analogue scale 0–10) were extracted from the electronic medical record for the day of surgery and postoperative day one for all patients. Pain scores and opioid requirements were available for all patients for at least 24-hours after surgery and were compared up to this time. The frequency of pain score assessment was variable for each patient but a minimum of every four hours. The mean pain score for the day of surgery and postoperative day one was determined by summing the pain scores and dividing by the number of observations. The number of patients reporting no pain for the 24-hour period was recorded.
Postoperative opioid consumption on the day of surgery and up to 24-hours after surgery, including the post-anesthesia care unit, was converted into oral morphine equianalgesic equivalent doses using standardized opioid conversion tables and presented as milligram dose per weight in kilograms.14 The number of patients not requiring opioids in the first 24-hours after surgery was determined. All initial opioids administered postoperatively were oxycodone (0.1 mg kg−1) prescribed every three hours for a pain score of four or greater. Patients who did not tolerate oxycodone were prescribed hydrocodone or hydromorphone.
The protocol for the general anesthetic regimen administered intraoperatively consisted of propofol, sevoflurane, ketorolac, acetaminophen, dexamethasone, ondansetron and a laryngeal mask airway or endotracheal tube if indicated. Intraoperative analgesics were morphine or fentanyl. Dosing was at the discretion of the attending anesthesiologist.
Patients with neuromuscular disease or a neurologic deficit in the involved leg were excluded. Medical records were reviewed for patient demographics including age, gender, weight and body mass index. (BMI) Surgical data were reviewed for surgeon, anesthesiologist placing the block, procedure type, block type, time required for the sciatic block and the incidence of the Fulkerson osteotomy, a procedure sometimes required as part of a MPFLR. No assessment of sensory block, motor block or time the block wore off was recorded.
All surgical procedures were performed by one of three attending pediatric orthopedic surgeons. One of five pediatric anesthesiologists performed all peripheral nerve blockade. All anesthesiologists had at least ten years of experience in pediatric regional anesthesia. All peripheral nerve blocks were performed under general anesthesia with ultrasound guidance. (Logiq E, General Electric, Boston, MA) All sciatic nerve blocks were done with a 21-gauge, 80,100 or 150 mm SonoPlex II stimulating needle. (Pajunk, Geisingen, Germany) All adductor canal blocks were performed with an 18 gauge, 4 inch Contiplex Tuohy stimulating needle (B. Braun, Meisungen, Germany) The total local anesthetic dose was 2.0 mg kg−1 of 0.5% ropivicaine up to a total of 30 milliliters. With the addition of the proximal sciatic block, half of the volume was deposited at each block site. Patients in group F received 0.5% ropivicaine. For all other patients the local anesthetic included dexamethasone (2 mg) and dexmedetomidine (50 mcg) per 30 milliliters of 0.5% ropivicaine.15
All sciatic blocks were single-injection blocks using the curved linear array transducer. (GE C1-5-D, Boston, MA) The posterior (PS) or anterior (AS) approach to the sciatic nerve was chosen at the anesthesiologists’ discretion. Peripheral nerve stimulation (2 mA, 0.10 ms, 2 Hz) was used to confirm the position of the sciatic nerve in all cases (plantar flexion of the foot or contraction of the hamstring muscle group) given that visualization of the nerve and needle may be difficult because of the depth of the sciatic nerve in these views. Injection proceeded when the twitch was lost at less than 0.4 mA. The anterior approach was performed in the proximal third of the thigh. The sciatic nerve was visualized 2–4 centimeters medial and posterior to the femur, inferior to the adductor magnus muscle and adductor fascia. (Figure 1A) The needle was advanced out of plane, taking care to avoid the superficial femoral artery. If peripheral nerve stimulation failed, needle position below the adductor fascia was visualized and injection proceeded. (Figure 1B) The posterior approach was done in the lateral position between the ischium and greater trochanter with injection inferior to the subgluteal fascia. Because the anterior sciatic block was a new block for all anesthesiologists, we searched for a potential learning effect by comparing the progression of pain scores as the number of anterior sciatic blocks increased for each anesthesiologist.
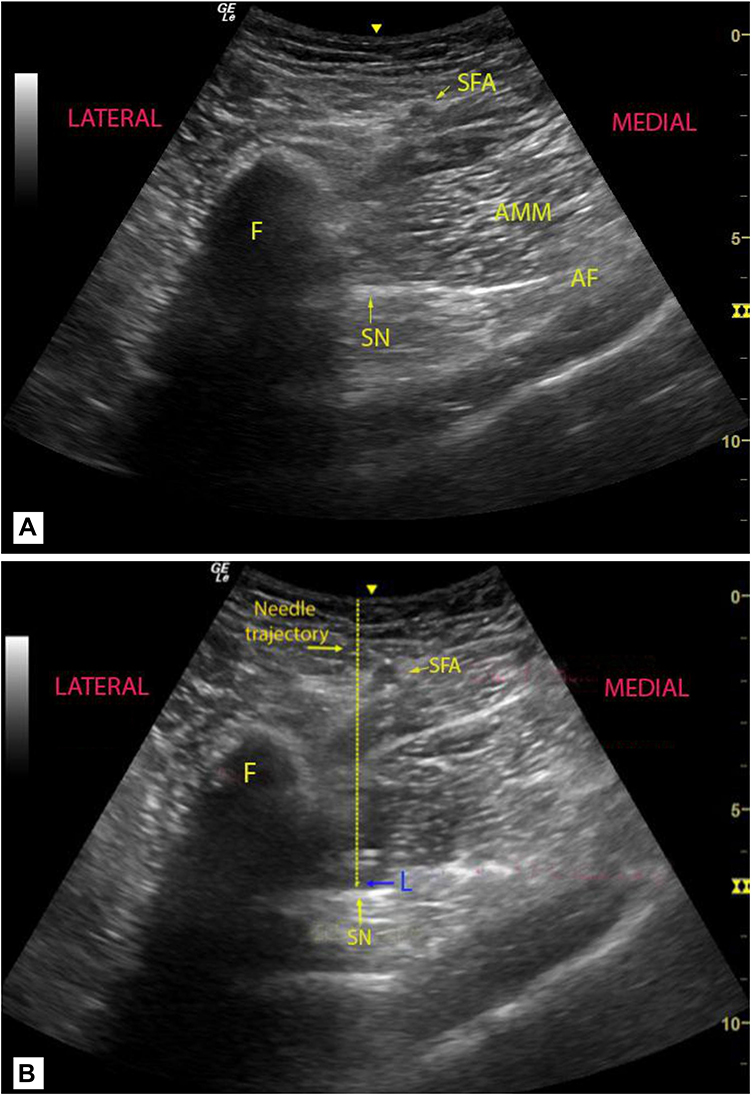 |
Figure 1 Ultrasound visualization of the proximal anterior sciatic block. (A) The ultrasound image obtained before needle placement. The curved array transducer is placed in the proximal third of the thigh medial to the femur at the level of the proximal adductor canal block. The sciatic nerve (SN) is well visualized 2–3 cm medial to the femur (F) and inferior to the adductor fascia (AF). Note the superficial femoral artery (SFA) which must be visualized prior to needle advancement. (AMM, adductor magnus muscle). (B) The ultrasound image immediately after local anesthetic injection. Note the local anesthetic (L) inferior to the adductor fascia. The needled trajectory is demonstrated. (Hashed line) The sciatic nerve (SN) is visualized within the local anesthetic and has moved inferiorly from the adductor fascia. |
All femoral and adductor canal blocks were continuous peripheral nerve blocks performed using the high-frequency linear array ultrasound transducer. (GE L4-12-T) The femoral nerve block was performed at the level of the inguinal ligament. The adductor canal block was performed by positioning the femoral artery medial to the sartorius muscle on the ultrasound scan, near the apex of the femoral triangle.16 Initial local anesthetic injections were given through the needle. Adductor canal and femoral nerve block catheters were advanced one to three centimeters beyond the needle and secured. Three milliliters were reserved to confirm catheter placement by ultrasound visualization of the local anesthetic injection. All femoral and adductor canal CPNBs had a continuous infusion initiated in the post anesthesia care unit with 0.2% ropivicaine at a rate of 0.1 cc kg−1 hr−1 (max rate 8 cc hr−1) for 48 to 72 hours and were removed by the patient after discharge to home. (Ambu Action Fuser Pump, Ambu Inc., Columbia, Maryland).
All patients were ambulated on the day of surgery. Patients were not discharged to home until they had been evaluated by a physical therapist and demonstrated adequate mobility with crutches. Patients were maintained in a knee brace in locked extension during weight bearing for the first two weeks after surgery.
Statistics
To examine the differences in maximum pain, mean pain, and opioid usage between groups, ordinal logistic regression models were employed with adjustment for the Fulkerson osteotomy, surgeon, age, gender, block type, body mass index (BMI), and anesthesiologist by adding these as explanatory variables to the model. All effects were included as fixed, including surgeon and anesthesiologist. Pairwise comparisons were made between groups with a Tukey adjustment for multiple comparisons. The Wilcoxon Rank Sum Test was used to compare length of stay between groups. Estimated differences and confidence intervals in mean difference in outcomes between groups were obtained with linear regression models, whereas p values were obtained with an ordinal logistic regression model with the same adjustment variables. (age, gender, block type, surgeon, anesthesiologist, BMI, Fulkerson osteotomy).
Chi squared tests were used for the binary outcomes of pain in the first 24-hours (yes/no), opioid use in the first 24-hours (yes/no) and comparisons of patient acceptable symptom state. We were unable to adjust for confounders for these outcomes because of the large number of variables given the number of patients in each group.17 However, we found no evidence that these confounders differed between groups. Pairwise comparisons were made between groups with a Bonferroni-Holm adjustment for multiple comparisons.
Results
Of the 147 patients reviewed, three patients went home on the day of surgery and were removed from the study. Of the remaining 144 patients, group A/F (n=62) received an adductor canal or femoral nerve CPNB and group AS (n=82) received an adductor canal CPNB and a proximal sciatic block. A comparison of the demographic data and distribution of block type are presented in Table 1. Both groups showed similar age, weight and BMI distributions, with the exception of BMI for the AS group, which had somewhat less variability than the other group. We found no significant differences in the distribution of the surgeon or anesthesiologist. Fifty-two percent of patients (75/144) had a Fulkerson osteotomy as part of their MPFLR. The Fulkerson osteotomy occurred with greater probability in group A/S (Table 1). Despite the increased use of the Fulkerson osteotomy in the proximal sciatic group, we found decreased pain scores and opioid usage in this group. (Table 2) In addition, we found no evidence of an effect of the Fulkerson osteotomy on pain scores or opioid usage while the blocks were in place in the regression analysis.
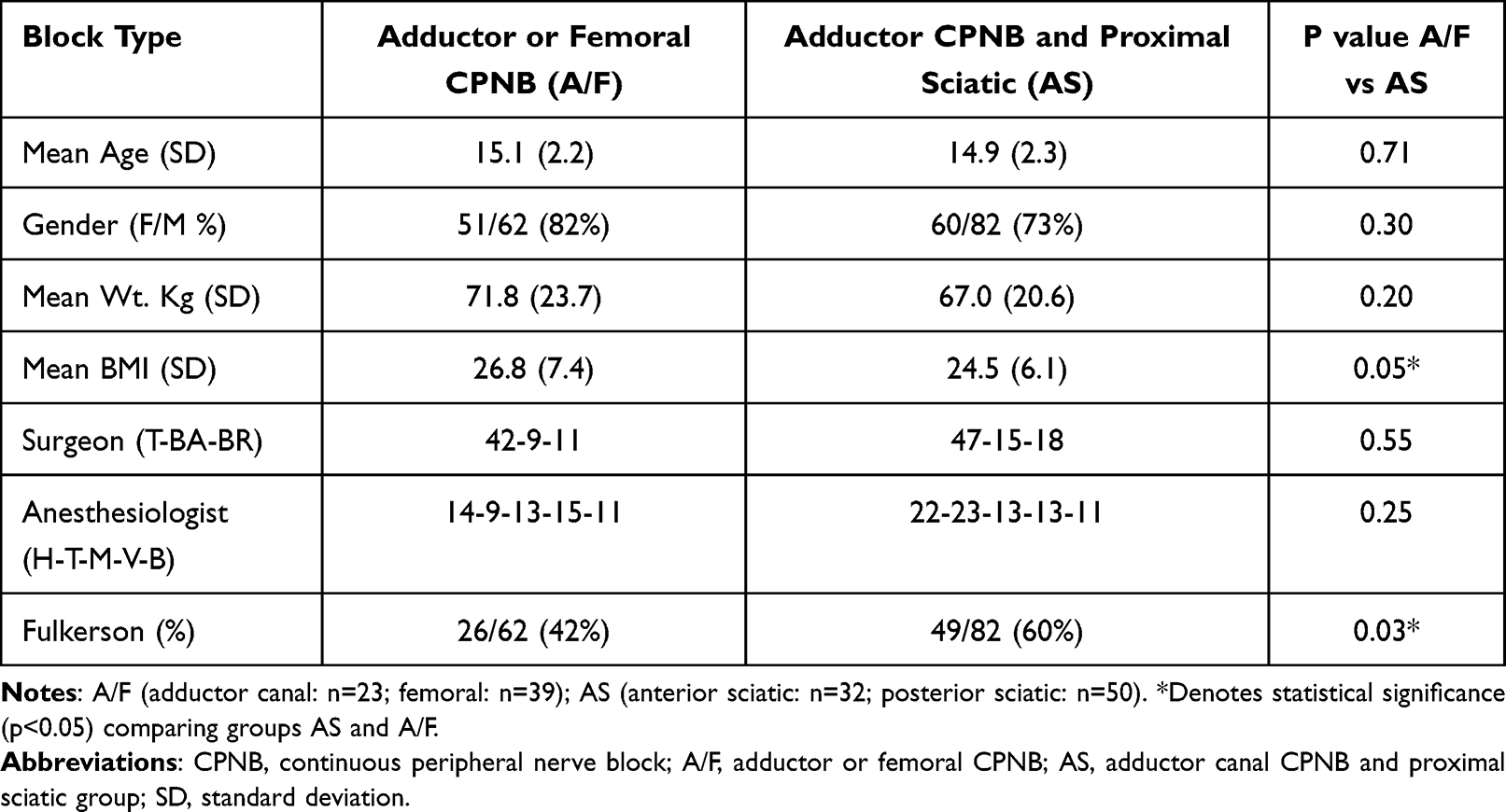 |
Table 1 Demographic and Surgical Data with (AS) and Without (A/F) the Proximal Sciatic Nerve Block |
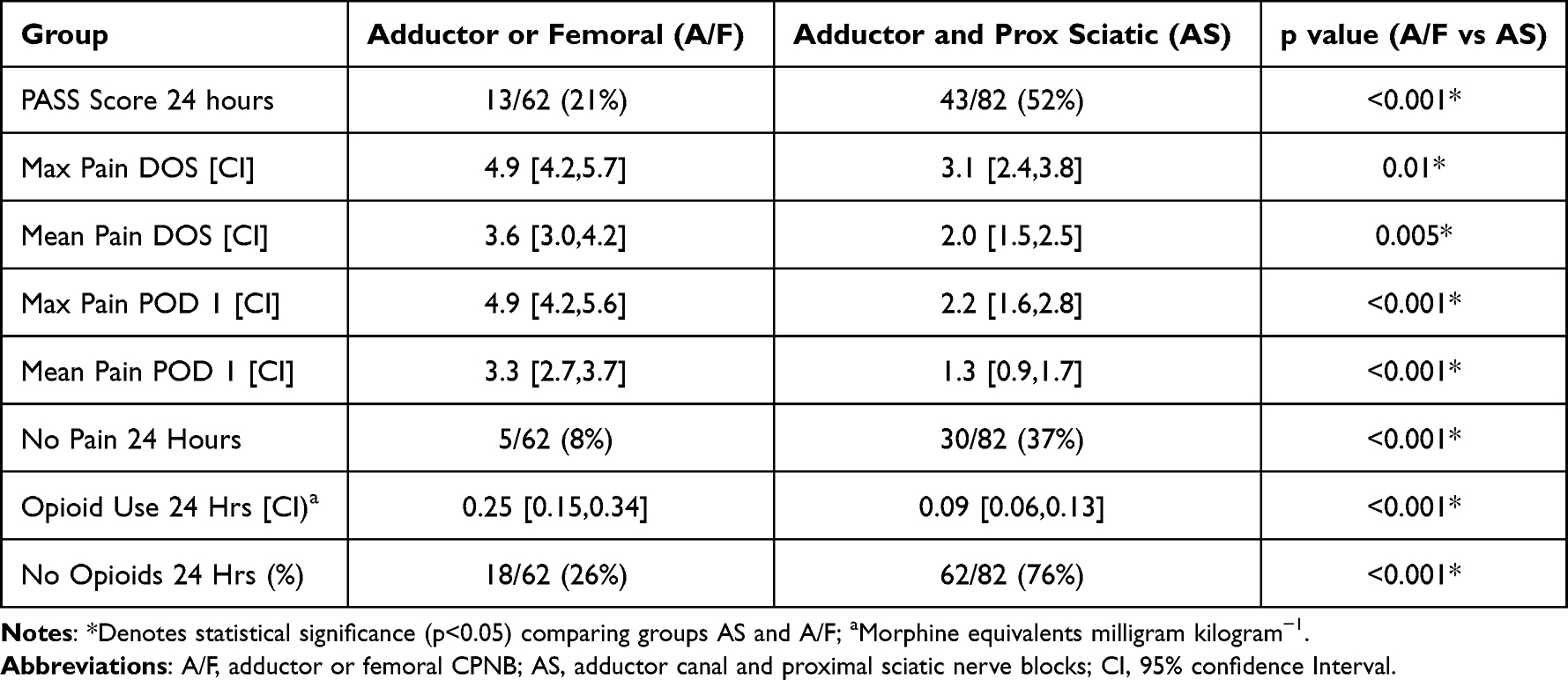 |
Table 2 Visual Analog Scale Pain Scores (0–10) and Opioid Usage with and without the Proximal Sciatic Nerve Block |
For the primary outcome, the percentage of patients achieving a patient acceptable symptom state (PASS) (pain score less than four) for the entire 24-hour period was significantly increased in the group receiving the combination proximal sciatic block and adductor canal CPNB when compared to the group receiving the femoral or adductor canal CPNB. (PASS: A/F 13/62 (21%) vs AS (43/82) (52%), p<0.001) (Table 2) There was a significant reduction in the reported maximum pain scores on the day of surgery and postoperative day one in the group with the additional sciatic block. (Max DOS: A/F 4.9 [95% CI 4.2,5.7] vs AS 3.1[95% CI 2.4,3.8], p=0.01) (Max POD 1: A/F 5.0 [95% CI: 3.6,6.3) vs A/AS 2.2 (95% CI: 1.6,2.8), p<0.001) (Table 2) There was evidence for a statistically significant reduction in mean pain scores in the proximal sciatic group on the day of surgery. (Mean DOS: A/F 3.6 [95% CI: 3.0,4.2] vs AS 2.0 [95% CI: 1.5,2.5], p= 0.005) (Table 2) There was a more pronounced reduction in mean pain scores on postoperative day one in the proximal sciatic group. (Mean POD 1: A/F 3.6 [95% CI: 3.0,4.2] vs AS 1.3 [95% CI: 0.9,1.7], p< 0.001) (Table 2) Patients who received the sciatic block were significantly more likely to report no pain for the entire 24-hour period when compared to Group A/F (No Pain 24-hours: A/F 5/62(8%) vs AS 30/82 (37%), p<0.001) (Table 2).
There was a significant reduction in opioid requirements (morphine equivalents mg kg−1) in the first 24-hours after surgery in group AS when compared to group A/F. (Opioids: A/F 0.25 [95% CI: 0.15,0.34) vs A/S 0.09 [95% CI: 0.06,0.13), p<0.001) (Table 2) There was a significant increase in the proportion of patients who did not require opioids in the first 24-hours after surgery associated with the sciatic block. (No opioids: A/F 18/62 (26%) vs AS 62/82 (76%), p<0.001) (Table 2) There was no evidence for differences in pain scores or opioid requirements at any time when comparing the adductor canal and femoral nerve groups or anterior and posterior sciatic groups (Table 3). Table 3 provides the effect size, p values and 95% confidence intervals for all pairwise comparisons for pain and opioid usage between groups. Table 4 provides the p values for all explanatory variables in the regression analysis. In addition to the block group, age showed a strong association with pain (maximum and mean) on the day of surgery, with younger patients indicating less pain. (Figure 2).
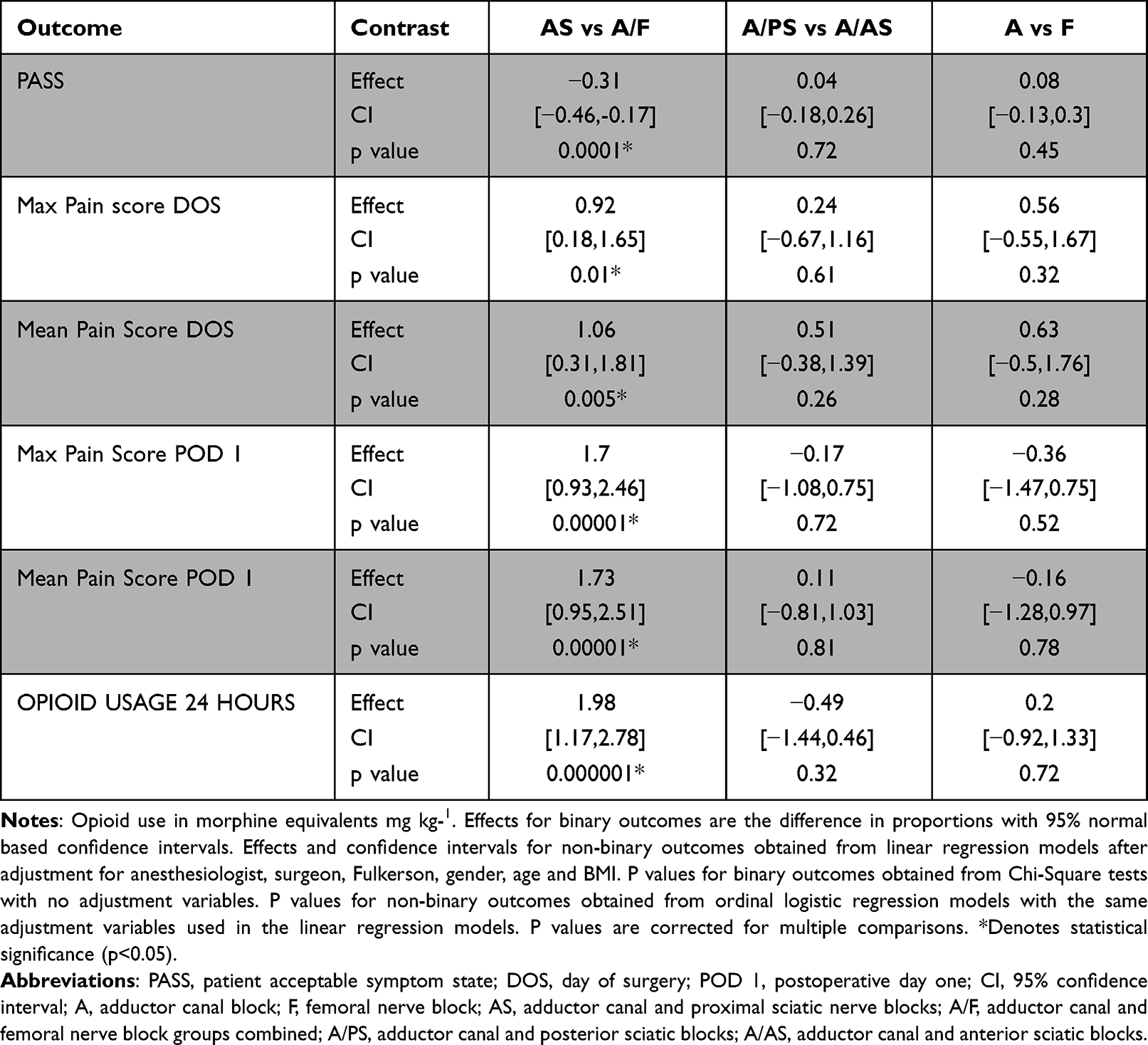 |
Table 3 P values for All Pairwise Comparisons for Pain and Opioid Usage Between All Groups |
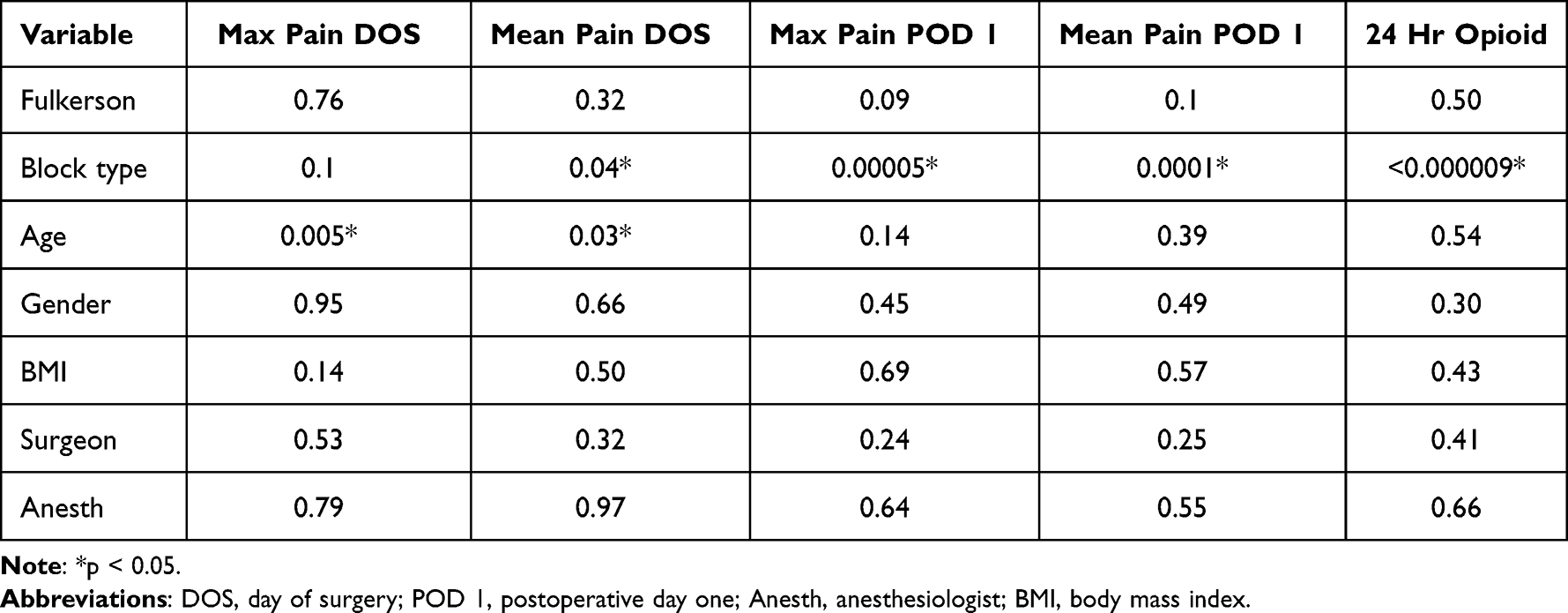 |
Table 4 Results of the Regression Analysis Comparing Pain and Opioid Usage with Associated p values |
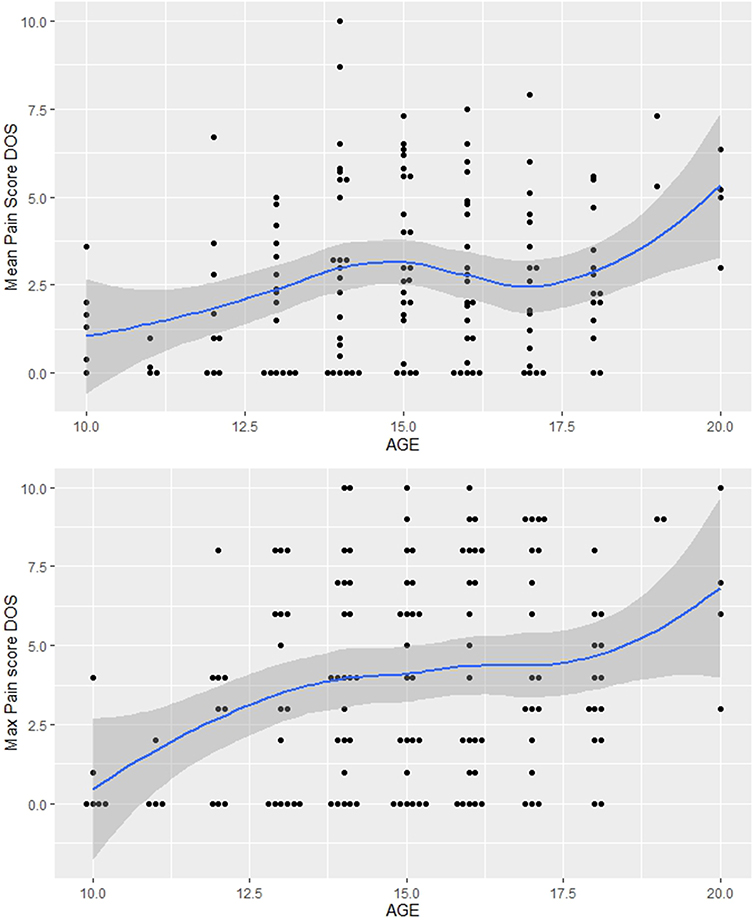 |
Figure 2 Relationship between age and pain on the day of surgery. Abbreviation: DOS, day of surgery. |
The mean times for the sciatic blocks were 9.7 (4.4) minutes for the anterior sciatic and 10.4 (4.8) minutes for the posterior sciatic. We were unable to demonstrate a change in the number of days length of stay in any group. (A/F 1.09 (0.29) vs AS 1.0 (0.45), p= 0.75) The effect sizes on pain scores and opioid usage associated with the addition of the Fulkerson osteotomy were not statistically significant. (Table 4) The progression of pain scores associated with the number of anterior sciatic blocks performed showed a consistent decrease in pain scores after five blocks had been previously performed. (Figure 3).
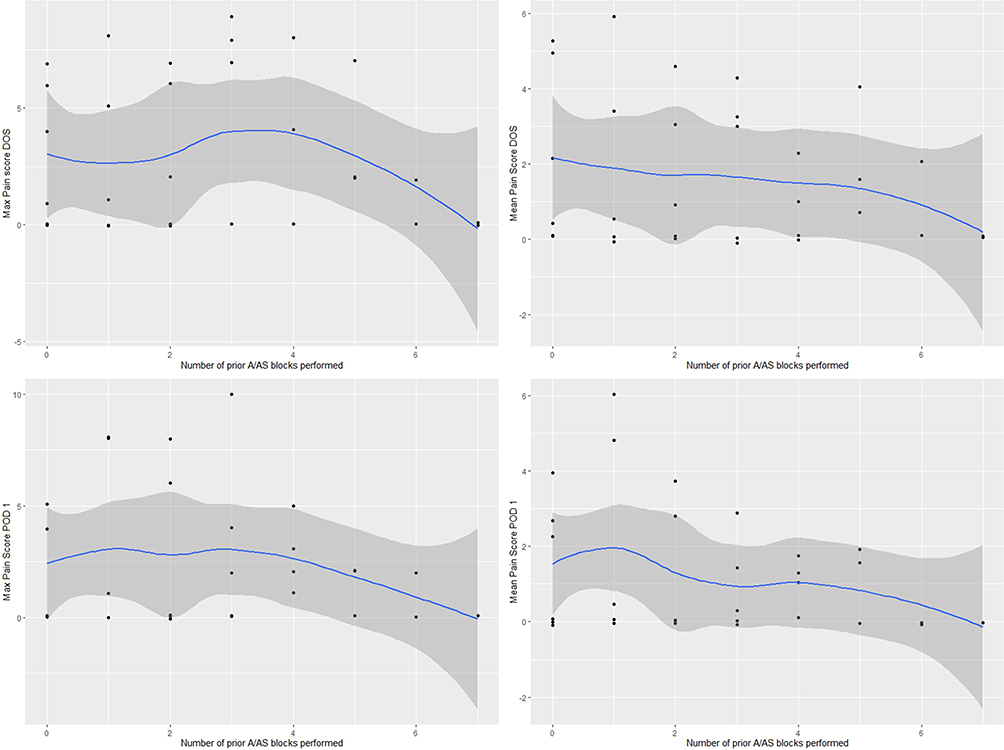 |
Figure 3 The progression of pain scores associated with the number of anterior sciatic blocks performed. Abbreviations: A/AS, anterior sciatic and adductor canal group; DOS, day of surgery; POD 1, postoperative day one. |
Two patients in the study group developed a nerve injury postoperatively. One patient in group AS developed a foot drop that persisted after the motor and sensory changes associated with the proximal anterior sciatic nerve block had resolved on postoperative day one. Nerve conduction studies six weeks postoperatively revealed an injury to the common peroneal nerve at a level below the knee. This patient had subsequent nerve decompression surgery with resolution of the foot drop. One patient in Group A/F presented three weeks after surgery at the first postoperative visit with continuous pain below the knee in the distribution of the saphenous nerve after his adductor canal CPNB. Nerve conduction studies demonstrated an entrapment of the saphenous nerve below the knee at six weeks postoperatively. This patient had ligation of the saphenous nerve below the knee with resolution of the pain. One patient in Group F fell at home while the block was still in place when his crutches slipped out from under him. He was not seriously injured.
Discussion
Other than the preliminary study by our group, this study is the first we are aware of to report the effects of peripheral nerve blockade for MPFLR and to describe the anterior approach to the sciatic nerve using ultrasound guidance in pediatric patients. We have transitioned to exclusively use the ultrasound-guided proximal anterior sciatic block because the anterior approach to the sciatic nerve allows one prep for both blocks, superior visualization of the sciatic nerve and does not require turning the patient on their side for the block. The primary finding of this study is that the femoral and adductor canal CPNB provided adequate analgesia (pain score less than four) for only 21% of our patients in the first 24-hours after MPFLR despite access to opioids and multimodal analgesia. Moreover, we found that patients who had the addition of a proximal sciatic block were more than twice as likely (52% vs 21%) to achieve a PASS (pain score less than four) for the entire 24-hours after surgery compared to the adductor canal and femoral nerve block group. Patients in the proximal sciatic group were nearly five times more likely to report no pain during the postoperative 24-hours. (37% vs 8%) Maximum and mean pain scores were significantly less for the 24-hour period with the addition of the sciatic block. These improvements in pain scores were observed despite the propensity for differences in pain scores to be attenuated by the use of opioids to control pain in both groups.
Along with improved analgesia, we found that patients who received the additional proximal sciatic block required 64% less opioids in the first 24-hours postoperatively. (0.25 vs 0.09 meq kg−1) Seventy-six percent of patients in the proximal sciatic group did not require opioids in the 24-hour period, three times more than the adductor and femoral group. In a time of widespread opioid dependence, and evidence that the legitimate use of opioids increases the risk of long-term addiction in adolescents, it is critical we find regional anesthetic techniques that can reduce opioid requirements.18
Controversy exists on how to best quantify the analgesic effect of regional anesthesia on acute postoperative pain. The amount of analgesics needed is an important indicator of improved analgesia. The minimal clinically important difference (MCID) attempts to determine the smallest change in pain scores that is perceived as beneficial to patients. However, the influence of a change in pain score depends on the absolute level of pain. Bodian et al reported that a change in pain score for patients experiencing pain in the four to seven range had the greatest clinical effect on the need for analgesics.19 The PASS score represents a satisfactory symptom state and is a good measure of the overall success of the intervention. We found the addition of the proximal sciatic block was associated with an average reduction of mean and maximum pain scores of 1 on the day of surgery and 1.7 on postoperative day one. This was in the range defined by Bodian as having the greatest clinical effect.
We found a reduction in pain scores in younger children on the day of surgery across both treatment groups. A Cochrane review of ultrasound guidance for peripheral nerve blockade in children previously reported that the younger the child the more likely they are to benefit from the use of ultrasound guidance.20 They speculated that this may be due to increased ultrasonic visibility of shallower structures in smaller children. Our results support these findings.
Cadaver studies of knee joint innervation have demonstrated wide variability in the 13 identified nerves innervating the knee.21,22 The superomedial compartment of the knee, the primary area requiring analgesia for MPFLR, is innervated by the nerve to the vastus medialis, the nerve to the vastus intermedius and the superior medial genicular nerve. The nerves to the vastus medialis and vastus intermedius originate from the femoral nerve. The superior medial genicular nerve may originate from either the femoral, obturator or sciatic.21 Those patients with innervation to the superomedial compartment originating primarily from the femoral nerve likely represent those with adequate analgesia with the adductor canal block or femoral nerve block. The remaining patients benefit from the addition of the sciatic block.
Twenty percent of patients in the sciatic group (16/82) had mild pain immediately after surgery that resolved by the evening of the day of surgery. (3% groups A/F (2/62); p=0.003) This may represent postoperative surgical or tourniquet pain in patients with innervation to the knee provided by the unblocked obturator nerve. It may also be a result of incomplete blockage of the sciatic nerve. In our experience, the ultrasound image of the sciatic nerve may not produce a well-defined view of the sciatic nerve or needle position in all cases.
Some surgeons are reluctant to include a proximal sciatic nerve block for knee surgery to avoid masking a common peroneal nerve injury and an increased risk of falls postoperatively. The common peroneal nerve is at risk in posterolateral procedures of the knee (total knee arthroplasty, anterior cruciate ligament reconstruction) but is not in close proximity to the surgical site during MPFLR.11 We did observe a common peroneal nerve injury in one patient in group AS. (anterior sciatic group) The sciatic block did not interfere in making the diagnosis in this patient after the block resolved because the injury was solely in the distribution of the common peroneal nerve ruling out an injury from a more proximal sciatic injection. The saphenous nerve injury did not become evident until several weeks postoperatively at the first postoperative visit. Nerve conduction studies for both of these patients were delayed until six weeks postoperatively because these injuries were felt to be secondary to compression of the nerve by the postoperative brace and would likely resolve in that time. We could find no report of a saphenous nerve injury due to an adductor canal block. A prospective study of 97 patients with an adductor canal block for total knee arthroplasty found no indications of injury to the medial crural branch of the saphenous nerve caused by the adductor canal block at the mid-thigh level. However, eighty-four percent of the patients had signs of injury to the infrapatellar branch of the saphenous nerve from the surgical procedure.23
We were unable to demonstrate a change in the length of stay with the addition of the proximal sciatic block. Since the completion of this study, our surgeons and patients now plan on patient discharge on the day of surgery. Nineteen of the twenty-five patients (76%) undergoing MPFLR since this study has ended have gone home on the day of surgery. This represents a significant change in our practice as a direct result of the addition of the proximal sciatic block.
We examined the progression of pain scores over time by comparing pain scores as the number of previously performed anterior sciatic blocks increased. Figure 3 is consistent with a learning effect that results in decreasing pain on the day of surgery and postoperative day one after five blocks. More data is needed to establish a learning effect and the dynamics of such an effect.
The Fulkerson osteotomy, relocating the attachment of the patellar tendon on the tibia, is performed in conjunction with MPFLR when the patellar attachment point is greater than 20 mm from the preferred point of attachment.24 Despite the Fulkerson osteotomy appearing with greater probability in the proximal sciatic group, we observed reduced pain scores and opioid requirements in the proximal sciatic group. We did not observe a clinically relevant effect size on pain scores or opioid usage with the addition of the Fulkerson osteotomy while the blocks were in place. The innervation of the tibial epiphysis originates within the trabecular bone and enters the knee joint via the intercondylar foramina where it joins nerves innervating the synovial membrane and meniscus, not adding any additional innervation to be addressed by the peripheral nerve block.25
We included the femoral nerve block cohort to provide previously unreported comparative data for the adductor canal and femoral nerve blocks for MPFLR and to illustrate our progression of peripheral nerve blockade over time. We chose to combine the adductor canal and femoral nerve block groups and the anterior and posterior sciatic groups because our primary aim was to determine the effect of adding a proximal sciatic block. We felt this was justified because numerous studies have established that the adductor canal block provides equivalent analgesia to the femoral nerve block for multiple different procedures involving the lower extremity.26–28 There is likewise no evidence that the anterior and posterior proximal sciatic nerve blocks produce any significant differences in analgesia in adults undergoing knee surgery.29,30 We did not find any significant differences in pain scores, opioid usage, PASS scores or any measured outcome in either the femoral or adductor CPNB groups or the anterior or posterior sciatic groups in the subgroup analysis. (Table 3)
Our methods selection may not be considered standard There are a limited number of definitive, evidence-based recommendations for the choice of local anesthetic, concentration and perineural adjuvants for peripheral nerve blockade in pediatric patients.31 We elected to use 0.5% ropivicaine because our youngest patient for this procedure is 10 years and the clearance of ropivicaine reaches its maximum at the age of five years.32 Dexmedetomidine was selected based on a previous meta-analysis confirming its safety as an adjunct for peripheral nerve blockade in children.33 The combination of dexamethasone and dexmedetomidine was based on previous studies suggesting improvement in analgesia duration in adults and children in peripheral nerve blockade and caudal analgesia.34,35
One limitation of this study is the absence of the perineural adjuvants dexamethasone and dexmedetomidine in the local anesthetic in the femoral nerve block group. We felt including the femoral group was justified because all femoral and adductor canal blocks were continuous nerve blocks, negating the effect of dexmedetomidine and dexamethasone in prolonging the adductor canal block in comparison to the femoral nerve block. Two recent reviews of dexamethasone as a perineural adjuvant concluded that there is a lack of consistent evidence for the superiority of perineural vs systemic dexamethasone, and no difference between the 4 mg and 8 mg dose.36,37 All patients received intravenous dexamethasone (4 or 8 mg) as part of their general anesthetic. Dexmedetomidine as a perineural adjuvant for surgery involving the knee has shown inconsistent results. Perineural dexmedetomidine has been shown to reduce pain scores and opioid usage after total knee arthroplasty.38 The only study evaluating dexmedetomidine as a perineural adjuvant in the adductor canal block for anterior cruciate ligament reconstruction found comparable pain scores and opioid usage in the first 24 hours after surgery and recommended against its use.39
This study has limitations inherent in a retrospective, non-randomized study design. There is a risk of bias as the pain management methods were compared without blinding or randomization. The different use of intraoperative opioids is an additional confounder. We made an effort to reduce the scope of potential confounders. The surgeons and anesthesiologists were similarly distributed between groups. The intra and postoperative anesthetic and analgesic protocols did not differ between groups. Significant differences after accounting for the addition of the Fulkerson osteotomy persisted between groups. We cannot discount the possibility that general improvements over time in both surgical and anesthetic technique may explain the differences in pain and opioid use outcomes. We lacked a control group that did not receive a block, making it impossible to make any conclusions on the effects of each block compared to a patient without regional anesthesia. This study was performed at a single-center, requiring a careful comparison with your own situation. There may have been other confounders between groups but the observed differences in pain scores and opioid usage were highly significant. Further studies with extended follow-up are required to determine how long these differences in opioid usage and pain scores persist beyond 24-hours.
Conclusion
We found that the use of an adductor canal and femoral continuous peripheral nerve block, multi-modal analgesia and opioid analgesics for MPFLR provided adequate analgesia (pain score less than four) for the entire 24-hours after surgery for only 21% of pediatric patients. The addition of a proximal sciatic nerve block was associated with significantly reduced mean and maximum pain scores and opioid requirements for 24-hours after surgery and supports a randomized clinical trial to confirm these findings. Based on the results of this study we recommend the addition of a proximal sciatic nerve block, anterior or posterior, to an adductor canal block to provide improved analgesia and reduced opioid requirements in the 24-hours after MPFLR in pediatric patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nietosvaara Y, Aalto K, Kallio PE. Acute patellar dislocation in children: incidence and associated osteochondral fractures. J Pediatr Orthop. 1994;14(4):513–515. doi:10.1097/01241398-199407000-00018
2. Fithian DC, Powers CM, Khan N. Rehabilitation of the knee after medial patellofemoral ligament reconstruction. Clin Sports Med. 2010;29(2):283–290. doi:10.1016/j.csm.2009.12.008
3. Teitge RA, Torga-Spak R. Medial Patellofemoral ligament reconstruction. Orthopedics. 2004;27(10):1037–1040. doi:10.3928/0147-7447-20041001-09
4. Sehmbi H, Brull R, Shah UJ, et al. Evidence basis for regional anesthesia in ambulatory arthroscopic knee surgery and anterior cruciate ligament reconstruction: part 2: adductor canal nerve block – a systematic review and meta-analysis. Anesth Analg. 2019;128(2):223–238. doi:10.1213/ANE.0000000000002570
5. Vorobeichik L, Brull R, Joshi GP, et al. Evidence basis for regional anesthesia in ambulatory anterior cruciate ligament reconstruction: part 1: femoral nerve block. Anesth. 2019;128(1):58–65.
6. Jiang X, Wang QG, Wu CI, et al. Analgesic efficacy of adductor canal block in total knee arthroplasty: a meta-analysis and systematic review. Orthop Surg. 2016;8(3):294–300. doi:10.1111/os.12268
7. Ochroch J, Qi V, Badiola I, et al. Analgesic efficacy of adding the IPACK block to a multimodal analgesia protocol for primary total knee arthroplasty. Reg Anesth Pain Med. 2020;45(10):799–804. doi:10.1136/rapm-2020-101558
8. Wegener JT, Ooji BV, Dijk NV, et al. Value of single injection or continuous sciatic nerve block in addition to a continuous femoral nerve block in patients undergoing total knee arthroplasty. Reg Anesth Pain Med. 2011;36(5):481–488. doi:10.1097/AAP.0b013e318228c33a
9. Harbell MW, Cohen JM, Kolodzie K, et al. Combined preoperative femoral and sciatic nerve blockade improves analgesia after anterior cruciate ligament reconstruction: a randomized controlled clinical trial. J Clin Anesth. 2016;33:68–74. doi:10.1016/j.jclinane.2016.02.021
10. Dang CP, Gautheron E, Guilley J, et al. The value of adding sciatic block to continuous femoral nerve block for analgesia after total knee arthroplasty. Reg Anesth Pain Med. 2005;30(2):128–133. doi:10.1097/00115550-200503000-00003
11. Jenkins MJ, Moussa F, Hwang P, et al. The distance of the common peroneal nerve to the posterlolateral structures of the knee. J Arth. 2016;31(12):2907–2911. doi:10.1016/j.arth.2016.05.005
12. Halpern LM, Kogan CJ, Michels PE. Regional anesthesia and the adolescent opioid epidemic. Med Clin Res. 2019;4(8):1–4.
13. Munoz-Levya F, El-Boghdadly K, Chan V. Is the minimal clinically important difference in acute pain a good measure of analgesic efficacy in regional anesthesia? Reg Anesth Pain Med. 2020;45(12):1000–1005. doi:10.1136/rapm-2020-101670
14. Canadian pharmacists association. Compendium of Pharmaceuticals and Specialties.
15. Lonquist PA. Adjuncts should always be used in pediatric regional anesthesia. Pediatr Anaesth. 2015;25:100–106. doi:10.1111/pan.12526
16. Abdallah FW, Mejia J, Prasad GA, et al. Opioid- and motor sparing Motor-sparing with proximal, midMid-, and distal locations for adductor canal block in anterior cruciate ligament reconstruction. Anesthesiology. 2019;131(3):619–629. doi:10.1097/ALN.0000000000002817
17. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
18. Miech R, Johnston L, O’Malley PM, et al. Prescription opioids in adolescence and future opioid misuse. Pediatrics. 2015;136:e1169–e1177. doi:10.1542/peds.2015-1364
19. Bodian CA, Freedman G, Hiossain S, et al. This visual analog scale for pain: clinical significance in postoperative patients. Anesthes. 2001;95(6):1356–1361. doi:10.1097/00000542-200112000-00013
20. Guay JG, Suresh S, Kopp S. The use of ultrasound guidance for perioperative neuraxial and peripheral nerve blocks in children: a cochrane review. Reg Anesth Pain Med. 2017;124(3):948–958.
21. Horner G, Dellon AL. Innervation of the human knee joint and implications for surgery. Clin Orthop Relat Res. 1994;301:221–226. doi:10.1097/00003086-199404000-00034
22. Roberts SL, Stout A, Dreyfuss P. Review of knee joint innervation: implications for diagnostic blocks and radiofrequency ablation. Pain Med. 2019. doi:10.1093/pm/ponz.189
23. Henningsen MH, Jaeger P, Hilsted KL, et al. Prevalence of saphenous nerve injury after adductor canal blockade in patients receiving total knee arthroplasty. Acta Anaesthesiol Scand. 2013;57(1):112–117. doi:10.1111/j.1399-6576.2012.02792.x
24. Fulkerson JP. Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop Relat Res. 1983;177:176–181. doi:10.1097/00003086-198307000-00027
25. Matsuo K, Ji S, Miya A, et al. Innervation of the tibial epiphysis through the intercondylar foramen. Bone. 2018;120:297–304. doi:10.1016/j.bone
26. Baile L, Griffin J, Elliott M, et al. Adductor canal nerve verses femoral nerve blockade for pain control and quadriceps function following anterior cruciate ligament reconstruction with patellar tendon autograft: a prospective randomized trial. Arthroscopy. 2019;35(3):921–929. doi:10.1016/j.arthro.2018.10.149
27. Lim YC, Quek HY, Phoo WH, et al. A randomized controlled trial comparing adductor canal block and femoral nerve block for knee arthroplasty. Singapore Med J. 2019;60(3):145–149. doi:10.11622/smedj.2018082
28. Xin J, Zhang Y, Li Q, et al. Adductor canal block is similar to femoral nerve block for the quality of rehabilitation after arthroscopic partial mes`iscectomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(7):2334–2342. doi:10.1007/s00167-019-05796-6
29. Ota J, Sakura S, Hara K, et al. Ultrasound guided anterior approach to the sciatic nerve block: a comparison with the posterior approach. Anesth Analg. 2009;108:660–665. doi:10.1213/ane.0b013e31818fc252
30. Alsatli R. Comparison of ultrasound-guided anterior versus transgluteal sciatic nerve blockade for knee surgery. Anesth Essays Res. 2012;6(1):29–33. doi:10.4103/0259-1162.103368
31. Suresh S, Ecoffey C, Bosenberg A, et al. The European Society of regional anesthesia and pain therapy/American Society of regional anesthesia and pain medicine recommendations on local anesthetics and adjuvant dosage in pediatric regional anesthesia. Reg Anesth Pain Med. 2018;43:211–216. doi:10.1097/AAP.0000000000000702
32. Mazoit J, Dalens B. Pharmacokinetics of local anesthetics in infants and children. Clin Pharmacokinet. 2004;43(1):17–32. doi:10.2165/00003088-200443010-00002
33. Lundblad M, Trifa M, Kaabachi O, et al. Alpha-2 adrenoreceptor agonists as adjuncts to peripheral nerve blocks in children: a meta-analysis. Paediatr Anaesth. 2016;26:232–238. doi:10.1111/pan.12825
34. Herman J, Urits I, Eskander J, et al. Adductor canal block duration of analgesia prolonged with perineural dexmedetomidine in addition to IPACK block for total knee arthroplasty. Cureus. 2020;12(9). doi:10.7759/cureus.10566
35. Hassan P, Hassan A, Elmetwally S. Caudal analgesia for hypospadias in pediatrics: comparative evaluation of adjuvants dexamethasone and dexmedetomidine combination vs dexamethasone or dexmedetomidine to bupivacaine: a prospective, double-blinded, randomized comparative study. Anesth Essays Res. 2018;12(3):644–650. doi:10.4103/aer.AER_77_18
36. Albrecht E, Kern C, Kirkham KR. A systematic review and meta-analysis of perineural dexamethasone for peripheral nerve blocks. Anaesthesia. 2017;70(1):71–83. doi:10.1111/anae.12823
37. Desai N, Kirkham K, Albrecht E. Local anesthetic adjuncts for peripheral regional anesthesia: a narrative review. Anaesthsia. 2021;76(1):100–109. doi:10.1111/anae.15245
38. Goyal R, Mittal G, Yadav AK, et al. Adductor canal block for post-operative analgesia after simultaneous bilateral total knee replacement: a randomized controlled trial to study the effect of addition of dexmedetomidine to ropivicaine. Indian J Anaesth. 2017;61(11):903–909. doi:10.4103/ija.IJA_277_17
39. Thapa D, Ahuja V, Pandey K, et al. Evaluation of anagesic efficacy of dexmedetomidine as adjuvant with ropivicaine ultrasound-guided adductor canal block in patients following anterior cruciate ligament reconstruction. Br J Pain. 2019;13(2):91–98. doi:10.1177/2049463718796865
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.