Back to Journals » International Medical Case Reports Journal » Volume 18
Peripheral IV Catheter-Associated Upper Extremity Deep Vein Thrombosis in a Patient with Psychiatric Illness: A Case Report and Literature Review
Authors Kwesiga T ![]() , Deifa AAA, Byaruhanga K, Ali MM, Abas SJ, Gindu L, Olive MM
, Deifa AAA, Byaruhanga K, Ali MM, Abas SJ, Gindu L, Olive MM ![]() , Ernest BM
, Ernest BM ![]() , Yusuf Snr AO, Roseline NM, Ronald M, Boniface Snr O, Kwandikwa AM, Kirabo NH
, Yusuf Snr AO, Roseline NM, Ronald M, Boniface Snr O, Kwandikwa AM, Kirabo NH ![]() , Duale II FA, Mswelo VE
, Duale II FA, Mswelo VE
Received 22 June 2025
Accepted for publication 15 November 2025
Published 25 November 2025 Volume 2025:18 Pages 1465—1472
DOI https://doi.org/10.2147/IMCRJ.S548815
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Thomas Kwesiga,1 Abdalla Ahmed Adam Deifa,1 Kusemererwa Byaruhanga,1 Mussa Makame Ali,1 Seif Juma Abas,1 Lucas Gindu,1 Mughanda Mugheni Olive,1 Badako Mogonza Ernest,1 Abdikadir Omar Yusuf Snr,1 Nsimire Mulanga Roseline,1 Musinguzi Ronald,2 Oscar Boniface Snr,3 Ayubu Mathias Kwandikwa,3 Nalumansi Hildah Kirabo,1 Fardowsa Abdikarim Duale II,1 Venance Emmanuel Mswelo1
1Department of Internal Medicine, Faculty of Clinical Medicine and Dentistry, School of Health sciences, Kampala International University, Kampala, Uganda; 2Department of Psychiatry, Faculty of Clinical Medicine and Dentistry, School of Health Sciences, Kampala International University, Kampala, Uganda; 3Department of Surgery, Faculty of Clinical Medicine and Dentistry, School of Health Sciences, Kampala International University, Kampala, Uganda
Correspondence: Thomas Kwesiga, Email [email protected]
Background: Upper‐extremity deep vein thrombosis (UEDVT) is relatively uncommon accounting for roughly 4– 10% of all deep vein thromboses but its incidence is rising, largely due to the widespread utilization of intravenous catheters. While central venous catheters are the typical culprits, peripheral IV cannulas are not benign and may provoke thrombosis via local endothelial trauma and venous stasis, especially in individuals with systemic prothrombotic predispositions.
Case Presentation: We report a 44-year-old man with bipolar affective disorder on haloperidol, promethazine, and carbamazepine. Five days after placement of a peripheral IV cannula in his right forearm, he developed gradually worsening pain and swelling from the mid-forearm extending into the upper arm. Duplex ultrasonography revealed occlusive thrombus in the antecubital vein, confirming catheter-associated UEDVT.
Intervention and Outcome: The patient was initially started on low molecular weight heparin, later transitioned to apixaban. His symptoms resolved within three weeks, and after three months of anticoagulation with normalization of D-dimer levels therapy was discontinued without recurrence.
Conclusion: Even peripheral IV cannulation may precipitate UEDVT when combined with local vein injury and systemic hypercoagulability. Antipsychotics, such as haloperidol and chlorpromazine, may further elevate thrombosis risk. Clinicians must maintain vigilance for UEDVT in patients with unilateral arm swelling post-cannulation, recognizing that prompt ultrasound evaluation and guideline-based anticoagulation are essential to prevent complications.
Keywords: upper extremity deep vein thrombosis, peripheral catheter, psychiatric patient, antipsychotics, case report
Introduction
Upper extremity deep vein thrombosis (UEDVT) constitutes approximately 4–10% of all deep vein thrombosis (DVT) cases, with its incidence on the rise, largely due to the growing utilization of central and peripheral venous access devices.1 The upper limb’s deep venous system comprises vessels that accompany arteries of the same name, such as the radial, ulnar, and brachial veins (usually paired), as well as the axillary and subclavian veins the most commonly affected in UEDVT.1 The brachial vein may also be involved. Additionally, the internal jugular vein is considered part of the deep venous system due to its anatomical and hemodynamic continuity with central venous structures.2
Clinical Presentation
The clinical severity of UEDVT correlates with the degree of venous occlusion. The hallmark symptoms include unilateral arm swelling, discomfort, heaviness, and functional limitation. In cases where thrombosis extends into the superior vena cava (SVC), patients may present with neck swelling, facial plethora, or chest wall edema. Prominent superficial veins across the shoulder or chest referred to as Urschel’s sign may be visible, particularly in chronic obstruction.3
In rare, severe instances, impaired venous outflow may lead to arterial compromise, culminating in phlegmasia cerulea dolens, a critical, limb-threatening condition characterized by cyanosis, severe pain, and venous gangrene.4
Diagnosis
Diagnosis of UEDVT is based on clinical suspicion supported by imaging. Duplex ultrasonography is the first-line modality due to its non-invasiveness, high sensitivity, and accessibility.1 Findings include non-compressibility of the affected vein, absence of Doppler flow, and reduced respiratory variation in venous waveforms suggestive of proximal venous obstruction.3
Imaging of the subclavian vein can be technically challenging due to acoustic interference from the clavicle. In such cases, CT venography or MR venography (MRV), particularly with venous-phase protocols, may be utilized to delineate thrombus burden and identify compressive anatomical anomalies, particularly in suspected thoracic outlet syndrome.5
Complications
Although UEDVT carries a lower risk of pulmonary embolism (PE) compared to lower limb DVT, symptomatic PE occurs in approximately 5–8% of cases, and asymptomatic PE may be present in up to 36%. Associated mortality from PE is estimated at around 0.7%.3
Post-thrombotic syndrome (PTS) is another important complication, seen in up to 13% of cases. It is characterized by chronic arm pain, swelling, and reduced functional capacity. In patients with long-term catheter use, thrombosis may also impair vascular access, disrupt infusion or blood draw functionality, and ultimately result in loss of usable venous access—a serious concern in oncology and critical care populations.
Management
The cornerstone of UEDVT management is timely anticoagulation, aimed at preventing thrombus extension, restoring venous patency, and mitigating complications. Per the 2021 American College of Chest Physicians (ACCP) guidelines, direct oral anticoagulants (DOACs) are preferred over warfarin in most eligible patients. Treatment often starts with therapeutic low molecular weight heparin (LMWH), such as enoxaparin, followed by a transition to DOACs like apixaban or rivaroxaban, with a minimum anticoagulation duration of three months.6
Advanced interventions including catheter-directed thrombolysis (CDT) or mechanical thrombectomy are reserved for cases with severe symptoms, significant thrombus burden, or threatened limb viability. Placement of a superior vena cava (SVC) filter should be reserved for exceptional cases specifically, in patients who have a contraindication to anticoagulation and are at risk for pulmonary embolism. Routine catheter removal is not necessary unless the device is malfunctioning, infected, or no longer required. If the catheter has already been removed before symptom onset, as in this case, no further intervention is needed.6,7
Case Presentation
A 44-year-old male known patient with bipolar affective disorder on irregular medication was admitted to the psychiatric ward with a diagnosis of Bipolar Affective Disorder, manic episode. During hospitalization, he was initiated on haloperidol 10mg orally once daily, promethazine 50mg once daily, and carbamazepine 200mg twice daily.
He presented with a 3-day history of progressive right forearm swelling and pain.
The swelling initially appeared around the mid-forearm, localized and mild, but gradually extended proximally to involve the elbow and lower upper arm. The patient described the pain as dull and persistent, exacerbated by movement and palpation, and partially alleviated by limb elevation.
He reported a recent peripheral intravenous cannulation in the right forearm for medication administration, inserted approximately 5 days prior, and removed 2 days before symptom onset. At the time of removal, there were no signs of local inflammation such as redness or discharge although mild discomfort persisted, later followed by swelling.
The patient denied any trauma, insect bites, or strenuous upper limb activity. There were no systemic symptoms such as fever, chills, chest pain, dyspnea, or facial/neck swelling. He also denied neurological symptoms such as numbness, paresthesia, or weakness although arm movement was somewhat restricted due to discomfort.
Past Medical History
Known case of Bipolar Affective Disorder. No previous history of DVT, PE, malignancy, autoimmune disease, major surgery, bleeding disorders, or diagnosed thrombophilia. Medication history: Day 1–2: IV diazepam 20mg three times a day, chlorpromazine 25mg IM three times a day, and IV promethazine 25 mg twice a day. Subsequent days: Oral haloperidol 10mg, carbamazepine 200mg, and promethazine 50mg.
Family and Social History
No family history of DVT or inherited thrombophilia. Smoker and reports occasional binge alcohol consumption prior to admission. Denies IV drug use. Unemployed; formerly worked as a security guard. Lives with his wife and three children; brought in by family.
Examination
General: Alert and cooperative with blunted affect. Afebrile, BP: 128/84 mmHg, HR: 84 bpm, RR: 18/min, SpO2: 98% on room air. No signs of respiratory distress.
Local Examination (Right Upper Limb)
Diffuse swelling extending from the hand to the cubital fossa. Mild cyanosis over the forearm. No visible superficial collateral veins over the shoulder or chest. Skin: Warm, no ulceration or ecchymosis. Mild tenderness at the cubital region. Pitting edema presents over the forearm and arm. No bony tenderness, fluctuance, or crepitus. Preserved range of motion but limited by swelling. Radial and brachial pulses palpable and symmetric. Capillary refill time normal. Sensory and motor functions intact. As it shown in Figures 1 and 2.
 |
Figure 1 Shows swollen anterior aspect of fore arm and distal part of arm. |
Systemic Examination
CVS- Normal heart sounds (S1, S2), no murmurs, no raised JVP.
RSE-Clear breath sounds bilaterally. PAE-Soft, non-tender, no hepatosplenomegaly. CNS- Normal tone, power, and reflexes; cranial nerves intact.
Investigations
Full Blood Count (FBC): Within normal limits, as shown on Table 1.
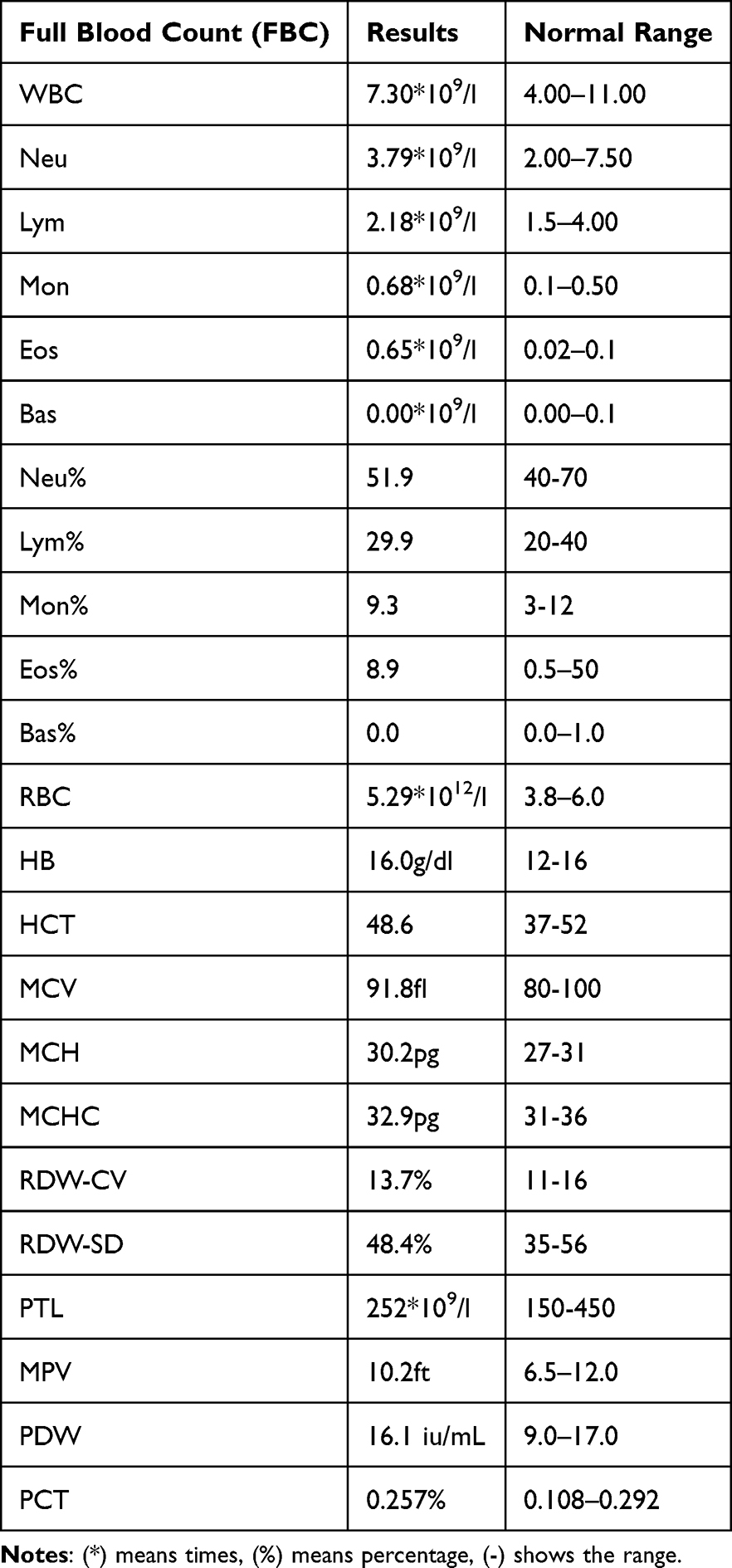 |
Table 1 Shows FBC Results |
PT, aPTT, and INR within normal limits, however has elevated D-dimer as shown in Table 2.
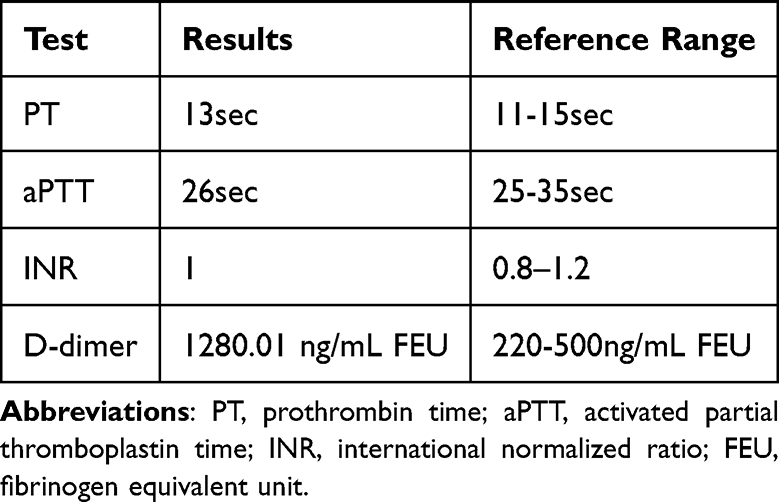 |
Table 2 Shows Coagulation Profile |
Doppler Ultrasound of Right Upper Limb: Evidence of acute thrombus in the antecubital vein, consistent with recent thrombosis, as it shown on Figure 3.
 |
Figure 2 Shows swollen of posterior part of forearm and hand. |
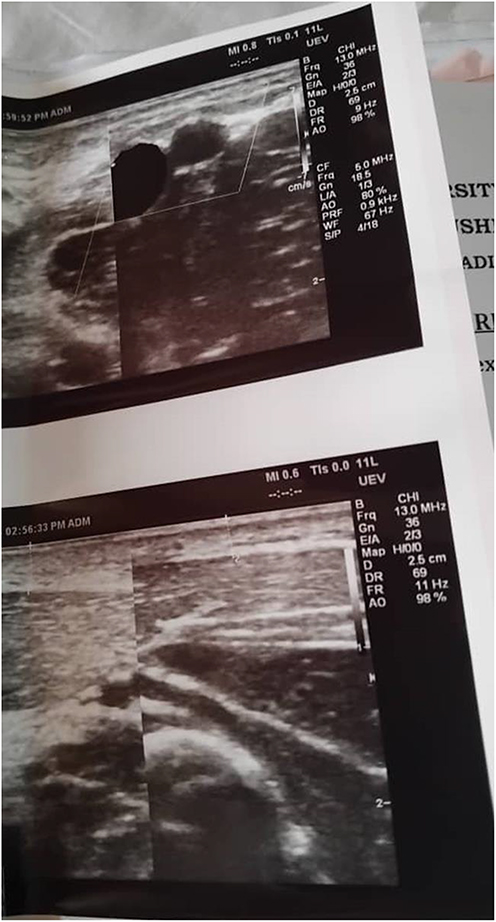 |
Figure 3 Shows ultrasound results of right upper limb-indicate the fresh thrombus at cubital vein. |
Working Diagnosis
Catheter-associated upper extremity deep vein thrombosis (UEDVT) involving the right axillary and subclavian veins.
Differential Diagnosis
Right forearm cellulitis.
Management
The patient was initiated on low molecular weight heparin (LMWH)-enoxaparin 60mg bd during hospitalization. On Day 6, he was discharged with oral apixaban 10mg bd for 7 days and then 5mg bd for 2 weeks for anticoagulation.
Follow-Up
At Week 3, the patient reported complete resolution of symptoms, including swelling.
At 3 months, apixaban was discontinued following normalization of D-dimer levels it was 308.06 ng/mL FEU. No recurrence or complications were reported.
Discussion
Upper extremity deep vein thrombosis (UEDVT), although far less common than lower limb DVT, is becoming increasingly recognized due to the widespread use of intravenous cannulation and central venous devices. UEDVT constitutes approximately 4–10% of all DVT cases and is typically categorized into primary and secondary types.
Primary UEDVT is less prevalent and typically results from effort-induced thrombosis, particularly Paget-Schroetter syndrome (PSS), a manifestation of venous thoracic outlet syndrome (vTOS).2 This condition predominantly affects young, physically active individuals, often involving the dominant upper limb. The pathogenesis involves compression of the subclavian vein as it traverses the thoracic outlet, particularly during repetitive arm movements. Contributing anatomical anomalies include hypertrophied scalene muscles, fibrous bands, cervical ribs, and prominent subclavius tendons.3
Repetitive microtrauma to the venous endothelium leads to local inflammation, venous wall remodeling, and eventual thrombosis. Over time, structural changes such as intraluminal webs or stenosis may develop, predisposing to recurrent thrombotic events.4
Secondary UEDVT represents the majority of cases and is commonly associated with intravascular devices such as central venous catheters (CVCs), peripherally inserted central catheters (PICCs), pacemakers, and defibrillator leads. Other risk factors include malignancy, recent surgery or trauma to the upper limb, pregnancy, and estrogen-containing contraceptive use.1
Catheter-associated thrombosis is the leading cause of secondary UEDVT, especially in hospitalized or critically ill patients. Thrombosis occurs following endothelial damage from catheter insertion and dwell time, coupled with blood flow disturbance and systemic hypercoagulability. Risk increases with multiple cannulation attempts, malpositioned catheter tips, large-bore devices, and prothrombotic states such as cancer or hereditary thrombophilias.5
Although peripheral intravenous (IV) cannulas are considered to have lower thrombogenic potential compared to central devices, they may still precipitate thrombosis in the setting of mechanical trauma, venous stasis, or a hypercoagulable environment. Symptoms of cannula-related UEDVT typically emerge within a few days, presenting with localized swelling, pain, and restricted mobility of the affected limb.6,7
In this case, a 44-year-old male developed painful right upper limb swelling following peripheral intravenous cannulation, a classical scenario for catheter-related secondary UEDVT. Although peripheral venous catheters are generally considered to carry a lower thrombotic risk compared to central venous catheters, they can still precipitate thrombosis, especially when associated with endothelial trauma, prolonged use, or mechanical irritation of the vessel wall.
The pathogenesis underlying catheter-associated thrombosis is well-explained by Virchow’s triad, which includes venous stasis, endothelial injury, and hypercoagulability. In this patient, mechanical injury from the cannula likely initiated endothelial inflammation and the coagulation cascade.8 Although the patient did not have typical prothrombotic conditions like malignancy or hereditary thrombophilia, the use of antipsychotic medications, such as haloperidol and chlorpromazine, may have contributed to a procoagulant state. These drugs have been reported to affect platelet aggregation and impair fibrinolysis, potentially increasing thrombotic risk also lead to weight gain and increased body mass index, moreover lead to immobility and sedation both of which are established risk for DVT.9
Clinically, the patient presented with progressive swelling and pain extending from the forearm to the upper arm, along with mild cyanosis and pitting edema features consistent with UEDVT. The absence of signs such as facial swelling or dilated collateral veins over the upper chest reduced the likelihood of superior vena cava (SVC) involvement. Diagnosis was confirmed by Doppler ultrasound, which demonstrated a fresh thrombus in the antecubital vein. Ideally, evaluation of proximal veins (eg, axillary or subclavian) should be considered when symptoms are extensive or if central vein involvement is suspected.
The patient received therapeutic low molecular weight heparin (LMWH) during hospitalization, later transitioned to apixaban, a direct oral anticoagulant (DOAC). This approach aligns with 2021 American College of Chest Physicians (ACCP) guidelines, which recommend DOACs over vitamin K antagonists (eg, warfarin) for most patients with venous thromboembolism (VTE).6 There were no indications for thrombolytic therapy or mechanical thrombectomy, as the patient remained hemodynamically stable with no signs of limb ischemia or phlegmasia cerulea dolens. Additionally, the catheter was removed two days prior to symptoms because it is no longer required.10
Potential complications of UEDVT include pulmonary embolism (PE) and post-thrombotic syndrome (PTS).11 In this case, the patient remained clinically stable, with no respiratory symptoms, and imaging for PE was not pursued. Follow-up at three weeks showed complete resolution of swelling, and anticoagulation was discontinued at three months, guided by normalized D-dimer levels and the absence of recurrence.
This case demonstrates that even peripheral IV catheters can lead to significant UEDVT, particularly in vulnerable populations such as psychiatric populations.
Limitation
This report is limited by lack of follow-up INR during visit and before discharge and availability of high-quality imaging. In addition, it presents a single case, limiting generalizability. However, the case highlights a rare but important complication with significant clinical implication.
Conclusion
Catheter-associated upper extremity DVT, though rare, should be considered in psychiatric patients presenting with arm swelling, clinicians should maintain vigilance in this population due to the combined risk of immobilization, repeated IV cannulations, and antipsychotic use. Early recognition and prompt anticoagulation can prevent complications such as pulmonary embolism.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgments
We acknowledge the patient and his family, and the internal medicine and Psychiatric departments of Kampala International University Teaching Hospital.
Author Contributions
All authors made a significant contribution to the work reported, took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study had no funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Heil J, Miesbach W, Vogl T, Bechstein WO, Reinisch A. Deep vein thrombosis of the upper extremity - A systematic review. Dtsch Arztebl Int. 2017;114(14):244–249. doi:10.3238/arztebl.2017.0244
2. Leung P, Lui B, Wang J, Ho P, Lim HY. A 12-year review of upper extremity deep vein thrombosis—are they the same as lower extremity deep vein thrombosis? J Clin Med. 2024;13(21):6440. doi:10.3390/jcm13216440
3. Engelberger RP, Kucher N. Management of deep vein thrombosis of the upper extremity. Circulation. 2012;126(6):768–773. doi:10.1161/CIRCULATIONAHA.111.051276
4. Onuoha CU. Phlegmasia cerulea dolens: a rare clinical presentation. Am J Med. 2015;128(9):e27–8. doi:10.1016/j.amjmed.2015.04.009
5. Joffe HV, Kucher N, Tapson VF, Goldhaber SZ. Upper-extremity deep vein thrombosis a prospective registry of 592 patients. Circulation. 2004;110(12):1605–1611.
6. Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic therapy for VTE disease compendium and review of CHEST guidelines 2012-2021. Chest. 2024;166(2):388–404. doi:10.1016/j.chest.2024.03.003
7. Ascer E, Gennaro M, Lorensen E, Pollina RM. Superior vena caval greenfield filters: indications, techniques, and results. J Vasc Surg. 1996;23(3):498–503. doi:10.1016/S0741-5214(96)80017-6
8. Schulman S, Makatsariya A, Khizroeva J, Bitsadze V, Kapanadze D. The basic principles of pathophysiology of venous thrombosis. Int J Mol Sci. 2024;25(21):1–17. doi:10.3390/ijms252111447
9. Schill J, Olsson H, Spigset O, Jo AK, Hägg S. Venous thromboembolism during treatment with antipsychotics: a review of current evidence. CNS Drugs. 2018;32(1):47–64. doi:10.1007/s40263-018-0495-7
10. Kucher N. Deep-vein thrombosis of the upper extremities. New England J Med. 2013;364(9):861–869.
11. Ortel TL, Neumann I, Ageno W, et al. American society of hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020;4(19):4693–4738. doi:10.1182/bloodadvances.2020001830
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.