Back to Journals » Clinical Ophthalmology » Volume 19
Peripheral Iridotomy-Less Approach in Descemet’s Membrane Endothelial Keratoplasty Using Pupil-Dilating Eye Drops, a Retrospective Case–Control Study
Authors Bayyoud T, Bartz-Schmidt KU, Rohrbach M, Gelisken F, Goldblum D, Martus P, Thaler S
Received 1 December 2024
Accepted for publication 2 April 2025
Published 13 April 2025 Volume 2025:19 Pages 1277—1288
DOI https://doi.org/10.2147/OPTH.S509682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Tarek Bayyoud,1 Karl Ulrich Bartz-Schmidt,1 Martin Rohrbach,1 Faik Gelisken,1 David Goldblum,2 Peter Martus,3 Sebastian Thaler1
1Department of Ophthalmology, University Hospital of Tübingen, Tübingen, 72076, Germany; 2Ophthalmology, Pallas Kliniken (Olten-Bern-Zürich-Aargau), Olten, 4600, Switzerland; 3Institute for Clinical Epidemiology and Applied Biometry, University of Tübingen, Tübingen, 72076, Germany
Correspondence: Tarek Bayyoud, Department of Ophthalmology, University Hospital of Tübingen, Elfriede-Aulhorn-Str. 7, 72076, Tübingen, Germany, Tel +49 07071-29-88188, Fax +49 07071-29-5018, Email [email protected]
Purpose: To assess clinical outcomes after Descemet’s Membrane Endothelial Keratoplasty (DMEK) with mydriatic eye drops without peripheral iridotomy (PI-less). We performed a retrospective, observational clinical study to determine the postoperative intraocular pressure (IOP) changes and graft viability in a cohort of patients with Fuchs’ endothelial corneal dystrophy (FECD) and bullous keratopathy (BK).
Patients and Methods: Included in this study were 41 PI-less DMEK patients with 44 eyes (median age: 77 years; range: 53– 88 years). Patients received either PI-less DMEK (group-1) or PI-less triple DMEK (group-2). The mean follow-up duration was 16 months. Eyes after standard DMEK or triple DMEK served as controls (n = 20). Included in the study were patients admitted to the hospital (securing IOP control), patients in which the tamponading agent was air or gas (SF6) and only patients with physiological air resorption, ie without routine, postoperative air/gas release (90% air/gas fill of the anterior chamber at end of surgery). Phakic eyes were not included. Postoperatively, mydriatic eye drops were administered for three days 4x/d (phenylephrine 25 mg/mL, tropicamide 5 mg/mL). The best-corrected visual acuity (BCVA), endothelial cell density (ECD), and IOP were assessed. Intra- and postoperative complications and management were recorded.
Results: BCVA improved significantly in both groups (group-1:0.90 ± 0.57 to 0.20 ± 0.23logMAR (p = 0.000); group-2:0.47 ± 0.23 to 0.17 ± 0.42logMAR (p = 0.0067). ECD decreased significantly: Group-1 2428± 225 cells/mm2 to 1810± 236 cells/mm2 (p = 0.005); group-2 2447 ± 178 cells/mm2 to 1866 ± 229 cells/mm2 (p = 0.012). After postoperative day-1 IOP decreased significantly: Group-1 p = 0.004 (10.0 ± 2.8 mmHg) and p = 0.002 (11.3 ± 3.1 mmHg); group-2 p = 0.002 (10.7 ± 3.6 mmHg) and p = 0.002 (11.4 ± 2.2 mmHg); for postoperative days 2 and 3, respectively. Postoperative adverse events included pupillary block necessitating emergency air release. Intergroup analysis did not show a significant difference in ECD, IOP (after postoperative day-1) and logMAR (after 6 months).
Conclusion: Patients may benefit from the promising results of the study regarding postoperative IOP developments and graft viability after DMEK using mydriatic eye drops (phenylephrine 25 mg/mL, tropicamide 5 mg/mL). PI-less triple DMEK in particular might improve accessibility, reduce surgical complexity, or lower costs, making it attractive in resource-limited settings. Close postoperative IOP monitoring is advised in PI-less DMEKs.
Plain Language Summary: What is already known on this topicThe standard procedure for a lamellar corneal transplant (DMEK) involves the placement of a peripheral iridotomy (PI) or iris hole;If corneal transplant surgery without PI (PI-less DMEK) is performed, then partial evacuation of air/gas from the anterior chamber of the eye 1-2 h after surgery besides postoperative pupil-dilating medication (mydriatics, phenylephrine 25 mg/mL, tropicamide 5 mg/mL) is necessary to avoid potentially sight-threatening increase in eye pressure (so-called pupillary block).
What this study addsPatients benefit from a DMEK without an iris hole, from having no routine postoperative air/ gas release and having no significantly increased risk of pupillary block;For the first time we have shown that the results of a PI-less triple DMEK (including cataract surgery) and a PI-less DMEK are comparable.
How this study might affect research, practice or policy
● The investigated PI-less triple DMEK procedure incorporating cataract surgery might offer unique benefits for the patients: This approach might improve accessibility, reduce surgical complexity, or lower costs, making it attractive in resource-limited settings.
Keywords: descemet membrane endothelial keratoplasty, DMEK, pupil-dilating eye drops, no peripheral iridotomy, PI-less
Introduction / Purpose
Fuchs endothelial corneal dystrophy (FECD) is a progressive corneal dystrophy initially characterized by collagenous excrescences (so-called guttae) at the level of the posterior elastic membrane (or Descemet’s membrane, DM) and eventually by stromal edema (bullous keratopathy, BK) with fibrosis leading to significant impairment of visual function.1,2 Selective replacement of the membrane with vital endothelial vision can be restored.3,4
The conventional surgical steps for replacement include the following: Preparing the donor tissue, descemetorhexis, peripheral iridotomy (ie, a preoperative or intraoperative inferior peripheral iridotomy [PI]), implanting and positioning the donor graft. The limitations with PI-based Descemet’s Membrane Endothelial Keratoplasty (DMEK) are possible glare, potential iris tissue distortions and intraoperative bleeding.
A prophylactic PI is usually placed to prevent pupillary block. We wanted to investigate in the current study whether the use of a prophylactic postoperative mydriasis instead of a prophylactic PI might have comparable outcomes. In addition, the replacing graft was attached to the posterior corneal surface using a subtotal (90%) gas/air bubble without a routine postoperative air/gas release. This might have practical benefits for the patients in need of a DMEK graft. An air management protocol was advocated to perfect the dissemination of any remaining risk to the patient.5,6 Recently, two studies on DMEK without PI are published and this PI-less method is familiar among the Descemet’s stripping (automated) Endothelial Keratoplasty (DS(A)EK) surgeons.7,8
The aim of this study was to evaluate whether a PI-less approach could provide significant patient benefits in DMEK and triple DMEK cases. The following parameters were assessed: Changes in intraocular pressure (IOP), intra-and postoperative adverse events (AE), best-corrected visual acuity (BCVA), endothelial cell density (ECD), and postoperative management including potential pupillary blocks.
Patients And Methods
We performed a retrospective, interventional, case–control series to learn about the preoperative and postoperative changes in intraocular pressure in a group of FECD/BK patients after PI-less DMEK and PI-less triple DMEK. Surgeries were performed at the University Eye Hospital of Tübingen by a single experienced surgeon (ST) over a period of 41 months.
A group of PI-less DMEK patients with FECD or BK with a follow-up of at least 1 month was selected. Patients received either PI-less DMEK or PI-less triple DMEK. A total of 41 patients (44 eyes) were included in the study. Signed informed consent was obtained from all the patients prior to surgery. The study followed the Tenets of the Declaration of Helsinki. The study was conducted according to the requirements of the Cornea Bank of the University Hospital of Tübingen and with independent institutional review board (IRB) approval (Project Number of the Independent Ethics Committee of the University of Tübingen: 839/2019BO2; data were analyzed anonymously). Eyes with comorbidities were included in the study. The concomitant conditions were registered. Eyes with ocular trauma were excluded from the study. Patients with preexisting PI were excluded. Inclusion criteria of the current study were: Only patients which were admitted to the hospital (securing IOP control), patients in which the tamponading agent was either air or gas (SF6) and only patients with a complete physiological air resorption, ie with no routine, postoperative air/gas release (90% air/gas fill of anterior chamber at end of surgery and then complete physiological air/gas resorption). Phakic eyes were not included.
Ethics
The study followed the Tenets of the Declaration of Helsinki. Signed informed consent was obtained from all the patients prior to surgery. The study was conducted according to the requirements of the Cornea Bank of the University Hospital of Tübingen and with independent institutional review board (IRB) approval (approved by the Ethics Committee of the University of Tübingen; Project Number: 839/2019BO2; data were analyzed anonymously).
Primary Outcome Measures
Primary outcome measures included BCVA in the logarithm of the minimum angle of resolution (logMAR), ECD, and IOP. BCVA was measured using Snellen visual acuity charts, IOP using Goldmann applanation tonometry, and ECD using specular microscopy (noncontact autofocus specular microscope; EM-3000, TOMEY CORP., Nagoya, Japan; automated count with quality checks). In addition, particular intraoperative and postoperative complications and management, including medical and surgical interventions, were carefully recorded.
Graft Preparation
Harvesting of DMEK grafts was performed according to the liquid bubble technique.9 After obtaining the donor globes, corneoscleral rings were dissected and stored in organ culture media (PAN Culture Medium I; PAN Biotech GmbH, Aidenbach, Germany). Only donor corneas with regular endothelial cell morphology and cell counts of 2300 cell/mm2 or more were allowed.
Surgery
All surgeries were performed by a single surgeon with extensive experience in anterior segment surgery (ST). A circular 7.5-mm-diameter descemetorhexis was performed under air by scoring and stripping off the Descemet membrane endothelial complex with an incisional hook (Price Hook, Moria S.A. Plc, France; Descemet incision hook, Geuder AG, Germany; Reversed Sinskey Hook, Katena Inc., USA). The graft was stained with trypan blue solution (Vision Blue; DORC, Zuidland, The Netherlands) and injected through a 2.75-mm limbal tunnel incision into the recipient anterior chamber via a glass injector. Iridotomy was not performed in any case. Intra-operative pupil status: In PI-less DMEK (group 1) mydriasis was performed at the end of the PI-less DMEK; in PI-less triple DMEK (group 2) mydriasis was performed during PI-less triple DMEK prior to cataract extraction. After orientation of the graft, facing the iris with its endothelial side, unfolding and attachment were performed using gentle corneal tapping and a bubble of air or gas (sulfur hexafluoride, 20%) between the iris and the endothelial layer of the donor DM. The anterior chamber was then filled with up to 90% air or gas. The air/gas (SF6) mixture was left as a tamponading agent until complete resorption occurred, ie no routine air/gas release in this study. Postoperatively, the patients were advised to maintain a supine position for 24 h. Postoperative medications included topical steroids (dexamethasone 0.1%) four times daily for 4 weeks and antibiotics for 2 weeks (moxifloxacin). The steroid regimen was subsequently reduced to once daily after three months and administered every other day for one year. Subsequently, the patient was advised to continue with 3–4 drops per week. The duration of surgery was registered. Postoperatively, our patients were routinely monitored 5 times a day including IOP. In cases of significantly elevated IOP, local and/or systemic medications were administered. Emergency ventilation (air/gas release) was performed in cases of insignificant reduction of IOP after medical treatment.
Data Collection and Analysis
Intra- and Postoperative Conditions
Intraoperative conditions were recorded, including patient-related and eye-related aspects (eg, agitation, positive vitreous pressure, intraoperative floppy iris, corneal abrasion), intraocular hemorrhage (eg, anterior chamber hyphema), state of the host membrane (eg, splits, fibrosis, adherence), and donor membrane (eg, peripheral tears of grafts of donors who had undergone cataract surgery).
The Postoperative conditions and management were recorded and analyzed for each case. The situations presented ranged from ocular-related (eg, increased IOP and cystoid macular edema), graft-related (eg, rejection, failure, and detachment), and patient-related (eg, patient adherence).10–12 Postoperative non-clearance of the cornea is considered as primary graft failure (PGF) and initial clearance followed by haziness after a month post surgery as secondary (SGF). Minor graft detachment was defined as separation of the graft by no more than one-third of the posterior stromal surface area. Major graft detachment was defined as an unattached graft in more than one-third of the posterior stromal surface area. Allograft rejection (AR) is defined as a sign of an immune reaction (eg, endothelial precipitates).
Postoperative Management
Postoperative management was classified as medical or surgical. The former consisted of IOP-lowering agents administered locally and/or systemically, and the latter encompassed air refill, air release, tissue grafts (eg, DMEK, amniotic membrane), and extraocular/intraocular drug delivery (eg, steroids). Patients received postoperative mydriatic eye drops (phenylephrine 25 mg/mL, tropicamide 5 mg/mL) administered 4x/d for three days.
Statistical Analysis
The level of significance was set at 0.05, and p-values are reported. For statistical analysis, the BCVA values were converted to logMAR units. Analyses were performed using a professional software (Microsoft Excel, version 2.73, Microsoft and SPSS, Version 28, IBM). Non-parametric analyses were applied using Wilcoxon-W and Mann–Whitney-U tests. In an ex post power consideration we can state, that group comparisons for DMEK vs controls could detect effect sizes of 1.09 to 1.16 (BCVA), 1.42 (ECD), and 1.13 to 1.15 (IOP). Effect sizes for triple DMEK vs controls were 1.14 to 1.27 (BCVA), 1.42 (ECD) and 1.14 to 1.16 (IOP).
Concomitant Ocular States
Eyes with comorbidities were included in the study. Concomitant conditions were registered, including previous surgeries (eg, glaucoma stent surgery, Descemet stripping only, or DMEK without endothelial keratoplasty), glaucoma, age-related macular degeneration, diabetic retinopathy, and significant others (postoperative cystoid macular edema, status post viral infection (eg, herpes virus), anterior megalophthalmos/megalocornea), epiretinal membranes, amblyopia, and uveitis). Eyes with ocular trauma were excluded from the study.
Results
Demographics of PI-Less DMEK and PI-Less Triple DMEK Patients
The age of the 41 patients (44 eyes) ranged from 53 to 88 years, with a median age of 77 years, and included 21 female and 20 male patients. The follow-up period ranged from 1 to 40 months (mean 16 months). The types of diagnoses for PI-less DMEK (N = 25) and PI-less triple DMEK (N = 19) included FECD (N = 29) and pseudophakic BK/BK secondary to FECD (N = 15). Concomitant cataracts were observed in 19 eyes.
Group 1 included pseudophakic eyes that received PI-less DMEK and group 2 included eyes with cataracts that received PI-less triple DMEK. Group 1 consisted of 25 eyes of 23 patients (counted twice for eye-related variables or counted once for patient-related variables) with a median age of 73 years (range: 54–82 years). The mean follow-up time was 14.8 months (SD, 8; range 1.2–28.8). Thirteen eyes (52%) were diagnosed with FECD, and 12 (48%) with pseudophakic BK.
Group 2 included 19 eyes of 18 patients (counted twice for eye-related variables or counted once for patient-related variables), with a median age of 78 years (range: 53–88 years). The mean follow-up time was 18.2 months (SD, 10.4; range, 1–40.3). Sixteen eyes (84%) were diagnosed with FECD, and three (16%) had BK secondary to FECD.
Best-Corrected Visual Acuity
The overall BCVA of postoperative eyes at 6 months of follow-up (no. of eyes completed 6 months of follow-up: 37) in both groups was significantly higher than that preoperatively (p = 0.000). The mean BCVA of the operated eyes of groups 1 and 2 was better 2 weeks postoperatively than at baseline. The majority of patients in both groups experienced visual improvement 2 weeks after surgery. Generally, in both groups, a secured visual improvement was noted postoperatively up to six months of follow-up. The overall mean values in logMAR were 0.19 ± 0.32 in postoperative eyes at 6 months of follow-up and 0.72 ± 0.50 in preoperative eyes. Data sets showed significant improvement of visual acuity at 6 months for each group compared to baseline (Table 1). The vision improved better in the control group of PI-less DMEK, although statistically not significant (p = 0.088). The number of included cases at baseline and each follow-up was for group 1 and 2: 25, 24, 24, 21 and 19, 18, 17, 16, respectively.
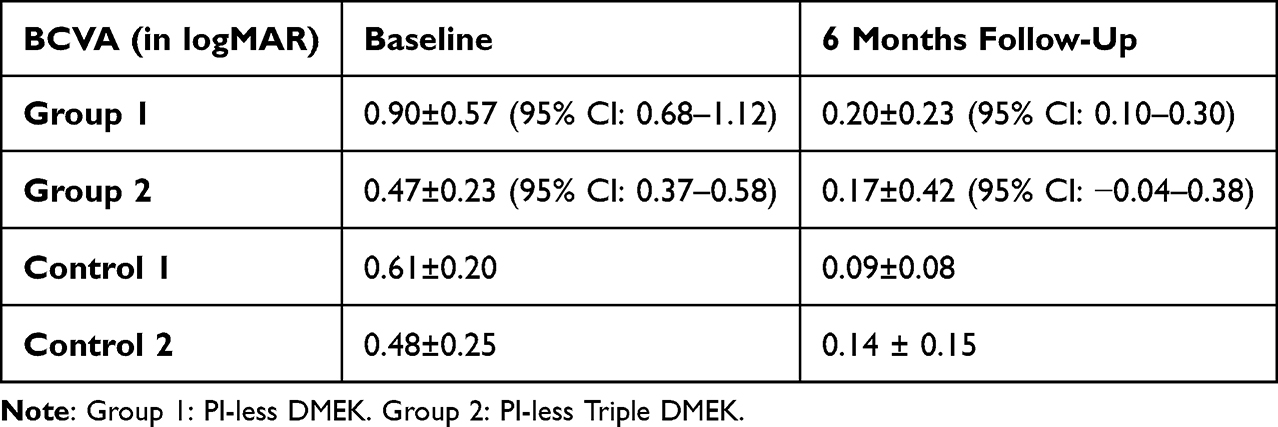 |
Table 1 BCVA Developments in PI-Less DMEK and PI-Less Triple DMEK |
The final visual improvement was comparable between the two groups (p = 0.018), although slightly but insignificantly in favor of group 2 (p = 0.288). Both groups showed rapid improvement in vision in the first two weeks after surgery. Follow-up visits showed further improvements in vision in each group. The follow-up intervals were 2-weeks, 2-months and 6-months. In general, the recovered sight was preserved throughout the study phase (Figure 1).
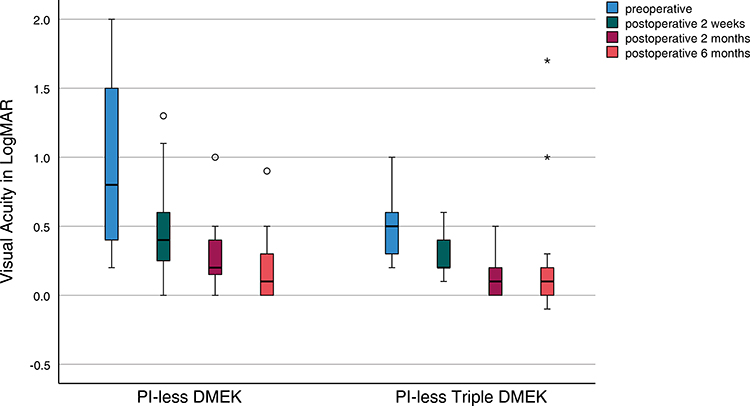 |
Figure 1 Visual acuity development in PI-less DMEK and PI-less Triple DMEK. Outliers are marked with a circle (PI-less DMEK) or an asterisk (PI-less Triple DMEK). |
Intra-Ocular Pressure Changes in PI-Less DMEK and PI-Less Triple DMEK
In most cases, IOP was within the normal range (Figure 2). However, in 3 cases, a postoperative IOP of more than 30 mmHg was recorded. In one of these three cases, the IOP was >60 mmHg). A pupillary block was observed in one case with significantly increased IOP (group 2). In the entire group, the mean preoperative IOP was 14 ± 3 mmHg (control group, 15 ± 3 mmHg). The overall mean postoperative IOP on the day of surgery was 18 ± 12 mm Hg (control, 14 ± 3 mm Hg). Three days after surgery, the overall mean IOP decreased, and the SD was smaller (data: IOP on postoperative day 1, 2, and 3: 13 ± 5 mmHg, 10 ± 3 mmHg, and 11 ± 3 mmHg, respectively; control: 13 ± 3 mmHg, 11 ± 3 mmHg, and 11 ± 2 mmHg, respectively). The observed pattern of a higher mean postoperative IOP on the day of surgery with an increased SD and the subsequent decline in mean IOP (on postoperative days 1 to 3) with a corresponding smaller SD was found for both groups. IOP data is shown in Table 2.
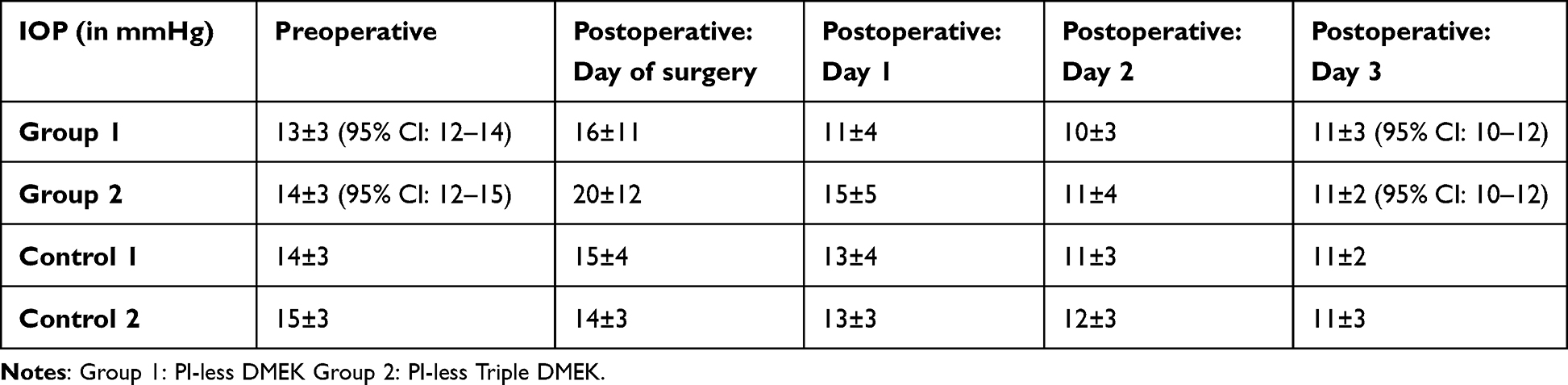 |
Table 2 IOP Developments in PI-Less DMEK and PI-Less Triple DMEK |
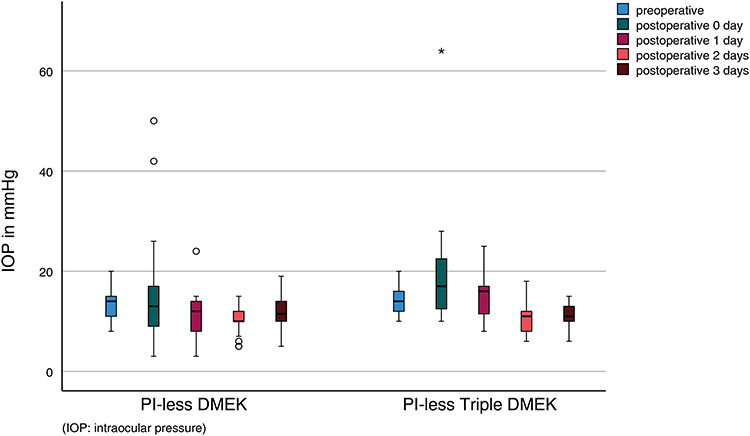 |
Figure 2 IOP development in PI-less DMEK and PI-less Triple DMEK. Outliers are marked with a circle (PI-less DMEK) or an asterisk (PI-less Triple DMEK). |
After postoperative day 1, IOP decreased significantly in both groups (group 1: p = 0.004 (10.0 ± 2.8 mmHg) and p = 0.002 (11.3 ± 3.1 mmHg); group 2: p = 0.002 (10.7 ± 3.6 mmHg) and 0.002 (11.4 ± 2.2 mmHg); on postoperative days 2 and 3, respectively) compared to preoperative IOP. Inter-group analysis revealed no significant difference after postoperative day 1 between the two groups (p = 0.852 and p = 0.988 for postoperative days 2 and 3, respectively). The control group analysis (Control 1: PI DMEK and Control 2: PI triple DMEK) showed significance for pre- and postoperative IOP in group 2, ie, a significantly increased IOP postoperatively on the day of surgery in PI-less triple DMEK patients compared to the control; p = 0.023).
Endothelial Cell Density
ECD decreased significantly over a follow-up period of 6 months in both groups (group 1: p = 0.005; group 2: p = 0.012). Generally, ECD was equal to or greater than 2300 cells per mm3 prior to surgery. The mean ECD of the donor tissues was 2436 ± 204 cells/mm2. At the final follow-up, the mean ECD was 1835 ± 228 cells/mm2(decrease of 24.7%).
Intergroup analysis showed no significant differences between the two groups (p = 0.450 at 6 months; data: preoperative, mean ECD: group 1 and 2: 2428 ± 225 (95% CI: 2368–2527) cells/mm2 and 2447 ± 178 (95% CI: 2367–2527) cells/mm2, respectively; control: 2520 ± 235 cells/mm2; 2680 ± 297 cells/mm2, respectively; final follow-up mean ECD: group 1 and 2: 1810 ± 236 (95% CI: 1663–1956) cells/mm2 (decrease of 25.4%) and 1866 ± 229 (CI: 1696–2035) cells/mm2(decrease of 23.7%), respectively; control: 1754 ± 363 cells/mm2 (decrease of 30.3%); 1835 ± 455 cells/mm2 (decrease of 31.5%) respectively; number of included cases at baseline and final follow-up: group 1 and 2: 25, 10, and 19, 8, respectively; Figure 3). The control group analysis showed no significant difference in ECD development (ECD preoperatively and ECD 6 months after surgery) in both groups (Control 1: PI DMEK; Control 2: PI triple DMEK).
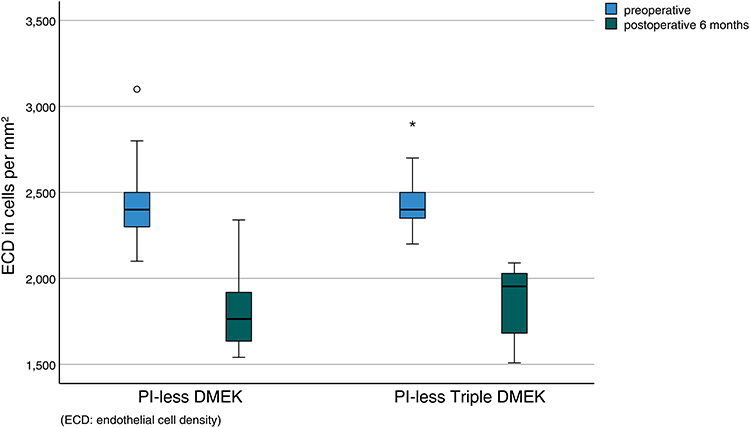 |
Figure 3 ECD changes for PI-less DMEK and PI-less Triple DMEK. Preoperative ECD is the ECD of the graft prior to DMEK. Outliers are marked with a circle (PI-less DMEK) or an asterisk (PI-less Triple DMEK). |
Intra- and Postoperative Conditions and Events
The intraoperative complications were host DMEK graft separation (peripheral or paracentral) (N = 1; control: N = 1), highly adherent, fibrosed host DM (N = 1; control: N = 2), positive vitreous pressure (N = 2; both in group 1; none with associated expulsive hemorrhage), agitated, moving patient (N = 1), intraoperative floppy iris syndrome (N = 1), corneal abrasion (only in control: N = 2), and graft with peripheral tears (ie, donor received clear corneal cataract surgery; only in control: N = 1). None of the eyes experienced intraoperative expulsive hemorrhage or postoperative anterior chamber bleeding.
The graft detachment and rebubbling rates in group 1 were 4% each (1/25). No major graft detachments occurred. The corresponding rates in group 2 were 47% and 42% (9/19 and 8/19). One major graft detachment was observed. Table 3 shows the number of other recorded postoperative complications including p-values.
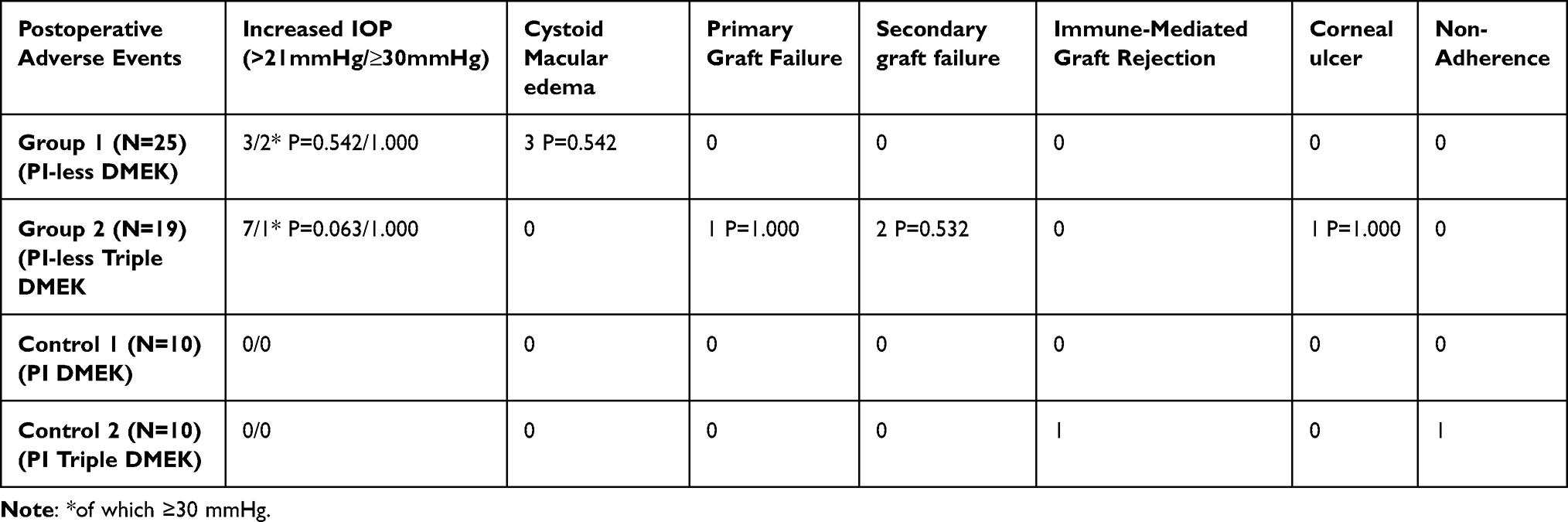 |
Table 3 Postoperative Adverse Events |
The duration of surgery for groups 1 and 2 was 22 ± 8.5 min (control: 21.5 ± 4.7 min) and 31 ± 5.9 min (control: 33.0 ± 6.3 min), respectively (Figure 4, Table 4). The tamponade agent SF6 was administered during the main surgery and the interventional surgery (ie, re-bubbling) in 2 (group 1) and 1 (group 2) cases, respectively (Control 2: N = 1, main surgery). A pupillary block was observed in one case (group 2) as mentioned in the intra-ocular pressure section.
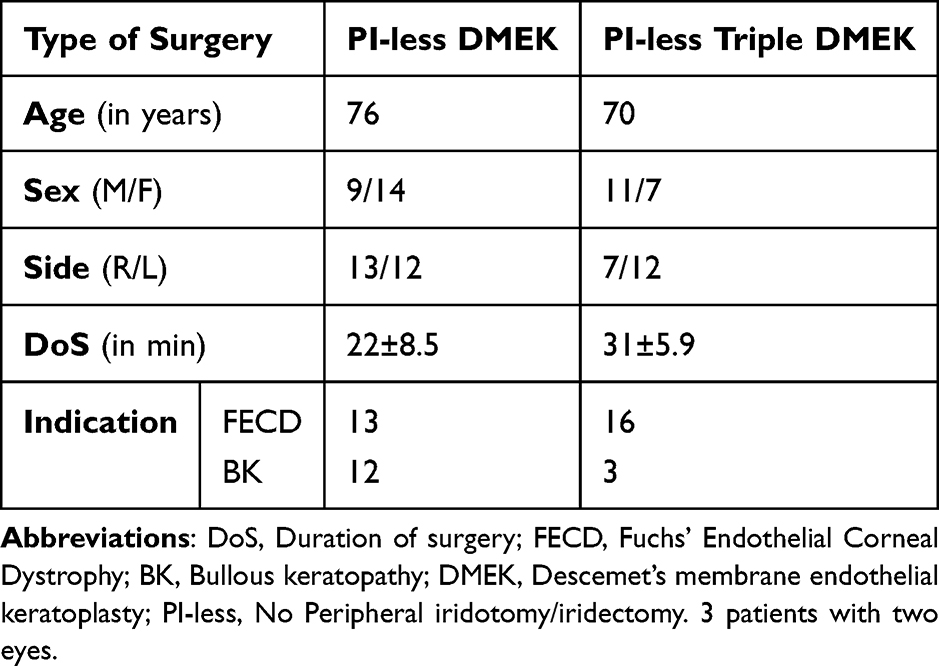 |
Table 4 Demographics to PI-Less DMEK |
 |
Figure 4 Schematic representation of a phakic eye after a standard DMEK (left) and a PI-less DMEK (right; PI-less: No Peripheral iridotomy): Arrows indicating potential fluid shifts from the anterior chamber to the posterior one and vice versa (left: Fluid shifts through a pre-existing PI or an intra-operatively placed PI; right: Fluid shifts through a medically dilated pupil) with a DMEK graft (dark colored) being attached using a gaseous/ tamponading agent (transparent bubble: air or SF6). |
Postoperative Management
Postoperative management (ie, type and timing of medical/surgical interventions) included medical adjustment of IOP by local and intravenous drugs (drugs administered: local: beta blockers (timolol, 5 mg/mL, bid), inhibitors of carbonic anhydrase (dorzolamide, 20 mg/mL, bid/tid; brinzolamide, 10 mg/mL, bid), alpha 2 adrenergic receptor agonists (brimonidine, 2 mg/mL, bid/tid), prostaglandins (tafluprost, 15 µg/mL, once daily; latanoprost 50 µg/mL, once daily); systemic: acetazolamide (100 mg/mL, prn), mannitol (0.2 g/mL, prn); IOP > 30 mmHg: group 1: N = 2; group 2: N = 1), surgical IOP correction (ie: air release; group 1: N = 0; group 2: N = 1), re-bubbling (group 1: N = 1; group 2: N = 8), tissue grafting (group 1: none; group 2: DMEK: N = 3; amniotic membrane: N = 1), and anti-inflammatory drug administration (local: Nevanac (1 mg/mL nepafenac; Alcon, Puurs, Belgium); and via ocular drug delivery (intravitreal or para-/retrobulbar): Triesence (40 mg/mL triamcinolone acetonide; Alcon, Fort Worth, TX, USA); and Diprosone (2.62 mg/6.43 mg betamethasone-dihydrogen-phosphate/ betamethasone-dipropionate depot, MSD Sharp & Dohme, Munich, Germany); group 1: Intravitreal: N = 1; para-/retrobulbar: N = 1; group 2: none). Graft failure (primary or secondary) accounted for graft loss (N = 3). No graft was lost because of the surgical procedures themselves. Detachments (major and/or minor) and immune rejection were successfully managed surgically and medically, respectively.
In general, postoperative interventions were performed at 11.9 and 134 days for re-bubbling and re-DMEKs, respectively. Surgical and medical IOP correction was performed immediately. No eyes had any kind of long-term or lasting pathology due to periods of significantly increased IOP. No patients have received a phakic DMEK in this study. Premature loss to follow-up (<100 days) was observed in five cases. The number of included cases for each examination and/or parameter fluctuated because of the following reasons: not measurement/unreliable data and/or patient nonadherent/unreliable response.
Discussion
PI-less DMEK and PI-less triple DMEK are safe and effective modifications of standard DMEK under close postoperative IOP monitoring. In addition, the waiver of a PI/PE saved surgical time, including possible adverse events (eg, anterior chamber bleeding, fibrinous adhesions, or pupillary distortions).11,13
PI-less DMEK can be offered in a clinical setting, ensuring close postoperative monitoring of IOP.7,8,14 The major finding was that PI-less DMEK in a minority of cases encountered suboptimal postoperative IOP spikes of clinical relevance.7,8 Thus, if left untreated or unnoticed, one might expect terminal visual loss. In our series, no eyes had any kind of long-term or lasting pathology due to periods of significantly increased IOP.
In both groups BCVA improved significantly as early as two weeks after surgery and continued to increase significantly for up to 6 months of follow-up. Outliers in each group were explained by the postoperative conditions and/or events, such as graft detachment and CME. In general, BCVA development in both groups was comparable to that in the study groups of Livny et al and Mukhija et al.7,8
The postoperative IOP significantly increased on the day of surgery (6.8%; N = 3) in group 1 (N = 2) and group 2 (N = 1). The highest IOP measured was 60 mmHg. Of note, the controls, ie including control 1 (PI DMEK) and 2 (PI triple DMEK), did not exhibit any case of significantly increased IOP. The IOP changes followed a similar postoperative pattern in the PI-less DMEK and PI-less triple DMEK groups.
ECD showed a constant and steady decrease over the first 6 postoperative months in both groups. The anticipated decline was in the range of the employed controls and was comparable to the other groups (Table 5). No significant increase in endothelial cell loss was observed in the control groups.
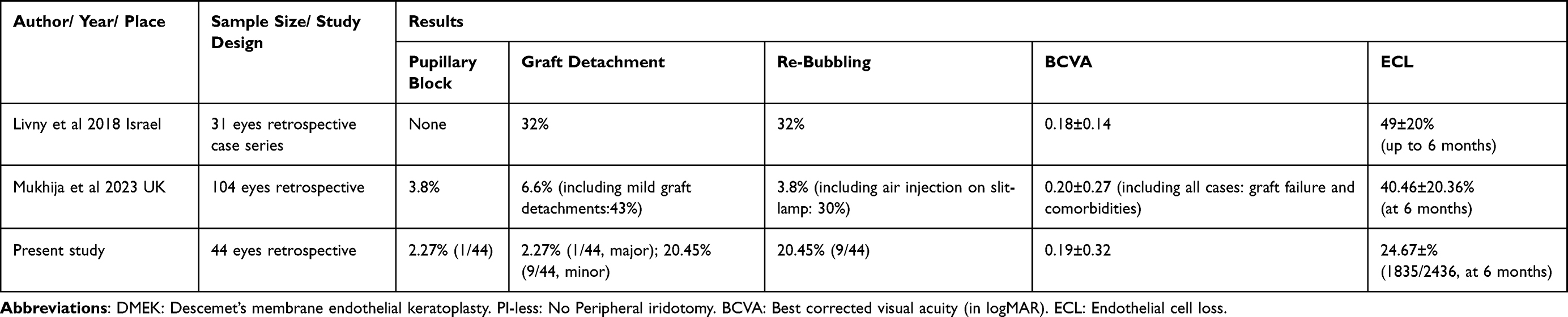 |
Table 5 Overview of Results of PI-Less DMEK in the Literature |
Postoperative conditions and/or events included CME, graft detachment, re-bubbling, and pupillary block. The CME rate was significantly higher in the PI-less DMEK group. CME was observed in three cases in the PI-less DMEK group and in none in the PI-less triple DMEK group. The other groups did not identify any potential risk factors for CME after DMEK, including concurrent DMEK and cataract surgery.10 The graft detachment rates were 2.27% (1/44) and 20.45% (9/44) for major and minor detachments, respectively. The re-bubbling rate was significantly higher in the PI-less triple-DMEK group. Re-bubbling was performed in a total of 20.45% (9/44) of cases. All rebubbling procedures were performed in the operating room. The higher re-bubbling rate might be explained by the weaker Iris-IOL diaphragm after triple DMEK. The tamponading effect on the graft may be weaker or not long-lasting. Other groups have reported higher re-bubbling rates in triple DMEK procedures.15 Pupillary block is a serious adverse event. The total number of serious adverse events in both groups was 1. The patient in question did not experience long-term damage. Postoperative management was conscientiously and meticulously performed. This spared our patients from serious adverse events, such as terminal visual loss in states of significantly increased IOP or in the case of a pupillary block. Urrets-Zavalia-Syndrome (UZS) was not observed in any patient. An acute increase in IOP postoperatively and routine instillation of strong mydriatics (phenylephrine 25 mg/mL, tropicamide 5 mg/mL) after surgery did not trigger iris ischemia or UZS. The mechanism of UZS has not yet been fully determined but might be multifactorial in nature.16–19
In comparison to the other groups, our results were similar with respect to developments in BCVA, ECD, and IOP. PI-less DMEK has been shown to be an effective alternative to standard DMEK. In our opinion it should not be performed in eyes with a narrow anterior chamber and in settings where IOP cannot be closely monitored.
The limitations of the current study are its retrospective nature, the relatively small sample size, and the inclusion of eyes with comorbid conditions. Of note, the study’s retrospective design limits its ability to establish causality, the long-term follow-up and outcomes, like endothelial cell loss, might skew the results.
In conclusion, PI-less DMEK and PI-less triple DMEK may safely be performed with a postoperative application of mydriatic eye drops (phenylephrine 25 mg/mL, tropicamide 5 mg/mL). The PI-less procedures were performed with subtotal tamponade (90%), without routine air/gas release after surgery, and careful postoperative care including regular intraocular pressure monitoring. The aforementioned points might also be considered in future research protocols. The investigated PI-less triple DMEK procedure incorporating cataract surgery might offer unique benefits for the patients. This approach might improve accessibility, reduce surgical complexity, or lower costs, making it attractive in resource-limited settings. Despite its benefits serious adverse events such as significantly increased IOP and pupillary blocks may occur. To improve our understanding of this topic in endothelial keratoplasty research, further long-term, preferably prospective studies are needed.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fuchs E. Dystrophia epithelialis corneae. Graefes Arch Clin Exp Ophthalmol. 1910;76:478–508.
2. Knapp A. Dystrophia epithelialis corneæ (fuchs), with the report of a case. Trans Am Ophthalmol Soc. 1911;12:745–747.
3. Melles GR, Ong TS, Ververs B, et al. Preliminary clinical results of descemet membrane endothelial keratoplasty. Am J Ophthalmol. 2008;145:222–227.
4. Herdt L, Vasiliauskaitė I, Kocaba V, et al. Descemet membrane endothelial keratoplasty (DMEK): 10-year clinical outcomes and graft survival. BMJ Open Ophthalmol. 2022;7(Suppl 2):A15–A16. doi:10.1136/bmjophth-2022-EEBA.37
5. Gonzalez A, Price FW, Price MO, et al. Prevention and management of pupil block after descemet membrane endothelial keratoplasty. Cornea. 2016;35:1391–1395. doi:10.1097/ICO.0000000000001015
6. Romano D, Aiello F, Parekh M, et al. Incidence and management of early postoperative complications in lamellar corneal transplantation. Graefes Arch Clin Exp Ophthalmol. 2023;261:3097–3111. doi:10.1007/s00417-023-06073-6
7. Livny E, Bahar I, Levy I, et al. “PI-less DMEK”: results of descemet’s membrane endothelial keratoplasty (DMEK) without a peripheral iridotomy. Eye. 2019;33:653–658. doi:10.1038/s41433-018-0294-x
8. Mukhija R, Quiney G, Nanavaty MA. Clinical Outcomes of descemet’s membrane endothelial keratoplasty without routine prophylactic peripheral iridotomy. Vision. 2023;7:41.
9. Szurman P, Januschowski K, Rickmann A, et al. Novel liquid bubble dissection technique for DMEK lenticule preparation. Graefes Arch Clin Exp Ophthalmol. 2016;254:1819–1823. doi:10.1007/s00417-016-3377-z
10. Kocaba V, Mouchel R, Fleury J, et al. Incidence of cystoid macular edema after descemet membrane endothelial keratoplasty. Cornea. 2018;37:277–282. doi:10.1097/ICO.0000000000001501
11. Benage M, Korchak M, Boyce M, et al. Intraoperative fibrin formation during descemet membrane endothelial keratoplasty. Am J Ophthalmol Case Rep. 2020;18:100686. doi:10.1016/j.ajoc.2020.100686
12. Hovanesian J, Singh IP, Bauskar A, et al. Identifying and addressing common contributors to nonadherence with ophthalmic medical therapy. Curr Opinion Ophthalmol. 2023;34(Suppl 1):S1–S13. doi:10.1097/ICU.0000000000000953
13. Arnalich-Montiel F, Pérez-Sarriegui A, Lauzirika G, et al. Pupillary abnormalities in descemet membrane endothelial keratoplasty after nearly full tamponade. Cornea. 2017;36:290–294. doi:10.1097/ICO.0000000000001141
14. Gumus G, Altan C, Yildirim Y, et al. Early intraocular pressure changes following different keratoplasty techniques and association with cornea parameters and anterior chamber depth. Ther Adv Ophthalmol. 2022;14:25158414221083359. doi:10.1177/25158414221083359
15. Semler-Collery A, Bloch F, Hayek G, et al. Comparison of triple-DMEK to pseudophakic-DMEK: a cohort study of 95 eyes. PLoS One. PLoS One. 2022;17:e0267940. doi:10.1371/journal.pone.0267940
16. Tuft SJ, Buckley RJ. Iris ischaemia following penetrating keratoplasty for keratoconus (Urrets-Zavalia syndrome). Cornea. 1995;14:618–622.
17. Nizamani NB, Bhutto IA, Talpur KI. Cluster of Urrets-Zavalia syndrome: a sequel of toxic anterior segment syndrome. Br J Ophthalmol. 2013;97:976–979. doi:10.1136/bjophthalmol-2012-302319
18. Maurino V, Allan BD, Stevens JD, et al. Fixed dilated pupil (Urrets-Zavalia syndrome) after air/gas injection after deep lamellar keratoplasty for keratoconus. Am J Ophthalmol. 2002;133:266–268. doi:10.1016/S0002-9394(01)01308-3
19. Anwar DS, Chu CY, Prasher P, et al. Features of Urrets-Zavalia syndrome after descemet stripping automated endothelial keratoplasty. Cornea. 2012;31:1330–1334. doi:10.1097/ICO.0b013e318259ca15
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.