Back to Journals » International Journal of Women's Health » Volume 17
Perioperative Platelet Transfusion Strategies and Multidisciplinary Collaboration Experience in Glanzmann Thrombasthenia Caused by ITGA2B Gene Variation During Pregnancy: A Case Report
Authors Cui X, Ji N ![]() , Wang S, Jamal H
, Wang S, Jamal H ![]() , Liu J, Wang Y, Sun H
, Liu J, Wang Y, Sun H
Received 21 June 2025
Accepted for publication 10 November 2025
Published 17 November 2025 Volume 2025:17 Pages 4559—4564
DOI https://doi.org/10.2147/IJWH.S548705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Xue Cui,1,* Nuowei Ji,1,* Shengnan Wang,1 Huawei Jamal,2 Jiaxin Liu,1 Ying Wang,3 Haiyan Sun1
1Department of Gynecology and Obstetrics, The Second Hospital of Dalian Medical University, Dalian, Liaoning Province, 116023, People’s Republic of China; 2Nursing Department, Lower Clapton General Practice, London, E5 0RD, UK; 3Department of Laboratory, The Second Hospital of Dalian Medical University, Dalian, Liaoning Province, 116023, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haiyan Sun, Department of Gynecology and Obstetrics, The Second Hospital of Dalian Medical University, Dalian, Liaoning Province, 116023, People’s Republic of China, Tel +86 411 84671291, Email [email protected]
Objective: To explore multidisciplinary peripartum management strategies and clinical implications for Glanzmann thrombasthenia (GT) caused by ITGA2B gene variation during pregnancy.
Case Presentation: A 33-year-old woman at 38+5weeks of gestation, diagnosed with GT, was confirmed with biallelic pathogenic ITGA2B mutations (chr17:42452041 and chr17:42,457,372). There was no history of consanguineous marriage in the past three generations of her family. Coagulation dysfunction was observed during pregnancy (fibrinogen: 2.69 g/L; thromboelastography (TEG) maximum clot strength: 12 mm). A multidisciplinary team (MDT) recommended preoperative transfusion of 3 therapeutic doses of platelets and 10 units of cryoprecipitate, with dynamic TEG monitoring showing improved clot strength (post-transfusion maximum clot strength: 29.2 mm). A cesarean section delivered a healthy male infant (3455 g, Apgar score 10). Intraoperative bleeding (900 mL) and postoperative incisional oozing were controlled with compression bandages and platelet transfusion. Both mother and infant had favorable outcomes, with the incision achieving Grade II/A healing.
Conclusion: Individualized coagulation regulation, multidisciplinary collaboration, dynamic TEG-guided platelet transfusion, and comprehensive postoperative hemostatic management are critical for GT with pregnancy. This case provides practical insights into peripartum care for GT patients.
Keywords: glanzmann thrombasthenia, pregnancy, ITGA2B gene variation, multidisciplinary collaboration, thromboelastography, TEG
Introduction
Glanzmann Thrombasthenia is a rare autosomal recessive disorder caused by variants in the ITGA2B or ITGB3 genes, leading to integrin αIIbβ3 dysfunction. Clinically characterized by spontaneous mucosal bleeding and high surgical bleeding risk, its estimated incidence is approxitely 1 in 1 million. Managing GT during pregnancy poses significant challenges: physiological hypervolemia, delivery trauma, and placental separation may trigger life-threatening hemorrhage, while maternal anti-αIIbβ3 antibodies may induce fetal thrombocytopenia and intracranial hemorrhage. Current international guidelines recommend optimizing peripartum care through multidisciplinary collaboration, recombinant activated factor VII (rFVIIa), or platelet transfusions. However, individualized protocols for genetically confirmed cases remain lacking. This report describes a pregnant woman with GT caused by biallelic ITGA2B mutations (chr17:42452041 and chr17:42,457,372). A tailored MDT approach—incorporating preoperative platelet transfusion protocols, intraoperative hemostatic agents, and postoperative supportive care–achieved maternal-fetal safety. This case addresses three critical questions: (1) the clinical value of dynamic coagulation monitoring in GT during pregnancy; (2) the feasibility of TEG-guided platelet transfusion; and (3) the pivotal role of multidisciplinary collaboration in managing complex hemorrhagic disorders. By synthesizing this experience, we provide reference for the management of pregnancy with Glanzmann Thrombasthenia.
Case Report
A 33-year-old female was admitted on September 4, 2024, with the chief complaints of “diagnosed Glanzmann Thrombasthenia 2 years prior, at 38+5weeks of gestation”. Two years ago, due to excessive menstrual bleeding and anemia, the patient’s younger sister was diagnosed with GT in the hematology department. Then the patient’s platelet membrane protein analysis was performed, showing CD61: 0%, CD42: 94.36%, and CD41: 0%, consistent with GT. Subsequent genetic testing identified pathogenic variations in the ITGA2B gene at chr17:42452041 and chr17:42457372. She was considered to be GT type I. Their parents are carriers of the pathogenic gene but exhibit normal phenotypes. The patient’s first pregnancy occurred in July 2023, but she experienced a missed abortion at 8 weeks of gestation and underwent an induced abortion. Half an hour after the surgery, the patient experienced increased vaginal bleeding. After administering uterotonic drugs and transfusing 1 unit of platelets, the patient’s bleeding stopped. This is the patient’s second pregnancy, during which she only experienced mild gum bleeding and petechiae. We conducted a coagulation function test at 22+4 weeks of gestation revealed fibrinogen levels of 2.69 g/L. TEG at 35+5 weeks demonstrated an α-angle of 14.90° and MA of 14.10 mm. No significant abnormalities in coagulation factor activity were detected at 36+3 weeks, and antiplatelet GPIIb/IIIa antibodies were negative at 36+5 weeks. Regular antenatal visits during pregnancy showed no significant abnormalities. She was admitted at 38+5 weeks for delivery planning. After admission, laboratory tests showed hemoglobin 146 g/L, platelet count 113×10^9/L, TEG MA 12 mm, and α-angle of 28.1°. Complete multidisciplinary consultation before delivery. The obstetrics department recommends that the pregnancy has reached 38+5 weeks, the coagulation function is very poor, and the optimal mode of delivery is cesarean section. The Department of Anesthesiology recommends that patient has extreme hypocoagulation, that general anesthesia is safer, double venous access should be opened, and arterial access should be prepared. The Department of Blood Transfusion recommends actively preparing blood products, determining the timing, composition and dose of transfusion, and retesting in time after infusion. The laboratory department recommends monitoring DIC and TEG before platelet transfusion, during transfusion, and prenatal time, and prepare rFVIIa. The Department of Hematology recommends that according to the literature on the management of GT in pregnant women, it is recommended to prepare 4 therapeutic amounts of platelets and transfuse 3 therapeutic amounts of platelets before surgery to prevent bleeding. Serial TEG evaluations post-transfusion demonstrated progressive improvement. On the day of the operation, the first therapeutic dose of apheresis platelets was infused at 6:05 am, the second therapeutic dose at 7:00 am and the third therapeutic dose of platelets and cryoprecipitate coagulation factor 10U were infused at 10:10 am. After 1 unit of platelets, MA increase to 24.3 mm (α-angle: 33.8°; clot formation time: 14.1 min) (Figure 1); after 2 units, MA 28.4 mm (α-angle: 37.0°; clot formation time: 9.1 min) (Figure 2); and after 3 units, MA 29.2 mm (α-angle: 35.2°; clot formation time: 8.1 min) (Figure 3).
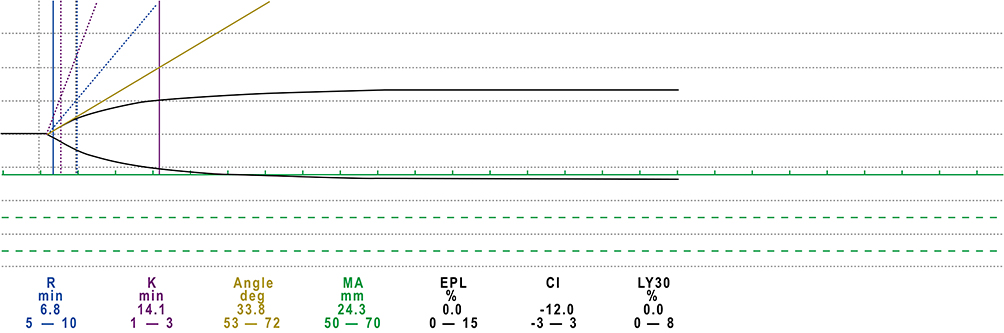 |
Figure 1 After 1 unit of platelets, MA 24.3 mm, α-angle 33.8°, clot formation time 14.1 min. |
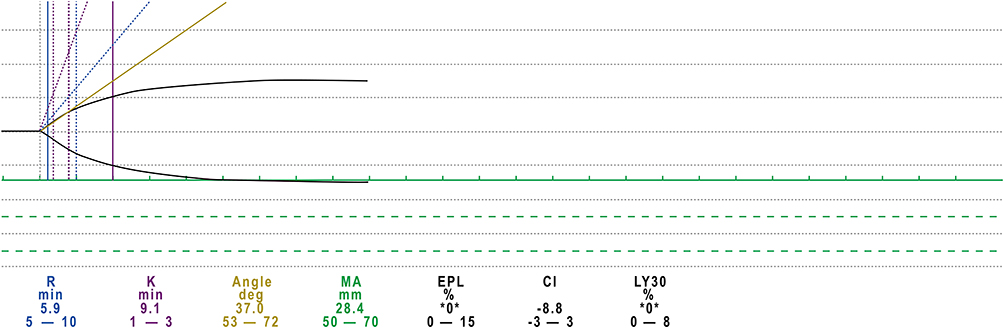 |
Figure 2 After 2 units of platelets, MA 28.4 mm, α-angle 37.0°, clot formation time 9.1 min. |
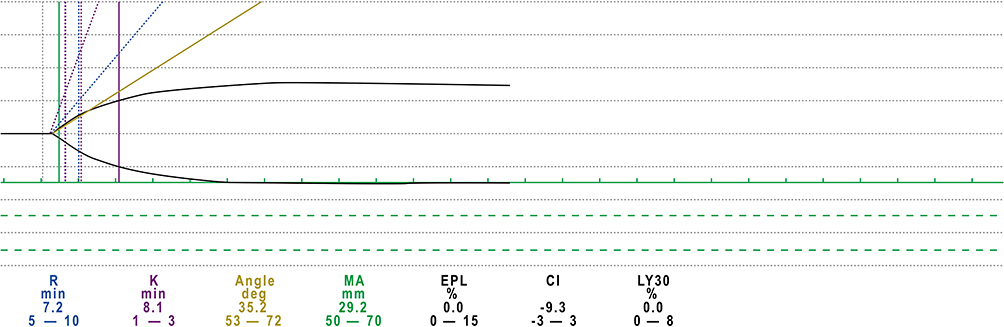 |
Figure 3 After 3 units of platelets, MA 29.2 mm, α-angle: 35.2°, clot formation time 8.1 min. |
Cesarean section was performed on September 5, 2024, 13:13, delivering a male infant (3455 g, Apgar score 10 at 1 minute). General anesthesia is used during the operation. Uterine atony and significant bleeding from the incision site required intramuscular carboprost (250 μg), intravenous oxytocin, tranexamic acid, and an additional platelet transfusion (intraoperative blood loss: 900 mL). Postoperative day 2 revealed serosanguinous drainage at the incision site, managed with compression dressing and another platelet transfusion. Prophylactic antibiotics, iron sucrose for anemia, albumin for hypoalbuminemia, and thromboprophylaxis (early ambulation, compression stockings, ankle exercises) were administered. The incision achieved Grade II/A healing by postoperative day 5. The baby was well and discharge along with his mum.
Discussion
Glanzmann thrombasthenia (GT), first described by Eduard Glanzmann in 1918, is a rare inherited platelet function disorder with an estimated incidence of 1/1,000,000. It is more prevalent in consanguineous marriages, with no gender predilection.1 GT is an autosomal recessive disorder caused by mutations in the ITGA2B or ITGB3 genes located on chromosome 17. The ITGA2B gene encodes the αIIb subunit, while ITGB3 encodes the β3 subunit of the integrin αIIbβ3 complex. Quantitative and/or qualitative defects in this integrin lead to impaired platelet aggregation, delayed or absent clot retraction, and lifelong bleeding tendencies. Common manifestations include mucocutaneous bleeding,2 epistaxis, gingival hemorrhage, and menorrhagia in females. In this case, the patient reported occasional gingival bleeding and cutaneous petechiae, which she neglected to address. Subsequent family analysis in 2022 revealed that the patient carried compound heterozygous pathogenic variants in ITGA2B (chr17:42452041 and chr17:42,457,372), while her parents were carriers. Her husband’s genetic testing confirmed a wild-type genotype.
GT patients typically exhibit normal platelet counts, with dispersed platelets of normal morphology on peripheral blood smears and no clustering. Routine coagulation tests usually show prothrombin time (PT), thrombin time (TT), activated partial thromboplastin time (APTT), and fibrinogen levels remain normal.1 Light transmission aggregometry (LTA), the gold standard for diagnosing GPIIb/IIIa defects, demonstrates markedly reduced or absent platelet aggregation in response to physiological agonists (eg, ADP, arachidonic acid, epinephrine, thrombin), with normal or near-normal responses to ristocetin. Flow cytometry typically reveals reduced CD41 and/or CD61 expression (GPIIb/IIIa), whereas CD42a and CD42b (GPIb/IX/V) are preserved. However, flow cytometry cannot detect qualitative glycoprotein defects in type III GT.1 In this patient, flow cytometry showed CD61: 0%, CD42: 94.36%, and CD41: 0%. Studies by Javed Ahammad et al,3 suggest that TEG parameters–normal platelet count, reduced maximum amplitude (MA), prolonged bleeding time, and elevated bleeding scores–may aid in preliminary GT diagnosis.
There is currently no cure for GT. For minor bleeding, local measures and antifibrinolytic agents are first-line therapies, while platelet transfusions are reserved for life-threatening hemorrhage.4 However, repeated transfusions risk alloimmunization (anti-HLA or anti-αIIbβ3 antibodies), leading to platelet refractoriness.5 Recombinant activated factor VII (rFVIIa) offers an alternative for refractory cases, regardless of antibody status.6,7 Pregnant GT patients face additional risks: fetal-maternal incompatibility (maternal anti-β3 antibodies) may cause neonatal thrombocytopenia and intracranial hemorrhage.6 Regular monitoring for platelet antibodies is critical during pregnancy and postpartum.7 Drawing from fetal-neonatal alloimmune thrombocytopenia (FNAIT) protocols, antenatal intravenous immunoglobulin (IVIG) from 20 weeks gestation8 and serial fetal ultrasound surveillance (starting at 16–18 weeks) are recommended for high-risk pregnancies. In this case, antiplatelet GPIIb/IIIa antibodies were negative at 36+5 weeks, and fetal ultrasound showed no abnormalities. Despite preoperative rFVIIa recommendation, the patient declined due to financial constraints, opting for platelet transfusion instead.
Pregnancy in GT necessitates rigorous preconception evaluation, including: ①Prior hemostatic success with rFVIIa or platelet transfusions. ②Alloimmunization status (anti-αIIbβ3 or anti-HLA antibodies). ③Assessment of bleeding comorbidities (eg, anemia, iron deficiency, dental/nasal health). ④Genetic counseling for consanguineous couples.2 A history of life-threatening postpartum hemorrhage (PPH) or neonatal intracranial hemorrhage contraindicates future pregnancies, while high anti-αIIbβ3 antibody titers warrant pregnancy deferral.
GT patients with planned pregnancies should be followed at a tertiary care referral center with a dedicated multidisciplinary team including a hematologist, maternal-fetal medicine specialist, geneticist, anesthesiologist, neonatal specialist, laboratory specialist, transfusion medicine specialist, psychologist, and pharmacist. Patients should be thoroughly evaluated prior to pregnancy.9 Low-dose aspirin and other antithrombotic agents are contraindicated during pregnancy, including in patients with a history or clinical risk factors for preeclampsia or other placenta-mediated complications.
The timing of delivery should be determined by comprehensive evaluation of platelet function, bleeding symptoms, effectiveness of drug treatment, obstetric complications, fetal maturity and intrauterine conditions, hospital blood supply and comprehensive treatment capacity, and timely delivery. Glanzmann thrombasthenia is not an indication for cesarean section. Because of the risk of neonatal thrombocytopenia and intracerebral hemorrhage, such as vaginal delivery, the use of fetal head suction is prohibited, and forceps delivery is avoided as far as possible. However, severely abnormal fetal heart rates may occur during the second stage of labor when the fetus is in a low or exit-pelvic position, which requires rapid acceleration of delivery to avoid neonatal hypoxic-ischemic encephalopathy. In such difficult situations, instrumental delivery may be less morbid for the mother and newborn than cesarean delivery, and should therefore be considered.10 In this case, due to our lack of clinical experience, the risk of bleeding is extremely high, and the bleeding during cesarean section is more controllable, so the pregnancy was terminated by cesarean section.
Prevention of postpartum hemorrhage at delivery is important, and guidelines recommend administration of rFVIIa 90 ug/kg in combination with antifibrinolytic agents immediately before vaginal delivery and repeated at 2-hour intervals for 3–4 doses,11 platelet transfusion is recommended as an alternative to vaginal delivery of rFVIIa and as first-line prophylaxis of PPH after cesarean delivery.12 Uterine contraction prophylaxis is recommended immediately after delivery.13,14 Several studies have found that intravenous administration of 1g tranexamic acid after cord clamping significantly reduces estimated blood loss, and if bleeding persists after 30 minutes, a further dose of 1 g is recommended.15 In this case, the patient was given uterine contraction drugs and 1 g tranexamic acid immediately after delivery, and blood oozing around the incision during the operation, and 1 therapeutic amount of platelets was transfused again, but the patient and his family refused to be transfused with rFVIIa due to economic reasons.
Given the prevalence of maternal alloimmunization in GT and the severe fetal sequelae, fetal thrombocytopenia should be considered in all women with GT, regardless of prior exposure to platelets or presence of significant alloantibody antibodies in maternal plasma. Therefore, it is currently recommended that all GT women be monitored for alloimmunization during the first trimester and throughout pregnancy.11 For neonates, oral administration of vitamin K is preferable to intramuscular injection after birth. Cord blood platelet counts should be measured, and cranial ultrasound should be considered for all neonates at risk of thrombocytopenia. In this case, the complete blood routine of the neonate was completed after delivery, and there was no obvious abnormality in platelets, there are no bleeding symptoms so far.
Conclusion
This case report demonstrates the successful multidisciplinary management of a pregnant patient with GT caused by biallelic ITGA2B mutations, highlighting the critical role of dynamic TEG-guided platelet transfusion, preoperative MDT coordination (involving obstetrics, hematology, and transfusion medicine), and targeted hemostatic interventions (tranexamic acid, carboprost) in achieving favorable maternal-fetal outcomes despite intraoperative bleeding (900 mL) and postoperative oozing. The case validates TEG as a practical tool for monitoring coagulation improvement (MA: 12 mm → 29.2 mm post-transfusion) in resource-limited settings where rFVIIa is unavailable, while underscoring the necessity of individualized protocols for genetically stratified GT pregnancies to optimize peripartum safety.
Data Sharing Statement
All available information is included in the manuscript.
Ethics Statement
The case report has been reviewed and approved by the Ethics Committee of The Second Hospital of Dalian Medical University for publication.
Acknowledgments
Written informed consent was obtained from the mother for publication of this case report and any accompanying clinical data. Parental consent was additionally provided on behalf of the newborn infant. All information has been anonymized to protect patient privacy, with removal of identifiers including names, hospital numbers, and specific dates. This case report was conducted in compliance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Botero JP, Lee K, Branchford BR, et al. Glanzmann thrombasthenia: genetic basis and clinical correlates. Haematologica. 2020;105(4):888–894. doi:10.3324/haematol.2018.214239
2. Fiore M, Sentilhes L, d’Oiron R. How I manage pregnancy in women with Glanzmann thrombasthenia. Blood. 2022;139:2632–2641. doi:10.1182/blood.2021011595
3. Ahammad J, Kamath A, Shastry S, Chitlur M, Kurien A. Clinico-hematological and thromboelastographic profiles in glanzmann’s thrombasthenia. Blood Coagulation Fibrinolysis. 2020;31:29–34. doi:10.1097/mbc.0000000000000870
4. Grainger JD, Thachil J, Will AM. How we treat the platelet glycoprotein defects; Glanzmann thrombasthenia and Bernard Soulier syndrome in children and adults. Br J Haematol. 2018;182:621–632. doi:10.1111/bjh.15409
5. Fiore M, d’Oiron R, Pillois X, Alessi MC. Anti-α(IIb) β(3) immunization in Glanzmann thrombasthenia: review of literature and treatment recommendations. Br J Haematol. 2018;181:173–182. doi:10.1111/bjh.15087
6. Nurden AT. Acquired antibodies to αIIbβ3 in glanzmann thrombasthenia: from transfusion and pregnancy to bone marrow transplants and beyond. Transf Med Rev. 2018;32:155–164. doi:10.1016/j.tmrv.2018.05.002
7. Poon MC, d’Oiron R. Alloimmunization in congenital deficiencies of platelet surface glycoproteins: focus on glanzmann’s thrombasthenia and bernard-soulier’s syndrome. Semin Thromb Hemost. 2018;44:604–614. doi:10.1055/s-0038-1648233
8. Lieberman L, Greinacher A, Murphy MF, et al. Fetal and neonatal alloimmune thrombocytopenia: recommendations for evidence-based practice, an international approach. Br J Haematol. 2019;185:549–562. doi:10.1111/bjh.15813
9. Rottenstreich A, Coller BS. Pregnancy and childbirth in patients with Glanzmann Thrombasthenia. Br J Haematol. 2024;205:815–818. doi:10.1111/bjh.19528
10. Ducarme G, Hamel J-F, Bouet P-E, et al. Maternal and neonatal morbidity after attempted operative vaginal delivery according to fetal head station. Obstetrics Gynecol. 2015;126(3):521–529. doi:10.1097/aog.0000000000001000
11. Bolton-Maggs PH, Chalmers EA, Collins PW, et al. A review of inherited platelet disorders with guidelines for their management on behalf of the UKHCDO. Br J Haematol. 2006;135:603–633. doi:10.1111/j.1365-2141.2006.06343.x
12. Siddiq S, Clark A, Mumford A. A systematic review of the management and outcomes of pregnancy in Glanzmann thrombasthenia. Haemophilia. 2011;17:e858–869. doi:10.1111/j.1365-2516.2011.02516.x
13. Sentilhes L, Goffinet F, Vayssière C, Deneux-Tharaux C. Comparison of postpartum haemorrhage guidelines: discrepancies underline our lack of knowledge. BJOG. 2017;124:718–722. doi:10.1111/1471-0528.14305
14. Sentilhes L, Winer N, Azria E, et al. Tranexamic acid for the prevention of blood loss after vaginal delivery. New Engl J Med. 2018;379:731–742. doi:10.1056/NEJMoa1800942
15. Shakur H, Roberts I, Fawole B, WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389(10084):2105–2116. doi:10.1016/s0140-6736(17)30638-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.