Back to Journals » Drug Design, Development and Therapy » Volume 20
Perioperative Flurbiprofen Axetil Administration and Acute Kidney Injury After Non-Cardiac Surgery: A Retrospective Cohort Study
Authors Wang S ![]() , Zhong YQ
, Zhong YQ ![]() , Zhao BC, Hou XM, Yin BY, Liu KX
, Zhao BC, Hou XM, Yin BY, Liu KX ![]() , Liu HM
, Liu HM ![]()
Received 21 January 2026
Accepted for publication 15 April 2026
Published 23 April 2026 Volume 2026:20 597928
DOI https://doi.org/10.2147/DDDT.S597928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Shuang Wang,1,2,* Yu-Qi Zhong,3,* Bing-Cheng Zhao,1,2 Xiao-Min Hou,1 Bin-Yan Yin,1 Ke-Xuan Liu,1,2 Hua-Min Liu1,2
1Department of Anesthesiology, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, 510515, People’s Republic of China; 2Guangdong Provincial Key Laboratory of Precision Anesthesia and Perioperative Organ Protection, Guangzhou, Guangdong, 510515, People’s Republic of China; 3Department of Anesthesiology, Weifang People’s Hospital, Weifang, Shandong, 261000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ke-Xuan Liu; Hua-Min Liu, Email [email protected]; [email protected]
Purpose: This study aims to evaluate the impact of different timing of flurbiprofen axetil (FA) administration on postoperative acute kidney injury (AKI) and other adverse events in non-cardiac surgery patients.
Patients and Methods: This retrospective cohort study included 45,062 adult patients undergoing non-cardiac surgery from January 1, 2019, to October 31, 2023. Perioperative FA analgesia records were extracted from electronic medical records. The primary outcome was AKI within 7 days after surgery. Secondary outcomes included postoperative adverse cardiovascular events (ACE), postoperative length of stay (LOS), and in-hospital mortality.
Results: The incidences of AKI, ACE, and mortality were 6.0% (2,683/45,062), 8.5% (3,809/45,062), and 0.1% (48/45,062), respectively. Intraoperative [odds ratio (OR), 0.71; 95% confidence interval (CI), 0.62– 0.82] and postoperative (OR, 0.73; 95% CI, 0.66– 0.79) FA administration was associated with lower odds of AKI compared with non-use. Compared to patients who did not receive FA analgesia at any point, those who received FA both during and post-surgery had a significantly lower odds of AKI (OR, 0.61; 95% CI, 0.51– 0.73). Subgroup analysis indicated a greater reduction in AKI odds for intraoperative FA administration in patients with a high inflammatory status (OR and 95% CI: 0.58 [0.47– 0.72] vs 0.84 [0.59– 1.20], P for interaction = 0.010). Postoperative, but not intraoperative FA administration, was associated with a lower odds of ACE (OR, 0.85; 95% CI, 0.79– 0.91), with this association was significant in patients without preoperative hypertension (OR and 95% CI: 0.81 [0.74– 0.88] vs 0.96 [0.81– 1.13], P for interaction< 0.05). Accelerated failure time model showed that both intraoperative and postoperative FA use was inversely correlated with postoperative LOS.
Conclusion: Perioperative FA analgesia was associated with a lower odds of postoperative AKI and shorter postoperative LOS, whereas only postoperative FA analgesia was linked to a lower odds of postoperative ACE.
Keywords: flurbiprofen axetil, acute kidney injury, adverse cardiovascular events, perioperative analgesia, postoperative complications
Introduction
Postoperative acute kidney injury (AKI) is recognized as a severe complication following surgery, with reported incidence ranging from 6.3% to 7.4% among inpatients undergoing non-cardiac procedures.1,2 AKI significantly increases the risk of adverse clinical outcomes, including prolonged hospitalization, intensive care unit (ICU) admission, progression of chronic kidney disease, and postoperative mortality.3,4 Given its high incidence and severe consequences, identifying modifiable risk factors for AKI is crucial for improving patient outcomes.
Flurbiprofen axetil (FA), a propionic acid-derived non-steroidal anti-inflammatory drug (NSAID), inhibits inflammatory responses and is widely used for postoperative analgesia in non-cardiac surgery.5–7 Despite the long history of use, NSAIDs remain a leading cause of drug-induced kidney injury as reported in prior study.8 Recent study has summarized FA related adverse events, including AKI, nausea and vomiting, and facial edema.9 Besides, several case reports have indicated that FA administration may induce renal papillary necrosis and acute tubulointerstitial nephritis.10,11 However, existing literatures report inconsistent findings regarding the association between FA analgesia and postoperative AKI, regardless of its administration during surgery or via analgesic pump postoperatively. Such as, FA administration following anesthesia induction was associated with a lower risk of postoperative AKI in adult patients undergoing spinal surgery,12 and early postoperative NSAID use did not increase AKI incidence in patients with major gastrointestinal surgery.13 Moreover, animal studies have suggested a renoprotective effect of FA in rats with 5/6 kidney ablation.14,15 These conflicting results highlight the need to clarify the relationship between FA and postoperative renal function in order to prevent drug-related renal injury.
Our previous study identified that inflammation is significantly associated with postoperative AKI.16 Thus, decreasing inflammation may be an approach for FA to lower postoperative AKI odds, suggesting a potential dose–response relationship.5,17 However, study has shown that intraoperative administration of high-dose FA (>250 mg) is associated with an increased risk of postoperative AKI.18 This leads to an important concern, that is, whether the continuous use of FA from intraoperative to postoperative, which resulted in a cumulative dose, is related to postoperative AKI. However, previous studies have predominantly focused on the relationship between AKI and FA use within specific, isolated perioperative period.
Given FA has been routinely used for both intraoperative and postoperative analgesia in clinical practice, this study aims to reveal the association of FA administrated at different perioperative periods on postoperative AKI and other adverse events, including adverse cardiovascular events (ACE), postoperative length of stay (LOS) and in-hospital mortality, in patients undergoing non-cardiac surgery. The timing of FA administration (intraoperative and postoperative periods) was our special attention. We hypothesized that FA analgesia is associated with low odds of postoperative AKI and other adverse outcomes, and its continuous use may further improve prognosis.
Materials and Methods
Study Population and Data Sources
This retrospective cohort study was approved by the institutional ethics committee of Nanfang Hospital, Southern Medical University (NFEC-202311-K33). The requirement for written informed consent was waived due to the retrospective design of the study. All patient data were de-identified and handled in strict compliance with confidentiality requirements. This study was conducted in accordance with the principles of the Declaration of Helsinki. We reviewed 99,969 patients who underwent non-cardiac surgery between January 1st, 2019, and October 31st, 2023. They were excluded if: 1) missed serum creatinine (Scr) measurements before or after surgery within 7 days (52,138); 2) age under 18 years (1,359); 3) underwent transplant surgery, had end-stage renal disease defined as an estimated glomerular filtration rate [eGFR]<15 mL/min/1.73m2, or a history of renal replacement therapy (1,350); 4) American Society of Anesthesiologists (ASA) physical status V or VI (60) (Figure 1). For individuals with multiple eligible surgeries throughout study period, only the first surgery record was retained. Data was obtained from Perioperative Data Warehouse from Department of Anesthesiology. Patient data meeting the inclusion criteria were automatically extracted from the electronic medical record system via our institutional perioperative data warehouse. One investigator (a certified clinical researcher with a Good Clinical Practice [GCP] certificate) designed the extraction algorithm by defining the eligibility criteria and variable specifications within the data warehouse platform. A second investigator (also GCP-certified) independently reviewed the extraction rules for accuracy and completeness prior to final data extraction. To ensure data fidelity, a random sample of 1% (1,000 patients) of the study population underwent manual chart review. Data in this subset were compared against the automatically extracted data by the two investigators. If any discrepancies were identified, the extraction rules were systematically reviewed and corrected. Following rule correction, the entire dataset was re-extracted and subjected to the same validation process.
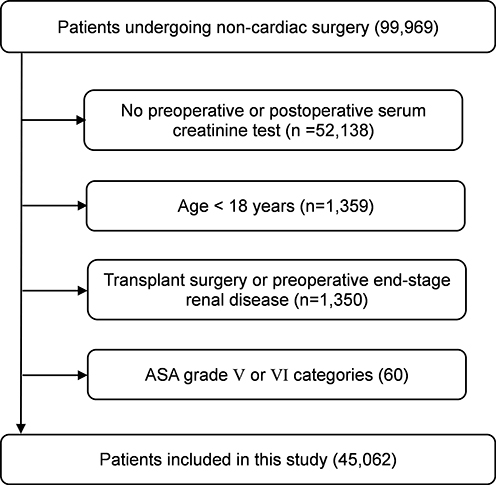 |
Figure 1 Flowchart of patients’ selection. Abbreviations: AKI, acute kidney injury; ACE, adverse cardiovascular events; ASA, American Society of Anesthesiologists. |
Exposure and Covariates
The interested exposure was perioperative FA analgesia, defined as receiving FA formulation, either intraoperative intravenous infusion, or postoperative patient-controlled analgesia (PCA). According to the standardized analgesic protocol at the study hospital, the PCA pump was initiated immediately after surgery. The pump was programmed to deliver a fixed-rate continuous background infusion of FA, while patients could self-administer additional bolus doses as needed for pain control by pressing a button on the pump. The absence of FA formulation record was considered equivalent to non-use, as FA is a prescription medication with mandatory recording. Patients were categorized into intraoperative FA administration and postoperative FA administration. To further clarify cumulative effect from intraoperative to postoperative periods, we subsequently stratified patients into the following four groups according to different timing of FA administration: non-use group (without administration of FA), intraoperative-only group (receiving FA intraoperatively without postoperative administration), postoperative-only group (receiving FA after surgery without intraoperative administration), and both use group (intraoperative and postoperative administration). Additionally, we extracted data of FA dosage to analyze dose–response relationships for intraoperative, postoperative and total cumulative administration.
Covariates potentially influencing development of postoperative AKI were selected based on previous studies or clinical knowledge, covering demographic characteristics, comorbidities, preoperative laboratory tests and surgical factors. Detailed definitions and coding schemes for each covariate were provided in Supplementary Table 1 in Appendix 1 and Appendix 2. We identified preoperative comorbidities using ICD-10 diagnosis codes. To ensure a comprehensive preoperative assessment of comorbidities, the admission records, past medical histories and discharge summaries in the electronic medical records have all been reviewed to supplement potential under-documentation of comorbidities in ICD-10 diagnosis codes. Preoperative laboratory values closest to the date of surgery were selected, with a maximum time window within 7 days. Surgical factors comprised procedure duration, type of surgery, type of anesthesia, intraoperative use of remifentanil and sufentanil.
Outcomes
The primary outcome is the incidence of AKI within the first 7 postoperative days. According to Kidney Disease: Improving Global Outcomes (KDIGO) criteria, AKI was defined as either a ≥26.5 µmol/L increase in Scr within 48 hours postoperatively or a Scr elevation to ≥1.5 times the baseline documented within the 7 postoperative days. AKI severity was classified according to KDIGO criteria: Stage 1, an increase in Scr by ≥26.5 µmol/L within 48 hours, or an increase to ≥1.5–1.9 times baseline; Stage 2, an increase in Scr to 2.0–2.9 times baseline; Stage 3, an increase in Scr to ≥3.0 times baseline, Scr ≥354 µmol/L (with an acute increase of ≥0.3 mg/dL), or initiation of renal replacement therapy.
The secondary outcomes included ACE, postoperative LOS, and in-hospital death. Postoperative ACE onset was determined based on any documented cardiovascular events in the surgical discharge summary, including cardiovascular death, myocardial infarction, pulmonary embolism, atrial fibrillation, cardiac arrest and stroke. In-hospital death was identified by reviewing death medical record system. Postoperative LOS was calculated as the interval between surgery completion and hospital discharge, measured in minutes and then converted to days.
Statistical Analysis
Descriptive Statistics
Patients’ characteristics were summarized among the four groups: the non-use group, the intraoperative-only group, the postoperative-only group, and the both use group. Normality of continuous variables was assessed using the Kolmogorov–Smirnov test and summarized as mean ± SD (normal distribution) or median with IQR (skewed distribution). Categorical variables were presented as number (percentage). Comparisons among groups were performed using one-way ANOVA for normal continuous variables, the Kruskal–Wallis test for skewed continuous variables, and the chi-square test for categorical variables.
Perioperative FA Administration and Primary Outcome
Univariable and multivariable logistic regression analyses were employed to investigate the correlations between FA administration and postoperative AKI. Results were reported as odds ratios (OR) with 95% confidence intervals (CI). Three models were conducted: Model 1 was constructed without adjusting for any covariate. Model 2 was adjusted for age, sex, smoking status, drinking status, diabetic mellitus, hypertension, and cardiac comorbidities. Model 3 was further adjusted for body mass index (BMI), hemoglobin, white blood cell, platelet, serum potassium, calcium, sodium, albumin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), urea, creatinine, procedure duration, ASA status, type of anesthesia, surgery sites, and intraoperative use of remifentanil and sufentanil. To evaluate potential effect modification by inflammatory status, patients were stratified using the INFLA-score19—a composite of four inflammatory biomarkers (including C-reactive protein [CRP], white blood cell count, platelet count, and granulocyte-to-lymphocyte ratio) ranging from –16 to 16, with higher scores indicating greater inflammation (detailed in Supplementary Table 2 in Appendix 1). Participants were dichotomized into high- and low-inflammatory groups based on the cohort median, and a multiplicative interaction term (FA use × INFLA-score category) was included in the regression models. Additional subgroup analyses were performed by sex, age, and preoperative comorbidities (hypertension, diabetes, and cardiac comorbidities). Ordinal logistic regression was also applied to explore the association between FA administration and AKI stages under the proportional odds assumption.
The distribution of FA dose is extremely skewed, as there is no clinically recommended dose in current guidelines, and dosing is instead based on anesthesiologists’ experience. Therefore, in the dose–response relationship analyses, we categorized patients in a data-driven manner according to the actual distribution of FA dose. We modeled the intraoperative, postoperative, and total-dose categories for intra- and postoperative, respectively. After considering the actual dose used in each period and the number of people in each category, the intraoperative dose was categorized into Non-use, 0–50 mg, and ≥50 mg; the postoperative dose and the total dose (intraoperative and postoperative combined) were both categorized into Non-use, 0–100 mg, 101–249 mg, and ≥250 mg, with the Non-use category serving as the reference. The associations of intraoperative, postoperative, and total dose of FA with AKI were modeled separately; trend tests were not performed due to the absence of a strict dose-gradient design.
Perioperative FA Administration and Secondary Outcome
For secondary outcomes, logistic regression models were used to analyze the associations between perioperative FA administration and postoperative ACE. The modeling strategy was consistent with that for the primary outcome, with three models being conducted. Interaction analyses were performed for sex, age, cardiac comorbidities, preoperative hypertension, and diabetes mellitus by introducing multiplicative interaction terms into the logistic regression models. An accelerated failure time model was used to evaluate the association between FA administration and postoperative LOS, with in-hospital death treated as a censoring of discharge alive. The results were presented as time ratios (TRs) with 95% CIs. Specifically, given the limited number of postoperative mortality events, we restricted our analysis to descriptive comparisons using chi-square tests. Patients were grouped simply according to intraoperative or postoperative FA administration, without further adjustment or stratification, to avoid the risk of overfitting associated with multivariable modeling.
Data Processing
Patients with over 30% missing data for any variables were excluded, whereas those with less than 30% missing data were imputed using the random forest method in R software (via the missRanger R package). As this was a retrospective cohort study, all eligible patients who underwent non-cardiac surgery at our institution were included, and no pre-specified sample size estimation was performed. We evaluated the statistical power based on the observed event rates (AKI and ACE) in the final sample using PASS software (version 2021, NCSS, LLC, USA). The achieved statistical power for this study was 1.00 to detect the observed effect at a two-sided significance level of α = 0.05. Data processing and statistical analysis were conducted using R software (version 4.4.3), with two-tailed tests and a statistical significance level at P value ≤0.05.
Results
Baseline Characteristics
Among the 45,062 eligible patients, the mean age was 52 ± 15 years, and 21,679 (48.1%) were females. The incidence of AKI in this study was 6.0% (2,683/45,062), and ACE was 8.5% (3,809/45,062). The distribution of patients across FA groups was as follows: non-use group (20,623, 45.8%), intraoperative-only group (2,374, 5.3%), postoperative-only group (17,497, 38.8%), and both use group (4,568, 10.1%). The characteristics of patients are listed in Table 1. The four groups showed significant differences in alcohol assumption. Preoperative laboratory measurements differed across the four groups except for ALT and Scr. Significant differences were also observed in preoperative hypertension, preoperative diabetes, operation duration, ASA physical status, and type of anesthesia.
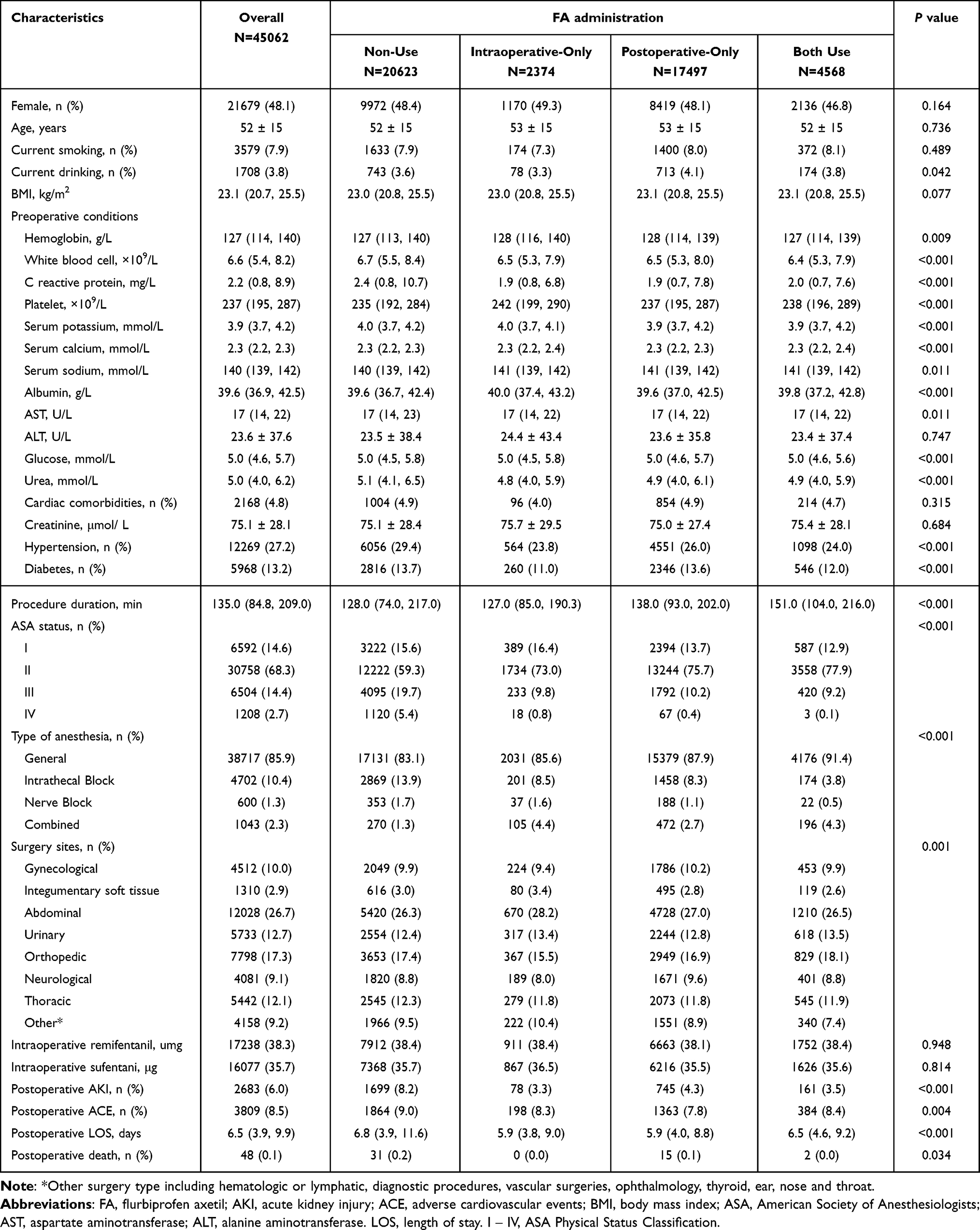 |
Table 1 Baseline Characteristics of Participants in Different Groups of Flurbiprofen Axetil Administration |
FA Administration and AKI
A lower incidence of AKI was observed in patients who received FA either intraoperatively or postoperatively, relative to those who did not receive FA (8.2% vs 3.3‒4.3%, Table 1). Univariate logistic regression analysis showed that both intraoperative FA administration (OR 0.52, 95% CI 0.46‒0.60) and postoperative FA administration (OR 0.51, 95% CI 0.47‒0.56) were associated with lower AKI odds. After adjusted for potential confounders, the associations remained significant (OR 0.71, 95% CI 0.62‒0.82 for intraoperative FA group; OR 0.73, 95% CI 0.66‒0.79 for postoperative FA group). After further dividing FA-treated patients into four groups (ie. non-use, intraoperative-only, postoperative-only, both use), the respective ORs and 95% CIs were 0.62 (0.49‒0.79), 0.72 (0.65‒0.79), 0.61 (0.51‒0.73), respectively, compared with non-use group (Figure 2). In addition, FA administration in any period was negatively associated with AKI stage (Supplementary Table 3 in Appendix1). Further dose–response analyses confirmed a similar trend across all FA dose levels, with the lowest incidence and odds of AKI in the 0–100 mg dose group (Supplementary Table 4 in Appendix1).
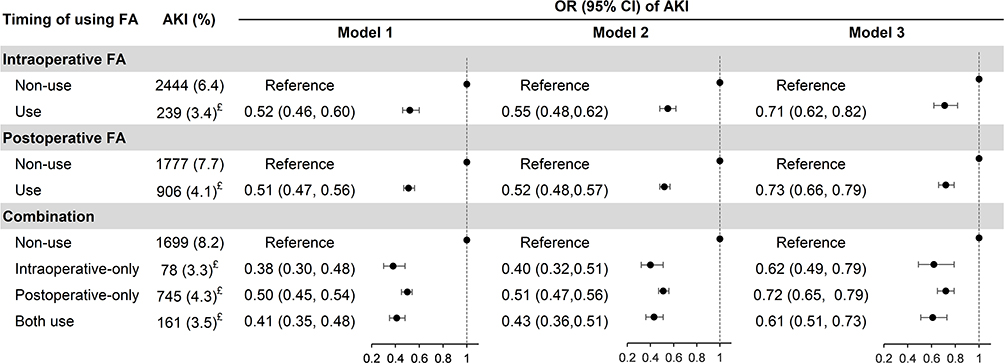 |
Figure 2 Logistic regression analysis for the association between different timing of FA administration and AKI. Model 1: unadjusted model; Model 2: adjusted for age, gender, smoking status, alcohol, diabetes, hypertension, cardiac comorbidities; Model 3: model 2 further adjusted for BMI, hemoglobin, white blood cell, platelet, serum potassium, calcium, sodium, albumin, AST, ALT, urea, creatinine, procedure duration, ASA status, type of anesthesia, surgery sites, and intraoperative use of remifentanil and sufentanil. £The incidence was significantly different compared to the non-use group. Abbreviations: FA, flurbiprofen axetil; AKI, acute kidney injury; OR, odds ratio; CI, confidence interval. |
Subgroup analyses revealed a significant interaction across inflammatory status for FA administration, with a lower AKI odds for intraoperative FA administration in high inflammatory status (interaction P, 0.010, Table 2). Associations were consistent across subgroups stratified by sex, age, and preoperative comorbidities (Supplementary Tables 5−9 in Appendix1).
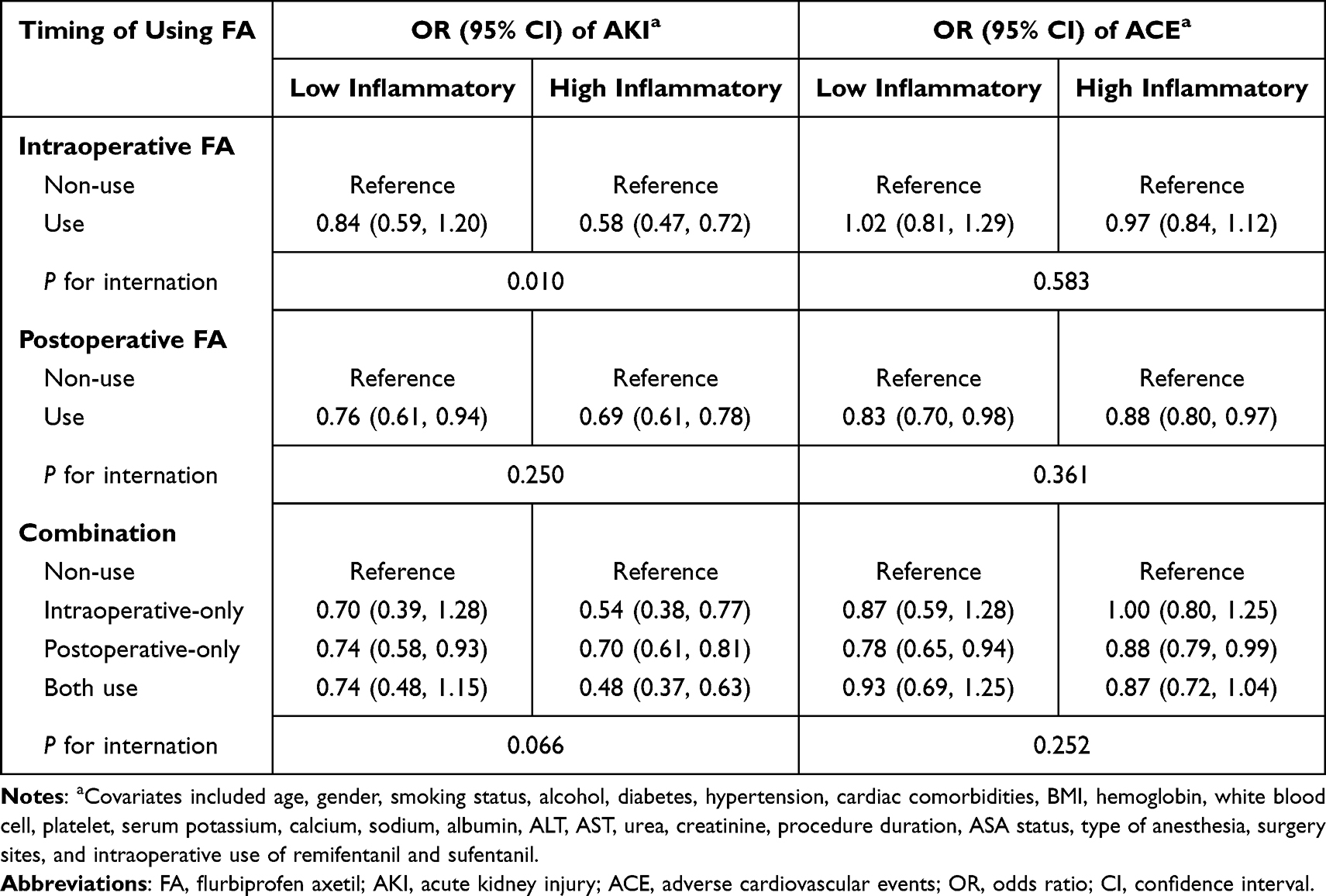 |
Table 2 Subgroup Analysis According to Preoperative Inflammatory Status for the Association Between Different Timing of FA Administration and AKI/ACE |
FA Administration and ACE
The incidence of ACE was higher in patients who did not receive FA (9.0% vs 7.8−8.4, Table 1). Multivariate analysis revealed that postoperative FA administration was associated with a significant lower odds of ACE (OR 0.85, 95% CI 0.79−0.91), while the intraoperative FA administration was not significantly associated with the odds of ACE (OR 1.00, 95% CI 0.91−1.10). Nevertheless, the combined FA administration from intraoperative to postoperative was associated with a lower odds of ACE with an edge significance (OR 0.91, 95% CI 0.80−1.02) (Figure 3). Dose–response relationship analyses showed that increased intraoperative FA dose was not significantly associated with ACE; in contrast, higher postoperative and total FA doses were potentially linked to a lower incidence and lower odds of ACE (Supplementary Table 4 in Appendix1).
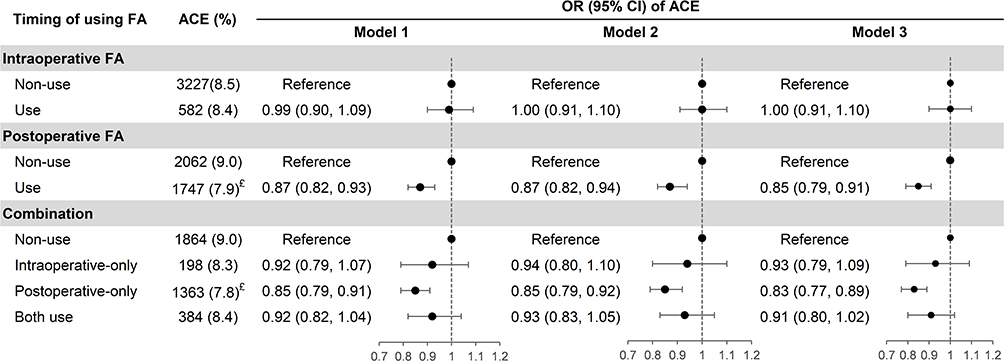 |
Figure 3 Logistic regression analysis for the association between different timing of FA administration and ACE. Model 1: unadjusted model; Model 2: adjusted for age, gender, smoking status, alcohol, diabetes, hypertension, cardiac comorbidities; Model 3: model 2 further adjusted for BMI, hemoglobin, white blood cell, platelet, serum potassium, calcium, sodium, albumin, AST, ALT, urea, creatinine, procedure duration, ASA status, type of anesthesia, surgery sites, and intraoperative use of remifentanil and sufentanil. £The incidence was significantly different compared to the non-use group. Abbreviations: FA, flurbiprofen axetil; OR, odds ratio; CI, confidence interval. |
Inflammatory status, sex, age, preoperative diabetic mellitus and preoperative cardiac comorbidities did not modify the associations (all interaction P > 0.05, Table 2, Supplementary Tables 10−12, Supplementary Table 14 in Appendix1). While in patients without hypertension, postoperative FA administration demonstrated a stronger association with ACE compared to patients with hypertension (interaction P = 0.022, Supplementary Table 13 in Appendix1).
FA Administration and Postoperative LOS and Mortality
We found perioperative FA analgesia in any periods was significantly associated with a shorter postoperative LOS (TR: 0.94, 95% CI: 0.92‒0.97 for intraoperative; TR: 0.93, 95% CI: 0.91‒0.94 for postoperative), with the combined use group experiencing the greatest extent (TR: 0.89, 95% CI: 0.87, 0.92) (Table 3). The intraoperative dose of ≥50 mg was significantly related to the shortening of postoperative LOS by 6% (TR: 0.94, 95% CI: 0.92, 0.96; median LOS: 6.0 vs 6.5 days). The postoperative or total dose of 101‒249 mg exhibited the most extent shortening (around 10%, TR and 95% CI: 0.90 [0.88–0.91] and 0.89 [0.87–0.91]) of postoperative LOS (median: 5.9 vs 6.8 days) compared with non-use group (Supplementary Table 4 in Appendix1).
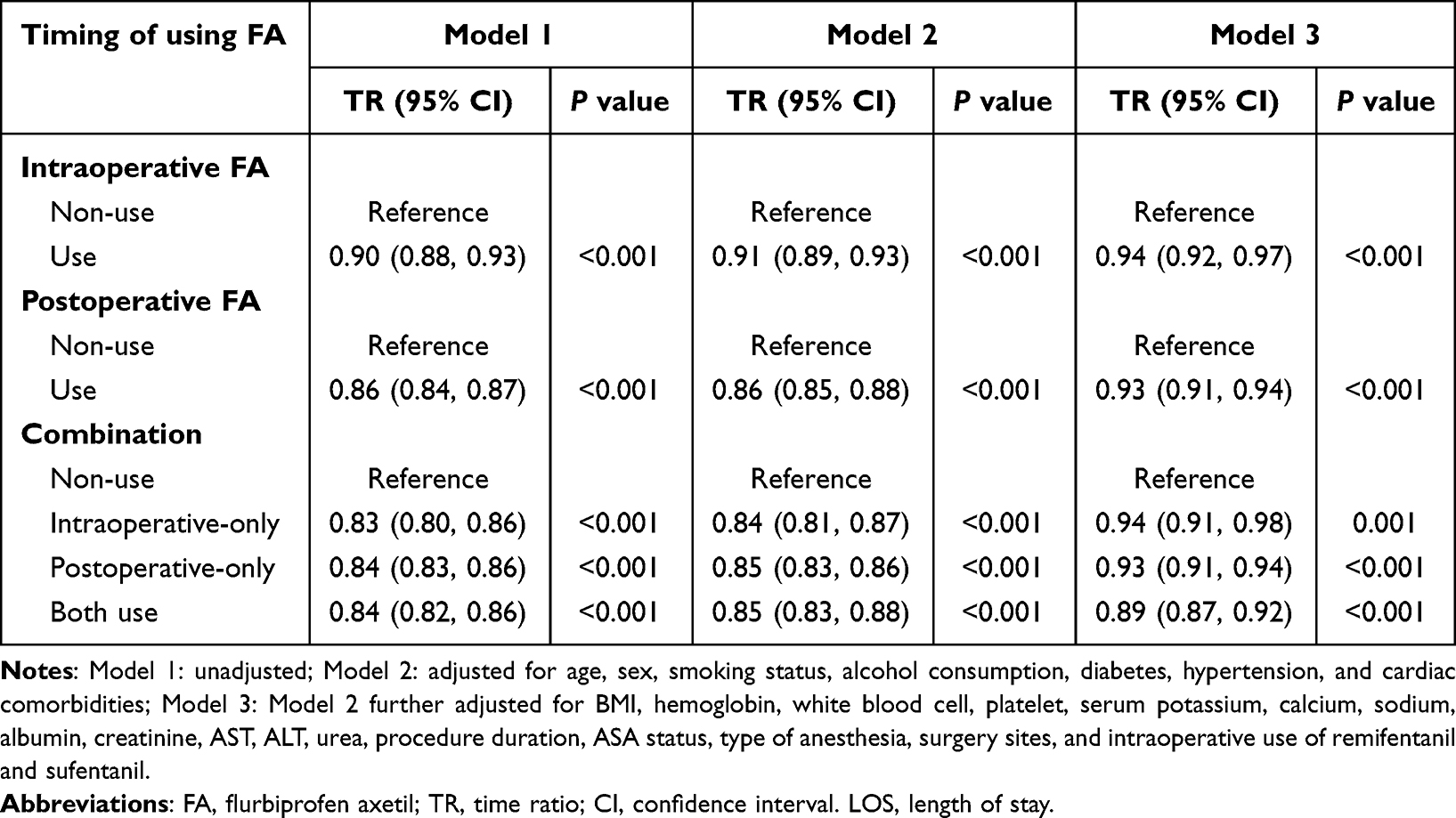 |
Table 3 Accelerated Failure Time Model Between Different Timing of FA Administration and Postoperative LOS |
Chi-square test indicated that the incidence of postoperative death varied significantly between intraoperative FA groups, whereas no significant difference was observed with regard to postoperative FA administration (Supplementary Table 15 in Appendix1).
Discussion
In this large retrospective cohort study of non-cardiac surgery patients, we found that perioperative FA analgesia was associated with a lower odds of AKI. Notably, intraoperative FA administration conferred a greater reduction in AKI occurrence among patients with a high preoperative inflammatory state. Furthermore, postoperative FA administration was linked to a lower odds of ACE, but the correlation extent was attenuated in patients with comorbid hypertension. In addition, FA analgesia in any periods was associated with shortened postoperative LOS.
The association of NSAIDs with AKI has been examined. For instance, Gomelsky et al reported that NSAIDs increased the odds of AKI,20 while Kaufhold et al described a case of acute tubulointerstitial nephritis associated with FA11 On the contrary, a recent retrospective study revealed that intraoperative FA administration is associated with a reduced risk of postoperative AKI in adult patients undergoing spinal surgery.12 The limited sample size in previous studies restricted covariate adjustment in regression models, thereby compromising the ability to adequately control for potential confounding factors. Our study extends the investigation to a large sample size of over 40,000 non-cardiac surgical patients, offering sufficient statistical power to adjust for an extensive set of confounders, and provide more robust evidence for clinical practice.
This study focused on different FA administration periods that may influence renal function—a topic that remains relatively underexplored in non-cardiac surgical settings. We demonstrated the negative association of FA, either intraoperative or postoperative, with postoperative AKI. This exploration is grounded in the routine clinical use of FA during the perioperative period. FA has been widely used as a background analgesic in clinical practice and various randomized controlled trials,21–24 yet its postoperative complications remained rarely studied. In addition, FA serves as an important component of multimodal analgesia strategy, and could provide an excellent analgesia effect, such as, mild pain, low incidences of gastrointestinal symptoms and postoperative cognitive impairment, and decreased opioid drug consumption, when combined with other analgesics.25–28 We additionally provided the evidence that continuous FA analgesia from intra- to postoperative was associated with lower odds of AKI. A study in non-cardiac surgery patients reported a U-shape relationship between intraoperative FA dose and AKI,18 which was similar with our results. Although our findings indicated that higher doses of FA were not associated with an increased odds of AKI, the magnitude of odds reduction was attenuated compared with lower FA doses. Nevertheless, the negative association of high dose FA with AKI remain significant.
Surgical stimuli contribute to a systemic inflammatory response, which may adversely affect renal function.18 While FA acts through the inhibition of cyclooxygenase enzyme to suppress prostaglandins synthesis, attenuating the pro-inflammatory effect related to prostaglandins, thereby potentially mitigating the adverse impact of surgical stress on postoperative outcomes.5,7,26,29,30 Further evidence lie in the targeted delivery of FA via lipid microspheres to surgical incisions and inflammatory sites, that can reduce its direct impact on kidney.26 We further conducted several subgroup analyses to better understand how FA influences postoperative AKI across patients with different health statuses. Our study confirmed a stronger association between intraoperative FA administration and AKI in patients with high inflammatory status. This effect may be attributed to the enhanced anti-inflammation efficacy under high inflammatory conditions.
Beyond its anti-inflammatory effects, the potential impact of FA on the kidney, as an NSAID, also involves its classic hemodynamic effects—a mechanism of particular importance in the perioperative context. FA inhibits the synthesis of prostaglandin, thereby interfering with the compensatory vasodilatory mechanism, which may cause hemodynamically mediated acute kidney injury.31 Animal studies have confirmed that NSAID use resulted in significant reductions in renal blood flow.32 However, in a randomized controlled trial, preoperative administration of FA did not significantly alter mean arterial pressure or heart rate during the perioperative period,33 and another study has shown that NSAID did not significantly reduce renal blood flow or glomerular filtration rate.34 These inconsistent findings drive further research to clarify the mechanism of FA on organ injury. Nevertheless, in the surgical context, we can understand the positive association of FA on renal function from several aspects. First, the inhibition of vasodilation by FA can prevent sudden changes in renal blood flow volume in the postoperative scene, thus maintaining hemodynamic stability and buffering the renal ischemia-reperfusion injury.35,36 Second, FA can ameliorate hemodynamic abnormalities induced by surgery and pain through activation of the renin-angiotensin system.37,38 In addition, prostaglandins participate in the inflammatory response. The inhibition of prostaglandins by FA may therefore reduce the inflammatory response. The above evidence suggests that FA-induced prostaglandins reduction does not invariably lead to clinically significant hemodynamic abnormalities or significant renal hypoperfusion. The ultimate renal outcome likely results from a comprehensive balance between its anti-inflammatory properties and hemodynamic effects.
In addition to the anti-inflammatory effects and hemodynamic modulation discussed above, certain clinical factors may also influence the association between perioperative FA use and postoperative outcomes. To address this concern, we implemented several measures to minimize potential confounding bias in our study. First, to address confounding by indication—ie, the possibility that clinicians might avoid NSAIDs in patients with preexisting renal dysfunction—we excluded patients with severe renal impairment and adjusted for preoperative serum creatinine in the multivariable models. Other common comorbidities and ASA classification were also included to account for baseline health status. Second, to account for differences in surgical intensity, we adjusted for the type of surgery in the regression models. Collectively, these design features and analytical adjustments substantially reduce the risk of residual confounding and strengthen the validity of our findings.
Previous studies have indicated that NSAIDs may increase the odds of cardiovascular events.39 Trelle et al’s network meta-analysis reported high odds of various cardiovascular events related to NSAIDs, including myocardial infarction, stroke, cardiovascular death40 The finding was soon supported by another meta-analysis confirming the positive association of NSAIDs with vascular and upper gastrointestinal complications41 The aforementioned studies encompassed all patients requiring anti-inflammatory therapy. However, in older patients undergoing non-cardiac surgery, Komatsu et al did not find a significant association between NSAIDs and cardiovascular complications.42 While we observed a significant negative association between postoperative FA analgesia via analgesic pump and postoperative ACE. Our study specifically focused on FA, one of commonly used NSAIDs, and we studied non-cardiac surgical patients, which may account for the inconsistent findings in previous literature. Nevertheless, we did not observe a significant association between intraoperative FA analgesia and postoperative ACE, a finding consistent with the study by Komatsu et al.42 Our study utilized a substantially larger sample size of 3809 ACE cases, extending beyond the 60 cases reported by Komatsu et al. The inconsistent associations of intraoperative FA analgesia with AKI and ACE may be attributed to the distinct pathophysiological mechanisms. In addition, we found an attenuated association between postoperative FA and ACE in patients with hypertension. This may be attributed to the shared pharmacological mechanism between NSAIDs and hypertension, such as vasoconstriction and sodium/water retention.43
Our study was conducted based on the two core analytical strategies—stratified by the timing of FA administration and grouped by patient baseline characteristics. By clarifying the impact of different perioperative administration windows on postoperative complications, this research offers an evidence-based reference for optimizing FA administration. Furthermore, heterogeneity analyses across populations with different clinical characteristics provide a theoretical foundation for the individualized use of FA. Nevertheless, these clinical implications require validation through prospective study. Our study has several limitations. First, postoperative AKI was defined exclusively based on changes in Scr measurement, owing to the absence of postoperative urine output data. Although this criterion is widely used in retrospective studies, it may lead to an underestimation of the actual incidence of AKI. Second, the lack of postoperative inflammatory cytokines data limited direct exploration of FA’s anti-inflammatory mechanism on renal protection. However, we indirectly explored this pathway by analyzing how preoperative inflammatory status modifies the association between FA and postoperative AKI. Third, our study lacked systematic assessment of postoperative pain, thereby precluding direct verification of the causal pathway linking analgesia to postoperative outcomes. Fourth, the small number of mortality events precluded multivariate logistic regression analysis. Accordingly, we performed only exploratory descriptive analyses, and the observed event rates were consistent with those reported in previous studies, underscoring the need for future investigations in larger cohorts. Finally, this single-center retrospective cohort study limited the generalization of the conclusion and causal inference.
Conclusions
Our study demonstrated that FA administration, whether intraoperatively or postoperatively, was associated with a lower odds of AKI. Preoperative inflammatory status may modify the association between perioperative FA use and AKI. Furthermore, postoperative FA analgesia was linked to a lower odds of ACE. Future prospective studies are needed to explore the causality between FA administration and postoperative outcomes, especially the timing of administration, and thereby providing evidence for confirmatory clinical strategies.
Abbreviations
ACE, adverse cardiovascular events; AKI, acute kidney injury; ALT, alanine aminotransferase; ASA, American Society of Anesthesiologists; AST, aspartate aminotransferase; BMI, body mass index; CI, confidence interval; eGFR, estimated glomerular filtration rate; FA, flurbiprofen axetil; KDIGO, Kidney Disease: Improving Global Outcomes; ICU, intensive care unit; LOS, length of stay; NSAIDs, non-steroidal anti-inflammatory drugs; OR, odds ratio.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Key Research and Development Program of China [2023YFC2506900], National Natural Science Foundation of China (82504493), Bethune Charitable Foundation (bnmr-2023-001), and Science and Technology Projects in Guangzhou (2024A04J5217).
Disclosure
All authors declare no competing interests in this work.
References
1. Walsh M, Devereaux PJ, Garg AX, et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology. 2013;119(3):507–12. doi:10.1097/ALN.0b013e3182a10e26
2. Sun LY, Wijeysundera DN, Tait GA, Beattie WS. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology. 2015;123(3):515–523. doi:10.1097/ALN.0000000000000765
3. Heung M, Steffick DE, Zivin K, et al. Acute kidney injury recovery pattern and subsequent risk of CKD: an analysis of veterans health administration data. Am J Kidney Dis. 2016;67(5):742–752. doi:10.1053/j.ajkd.2015.10.019
4. Shan X, Littlejohn JE, Peng K, Ji F, Liu H. The effect of perioperative AKI on surgical outcomes. Anesthesiol Perioper Sci. 2023;1(4):28. doi:10.1007/s44254-023-00032-4
5. Geng W, Hong W, Wang J, et al. Flurbiprofen axetil enhances analgesic effects of sufentanil and attenuates postoperative emergence agitation and systemic proinflammation in patients undergoing tangential excision surgery. Mediators Inflamm. 2015;2015:601083 doi:10.1155/2015/601083.
6. Esme H, Kesli R, Apiliogullari B, Duran FM, Yoldas B. Effects of flurbiprofen on CRP, TNF-α, IL-6, and postoperative pain of thoracotomy. Int J Med Sci. 2011;8(3):216–221. doi:10.7150/ijms.8.216
7. Zhou ZJ, Tang J, Li WH, Tao WD. Preoperative intravenous flurbiprofen reduces postoperative pain and inflammatory cytokines in elderly patients after Hip arthroplasty. Exp Ther Med. 2019;17(1):354–358 doi:10.3892/etm.2018.6911.
8. Otsuka N, Yataba I, Matsushita I, Matsumoto H, Hoshino Y, Terada Y. A minimal impact of long-term S-flurbiprofen plaster application on kidney function in osteoarthritis patients. Clin Exp Nephrol. 2017;21(6):1060–1067 doi:10.1007/s10157-017-1406-9.
9. Yang C, Guo Q, Cheng Y, Liu F, Zhang H, Wang H. In-depth summary of adverse events associated with Flurbiprofen: a real-world pharmacovigilance study from 2004 to 2024 using the FAERS database. PLoS One. 2025;20(8):e0329636 doi:10.1371/journal.pone.
10. Colomé Nafría E, Solans R, Espinach J, Delgadillo J, Fonollosa V. Renal papillary necrosis induced by flurbiprofen. DICP. 1991;25(7–8):870–871. doi:10.1177/106002809102500731
11. Kaufhold J, Wilkowski M, McCabe K. Flurbiprofen-associated acute tubulointerstitial nephritis. Am J Nephrol. 1991;11(2):144–146. doi:10.1159/000168291
12. Liu Y, Li B, Hang L, Zhang L. Association between perioperative flurbiprofen administration and acute kidney injury (AKI) in spine surgery: a retrospective cohort study. Perioper Med. 2024;13(1):59. doi:10.1186/s13741-024-00419-2
13. STARSurg Collaborative. Perioperative Nonsteroidal Anti-inflammatory Drugs (NSAID) Administration and Acute Kidney Injury (AKI) in major gastrointestinal surgery: a prospective, multicenter, propensity matched cohort study. Ann Surg. 2022;275(5):904–910. doi:10.1097/SLA.0000000000004314
14. Fujihara CK, Malheiros DM, Donato JL, Poli A, De Nucci G, Zatz R. Nitroflurbiprofen, a new nonsteroidal anti-inflammatory, ameliorates structural injury in the remnant kidney. Am J Physiol. 1998;274(3):F573–F579 doi:10.1152/ajprenal.1998.274.3.F573.
15. Gonçalves AR, Fujihara CK, Mattar AL, et al. Renal expression of COX-2, ANG II, and AT1 receptor in remnant kidney: strong renoprotection by therapy with losartan and a nonsteroidal anti-inflammatory. Am J Physiol Renal Physiol. 2004;286(5):F945–F954. doi:10.1152/ajprenal.00238.2003
16. Yan YT, Liu R, Liu J, et al. Correlation of novel inflammation index with postoperative acute kidney injury in patients with joint arthroplasty: a retrospective cohort study. J Inflamm Res. 2025;18:6091–6102. doi:10.2147/JIR.S512306
17. Li M, Zhang K, Li T, et al. Sciatic nerve block combined with flurbiprofen inhibits spinal cord inflammation and improves postoperative pain in rats with plantar incision. J Pain Res. 2023;16:1533–1546. doi:10.2147/JPR.S404226
18. Wang D, Yang SK, Zhao MX, et al. Low dose of flurbiprofen axetil decrease the rate of acute kidney injury after operation: a retrospective clinical data analysis of 9915 cases. BMC Nephrol. 2020;21(1):52. doi:10.1186/s12882-020-1711-5
19. Pounis G, Bonaccio M, Di Castelnuovo A, et al. Polyphenol intake is associated with low-grade inflammation, using a novel data analysis from the Moli-sani study. Thromb Haemost. 2016;115(2):344–352 doi:10.1160/TH15-06-0487.
20. Ungprasert P, Cheungpasitporn W, Crowson CS, Matteson EL. Individual non-steroidal anti-inflammatory drugs and risk of acute kidney injury: a systematic review and meta-analysis of observational studies. Eur J Intern Med. 2015;26(4):285–291. doi:10.1016/j.ejim.2015.03.008
21. Feng CD, Xu Y, Chen S, et al. Opioid-free anaesthesia reduces postoperative nausea and vomiting after thoracoscopic lung resection: a randomised controlled trial. Br J Anaesth. 2024;132(2):267–276. doi:10.1016/j.bja.2023.11.008
22. Ye Z, Zhu Y, Zhang R, Wang Y, Huang J, Gan X. Effect of multimodal preemptive analgesia of flurbiprofen axetil, nalbuphine, and retrobulbar block on postoperative pain and enhanced recovery in patients undergoing oculoplastic day surgery: a prospective, randomized, double-blinded study. Ophthalmic Plast Reconstr Surg. 2023;39(3):260–265. doi:10.1097/IOP.0000000000002308
23. Zhou J, Pu Q, Lin L, et al. Effect of patient-controlled intravenous analgesia combined with flurbiprofen axetil and dezocine on postoperative analgesia for lobectomy (EPIC-FAD): a trial protocol. Trials. 2021;22(1):175. doi:10.1186/s13063-021-05108-9
24. Kianian S, Bansal J, Lee C, et al. Perioperative multimodal analgesia: a review of efficacy and safety of the treatment options. Anesthesiol Perioper Sci. 2024;2(1):9 doi:10.1007/s44254-023-00043-1.
25. Wei X, Wang Z, Chen Y, et al. Administration of flurbiprofen axetil and dezocine for the postoperative analgesia in patients with non‑small cell lung cancer: a randomized, controlled study. Oncol Lett. 2024;28(1):294. doi:10.3892/ol.2024.14426
26. Lin X, Zhang R, Xing J, Gao X, Chang P, Li W. Flurbiprofen axetil reduces postoperative sufentanil consumption and enhances postoperative analgesic effects in patients with colorectal cancer surgery. Int J Clin Exp Med. 2014;7(12):4887–4896.
27. Sun M, Cong X, Chang E, Miao M, Zhang J. Efficacy of flurbiprofen for postoperative pain in chinese surgical patients: a meta-analysis. J Surg Res. 2020;252:80–88. doi:10.1016/j.jss.2019.11.032
28. Wang Q, Yan XQ, Ma XM, et al. Multimodal analgesia in cardiac surgery: impact on postoperative medication consumption and cognitive function. World J Cardiol. 2025;17(5):103168. doi:10.4330/wjc.v17.i5.103168
29. Takada M, Fukusaki M, Terao Y, et al. Preadministration of flurbiprofen suppresses prostaglandin production and postoperative pain in orthopedic patients undergoing tourniquet inflation. J Clin Anesth. 2007;19(2):97–100. doi:10.1016/j.jclinane.2006.05.028
30. Ashraf Z, Alamgeer, Kanwal M, et al. Flurbiprofen–antioxidant mutual prodrugs as safer nonsteroidal anti-inflammatory drugs: synthesis, pharmacological investigation, and computational molecular modeling. Drug Des Devel Ther. 2016;10:2401–2419. doi:10.2147/DDDT.S109318
31. Lucas GNC, Leitão ACC, Alencar RL, Xavier RMF, Daher EF, Silva Junior GBD. Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. J Bras Nefrol. 2019;41(1):124–130. doi:10.1590/2175-8239-jbn-2018-0107
32. Arpacı H, Çomu FM, Küçük A, et al. Effects of lornoxicam and intravenous ibuprofen on erythrocyte deformability and hepatic and renal blood flow in rats. Drug Des Devel Ther. 2016;10:2477–2481. doi:10.2147/DDDT.S113806
33. Zhao Y, Mu H, Zhang J, Lu Y. Efficacy and safety of flurbiprofen‑axetil combined with nalbuphine pretreatment on remifentanil‑induced postoperative hyperalgesia: a randomized clinical trial. Exp Ther Med. 2023;26(4):475. doi:10.3892/etm.2023.12174
34. Fredman B, Zohar E, Golan E, Tillinger M, Bernheim J, Jedeikin R. Diclofenac does not decrease renal blood flow or glomerular filtration in elderly patients undergoing orthopedic surgery. Anesth Analg. 1999;88(1):149–154. doi:10.1097/00000539-199901000-00028
35. Fu H, Chen H, Wang C, et al. Flurbiprofen, a cyclooxygenase inhibitor, protects mice from hepatic ischemia/reperfusion injury by inhibiting GSK-3β signaling and mitochondrial permeability transition. Mol Med. 2012;18(1):1128–1135 doi:10.2119/molmed.2012.00088.
36. Takada M, Taruishi C, Sudani T, Suzuki A, Iida H. Intravenous flurbiprofen axetil can stabilize the hemodynamic instability due to mesenteric traction syndrome--evaluation with continuous measurement of the systemic vascular resistance index using a FloTrac® sensor. J Cardiothorac Vasc Anesth. 2013;27(4):696–702 doi:10.1053/j.jvca.2012.11.019.
37. Sear JW. Kidney dysfunction in the postoperative period. Br J Anaesth. 2005;95(1):20–32 doi:10.1093/bja/aei018.
38. Carmichael P, Carmichael AR. Acute renal failure in the surgical setting. ANZ J Surg. 2003;73(3):144–153. doi:10.1046/j.1445-2197.2003.02640.x
39. Dean L. Flurbiprofen Therapy and CYP2C9 Genotype. In: Pratt VM, Scott SA, Pirmohamed M, Esquivel B, Kattman BL, Malheiro AJ, editors. Medical Genetics Summaries. Bethesda (MD): National Center for Biotechnology Information (US); 2019.
40. Trelle S, Reichenbach S, Wandel S, et al. Cardiovascular safety of non-steroidal anti-inflammatory drugs: network meta-analysis. BMJ. 2011;342():c7086. doi:10.1136/bmj.c7086
41. Bhala N, Emberson J, Merhi A, et al; Coxib and traditional NSAID Trialists’ (CNT) Collaboration. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet. 2013;382(9894):769–779 doi:10.1016/S0140-6736(13)60900-9.
42. Komatsu R, Singleton MD, Dinges EM, Wu J, Bollag LA. Association between perioperative non-steroidal anti-inflammatory drug use and cardiovascular complications after non-cardiac surgery in older adult patients. JA Clin Rep. 2024;10(1):29. doi:10.1186/s40981-024-00712-5
43. Kim S, Joo KW. Electrolyte and Acid-base disturbances associated with non-steroidal anti-inflammatory drugs. Electrolyte Blood Press. 2007;5(2):116–125. doi:10.5049/EBP.2007.5.2.116
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dexmedetomidine May Reduce the Incidence of Acute Kidney Injury in Elderly Patients Undergoing Orthopedic Surgery: A Randomized, Double-Blind Clinical Trial
Zheng XY, Su Z, Zhang Y, Yan J, Li XY, Peng K, Liu H, Shan XS, Ji FH
Drug Design, Development and Therapy 2026, 20:571990
Published Date: 20 February 2026