Back to Journals » Drug Design, Development and Therapy » Volume 20
Perioperative EGFR-Targeted Therapy in Resectable EGFR-Mutated NSCLC: A Narrative Review from Drug Design to Pain-Informed MRD-Guided Care
Authors Xiong L ![]() , Yang X, Yuan H, Qin L, Lin B, Chen F, Wen Y
, Yang X, Yuan H, Qin L, Lin B, Chen F, Wen Y ![]()
Received 8 December 2025
Accepted for publication 31 January 2026
Published 7 March 2026 Volume 2026:20 587428
DOI https://doi.org/10.2147/DDDT.S587428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Lile Xiong,1 Xiufen Yang,2 Hua Yuan,1 Lan Qin,3 Binghu Lin,1 Fengjiao Chen,1 Yi Wen1
1Department of Thoracic Surgery, Shenzhen People’s Hospital, Shenzhen, Guangdong, People’s Republic of China; 2Department of Emergency, Shenzhen People’s Hospital, Shenzhen, Guangdong, People’s Republic of China; 3Department of Nursing, Shenzhen People’s Hospital, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Yi Wen, Email [email protected]
Abstract: Perioperative EGFR-targeted therapy has transformed the management of resectable EGFR-mutated NSCLC. However, prolonged exposure introduces chronic toxicity and pain that may erode long-term benefit. This narrative review synthesizes evidence from pivotal perioperative EGFR-TKI trials, emerging fourth-generation EGFR-TKIs, and studies on pain, toxicity, adherence, and patient-reported outcomes, with a focus on minimal residual disease (MRD)-guided treatment adaptation. Current data show that adjuvant and neoadjuvant EGFR-TKIs substantially reduce recurrence and may improve survival, yet pain and related functional impairment remain under-recognized, under-measured, and inconsistently managed. Procedure-related and treatment-emergent pain, neuropathy, and musculoskeletal symptoms interact with psychological, comorbid, and social factors to undermine adherence, particularly during prolonged adjuvant therapy. Fourth-generation EGFR-TKIs and MRD-guided strategies create opportunities to optimize exposure and duration but demand structured monitoring of pain, standardized electronic patient-reported outcomes, and integrated oncology–anesthesiology–palliative care pathways. We propose an efficacy–safety–pain–adherence loop in which pain is treated as a core determinant of therapeutic success, aiming to maximise cure potential while preserving quality of life.
Plain Language Summary: Many people with early-stage non–small cell lung cancer (NSCLC) can have surgery to remove the tumour. Even after a “complete” resection, however, the cancer often comes back. For patients whose tumours have changes in a gene called EGFR, tablets known as EGFR tyrosine kinase inhibitors (EGFR-TKIs) are now used before or after surgery to lower the risk of the cancer returning. These targeted drugs can keep the disease under control for longer, but they are taken for many months or years and can cause ongoing side effects such as skin problems, diarrhoea, nail changes, and muscle or nerve pain. Lung surgery itself may also lead to long-lasting pain in the chest and shoulder.
In this review, we explain how EGFR-TKIs are designed, how they are used around the time of surgery, and how they affect pain, daily activities, and patients’ ability or willingness to keep taking treatment. We also describe blood tests that can detect tiny amounts of cancer DNA—called minimal residual disease—and electronic tools that let patients report symptoms from home.
Based on these data, we suggest a practical approach in which doctors and nurses monitor pain and other symptoms regularly, combine this information with blood test results, and adjust the dose and duration of EGFR-TKIs when needed. The goal is to give patients the best chance of being cured while protecting their comfort, function, and overall quality of life.
Keywords: EGFR-mutated NSCLC, perioperative targeted therapy, fourth-generation EGFR-TKI, pain management, patient-reported outcomes
Introduction
Evolving Perioperative Treatment Landscape in Resectable NSCLC and the Rise of Targeted Therapy
Lung cancer—predominantly non-small cell lung cancer (NSCLC)—remains the leading cause of cancer-related mortality worldwide,1 although a proportion of patients present with early-stage or locally advanced disease that is resectable.2 For decades, anatomical resection followed by adjuvant platinum-based chemotherapy has been standard, yet the absolute survival benefit is modest (≈5% at 5 years) and 25–70% of patients relapse despite complete resection.3,4
The success of targeted agents in advanced oncogene-driven NSCLC has led to their evaluation in the curative-intent setting, with EGFR-mutated disease providing the most mature example. The Phase III ADAURA trial established adjuvant osimertinib as a standard of care, showing marked improvements in disease-free and overall survival for completely resected stage IB–IIIA EGFR-mutated NSCLC.5 Similar perioperative immunotherapy trials further support the value of systemic therapy around surgery.6,7 Collectively, these advances are reshaping perioperative management toward biomarker-guided multimodality care. However, most trials prioritise radiologic or pathologic outcomes, while perioperative pain, symptom burden and functional recovery—key determinants of real-world benefit—receive far less attention. Incorporating targeted agents into the perioperative window therefore introduces additional considerations for tolerability and symptom control—particularly postoperative pain—that are not fully addressed in current paradigms.
Perioperative Pain Burden and Chronic Postsurgical Pain in Lung Cancer Surgery
Thoracic surgery is associated with intense acute postoperative pain and a high incidence of chronic postsurgical pain (CPSP), often neuropathic and disabling.8 CPSP occurs in about 40–60% of patients after thoracotomy and 20–30% after video-assisted thoracoscopic surgery, driven by intercostal nerve injury, peri-incisional inflammation and central sensitisation.9 Psychological factors and social context further modulate pain experience, supporting multimodal, multidisciplinary management strategies. In patients receiving perioperative systemic therapy, this vulnerability to pain may interact with treatment-related toxicities such as musculoskeletal or neuropathic symptoms. Overlapping burdens influence adherence, dose intensity, rehabilitation, sleep and physical activity, ultimately shaping the effectiveness of perioperative regimens; pain is therefore not merely a postoperative complication but a key modifier of perioperative targeted therapy.
Next-Generation EGFR-TKIs and MRD-Guided Strategies: Opportunities and Challenges in the Perioperative Setting
Next-generation EGFR tyrosine kinase inhibitors (TKIs) have been designed to overcome atypical and acquired resistance and extend benefit beyond common sensitising mutations. Sunvozertinib (DZD9008), for example, selectively targets EGFR exon 20 insertion mutations and has shown durable responses with a manageable safety profile in platinum-pretreated advanced NSCLC, supporting accelerated regulatory approval.10–12 Although current evidence derives from advanced disease, such “fourth-generation” agents are plausible candidates for perioperative trials in biomarker-selected resectable NSCLC and raise specific questions regarding pharmacokinetics under surgical stress, overlapping toxicities with postoperative symptoms and interactions with acute and chronic pain syndromes.Circulating tumour DNA (ctDNA)–based minimal residual disease (MRD) assays are refining postoperative risk stratification: postoperative ctDNA positivity predicts substantially higher recurrence risk, whereas ctDNA clearance correlates with improved survival.13–15 Integrating MRD status with functional and symptom endpoints—including pain and patient-reported outcomes—may enable perioperative decision-making that better balances oncologic control against toxicity and pain burden.
Central Role of Pain and Symptom Management in Treatment Adherence, Quality of Life and Long-Term Outcomes
For oral targeted therapies around surgery, adherence and persistence are critical determinants of real-world effectiveness. Observational studies show suboptimal adherence to EGFR- or ALK-directed agents, influenced by dosing schedules, treatment duration and toxicity profiles.16 Educational and behavioural interventions can improve adherence,17 while electronic patient-reported outcome (ePRO) monitoring reduces symptom burden and enhances quality of life.18 Given the high prevalence of surgical and neuropathic pain, together with TKI-associated musculoskeletal, dermatologic and other adverse events, pain and symptom management are central—not ancillary—to maintaining dose intensity and achieving the intended oncologic benefit. Uncontrolled pain or cumulative symptoms drive dose reductions, interruptions and early discontinuation and contribute to psychological distress and functional decline. Across studies of oral anticancer agents, higher symptom burden—particularly pain and fatigue—has been consistently associated with missed doses and early discontinuation, highlighting pain control as a modifiable determinant of adherence.
Multidisciplinary Clinical and Nursing Collaboration in Perioperative Targeted Therapy and Pain Management
Perioperative care for resectable NSCLC spans surgery, systemic therapy, pain control, rehabilitation and survivorship, and requires coordination among thoracic surgeons, medical oncologists, anaesthesiologists, pain specialists, rehabilitation teams and oncology nurses. Multidisciplinary pathways that align treatment scheduling with multimodal analgesia, early mobilisation and psychosocial support are key to optimising oncologic and pain-related outcomes. Oncology nurses play pivotal roles in serial pain assessment, implementation of ePRO or symptom diaries, patient education and identification of individuals with psychological vulnerability or pre-existing chronic pain.
Objectives of This Narrative Review
This narrative review focuses on perioperative targeted therapy in resectable NSCLC, with an emphasis on EGFR-directed TKIs. Its objectives are to integrate evidence from drug design and clinical development relevant to perioperative EGFR-TKI use; evaluate pain-related tolerability, analgesic strategies and patient experience—including CPSP and ePRO-based monitoring; and propose an integrated “efficacy–safety–pain–adherence” framework to guide future research and clinical practice (Figure 1). To our knowledge, this is the first review to bring together perioperative targeted therapy, pain-related tolerability and multidisciplinary pain-management strategies within a single framework for resectable NSCLC.
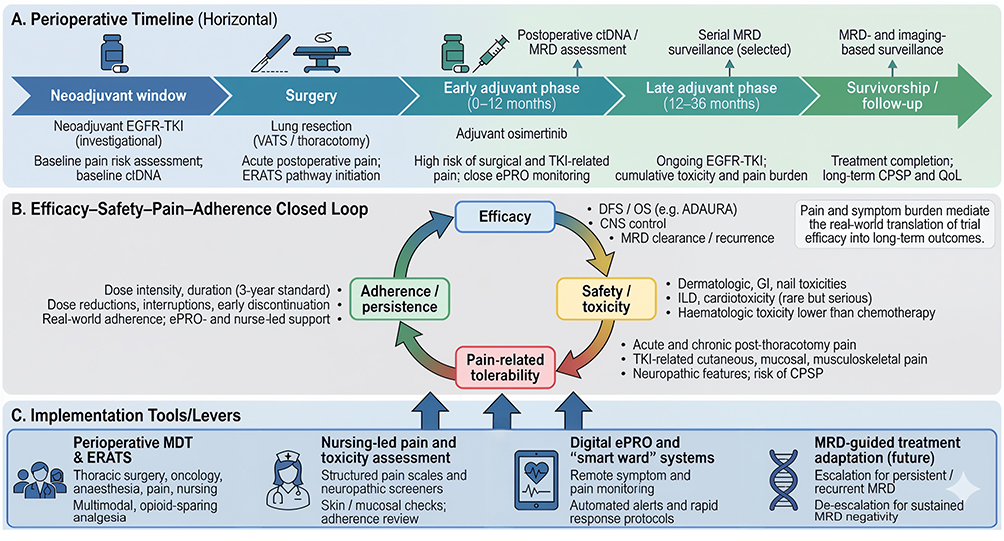 |
Figure 1 Conceptual efficacy–safety–pain–adherence framework for perioperative EGFR-targeted therapy in resectable EGFR-mutated NSCLC. (A) Perioperative Timeline (Horizontal). (B) Efficacy-Safety-Pain-Adherence Closed Loop. (C) Implementation Tools/Levers. |
This narrative review was informed by literature identified through searches of major biomedical databases (eg, PubMed/Medline and Embase) and relevant conference abstracts, focusing on perioperative EGFR-TKI trials, ctDNA/MRD studies, postoperative and chronic pain after lung resection, and patient-reported outcomes/adherence interventions. Priority was given to pivotal randomised trials, large prospective cohorts, and consensus guidelines; mechanistic and implementation studies were included to support the proposed framework. Given the narrative scope, formal risk-of-bias assessment and meta-analysis were not performed.
Molecular Mechanisms and Fundamentals of Drug Design
Oncogenic Drivers in Resectable NSCLC and Their Therapeutic Relevance
Early-stage NSCLC is genetically diverse even when potentially curable by surgery. Prospective cohorts such as EARLY-EGFR have shown that sensitizing EGFR mutations—including exon 19 deletions and L858R—are highly prevalent in resected stage I–III adenocarcinoma, particularly in Asian populations.19 In Western cohorts, KRAS mutations (notably G12C) are more common, whereas ALK rearrangements, MET exon 14 skipping and RET fusions define smaller but clinically relevant subgroups.20
Driver alterations also shape recurrence patterns. EGFR-mutant and ALK-rearranged tumours exhibit an early relapse peak within two to three years after surgery, suggesting persistent MRD and ongoing oncogenic signalling.21 These observations support perioperative systemic therapy aimed at suppressing MRD and preventing micrometastatic outgrowth and justify broad next-generation sequencing (NGS) for stage I–III disease to identify actionable drivers and anticipate resistance and toxicity profiles relevant to perioperative decision-making.22
Structural Evolution of EGFR-TKIs Toward Fourth-Generation Agents
The development of EGFR TKIs exemplifies progressive refinement in mutant selectivity and resistance avoidance. First-generation reversible TKIs (gefitinib, erlotinib) occupy the ATP-binding pocket via hinge-region hydrogen bonds but lack strong selectivity for mutant EGFR; acquisition of the T790M gatekeeper mutation restores ATP affinity and confers resistance.23 Second-generation agents (afatinib, dacomitinib) introduce irreversible covalent binding to Cys797 but maintain broader ErbB-family inhibition, leading to dermatologic and gastrointestinal toxicities that can limit tolerability in the perioperative setting.24
Third-generation inhibitors such as osimertinib combine irreversible Cys797 binding with enhanced mutant selectivity and improved safety; nonetheless, C797S remains a major on-target resistance mechanism.25 Fourth-generation compounds, including sunvozertinib (DZD9008), employ compact scaffolds and alternative binding modes to retain potency against C797S and exon 20 insertions while relatively sparing wild-type EGFR.26,27 These design features translate into durable responses and more manageable toxicity profiles—attributes that are particularly important in perioperative contexts where adverse events, pain and adherence directly influence recovery and long-term outcomes. Representative fourth-generation EGFR-TKIs and their potential perioperative relevance are summarised in Table 1.
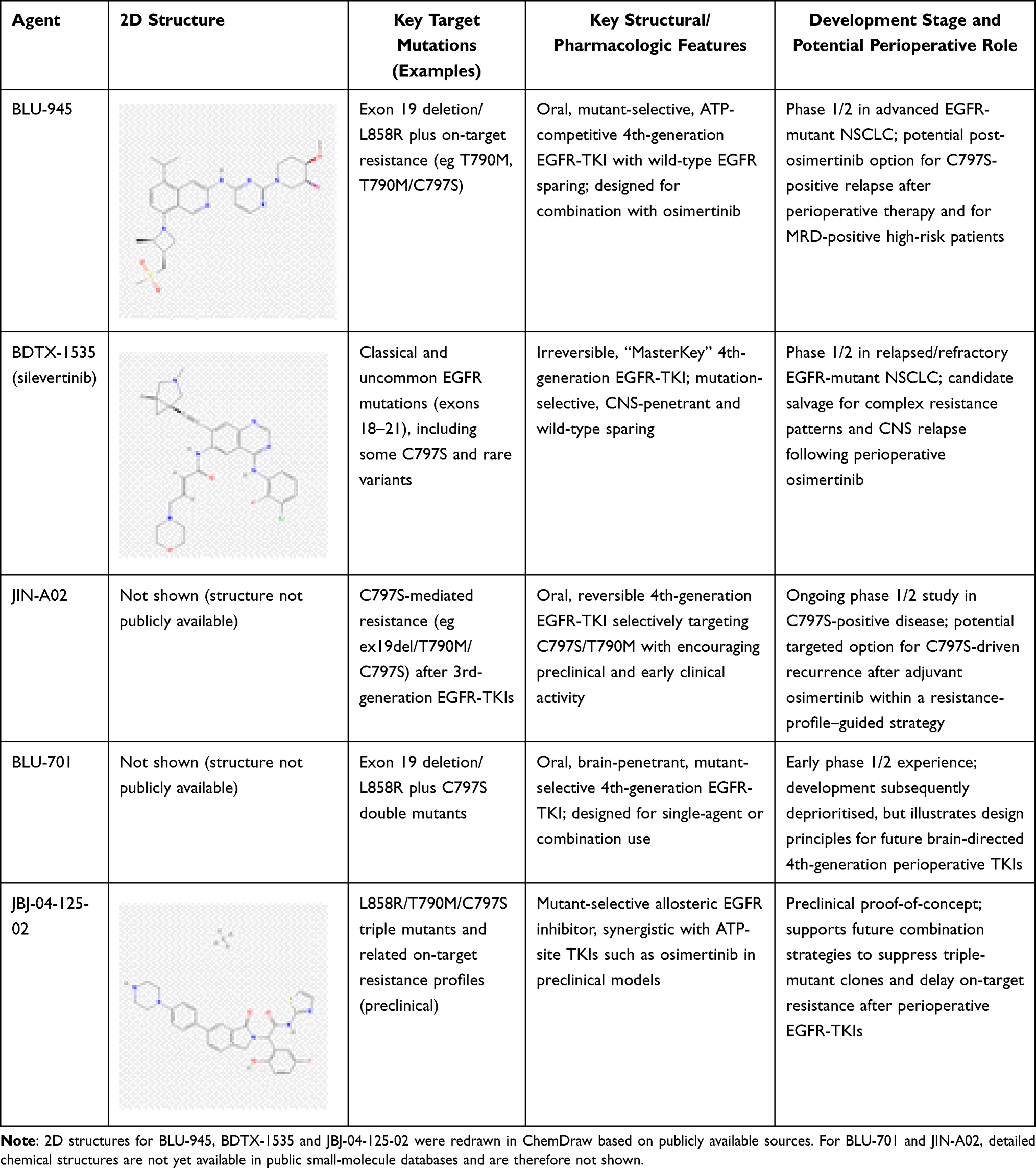 |
Table 1 Representative Fourth-Generation EGFR-TKIs and Their Potential Perioperative Relevance |
Perioperative Pharmacokinetics, Surgical Stress Physiology and Drug Safety
The perioperative period is characterised by dynamic physiological changes that can alter the pharmacokinetics of oral targeted therapies. Osimertinib exposure, for example, varies widely among patients and may be further modified after thoracic surgery by transient hepatic dysfunction, changes in CYP3A activity and altered gastrointestinal motility.28 Surgical stress and concurrent physiological changes can also affect plasma protein binding and tissue distribution, altering the pharmacologically active fraction of TKIs.29 Concomitant use of antibiotics, corticosteroids, proton-pump inhibitors or analgesics adds complexity through drug–drug interactions.30
Toxicities such as diarrhoea, anorexia and rash can compromise nutrition, wound healing and participation in rehabilitation programmes. Understanding the interplay between pharmacokinetics, postoperative physiology and pain control is therefore critical to maintaining adequate therapeutic exposure while supporting safe recovery in the perioperative phase.
Targeted Therapies and Pain-Related Neurobiology: Mechanistic Cross-Talk
Perioperative EGFR-targeted therapy intersects with nociceptive and neuropathic pain mechanisms that are central to thoracic surgery. Surgical trauma induces intercostal nerve injury, local inflammation and central sensitisation; CPSP can persist for years in 15–20% of patients.31
EGFR signalling modulates neuronal excitability through PI3K–AKT, MAPK and TRPV1-related pathways. Activation of EGFR in dorsal root ganglia and spinal microglia enhances glutamate release and synaptic sensitisation, amplifying nociceptive transmission.32 Conversely, chronic EGFR inhibition may interfere with neural repair and Schwann-cell function, contributing to neuropathic-like symptoms such as paraesthesia or myalgia. The net effect depends on drug selectivity, dose intensity and timing of exposure relative to tissue injury. Because the intensity of acute postoperative pain strongly predicts CPSP risk,33 strategic coordination of EGFR-TKI initiation with optimised multimodal analgesia is essential.
Inflammatory cytokines released after surgery (eg IL-6, TNF-α) can modify TKI pharmacodynamics and pain thresholds, creating bidirectional feedback between inflammation, analgesic response and toxicity. Emerging preclinical models suggest that EGFR–MAPK interference can modulate TRPV1 and NaV1.8 channels, potentially influencing neuronal plasticity and pain chronification. Clinically, selecting TKIs with low neurotoxicity potential, employing regional analgesia where feasible and involving pain specialists early may improve pain outcomes and support adherence to perioperative targeted therapy.
Translational Continuum from Molecular Design to Perioperative Clinical Application
Perioperative EGFR-targeted therapy exemplifies a translational continuum that links medicinal chemistry, molecular diagnostics, and clinical implementation.34 Fourth-generation EGFR-TKIs were rationally designed through iterative structure–activity optimisation and, in some cases, allosteric modulation to overcome resistance mediated by C797S substitution and exon 20 insertions.35,36 Within this continuum, plasma ctDNA-based MRD assays provide real-time estimation of recurrence risk and treatment response and form the basis for risk-adapted perioperative strategies, which are discussed in detail in MRD-Guided Adaptation of Perioperative EGFR-TKI Therapy.
Clinical Evidence for Perioperative EGFR-Targeted Therapy
From Platinum-Based Chemotherapy to Genotype-Directed Perioperative Therapy
Meta-analytic data from the Lung Adjuvant Cisplatin Evaluation (LACE) confirmed that postoperative cisplatin-based chemotherapy confers only a modest survival benefit (HR 0.89) and that this benefit is stage dependent—clear in stage II–III but minimal in stage I disease.37,38 With routine molecular profiling, EGFR-mutated NSCLC has emerged as a biologically distinct subset characterised by oncogene addiction, stereotyped recurrence patterns and profound TKI sensitivity in advanced disease.39 Retrospective cohorts suggest that the benefit of platinum chemotherapy is attenuated in early-stage EGFR-mutant tumours, with several analyses showing no significant improvement in recurrence-free survival.40,41 These observations support genotype-directed perioperative therapy that targets underlying oncogenic drivers rather than non-specific cytotoxic pathways.
Large perioperative chemo-immunotherapy trials have established event-free survival benefits in unselected populations;42 however, evidence in EGFR-mutated subgroups remains limited and is often based on small numbers and exploratory analyses.43 Given the established efficacy of EGFR-TKIs in oncogene-driven disease and the potential for overlapping pulmonary toxicities, the optimal role and sequencing of immunotherapy in resectable EGFR-mutated NSCLC remains uncertain and should be individualised and preferably addressed in prospective biomarker-stratified studies.44
Adjuvant EGFR-TKIs After Complete Resection of EGFR-Mutated NSCLC
First-Generation Adjuvant EGFR-TKIs
Evidence supporting adjuvant EGFR-TKIs has expanded rapidly, encompassing phase III trials, pooled analyses and real-world cohorts.45 Across stage IB–IIIA disease, adjuvant TKIs consistently improve DFS, although the magnitude of overall-survival (OS) benefit varies by stage, TKI generation and treatment duration.46 Toxicity profile and treatment burden relative to platinum chemotherapy are crucial in the perioperative context, where postoperative recovery, pain and adherence strongly influence long-term outcomes.
ADJUVANT/CTONG1104 remains the most mature first-generation trial. Twenty-four months of gefitinib improved DFS versus vinorelbine–cisplatin in resected stage II–IIIA EGFR-mutant NSCLC, with markedly fewer haematologic toxicities.47 Long-term follow-up confirmed a persistent DFS advantage, whereas OS was similar (HR 0.92), likely reflecting access to TKIs at recurrence in the chemotherapy arm.48,49 In higher-risk disease, EVAN showed that two years of erlotinib yielded a clinically meaningful OS benefit in stage IIIA patients (5-year OS ≈85% vs 51%).50
Meta-analytic synthesis reinforces these findings: pooled analyses of randomised trials, including third-generation TKIs, show substantial DFS improvement (HR ≈0.46),45 but only a modest overall-survival advantage (HR ≈0.7), mainly in stage III disease and with higher-potency agents.46 A Bayesian network meta-analysis comparing TKI monotherapy, TKI plus chemotherapy and chemotherapy alone suggested no inferiority for TKI monotherapy and higher rates of grade ≥3 toxicity with combination regimens.51 Real-world data similarly indicate that prolonged TKI exposure (≥2 years) improves DFS and OS, whereas adding platinum chemotherapy confers little incremental benefit.52
In lower-stage disease, the CORIN (GASTO1003) Phase II trial showed that 12 months of icotinib significantly improved 5-year DFS (88.5% vs 67.7%) in resected stage IB EGFR-mutant NSCLC.53,54 These results support adjuvant targeted therapy for high-risk stage IB patients, particularly in settings where third-generation TKIs are unavailable. Overall, first-generation agents (gefitinib, erlotinib, icotinib) consistently improve DFS and can enhance OS in selected cohorts.55 However, limited CNS penetration, cutaneous and gastrointestinal toxicity and inconsistent OS benefit have prevented them from becoming the preferred adjuvant option in contemporary practice.
Third-Generation Osimertinib and the ADAURA Paradigm
In ADAURA, three years of adjuvant osimertinib significantly improved disease-free survival and reduced CNS relapse versus placebo in resected stage IB–IIIA EGFR-mutated NSCLC, with a confirmed overall-survival benefit on mature follow-up.56 The safety profile was predominantly low-grade and manageable, supporting prolonged postoperative exposure with proactive toxicity and symptom monitoring.57
Three-year safety data showed predominantly low-grade, manageable adverse events concentrated in the first treatment year.58 Health-related quality of life remained stable compared with placebo, supporting sustained postoperative exposure with limited symptomatic burden—an important consideration for patients already dealing with surgical pain and functional recovery. Comparative analyses highlight a clear hierarchy: osimertinib delivers the largest and most consistent DFS and OS benefits, superior CNS protection and a more favourable tolerability profile than earlier-generation TKIs.56 Where osimertinib is inaccessible, first-generation TKIs remain pragmatic alternatives but should be viewed as context-dependent options rather than preferred perioperative therapy. Targeted therapy provides greater DFS benefit than chemo-immunotherapy in completely resected EGFR-mutant disease, reinforcing its role as the backbone of adjuvant systemic therapy.59
Collectively, the evolving evidence base establishes osimertinib as the reference standard for adjuvant treatment of resected stage II–IIIA and selected IB EGFR-mutant NSCLC. Key perioperative trials of adjuvant EGFR-TKIs in resected EGFR-mutant NSCLC are summarised in Table 2. This “ADAURA paradigm” underpins ongoing efforts to integrate EGFR-TKIs with neoadjuvant strategies, MRD-guided personalisation and structured perioperative symptom—including pain—management discussed in subsequent sections.
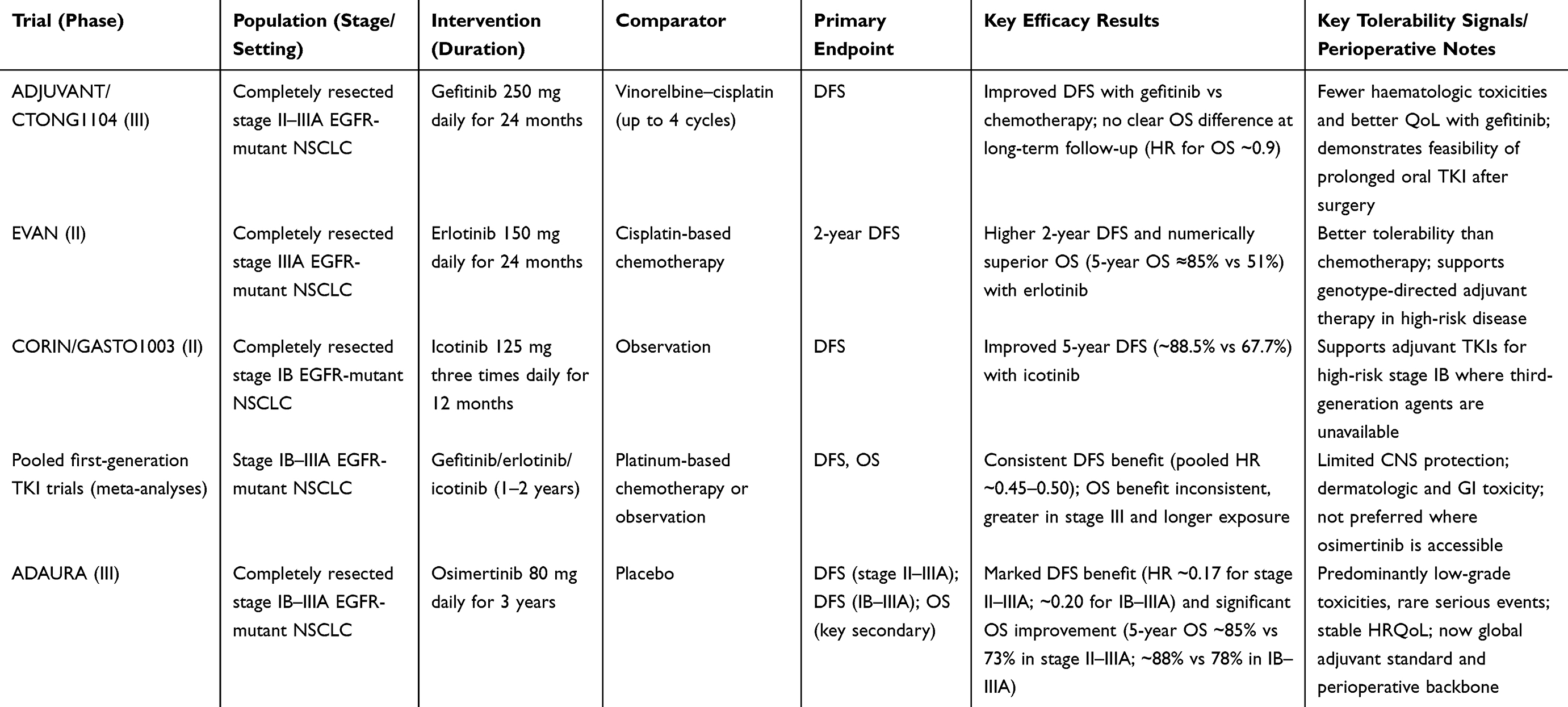 |
Table 2 Key Perioperative Adjuvant EGFR-TKI Trials in Resected EGFR-Mutated NSCLC |
Neoadjuvant EGFR-TKIs in Resectable EGFR-Mutant NSCLC
Applying EGFR-TKIs preoperatively is conceptually attractive: early systemic therapy may eradicate micrometastases, shrink tumours to facilitate resection and provide an in vivo assessment of drug sensitivity.60 However, neoadjuvant TKIs must preserve surgical feasibility and downstream adjuvant options, particularly given the established ADAURA standard.
Early-phase studies with first- and second-generation TKIs have shown consistent radiographic activity but modest pathological responses. Single-arm trials of gefitinib or erlotinib in stage II–IIIA EGFR-mutant NSCLC reported objective response rates of 50–70%, R0 resection rates around 90%, but low major pathological response (MPR ≈10%) and complete response (pCR ≈3%).61 These data confirm surgical feasibility and antitumour activity yet indicate that short-course TKIs mainly induce cytoreduction rather than true eradication.
The randomised EMERGING-CTONG1103 trial provides the strongest comparison to date. In stage IIIA-N2 EGFR-mutant NSCLC, perioperative erlotinib improved progression-free survival (≈21.5 vs 11.4 months) and objective response (54% vs 34%) versus cisplatin–gemcitabine.62 R0 resection and surgical complication rates were similar, but MPR rates remained ≈10% and pCR was not achieved; OS was comparable at follow-up. These results highlight feasibility and cytoreductive potential but underscore the limited depth of pathological response and the absence of a proven survival advantage.
Third-generation osimertinib has shown greater promise. In the multicentre NEOS phase IIb trial, six weeks of neoadjuvant osimertinib in stage IIA–IIIB disease achieved an ORR of 71% and an R0 resection rate of 94%, with predominantly low-grade adverse events.63 Retrospective and real-world series corroborate safety: surgery after appropriate TKI interruption does not appear to increase perioperative morbidity or mortality.64,65
The phase III NeoADAURA trial is now directly comparing neoadjuvant osimertinib ± chemotherapy with chemotherapy alone. Early 2025 results reported MPR rates of ≈25–26% versus 2%, greater nodal downstaging, high surgical completion (≈94%) and improved 12-month event-free survival (≈93–95% vs 83%).66,67 Although mature OS and recurrence data are pending, these findings suggest that neoadjuvant osimertinib, alone or combined with chemotherapy, can meaningfully deepen pathological responses while maintaining surgical feasibility. Current guidelines therefore classify neoadjuvant EGFR-TKIs as promising yet investigational.68 Adjuvant osimertinib remains the only targeted agent with proven survival benefit, and questions around optimal sequencing with MRD-guided strategies and perioperative symptom management remain central research priorities.
MRD-Guided Adaptation of Perioperative EGFR-TKI Therapy
ctDNA–based MRD assays provide a biologically informed framework for refining perioperative EGFR-TKI strategies beyond fixed-duration therapy. A 2023 meta-analysis of 16 lung-cancer cohorts showed that postoperative ctDNA positivity has high specificity (≈0.90–0.95) for recurrence but only moderate sensitivity at a single time point; longitudinal surveillance increases sensitivity to ≈75–80% while maintaining high specificity13 Thus, MRD positivity reliably identifies high-risk patients, whereas MRD negativity—although favourable—remains insufficient to justify omission of adjuvant therapy in current practice.
Prospective perioperative cohorts validate the prognostic importance of ctDNA. In LUNGCA-1, postoperative ctDNA positivity predicted markedly higher recurrence rates and shorter relapse-free survival, often preceding radiologic relapse by several months.69 Longitudinal analyses demonstrate that persistently positive or recurrent ctDNA identifies a subgroup with inferior long-term outcomes, whereas durable ctDNA clearance correlates with favourable prognosis.70 Even in early-stage tumours—particularly stage I—where ctDNA shedding is limited, postoperative positivity marks a small but clinically meaningful high-risk subset.71
Technological advances have improved MRD detection. Tumour-informed, ultra-sensitive assays such as PROPHET use whole-exome sequencing of the resected tumour to track dozens of patient-specific clonal variants, lowering detection limits to 10−3–10−5 and extending lead time to recurrence compared with tumour-naïve fixed panels.72 TRACERx modelling indicates that many early-stage tumours shed ctDNA near assay thresholds, highlighting that sampling schedules and analytical sensitivity critically determine MRD performance.73 Current reviews emphasise that MRD should complement—not replace—clinicopathologic risk factors when designing perioperative algorithms.74,75
In EGFR-mutant NSCLC, emerging data suggest that MRD can guide both intensification and de-escalation of adjuvant TKIs. A 2024 observational study in JTO Clinical and Research Reports followed 71 patients with resected stage I–III EGFR-mutant NSCLC receiving adjuvant TKIs plus tumour-informed MRD testing.76 Longitudinal sensitivity reached ≈86%, and negative predictive value ≈90%. Among patients who discontinued TKIs after sustained MRD negativity, 2-year DFS remained ≈80%, and most recurrences were salvageable with TKI re-initiation—providing hypothesis-generating support for MRD-guided de-escalation within prospective protocols, while recognising the absence of phase III validation. Conversely, persistent or recurrent MRD despite adjuvant therapy identified a high-risk subgroup, supporting MRD positivity as a trigger for escalation or clinical-trial enrolment.
Exploratory analyses from ADAURA (2025) showed that MRD positivity preceded DFS events by ≈4–5 months, and combined DFS/MRD event-free rates were higher with adjuvant osimertinib than with placebo.77 Many DFS or MRD events in the osimertinib arm occurred within 12 months of planned cessation, suggesting that re-emergent MRD may identify patients who could benefit from extended-duration therapy. Conceptually, MRD may serve as a bidirectional signal for future trial designs (eg, exploring earlier discontinuation in sustained MRD-negative patients and extension/intensification in persistent MRD-positive patients); however, routine clinical adoption remains premature in the absence of phase III validation.
Randomised MRD-guided perioperative trials in EGFR-mutant NSCLC are still scarce, but analogous designs in other malignancies demonstrate feasibility. The DYNAMIC trial in stage II colon cancer showed that ctDNA-guided adjuvant chemotherapy reduced treatment intensity without compromising relapse-free survival.78 In advanced EGFR- or ALK-positive NSCLC, ctDNA-guided TKI de-escalation after local consolidation permitted treatment breaks, with retreatment at MRD recurrence yielding high response rates.79 These models highlight operational principles—pre-specified MRD thresholds, structured surveillance intervals and retreatment criteria—that are directly applicable to future EGFR-mutant NSCLC trials. Selected studies informing ctDNA/MRD-guided perioperative strategies in NSCLC and related settings are summarised in Table 3.
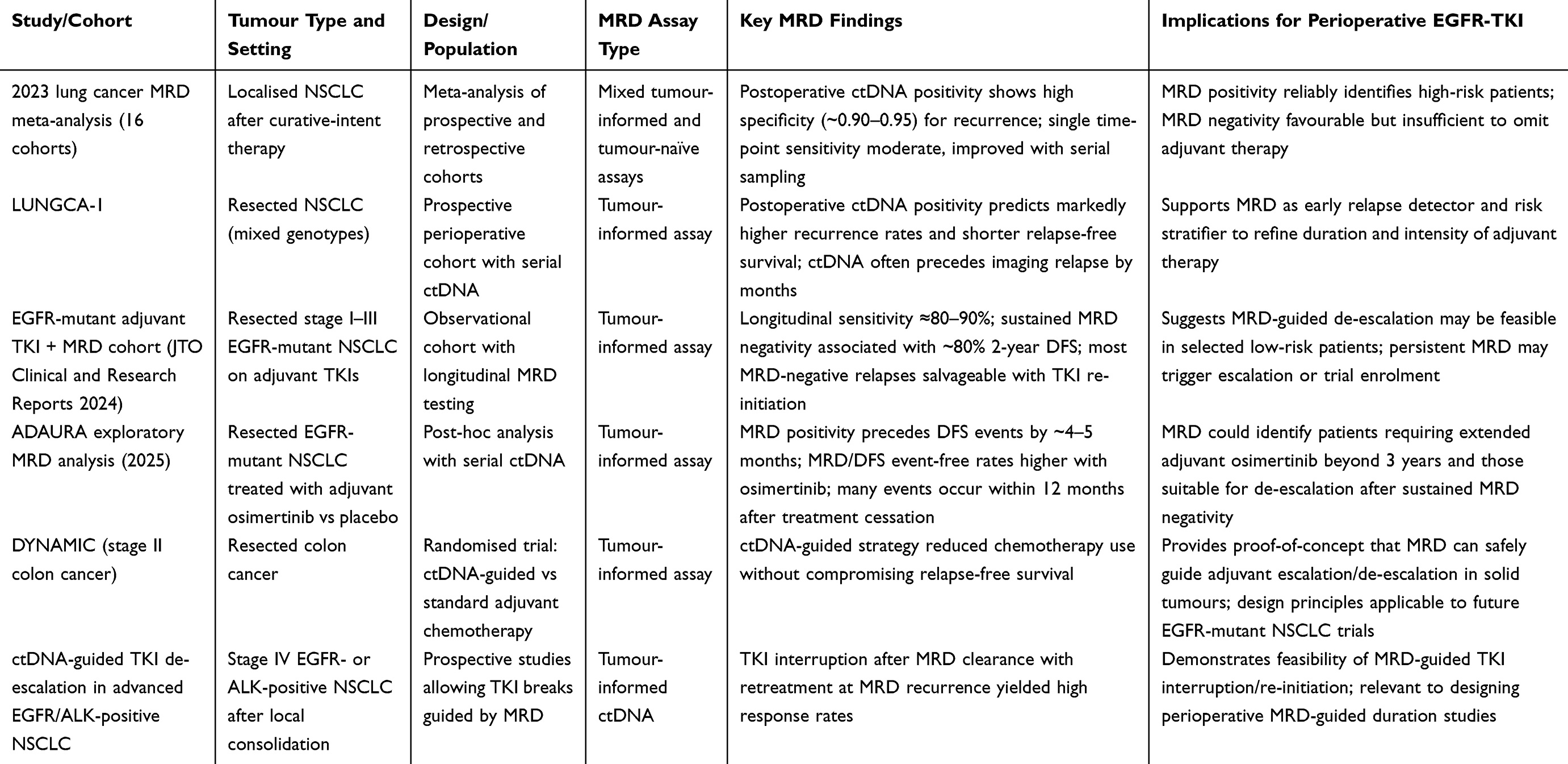 |
Table 3 Selected Studies Informing ctDNA/MRD-Guided Perioperative Strategies |
Important challenges persist. Assay heterogeneity in design, sensitivity and error suppression limits comparability. Even state-of-the-art assays may miss biologically relevant MRD in low-shedding tumours, whereas clonal haematopoiesis can generate false positives, requiring careful bioinformatic filtering.80 Clinically, overreliance on MRD negativity risks undertreatment. These caveats underscore the need for cautious, trial-based adoption in which MRD informs—but does not solely determine—perioperative decision-making.
A conceptual MRD-integrated framework for resectable EGFR-mutant NSCLC may comprise three strata: MRD-positive early postoperative or persistent MRD: candidates for treatment escalation (extended osimertinib, combinations or next-generation EGFR inhibitors); High-risk but MRD-negative patients (eg N2 disease): continuation of standard 3-year osimertinib with MRD monitoring rather than early de-escalation; Low-risk, sustained MRD-negative patients: potential de-escalation, particularly when toxicity, pain burden or adherence issues arise. This MRD-integrated, pain-informed stratification approach is illustrated in Figure 2.
 |
Figure 2 MRD-integrated, pain-informed perioperative stratification model for EGFR-mutated NSCLC. |
Overall, MRD-guided adaptation of EGFR-TKI therapy is promising yet remains investigational. ctDNA MRD is a powerful prognostic marker and early relapse detector, but assay heterogeneity, imperfect sensitivity and lack of phase III validation mean that three years of adjuvant osimertinib is still the standard of care. As MRD technologies mature and are embedded into perioperative trial design, MRD-guided personalisation of EGFR-TKI therapy is likely to become central to curative-intent management of resectable EGFR-mutant NSCLC.
Perioperative Targeted Therapy in Other Oncogene-Driven Subsets (ALK, MET, RET and KRAS)
Although EGFR-mutated NSCLC provides the most mature perioperative model, parallel strategies are emerging across other oncogene-defined subsets. Alterations in ALK, RET, MET and KRAS account for a meaningful minority of early-stage NSCLC, and highly active TKIs developed for metastatic disease are now being tested before and after surgery.81 These translational efforts mirror the EGFR experience but must address smaller populations, existing chemo-immunotherapy standards and the need to balance prolonged targeted therapy with perioperative tolerability and symptom burden.
ALK-rearranged NSCLC has advanced the furthest. The phase III ALINA trial randomised patients with completely resected stage IB (≥4 cm)–IIIA ALK-positive NSCLC to 24 months of alectinib or platinum-based chemotherapy.82 Alectinib produced a striking DFS benefit (3-year DFS ≈88% vs 53% in stage II–IIIA; HR ≈0.24) and markedly reduced CNS relapse, with toxicity consistent with prior experience. Based on these results, adjuvant alectinib is now approved for resected ALK-positive NSCLC, establishing a second genotype-directed perioperative standard alongside osimertinib.83
In RET fusion–positive NSCLC, the highly selective inhibitor selpercatinib has shown robust efficacy in advanced disease. The global phase III LIBRETTO-432 trial mirrors ADAURA and ALINA by evaluating three years of adjuvant selpercatinib versus placebo in stage IB–IIIA disease.84 Its outcomes will determine whether RET-directed adjuvant therapy can extend targeted approaches into early-stage disease.
For MET exon 14 skipping (METex14) or high-level MET amplification, perioperative data remain limited but conceptually aligned with the EGFR paradigm. Capmatinib and tepotinib induce durable responses in advanced METex14-mutant NSCLC.85 The GEOMETRY-N phase II trial is evaluating neoadjuvant and adjuvant capmatinib in resectable MET-driven NSCLC, focusing on pathological response and surgical feasibility.86 Older age, comorbidities and MET inhibitor–specific toxicities (oedema, hepatotoxicity) are likely to influence clinical integration and perioperative tolerability.
By contrast, KRAS-mutant NSCLC—particularly KRAS G12C—remains at an earlier stage of perioperative development. Sotorasib and adagrasib have demonstrated superiority to docetaxel in previously treated stage IV disease,87,88 but phase III perioperative data are lacking. Ongoing phase II trials include neoadjuvant sotorasib plus platinum–pemetrexed (NCT05118854) and adagrasib ± nivolumab (NCT2024-09121), which are assessing MPR, surgical feasibility and short-term recurrence.89,90 Interpretation will require careful consideration of existing chemo-immunotherapy standards, and the optimal perioperative duration—short-course neoadjuvant versus extended adjuvant—remains undefined.
Taken together, perioperative targeted therapy beyond EGFR is rapidly evolving but heterogeneous in maturity. Alectinib for ALK-positive disease now constitutes an established adjuvant standard, whereas RET-, MET- and KRAS-directed approaches remain investigational. Across all molecular subsets, successful integration depends on timely molecular testing, proactive management of overlapping toxicities and inclusion of patient-centred endpoints—pain, functional recovery and quality of life—alongside traditional survival outcomes.91 These principles directly connect to the following section on safety, pain-related tolerability and multidisciplinary supportive care in perioperative targeted therapy.
These efficacy data define the “efficacy” axis of the loop; subsequent sections address how chronic toxicities and pain can erode adherence and thereby attenuate real-world benefit.
Safety, Pain-Related Tolerability and Supportive Care in Perioperative Targeted Therapy
Overall Safety and Tolerability of Perioperative EGFR-TKIs
Because perioperative EGFR-TKIs are often administered for months or years after major thoracic surgery, long-term safety and tolerability are central determinants of real-world benefit. In ADAURA, three years of adjuvant osimertinib was mainly associated with low-grade, class-specific toxicities—diarrhoea, rash, paronychia and stomatitis—while grade ≥3 events were uncommon. Health-related quality-of-life scores remained similar to placebo, indicating that most adverse events can be managed by structured dose interruptions or reductions rather than permanent discontinuation.
Neoadjuvant trials provide complementary information on short-term perioperative risk. In NEOS (phase IIb), six weeks of preoperative osimertinib yielded an objective response rate >70%, with treatment-related events in roughly three-quarters of patients but grade 3 toxicity in only 7–8%; more than 90% achieved R0 resection without excess perioperative morbidity.63 A 2025 systematic review of neoadjuvant targeted-therapy trials reported grade ≥3 toxicity rates generally below 10% and no signal for impaired operability or postoperative recovery.92
Taken together, consensus reviews conclude that perioperative EGFR-TKIs are better tolerated than platinum-based chemotherapy or chemo-immunotherapy, especially with respect to haematologic toxicity, nausea, vomiting and neuropathy. Instead, toxicity is dominated by chronic low-grade dermatologic, gastrointestinal and nail-related effects, punctuated by rare pulmonary or cardiac events—patterns that directly shape adherence, pain burden and functional recovery. Accordingly, early-stage guidelines emphasise pretreatment counselling, regular toxicity monitoring, early intervention for rash and diarrhoea, baseline and periodic cardiac evaluation to preserve dose intensity while minimising harm.93
Targeted Therapy–Specific Adverse Events and Their Impact on Pain and Recovery
Perioperative EGFR-TKIs produce a characteristic spectrum of mechanism-based, predominantly non-haematologic toxicities that interact directly with pain and function.
Dermatologic reactions are among the most common. Acneiform rash, xerosis, pruritus and paronychia occur frequently even with third-generation agents and are particularly prevalent in Asian populations.94 These cutaneous events are often painful or intensely pruritic; nail-fold inflammation, fissures and fingertip tenderness interfere with fine motor tasks and daily activities.95 In the absence of proactive skin care—emollients, topical corticosteroids, oral antibiotics and low-threshold dermatology referral—rash and nail changes become major drivers of treatment interruptions and quality-of-life decline.96
Gastrointestinal events, especially diarrhoea and stomatitis, form a second major toxicity cluster. Across trials, diarrhoea affects 20–80% of patients, with a smaller subset experiencing grade ≥3 episodes that cause dehydration, electrolyte imbalance and cramping abdominal pain.97 Mechanisms include altered epithelial transport, dysbiosis and mucosal inflammation. Early management with diet modification, loperamide-based regimens and structured patient education can substantially mitigate severity.98 In perioperative patients, reduced oral intake, fluid shifts and vulnerability to malnutrition magnify the impact of even moderate diarrhoea or mucositis, delaying mobilisation and prolonging hospital stay.
Less common but clinically significant toxicities include ILD, hepatotoxicity and cardiotoxicity. Pharmacovigilance data suggest that EGFR-TKI–associated ILD, though rare, remains a leading cause of treatment-related mortality and is more frequent in some ethnic groups.99,100 ILD typically presents with acute dyspnoea, hypoxaemia and pleuritic pain, and may mimic postoperative pneumonia or pulmonary embolism; prompt recognition, immediate drug discontinuation and early corticosteroids are critical. Regulatory reviews of osimertinib identify ILD, cardiomyopathy and QTc prolongation as uncommon (<1%) but serious adverse reactions that can trigger rehospitalisation and abrupt cessation of adjuvant therapy.101 Although infrequent, these events exert a disproportionate psychological and functional impact, reinforcing the need for vigilant, multidisciplinary monitoring.
Pain-Related Adverse Events: Mechanisms and Clinical Phenotypes
Pain in the perioperative EGFR-TKI setting arises from converging sources: thoracic surgery, tumour biology and prolonged targeted therapy. After lung resection, up to one-third of patients develop chronic postsurgical pain, frequently with neuropathic features such as burning, allodynia or electric shocks along the chest wall or shoulder, which can persist for years and substantially impair quality of life.102,103 EGFR-TKI–related pain syndromes may overlay or amplify this background, complicating attribution and influencing decisions on dose modification or discontinuation.
As outlined in Targeted Therapy–Specific Adverse Events and Their Impact on Pain and Recovery, painful cutaneous and mucosal toxicities are hallmark EGFR-TKI effects that frequently limit daily function and medication adherence.104 At a mechanistic level, EGFR signalling regulates keratinocyte proliferation, epidermal integrity and barrier repair; inhibition promotes differentiation, thins the epidermis and favours inflammation and peripheral sensitisation.105 EGFR-driven pathways intersect with PI3K and MAPK nociceptive cascades, enhancing neuronal excitability and contributing to pain hypersensitivity.106
Musculoskeletal and neuropathic symptoms—including arthralgia, myalgia, tendon discomfort and distal paraesthesia—are also reported. Distinguishing these from post-thoracotomy, drain-related or tumour-related pain requires systematic assessment using numeric rating scales and neuropathic screening tools (eg DN4, S-LANSS, painDETECT), together with temporal correlation to surgery and treatment exposure.107 Rare but serious complications such as drug-induced ILD or cardiac ischaemia may present with chest pain, highlighting the importance of differentiating benign TKI-related discomfort from emergencies requiring urgent evaluation.108 Comprehensive, structured pain assessment is therefore fundamental to balanced decisions on dose adjustment, multimodal analgesia and continuation of perioperative EGFR-TKI therapy. Common EGFR-TKI toxicities that influence perioperative pain and recovery, together with practical management recommendations, are summarised in Table 4.
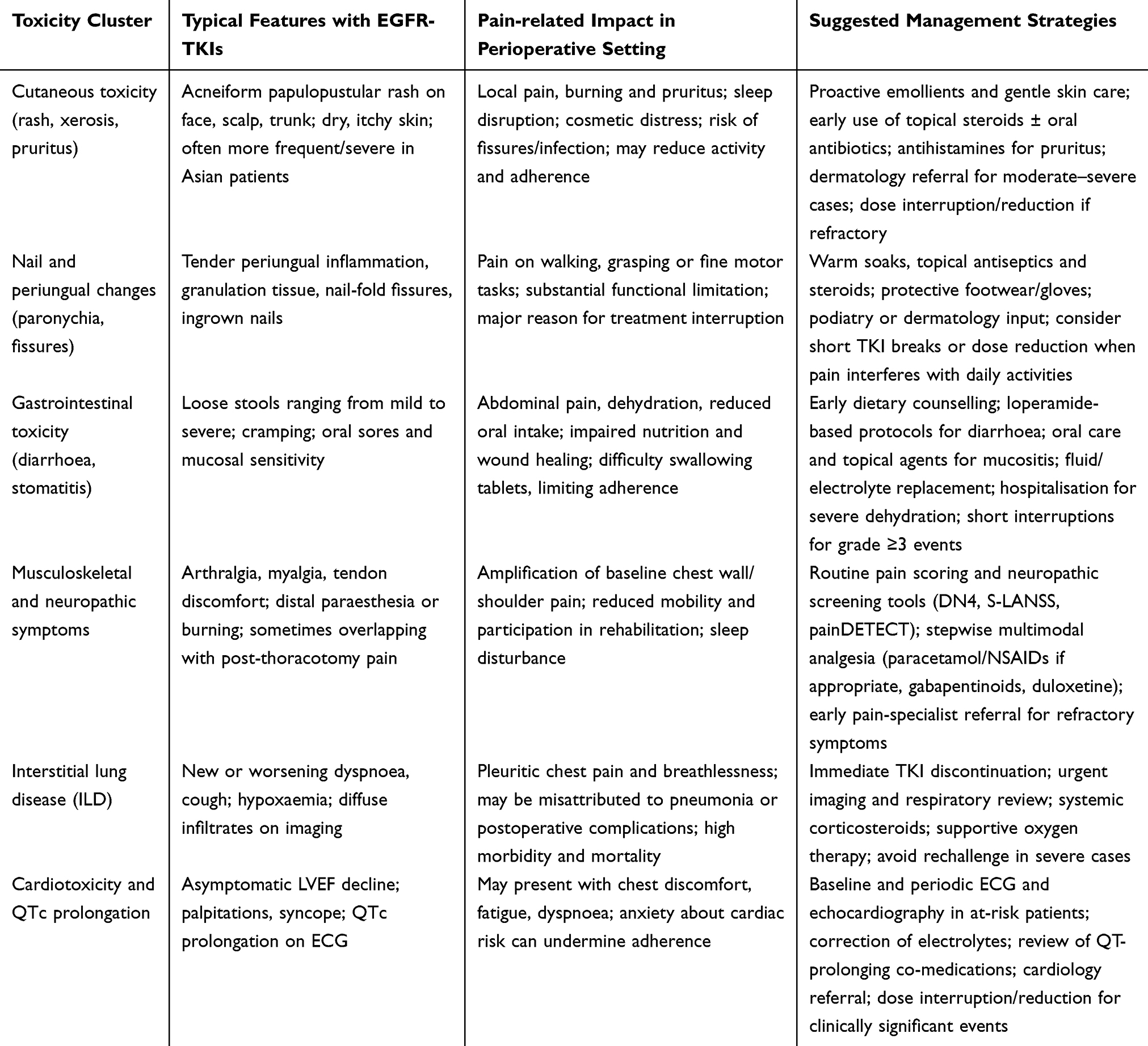 |
Table 4 Common EGFR-TKI Toxicities Relevant to Perioperative Pain and Recovery, and Suggested Management |
Multidisciplinary Perioperative Pain Management and ERAS-Based Care Pathways
Optimising pain control and tolerability during perioperative EGFR-TKI therapy requires coordinated input from thoracic surgeons, anaesthesiologists, pain specialists, medical oncologists, nurses and rehabilitation teams. Enhanced Recovery After Surgery (ERAS) programmes emphasise preoperative optimisation, minimally invasive techniques, early mobilisation and multimodal, opioid-sparing analgesia to reduce complications and facilitate timely resumption of systemic therapy after lung resection.109 Embedding EGFR-TKI–specific considerations into ERAS pathways—systematic review of drug–drug interactions, planned TKI interruption and restart around surgery, and early recognition of cutaneous, mucosal or respiratory symptoms—helps avoid unnecessary discontinuation and supports safe reinstitution of targeted therapy.110
Oncology nursing frameworks add an essential longitudinal perspective, with nurse-led pain assessment, skin and mucosal surveillance, and patient education integrated into ERAS pathways and oral targeted-therapy programmes, as detailed in Nursing Roles in Pain Assessment, Symptom Surveillance and Adherence Support.111
Early integration of supportive and palliative care—extended to high-risk surgical candidates rather than confined to advanced disease—can further improve pain control, quality of life and care coordination.112 Within resectable EGFR-mutant NSCLC, such multidisciplinary models ensure that decisions to continue, interrupt or adjust perioperative TKIs explicitly weigh tumour control against postoperative pain, functional recovery and patient preference.
Dose Modification, Treatment Interruption and Supportive-Care Decision Frameworks
Dose modification is a key tool in sustaining the efficacy–safety–pain–adherence loop. Decisions to reduce, interrupt or discontinue perioperative EGFR-TKIs should incorporate not only CTCAE grade but also patient-reported pain, functional interference and quality of life. Real-world studies show that a substantial proportion of patients receiving osimertinib require dose adjustment, yet moderate down-titration often preserves antitumour efficacy while improving tolerability.113 Therapeutic drug monitoring, where available, may allow pre-emptive adjustment in high-exposure patients, limiting severe toxicity without compromising outcomes.114
From a pain-centred perspective, persistent grade 2 toxicities that cause clinically meaningful pain—numeric rating ≥4, sleep disruption or limitation of daily activities—should prompt early intervention with topical therapy, adjuvant analgesics and, if needed, temporary interruption or stepwise dose reduction, rather than waiting for grade 3 escalation.115 Recent consensus recommendations advocate embedding patient-reported outcomes into dose-optimisation frameworks, recognising that clinician-graded adverse events frequently underestimate symptom burden.116
Patients at heightened risk of chronic postsurgical pain—those with severe acute postoperative pain, pre-existing chronic pain or psychological comorbidity—warrant tailored strategies linking perioperative pain pathways with EGFR-TKI management. These include structured preoperative risk screening, aggressive multimodal analgesia, early pain-specialist referral and predefined thresholds for reassessing dose or duration when pain worsens or function declines.117
This section populates the “safety” and “pain” axes and defines actionable thresholds that should feed back into adherence-preserving dose optimisation.
Real-World Tolerability, Adherence and Pain Burden with Perioperative EGFR-TKIs
Real-World Safety and Tolerability of Perioperative EGFR-TKIs
Outside clinical trials, the tolerability of perioperative EGFR-TKIs is increasingly described in national and multicentre cohorts. Real-world studies of adjuvant osimertinib in resected EGFR-mutant NSCLC confirm broadly ADAURA-like safety, with mostly low-grade adverse events and few treatment-related deaths.118 However, UK and European datasets show that up to one-third of patients discontinue adjuvant osimertinib before the planned three years, most often because of cumulative toxicity, comorbidities or patient preference rather than disease progression, and with higher rates of dose reduction and early interruption than reported in trials.119,120
Although most registries lack granular pain data, several observations are directly relevant to pain and functional recovery. First, as outlined in Perioperative Pain Burden and Chronic Postsurgical Pain in Lung Cancer Surgery, chronic chest wall and shoulder pain are common long after lung resection and frequently have neuropathic features. This pre-existing pain may amplify perceived toxicity and contribute to non-completion of adjuvant perioperative EGFR-TKI therapy. Second, registry and ERAS-linked datasets indicate that failure to initiate or complete prescribed adjuvant treatment is common and correlates with postoperative complications, poor recovery and high symptom burden, even in the absence of CTCAE grade ≥3 toxicity.110 These findings suggest that real-world tolerability of perioperative EGFR-TKIs reflects not only intrinsic drug toxicity but also the background of post-thoracotomy pain, fatigue and psychosocial stress that shapes recovery from lung cancer surgery.
Pain, Analgesic Burden and Adherence to Perioperative EGFR-TKIs
Building on the adherence patterns described in Section 1.4, large claims and review data for EGFR-TKIs and other oral anticancer agents show that symptom burden—including pain, fatigue and nausea—is a key driver of missed doses and early discontinuation, with older age, female sex and polypharmacy identifying more vulnerable subgroups.121
A meta-analysis of healthcare professional–led adherence interventions showed that programmes integrating structured toxicity education, proactive symptom management and regular follow-up improved adherence compared with usual care, underscoring that symptom control—not reminders alone—is key to sustaining long-term oral therapy.17 Qualitative studies in patients receiving EGFR-TKIs for advanced NSCLC report that chronic discomfort, skin and mucosal irritation and fear of cumulative toxicity often lead patients to “negotiate” treatment by skipping doses or shortening duration when pain and fatigue interfere with everyday life.122
Extrapolated to the perioperative context, these data imply that post-thoracotomy chest and shoulder pain, compounded by TKI-related cutaneous or oral pain, are likely important—and potentially modifiable—drivers of dose reduction, interruption and early discontinuation. Systematic assessment of pain intensity and functional interference, embedded within adherence monitoring, is therefore a core component of perioperative EGFR-TKI management and directly motivates the PRO- and nursing-based strategies discussed in Patient-Reported Outcome Tools and Digital Monitoring of Pain–5.4.
In the perioperative setting, post-thoracotomy pain and EGFR-TKI–related painful toxicities (paronychia, mucositis, myalgia/neuropathy) can jointly drive dose interruptions and non-persistence. Because adjuvant benefit depends on sustained exposure, pain interference with function should be treated as an early warning signal prompting protocolised supportive care and dose optimisation rather than a secondary comfort issue.
Patient-Reported Outcome Tools and Digital Monitoring of Pain
In routine care, patient-reported outcome (PRO) instruments provide practical tools to track perioperative pain and TKI-related symptoms. Generic oncology measures such as the EORTC QLQ-C30 and lung cancer–specific modules (QLQ-LC13/LC29) capture pain intensity, analgesic use and functional limitation, and have been widely used to characterise postoperative chest and shoulder pain trajectories.123 The PRO-CTCAE library offers complementary coverage of treatment-related toxicities, including TKI-associated dermatologic and mucosal events, although certain symptom domains remain underrepresented.
Electronic PRO (ePRO) systems extend this approach beyond clinic visits. Randomised and quasi-experimental trials in lung cancer–surgery populations show that ePRO-based symptom monitoring—with or without integration of wearable-derived data—can improve pain control, reduce unplanned healthcare utilisation and enhance activity levels and patient satisfaction.124
For perioperative EGFR-TKIs, embedding brief pain assessments—such as daily or weekly numeric rating scales coupled with simple neuropathic screeners—into ePRO pathways offers a realistic means of linking dose adjustments and supportive care directly to evolving pain profiles, rather than relying solely on intermittent clinician-graded CTCAE evaluations. These data provide a rationale for integrating brief, pain-focused ePRO modules into perioperative EGFR-TKI pathways, as further detailed in the implementation framework in Multidisciplinary Collaboration and Key Perioperative Touchpoints.
For future perioperative EGFR-TKI trials, a pragmatic minimum set could include: (i) pain intensity and interference (numeric rating scale plus brief interference items), (ii) neuropathic pain screening when relevant, (iii) PRO-CTCAE items capturing painful dermatologic/mucosal toxicities, (iv) functional recovery metrics (return to baseline activity/work), and (v) adherence/persistence measures (dose interruptions, relative dose intensity, and time-to-discontinuation). Pre-specified thresholds should trigger protocolised supportive care and dose optimisation.
Nursing Roles in Pain Assessment, Symptom Surveillance and Adherence Support
Evidence from thoracoscopic lung-surgery cohorts shows that nurse-led pain assessment using validated scales and structured documentation improves recognition of undertreated pain and facilitates timely escalation of multimodal analgesia within ERAS pathways.125 Postoperative protocols that combine early mobilisation, respiratory exercises and routine pain scoring enhance functional recovery and are associated with higher rates of initiation and completion of adjuvant systemic therapy.126,127
For oral targeted agents, including EGFR-TKIs, professional nursing guidelines recommend early (within 1–2 weeks) and ongoing monitoring of symptoms and adherence, with nurses leading education, toxicity counselling and refill checks.128,129 In the perioperative EGFR-TKI setting, these principles translate into nurse-led workflows that link routine pain scores, skin and mucosal assessments and reports of fatigue or sleep disruption to predefined clinical algorithms—specifying when to intensify multimodal analgesia, when to trigger medical review and when to consider dose modification. These nurse-driven processes form a practical bridge between the pain- and adherence-focused evidence summarised in Safety, Pain-Related Tolerability and Supportive Care in Perioperative Targeted Therapy and Real-World Tolerability, Adherence and Pain Burden with Perioperative EGFR-TKIs and the multidisciplinary implementation strategies outlined in Clinical and Nursing Implementation of an Efficacy–Safety–Pain–Adherence Framework.
Integrative Strategies and Practical Implications
Taken together, emerging real-world data, PRO-based symptom monitoring and nurse-led adherence programmes indicate that tolerability, pain control and treatment continuity must be managed as a single, integrated domain in perioperative EGFR-TKI therapy. These insights provide the practical foundation for the efficacy–safety–pain–adherence framework and multidisciplinary implementation models developed in Clinical and Nursing Implementation of an Efficacy–Safety–Pain–Adherence Framework.
Real-world discontinuation and symptom burden illustrate the “adherence” axis, supporting the need for ePRO-driven monitoring to close the loop.
Clinical and Nursing Implementation of an Efficacy–Safety–Pain–Adherence Framework
From Drug Development to Bedside: A Closed-Loop Model
As summarised in Adjuvant EGFR-TKIs After Complete Resection of EGFR-Mutated NSCLC–3.4, perioperative use of third-generation EGFR-TKIs such as osimertinib has become a standard component of curative-intent care in resected EGFR-mutated NSCLC, and ctDNA-based MRD studies together with perioperative trials like NeoADAURA are reshaping expectations around duration, sequencing and risk-adapted use.130
Within this evolving landscape, an efficacy-focused paradigm is no longer sufficient. We therefore propose an efficacy–safety–pain–adherence framework (Figure 1) that explicitly links four domains—oncologic efficacy, toxicity, pain-related tolerability and long-term adherence—with bidirectional feedback between drug development, clinical trials and bedside practice. In this closed-loop model, perioperative treatment decisions are informed not only by stage, mutation subtype and MRD status, but also by baseline pain risk, prior pain history and patient-reported symptom trajectories.
Trial data indicate that long-term adjuvant osimertinib can maintain health-related quality of life despite chronic exposure, provided that toxicities are recognised early and managed proactively.131 In this context, structured pain assessments and digital PRO tools embedded in routine care act as the monitoring backbone of the framework, enabling timely corrective actions rather than waiting until uncontrolled symptoms force irreversible treatment discontinuation (see Multidisciplinary Collaboration and Key Perioperative Touchpoints).
Practical Operationalisation of the Efficacy–Safety–Pain–Adherence Loop
To translate the proposed framework into clinical and trial workflows, perioperative care can be structured around four linked elements: baseline risk assessment, longitudinal monitoring, pre-specified intervention thresholds, and protocolised response pathways. Before treatment, teams should document pre-existing pain (including neuropathic features), psychosocial vulnerability, and functional status, counsel expected EGFR-TKI toxicities, and agree on an adherence plan and contact pathway. During treatment initiation and early postoperative recovery, symptom capture should be more frequent (eg, weekly to biweekly), transitioning to at least monthly assessments during adjuvant therapy; monitoring should include pain intensity and interference, key EGFR-TKI toxicities, and missed doses. Clinically meaningful pain that interferes with sleep or daily activities, persistent low-grade toxicities with functional impact, recurrent missed doses, or red-flag cardiopulmonary symptoms should trigger early escalation of supportive care, including dermatologic and gastrointestinal management, neuropathic analgesics when appropriate, and timely referral to pain or regional-anaesthesia services, with MDT review for complex cases. Within this structure, ctDNA/MRD results may inform risk discussions and trial enrolment; however, MRD-guided de-escalation or intensification should be regarded as investigational and ideally implemented only within prospective protocols or clinical trials.
Multidisciplinary Collaboration and Key Perioperative Touchpoints
Enhanced Recovery After Thoracic Surgery (ERATS) programmes, summarised in Multidisciplinary Perioperative Pain Management and ERAS-Based Care Pathways, provide a natural backbone on which to integrate perioperative EGFR-TKI management and pain-focused interventions. However, current ERATS pathways rarely incorporate targeted therapy–specific toxicities or long-term pain trajectories.132
A dedicated perioperative multidisciplinary team (MDT) for resectable, EGFR-mutated NSCLC should therefore define explicit decision nodes along four key touchpoints—pre-treatment planning, the neoadjuvant window, the perioperative inpatient stay and the adjuvant follow-up phase—at which oncologists, thoracic surgeons, anaesthesiologists, pain specialists, pharmacists and nurses coordinate around both systemic therapy and pain management.
At the pre-treatment planning stage, MDT meetings can align on neoadjuvant versus adjuvant strategies, anticipated EGFR-TKI choice and timing of interruption and resumption around surgery, while concurrently documenting baseline pain, psychosocial factors and patient expectations.133 During the neoadjuvant window, nurses and advanced practitioners can use standardised tools to track cutaneous, musculoskeletal and neuropathic symptoms, flagging patterns that may predict postoperative pain amplification or adherence challenges.
Examples of ERATS-aligned additions for patients receiving perioperative EGFR-TKIs include: standardised restart checklists (wound healing, oral intake, cardiopulmonary symptoms), drug–drug interaction screening with analgesics and perioperative medications, early dermatology/oral-care pathways for painful rash/mucositis, and discharge-to-home ePRO monitoring with pre-defined escalation rules.
During the perioperative inpatient stay, ERATS elements (regional anaesthesia, scheduled non-opioid analgesia, early mobilisation, respiratory physiotherapy) should be tailored to the presence of concurrent or recent EGFR-TKI exposure—for example, considering drug–drug interactions with non-steroidal anti-inflammatory drugs, steroids or neuropathic agents, and ensuring wound-healing assessment before restarting TKIs.134 In the adjuvant phase, MDT visits can synchronise ctDNA/MRD results with structured review of pain and functional recovery; patients with MRD positivity and high pain burden may require intensified supportive care and closer analgesic follow-up to sustain adherence to prolonged TKI therapy. Implementation of such MDT-based pathways is demanding, but nursing and allied-health leadership, together with institutional guidelines such as the AORN-enhanced recovery recommendations, can translate high-level ERATS principles into daily bedside practice.135
Nursing Data, Digital Tools and the “Smart Ward”
Meta-analyses and lung cancer–specific studies, summarised in Sections 1.4 and 5.3, show that ePRO-based symptom-monitoring programmes can improve health-related quality of life, reduce hospitalisations and, in some settings, prolong survival when used to trigger timely clinical responses. As outlined in From Drug Development to Bedside: A Closed-Loop Model, combining structured pain assessments with ePRO-based symptom monitoring provides the core clinical signals within the efficacy–safety–pain–adherence framework. These findings align with expert guidance from oncology societies, which now regard remote ePRO monitoring as a component of high-quality cancer care.136 Within this landscape, nurses are central to operationalising a pain-centred, adherence-sensitive perioperative pathway.
In a “smart ward” model for perioperative EGFR-mutated NSCLC, nursing teams can use ePRO platforms integrated into the electronic health record to capture pain scores, neuropathic symptoms, functional status and TKI-specific adverse events during neoadjuvant or adjuvant therapy and after discharge. Large multi-centre implementation projects such as the SIMPRO consortium emphasise that successful deployment depends on workflow redesign, shared response protocols and institutional support rather than technology alone.137 Within this framework, nurses often act as first-line responders to red-flag alerts—such as rapidly escalating chest wall pain, uncontrolled neuropathic symptoms or skin/mucosal pain that interferes with function—initiating protocolised dose modifications, arranging earlier MDT review or activating specialised pain services.
At the same time, smart ward infrastructure enables structured data capture at scale. Routine aggregation of pain scores, rescue-analgesic use, unscheduled contacts and missed or delayed EGFR-TKI doses can be used to refine institutional thresholds for intervention, identify high-risk phenotypes (eg patients with persistently high pain despite good oncologic response) and contribute anonymised data to registries and pragmatic real-world evidence studies. In this way, nursing-led digital monitoring functions both as a clinical tool and as a research engine, reinforcing the efficacy–safety–pain–adherence loop between bedside experience and future trial and guideline development.
Implementation barriers include variable access to tumour-informed ctDNA assays, cost and turnaround time, infrastructure for longitudinal blood draws and data integration, and the workforce burden of responding to ePRO alerts. Digital literacy and language barriers may also affect engagement. These constraints support stepwise deployment with clear response protocols, prioritisation of high-risk patients, and prospective evaluation of feasibility and cost-effectiveness.
Conclusion
Perioperative EGFR-targeted therapy is transforming curative-intent care for resectable EGFR-mutated NSCLC, but prolonged treatment introduces chronic toxicity and pain that can erode adherence and real-world benefit. ADAURA demonstrates that adjuvant osimertinib can deliver substantial survival gains with manageable toxicity when symptoms are proactively monitored. Elevating pain from a secondary “comfort” issue to a core determinant of treatment success—and embedding it within an efficacy–safety–pain–adherence framework (the proposed loop)—may help translate trial efficacy into better lived survivorship; MRD-guided tailoring of duration should remain limited to prospective protocols/trials. As a narrative review, selection bias cannot be fully excluded, and evidence strength varies across domains.
Abbreviations
ALK, Anaplastic lymphoma kinase; CNS, Central nervous system; CPSP, Chronic postsurgical pain; ctDNA, Circulating tumour DNA; DFS, Disease-free survival; EGFR, Epidermal growth factor receptor; EGFR-TKI, Epidermal growth factor receptor tyrosine kinase inhibitor; EFS, Event-free survival; ERAS, Enhanced Recovery After Surgery; ERATS, Enhanced Recovery After Thoracic Surgery; ePRO, Electronic patient-reported outcome; HR, Hazard ratio; HRQoL, Health-related quality of life; ILD, Interstitial lung disease; KRAS, KRAS proto-oncogene, GTPase; MDT, Multidisciplinary team; MET, MET proto-oncogene, receptor tyrosine kinase; MPR, Major pathological response; MRD, Minimal residual disease; NSCLC, Non-small cell lung cancer; ORR, Objective response rate; OS, Overall survival; pCR, Pathological complete response; PRO, Patient-reported outcome; PRO-CTCAE, Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events; R0, Complete microscopic resection; RET, REarranged during transfection proto-oncogene; RWE, Real-world evidence; TKI, Tyrosine kinase inhibitor.
Data Sharing Statement
Data sharing is not applicable to this article as no new datasets were generated or analyzed. All data discussed are from previously published studies cited in the references.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shenzhen Science and Technology Program (JCYJ20250604142253071), Project Proposal for Teaching Research and Reform at Shenzhen People’s Hospital in 2025 (SYJX2025-N0030), and the Shenzhen People’s Hospital Youth Project (SYHL2023-N0009).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hyuna S, Jacques F, S RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3).
2. Bharathi M, P PD, P NA. Perioperative systemic therapy for resectable non-small cell lung cancer. J Natl Compr Canc Netw. 2022;20(8).
3. Savvas L, Marco S. Perioperative systemic therapies for non-small-cell lung cancer: recent advances and future perspectives. Front Surg. 2023;9.
4. Yuko O, Ichidai T. Latest advances in perioperative care for resectable non-small lung cancer. Respir Investig. 2025;63(4).
5. S JD, Tina C, W MW, et al. Neoadjuvant and adjuvant treatments for early stage resectable NSCLC: consensus recommendations from the International Association for the study of lung cancer. J Thorac Oncol. 2024;19(10).
6. Mariano P, Ernest N, G-L JL, et al. Perioperative nivolumab and chemotherapy in stage III Non-Small-Cell Lung Cancer. N Engl J Med. 2023;389(6).
7. Mariano P, Ernest N, Amelia I, et al. Perioperative chemotherapy and nivolumab in non-small-cell lung cancer (NADIM): 5-year clinical outcomes from a multicentre, single-arm, Phase 2 trial. Lancet Oncol. 2024;25(11).
8. Nikitas J, Yanagawa J, Sacks S, et al. Pathophysiology and management of chest wall pain after surgical and non-surgical local therapies for lung cancer. JTO Clin Res Rep. 2024;5(7):100690. doi:10.1016/j.jtocrr.2024.100690
9. Khan JS, Dana E, Xiao MZ, et al. Prevalence and risk factors for chronic postsurgical pain after thoracic surgery: a prospective cohort study. J Cardiothorac Vasc Anesthesia. 2024;38(2):490–24. doi:10.1053/j.jvca.2023.09.042
10. Mengzhao W, Yun F, Meili S, et al. Sunvozertinib for patients in China with platinum-pretreated locally advanced or metastatic non-small-cell lung cancer and EGFR exon 20 insertion mutation (WU-KONG6): single-arm, open-label, multicentre, phase 2 trial. Lancet Respir Med. 2023;12(3).
11. Doucet L, Greillier L, Planchard D, et al. 1260P Efficacy and safety of sunvozertinib in prior platinum treated NSCLC patients with EGFR exon 20 insertion mutations: primary analysis from the multinational WU-KONG1B pivotal study. Ann Oncol. 2024;35:S807–S808. doi:10.1016/j.annonc.2024.08.1317
12. Wang M, Yang JC-H, Mitchell PL, et al. Sunvozertinib, a selective EGFR inhibitor for previously treated non–small cell lung cancer with EGFR exon 20 insertion mutations. Cancer Discovery. 2022;12(7):1676–1689. doi:10.1158/2159-8290.CD-21-1615
13. Zhong R, Gao R, Fu W, et al. Accuracy of minimal residual disease detection by circulating tumor DNA profiling in lung cancer: a meta-analysis. BMC Med. 2023;21(1):180. doi:10.1186/s12916-023-02849-z
14. Tang L, Li R, Wen H, Zhou Q, Xu C. Circulating tumor DNA (ctDNA)-based minimal residual disease in non-small cell lung cancer. Chin Med J Pulmonary Critical Care Med. 2023;1(4):207–214. doi:10.1016/j.pccm.2023.04.001
15. Rosenlund L, Guldbrandsen K, Ahlborn LB, et al. ctDNA can detect minimal residual disease in curative treated non-small cell lung cancer patients using a tumor agnostic approach. Lung Cancer. 2025;203:108528. doi:10.1016/j.lungcan.2025.108528
16. Nduaguba S, Cipoletti A, Misra R. CO161 adherence and persistence to oral targeted therapies for non-small-cell lung cancer and association with survival outcomes. Value Health. 2024;27(6):S47. doi:10.1016/j.jval.2024.03.248
17. Angus F, Liao W-C, Adekoya V, Chen L-C. The effect of healthcare professional-implemented interventions on adherence to oral targeted therapy in patients with cancer: a systematic review and meta-analysis. Support Care Cancer. 2025;33(2):110. doi:10.1007/s00520-024-09136-4
18. Li Y, Li J, Hu X. The effectiveness of symptom management interventions based on electronic patient-reported outcomes (ePROs) for symptom burden, quality of life, and overall survival among patients with cancer: a meta-analysis of randomized controlled trials. Int J Nurs Studies. 2023;147:104588. doi:10.1016/j.ijnurstu.2023.104588
19. Soo RA, Reungwetwattana T, Perroud HA, et al. Prevalence of EGFR mutations in patients with resected stages I to III NSCLC: results from the EARLY-EGFR study. J Thorac Oncol. 2024;19(10):1449–1459. doi:10.1016/j.jtho.2024.06.008
20. Wang M, Fan Y, Sun M, et al. Sunvozertinib for patients in China with platinum-pretreated locally advanced or metastatic non-small-cell lung cancer and EGFR exon 20 insertion mutation (WU-KONG6): single-arm, open-label, multicentre, phase 2 trial. Lancet Respir Med. 2024;12(3):217–224. doi:10.1016/S2213-2600(23)00379-X
21. Seong H, Kim SH, Kim M-H, Eom JS. Prognostic Impact of ALK rearrangements in resected NSCLC: a systematic review and meta-analysis. Anticancer Res. 2025;45(10):4519–4534. doi:10.21873/anticanres.17799
22. Ettinger DS, Wood DE, Aisner DL, et al. NCCN guidelines insights: non–small cell lung cancer, version 2.2021: featured updates to the NCCN guidelines. J National Compr Cancer Network. 2021;19(3):254–266. doi:10.6004/jnccn.2021.0013
23. Eck MJ, Yun C-H. Structural and mechanistic underpinnings of the differential drug sensitivity of EGFR mutations in non-small cell lung cancer. Biochimica Et Biophysica Acta (BBA)-Proteins and Proteomics. 2010;1804(3):559–566. doi:10.1016/j.bbapap.2009.12.010
24. Jung HA, Park S, Lee S-H, Ahn JS, Ahn M-J, Sun J-M. The role of brain radiotherapy before first-line Afatinib therapy, compared to gefitinib or erlotinib, in patients with EGFR-mutant non-small cell lung cancer. Cancer Res Treat. 2023;55(2):479–487. doi:10.4143/crt.2022.1344
25. Rotow JK, Lee JK, Madison RW, Oxnard GR, Jänne PA, Schrock AB. Real-world genomic profile of EGFR second-site mutations and other osimertinib resistance mechanisms and clinical landscape of NSCLC post-osimertinib. J Thorac Oncol. 2024;19(2):227–239. doi:10.1016/j.jtho.2023.09.1453
26. Mansour MA, AboulMagd AM, Abbas SH, Abdel-Rahman HM, Abdel-Aziz M. Insights into fourth generation selective inhibitors of (C797S) EGFR mutation combating non-small cell lung cancer resistance: a critical review. RSC Adv. 2023;13(27):18825–18853. doi:10.1039/D3RA02347H
27. Seo D, Lim JH. Targeted therapies for EGFR Exon 20 insertion mutation in non-small-cell lung cancer. Int J Mol Sci. 2024;25(11):5917. doi:10.3390/ijms25115917
28. Boosman RJ, Jebbink M, Veldhuis WB, et al. Exposure–response analysis of osimertinib in EGFR mutation positive non-small cell lung cancer patients in a real-life setting. Pharm Res. 2022;39(10):2507–2514. doi:10.1007/s11095-022-03355-2
29. Johnson M, Lin YW, Schmidt H, et al. Exposure–response modelling of osimertinib in patients with non‐small cell lung cancer. Br J Clin Pharmacol. 2024;90(12):3263–3276. doi:10.1111/bcp.16199
30. Tucker GT. Pharmacokinetic considerations and challenges in oral anticancer drug therapy. Clin Pharm. 2019;10.
31. Yoon S, Hong W-P, Joo H, et al. Long-term incidence of chronic postsurgical pain after thoracic surgery for lung cancer: a 10-year single-center retrospective study. Reg Anesth Pain Med. 2020;45(5):331–336. doi:10.1136/rapm-2020-101292
32. Peng W, Yao C, Pan Q, et al. Novel considerations on EGFR-based therapy as a contributor to cancer cell death in NSCLC. Front Oncol. 2023;13:1120278. doi:10.3389/fonc.2023.1120278
33. Bhatt K, Palomares A, Forget P, et al. Importance of pain management in cancer patients and survivors. Ann Oncol. 2024;35(5):473–474. doi:10.1016/j.annonc.2024.01.006
34. M MA, A AM, A SH, A-r HM, Mohamed -A-A. Insights into fourth generation selective inhibitors of (C797S) EGFR mutation combating non-small cell lung cancer resistance: a critical review. RSC Adv. 2023;13(27).
35. Li X, Bing X, Jianshe W, et al. Recent advances of novel fourth generation EGFR inhibitors in overcoming C797S mutation of lung cancer therapy. Eur J Med Chem. 2022;245.
36. Debasis D, Lingzhi X, Jian H. Next-generation EGFR tyrosine kinase inhibitors to overcome C797S mutation in non-small cell lung cancer (2019-2024). RSC Med Chem. 2024;15(10).
37. Pignon J-P, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26(21):3552–3559. doi:10.1200/JCO.2007.13.9030
38. Le Chevalier T. Adjuvant chemotherapy for resectable non-small-cell lung cancer: where is it going? Ann Oncol. 2010;21:vii196–vii198.
39. Antonio P, Tony S, Mok I, et al. Adjuvant treatments for surgically resected non–small cell lung cancer harboring EGFR mutations. JAMA Oncol. 2023;9:1124. doi:10.1001/jamaoncol.2023.0459
40. Tsutani Y, Ito M, Shimada Y, et al. The impact of epidermal growth factor receptor mutation status on adjuvant chemotherapy for patients with high-risk stage I lung adenocarcinoma. J Thoracic Cardiovasc Surg. 2022;164(5):1306–1315.e1304. doi:10.1016/j.jtcvs.2022.01.025
41. Miyoshi T, Aokage K, S-i W, et al. The effect of epidermal growth factor receptor mutation on adjuvant chemotherapy with tegafur/uracil for patients with completely resected, non-lymph node metastatic non-small cell lung cancer (> 2 cm): a multicenter, retrospective, observational study as exploratory analysis of the CSPOR-LC03 study. Jpn J Clin Oncol. 2024;54(11):1185–1193. doi:10.1093/jjco/hyae073
42. S JD, G MC, Heather W, et al. Neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab compared with neoadjuvant chemotherapy alone in patients with early-stage non-small-cell lung cancer (KEYNOTE-671): a randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet. 2024;404(10459).
43. Stephanie PLS, Wen-Zhao Z, Rui F, et al. Asian Thoracic Oncology Research Group expert consensus statement on the peri-operative management of non-small cell lung cancer. Lung Cancer. 2025;200.
44. Masahiro T, H RS, Thomas J, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med. 2023;389(2).
45. Zhao P, Zhen H, Zhao H, Zhao L, Cao B. Efficacy and safety of adjuvant EGFR-TKIs for resected non-small cell lung cancer: a systematic review and meta-analysis based on randomized control trials. BMC Cancer. 2022;22(1):328. doi:10.1186/s12885-022-09444-0
46. Zhang S-L, Yi X-F, Huang L-T, Sun L, Ma J-T, Han C-B. Rational application of EGFR-TKI adjuvant therapy in patients with completely resected stage IB-IIIA EGFR-mutant NSCLC: a systematic review and meta-analysis of 11 randomized controlled trials. BMC Cancer. 2023;23(1):719. doi:10.1186/s12885-023-11194-6
47. Zhong W-Z, Wang Q, Mao W-M, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II–IIIA (N1–N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): a randomised, open-label, phase 3 study. Lancet Oncol. 2018;19(1):139–148. doi:10.1016/S1470-2045(17)30729-5
48. Zhong W-Z, Wang Q, Mao W-M, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFR-mutant NSCLC: final overall survival analysis of CTONG1104 phase III trial. J Clin Oncol. 2021;39(7):713–722. doi:10.1200/JCO.20.01820
49. Zeng J, Mao W-M, Chen Q-X, et al. Quality of life with adjuvant gefitinib versus vinorelbine plus cisplatin in patients with completely resected stage II–IIIA (N1–N2) EGFR-mutant non-small-cell lung cancer: results from the ADJUVANT (CTONG1104) study. Lung Cancer. 2020;150:164–171. doi:10.1016/j.lungcan.2020.09.027
50. Yue D, Xu S, Wang Q, et al. Erlotinib versus vinorelbine plus cisplatin as adjuvant therapy in Chinese patients with stage IIIA EGFR mutation-positive non-small-cell lung cancer (EVAN): a randomised, open-label, phase 2 trial. Lancet Respir Med. 2018;6(11):863–873. doi:10.1016/S2213-2600(18)30277-7
51. Cui X, Li X, Lv C, Yan S, Wang J, Wu N. Efficacy and safety of adjuvant EGFR TKI alone and in combination with chemotherapy for resected EGFR mutation-positive non-small cell lung cancer: a Bayesian network meta-analysis. Crit rev oncol/hematol. 2023;186:104010. doi:10.1016/j.critrevonc.2023.104010
52. Liu J-F, Sun X-S, Yin J-H, Xu X-E. Adjuvant EGFR-TKI therapy in resected EGFR-mutation positive non-small cell lung cancer: a real-world study. Front Oncol. 2023;13:1132854. doi:10.3389/fonc.2023.1132854
53. Ou W, Li N, Wang B-X, et al. Adjuvant icotinib versus observation in patients with completely resected EGFR-mutated stage IB NSCLC (GASTO1003, CORIN): a randomised, open-label, phase 2 trial. EClinicalMedicine. 2023;57.
54. Passiglia F, Novello S. Should adjuvant treatment be offered to patients with stage IB non-small cell lung cancer? Eclinicalmedicine. 2023;57.
55. Passaro A, Mok TS, Attili I, et al. Adjuvant treatments for surgically resected non–small cell lung cancer harboring egfr mutations: a review. JAMA Oncol. 2023;9(8):1124–1131.
56. Wu Y-L, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non–small-cell lung cancer. N Engl J Med. 2020;383(18):1711–1723. doi:10.1056/NEJMoa2027071
57. Tsuboi M, Herbst RS, John T, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med. 2023;389(2):137–147. doi:10.1056/NEJMoa2304594
58. John T, Grohé C, Goldman JW, et al. Three-year safety, tolerability, and health-related quality of life outcomes of adjuvant osimertinib in patients with resected stage IB to IIIA EGFR-mutated NSCLC: updated analysis from the phase 3 ADAURA trial. J Thorac Oncol. 2023;18(9):1209–1221. doi:10.1016/j.jtho.2023.05.015
59. Li Z, Zhang X, Wang Y, et al. Adjuvant therapy in completely resected, EGFR-mutant non-small cell lung cancer: a comparative analysis of treatment efficacy between EGFR-TKI and anti-PD-1/PD-L1 immunotherapy. J ImmunoTher Cancer. 2023;11(10):e007327. doi:10.1136/jitc-2023-007327
60. Lee JM, McNamee CJ, Toloza E, et al. Neoadjuvant targeted therapy in resectable NSCLC: current and future perspectives. J Thorac Oncol. 2023;18(11):1458–1477. doi:10.1016/j.jtho.2023.07.006
61. Yu Z, Xu F, Zou J. Feasibility and safety of EGFR-TKI neoadjuvant therapy for EGFR-mutated NSCLC: a meta-analysis. Eur J Clin Pharmacol. 2024;80(4):505–517. doi:10.1007/s00228-024-03620-w
62. Zhong W-Z, Chen K-N, Chen C, et al. Erlotinib versus gemcitabine plus cisplatin as neoadjuvant treatment of stage IIIA-N2 EGFR-mutant non–small-cell lung cancer (EMERGING-CTONG 1103): a randomized phase II study. J Clin Oncol. 2019;37(25):2235–2245. doi:10.1200/JCO.19.00075
63. Lv C, Fang W, Wu N, et al. Osimertinib as neoadjuvant therapy in patients with EGFR-mutant resectable stage II-IIIB lung adenocarcinoma (NEOS): a multicenter, single-arm, open-label phase 2b trial. Lung Cancer. 2023;178:151–156. doi:10.1016/j.lungcan.2023.02.011
64. Shao W, Liu Z, Li B, et al. Neoadjuvant targeted therapy versus targeted combined with chemotherapy for resectable EGFR-mutant non–small cell lung cancer: a retrospective controlled real-world study. Front Oncol. 2024;14:1349300. doi:10.3389/fonc.2024.1349300
65. Marjanski T, Dziedzic R, Kowalczyk A, Rzyman W. Safety of surgery after neoadjuvant targeted therapies in non-small cell lung cancer: a narrative review. Int J Mol Sci. 2021;22(22):12244. doi:10.3390/ijms222212244
66. Tsuboi M, Weder W, Escriu C, et al. Neoadjuvant osimertinib with/without chemotherapy versus chemotherapy alone for EGFR-mutated resectable non-small-cell lung cancer: neoADAURA. Future Oncol. 2021;17(31):4045–4055. doi:10.2217/fon-2021-0549
67. Agrawal P, Rotow JK, Rocco G, et al. Outcomes with neoadjuvant chemotherapy and/or osimertinib in patients with EGFR- mutant resectable non-small cell lung cancers. Am Soc Clin Oncol. 2025;43:8052. doi:10.1200/JCO.2025.43.16_suppl.8052
68. Passaro A, Leighl N, Blackhall F, et al. ESMO expert consensus statements on the management of EGFR mutant non-small-cell lung cancer. Ann Oncol. 2022;33(5):466–487. doi:10.1016/j.annonc.2022.02.003
69. Xia L, Mei J, Kang R, et al. Perioperative ctDNA-based molecular residual disease detection for non–small cell lung cancer: a prospective multicenter cohort study (LUNGCA-1). Clin Cancer Res. 2022;28(15):3308–3317. doi:10.1158/1078-0432.CCR-21-3044
70. Ohara S, Suda K, Sudhaman S, et al. Clinical significance of perioperative minimal residual disease detected by circulating tumor DNA in patients with lung cancer with a long follow-up data: an exploratory study. JTO Clin Res Rep. 2025;6(3):100762. doi:10.1016/j.jtocrr.2024.100762
71. Wang B, Zou B, Xu S, et al. Postoperative ctDNA detection predicts relapse but has limited effects in guiding adjuvant therapy in resectable stage I NSCLC. Front Oncol. 2023;13:1083417. doi:10.3389/fonc.2023.1083417
72. Cao D, Zhou Q, Fan X, et al. Individualized tumor-informed circulating tumor DNA analysis for molecular residual disease detection in predicting recurrence and efficacy of adjuvant chemotherapy in colorectal cancer. Am Soc Clin Oncol. 2024;42:3615. doi:10.1200/JCO.2024.42.16_suppl.3615
73. Abbosh C, Birkbak NJ, Wilson GA, et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature. 2017;545(7655):446–451. doi:10.1038/nature22364
74. Wang Y, Shao W, Li H, et al. Clinical application of minimal residual disease detection by ctDNA testing in non-small cell lung cancer: a narrative review. Transl Lung Cancer Res. 2025;14(3):1007. doi:10.21037/tlcr-24-942
75. Abbosh C, Hodgson D, Doherty GJ, et al. Implementing circulating tumor DNA as a prognostic biomarker in resectable non-small cell lung cancer. Trends Cancer. 2024;10(7):643–654. doi:10.1016/j.trecan.2024.04.004
76. Dong S, Yan B, Liu S-Y, et al. Monitoring of circulating tumor DNA and indication of de-escalation adjuvant targeted therapy for EGFR-mutated NSCLC after complete resection. JTO Clin Res Rep. 2025;6(1):100758. doi:10.1016/j.jtocrr.2024.100758
77. Herbst RS, John T, Grohé C, et al. Molecular residual disease analysis of adjuvant osimertinib in resected EGFR-mutated stage IB–IIIA non-small-cell lung cancer. Nat Med. 2025;1–11.
78. Tie J, Cohen JD, Lahouel K, et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage II colon cancer. N Engl J Med. 2022;386(24):2261–2272. doi:10.1056/NEJMoa2200075
79. Dong S, Wang Z, Zhang J-T, et al. Circulating tumor DNA-guided de-escalation targeted therapy for advanced non− small cell lung cancer: a nonrandomized controlled trial. JAMA Oncol. 2024;10(7):932–940. doi:10.1001/jamaoncol.2024.1779
80. Ohara S, Suda K, Tsutani Y. Utility and future perspectives of circulating tumor DNA analysis in non-small cell lung cancer patients in the era of perioperative chemo-immunotherapy. Cells. 2025;14(17):1312. doi:10.3390/cells14171312
81. Petrella F, Cara A, Cassina EM, et al. Perioperative strategies in resectable non-squamous non-small cell lung cancer with EGFR mutations and ALK rearrangement. Cancers. 2025;17(11):1844. doi:10.3390/cancers17111844
82. Wu Y-L, Dziadziuszko R, Ahn JS, et al. Alectinib in resected ALK-positive non–small-cell lung cancer. N Engl J Med. 2024;390(14):1265–1276. doi:10.1056/NEJMoa2310532
83. Avrillon V, Pérol M. Alectinib for treatment of ALK-positive non-small-cell lung cancer. Future Oncol. 2016;13(4):321–335. doi:10.2217/fon-2016-0386
84. Goldman JW, Sands J, Hallqvist A, et al. LIBRETTO-432: A Phase 3 Study of Adjuvant Selpercatinib or Placebo in Stage IB-IIIA RET Fusion-Positive (RET+) NSCLC. American Society of Clinical Oncology; 2024.
85. Wolf J, Hochmair M, Han J-Y, et al. Capmatinib in MET exon 14-mutated non-small-cell lung cancer: final results from the open-label, phase 2 GEOMETRY mono-1 trial. Lancet Oncol. 2024;25(10):1357–1370. doi:10.1016/S1470-2045(24)00441-8
86. Lee JM, Awad MM, Saliba T, Caro N, Banerjee H, Kelly K. Abstract CT547: Neoadjuvant and adjuvant capmatinib in resectable non-small cell lung cancer with MET exon 14 skipping mutation or high MET amplification: GEOMETRY-N trial. Cancer Res. 2022;82(12_Supplement):CT547–CT547. doi:10.1158/1538-7445.AM2022-CT547
87. de Langen AJ, Johnson ML, Mazieres J, et al. Sotorasib versus docetaxel for previously treated KRAS G12C–mutated non–small–cell lung cancer: a plain language summary. Future Oncol. 2025;21(9):1033–1044. doi:10.1080/14796694.2025.2474789
88. Barlesi F, Yao W, Duruisseaux M, et al. Adagrasib versus docetaxel in KRASG12C-mutated non-small-cell lung cancer (KRYSTAL-12): a randomised, open-label, phase 3 trial. Lancet. 2025;406(10503):615–626. doi:10.1016/S0140-6736(25)00866-9
89. Shaverdashvili K, Burns TF. Advances in the treatment of KRASG12C mutant non–small cell lung cancer. Cancer. 2025;131:e35783.
90. Scott S, Hu C, Smith K, et al. EP02. 04-007 phase 2 trial of neoadjuvant KRASG12C directed therapy with adagrasib (MRTX849) with or without nivolumab in resectable NSCLC (Neo-KAN). J Thorac Oncol. 2022;17(9):S235. doi:10.1016/j.jtho.2022.07.392
91. Voruganti T, Marar R, Bleiberg B, et al. Perioperative therapy in oncogene-driven non–small cell lung cancer: current strategies and unanswered questions. Am Soc Clin Oncol Educat Book. 2025;45(3):e472804. doi:10.1200/EDBK-25-472804
92. Teodonio L, Peritore V, Andreetti C. Current indications for surgery in patients with lung cancer after neoadjuvant targeted therapy: a systematic review. Updates Surg. 2025;77:1–11. doi:10.1007/s13304-025-02116-1
93. Spicer JD, Cascone T, Wynes MW, et al. Neoadjuvant and adjuvant treatments for early stage resectable NSCLC: consensus recommendations from the International Association for the Study of Lung Cancer. J Thorac Oncol. 2024;19(10):1373–1414. doi:10.1016/j.jtho.2024.06.010
94. Iimura Y, Iihara H, Saito Y, et al. Epidermal growth factor receptor inhibitor-related skin toxicities: a review of management and possible preventive and therapeutic approaches for Asian patients by the Japanese Pharmacist-led Oncodermatology Study Team. Int J Clin Oncol. 2025;1–16.
95. Smith SM. Positive quality intervention: managing egfr inhibitor induced rash.
96. Wydad N, Mariem H, Chaimae A, et al. Cutaneous toxicity of anti-EGFR in NSCLC in the National Oncology Institute of Rabat: a literature review and a clinical case.
97. Daniela C-F, Pamela SP, T JG, et al. Management of diarrhea induced by EGFR-TKIs in advanced lung adenocarcinoma. Ther Adv Med Oncol. 2023;15.
98. Tao G, Chityala PK. Epidermal growth factor receptor inhibitor-induced diarrhea: clinical incidence, toxicological mechanism, and management. Toxicol Res. 2021;10(3):476–486. doi:10.1093/toxres/tfab026
99. Fukuda Y, Uchida Y, Ando K, Manabe R, Tanaka A, Sagara H. Risk factors for interstitial lung disease in patients with non-small cell lung cancer with epidermal growth factor receptor-tyrosine kinase inhibitors: a systematic review and meta-analysis. Respir Investigation. 2024;62(3):481–487. doi:10.1016/j.resinv.2024.03.007
100. Li MS, Lee KW, Mok KK, et al. Brief report: risk of recurrent interstitial lung disease from Osimertinib versus erlotinib rechallenge after symptomatic Osimertinib-induced interstitial lung disease. JTO Clin Res Rep. 2024;5(4):100648. doi:10.1016/j.jtocrr.2024.100648
101. Koch AL, Vellanki PJ, Drezner N, et al. FDA approval summary: osimertinib for adjuvant treatment of surgically resected non–small cell lung cancer, a Collaborative Project Orbis Review. Clin Cancer Res. 2021;27(24):6638–6643. doi:10.1158/1078-0432.CCR-21-1034
102. Maloney J, Wie C, Pew S, et al. Post-thoracotomy pain syndrome. Curr Pain Headache Rep. 2022;26(9):677–681. doi:10.1007/s11916-022-01069-z
103. Miyazaki T, Doi R, Matsumoto K. Post-thoracotomy pain syndrome in the era of minimally invasive thoracic surgery. J Thoracic Dis. 2024;16(5):3422. doi:10.21037/jtd-24-158
104. Gorji M, Joseph J, Pavlakis N, Smith SD. Prevention and management of acneiform rash associated with EGFR inhibitor therapy: a systematic review and meta‐analysis. Asia-Pacific J Clin Oncol. 2022;18(6):526–539. doi:10.1111/ajco.13740
105. Chen X, Nie X, Lin X, et al. Regulation of keratinocyte barrier function and inflammatory response by the EGFR-STAT3 pathway: potential therapeutic implications of osimertinib and Afatinib. Cytokine. 2025;185:156802. doi:10.1016/j.cyto.2024.156802
106. Borges JP, Mekhail K, Fairn GD, Antonescu CN, Steinberg BE. Modulation of pathological pain by epidermal growth factor receptor. Front Pharmacol. 2021;12:642820. doi:10.3389/fphar.2021.642820
107. Ríos-León M, Taylor J, Segura-Fragoso A, Barriga-Martín A. Usefulness of the DN4, S-LANSS, and painDETECT screening questionnaires to detect the neuropathic pain components in people with acute whiplash-associated disorders: a cross-sectional study. Pain Med. 2024;25(5):344–351. doi:10.1093/pm/pnad165
108. Lefaucheur J-P. The intrinsic reason why LANSS, DN4, and PainDETECT questionnaires cannot distinguish neuropathic pain from nociplastic pain. Front Pain Res. 2025;6:1658126. doi:10.3389/fpain.2025.1658126
109. Batchelor TJ, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91–115. doi:10.1093/ejcts/ezy301
110. Rabinovich EP, Martin LW. Getting patients to adjuvant therapy after lung cancer resection: ERAS protocols and return to intended oncologic therapy. J Thoracic Cardiovasc Surg. 2025;169(5):1367–1372. doi:10.1016/j.jtcvs.2024.10.007
111. Makkad B, Heinke TL, Sheriffdeen R, et al. Practice advisory for postoperative pain management of thoracic surgical patients: executive summary: a report from the society of cardiovascular anesthesiologists. J Cardiothorac Vasc Anesthesia. 2025;39(4):880–888. doi:10.1053/j.jvca.2024.12.003
112. Bradley N, McConnell T, Blair C, et al. Integrated palliative care and oncology: a realist synthesis. BMC Med. 2025;23(1):272. doi:10.1186/s12916-025-04083-1
113. Hori T, Yamamoto K, Ito T, Ikushima S, Omura T, Yano I. Effect of early dose reduction of osimertinib on efficacy in the first-line treatment for EGFR-mutated non-small cell lung cancer. Invest New Drugs. 2024;42(3):281–288. doi:10.1007/s10637-024-01432-4
114. Kruithof PD, Brouns AJ, Degens JH, et al. Osimertinib dose optimization guided by therapeutic drug monitoring in patients with EGFR-mutated advanced non-small cell lung cancer: a case series. Clin Lung Cancer. 2025;26:e496–e502. doi:10.1016/j.cllc.2025.05.012
115. Pe M, Voltz-Girolt C, Bell J, et al. Using patient-reported outcomes and health-related quality of life data in regulatory decisions on cancer treatment: highlights from an EMA-EORTC workshop. Lancet Oncol. 2025;26(6):687–690. doi:10.1016/S1470-2045(25)00150-0
116. Bhatnagar V, Dutcus C, Ghiorghiu S, et al. Supporting a patient-centric approach to dose optimization in oncology: the essential role of patient-reported outcomes (PROs): friends of cancer research; 2022.
117. Syed O, Nemr C, O’Donnell R, Knezevic NN. Risk factors for chronic post-surgical pain following orthopedic surgery “Who’s at risk”. Curr Anesthesiol Rep. 2024;15(1):3. doi:10.1007/s40140-024-00668-3
118. Veccia A, Dipasquale M, Lorenzi M, et al. Osimertinib in the treatment of epidermal growth factor receptor-mutant early and locally advanced stages of non-small-cell lung cancer: current evidence and future perspectives. Cancers. 2025;17(4):668.
119. Sami ER, Sabeshan P, Datta I, et al. 84 National Real World Study of adjuvant osimertinib in resected EGFR mutated lung cancer. Lung Cancer. 2024;190.
120. Thalia A, Wontumi S, Achim T, et al. 85 Assessing tolerability and toxicity of adjuvant Osimertinib following tumour resection of early-stage EGFR-mutated non-small cell lung cancer through real-world data. Lung Cancer. 2024;190.
121. Ihara Y, Yamamoto S, Mizutani M, Akiyama S, Okada N, Shimomura Y. Risk factors for lower adherence to epidermal growth factor receptor tyrosine kinase inhibitors for non-small cell lung cancer: a nationwide retrospective cohort study in Japan. Oncology. 2025;1–10. doi:10.1159/000548812
122. Wen M-J, Hsu H-L, Chang C-L, et al. Understanding the medication experience of patients with advanced non-small cell lung cancer taking epidermal growth factor receptor-tyrosine kinase inhibitors: a phenomenological study. PLoS One. 2023;18(5):e0286333. doi:10.1371/journal.pone.0286333
123. Yi H, Ou-Yang X, Hong Q, et al. Patient-reported outcomes in lung cancer surgery: a narrative review. Asian J Surg. 2025;48(1):40–48. doi:10.1016/j.asjsur.2024.07.304
124. Xu J, Ni H, Zhan H, et al. Efficacy of digital therapeutics for perioperative management in patients with lung cancer: a randomized controlled trial. BMC Med. 2025;23(1):186. doi:10.1186/s12916-025-04012-2
125. Wu D, Dai J, Sheng Y, et al. Evidence summary on pain management in thoracoscopic lung cancer surgery. Asia PacJ Oncol Nurs. 2025;12:100693. doi:10.1016/j.apjon.2025.100693
126. Yin J, Zhou J, Cao L, Chen G. Associations between postoperative pulmonary interventions based on enhanced recovery programs and outcomes in patients with lung cancer: a retrospective propensity score matching study. Eur J Oncol Nurs. 2025;75:102817. doi:10.1016/j.ejon.2025.102817
127. Hu X, He X. Enhanced recovery of postoperative nursing for single-port thoracoscopic surgery in lung cancer patients. Front Oncol. 2023;13:1163338. doi:10.3389/fonc.2023.1163338
128. Anderson MK, Bettencourt EV, LeFebvre KB, editors. Defining the role and responsibilities of the oral anticancer medication nurse navigator. In: Seminars in Oncology Nursing. Elsevier; 2024.
129. Johnson LA. Oral oncolytic therapy and the oncology nurse navigator: maximizing patient education and follow-up. 2025.
130. He J, Tsuboi M, Weder W, et al. Neoadjuvant osimertinib for resectable EGFR-mutated non–small cell lung cancer. J Clin Oncol. 2025;JCO–25–00883.
131. Türk HM, Tsuboi M, Herbst R, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. 2023.
132. Khoury AL, Kolarczyk LM, Strassle PD, et al. Thoracic enhanced recovery after surgery: single academic center observations after implementation. Ann Thorac Surg. 2021;111(3):1036–1043. doi:10.1016/j.athoracsur.2020.06.021
133. Cohen JB, Smith BB, Teeter EG. Update on guidelines and recommendations for enhanced recovery after thoracic surgery. Curr Opin Anesthesiol. 2024;37(1):58–63. doi:10.1097/ACO.0000000000001328
134. Khoury AL, McGinigle KL, Freeman NL, El-Zaatari H, Feltner C, Long JM. Enhanced recovery after thoracic surgery: systematic review and meta-analysis. JTCVS Open. 2021;7:370. doi:10.1016/j.xjon.2021.07.007
135. Speth J. Guidelines in practice: implementation of enhanced recovery after surgery: earn 2.3 contact hours. AORN J. 2025;121(5):361–370. doi:10.1002/aorn.14332
136. Basch E, Rocque G, Mody G, Mullangi S, Patt D. Tenets for implementing electronic patient-reported outcomes for remote symptom monitoring during cancer treatment. JCO Clin Cancer Inform. 2023;7:e2200187. doi:10.1200/CCI.22.00187
137. Hassett M, Dias S, Cronin C, et al. Strategies for implementing an electronic patient-reported outcomes-based symptom management program across six cancer centers. BMC Health Serv Res. 2024;24(1):1386. doi:10.1186/s12913-024-11536-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.