Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Perioperative Blood Pressure Optimization to Improve Outcomes in Orthopedic Patients: A Clinical Review
Authors Yang YF, Ma X, Ahmad MA, Lee P, Qin Y, Ji FH ![]() , Sudhan N, Peng K
, Sudhan N, Peng K ![]()
Received 15 September 2025
Accepted for publication 30 November 2025
Published 8 December 2025 Volume 2025:21 Pages 1667—1677
DOI https://doi.org/10.2147/TCRM.S567548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Yu-fan Yang,1,2,* Xiaqing Ma,3,4,* Mudussar Abrar Ahmad,5 Paul Lee,6 Yibin Qin,3 Fu-hai Ji,1,2 Nazneen Sudhan,4 Ke Peng1,2,4
1Department of Anesthesiology, First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Institute of Anesthesiology, Soochow University, Suzhou, Jiangsu, People’s Republic of China; 3Department of Anesthesiology, Affiliated Hospital of Nantong University, Medical School of Nantong University, Nantong, Jiangsu, People’s Republic of China; 4Department of Anesthesia and Intensive Care, Barking Havering and Redbridge University Hospitals NHS Trust, Romford, UK; 5Department of Orthopedics, Barking Havering and Redbridge University Hospitals NHS Trust, Romford, UK; 6College of Health and Science, University of Lincoln, Lincoln, UK
*These authors contributed equally to this work
Correspondence: Ke Peng, Email [email protected] Nazneen Sudhan, Email [email protected]
Abstract: Perioperative blood pressure fluctuations significantly contribute to postoperative complications in orthopedic surgery, particularly among high-risk patients. This clinical review synthesizes current evidence on individualized blood pressure management across the perioperative continuum, highlighting procedure-specific risks such as bone cement implantation syndrome, tourniquet-induced hemodynamic changes, and cerebral hypoperfusion in the beach-chair position. Special considerations for vulnerable populations, including frail elderly and anticoagulated patients, are discussed to balance bleeding and thrombotic risks. Maintaining mean arterial pressure within 10– 20% of baseline through tailored anesthesia, goal-directed fluid therapy, and continuous monitoring is associated with improved outcomes. A multidisciplinary, risk-stratified approach is recommended to reduce perioperative morbidity and improve postoperative outcomes. Future research should validate personalized blood pressure targets and explore the role of advanced hemodynamic monitoring in enhancing patient safety.
Keywords: perioperative blood pressure, cardiovascular risk, orthopedic surgery, high-risk patients, hemodynamic monitoring, patient safety
Introduction
Orthopedic surgery is one of the most frequently performed procedures worldwide, with millions of joint arthroplasties, spinal reconstructions, limb operations, and trauma-related interventions annually.1–3 Blood pressure instability in the perioperative period (encompassing preoperative, intraoperative, and postoperative phases) is a well-established yet potentially modifiable risk factor for adverse outcomes, particularly among older adults with multiple cardiovascular comorbidities. Both hypertensive peaks and hypotensive episodes have been independently associated with myocardial injury, stroke, acute kidney injury, cognitive decline, prolonged hospitalization, and death.4–7
Unique intraoperative challenges in orthopedic surgery such as bone cement implantation, beach-chair positioning, and tourniquet inflation–deflation sequences may trigger abrupt hemodynamic changes that exceed the autoregulatory reserve of vital organs. These factors directly disrupt vascular dynamics or alter organ perfusion pressure, making hemodynamic stresses more prominent compared to other surgical fields. These procedure-specific risks are often under-recognized in routine anesthesia practice, yet they represent critical windows for systemic inflammatory responses and cardiovascular events.8–10 Consequently, the traditional “one-size-fits-all” approach to blood pressure management is inadequate for orthopedic patients.
We searched PubMed, Embase, and Cochrane Library databases using keywords including perioperative blood pressure, orthopedic surgery, hemodynamic management, and complications. Inclusion criteria were clinical reviews, randomized controlled trials, and cohort studies. Two authors independently screened literature, extracted data, and resolved discrepancies through discussion. Recent reviews (2021–2025) on this topic mainly focus on single procedures (eg, joint arthroplasty) or specific populations (eg, geriatric patients), lacking a comprehensive analysis of multiple orthopedic procedures and integrated risk-stratified management.2,11–13 This review focuses on summarizing evidence published in the past 25 years (2001–2025) on perioperative blood pressure management in orthopedic surgery. It emphasizes procedure-specific hemodynamic challenges and risk-stratified strategies for vulnerable populations, addressing gaps in existing reviews that lack integrated analysis of both procedure and patient characteristics.
This clinical review synthesizes current evidence on perioperative blood pressure optimization in orthopedic surgery across three domains: (1) procedure-specific hemodynamic signatures (cemented arthroplasty, beach-chair position, spinal surgery, limb tourniquet use, and major trauma); (2) risk-stratified targets for vulnerable patients (hypertensive, geriatric frail, anticoagulated, and chronic kidney disease); and (3) integrated roles of anesthesia techniques, goal-directed fluid therapy, multimodal analgesia, and advanced monitoring in preserving end-organ perfusion and improving overall surgical safety.
Blood Pressure Fluctuations in Orthopedic Surgery
Orthopedic surgery exposes patients to unique perioperative hemodynamic stresses. Table 1 provides a concise overview of these scenarios, the pathophysiology, and evidence-based countermeasures.
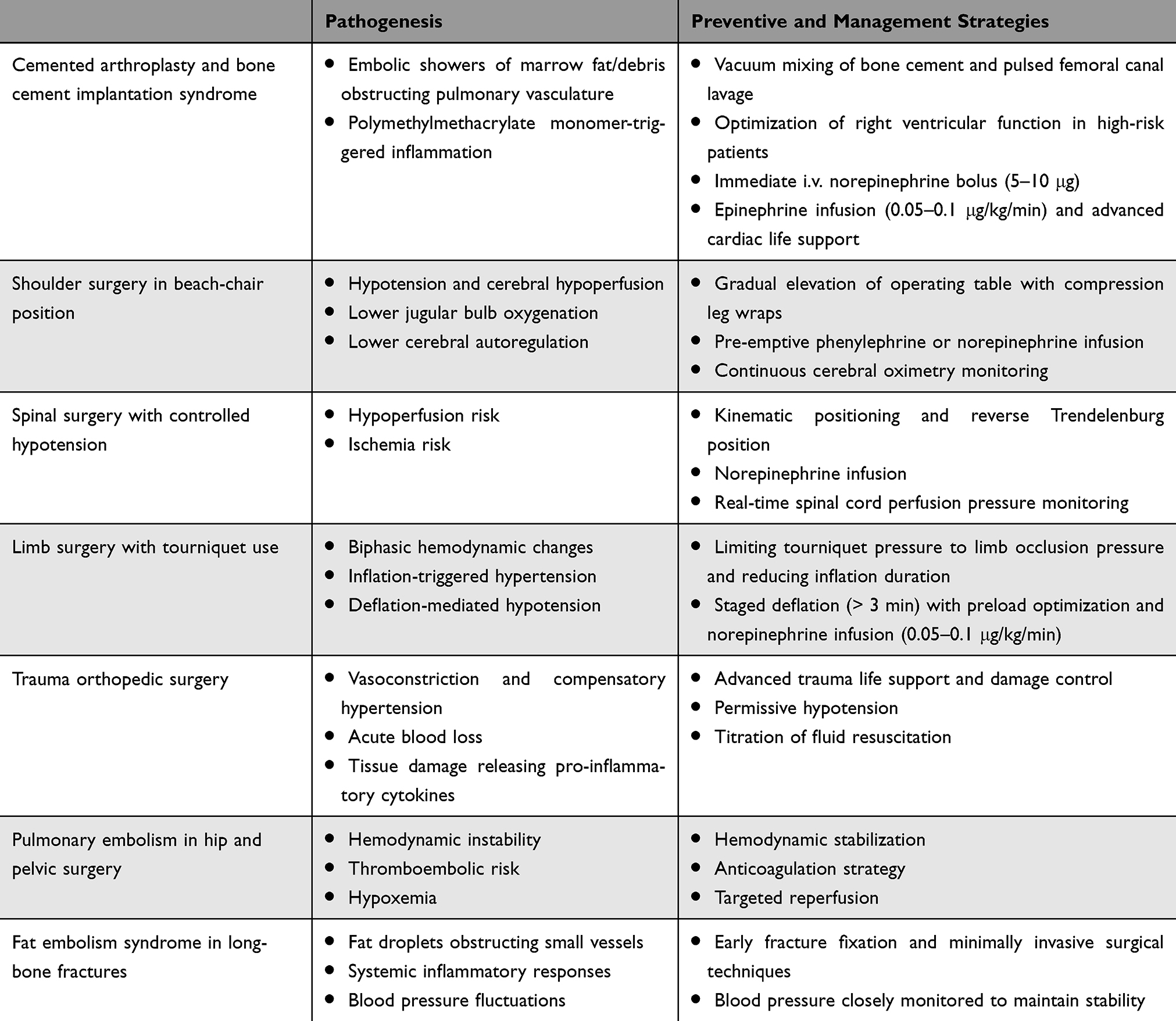 |
Table 1 Summary of Blood Pressure Fluctuations in Orthopedic Surgery |
Cemented Arthroplasty and Bone Cement Implantation Syndrome
Bone cement implantation syndrome is a critical challenge in cemented arthroplasty, characterized by acute hypotension (> 30% decrease in mean arterial pressure [MAP]), hypoxemia (SpO2 < 90%), and cardiac instability (arrhythmias, cardiac arrest) within minutes of cement insertion.13–16 Embolic showers of marrow fat and debris obstruct the pulmonary vasculature, while polymethylmethacrylate monomer triggers complement activation (C3a/C5a anaphylatoxins) and histamine release, leading to pulmonary vasoconstriction, right ventricular failure, and systemic vasodilation.
Preventive strategies include vacuum mixing of cement, pulsed lavage of the femoral canal, and echocardiographic exclusion of pulmonary hypertension in high-risk patients.11,17 Treatment mandates immediate norepinephrine (5–10 μg bolus) rather than phenylephrine, as norepinephrine combines α-mediated vasoconstriction with β-mediated inotropy to counter pulmonary hypertension. Refractory cases require epinephrine infusion (0.05–0.1 μg/kg/min) and advanced life support.
Shoulder Surgery in Beach-Chair Position
For patients undergoing shoulder surgery, beach-chair position (elevating the patient’s upper body to 30–60°) is associated with decreased regional brain oxygenation, reduced cerebral blood flow, lower jugular bulb oxygenation, impaired cerebral autoregulation, and neurological complications.18–21 A study suggested that for patients receiving sevoflurane anesthesia in the beach-chair position, cerebral blood flow was maintained only when MAP exceeded 70 mmHg, consistent with the intact cerebral autoregulation. Older patients and individuals with known cerebrovascular disease are at increased risks; neurological deficits can appear hours after surgery even when perioperative vital signs seem stable.
To mitigate these risks, anesthesia management includes gradual table elevation with compression leg wraps to preserve venous return, pre-emptive phenylephrine or norepinephrine infusion initiated before positioning to stabilize MAP ≥ 70 mmHg, and continuous cerebral oximetry monitoring employed with an alert threshold set at 20% reduction from baseline. If cerebral desaturation occurs, immediate interventions include increasing FiO2, raising MAP, or repositioning the head to improve jugular drainage.
Spinal Surgery with Controlled Hypotension
Deliberate reduction of mean arterial pressure (MAP 65–70 mmHg) is frequently employed in spinal surgery to minimize bleeding, improve the operative field, and prevent spinal cord hypoperfusion.12,22 Prone positioning and cerebrospinal fluid drainage lower spinal cord perfusion pressure (SCCP; MAP – cerebrospinal fluid pressure); when SCPP falls below 60 mmHg, motor-evoked potentials deteriorate and ischemic injury risk rises markedly. A study showed that controlled hypotension with combined use of dexmedetomidine and nicardipine achieved this goal more effectively than nicardipine alone, providing steadier hemodynamics and less blood loss in older patients undergoing spinal surgery.23
To balance surgical visibility and neuroprotection, strategies include: (1) kinematic positioning with abdominal decompression and reverse Trendelenburg to optimize venous return; (2) low-dose norepinephrine infusion to maintain MAP ≥ 65 mmHg and improve spinal cord microcirculation under continuous neuromonitoring with motor-evoked potentials; and (3) maintaining MAP > 85 mmHg in spinal cord injury to prevent secondary ischemia.24,25 Additionally, multimodal intraoperative neurophysiological monitoring (somatosensory and motor evoked potentials) can guide anesthetic care, minimize the risk of secondary spinal cord injury, and improve postoperative outcomes.26
Limb Surgery with Tourniquet Use
Tourniquet use is a common practice in knee or limb surgery to minimize intraoperative bleeding and enhance surgical visibility. However, tourniquet use can induce biphasic hemodynamic changes: inflation-triggered hypertension from sympathetic/renin-angiotensin activation, and deflation-mediated hypotension via nitric oxide surge and metabolic acidosis. These fluctuations increase myocardial strain and cerebral hypoperfusion risks, particularly in patients with coronary or cerebrovascular disease.
Current practice therefore limits cuff pressure to 40–80 mmHg above limb-occlusion pressure and duration to < 120 minutes, employs staged deflation (> 3 min) with preload optimization (eg, crystalloid 500 mL), and initiates a norepinephrine infusion (0.05–0.1 μg/kg/min) before release to maintain blood pressure and counter acidosis-induced myocardial suppression.27 Recent studies have reported that femoral artery block or adjuncts such as lidocaine or ketamine to general anesthesia attenuated tourniquet-induced hypertension without prolonging recovery.28–30
Trauma Orthopedic Surgery
Traumatic injury activates the sympathetic-adrenal axis, triggering a massive release of catecholamines (epinephrine and norepinephrine) and cytokines (such as tumor necrosis factor-α and interleukin-6) into the circulation; this produces vasoconstriction, compensatory hypertension, and a hyper-inflammatory state that increases myocardial oxygen demand while promoting microvascular leak and systemic vasodilation.31 Concurrent hemorrhage reduces effective circulating volume, activates the renin–angiotensin system, and further destabilizes blood pressure. A recent study showed that enhanced inflammatory responses were associated with a higher mortality in geriatric trauma patients.32
The recommended resuscitation strategy for multiply injured patients includes advanced trauma life support and damage control surgery.33 According to the National Institute for Health and Care Excellence guidelines, for patients with hemorrhagic injury and active bleeding, a restrictive approach to titrate volume resuscitation is applied to maintain central circulation (MAP 50 mmHg) until early control of bleeding is achieved.34 Data from a meta-analysis confirmed that the permissive hypotension approach, compared to conventional resuscitation, improved 30-day or in-hospital mortality, and reduced blood loss and blood product utilizations for adults with hemorrhagic shock.35
Pulmonary Embolism in Hip and Pelvic Surgery
Pulmonary embolism in hip and pelvic surgery typically presents with sudden, otherwise unexplained hypotension, refractory tachycardia, or syncope; hypoxemia and pleuritic chest pain may follow but are often delayed. Orthopedic-specific triggers such as bone cement-induced endothelial injury, limb immobilization, and tourniquet-induced fibrinolytic inhibition augment Virchow’s triad, leading to right ventricular failure and obstructive shock.36
Prevention centers on pharmacological thromboprophylaxis tailored to bleeding risk: low-molecular-weight heparin, direct oral anticoagulants, and intermittent pneumatic compression. Intraoperative meticulous cementing technique, early tourniquet release, and maintaining MAP > 65 mmHg can limit additional embolic load. Once pulmonary embolism is suspected, management priorities are (1) immediate hemodynamic support (oxygen, cautious fluid loading, and norepinephrine infusion titrated to MAP > 65 mmHg); (2) anticoagulation after surgical hemostasis (eg, rivaroxaban initiation after blood pressure control); and (3) targeted reperfusion with catheter-directed thrombolysis or systemic thrombolysis in massive pulmonary embolism with shock.37,38 In a recent multicenter trial, prophylaxis with enoxaparin, compared with aspirin, reduced the incidence of symptomatic venous thromboembolism including pulmonary embolism within 90 days after hip or knee arthroplasty.39
Fat Embolism Syndrome in Long-Bone Fractures
Fat embolism syndrome is a potentially lethal complication of long-bone fractures, intramedullary nailing, and joint arthroplasty. Mechanical disruption of bone marrow releases fat droplets that traverse the venous circulation and lodge in pulmonary arterioles, while enzymatic lipolysis generates toxic free fatty acids that trigger a systemic inflammatory response.40 Clinically, the syndrome presents with the classic triad of respiratory distress, altered mental status, and petechial rash, often accompanied by abrupt hypotension and fever; onset is typically 12–72 h after injury or instrumentation. The relationship between fat embolism and blood pressure is bidirectional: hypertension may elevate intramedullary pressure, facilitating the entry of more fat droplets into the circulation, whereas fat embolism syndrome also causes blood pressure fluctuations.
Early fracture fixation, meticulous intramedullary decompression, and minimally invasive surgical techniques reduce embolic load. Intraoperative strict blood pressure control, avoiding both hypertensive spikes that raise intramedullary pressure and hypotensive episodes that exacerbate tissue hypoperfusion, is essential, particularly in older or frail patients. Established fat embolism syndrome is managed supportively: high-flow oxygen or mechanical ventilation for respiratory failure, judicious fluid resuscitation to maintain MAP > 65 mmHg, and prompt correction of coagulopathy or acidosis. Corticosteroids remain controversial and are reserved for severe cases refractory to conventional therapy.
Blood Pressure Management in High-Risk Patients
Figure 1 presents an algorithm that outlines the personalized blood-pressure management for hypertensive, geriatric frail, anticoagulated, and chronic kidney disease patients.
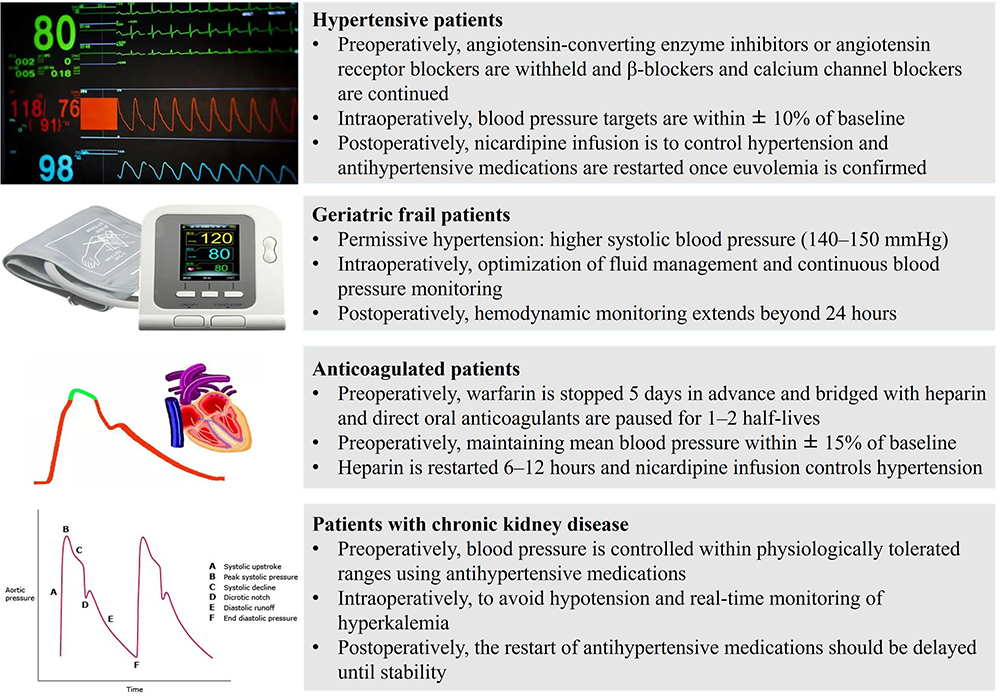 |
Figure 1 Perioperative blood pressure management in high-risk patients undergoing orthopedic surgery. |
Hypertensive Patients
Hypertensive orthopedic patients require tailored blood pressure management to mitigate their elevated risks of hemodynamic fluctuations and postoperative cardiovascular events. Preoperative planning focuses on preventing intraoperative hypotension while avoiding rebound hypertension. Angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) are typically withheld on the morning of surgery, and β-blockers and calcium channel blockers are continued to avoid rebound hypertension. According to the recent Stop-or-Not randomized clinical trial, while postoperative complications were not influenced, an ACEIs/ARBs discontinuation strategy can be considered to reduce the risk of intraoperative hypotension.41
Intraoperative MAP is targeted within ± 10% of the patient’s baseline, a strategy validated by the INPRESS trial that reduced postoperative organ dysfunction compared with standard care.42 Postoperatively, nicardipine infusion is titrated to control rebound hypertension (systolic blood pressure [SBP] > 160 mmHg); antihypertensive medications including ACEIs/ARBs are then restarted once euvolemia is confirmed. In patients with coronary artery disease, diastolic blood pressure is maintained > 70 mmHg to preserve coronary perfusion.43 These approaches represent a paradigm shift from rigid normotension towards physiologic individualization, acknowledging the altered autoregulation thresholds in chronic hypertension.
Geriatric Frail Patients
Frail elders (Clinical Frailty Scale ≥ 5) undergoing orthopedic surgery present unique hemodynamic challenges due to age-related and frailty-associated impairments, including blunted autonomic regulation, diminished cardiac reserve, and right-shifted cerebral and renal autoregulation.44 These factors necessitate a judicious hemodynamic management paradigm including permissive hypertension (higher SBP targets of 140–150 mmHg), intraoperative precision management (avoiding any MAP decrease > 20% from baseline), and extended postoperative vigilance.
Intraoperative management utilizes low-dose norepinephrine (0.02–0.05 μg/kg/min) to support vasomotor tone, continuous arterial monitoring to detect occult hypotension, and cautious fluid titration to maintain euvolemia.45,46 Hemodynamic monitoring extends beyond 24 h postoperatively to capture blood pressure fluctuations, and antihypertensive therapy is restarted after 24-h stability and confirmed euvolemia, ensuring perfusion remains within the individual’s shifted, higher autoregulatory range. A multidisciplinary approach involving anesthetists, surgeons, cardiologists, and geriatricians to tailor perioperative management optimizes patient outcomes.
Anticoagulated Patients
Anticoagulated patients undergoing orthopedic surgery face unique challenges in blood pressure management due to a thrombosis-bleeding paradox. Common anticoagulants include warfarin, direct oral anticoagulants (DOACs) such as dabigatran, rivaroxaban and apixaban, and heparin derivatives. These medications prevent thrombin formation in the coagulation cascade but increase the risk of perioperative bleeding. Poor blood pressure control in patients with anticoagulant therapy may result in fatal events such as intracranial bleeding.47
Warfarin should be stopped 5 days preoperatively, with low-molecular-weight heparin (LMWH) bridging for high thrombotic risk, while DOACs are paused for 1–2 half-lives based on renal function.48 Intraoperative MAP should be maintained within ± 10% of baseline in cases with high bleeding risk, or up to ± 20% when hemostasis is secure. Postoperatively, LMWH can be restarted 6–12 hours after hemostasis is achieved. Nicardipine infusion provides smooth control of rebound hypertension without affecting heart rate. Maintaining stable blood pressure acts as the key safeguard, balancing the risks of bleeding and thrombosis throughout the perioperative period.
Patients with Chronic Kidney Disease
For patients with chronic kidney disease (CKD) undergoing orthopedic surgery, surgical stress and blood loss can exacerbate renal dysfunction. Meticulous blood pressure management is required due to the interplay between CKD, hypertension, and the potential for renal function deterioration. Preoperatively, blood pressure is controlled with ACEIs, ARBs, or calcium-channel blockers to a systolic range that the patient tolerates without orthostatic symptoms, while serum potassium and creatinine are rechecked within 48 hours of surgery.49 Careful monitoring is required as ACEIs/ARBs can potentially cause hyperkalemia and worsening renal function, especially in patients with advanced CKD.
Intraoperatively, the primary goals are to avoid hypotension, maintain adequate renal perfusion and oxygenation, and manage bleeding while preventing blood pressure fluctuations. Real-time monitoring and vigilance for hyperkalemia during tourniquet release are essential. Postoperatively, antihypertensives are reintroduced only after documented euvolemia and stable renal function, ensuring renal perfusion without exposing fragile capillaries to hypertensive stress. Moreover, perioperative care should exclude nephrotoxic agents and adopt kidney-sparing strategies.
Anesthesia and Analgesia on Blood Pressure Management
To consolidate the evidence, Table 2 summarizes the key anesthetic, analgesic, fluid, and monitoring strategies and their differential impact on perioperative blood pressure control.
 |
Table 2 Summary of Anesthesia and Analgesia on Blood Pressure Management |
Anesthesia Techniques
The choice of anesthetic modality exerts a pivotal influence on perioperative hemodynamics in orthopedic procedures. Regional anesthesia, including neuraxial and peripheral nerve blocks, reduces hypotension risk compared to general anesthesia, as the selective blockade maintains compensatory vasoconstriction in non-blocked vascular beds, preventing the systemic vasodilation and myocardial depression of general anesthetic drugs. In a multicenter study of older patients undergoing hip-fracture surgery, intraoperative hypotension occurred in 78.3% of those receiving general anesthesia versus 31.6% in the regional anesthesia group.50
Nevertheless, general anesthesia remains indispensable for complex spinal or trauma cases that require prone positioning or neuromonitoring. Balanced anesthesia that incorporates ketamine or esketamine offsets propofol- or volatile-induced vasodilation and reduces hypotension.51,52 For spinal fusion surgery, total intravenous anesthesia preserves motor-evoked-potential signals while permitting precise norepinephrine titration to maintain spinal-cord perfusion pressure. In the beach-chair position, an interscalene block blunts sympathetic responses to upright positioning and may prevent cerebral hypoperfusion.53 Interscalene block offers optimal analgesia for shoulder surgery, whereas suprascapular or supraclavicular blocks provide effective and safe alternatives.54
Fluid Therapy
Fluid therapy plays a crucial role in blood pressure management during orthopedic surgery. Liberal strategies exacerbate tissue edema and impair oxygenation, which is especially detrimental in spine surgery (increased orbital pressure) and cemented arthroplasty (reduced cement-bone interface strength). Different surgical procedures therefore demand different fluid therapies. In major orthopedic surgeries such as total hip replacement, spinal reconstruction, and pelvic tumour resection, substantial blood loss and fluid shift are common, and goal-directed fluid therapy (GDFT) is recommended to optimize blood volume, maintain microcirculation and organ perfusion, and reduce perioperative complications.55–57 Using dynamic indices such as stroke volume variation or pulse pressure variation, GDFT guides fluid administration and avoids both hypotension and hypertension. In less invasive arthroscopic cases such as arthroscopic procedures, a more restrictive strategy that balances intake and output prevents fluid overload.
Crystalloids remain the first-line resuscitation fluid, while colloids such as hydroxyethyl starch (HES) can be used in certain situations. Although the use of HES has been linked to acute kidney injury, recent meta-analyses showed it is safe and efficacious perioperatively and that a crystalloid-HES combination offers clinical benefits over crystalloid alone.58 Thus, fluid therapy should be tailored to the type of surgery, the patient’s condition, and real-time hemodynamic status.
Perioperative Analgesia
Uncontrolled postoperative pain triggers a sympathetic surge and catecholamine release that elevate heart rate and SBP, whereas excessive opioid administration induces vagotonic hypotension through histamine-mediated vasodilation and baroreflex suppression. Effective pain control therefore mitigates these hemodynamic threats, particularly after joint replacement or spinal fusion with moderate-to-severe pain. Multimodal analgesia combines regional techniques (spinal, epidural, and peripheral nerve blocks) with systemic analgesics including non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, gabapentinoids and patient-controlled analgesia. Regional techniques provide excellent analgesia with minimal hemodynamic changes, NSAIDs reduce inflammation without causing opioid-related instability, acetaminophen offers effective relief with negligible impacts on blood pressure, and patient-controlled analgesia allows precise titration while lowering the risk of opioid-induced adverse effects. Recent literature supports multimodal analgesia in orthopedic surgery to improve pain control, reduce postoperative opioid consumption, and enhance overall outcomes.59–61
Perioperative Blood Pressure Monitoring
Perioperative blood pressure monitoring is a critical aspect of managing patients undergoing orthopedic surgery. It ensures hemodynamic stability and helps in preventing complications associated with blood pressure fluctuations. Modern practice therefore favours high-resolution, beat-to-beat monitoring: continuous invasive arterial lines remain the gold standard, while non-invasive alternatives such as cleared finger-cuff devices (ClearSight®, Nexfin®) and volume-clamp technology yield MAP, systolic and diastolic readings within 5 mmHg of invasive standards.62–64 Based on continuous capture of data, personalized perioperative blood pressure management has gained attention as a method to improve outcomes. A recent study suggested maintaining intraoperative MAP above the preoperative mean nighttime MAP in patients having major non-cardiac surgery.65 This approach can be adapted to orthopedic surgery to tailor blood pressure targets to individual patient needs, potentially reducing the incidence of postoperative complications.
Conclusions
Optimizing perioperative blood pressure in orthopedic surgery is no longer a one-size-fits-all endeavour; it is a dynamic, patient-centered process that begins before anesthesia and extends well into the postoperative ward. By integrating procedure-specific insights with risk-stratified targets, clinicians can transform hemodynamic uncertainty into predictable control. Early recognition of cement-related instability, tourniquet-induced biphasic swings, and trauma-driven inflammatory surges, combined with personalized vasopressor regimens and vigilant monitoring, results in fewer myocardial injuries, strokes, and renal insults. Future research should focus on refining closed-loop vasopressor systems through animal studies, validating AI-driven algorithms using computer simulations, and embedding multidisciplinary pathways in clinical trials. By uniting anesthetists, surgeons, geriatricians, and nephrologists, we can offer proactive precision medicine, ultimately delivering safer surgery and faster functional restoration for every orthopedic patient.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (82471290 to KP), Suzhou Basic Research Pilot Project (SSD2024082 to KP), and 333 High-level Talent Training Project in Jiangsu Province ((2024)3-2272 to KP). The funders have no role in the study design, data collection, data analysis, interpretation, or writing of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jones CM, Potluri AS, Federico VP, et al. Trends in medicare arthroplasty procedure volume: projecting from 2025 to 2040. J Arthroplasty. 2025;40:2781–2790.e1. doi:10.1016/j.arth.2025.05.124
2. Yamout T, Orosz LD, Good CR, Jazini E, Allen B, Gum JL. Technological advances in spine surgery: navigation, robotics, and augmented reality. Orthop Clin North Am. 2023;54:237–246. doi:10.1016/j.ocl.2022.11.008
3. Dehghan N, McKee MD. What’s new in orthopaedic trauma. J Bone Joint Surg Am. 2019;101:1138–1143. doi:10.2106/JBJS.19.00327
4. Lizano-Diez I, Poteet S, Burniol-Garcia A, Cerezales M. The burden of perioperative hypertension/hypotension: a systematic review. PLoS One. 2022;17:e0263737. doi:10.1371/journal.pone.0263737
5. Fatani N, Dixon DL, Van Tassell BW, Fanikos J, Buckley LF. Systolic blood pressure time in target range and cardiovascular outcomes in patients with hypertension. J Am Coll Cardiol. 2021;77:1290–1299. doi:10.1016/j.jacc.2021.01.014
6. Gregory A, Stapelfeldt WH, Khanna AK, et al. Intraoperative hypotension is associated with adverse clinical outcomes after noncardiac surgery. Anesth Analg. 2021;132:1654–1665. doi:10.1213/ANE.0000000000005250
7. Gu WJ, Hou BL, Kwong JSW, et al. Association between intraoperative hypotension and 30-day mortality, major adverse cardiac events, and acute kidney injury after non-cardiac surgery: a meta-analysis of cohort studies. Int J Cardiol. 2018;258:68–73. doi:10.1016/j.ijcard.2018.01.137
8. Yang TH, Yang RS, Lin CP, Tseng TH. Bone cement implantation syndrome in bone tumor surgeries: incidence, risk factors, and clinical experience. Orthop Surg. 2021;13:109–115. doi:10.1111/os.12842
9. Aby K, Antony R, Li Y. ProBDNF upregulation in murine hind limb ischemia reperfusion injury: a driver of inflammation. Biology (Basel). 2023;13:12. doi:10.3390/biology13010012
10. Packialakshmi B, Stewart IJ, Burmeister DM, et al. Tourniquet-induced lower limb ischemia/reperfusion reduces mitochondrial function by decreasing mitochondrial biogenesis in acute kidney injury in mice. Physiol Rep. 2022;10:e15181. doi:10.14814/phy2.15181
11. Emara AK, Ng M, Krebs VE, Bloomfield M, Molloy RM, Piuzzi NS. Femoral stem cementation in hip arthroplasty: the know-how of a “lost. Art. Curr Rev Musculoskelet Med. 2021;14:47–59. doi:10.1007/s12178-020-09681-5
12. Ma RX, Qiao RQ, Xu MY, Li RF, Hu YC. Application of controlled hypotension during surgery for spinal metastasis. Technol Cancer Res Treat. 2022;21:15330338221105718. doi:10.1177/15330338221105718
13. Yang Y, Meng X, Huang Y. Study of the cement implantation syndrome: a review. Medicine (Baltimore). 2024;103:e38624. doi:10.1097/MD.0000000000038624
14. Armstrong RA, Cook TM, Kane AD, et al. Peri-operative cardiac arrest: management and outcomes of patients analysed in the 7th National Audit Project of the Royal College of Anaesthetists. Anaesthesia. 2024;79:31–42. doi:10.1111/anae.16157
15. Donaldson AJ, Thomson HE, Harper NJ, Kenny NW. Bone cement implantation syndrome. Br J Anaesth. 2009;102:12–22. doi:10.1093/bja/aen328
16. Weingartner K, Stormann P, Schramm D, et al. Bone cement implantation syndrome in cemented Hip hemiarthroplasty-a persistent risk. Eur J Trauma Emerg Surg. 2022;48:721–729. doi:10.1007/s00068-020-01587-8
17. Castro Pinto T, Seabra D, Castro A, Guedes C. Bone cement implantation syndrome: the role of echocardiography and multidisciplinarity. BMJ Case Rep. 2024;17.
18. Murphy GS, Greenberg SB, Szokol JW. Safety of beach chair position shoulder surgery: a review of the current literature. Anesth Analg. 2019;129:101–118. doi:10.1213/ANE.0000000000004133
19. Hanouz JL, Fiant AL, Gerard JL. Middle cerebral artery blood flow velocity during beach chair position for shoulder surgery under general anesthesia. J Clin Anesth. 2016;33:31–36. doi:10.1016/j.jclinane.2016.01.009
20. Hayashi K, Tanabe K, Minami K, Sakata K, Nagase K, Iida H. Effect of blood pressure elevation on cerebral oxygen desaturation in the beach chair position. Asian J Anesthesiol. 2017;55:13–16. doi:10.1016/j.aja.2017.05.007
21. Chan JH, Perez H, Lee H, Saltzman M, Marra G. Evaluation of cerebral oxygen perfusion during shoulder arthroplasty performed in the semi-beach chair position. J Shoulder Elbow Surg. 2020;29:79–85. doi:10.1016/j.jse.2019.05.022
22. Dutton RP. Controlled hypotension for spinal surgery. Eur Spine J. 2004;13 Suppl 1:S66–71. doi:10.1007/s00586-004-0756-7
23. Zhang X, Liu S. Combined use of dexmedetomidine and nicardipine provides better controlled hypotension in elderly patients undergoing orthopedic surgery. Asian J Surg. 2020;43:1126–1127. doi:10.1016/j.asjsur.2020.08.018
24. Nuwer MR, Schrader LM. Spinal cord monitoring. Handb Clin Neurol. 2019;160:329–344.
25. Yue JK, Tsolinas RE, Burke JF, et al. Vasopressor support in managing acute spinal cord injury: current knowledge. J Neurosurg Sci. 2019;63:308–317. doi:10.23736/S0390-5616.17.04003-6
26. Rebelo P, Sousa CP, Campos MT. The value of intraoperative neurophysiological monitoring during patient positioning in spine surgery: a preventive strategy. Cureus. 2024;16:e73662. doi:10.7759/cureus.73662
27. Salari P, Balato G, Cavallo G, Strigelli V, Meccariello A, Baldini A. A staged use of tourniquet does not influence the fast-track recovery after total knee arthroplasty: a prospective randomized study. Arch Orthop Trauma Surg. 2024;144:4677–4684. doi:10.1007/s00402-024-05300-x
28. Sun Y, Zhao J, Guo W, et al. Single injection of lidocaine to reduce tourniquet hypertension in ambulatory arthroscopic patients under general anaesthesia: randomized, double-blind, placebo-controlled clinical trial. BJS Open. 2023;7. doi:10.1093/bjsopen/zrad014
29. Wahal C, Grant SA, Gadsden J, Rambhia MT, Bullock WM. Femoral artery block (FAB) attenuates thigh tourniquet-induced hypertension: a prospective randomized, double-blind, placebo-controlled trial. Reg Anesth Pain Med. 2021;46:228–232. doi:10.1136/rapm-2020-102113
30. Satsumae T, Yamaguchi H, Sakaguchi M, et al. Preoperative small-dose ketamine prevented tourniquet-induced arterial pressure increase in orthopedic patients under general anesthesia. Anesth Analg. 2001;92:1286–1289. doi:10.1097/00000539-200105000-00039
31. Sritharan K, Thompson H. Understanding the metabolic response to trauma. Br J Hosp Med. 2009;70:M156–8. doi:10.12968/hmed.2009.70.Sup10.44641
32. Mors K, Wagner N, Sturm R, et al. Enhanced pro-inflammatory response and higher mortality rates in geriatric trauma patients. Eur J Trauma Emerg Surg. 2021;47:1065–1072. doi:10.1007/s00068-019-01284-1
33. Stahel PF, Smith WR, Moore EE. Current trends in resuscitation strategy for the multiply injured patient. Injury. 2009;40 Suppl 4:S27–35. doi:10.1016/j.injury.2009.10.034
34. Glen J, Constanti M, Brohi K, Guideline Development G. Assessment and initial management of major trauma: summary of NICE guidance. BMJ. 2016;353:i3051. doi:10.1136/bmj.i3051
35. Tran A, Yates J, Lau A, Lampron J, Matar M. Permissive hypotension versus conventional resuscitation strategies in adult trauma patients with hemorrhagic shock: a systematic review and meta-analysis of randomized controlled trials. J Trauma Acute Care Surg. 2018;84:802–808. doi:10.1097/TA.0000000000001816
36. Lieberman JR, Cheng V, Cote MP. Pulmonary embolism rates following total hip arthroplasty with prophylactic anticoagulation: some pulmonary emboli cannot be avoided. J Arthroplasty. 2017;32:980–986. doi:10.1016/j.arth.2016.09.006
37. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41:543–603.
38. Pei DT, Liu J, Yaqoob M, et al. Meta-analysis of catheter directed ultrasound-assisted thrombolysis in pulmonary embolism. Am J Cardiol. 2019;124:1470–1477. doi:10.1016/j.amjcard.2019.07.040
39. Group CS, Sidhu VS, Kelly TL, et al. Effect of aspirin vs enoxaparin on symptomatic venous thromboembolism in patients undergoing hip or knee arthroplasty: the CRISTAL randomized trial. JAMA. 2022;328:719–727. doi:10.1001/jama.2022.13416
40. Rothberg DL, Makarewich CA. Fat embolism and fat embolism syndrome. J Am Acad Orthop Surg. 2019;27:e346–e55. doi:10.5435/JAAOS-D-17-00571
41. Legrand M, Falcone J, Cholley B, et al. Continuation vs discontinuation of renin-angiotensin system inhibitors before major noncardiac surgery: the stop-or-not randomized clinical trial. JAMA. 2024;332:970–978. doi:10.1001/jama.2024.17123
42. Futier E, Lefrant JY, Guinot PG, et al. Effect of individualized vs standard blood pressure management strategies on postoperative organ dysfunction among high-risk patients undergoing major surgery: a randomized clinical trial. JAMA. 2017;318:1346–1357. doi:10.1001/jama.2017.14172
43. Huang CC, Leu HB, Yin WH, et al. Optimal achieved blood pressure for patients with stable coronary artery disease. Sci Rep. 2017;7:10137. doi:10.1038/s41598-017-10628-z
44. Lee JH, Park YS, Kim MJ, et al. Clinical Frailty Scale as a predictor of short-term mortality: a systematic review and meta-analysis of studies on diagnostic test accuracy. Acad Emerg Med. 2022;29:1347–1356. doi:10.1111/acem.14493
45. Mostafa M, Hasanin A, Mostafa M, et al. Hemodynamic effects of norepinephrine versus phenylephrine infusion for prophylaxis against spinal anesthesia-induced hypotension in the elderly population undergoing hip fracture surgery: a randomized controlled trial. Korean J Anesthesiol. 2021;74:308–316. doi:10.4097/kja.20519
46. Vallee F, Passouant O, Le Gall A, et al. Norepinephrine reduces arterial compliance less than phenylephrine when treating general anesthesia-induced arterial hypotension. Acta Anaesthesiol Scand. 2017;61:590–600. doi:10.1111/aas.12905
47. Guzet F, Bitigen A, Karabay CY, Cimen AO, Teyfik N. Blood pressure control in anticoagulated hypertensive patients. Blood Press Monit. 2015;20:20–26. doi:10.1097/MBP.0000000000000084
48. Santana DC, Hadad MJ, Emara A, et al. Perioperative management of chronic antithrombotic agents in elective hip and knee arthroplasty. Medicina (Kaunas). 2021;57.
49. Jin H, He M, Yang G, et al. A retrospective study of the perioperative period management of joint arthroplasty in patients with chronic kidney disease. Orthop Surg. 2023;15:591–605. doi:10.1111/os.13589
50. Li T, Li J, Yuan L, et al. Effect of regional vs general anesthesia on incidence of postoperative delirium in older patients undergoing hip fracture surgery: the RAGA randomized trial. JAMA. 2022;327:50–58. doi:10.1001/jama.2021.22647
51. Ma J, Wang F, Wang J, et al. The effect of low-dose esketamine on postoperative neurocognitive dysfunction in elderly patients undergoing general anesthesia for gastrointestinal tumors: a randomized controlled trial. Drug Des Devel Ther. 2023;17:1945–1957. doi:10.2147/DDDT.S406568
52. Foster M, Self M, Gelber A, et al. Ketamine is not associated with more post-intubation hypotension than etomidate in patients undergoing endotracheal intubation. Am J Emerg Med. 2022;61:131–136. doi:10.1016/j.ajem.2022.08.054
53. Cosarcan SK, Gurkan Y, Dogan AT, Koyuncu O, Ercelen O. Could interscalene block possibly be protective against cerebral ischemia during shoulder surgery in a beach chair position? Cureus. 2021;13:e16773. doi:10.7759/cureus.16773
54. Hussain N, Goldar G, Ragina N, Banfield L, Laffey JG, Abdallah FW. Suprascapular and interscalene nerve block for shoulder surgery: a systematic review and meta-analysis. Anesthesiology. 2017;127:998–1013. doi:10.1097/ALN.0000000000001894
55. Peng K, Li J, Cheng H, Ji FH. Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery. Med Princ Pract. 2014;23:413–420. doi:10.1159/000363573
56. Habicher M, Balzer F, Mezger V, et al. Implementation of goal-directed fluid therapy during Hip revision arthroplasty: a matched cohort study. Perioper Med (Lond). 2016;5:31. doi:10.1186/s13741-016-0056-x
57. Giglio M, Biancofiore G, Corriero A, et al. Perioperative goal-directed therapy and postoperative complications in different kind of surgical procedures: an updated meta-analysis. J Anesth Analg Crit Care. 2021;1:26. doi:10.1186/s44158-021-00026-3
58. Chappell D, van der Linden P, Ripolles-Melchor J, James MFM. Safety and efficacy of tetrastarches in surgery and trauma: a systematic review and meta-analysis of randomised controlled trials. Br J Anaesth. 2021;127:556–568. doi:10.1016/j.bja.2021.06.040
59. Yu C, Madsen M, Akande O, Oh MY, Mattie R, Lee DW. Narrative review on postoperative pain management following spine surgery. Neurospine. 2025;22:403–420. doi:10.14245/ns.2550410.205
60. van de Wijgert IH, Fenten MGE, Rood A, van Boekel RLM, van Hooff ML, Vissers KCP. Erector spinae plane block in multimodal analgesia after lumbar spinal fusion surgery: a blinded randomized placebo-controlled trial. Anesth Analg. 2025. doi:10.1213/ANE.0000000000007611
61. Laursen CCW, Lunn TH, Hagi-Pedersen D, et al. Recommended use of non-steroidal anti-inflammatory drugs for pain treatment following primary total hip and knee arthroplasties in Denmark. A National Survey. Acta Anaesthesiol Scand. 2025;69:e70055. doi:10.1111/aas.70055
62. Meidert AS, Nold JS, Hornung R, Paulus AC, Zwissler B, Czerner S. The impact of continuous non-invasive arterial blood pressure monitoring on blood pressure stability during general anaesthesia in orthopaedic patients: a randomised trial. European Journal of Anaesthesiology. 2017;34:716–722. doi:10.1097/EJA.0000000000000690
63. Balzer F, Habicher M, Sander M, et al. Comparison of the non-invasive Nexfin® monitor with conventional methods for the measurement of arterial blood pressure in moderate risk orthopaedic surgery patients. The Journal of International Medical Research. 2016;44:832–843. doi:10.1177/0300060516635383
64. Berkelmans GFN, Kuipers S, Westerhof BE, Spoelstra-de Man AME, Smulders YM. Comparing volume-clamp method and intra-arterial blood pressure measurements in patients with atrial fibrillation admitted to the intensive or medium care unit. J Clin Monit Comput. 2018;32:439–446. doi:10.1007/s10877-017-0044-9
65. Bergholz A, Grüßer L, Khader W, et al. Personalized perioperative blood pressure management in patients having major non-cardiac surgery: a bicentric pilot randomized trial. J Clin Anesth. 2025;100:111687. doi:10.1016/j.jclinane.2024.111687
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.